Back to Journals » Advances in Medical Education and Practice » Volume 16
Exploring “Service” versus “Education” in Anesthesiology Postgraduate Medical Training: Getting Answers but Not Always Asking the Right Questions
Authors Leng JC, Allen BFS, Li J ![]() , Schatman ME
, Schatman ME ![]() , Mariano ER
, Mariano ER ![]()
Received 19 September 2025
Accepted for publication 16 October 2025
Published 1 November 2025 Volume 2025:16 Pages 2025—2028
DOI https://doi.org/10.2147/AMEP.S568798
Checked for plagiarism Yes
Editor who approved publication: Dr Sateesh Arja
Jody C Leng,1,2 Brian FS Allen,3 Jinlei Li,4 Michael E Schatman,5,6 Edward R Mariano1,2
1Anesthesiology, Perioperative and Pain Medicine Service, Veterans Affairs Palo Alto Health Care System, Palo Alto, CA, USA; 2Department of Anesthesiology, Perioperative and Pain Medicine, Stanford University School of Medicine, Stanford, CA, USA; 3Department of Anesthesiology, Vanderbilt University Medical Center, Nashville, TN, USA; 4Department of Anesthesiology, Yale University School of Medicine, New Haven, CT, USA; 5Department of Anesthesiology, Perioperative Care and Pain Medicine, NYU Grossman School of Medicine, New York, NY, USA; 6Department of Population Health – Division of Medical Ethics, NYU Grossman School of Medicine, New York, NY, USA
Correspondence: Edward R Mariano, Anesthesiology, Perioperative and Pain Medicine Service, Veterans Affairs Palo Alto Health Care System, Palo Alto, CA, USA, Email [email protected]
Postgraduate medical education is a required phase of training for physicians in the United States, who wish to be licensed by their states to practice clinically. Its mandatory nature creates a natural tension, and the design of these programs has been a source of debate between educators and trainees for over a century. In anesthesiology, the first academic residency program was started at the University of Wisconsin by Dr. Ralph Waters,1 and graduates of this program led to the establishment of anesthesiology residency programs across the country. Until the 1980s, anesthesiology residency was limited to 3 postgraduate training years: a clinical base year (ie internship) followed by two specialized clinical anesthesiology years; the third clinical anesthesiology year (ie “CA-3”) was then added with restructuring of the curriculum to include training in subspecialty areas.2
Where is anesthesiology residency training today? Not including the clinical base year and optional fellowship, clinical anesthesiology residency is of 3 years duration. This period of focused clinical training is 1095 days, or 26,280 hours, without subtracting time off for leave and academic activities, and has been of the same duration for the past 40 years despite the rapid growth in surgical and noninvasive procedures, patient complexity, perioperative optimization, technological development, and published research. Each accredited training program in the United States must meet robust clinical and didactic education standards as established and overseen by the national Accreditation Council for Graduate Medical Education (ACGME)3 to ensure the appropriate training of upcoming generations of physicians capable of tackling ongoing medical discovery and advancements throughout their careers.
A study by Li et al4 offers a framework for classifying routine anesthesiology trainee activities and their perceived educational value derived from surveying residents, fellows, and faculty within one academic anesthesiology department. Using a validated survey and latent factor analysis, the authors delineate three distinct domains for training activities in anesthesiology: mandatory training-related obligations (eg, medical record and ACGME record documentation) that were associated with the least educational value, procedural responsibilities (eg, arterial line placement, epidural analgesia), and classroom activities (eg, simulation, mock oral exam) that were associated with higher educational value. These domains echo similar patterns observed in other specialties such as pediatrics, emergency medicine, and surgery.5–7
Similar to the ACGME annual resident and faculty surveys, the study by Li et al4 establishes a dichotomy between service and educational activities in resident training. If there is an option to label an activity as “service”, there must be items on the list that are not educational. This powerful suggestion may be akin to the phenomenon of “nocebo”, which has been well-described in pain research and clinical medicine.8,9 In anesthesiology, nocebo can be observed when a skin puncture is preempted with “this will feel like a bee sting”, and the patient, not surprisingly, anticipates a painful stimulus and reacts accordingly.10 Can simply asking a question about “service” versus “education” regarding anesthesiology training predispose the respondent to assume that certain activities must be non-educational? As service-oriented professional obligations are often not the focus of standardized tests or assessments, they can be overlooked and underappreciated by learners, as demonstrated by a Swedish study highlighting different concepts of gaining competency in anesthesiology.11
While the questions seem simple to answer, we posit that a physician’s classification of an activity on the scale between service and education is a complex summation of perceived value, necessity, difficulty, and appropriateness of that task. The components of this “service versus education” calculus and the change in perception based on postgraduate year-in-training elucidated by Li et al4 map closely to the concepts of Cognitive Load Theory (CLT) in medical education (Figure 1).
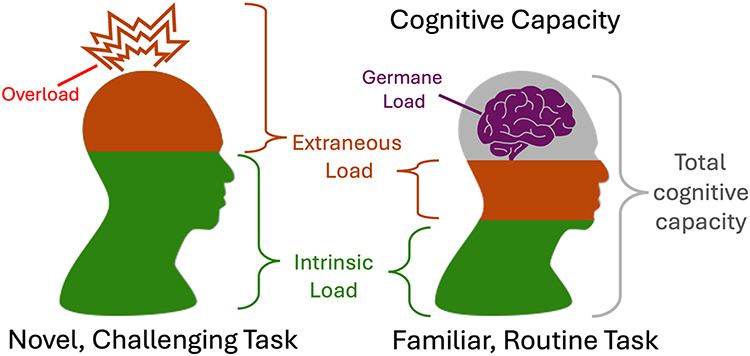 |
Figure 1 The transition from an early learner in anesthesiology to an experienced learner or faculty anesthesiologist using the model of cognitive load theory. |
This theory posits that individuals possess a finite amount of working memory that may be employed when performing tasks.12 CLT suggests that tasks have both an intrinsic cognitive component associated with the task itself and an extraneous load reflecting the environment or other external factors. Consider the example of a new driver versus one with many years of experience and the ability of each to focus on casual conversation during a freeway lane change. In Li et al,4 many of the surveyed tasks that correspond more toward service (such as those of the mandatory training related obligations) are associated with extraneous factors such as medical record documentation, patient transport, poor supervision, fatigue, time pressure, and distraction. CLT suggests that when intrinsic and extraneous load exceeds cognitive capacity, overload occurs and tasks feel overwhelming, unpleasant, or unsafe.
With practice and deliberate effort, tasks are expected to require less intrinsic load, while extraneous factors may be more favorably managed. The concept of germane load (Figure 1), the amount of cognitive capacity allocated to learning, comes into play when the sum of intrinsic and extraneous load is less than the amount of cognitive capacity available, and new information can be integrated into long term memory. In other words, germane load is the positive form of cognitive load for learners that we strive to achieve in graduate medical education. In Li et al,4 the procedural responsibilities (airway management, epidural placement) and classroom activities (problem-based learning, grand rounds) are more likely to be the intrinsic load at the beginning of anesthesia training, and with time, an increasing portion becomes germane load, thus the transition from a junior trainee to an experienced anesthesiologist (Figure 1).
The cognitive load of performing the many tasks required of an anesthesiologist decreases with experience and ideally transitions from overload to germane over time. Perhaps, this explains the survey differences observed between trainees and faculty educators in Li et al:4 more seasoned physicians recognize the nuanced educational value in routine tasks such as postoperative patient transport, whereas early trainees may still be more focused on learning fundamental medical knowledge topics required for upcoming exams. If so, CLT suggests methods by which even highly service-oriented tasks can be transformed into educational opportunities. For example, extraneous load may be reduced by optimizing the learning environment, performance pressure, and adequate supervision.13 In the study by Li et al,4 learners, more so than faculty, reported that factors such as fatigue, high caseload and poor supervision substantially eroded the educational value of otherwise meaningful tasks.14 These findings are consistent with broader evidence linking a positive learning climate to academic performance and learner well-being.15
Further, educators may choose to address and reframe the presentation of activities that are perceived to be of low educational value.16 For example, nighttime call duties could be reframed as deliberate practice in clinical decision-making and emergency management with less direct supervision, enhanced by targeted feedback and debriefings. It is worth noting that the ratings by senior trainees in the study by Li et al4 aligned more closely with faculty than among more junior residents.4
Although a career in medicine involves lifelong learning, every aspect is not educational all the time, and mundane tasks certainly exist at all levels of medical training and practice. While Li et al4 suggest that many service responsibilities may become educational opportunities if thoughtfully structured, some tasks should be rightfully reconsidered to offload the weight of system inefficiencies on trainees. Documentation burdens such as case log entry may be mitigated with technological advances such as ACGME database integration with the electronic medical record, a solution that is already feasible.17 Preoperative transport of healthy patients to the operating room can be performed by nonphysicians and allow resident and practicing anesthesiologists additional time for anesthetic preparation and short breaks between cases. Teaching hospitals should continue to reevaluate and redesign their systems for healthcare delivery to maximize clinical education while still ensuring that necessary patient care activities are performed using available resources.
Ultimately, postgraduate medical education is training for real life clinical practice and should prepare trainees for a long, fulfilling career in medicine. Assessing professional fulfillment is difficult, but one published scale includes the following domains: feeling happy; feeling worthwhile; work is satisfying; feeling in control when dealing with difficult problems; work is meaningful; and contributing professionally.18 Anesthesiology is a unique specialty in which the physician has direct second-to-second responsibility for the medical care, safety, and wellbeing of another human, and there is an almost infinite range of activities that can fall within this purview. Although the anesthesiologist, whether in training or in practice, will invariably perform activities that may not always have obvious educational value, perhaps the performance itself in the care of a patient can contribute to at least one of these domains of professional fulfillment.
Disclosure
Dr Michael Schatman is the senior medical advisor for Apurano Pharma. The authors report no other conflicts of interest in this work.
References
1. Ahmad M, Tariq R. History and evolution of anesthesia education in United States. J Anesth Clin Res. 2017;8(6):734. doi:10.4172/2155-6148.1000734
2. Shapiro DM, Hargett MJ, Kopp S, Neal JM, Mariano ER, Liguori G. History and evolution of regional anesthesiology and acute pain medicine fellowship training. Reg Anesth Pain Med. 2020;45(4):311–314. doi:10.1136/rapm-2019-100915
3. ACGME. ACGME program requirements for graduate medical education in anesthesiology. Available from: https://www.acgme.org/globalassets/pfassets/programrequirements/040_anesthesiology_2023.pdf.
4. Li J, Lin HM, Yanez ND, He Z, Treggiari MM, Kurup V. “Service” versus “education” in anesthesiology: domain classification of activities based on perceptions from learners and teachers. Adv Med Educ Pract. 2025;16:1359–1369. doi:10.2147/AMEP.S527329
5. Kesselheim JC, Sun P, Woolf AD, London WB, Boyer D. Balancing education and service in graduate medical education: data from pediatric trainees and program directors. Acad Med. 2014;89(4):652–657. doi:10.1097/ACM.0000000000000174
6. Quinn A, Brunett P. Service versus education: finding the right balance: a consensus statement from the Council of Emergency Medicine Residency Directors 2009 Academic Assembly “Question 19” working group. Acad Emerg Med. 2009;16(Suppl 2):S15–8. doi:10.1111/j.1553-2712.2009.00599.x
7. Reines HD, Robinson L, Nitzchke S, Rizzo A. Defining service and education: the first step to developing the correct balance. Surgery. 2007;142(2):303–310. doi:10.1016/j.surg.2007.04.011
8. Tu Y, Zhang L, Kong J. Placebo and nocebo effects: from observation to harnessing and clinical application. Transl Psychiatry. 2022;12(1):524. doi:10.1038/s41398-022-02293-2
9. Jensen KB, Kaptchuk TJ, Kirsch I, et al. Nonconscious activation of placebo and nocebo pain responses. Proc Natl Acad Sci U S A. 2012;109(39):15959–15964. doi:10.1073/pnas.1202056109
10. Arrow K, Burgoyne LL, Cyna AM. Implications of nocebo in anaesthesia care: a reply. Anaesthesia. 2022;77(8):946. doi:10.1111/anae.15758
11. Chin H, Ingerman A, Herges HO. Anesthesiologists’ conceptions of learning anesthesia in the context of their specialty training program: a phenomenographic study. BMC Med Educ. 2023;23(1):594. doi:10.1186/s12909-023-04573-x
12. Howie EE, Dharanikota H, Gunn E, et al. Cognitive load management: an invaluable tool for safe and effective surgical training. J Surg Educ. 2023;80(3):311–322. doi:10.1016/j.jsurg.2022.12.010
13. Young JQ, Van Merrienboer J, Durning S, Ten Cate O. Cognitive load theory: implications for medical education: AMEE Guide No. 86. Med Teach. 2014;36(5):371–384. doi:10.3109/0142159X.2014.889290
14. Sewell JL, Boscardin CK, Young JQ, Ten Cate O, O’Sullivan PS. Learner, patient, and supervisor features are associated with different types of cognitive load during procedural skills training: implications for teaching and instructional design. Acad Med. 2017;92(11):1622–1631. doi:10.1097/ACM.0000000000001690
15. Ahmady S, Khajeali N, Sharifi F, Mirmoghtadaei ZS. Factors related to academic failure in preclinical medical education: a systematic review. J Adv Med Educ Prof. 2019;7(2):74–85. doi:10.30476/JAMP.2019.44711
16. Tokuno J, Carver TE, Fried GM. Measurement and management of cognitive load in surgical education: a narrative review. J Surg Educ. 2023;80(2):208–215. doi:10.1016/j.jsurg.2022.10.001
17. Wanderer JP, Charnin J, Driscoll WD, Bailin MT, Baker K. Decision support using anesthesia information management system records and accreditation council for graduate medical education case logs for resident operating room assignments. Anesth Analg. 2013;117(2):494–499. doi:10.1213/ANE.0b013e318294fb64
18. Trockel M, Bohman B, Lesure E, et al. A brief instrument to assess both burnout and professional fulfillment in physicians: reliability and validity, including correlation with self-reported medical errors, in a sample of resident and practicing physicians. Acad Psychiatry. 2018;42(1):11–24. doi:10.1007/s40596-017-0849-3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.