Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Exploring Primary Care Physicians’ Current Referral Practices to Physiotherapy and Specialized Care for Musculoskeletal Conditions: A Cross-Sectional Study
Authors AlMuhana NA ![]() , Alimam D
, Alimam D ![]() , Kofi M
, Kofi M ![]() , Albaqih SM, Alsobayel H
, Albaqih SM, Alsobayel H
Received 23 November 2025
Accepted for publication 1 April 2026
Published 23 April 2026 Volume 2026:19 583766
DOI https://doi.org/10.2147/JMDH.S583766
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Norah Ali AlMuhana,1,2 Dalia Alimam,1 Mostafa Kofi,3 Saeed Mohammed Albaqih,3 Hana Alsobayel1,4
1Department of Rehabilitation Sciences, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia; 2Physiotherapy Department, Prince Sultan Military Medical City (PSMMC), Ministry of Defense Health Services, Riyadh, Saudi Arabia; 3Department of Family and Community Medicine, Prince Sultan Military Medical City (PSMMC), Ministry of Defense Health Services, Riyadh, Saudi Arabia; 4Research Chair in Healthcare Innovation, Department of Rehabilitation Sciences, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia
Correspondence: Norah Ali AlMuhana, Physiotherapy Department, Prince Sultan Military Medical City (PSMMC), Ministry of Defense Health Services, Riyadh, Saudi Arabia, Email [email protected]
Purpose: Musculoskeletal (MSK) disorders are a leading global cause of disability and healthcare utilization. In Saudi Arabia, the referral behaviors of primary care physicians (PCPs) for MSK management remain underexplored. This study aims to investigate referral patterns and awareness of prognostic stratification tools among primary-care physicians managing musculoskeletal conditions in Riyadh, Saudi Arabia.
Methods: A web-based cross-sectional survey of 283 PCPs in Riyadh, Saudi Arabia, assessed demographic variables, MSK caseloads, referral frequencies to physiotherapy, specialist, and radiology services, satisfaction with existing pathways, and familiarity with stratified-care tools (eg, Keele STarT MSK). Associations between the healthcare sector and referral behaviors were examined using chi-square (χ2) tests with Cramér’s V, and binary logistic regression was conducted to identify independent predictors of physiotherapy referral frequency. Open-ended responses were analyzed thematically.
Results: Most respondents (61.8%) were male and worked in government sectors. Physiotherapy referrals were infrequent (37.8% rarely referred), with significant sectoral differences (p < 0.001). Over half (53.4%) were unfamiliar with prognostic tools, while 18.4% reported occasional use. Barriers included lack of electronic integration (28%), unclear guidelines (27%), and time constraints (24%). Physicians recommended clearer referral criteria, electronic medical record (EMR) linked digital pathways, and interprofessional education. Multivariable binary logistic regression identified MSK caseload and senior registrar rank as significant independent predictors of more frequent physiotherapy referral. Physicians seeing 3– 5 patients daily (OR = 11.597, 95% CI: 2.202– 61.085, p =0.004) and senior registrars compared with consultants (OR = 2.857, 95% CI: 1.420– 5.746, p =0.003) showed the highest odds of more frequent referral.
Conclusion: Referral practices for MSK conditions among Saudi PCPs remain inconsistent and largely uninformed by evidence-based stratification tools. These findings suggest that enhancing multidisciplinary collaboration, training, and digital integration within EMRs may help align referral behavior with best practices and support Saudi Vision 2030 health system reforms. Future research should evaluate implementation strategies for these improvements within the Saudi primary care context.
Keywords: primary care physicians, physiotherapy referral, musculoskeletal disorders, stratified care, multidisciplinary healthcare, Saudi Arabia
Introduction
Musculoskeletal (MSK) disorders are among the leading global contributors to disability, pain, and healthcare utilization, accounting for nearly one-fifth of all years lived with disability (YLDs) worldwide.1–3 If not identified and managed early, MSK conditions often progress into chronic pain syndromes characterized by persistent pain, physical dysfunction, and psychological distress,4 which significantly degrade quality of life.5,6 While also increasing the economic burden on health systems.7
Primary care physicians (PCPs) play a central role in the initial management of MSK complaints, often serving as the first point of contact for affected individuals.8–11 Physiotherapy is widely recognized as a core component of MSK care due to its emphasis on functional restoration, patient self-management, and non-pharmacological interventions.12,13 However, referral patterns from PCPs to physiotherapy services remain inconsistent across and within countries, often shaped by clinical familiarity, institutional policies, and service accessibility.14,15
In Saudi Arabia, the burden of MSK conditions has risen sharply in recent decades, reflecting regional demographic transitions, sedentary lifestyles, and higher occupational and postural demands.16,17 High prevalence rates have been reported among healthcare workers, schoolteachers, and postpartum women.18–22 Nevertheless, limited data are available on how MSK patients are triaged within Saudi primary care settings, particularly regarding referral decisions between physiotherapy, specialist consultation, and diagnostic imaging.
Globally, clinical tools, such as prognostic risk stratification instruments, have been integrated into MSK care to guide early management, reduce chronicity, and improve patient outcomes.23–25 These tools help clinicians identify patients at high risk of poor outcomes and support targeted interventions tailored to risk severity and psychosocial factors.26–28 Their integration into referral pathways has improved patient outcomes, such as pain and disability.28,29 Moreover, prognostic stratification tools provide clinicians with a structured framework for tailoring treatment intensity to individual patient risk profiles, thereby improving clinical decision-making and rehabilitation outcomes.14,30 Stratification tools have low adoption despite their proven benefits, a challenge that is being explored internationally.30 Yet uptake in Saudi primary care remains largely unexplored. Furthermore, referral behavior is not only a clinical decision; it is often influenced by systemic factors such as service availability, waiting times, digital infrastructure, communication between providers, and the clarity of referral guidelines.29 In fragmented health systems like Saudi Arabia’s, where public, semi-governmental, and private sectors operate concurrently, institutional disparities can lead to widely variable referral practices.31,32 Although initiatives are underway to improve digital integration and care coordination under the national “Vision 2030” reform agenda, data on how these systemic shifts impact MSK referral behaviors in primary care remain limited.
To date, evidence on physiotherapy referral behaviors among primary care physicians in Saudi Arabia remains limited. Referral patterns have been documented in high-income Western settings.11,14 The Saudi context — characterized by a fragmented three-sector health system, variable availability of physiotherapy, and limited integration of electronic referral pathways — has received little systematic attention. In particular, no study has examined whether familiarity with validated MSK prognostic stratification tools influences referral decisions among Saudi PCPs, nor whether the healthcare sector, independent of physician-level characteristics, predicts referral frequency. This knowledge gap is especially relevant given Saudi Arabia’s ongoing Vision 2030 health reforms, which aim to strengthen primary care capacity and promote evidence-based MSK management. Addressing this gap may inform targeted training initiatives, support the development of national referral guidelines, and provide an evidence base for digitally integrated referral pathways within the Saudi primary care system.
Therefore, this study aims to assess physiotherapy referral patterns among primary care physicians in Saudi Arabia, focusing on sectoral differences, perceived barriers, and familiarity with prognostic tools.
Study Objective
To assess the current referral practices of primary care physicians for musculoskeletal conditions in Riyadh, Saudi Arabia, this study investigates the frequency of physiotherapy referrals, the extent of awareness and use of stratification tools (such as Keele STarT MSK), and the system-level barriers influencing these decisions.
Research Questions
Question 1: What are the current referral practices of primary care physicians for MSK conditions in Riyadh?
Question 2: What was the level of awareness and utilization of MSK risk stratification tools, particularly the Keele STarT MSK tool, among PCPs?
Material and Methods
Study Design
A cross-sectional web-based survey design guided by STROBE (Strengthening the Reporting of Observational Studies in Epidemiology)33 (Supplementary Table 1, and CHERRIES (Checklist for Reporting Results of Internet E-Surveys)34 (Supplementary Table 2) reporting frameworks. The survey aimed to collect both quantitative and qualitative data on referral practices for patients with MSK conditions among PCPs in Riyadh, Saudi Arabia.
Participants
Eligible participants included licensed family physicians, general practitioners, or resident medical officers currently providing adult MSK primary care in Riyadh. Physicians not involved in direct MSK care or those in training without independent caseloads were excluded.
Study Setting
Eligible physicians worked in one of the three major healthcare sectors: Ministry of Health (MOH) primary health-care centers, other government sectors (eg., military, university, and semi-government hospitals), and private clinics were recruited.
Sampling Strategy and Sample Size
A convenience sampling approach with purposive elements was used, aiming to recruit participants across all three healthcare sectors. The survey was distributed through open professional networks, including institutional Email lists, professional WhatsApp groups, and social media platforms. Based on official data indicating 1,583 licensed family medicine physicians in Riyadh,35 a minimum sample size of 309 was calculated using Cochran’s formula with the finite population correction.36 Although the achieved sample of 283 fell marginally below the calculated minimum of 309, post hoc power estimation indicated adequate power (>0.80) for the primary chi-square comparisons, given the observed effect sizes (Cramér’s V range: 0.18–0.38). This shortfall represents a minor constraint on generalizability rather than a critical limitation of internal validity. Ultimately, 283 valid responses were received. As the precise number of physicians who received the invitation could not be determined, an exact response rate could not be calculated. This open dissemination approach carries a potential risk of selection bias, as physicians more engaged with professional networks may have been overrepresented, and this is acknowledged as a study limitation.
Survey Instrument Development
A structured, self-administered online survey was developed to investigate primary care physicians’ referral behaviors for MSK conditions. The questionnaire comprised 25 items grouped into six thematic sections: (1) consent and eligibility screening, (2) demographic information, (3) knowledge and familiarity with MSK clinical decision-making tools, (4) attitudes and satisfaction with current referral systems, (5) clinical practice, referral behaviors, and system-level barriers, and (6) optional contact information. Referral frequency categories (<10%, 10–30%, 31–60%, >60%) were selected to capture clinically meaningful thresholds that distinguish rare, occasional, moderate, and frequent referral practices, enabling descriptive comparisons across physician groups. The survey was pilot-tested and refined based on participant feedback to ensure clarity and content validity. It was disseminated electronically via Google Forms, and all responses were collected anonymously. The full survey instrument is provided as Supplementary Figure 1.
Pilot Study Results
A pilot test was conducted with 16 PCPs purposively selected to represent all three healthcare sectors (MOH n=7, other government n=5, private n=4), including a mix of professional ranks, consultants, senior registrars, and registrars. No residents participated in the pilot to ensure responses reflected independent clinical experience. The pilot evaluated clarity, usability, and content validity. Participants reported an average survey completion time of seven minutes, with most rating it as “clear” or “very clear.” Revisions were made to improve item clarity and relevance, including merging overlapping items and adding “chronic pain” as a referral reason. The survey was then finalized for full deployment. Although Cronbach’s alpha was not calculated due to the exploratory nature of the survey, face validity was confirmed through expert review.
Survey Reporting
The web-based survey is reported in accordance with CHERRIES. We report participation and completion rates and describe measures taken to ensure data integrity (time-to-complete threshold, timestamp, and demographic pattern checks). Technical measures to prevent duplicate entries (cookies/login/IP) were not implemented at collection and are acknowledged as a limitation.
Data Quality and Bias Control
The questionnaire included adaptive logic to reduce random responses to minimize potential bias. Because the survey was distributed through open professional channels (e-mail, QR codes, and social media groups), technical restrictions such as IP filtering or limiting one response per ID were not applied. However, post-hoc validation procedures were implemented to ensure data integrity. These included: (1) cross-checking for duplicate timestamps and identical demographic profiles (eg., gender, professional rank, and years of experience); (2) Responses completed in less than three minutes were excluded, as this threshold represented less than half the mean completion time observed during the pilot study (mean = 7 minutes), and was considered insufficient to allow accurate and thoughtful completion of all 25 items; and (3) examining internal consistency between related items (eg., years in practice aligned with current clinical rank). No duplicate or invalid entries were identified, and all 283 submitted responses met the inclusion criteria and were retained for analysis.
Outcomes & Denominators
Items regarding tool familiarity and use were answered by a subset of respondents who indicated awareness of any decision tool; therefore, denominators for those tables reflect the number of respondents to those specific items. Primary analyses use item-specific denominators; we avoid extrapolating subset percentages to the full sample.
Data Collection Procedure
Data were collected from May to September 2025 using Google Forms. All responses were collected anonymously.
Ethical Considerations
This research was approved by the Institutional Review Board (IRB) of King Saud University (Approval Number: E-25-9743). Informed consent was obtained electronically before participation. All responses were anonymized, and data were securely stored in password-protected files.
Data Analysis
Quantitative data were analyzed using IBM SPSS Statistics version 31 (IBM Corp., Armonk, NY, USA). Descriptive statistics (frequencies, percentages, means) were calculated for participant characteristics and referral behaviors. Bivariate associations between referral patterns and independent variables (eg., healthcare sector, professional rank) were assessed using χ2-tests. Effect sizes were calculated with Cramér’s V, where 0.10–0.19 indicates a small effect, 0.20–0.39 a moderate effect, and ≥ 0.40 a large effect.37 Additionally, multivariable binary logistic regression was performed using the Enter method, with all predictor variables entered simultaneously to identify independent predictors of physiotherapy referral frequency. The outcome variable was dichotomized as rare referral (<10% of MSK cases; coded 0) versus more frequent referral (≥10%; coded 1). Independent variables included the healthcare sector, professional rank, years of experience, and MSK case load. Results are reported as odds ratios (ORs) with 95% confidence intervals (CIs) and Wald statistics. Open-ended responses were analyzed thematically through inductive coding to identify main categories related to system-level barriers and physician recommendations.
Results
Demographic Characteristics
A total of 283 physicians participated in the survey. Most respondents were male (61.8%) and Saudi nationals (74.6%). Nearly half were consultants (47.3%), followed by senior registrars (26.9%), registrars (18.4%), and residents (7.4%). In terms of practice experience, the largest groups reported 1–5 years (39.9%) or 6–10 years (34.6%) of clinical practice. Regarding healthcare sectors, 45.9% of the respondents worked in other government institutions (including military, university, specialist hospital, etc)., 33.9% in the Ministry of Health (MOH), and 20.1% in private practice (Table 1).
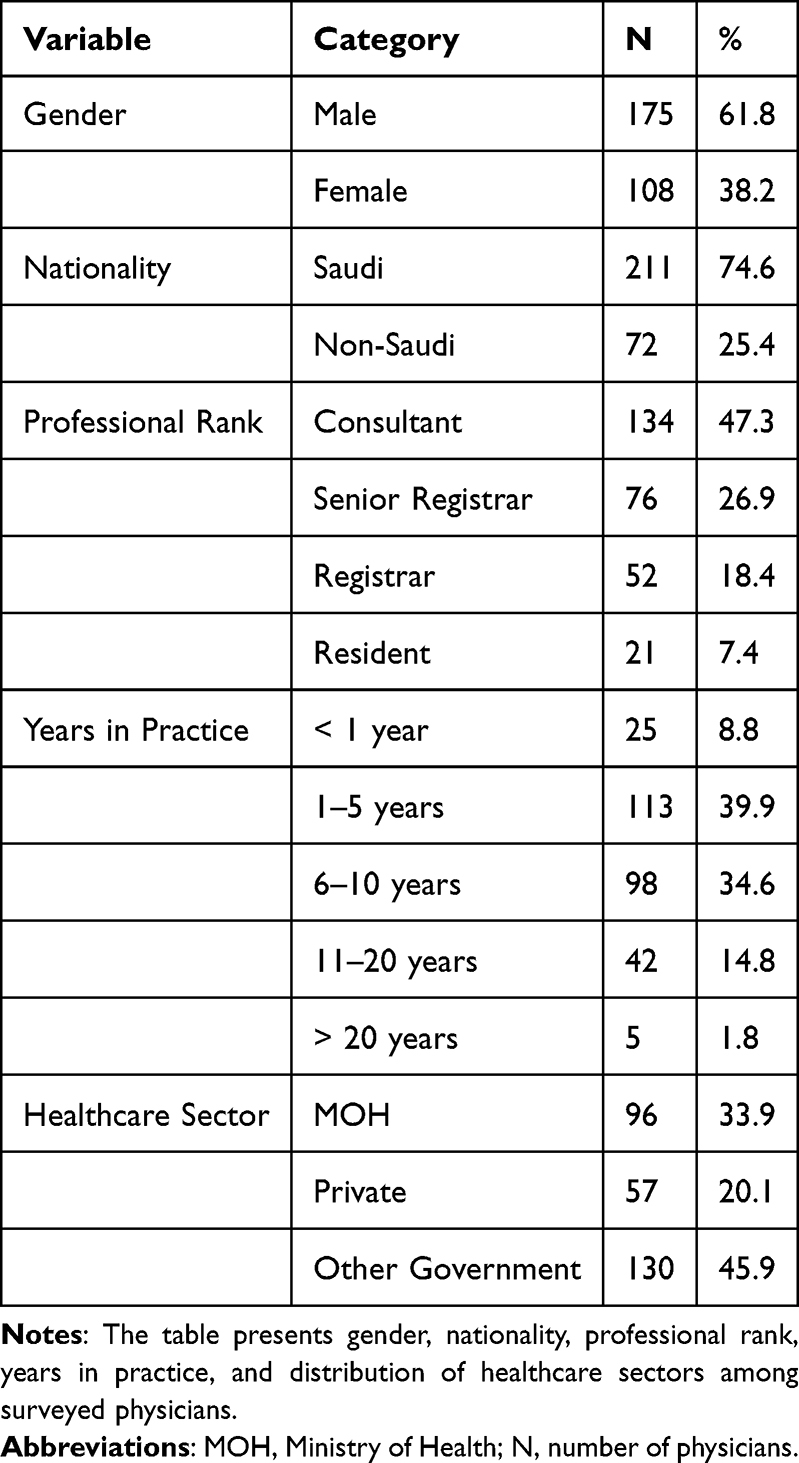 |
Table 1 Demographic Characteristics of Participants (N = 283) |
Clinical and Referral Practices
MSK Caseload and Referral Patterns
Most physicians saw 1–2 MSK patients daily (55.5%), while 35.0% saw 3–5 patients, and only 4.6% more than five. Referrals to physiotherapy were generally infrequent: 37.8% rarely referred (<10% of cases) and 48.8% referred only in 10–30% of cases. (Figure 1) Referrals to specialist clinics followed a similar pattern, with 52.7% referring in 10–30% of cases, while only 2.1% referred “very often”. (Figure 2) On the other hand, referrals to radiology were more common, with nearly half (49.8%) referring in 10–30% of cases and 29.3% in 31–60% (Figure 3).
 |
Figure 1 Bar chart of the percentage of musculoskeletal (MSK) referrals to physiotherapy among primary care physicians. |
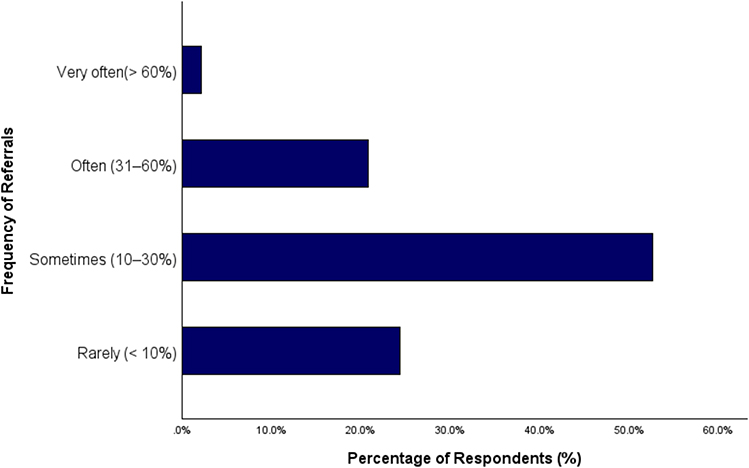 |
Figure 2 Bar chart of the percentage of musculoskeletal (MSK) referrals to specialist clinics among primary care physicians. |
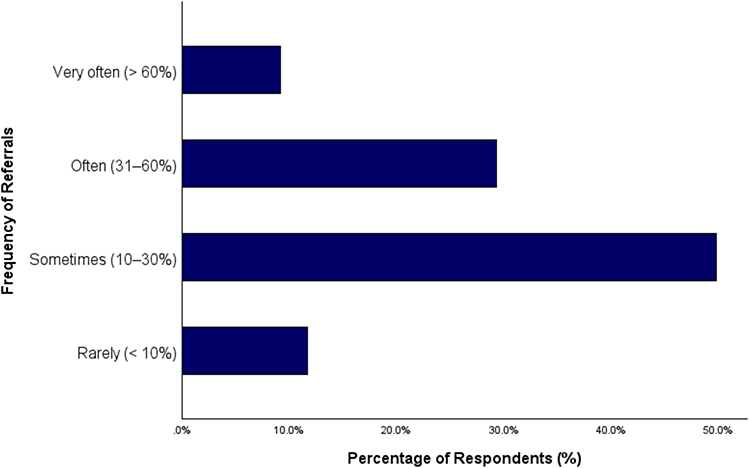 |
Figure 3 Bar chart of the percentage of musculoskeletal (MSK) referrals to radiology among primary care physicians. |
Associations Between the Health Sector and Referral Patterns
Chi-square analyses showed no significant differences in MSK caseloads across healthcare sectors (p = 0.055) (Figure 4). However, referral practices varied notably between healthcare sectors. Physiotherapy referrals were significantly more common in other governmental sectors (χ2(6) = 30.38, p < 0.001), while physicians in the private sector were more likely to refer patients to specialist clinics regularly (χ2(6) = 21.72, p = 0.001). Additionally, referrals to radiology were disproportionately higher in other governmental sectors (χ2(6) = 41.03, p < 0.001), highlighting sector-specific differences in referral decision-making patterns. MSK caseload was also significantly associated with physiotherapy referral frequency (χ2(3) = 19.268, p <0.001, Cramér’s V = 0.261), with physicians reporting higher daily MSK caseloads being more likely to refer patients to physiotherapy (Table 2 and Figure 5).
 |
Table 2 Association Between the Healthcare Sector and Referral Practice |
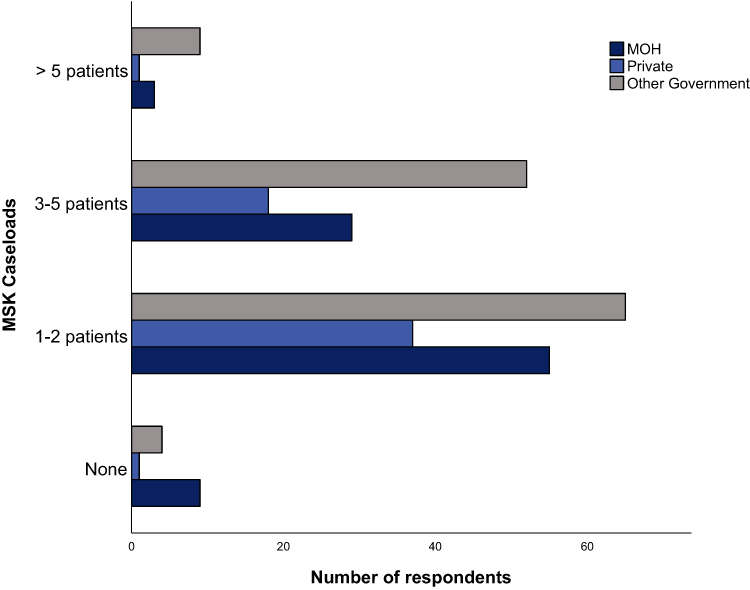 |
Figure 4 Bar chart of the distribution of daily musculoskeletal (MSK) caseloads across different healthcare sectors. Abbreviations: MSK, Musculoskeletal; MOH, Ministry of Health. |
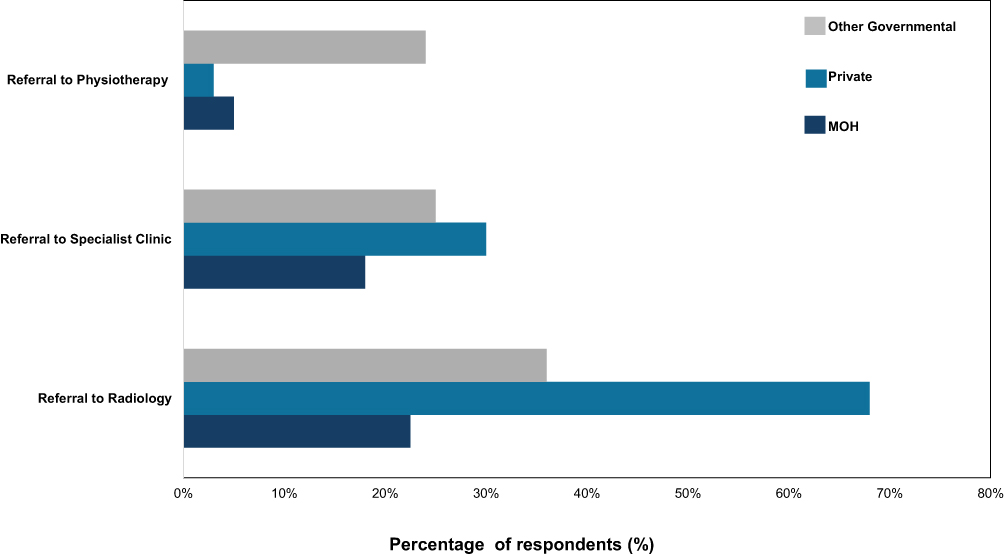 |
Figure 5 Clustered bar chart of the percentage of MSK patients referred to physiotherapy, specialist clinics, and radiology across healthcare sectors. Abbreviations: MSK, Musculoskeletal; MOH, Ministry of Health. |
Familiarity and Use of Prognostic Tools
Over half of respondents (53.4%) were unfamiliar with prognostic or stratification tools in MSK care. Another 28.3% were aware of them but not using them, and only 18.4% reported occasional or regular use.
Among those reporting the use of such tools, the Keele STarT MSK Tool (21.5%) and STarT Back Tool (16.5%) were mentioned, alongside general measures such as the VAS (16.5%). Reported barriers included lack of electronic integration (28.0%), absence of guidelines (27.1%), and time constraints (24.3%). Moreover, a total of 44.5% of physicians reported using guidelines or tools in their clinical practice, whereas 55.5% indicated that they did not (Table 3).
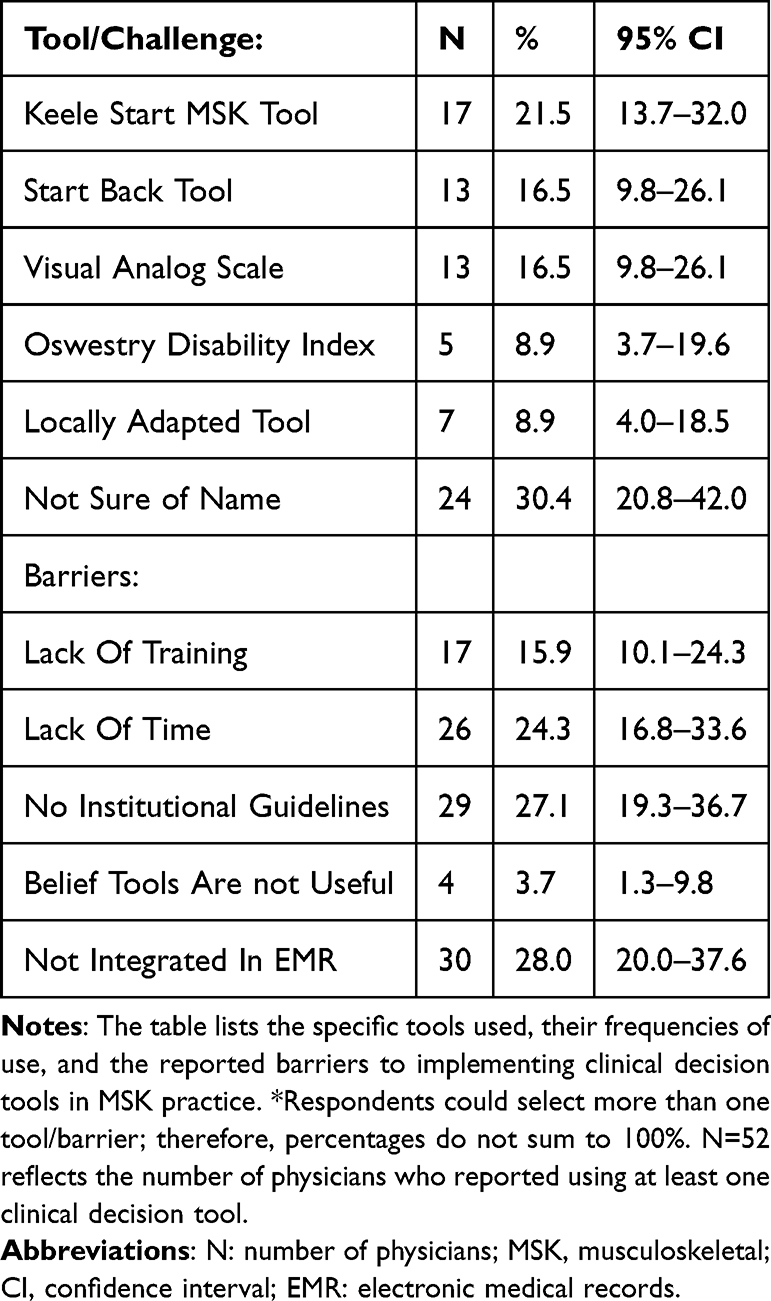 |
Table 3 Clinical Practice and Referral Patterns of Participants (N = 52*) |
Satisfaction with Referral Systems and Communication
Just over half of physicians (51.6%) reported being satisfied with PT referrals, while 39.9% felt neutral, and 8.5% were dissatisfied. For specialist referrals, 52.3% were satisfied, 41.7% felt neutral, and 6.0% were dissatisfied. Importantly, most respondents (67.1%) believed the system only “rarely” or “sometimes” met patient needs, with MOH physicians significantly more likely to report inadequacy compared to private sector physicians (χ2 (6) = 15.25, p =0.018). Communication between primary care physicians and specialists was also an issue: nearly half (49.1%) rated communication as “poor” or “needs improvement,” with significant variation across sectors (χ2 (6) = 16.41, p =0.012) (Table 4).
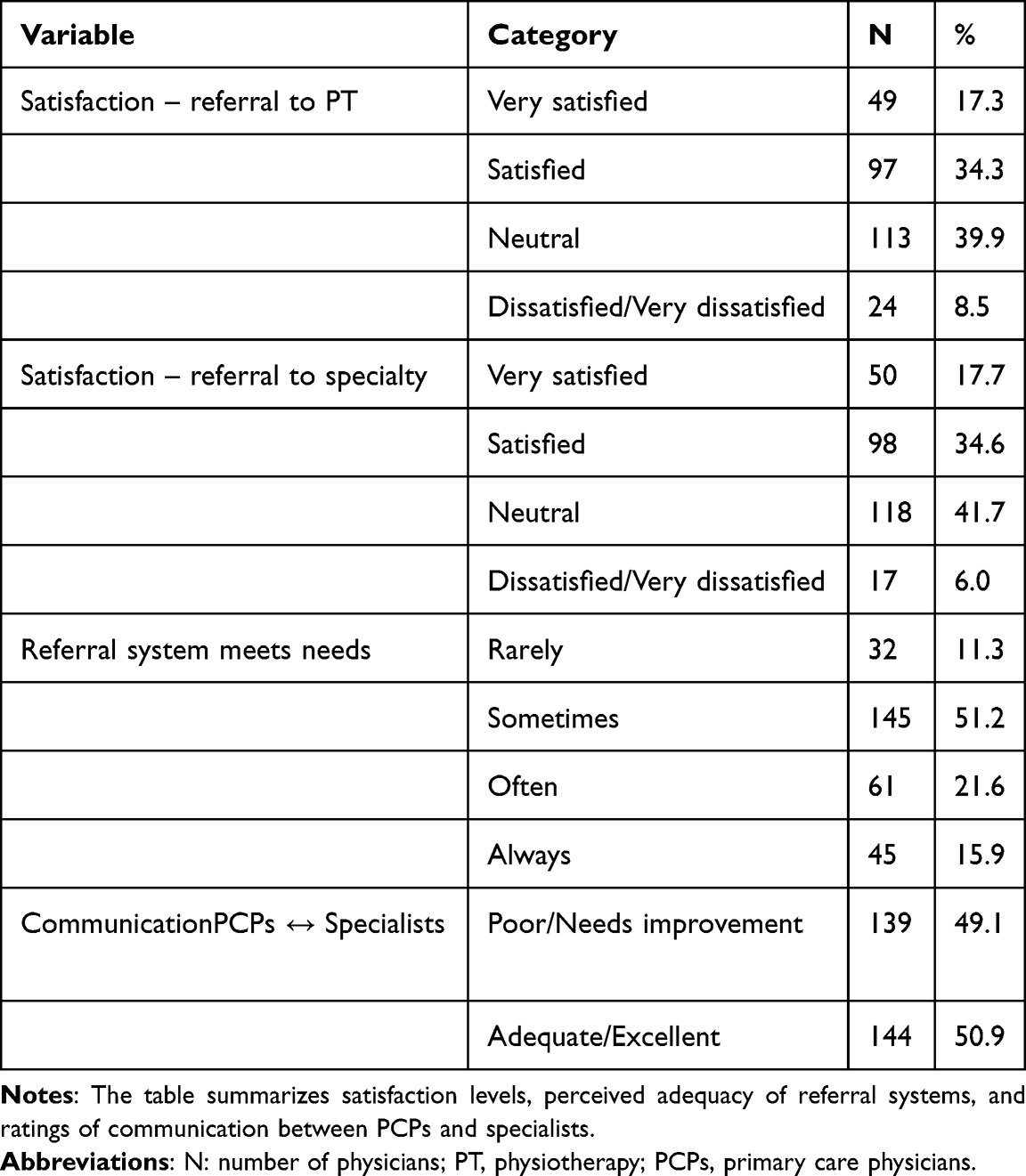 |
Table 4 Clinical Practice and Referral Patterns of Participants (N = 283) |
Factors Influencing Referral Decisions
Physicians most referred patients to PT due to chronic pain (31.9%) or functional limitations (32.0%) (Figure 6). Decision-making was shaped by the availability of PT services (27.1%), condition severity (23.9%), and knowledge of PT benefits (21.8%), with patient preference and insurance considerations being less influential (Table 5).
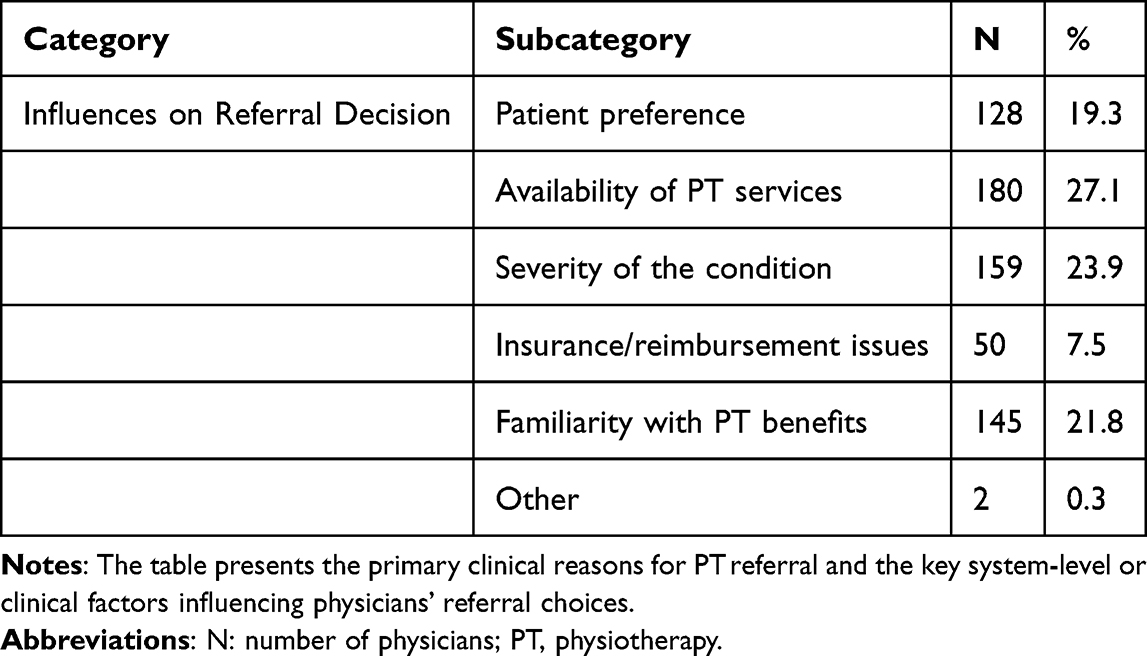 |
Table 5 Reasons and Influences on Referral to Physiotherapy (N = 283) |
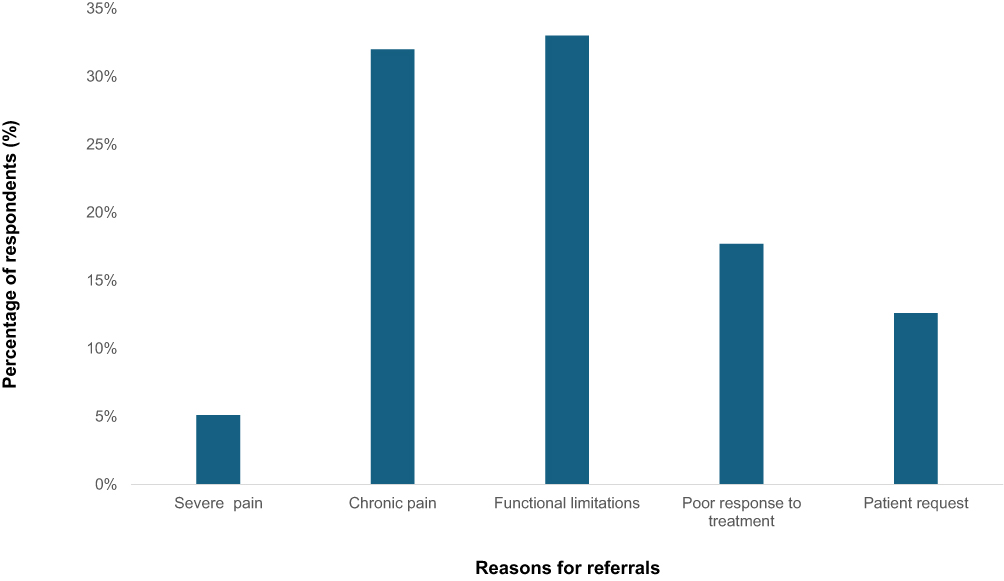 |
Figure 6 Bar chart of the percentage of primary reasons for referral to physiotherapy among primary care physicians. |
Five hundred sixty-four responses identified key barriers in the referral system. The most common challenge was long waiting times for specialist or physiotherapy appointments (38.3%), followed by unclear referral guidelines or digital pathways (25.5%), and patient reluctance or poor compliance with referrals (17.2%). Limited access to MSK services was reported by 10.6%, while insurance or cost-related issues were noted by 8.0%. Only 0.4% mentioned “other” issues (Table 6).
 |
Table 6 System-Level Referral Challenges Reported by Physicians (Q22) |
Physicians’ Suggestions for Enhancing Referral and Decision-Making
Thematic analysis revealed that physicians consistently called for structural improvements in the referral process. The most common recommendation was the establishment of clear clinical referral guidelines (38%), followed by digital solutions integrated with EMRs (26%). Respondents also highlighted the importance of improving service access and appointment systems (24%), education and training for physicians and patients (19%), stronger interprofessional collaboration (14%), and insurance/policy reforms (12%) (Table 7 and Figure 7).
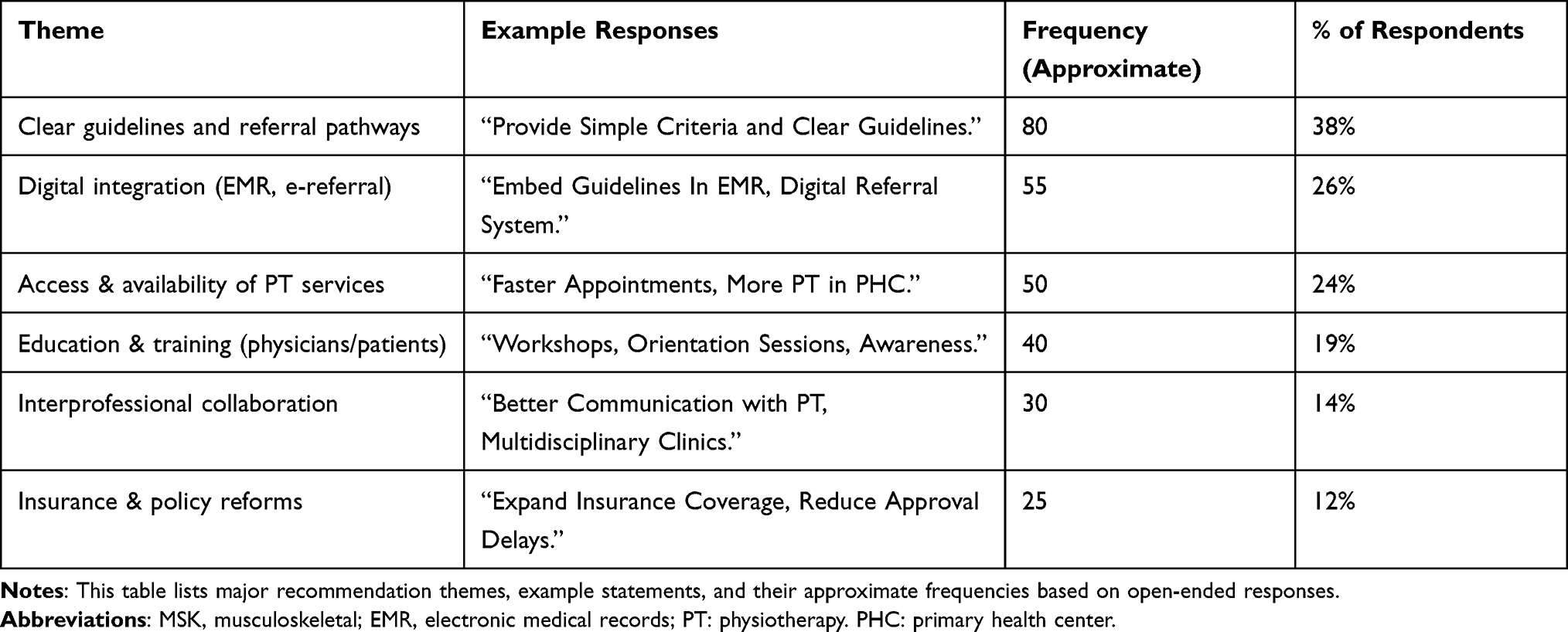 |
Table 7 Thematic Analysis of Physicians’ Suggestions for Enhancing Referral and Decision-Making |
 |
Figure 7 Bar chart showing the percentage of thematic categories in physicians’ recommendations for improving MSK referral pathways and decision-making. Abbreviations: EMR, Electronic Medical Record; e-referral, electronic referral; MSK, Musculoskeletal. Note: Frequencies represent the approximate number of times each theme was mentioned in open-ended survey responses. |
Multivariable Binary Logistic Regression
A multivariable binary logistic regression was conducted to identify independent predictors of physiotherapy referral frequency, with referral dichotomized as rare (<10%; coded 0) versus more frequent (≥10%; coded 1). All 283 participants were included with no missing data. The overall model was statistically significant (χ2(12) = 38.695, p <0.001) and demonstrated acceptable calibration (Hosmer–Lemeshow χ2(8) = 6.634, p =0.577). The model explained 17.4% of variance in referral frequency (Nagelkerke R2 = 0.174) and correctly classified 66.4% of cases (Table 8).
 |
Table 8 Multivariable Binary Logistic Regression—Independent Predictors of Physiotherapy Referral Frequency (N = 283) |
MSK caseload was a significant predictor at the block level (p =0.022). Physicians seeing 3–5 MSK patients daily were approximately 11.6 times more likely to refer to physiotherapy compared with those seeing no MSK patients (OR = 11.597, 95% CI: 2.202–61.085, p =0.004), and those seeing more than five patients daily showed similarly elevated odds (OR = 11.673, 95% CI: 1.475–92.368, p =0.020). Professional rank was also significant at the block level (p =0.023), with senior registrars being significantly more likely to refer than consultants (OR = 2.857, 95% CI: 1.420–5.746, p =0.003). Years of experience (block p =0.372) and healthcare sector (block p =0.154) were not significant independent predictors in the multivariable model.
Discussion
Referral Frequencies and Sectoral Differences
This study assessed referral behaviors of PCPs in Riyadh, Saudi Arabia, focusing on their use of physiotherapy services, awareness of MSK stratification tools, and systemic challenges impacting referral patterns. Physiotherapy referrals were notably less frequent than specialist and radiology referrals, a pattern consistent with international evidence suggesting PCPs in high-income countries similarly prefer imaging and specialist pathways over physiotherapy for MSK conditions.11,14 Physicians in governmental and academic sectors were more likely to refer to physiotherapy, while private-sector PCPs preferred specialist referrals. These findings align with previous research indicating that institutional factors, such as internal referral structures, reimbursement schemes, and resource availability, strongly influence referral behaviors.8 As observed in the United States and Europe, PCPs in Riyadh tend to refer MSK patients to imaging or specialist clinics rather than to physiotherapy services.11,14 However, the distinction in referral preferences between healthcare sectors in Saudi Arabia is particularly noteworthy.
Government-sector physicians were significantly more likely to refer patients to physiotherapy, possibly because of easier access to such services within the system and fewer insurance restrictions.31 In contrast, private-sector physicians may face reimbursement barriers and patient preferences for specialist consultations, which may contribute to lower physiotherapy referral rates.11 These differences underscore how organizational structure, administrative procedures, and healthcare financing models influence clinical decision-making, particularly in mixed public-private health systems such as Saudi Arabia. It should be noted that observed sectoral differences may be partially attributable to unmeasured confounders—including physician workload, patient demographics, and institutional resource availability—that were not captured in the current survey. Residual confounding cannot be excluded.
Limited Familiarity and Utilization of Prognostic Tools
Despite strong evidence supporting tools such as the STarT Back Screening Tool and the Keele STarT MSK Tool,27,28 the low familiarity and limited implementation among Saudi PCPs remain limited — a pattern consistent with broader international implementation challenges. Tousignant-Laflamme et al (2022) emphasized that rehabilitation clinicians must master validated prognostic instruments to achieve personalized, value-based care38 Their work underscored that traditional diagnostic reasoning should evolve toward a prognosis-informed model that integrates biopsychosocial risk factors to guide stratified management. Such an approach enables clinicians to match treatment intensity with patient needs, thereby improving outcomes while optimizing healthcare efficiency.23 Tousignant-Laflamme et al further highlighted that the global uptake of prognostic models such as the STarT Back and STarT MSK tools remains limited due to gaps in clinician training, insufficient methodological rigor, and the lack of structured implementation frameworks.38 These barriers parallel the Saudi primary care context, where the absence of national guidelines,39 limited digital integration,40 and minimal emphasis on musculoskeletal stratification in medical education41 appear to hinder tool adoption. Embedding validated prognostic tools like the Keele STarT MSK within referral pathways could therefore enhance clinical decision-making, support interprofessional collaboration, and align physiotherapy practice in Saudi Arabia with international standards for personalized rehabilitation and value-based care.38
In the Saudi context, without clear pathways and decision aids, referral decisions may continue to be guided by physician intuition or institutional norms rather than evidence-based frameworks. In contrast, similar situations are experienced in other countries. For example, Fanaki et al established that PCPs may not embrace modern diagnostic tools due to workflow burden and low electronic embedding42 Moreover, Shorthouse et al reported that, in the absence of standardized care pathways and despite using a triage tool, clinicians frequently relied on subjective judgment and informal reasoning when managing musculoskeletal referrals43 Within the Saudi context, our results align with Al Asmri et al (2020), who emphasized that fragmented health information systems and the absence of centralized referral protocols limit the uptake of evidence-based practices8 Combined with our results, this underscores the potential benefit of standardized EMR integration and national MSK referral guidelines. Encouragingly, the majority of respondents expressed interest in receiving training and integrating these tools digitally, highlighting a promising opportunity for targeted educational and technological interventions.
Satisfaction with Referral Systems and Communication
Saudi PCPs’ care plan decisions are influenced by their satisfaction with the existing referral system. Despite reported satisfaction with referral processes, the majority of physicians indicated the system does not consistently meet patient needs — a finding that highlights a disconnect between perceived adequacy and actual performance. This finding resonates with existing evaluations of the Saudi health system, which frequently cite fragmented care coordination, limited digitization, and inadequate provider communication.8 Specifically, interprofessional communication between PCPs and physiotherapists or specialists was rated as poor by nearly half the respondents. These gaps may result in delayed referrals, inconsistent follow-up, and reduced continuity of care. In contrast, health systems in countries such as the United Kingdom have demonstrated improved outcomes with centralized digital referral systems and stronger communication protocols.14
Saudi Arabia’s national Vision 2030 healthcare reform aims to digitize health services and promote integrated care. Our findings suggest that such reforms may benefit from including interoperable referral systems and structured communication platforms, particularly for MSK care.
Barriers to Physiotherapy Referral
Referral decisions were shaped by both clinical factors — principally chronic pain and functional limitation — and system-level influences, including service availability and familiarity with physiotherapy benefits.
The most frequently reported barrier was long waiting times for physiotherapy or specialist appointments. Similarly, Al-Abbad and Madi affirm that long wait times hinder the effectiveness of referral systems in the Middle East.9 Other barriers included the lack of referral guidelines, limited access to physiotherapists in certain facilities, and fragmented digital systems. These findings reflect international concerns about delayed MSK referrals, particularly in resource-constrained settings. This aligns with international evidence indicating that organizational and system-level barriers, including inconsistent referral guidelines, limited streamlined access routes, and limited professional autonomy for physiotherapists, often impede MSK care pathways. For example, Babatunde et al (2020) found that triage/self-referral models are frequently hampered by “procedural and administrative issues” across diverse health systems44 These findings suggest that Saudi PCPs do not oppose physiotherapy referrals but rather practice in environments that may limit or disincentivize them. Addressing these structural barriers may help enable timely, evidence-based MSK care.
Physician Decision-Making and Referral Influences
Saudi PCPs are motivated by varying factors to make physiotherapy referrals. Our results showed that PCPs are more likely to make physiotherapy referrals based on service availability, condition severity, familiarity with physiotherapy benefits, and patient preference. In particular, PCPs have more incentives to make physiotherapy referrals if they are convinced that those services are available and that patients’ conditions warrant a referral. These findings suggest that administrative, operational, and finance-related factors may play an important role in PCPs’ referral decisions.18 Furthermore, we showed that Saudi PCPs consider chronic pain and functional limitation as the core elements when making referral decisions. This finding clarifies the above observation that PCPs consider the severity of the condition when referring patients for physiotherapy. While these observations show that the Saudi referral system is largely reactive, they also affirm that PCPs consider patients’ needs. Comparatively, the situation in other international countries is based on early referrals to prevent chronicity and unnecessary healthcare costs.45,46 Specifically, the contrasting situation is that physiotherapy referrals can boost health outcomes.46 Since the findings established that Saudi PCPs make referrals based on familiarity with physiotherapy benefits, preventive measures can be boosted through targeted training on MSK conditions.
Multivariable Regression
Multivariable regression analysis identified MSK caseload as the most significant independent predictor of physiotherapy referral frequency. Physicians managing 3–5 patients daily have odds ratios of over 11 times higher than those reporting no MSK caseload. This result makes clinical sense — increased exposure to MSK conditions likely encourages familiarity with physiotherapy indications, established referral habits, and confidence in non-pharmacological treatment options. While prior studies have used regression to examine predictors of physiotherapy referral, these have largely focused on patient-level characteristics such as insurance type, diagnostic subgroup, and demographics.11 The role of physician-level MSK caseload volume as an independent predictor has received limited attention in the literature. Professional rank was the second key predictor, with senior registrars about 2.9 times more likely to refer than consultants. This may indicate that mid-senior physicians have developed some familiarity with physiotherapy indications but have not yet adopted the more specialized referral patterns typical of consultants. Years of experience and the healthcare sector were not significant independent predictors after adjustment for caseload, suggesting that their initial associations with referral frequency could partly be due to the confounding effect of MSK exposure volume.
Physicians’ Recommendations and Implications for Policy
The open-ended responses offered several actionable recommendations. Most frequently, PCPs requested clear national referral guidelines and standardized clinical pathways for MSK care. Such guidelines would ensure consistency in referral decision-making and reduce reliance on individual discretion or sectoral norms. Physicians also strongly advocated digital integration, including embedding referral tools and pathways into existing EMR systems. Digital transformation is a cornerstone of Saudi healthcare reform, and these findings suggest that MSK care could serve as a test case for broader digital adoption.
Additionally, physicians called for improved interprofessional collaboration and ongoing education about physiotherapy indications, benefits, and care models. These findings are consistent with the literature, which emphasizes the importance of multidisciplinary MSK care and shared decision-making.26 Finally, suggested insurance and policy reforms—such as expanded physiotherapy coverage and reduced approval delays—reflect growing awareness among PCPs of the role of financing mechanisms in shaping care accessibility and equity.
Study Limitations and Future Directions
This study has several limitations. The cross-sectional design limits causal inference, and the convenience-based sample from Riyadh constrains generalizability to other Saudi regions or international settings. Further, the findings are based on self-reported data that is prone to social desirability bias. To mitigate these limitations, future studies should cover contextual factors within a longitudinal design. The survey instrument was developed for exploratory purposes and did not undergo formal psychometric reliability testing (eg., Cronbach’s alpha). This represents a limitation of the current instrument; future studies should employ validated tools or conduct a full reliability assessment prior to administration. Furthermore, the absence of technical duplicate-entry controls (such as IP filtering or login-based restrictions) is acknowledged as a methodological limitation, although post-hoc data quality checks identified no duplicate or invalid entries. Additionally, the regression analyses partially account for measured covariates; however, residual confounding from unmeasured variables such as physician workload, patient case mix, and institutional protocols cannot be excluded.
The wide confidence intervals observed for MSK caseload categories reflect the small reference group size (n = 14 for “no MSK patients”), and these estimates should be interpreted with appropriate caution.
Conclusion
This study provides a comprehensive examination of physiotherapy referral practices for MSK conditions among PCPs in Riyadh, Saudi Arabia. Despite the rising burden of MSK disorders, physiotherapy referrals remain relatively infrequent and are influenced by the healthcare sector, professional rank, and the limited use of evidence-based tools. These findings should be interpreted in the context of the study’s cross-sectional design, self-reported data, and convenience-based sampling, which limit causal inference and generalizability beyond the Riyadh setting. Physicians working in government institutions were more likely to refer to physiotherapy, while private-sector physicians favored specialist consultations, highlighting disparities in access and administrative processes. The low awareness and adoption of prognostic stratification tools—such as the Keele STarT MSK Tool—reflect a critical gap between evidence and practice. Systemic challenges, including long waiting times, fragmented referral pathways, and poor interprofessional communication, further compound delays in optimal MSK care. To improve referral quality and patient outcomes, national reforms may benefit from prioritizing the development of standardized clinical guidelines, the integration of decision-support tools into EMRs, and targeted training for PCPs on evidence-based MSK management. Strengthening digital infrastructure and expanding physiotherapy availability across all sectors may also help to address current disparities.
Future research should explore implementation strategies for digital referral systems and evaluate their impact on access, efficiency, and patient outcomes. Addressing these gaps will be key to delivering timely, equitable, and effective MSK care in Saudi Arabia’s evolving healthcare landscape.
Data Sharing Statement
The data produced and/or analyzed in this study can be obtained from the corresponding author upon reasonable request.
Acknowledgments
The authors gratefully acknowledges the Prince Sultan Military Medical City (PSMMC) for their logistical support. The authors also thank the primary care physicians who participated in the study.
Funding
No external funding was received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Rehabilitation 2030 initiative. Available from: https://www.who.int/initiatives/rehabilitation-2030.
2. Safiri S, Kolahi AA, Cross M, et al. Prevalence, deaths, and disability-adjusted life years due to musculoskeletal disorders for 195 countries and territories 1990–2017. Arthritis Rheumatol. 2021;73(4):702–18. doi:10.1002/art.41571
3. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222.
4. Puntillo F, Giglio M, Paladini A, et al. Pathophysiology of musculoskeletal pain: a narrative review. Therap Advanc Musculoskeletal Dis. 2021;13:1759720X21995067. doi:10.1177/1759720X21995067
5. Heikkala E, Karppinen J. Chronic disease clusters and health-related quality of life among individuals with musculoskeletal pain: a Northern Finland Birth Cohort 1966 study. Fam Pract. 2025;42(4):cmaf057. doi:10.1093/fampra/cmaf057
6. Theofilou P, Panagiotaki H. The association between musculoskeletal disorders and quality of life. J Trauma Treat. 2012;1:e101.
7. Qiu K, Wang C, Mo X, et al. The global macroeconomic burden of musculoskeletal disorders. Int J Surg. 2025;111(11):7857–7866. doi:10.1097/JS9.0000000000003072
8. Asmri MA, Almalki MJ, Fitzgerald G, Clark M. The public health care system and primary care services in Saudi Arabia: a system in transition. East Mediterr Health J. 2020;26(4):468–476. doi:10.26719/emhj.19.049
9. Al-Abbad H, Madi S. Perception of tertiary care clients toward the availability of physical therapy service at primary health care centers in Saudi Arabia: a cross-sectional survey. J Phys Ther Sci. 2020;32(5):323–331. doi:10.1589/jpts.32.323
10. Almedlej R, Alsobayel H, Abdelkader S, Alodaibi F. Assessing and comparing musculoskeletal knowledge and red flag identification skills: a cross-sectional study of physical therapists and primary care physicians. Int J Phys Ther Res Pract. 2024;3(7):317–324. doi:10.62464/ijoprp.v3i7.44
11. Freburger JK, Khoja S, Carey TS. Primary care physician referral to physical therapy for musculoskeletal conditions, 2003–2014. J Gen Intern Med. 2018;33(6):801–803. doi:10.1007/s11606-018-4426-6
12. Diener I. Physiotherapy support for self-management of persisting musculoskeletal pain disorders. South African J Physiotherapy. 2021;77(1):1564. doi:10.4102/sajp.v77i1.1564
13. Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391(10137):2368–2383.
14. Dziedzic KS, French S, Davis AM, Geelhoed E, Porcheret M. Implementation of musculoskeletal models of care in primary care settings: theory, practice, evaluation and outcomes for musculoskeletal health in high-income economies. Best Pract Res. 2016;30(3):375–397.
15. Oppong R, Lewis M, Campbell P, et al. Comparison of health-care utilization, costs and health-related quality of life across the subgroups defined by the Keele STarT MSK Tool. Rheumatology. 2023;62(6):2076–2082. doi:10.1093/rheumatology/keac560
16. Alzahrani H, Alshehri MA, Alotaibi M, et al. Burden of musculoskeletal disorders in the gulf cooperation council countries, 1990–2019: findings from the global burden of disease study 2019. Front Med. 2022;9:855414. doi:10.3389/fmed.2022.855414
17. Al-Ajlouni YA, Al Ta’ani O, Mushasha R, et al. The burden of musculoskeletal disorders in the Middle East and North Africa (MENA) region: a longitudinal analysis from the global burden of disease dataset 1990-2019. BMC Musculoskelet Disord. 2023;24(1):439. doi:10.1186/s12891-023-06556-x
18. Alruwaili SH, Thirunavukkarasu A, Alanazi RM, et al. Prevalence, patterns, and associated factors for musculoskeletal disorders among the healthcare workers of Northern Saudi Arabia: a multicenter cross-sectional study. J Pain Res. 2023;16:3735–3746. doi:10.2147/JPR.S415919
19. Hendi OM, Abdulaziz AA, Althaqafi AM, Hindi AM, Khan SA, Atalla AA. Prevalence of musculoskeletal disorders and its correlation to physical activity among health specialty students. Int J Preventive Med. 2019;10(1):48. doi:10.4103/ijpvm.IJPVM_436_18
20. Aljanakh M, Shaikh S, Siddiqui AA, Al-Mansour M, Hassan SS. Prevalence of musculoskeletal disorders among dentists in the Ha’il Region of Saudi Arabia. Ann Saudi Med. 2015;35(6):456–461. doi:10.5144/0256-4947.2015.456
21. Darwish MA, Al-Zuhair SZ. Musculoskeletal pain disorders among secondary school Saudi female teachers. Pain Res Treat. 2013;2013(1):878570. doi:10.1155/2013/878570
22. Shaheen AAM, Almuwais A, Alrushud A, et al. Prevalence and risk factors for neck and upper limb musculoskeletal disabilities among postpartum women. Clin Exp Obstet Gynecol. 2025;52(2). doi:10.31083/ceog25833
23. Foster NE, Dunn KM, Protheroe J, et al. Stratified primary care for adults with musculoskeletal pain: the STarT MSK research programme including RCTs. Programme Grants Appl Res;2023. 1–103. doi: 10.3310/FBVX4177
24. Beneciuk JM, Robinson ME, George SZ. Subgrouping for patients with low back pain: a multidimensional approach incorporating cluster analysis and the STarT Back Screening Tool. J Pain. 2015;16(1):19–30. doi:10.1016/j.jpain.2014.10.004
25. Murphy S, Blake C, Power C, Fullen B. Comparison of a stratified group intervention (STarT Back) with usual group care in patients with low back pain: a nonrandomized controlled trial. SPINE. 2016;41(8):645–652. doi:10.1097/BRS.0000000000001305
26. Saunders B, Hill JC, Foster NE, et al. Stratified primary care versus non-stratified care for musculoskeletal pain: qualitative findings from the STarT MSK feasibility and pilot cluster randomized controlled trial. BMC Fam Pract. 2020;21:1–12. doi:10.1186/s12875-020-1098-1
27. Foster NE, Mullis R, Hill JC, et al. Effect of stratified care for low back pain in family practice (IMPaCT Back): a prospective population-based sequential comparison. Ann Fam Med. 2014;12(2):102–111. doi:10.1370/afm.1625
28. Hill J, Garvin S, Chen Y, et al. Stratified primary care versus non-stratified care for musculoskeletal pain: findings from the STarT MSK feasibility and pilot cluster randomized controlled trial. BMC Family Pract. 2020;21:1–18. doi:10.1186/s12875-019-1074-9
29. Vries T, Deen W, Lucas C. Does the Keele STarT MSK tool predict the risk of poor outcome in non-specific shoulder complaints in primary care in a Dutch population? Physiotherapy. 2024;123:38–46. doi:10.1016/j.physio.2023.10.008
30. Tousignant-Laflamme Y, Houle C, Cook C, Naye F, LeBlanc A, Décary S. Mastering prognostic tools: an opportunity to enhance personalized care and to optimize clinical outcomes in physical therapy. Phys Ther. 2022;102(5):pzac023. doi:10.1093/ptj/pzac023
31. Alabbasi KH, Kruger E, Tennant M. Strengthening Saudi Arabia’s primary health care through an e-referral system: a case study. Clin Pract. 2022;12(3):374–382. doi:10.3390/clinpract12030042
32. Al-Anezi FM. Challenges of healthcare systems in saudi arabia to delivering vision 2030: an empirical study from healthcare workers perspectives. J Healthcare Leadership. 2025;17:173–187. doi:10.2147/JHL.S516159
33. Von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495–1499. doi:10.1016/j.ijsu.2014.07.013
34. Eysenbach G. Improving the quality of web surveys: the checklist for reporting results of internet E-Surveys (CHERRIES). Toronto, Canada: Gunther Eysenbach Centre for Global eHealth Innovation; 2004:e34.
35. Saudi Ministry of Health. Ministry of Health Statistical Yearbook. 2020. Available from: https://www.moh.gov.sa/Ministry/Statistics/book/Pages/default.aspx.
36. Cochran WG. Sampling Techniques. john wiley & sons; 1977.
37. Cohen J. Statistical Power Analysis for the Behavioral Sciences. routledge; 2013.
38. Tousignant-Laflamme Y, Houle C, Longtin C, et al. Prognostic factors specific to work-related musculoskeletal disorders: an overview of recent systematic reviews. Musculoskeletal Sci Pract. 2023;66:102825. doi:10.1016/j.msksp.2023.102825
39. Abdellatif HM, Al-Muallem A, Almansoof AS, et al. Clinical practice guidelines in an era of accountability, Saudi Arabia: a call for action. J Epidemiol Global Health. 2023;13(3):391–396. doi:10.1007/s44197-023-00135-y
40. Crisera VG, AlMubarak AK, Saeedi MY, Memish ZA. Revolutionizing healthcare in KSA: a deep dive into clinical practice guideline development and implementation. J Taibah Univ Sci. 2024;19(6):1202–1211. doi:10.1016/j.jtumed.2024.11.010
41. Alrwaily M, Alanazi F. Evaluation of musculoskeletal medicine knowledge among physicians and physical therapists in Saudi Arabia: a cross-sectional study. 2021.
42. Fanaki C, Fortin J, Sirois M-J, et al. Potential factors influencing adoption of a primary care pathway to prevent functional decline in older adults. Can Geriatr J. 2023;26(2):227. doi:10.5770/cgj.26.646
43. Shorthouse F, Griffin N, McNicholas C, Spahr N, Jones G. Agreement and consistency in the triaging of musculoskeletal primary care referrals by vetting clinicians using a knowledge-based triage tool. Primary Health Care Res Develop. 2023;24:e63. doi:10.1017/S1463423623000361
44. Babatunde OO, Bishop A, Cottrell E, et al. A systematic review and evidence synthesis of non-medical triage, self-referral and direct access services for patients with musculoskeletal pain. PLoS One. 2020;15(7):e0235364. doi:10.1371/journal.pone.0235364
45. Igwesi-Chidobe CN, Bishop A, Humphreys K, et al. Implementing patient direct access to musculoskeletal physiotherapy in primary care: views of patients, general practitioners, physiotherapists and clinical commissioners in England. Physiotherapy. 2021;111:31–39. doi:10.1016/j.physio.2020.07.002
46. Bornhöft L, Larsson ME, Nordeman L, Eggertsen R, Thorn J. Health effects of direct triaging to physiotherapists in primary care for patients with musculoskeletal disorders: a pragmatic randomized controlled trial. Therap Advanc Musculoskeletal Dis. 2019;11:1759720X19827504. doi:10.1177/1759720X19827504
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.