Back to Journals » Journal of Pain Research » Volume 15
Exploring Psychoneurological Symptom Clusters in Acute Stroke Patients: A Latent Class Analysis
Authors Dong X ![]() , Yang S, Guo Y, Lv P, Liu Y
, Yang S, Guo Y, Lv P, Liu Y
Received 26 November 2021
Accepted for publication 10 March 2022
Published 25 March 2022 Volume 2022:15 Pages 789—799
DOI https://doi.org/10.2147/JPR.S350727
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jonathan Greenberg
Xiaofang Dong,1 Sen Yang,2 Yuanli Guo,1 Peihua Lv,1 Yanjin Liu1
1Neurology Department, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan Province, People’s Republic of China; 2Orthopedics Department, The Seventh People’s Hospital of Zhengzhou, Zhengzhou, Henan Province, People’s Republic of China
Correspondence: Yanjin Liu, Neurology Department, The First Affiliated Hospital of Zhengzhou University, No. 1 Eastern Jianshe Road, Zhengzhou, Henan, 450052, People’s Republic of China, Tel +86 13523548732, Email [email protected]; [email protected]
Purpose: To identify latent classes of acute stroke patients with distinct experiences with the symptom clusters of depression, anxiety, fatigue, sleep disturbance, and pain symptoms and assess, if the selected variables determine a symptom-cluster experience in acute stroke patients.
Participants and Methods: A sample of 690 participants were collected from July 2020 to December 2020 in a cross-sectional descriptive study. Latent class analysis was conducted to distinguish different clusters of acute stroke participants who experienced five patient-reported symptoms. Furthermore, multinomial logistic regression was selected to verify the influencing indicators of each subgroup, with selected socio-demographic variables, clinical characteristics, self-efficacy, and perceived social support as independent variables and the different latent classes as the dependent variable.
Results: Three latent classes, named “all high symptom,” “high psychological disorder,” and “all low symptom,” were identified, accounting for 9.6%, 26.3%, and 64.1% of symptom clusters, respectively. Patients in the “all high symptom” and “high psychological disorder” classes reported significantly lower quality of life (F=40.21, p < 0.05). Female gender, younger age, higher National Institutes of Health Stroke Scale scores, and lower self-efficacy and perceived social support were risk factors associated with the “high psychological disorder” class. Younger patients with lower self-efficacy and perceived social support were more likely to be in the “all high symptom” class.
Conclusion: This study identified latent classes of acute stroke patients that can be used in predicting symptom-cluster experiences following a stroke. Also, the ability to characterize subgroups of patients with distinct symptom experiences helps identify high-risk patients. Focusing on symptom clusters in clinical practice can inspire us to create effective targeted interventions for subgroups of stroke patients suffering from the same symptom cluster.
Keywords: pain, fatigue, sleep disturbance, anxiety, depression
Introduction
Stroke is one of the common chronic diseases that seriously threatens human health and is characterized by high morbidity, recurrence, mortality, disability, and disease burden. Globally, stroke is currently the second leading cause of death and long-term disability,1 with more than 400,000 survivors living with complications.2 There are about 7.5 million stroke patients in China, increasing by an estimated 2.5 million people every year.3 About 75–80% of stroke survivors have varying degrees of dysfunction, and the recurrence rate of the disease within 5 years is as high as 40.0%.4 The WHO and Harvard University’s Global Burden of Disease Project introduced the concept of disability-adjusted life years (DALYs),5 or the total healthy life years lost from morbidity to death. The project report shows that stroke DALYs rank First among chronic diseases, suggesting a severe disease burden.
Stroke patients commonly experience symptoms of depression, anxiety, fatigue, sleep disturbance, and pain, collectively known as psychoneurological (PN) symptoms, more often simultaneously rather than in isolation,6–8 which not only impact stroke patients during their hospitalization but may also exist persistently at the stage of rehabilitation. The prevalence rates of post-stroke depression, anxiety, fatigue, sleep disturbance, and pain after stroke have been reported as 20.0–65.0%,9 24.8–33.8%,10 43.0–57.0%,11 30.1–46.5%,12 and 18.0–35.0%,13 respectively. Although often co-occurring, these PN symptoms are usually diagnosed, treated, and managed separately. In addition, people experiencing concurrent symptoms suffer poorer quality of life (QOL) than those with only one in other kinds of diseases.14 Thus, considering symptoms as a cluster can assist clinical medical staff in taking more targeted interventions.15
Despite the rapid growth in the symptom cluster field, previous studies have mainly targeted patients with various tumour types,16,17 chronic obstructive pulmonary disease (COPD),18 and heart failure.19 Although some advances have been made regarding PN symptom clusters in stroke patients,20 it is still unknown to us which kinds of stroke patients are prone to report a special PN symptom cluster. Furthermore, PN symptom studies in recent years on stroke patients have limited generalizability due to small sample sizes.21 In addition, the ever-changing PN symptoms may be relatively more diverse and critical during active treatment, such as during the acute phase. Thus, it may be helpful to discuss PN symptoms using reliable patient-reported outcome measures in conjunction with latent class analysis (LCA) at the acute phase.
The Theory of Unpleasant Symptoms (TOUS) includes three core concepts: symptoms, influential factors, and performance.22 Symptoms are a multi-dimensional concept, including four common dimensions: intensity, timing, distress, and quality. Each symptom and its dimensions can exist alone or in combination with other symptoms. Co-occurrences exist in clusters, and their impact on individuals is far greater than that of individual symptoms. The influencing factors mainly include physiological factors (such as age, gender, structural abnormalities, etc.), psychological factors (emotional variables and cognitive variables), and environmental factors (social environmental factors and physical environmental factors). The performance results include two aspects: functional activity and cognitive activity. The more severe the symptoms, the worse the performance outcome, such as the lower QOL. The TOUS is suitable for our research because it clearly defines the concept of symptom clusters, influencing factors, and outcomes of symptom clusters.23
Hence, our research goals were to determine different subgroups of stroke patients with PN symptoms in the acute phase; to assess differences in socio-demographic, clinical characteristics, self-efficacy, and perceived social support among these subgroups; and compare the differences in QOL between latent symptom cluster classes.
Participants and Methods
Design and Participants
This was a cross-sectional descriptive study. Data collection was from July 2020 to December 2020. The inclusion criteria were: (a) stroke diagnosed within 1 month prior, (b) ≥18 years old, (c) able to read and write independently and participate in this research voluntarily. We excluded participants with additional tumours or severe diseases and those who were unconscious, uncooperative, or had cognitive dysfunction.
Data Collection
The research was approved by the Ethical Committee of the First Affiliated Hospital of Zhengzhou University. Stroke patients admitted to the hospital in the acute phase were recruited for this study in the neurology wards of the comprehensive teaching hospital from July 2020 to December 2020. Data collection was completed by five postgraduate nursing students who had received strict and unified training (eg, aims of the research, rule of confidentiality, and assessing the quality of questionnaires). A pilot study was conducted 1 week before formal data collection to test the feasibility. On the morning of the data collection day, informed consent were obtained from the eligible participants. The five investigators conducted a face-to-face, one-to-one data collection method using the translated Chinese version of the instruments. The survey sites were set in the meeting rooms of the neurology departments to avoid interference. For bed-ridden patients, the surveys were conducted at their bedsides. The interviewers read and explained some items for those participants who had difficulty understanding the questionnaire and checked for its completeness. Clinical characteristics, including National Institutes of Health Stroke Scale (NIHSS) scores, Modified Rankin Scale (mRS), and infarct size, were recorded according to medical records after getting permission from the hospital.
Sample Size
According to the principle of calculating sample sizes for cross-sectional descriptive studies, a sample 5–10 times the number of independent variables was selected.24 Sample size was 690 taking into account the 10% dropout rate.
Measurements
Socio-Demographic and Clinical Characteristics
Socio-demographic variables, including age, gender, marital status, living situation, level of education, and place of residence, were self-reported. Clinical characteristics, such as the NIHSS score and the mRS, were acquired from the patients’ electronic medical records.
Numeric Rating Scale
The numeric rating scale (NRS) is a simple and realistic pain assessment method in clinical and scientific research. Participants were asked to assign a number from 0 to 10 to their pain during rest and activity. The Cronbach’s α is 0.973 for the stroke patients.
Fatigue Severity Scale
The 9-item fatigue severity scale (FSS) is divided into fatigue experience, fatigue triggers, and interference with everyday life. The final score of this 7-point Likert-type scale is the average of all item scores, with a higher score indicating worse fatigue.25 A score greater than 4 was diagnosed as fatigue. The FSS is a reliable and valid instrument that can be used to assess fatigue problem in Chinese patients.26 In this study, the Cronbach’s α was 0.928.
Hospital Anxiety and Depression Scale
The 14-item Hospital Anxiety and Depression Scale (HADS) is often used to assess the psychological status of patients or diagnose anxiety and depression,27 and is divided into 7-item anxiety and depression subscales. The total score of the 4-point Likert-type scale is the summation of each subscale’s items. The score for each subscale was assessed as negative, mild, moderate, and severe;27 the scale showed good psychometric properties in China.28 The Cronbach’s α of our research was 0.907.
Pittsburgh Sleep Quality Index
The Pittsburgh Sleep Quality Index (PSQI) is a self-report scale to evaluate subjective sleep quality over the past half month.29 The scale comprises 19 self-rating items and five items assessed by medical staff. The PSQI score ranges from 0 to 21. In this study, a total score <7 indicated good sleep, and a total score ≥7 was considered a sleep disorder. Chinese version of the PSQI demonstrated good psychometric properties.30 The Cronbach’s α of our research was 0.895.
Self-Efficacy for Managing Chronic Diseases
The 6-item Self-Efficacy for Managing Chronic Diseases (CDSES) scale assesses an individual’s confidence in their capability to handle fatigue, pain, mood problems, and other symptoms with self-management skills.31 The score of each item is from 1 to 10, where 1 is “not at all confident,” and 6 is “totally confident.” The scale has demonstrated well psychometric properties in Chinese patients,32 and the Cronbach’s α was 0.896.
Perceived Social Support Scale
The 12-item Perceived Social Support Scale (PSSS) assesses one’s support by family, friends, and others.33 The highest score of this 7-point Likert-type scale is 84, and higher scores mean better perceived social support. The Chinese version has presented impressive psychometric properties and the Cronbach’s α is 0.905 in stroke patients.34
Stroke Impact Scale
The 59-item Stroke Impact Scale (SIS) assesses strength, hand function, activities of daily living (ADLs), mobility, communication, emotion, memory, and social participation, with higher scores indicating greater QOL.35 The Cronbach’s α was 0.820 in our research.
Statistical Analyses
Data analyses were conducted with SPSS 21.0 and Mplus 7.4. Descriptive analysis, variance analysis, chi-square tests, and multiple logistic regression analysis were performed with SPSS 21.0, while LCA was carried out using Mplus 7.4. All data were checked for normality, and statistical significance was established at p <0.05.
First, LCA was used to distinguish subgroups of acute stroke patients who experienced PN symptoms. The Akaike information criterion (AIC), Bayesian information criterion (BIC), entropy, Lo-Mendell-Rubin adjusted likelihood ratio test (LMRT), and bootstrapped likelihood ratio test (BLRT) were used to assess the optimal number of latent classes.36 AIC and BIC are the most important indicators to assess the best model; the smaller the value, the better the model. Second, variance analysis and chi-square tests were chosen to test various socio-demographic and clinical variables among different subgroups. Then, Multinomial logistic regression was selected to verify the influencing indicators of each subgroup, with selected socio-demographic variables, clinical characteristics, self-efficacy, and perceived social support as independent variables and the different latent classes as the dependent variable.
Results
Sample Characteristics
In total, 660 individuals completed the data collection effectively, providing a 95.65% questionnaire response rate (Table 1). The participants were predominantly male (54.1%), younger (64.1%), married (89.1%), living in a rural area (65.5%), and living with others (79.5%), with one-third of them having at least a junior high school diploma (34.1%). The mean CDSES and PSSS scores were 41.70 (SD 16.65) and 50.54 (SD 13.86), respectively.
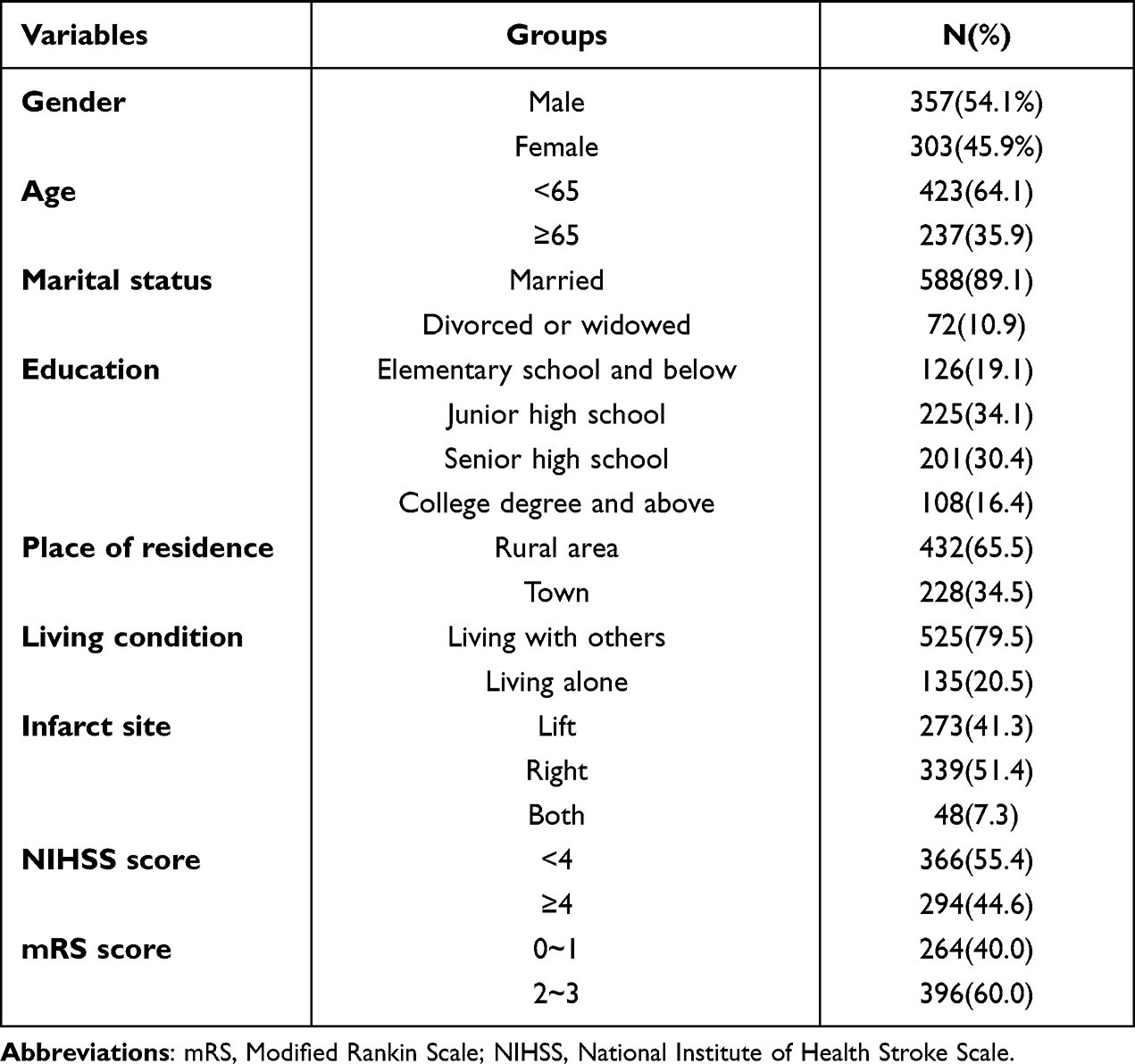 |
Table 1 Characteristics of the Sample (N=660) |
Identification of PN Symptom Clusters
Three subgroups of patients were identified with LCA indicators. Compared to other models, Model 3 was the best, owing to smaller AIC and BIC values and the highest entropy value. LMRT (p <0.05) and BLRT (p <0.05) were statistically significant for this model (Table 2). PN symptoms were classified into three latent classes, experienced by 9.6%, 26.3%, and 64.1% of patients (Figure 1). PN symptoms clusters were labelled according to scores of depression, anxiety, fatigue, sleep disturbance, and pain. Clinically, pain, fatigue, sleep disturbance, depression, and anxiety were high in Class 1, labelled the “all high symptom” class. Class 2 had a moderate level of pain, sleep disturbance, and fatigue but a relatively high level of depression and anxiety; this group was labelled the “high psychological disorder” class. At the same time, the scores of five symptoms were below in Class 3, labelled the “all low symptom” class.
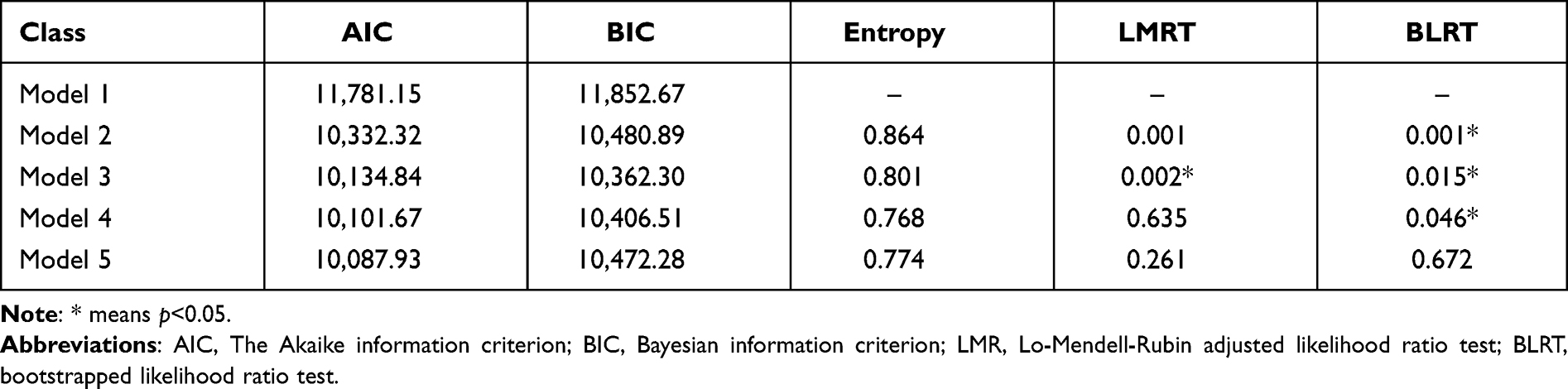 |
Table 2 Fit Indices of LCA for Psychoneurological Symptom Cluster |
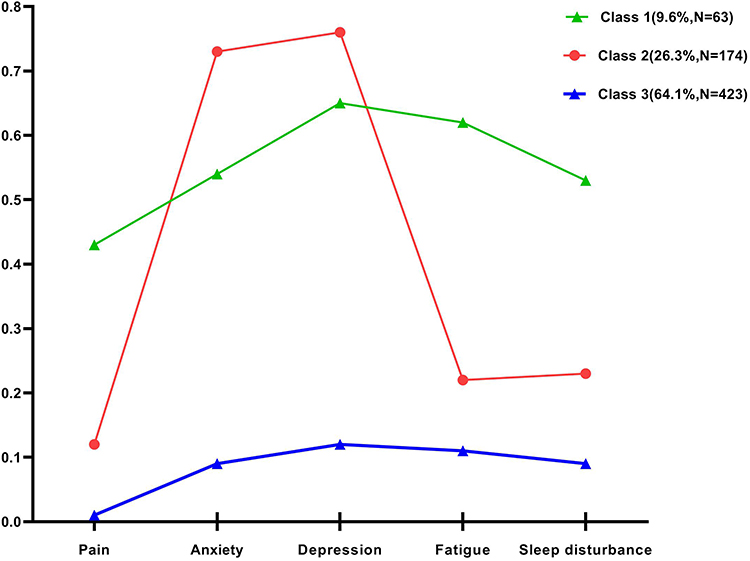 |
Figure 1 Differences in the three symptom classes. |
Socio-Demographic and Clinical Variables and Symptom Clusters
Age, gender, living condition, NIHSS score, PSSS score, and CDSES score were statistical significance between three classes (Table 3), which were retained in the multinomial logistic regression. Predictors for the “high psychological disorder” and “all high symptom” classes are demonstrated below.
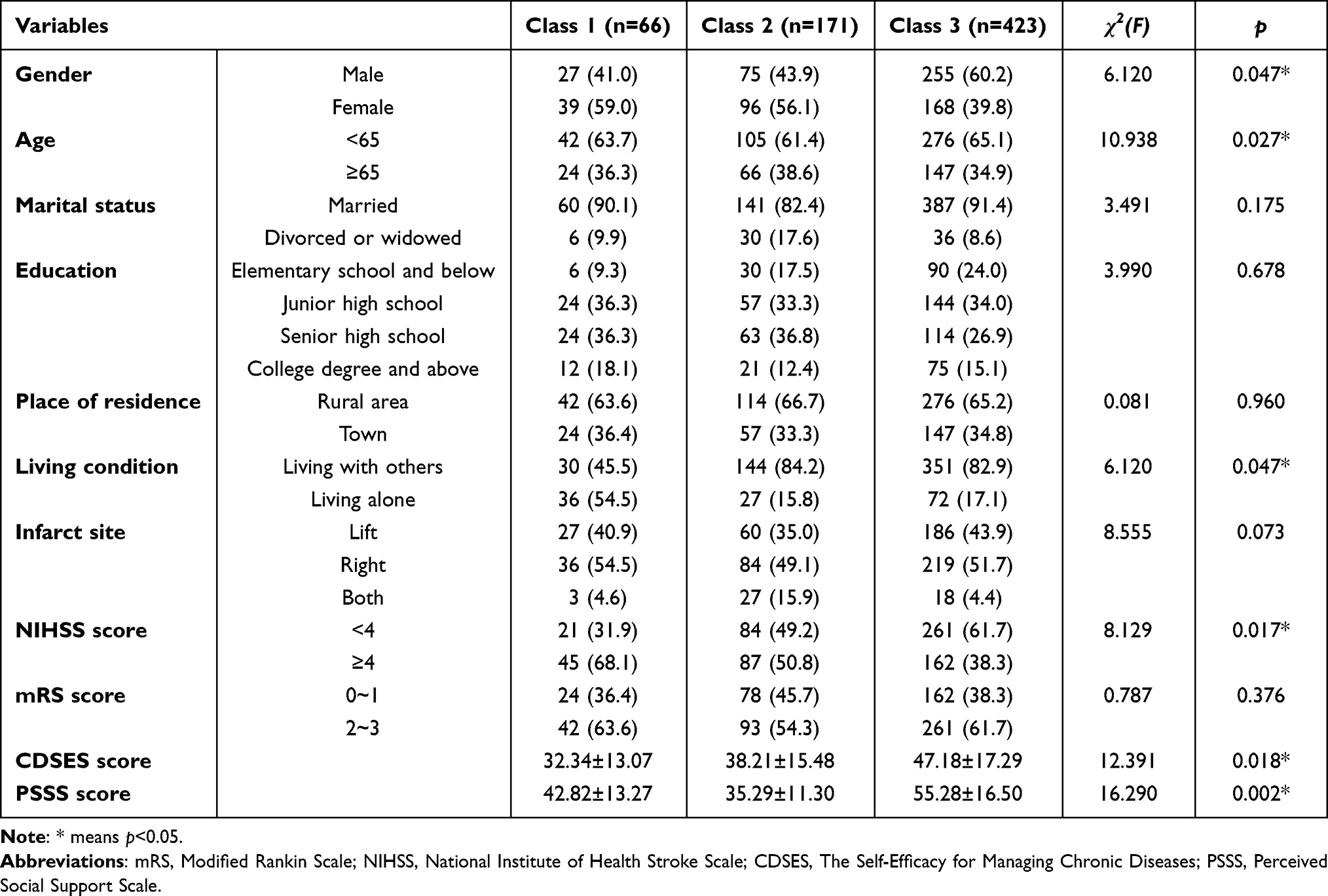 |
Table 3 Different in Socio-Demographic and Clinical Characteristics Among the Latent Classes (n=660) |
Comparison of Class 1 versus Class 3: Younger age (less than 65 years), lower self-efficacy, and lower perceived social support were risk factors for the “all high symptom” cluster compared to the “all low symptom” cluster (Table 4). Younger patients were more likely to be in Class 1 [odds ratio (OR)=1.505, 95% confidence interval (CI): 1.044–2.170]. In addition, patients with higher self-efficacy and perceived social support were less likely to be in Class 1.
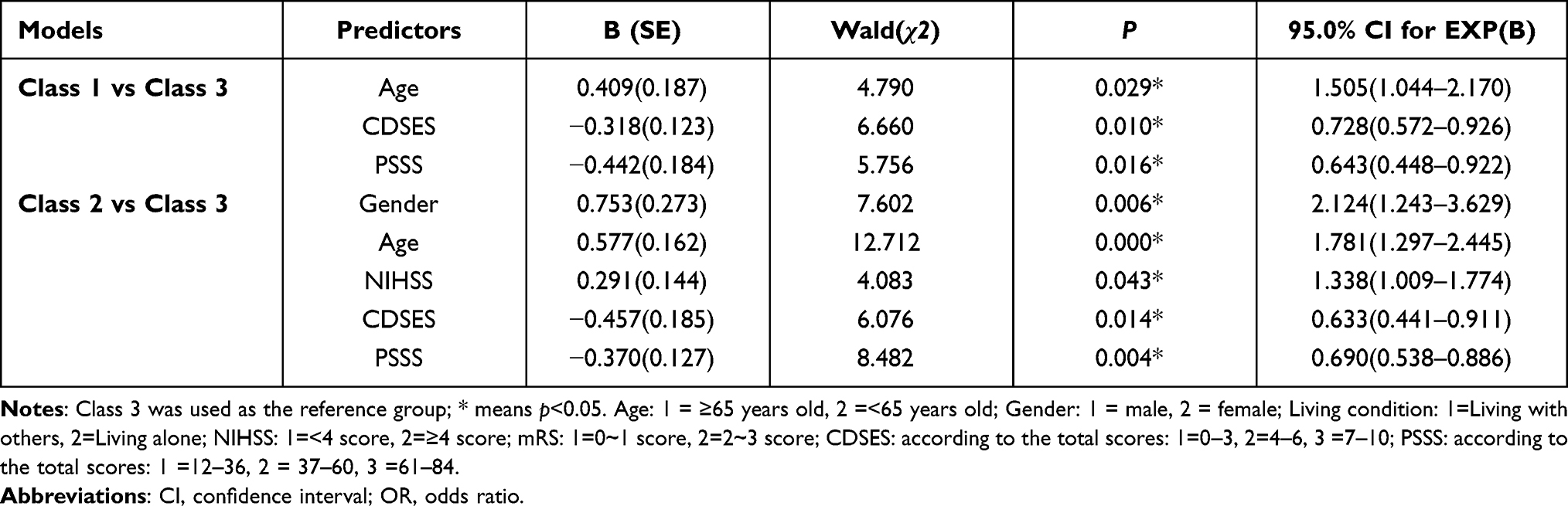 |
Table 4 Predicting About Three Latent Classes of Psychoneurological Symptom Cluster |
Comparison of Class 2 versus Class 3: The indicators that can be used to distinguish and predict the “ high psychological disorder” class were female (OR=2.124, 95% CI:1.243–3.629), younger age group (OR=1.781,95% CI:1.297–2.445), higher NIHSS score (OR=1.338,95% CI:1.009–1.774), lower self-efficacy score (OR=0.633, 95% CI:0.441–0.911), and perceived social support score (OR=0.690, 95% CI:0.538–0.886).
Differences in Quality of Life
QOL differences among different clusters are shown in Table 5. The results are consistent with expectations; the “all low symptom” class had the best QOL scores, followed by the “high psychological disorder” and “all high symptom” classes. Those in the “all low symptom” class showed better function and higher QOL than those in the “all high symptom” and “high psychological disorder” classes.
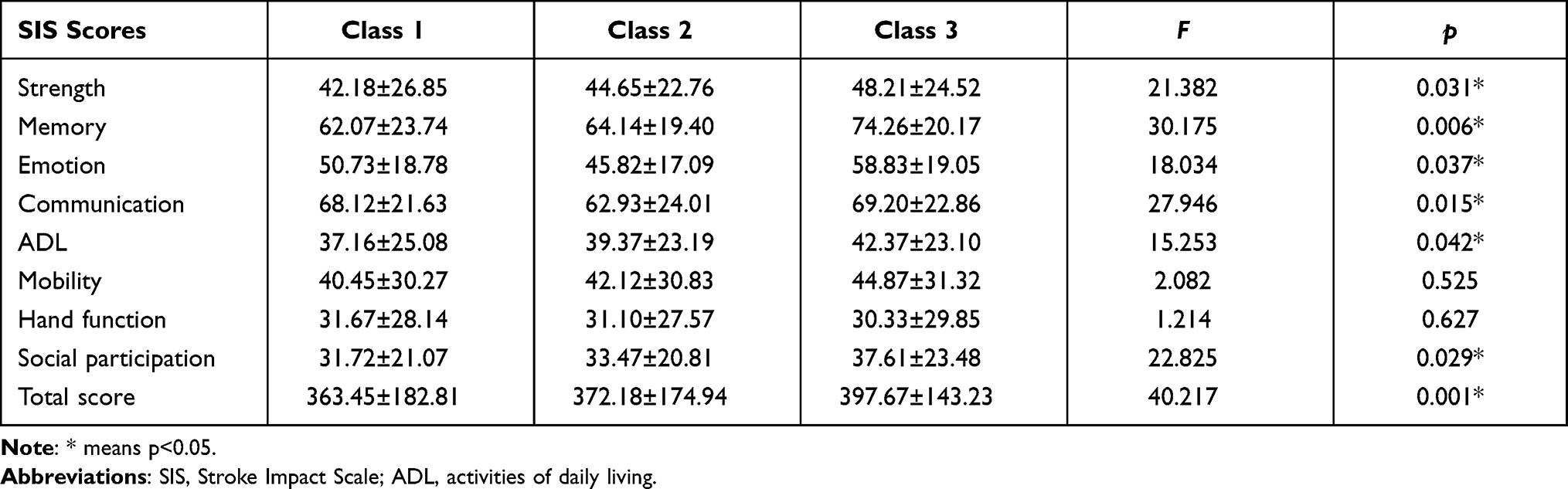 |
Table 5 Differences in Quality of Life Scores Among the Latent Classes (N=660) |
Discussion
Identification of PN Symptom Clusters
Patients with acute stroke usually suffer from depression, anxiety, fatigue, sleep disturbance, and pain, resulting from sudden stroke onset, invasive operation, change of environment, or concurrent complications. According to the core concepts of TOUS, the more severe the symptoms, the worse the performance outcome, such as the lower QOL. As a result, medical workers need to recognize different subgroups of PN symptoms and identify the predictors. Also, it is necessary to compare the QOL among different clusters. However, very few studies have explicitly tested the influence of socio-demographic variables, clinical characteristics, self-efficacy and perceived social support on symptoms patterns among stroke patients,20 and none have studied the influence of such variants on PN symptom clusters. To our knowledge, the current study is the first to explore PN symptom clusters and to examine the relationships between symptom clusters and QOL in patients with stroke.
It is interesting to note that three relatively different classes of participants were determined, namely those who showed low scores in all symptoms (64.1%), those who reported high depression and anxiety with low scores in other symptoms (26.3%), and those who reported high levels of all five symptoms (9.6%). Other studies have identified symptom clusters in breast cancer survivors, heart failure patients, colon cancer patients, and COPD patients. However, the number and type of symptom clusters are quite different from previous studies. Wong’s study found that neuropsychiatric symptom clusters in stroke and transient ischemia were divided into “behavioural problems cluster”, “psychosis cluster”, “mood disturbance cluster”, and “euphoria cluster” using confirmatory factor analysis.20 Also, LCA classified cancer patients with PN symptoms into “the all-high-symptom subgroup” and “all-low-symptom subgroup”.37 Differences among studies may be related to differences in demographic and clinical characteristics of the study population, inclusion and exclusion criteria, and diseases and statistical methodology.
Factors Associated with Symptom Clusters
Younger patients (less than 65 years old) were more likely to be in the “high psychological disorder” as well as “all high symptom” clusters. Younger stroke patients suffer from more serious PN symptoms than those in older patients, which is in line with other studies.38,39 Because people in this age group bear many social responsibilities and family burdens, such as raising families and career development, the damage caused by stroke to the patient’s body and spirit and the impact on the family and society are even more serious. In addition, female patients constitute a much larger percentage than males in the “high psychological disorder” class, indicating that female sex is a risk factor for PN symptoms. Also, a high NIHSS score was identified as an independent risk factor. This may be related to societal roles of females in the family, excessive housework, rejection and discrimination in social status, and insufficient coping ability, which may cause psychological disorders after a sudden heavy stroke.40 Thus, medical staff should pay more attention to younger female stroke survivors with higher NIHSS scores who are more likely to have psychological health problems.
In addition, stroke patients with lower perceived social support are more likely to be in the “high psychological disorder” and “all high symptom” classes, illustrating that higher perceived social support is a protective factor for PN symptoms after acute stroke, which is in line with other studies.41 According to the stress buffer theory, social support can buffer the adverse effects (eg, sudden stroke, self-care limitation, medical expenses) of the disease on patients and is regarded as an important external factor in promoting physical, psychological, and social health of patients. Once there is a decrease in perceived social support, PN problems will follow. This demonstrates the importance of devising economic methods to help isolated patients maintain a stable social network.42
One of the findings was that low self-efficacy was a risk factor for PN symptoms in acute stroke. Some studies have emphasized the significance of self-efficacy, such as self-regulatory mechanisms, in dealing with psychological disorders.43 This finding is consistent with earlier reports.44 Other studies focusing on specific self-efficacy (eg, balance and fall self-efficacy),45 have found a positive influence of these dimensions on QOL.46 Self-efficacy refers to the self-confidence of an individual to complete a specific behaviour, which can improve the patient’s disease outcome by regulating one’s behaviour, such as coping with bad emotions, reducing disease symptoms, and improving QOL.47 We found that higher self-efficacy was more beneficial in alleviating PN symptoms. A higher level of self-efficacy can effectively change some’s perception of the disease and improve psychological adaptation and the enthusiasm to participate in rehabilitation, thereby alleviating symptoms. For this reason, intervention programs can be formulated based on self-efficacy theory to increase patients’ confidence in coping with adverse health outcomes and negative emotions in clinical nursing work.43
Symptom Clusters and QOL
It has been proven that patients with symptom clusters have more functional limitations and poorer QOL than those with few or no symptoms. The results show that interventions to assuage elements of the symptom cluster may enhance stroke patients’ QOL. Both pharmacological and non-pharmacological treatments have proved effective for pain, depression, anxiety, post-stroke fatigue, and sleep disturbance. Pain after stroke can be treated using occupational and physical therapies and medications.48 Post-stroke depression and anxiety, to a certain extent, can be relieved by medication and various other methods, such as cognitive-behavioural therapy, physical activity, interpersonal therapy, psychotherapy, and deep breathing.49 Psychotherapy, mindfulness-based stress reduction, antidepressant treatment, and exercises may relieve post-stroke fatigue.49 Treatments for sleep disturbance after stroke include insomnia medicine, exercise, and acupuncture.50 An intervention, such as physical activity, that can alleviate one symptom within the cluster may reduce other problems and enhance functions and QOL of acute stroke patients. Focusing on symptom clusters in clinical practice can inspire us to create effective targeted interventions for subgroups of stroke patients suffering from the same symptom cluster.
Implications for Nursing
This study is the first to use LCA to evaluate PN symptom clusters reported by acute stroke patients and explore whether their self-efficacy, perceived social support, clinical characteristics, and socio-demographic variables were associated with different groups. This study demonstrates great potential for nursing clinical practice and research. LCA is an experimental analysis method that promotes the emergence of distinct data clusters due to similar dependent variables. Our outcomes are beneficial evidence for medical workers to manage multiple symptoms to reduce the negative impact on patient outcomes. Tranching stroke patients by symptom cluster will likely help stratify those considered a high-risk group facing worse outcomes. To promote symptom management, it is essential to educate patients and their caregivers to identify symptom clusters instead of one symptom. In the long run, self-management will be improved if patients and their caregivers recognize that multiple symptoms can occur simultaneously and lead to worse outcomes compared with single symptoms.
Limitations
There are some limitations to this study. First, this was a single-institution study. Most patients were middle-aged, male, less educated, living in rural areas, and married, limiting the generalizability of these findings to individuals with similar demographic characteristics. Also, due to financial and human resource constraints, we did not include all the PN symptoms, such as cognitive impairment after stroke. Therefore, longitudinal studies should be designed to investigate changes in PN symptom clusters at different treatment stages in the near future.
Conclusion
Three latent classes of PN symptoms reported by acute stroke patients were identified. Approximately 10% of the participants experienced high levels of the five symptoms. Also, participants in the “all high symptom” class and “high psychological disorder” class showed significantly lower QOL. These conclusions can give rise to the research and implementation of targeted interventions for multiple symptoms simultaneously, which may facilitate patient outcomes, such as QOL. Additionally, findings related to socio-demographic variables, clinical factors, self-efficacy, and perceived social support may be utilized to distinguish high-risk patients suffering from high levels of the five symptoms and promote tailored interventions.
Acknowledgments
We acknowledge postgraduate nursing students (Gege Zhang, Xiaoyu Lei, Rui Liang, Lin Zhang, and Caixia Yang) for their selfless help when collecting data. We also express our gratitude to all the participants. The present study was supported by the Key Scientific Research Project Plan of Colleges and Universities in Henan Province(No. 22A320023), China.
Disclosure
All authors confirm they have no conflicts of interest for this work.
References
1. Benjamin EJ, Blaha MJ, Chiuve SE, et al. Heart disease and stroke statistics-2017 update: a report from the American Heart Association. Circulation. 2017;135(10):e146–e603. doi:10.1161/CIR.0000000000000485
2. Krueger H, Koot J, Hall RE, et al. Prevalence of individuals experiencing the effects of stroke in Canada: trends and projections. Stroke. 2015;46(8):2226–2231. doi:10.1161/STROKEAHA.115.009616
3. Liu L, Wang D, Wong KS, et al. Stroke and stroke care in China: huge burden, significant workload, and a national priority. Stroke. 2011;42(12):3651–3654. doi:10.1161/STROKEAHA.111.635755
4. Wu X, Zhu B, Fu L, et al. Prevalence, incidence, and mortality of stroke in the Chinese island populations: a systematic review. PLoS One. 2013;8(11):e78629. doi:10.1371/journal.pone.0078629
5. Katan M, Luft A. Global Burden of Stroke. Semin Neurol. 2018;38(2):208–211. doi:10.1055/s-0038-1649503
6. Smith EE, Sahlas DJ, Foley N, et al. Non-pharmacological interventions for post-stroke fatigue: systematic review and network meta-analysis. Int J Stroke. 2020;9(3):621.
7. Dharmakulaseelan L, Chan-Smyth N, Black SE, et al. Embolic stroke of undetermined source and sleep disorders. Stroke. 2020;51(4):1294–1296. doi:10.1161/STROKEAHA.119.028796
8. Scuteri D, Mantovani E, Tamburin S, et al. Opioids in post-stroke pain: a systematic review and meta-analysis. Front Pharmacol. 2020;11:587050. doi:10.3389/fphar.2020.587050
9. Cai W, Stewart R, Mueller C, et al. Poststroke depression and risk of stroke recurrence and mortality: protocol of a meta-analysis and systematic review. BMJ Open. 2018;8(12):e026316. doi:10.1136/bmjopen-2018-026316
10. Rafsten L, Danielsson A, Sunnerhagen KS. Anxiety after stroke: a systematic review and meta-analysis. J Rehabil Med. 2018;50(9):769–778. doi:10.2340/16501977-2384
11. Cumming TB, Packer M, Kramer SF, et al. The prevalence of fatigue after stroke: a systematic review and meta-analysis. Int J Stroke. 2016;11(9):968–977. doi:10.1177/1747493016669861
12. Baylan S, Griffiths S, Grant N, et al. Incidence and prevalence of post-stroke insomnia: a systematic review and meta-analysis. Sleep Med Rev. 2020;49:101222. doi:10.1016/j.smrv.2019.101222
13. Liampas A, Velidakis N, Georgiou T, et al. Prevalence and management challenges in central post-stroke neuropathic pain: a systematic review and meta-analysis. Adv Ther. 2020;37(7):3278–3291. doi:10.1007/s12325-020-01388-w
14. Daraï C, Bendifallah S, Foulot H, et al. [Impact of osteopathic manipulative therapy in patient with deep with colorectal endometriosis: a classification based on symptoms and quality of life]. Gynecol Obstet Fertil Senol. 2017;45(9):472–477. French. doi:10.1016/j.gofs.2017.07.006
15. Williams LA. Clinical management of symptom clusters. Semin Oncol Nurs. 2007;23(2):113–120. doi:10.1016/j.soncn.2007.01.006
16. Kwekkeboom KL. Cancer symptom cluster management. Semin Oncol Nurs. 2016;32(4):373–382. doi:10.1016/j.soncn.2016.08.004
17. Baden M, Lu L, Drummond FJ, et al. Pain, fatigue and depression symptom cluster in survivors of prostate cancer. Support Care Cancer. 2020;28(10):4813–4824. doi:10.1007/s00520-019-05268-0
18. Lim KE, Kim SR, Kim HK, et al. Symptom clusters and quality of life in subjects with COPD. Respir Care. 2017;62(9):1203–1211. doi:10.4187/respcare.05374
19. Stockdill ML, Patrician PA, Bakitas M. Understanding and measuring symptom burden in heart failure: a concept analysis. West J Nurs Res. 2019;41(10):1423–1447. doi:10.1177/0193945919833710
20. Wong A, Lau AY, Yang J, et al. Neuropsychiatric symptom clusters in stroke and transient ischemic attack by cognitive status and stroke subtype: frequency and relationships with vascular lesions, brain atrophy and amyloid. PLoS One. 2016;11(9):e0162846. doi:10.1371/journal.pone.0162846
21. Naess H, Lunde L, Brogger J. The triad of pain, fatigue and depression in ischemic stroke patients: the Bergen Stroke Study. Cerebrovasc Dis. 2012;33(5):461–465. doi:10.1159/000336760
22. Lenz ER, Pugh LC, Milligan RA, et al. The middle-range theory of unpleasant symptoms: an update. ANS Adv Nurs Sci. 1997;19(3):14–27. doi:10.1097/00012272-199703000-00003
23. Omran S, Khader Y, McMillan S. Symptom clusters and quality of life in hospice patients with cancer. Asian Pac J Cancer Prev. 2017;18(9):2387–2393. doi:10.22034/APJCP.2017.18.9.2387
24. Law KS, Wong CS, Song LJ. The construct and criterion validity of emotional intelligence and its potential utility for management studies. J Appl Psychol. 2004;89(3):483–496. doi:10.1037/0021-9010.89.3.483
25. Krupp LB, LaRocca NG, Muir-Nash J, et al. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch Neurol. 1989;46(10):1121–1123. doi:10.1001/archneur.1989.00520460115022
26. Feng C, He Q, Wu Y, et al. Psychometric properties of fatigue severity scale in Chinese systemic lupus erythematosus patients. Health Qual Life Outcomes. 2019;17(1):71. doi:10.1186/s12955-019-1141-x
27. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
28. Yue T, Li Q, Wang R, et al. Comparison of Hospital Anxiety and Depression Scale (HADS) and Zung Self-Rating Anxiety/Depression Scale (SAS/SDS) in evaluating anxiety and depression in patients with psoriatic arthritis. Dermatology. 2020;236(2):170–178. doi:10.1159/000498848
29. Buysse DJ, Reynolds CF
30. Yan DQ, Huang YX, Chen X, et al. Application of the Chinese version of the Pittsburgh Sleep Quality Index in people living with HIV: preliminary reliability and validity. Front Psychiatry. 2021;12:676022. doi:10.3389/fpsyt.2021.676022
31. Lorig KR, Sobel DS, Ritter PL, et al. Effect of a self-management program on patients with chronic disease. Eff Clin Pract. 2001;4(6):256–262.
32. Wang Y, Li K, Li H, et al. Development, reliability, and validity of the home blood pressure monitoring adherence scale for patients with chronic kidney disease. Patient Prefer Adherence. 2020;14:1863–1872. doi:10.2147/PPA.S264287
33. Zimet GD, Powell SS, Farley GK, et al. Psychometric characteristics of the multidimensional scale of perceived social support. J Pers Assess. 1990;55(3–4):610–617.
34. Huang Y, Wu R, Wu J, et al. Psychological resilience, self-acceptance, perceived social support and their associations with mental health of incarcerated offenders in China. Asian J Psychiatr. 2020;52:102166. doi:10.1016/j.ajp.2020.102166
35. Duncan PW, Wallace D, Lai SM, et al. The stroke impact scale version 2.0. Evaluation of reliability, validity, and sensitivity to change. Stroke. 1999;30(10):2131–2140. doi:10.1161/01.STR.30.10.2131
36. Kim SY. Determining the number of latent classes in single- and multi-phase growth mixture models. Struct Equ Modeling. 2014;21(2):263–279. doi:10.1080/10705511.2014.882690
37. Kim HJ, Malone PS. Roles of biological and psychosocial factors in experiencing a psychoneurological symptom cluster in cancer patients. Eur J Oncol Nurs. 2019;42:97–102. doi:10.1016/j.ejon.2019.08.005
38. Olibamoyo O, Adewuya A, Ola B, et al. Prevalence and correlates of depression among Nigerian stroke survivors. S Afr J Psychiatr. 2019;25:1252. doi:10.4102/sajpsychiatry.v25i0.1252
39. Kapoor A, Scott C, Lanctot KL, et al. Symptoms of depression and cognitive impairment in young adults after stroke/transient ischemic attack. Psychiatry Res. 2019;279:361–363. doi:10.1016/j.psychres.2019.06.022
40. Verdelho A, Hénon H, Lebert F, et al. Depressive symptoms after stroke and relationship with dementia: a three-year follow-up study. Neurology. 2004;62(6):905–911. doi:10.1212/01.WNL.0000115107.66957.8C
41. Medeiros GC, Roy D, Kontos N, et al. Post-stroke depression: a 2020 updated review. Gen Hosp Psychiatry. 2020;66:70–80. doi:10.1016/j.genhosppsych.2020.06.011
42. Northcott S, Moss B, Harrison K, et al. A systematic review of the impact of stroke on social support and social networks: associated factors and patterns of change. Clin Rehabil. 2016;30(8):811–831. doi:10.1177/0269215515602136
43. Torrisi M, De cola MC, Buda A, et al. Self-efficacy, poststroke depression, and rehabilitation outcomes: is there a correlation? J Stroke Cerebrovasc Dis. 2018;27(11):3208–3211. doi:10.1016/j.jstrokecerebrovasdis.2018.07.021
44. Robinson-Smith G, Johnston MV, Allen J. Self-care self-efficacy, quality of life, and depression after stroke. Arch Phys Med Rehabil. 2000;81(4):460–464. doi:10.1053/mr.2000.3863
45. Tsai SF, Yin JH, Tung TH, et al. Falls efficacy among stroke survivors living in the community. Disabil Rehabil. 2011;33(19–20):1785–1790. doi:10.3109/09638288.2010.546938
46. Tang A, Tao A, Soh M, et al. The effect of interventions on balance self-efficacy in the stroke population: a systematic review and meta-analysis. Clin Rehabil. 2015;29(12):1168–1177. doi:10.1177/0269215515570380
47. Pearce G, Pinnock H, Epiphaniou E, et al. Experiences of self-management support following a stroke: a meta-review of qualitative systematic reviews. PLoS One. 2015;10(12):e0141803. doi:10.1371/journal.pone.0141803
48. Harrison RA, Field TS. Post stroke pain: identification, assessment, and therapy. Cerebrovasc Dis. 2015;39(3–4):190–201. doi:10.1159/000375397
49. Lanctôt KL, Lindsay MP, Smith EE. Canadian stroke best practice recommendations: mood, cognition and fatigue following stroke, 6th edition update 2019. Int J Stroke. 2020;15(6):668–688. doi:10.1177/1747493019847334
50. Lowe A, Bailey M, O’Shaughnessy T, et al. Treatment of sleep disturbance following stroke and traumatic brain injury: a systematic review of conservative interventions. Disabil Rehabil. 2020:1–13. DOI:10.1080/09638288.2020.1856948
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.