Back to Journals » Patient Preference and Adherence » Volume 14
Exploring Potentially Modifiable Factors That Influence Treatment Non-Adherence Amongst Pediatric Growth Hormone Deficiency: A Qualitative Study
Authors Graham S ![]() , Auyeung V, Weinman J
, Auyeung V, Weinman J ![]()
Received 23 June 2020
Accepted for publication 11 August 2020
Published 13 October 2020 Volume 2020:14 Pages 1889—1899
DOI https://doi.org/10.2147/PPA.S268972
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Selina Graham, Vivian Auyeung, John Weinman
School of Cancer and Pharmaceutical Sciences, King’s College London, London, UK
Correspondence: Selina Graham
School of Cancer and Pharmaceutical Sciences, King’s College London, Franklin-Wilkins Building, London, UK
Email [email protected]
Introduction: A recent systematic review found that up to 71% of children with growth hormone deficiency and their families are non-adherent to treatment as prescribed. A key way to better understanding the complex issue of pediatric non-adherence is to explore the perceptions and experiences of the parent/caregiver. Our study is the first to look specifically at the potentially modifiable factors that influence non-adherence to rhGH treatment amongst parents/caregivers of children with this endocrine disorder.
Methods: Fourteen semi-structured telephone interviews were conducted to explore parents/caregivers’ perceptions and experiences of their child’s condition and prescribed treatment, in addition to their perceived relationship with their healthcare professional. The findings were thematically analyzed and narratively synthesized, in line with the qualitative approach of Braun and Clarke (2006).
Results: Potentially modifiable factors that influence non-adherence to growth hormone treatment were grouped under four themes: 1. Device Burdens, 2. Treatment Considerations, 3. Logistical Interferences and 4. Interpersonal Influences.
Conclusion: Our exploratory study presents the wide range of potentially modifiable factors that influence the way in which growth hormone treatment is used. These findings can, in turn, be used to inform and promote the development of targeted, adherence-focused interventions, to support growth hormone deficient children and their families and optimize the use of prescribed growth hormone treatment within endocrine clinical practice.
Keywords: growth hormone deficiency, GHD, recombinant human growth hormone treatment, rhGH, parent, caregiver, adherence, qualitative
Introduction
Growth hormone deficiency (GHD) occurs when the anterior pituitary gland fails to produce and secrete sufficient levels of growth hormone (GH) to enable the body to grow and manifest at a normal rate.1–5 According to NICE (2010), GHD is a rare medical condition, in which has been reported to affect approximately between one in every 3500–4000 children in the UK.3
As sufficient levels of GH are not produced or secreted naturally, supplementary biosynthetic injections as a prescription medication have been used to replace and replenish the deficient hormone.6–9 Recombinant human growth hormone (rhGH) treatment still remains the only established active treatment option to effectively correct growth failure and increase stature.10 The primary objective of the treatment during childhood and adolescence is to accelerate and normalize height velocity and linear growth, returning the child to the normal growth curve, in order to attain a “normal” or near-normal final adult height within the genetic mid-parental height potential.7,11–13 RhGH treatment is administered via a daily subcutaneous injection, given by the parent/caregiver or self-administered within the home environment.5,9,14 Due to the nature of the condition, rhGH treatment is designed to be a continuous, long-term self-management solution for optimal therapeutic results, typically lasting several years, from childhood to late teenage years/early adulthood.
Despite the advancements of rhGH treatment and the benefits on long-term health outcomes, research has shown that many children with GHD still do not achieve their target genetic adult height.1,15,16 Sub-optimal outcomes have been largely attributed to treatment non-adherence.1,7,15,16
Treatment adherence, defined as “the extent to which a patient’s behavior matches agreed recommendations from their health professional”3,17,18 is essential for achieving therapeutic outcomes. Non-adherence can vary from taking a smaller dose than prescribed, missing a dose intermittently or taking no doses of medication, throughout the different phases of initiation, implementation, and duration/persistence of the regimen.15,18 Sub-optimal adherence compromises the long-term clinical effectiveness of rhGH treatment, leading to delayed growth response, reduced height velocity outcomes, and minimized final adult height.15,16,19,20 As rhGH treatment remains a costly treatment, the impact of non-adherence on the healthcare system, in terms of economic costs, is substantial.21 A recent systematic review on rhGH non-adherence reported that up to 71% of children with GHD and their families are non-adherent to treatment as prescribed.22 Given the effect of non-adherence on the child and their family, the healthcare professionals, and the healthcare system, treatment non-adherence is an important health issue, that warrants attention.17,21
Adherence to rhGH treatment is a complex and multi-faceted issue, that remains poorly understood by both research and clinical practice.1,2,23–25 Previous research primarily involved retrospective database searching, focusing on sociodemographic and clinical variables to explain poor medication adherence (eg, age, parental education level).26,27 Such factors are not amenable to modification and this has therefore led to an increased focus on potentially modifiable factors, such as perceptions, motivations, and beliefs that individuals hold as they make sense of their/their child’s illness and treatment; these concepts have been shown to be strong, predictive determinants of non-adherence across a range of health conditions.28–33
Treatment adherence amongst pediatric patients requires the involvement of a third party: the parent/caregiver.34–36 Many children are diagnosed and prescribed rhGH treatment from early childhood, which requires parents/caregivers to assume the undertaking of the daily injection administration.35,37 Parents/caregivers commonly face a number of increased challenges for the first years of rhGH treatment, and often further into the child’s teenage and young adult years.35–39 Thus, a key way to better understanding the complex issue of pediatric non-adherence to rhGH treatment is to explore the personal perspectives of the parent/caregiver.
Several qualitative studies have explored factors relating to treatment non-adherence, among various clinical indications for rhGH treatment.35–38 There has been limited evidence, however, with regard to the factors that influence non-adherence specifically amongst parents/caregivers of children with GHD. Thus, in light of the findings from the recent systematic review22 and supporting literature,4,7,8,15,40,41 the aim of this qualitative study was to specifically explore the potentially modifiable factors that influence non-adherence to rhGH treatment amongst parents/caregivers of children with GHD. A detailed insight into the barriers to treatment adherence will, in turn, facilitate the design and development of targeted intervention strategies.
Methodology
Ethical Consideration
UK ethical approval was granted by the North East – Newcastle & North Tyneside Research Ethics Committee (ref. 20/NE/0035).
Study Design
A qualitative research approach using semi‐structured interviews was used. The study explored parents’/caregivers’ perceptions and experiences of their child’s condition and prescribed treatment, in addition to their relationship with their HCP.
Participant Recruitment
The target population was purposively recruited between November 2018 and May 2019 via three endocrine outpatient clinics in the United Kingdom (Evelina London Children’s Hospital, Great Ormond Street Hospital and Addenbrooke’s Hospital), a patient research organization: Patient Intelligence Panel Health (PIP Health) and a national GHD-related advocacy and support charity (Child Growth Foundation). Participant identification was conducted by clinical leads [hospital site] and participant leads [Patient-related organizations] with use of a pre-specified inclusion/exclusion criteria. Parent/caregivers were eligible if their child was ≤12 years, diagnosed with GHD (inclusive of subgroups: idiopathic, congenital, secondary/acquired, isolated, or organic) and currently receiving the prescription of rhGH treatment at the commencement of the study. Parent/caregivers were eligible if they were responsible for administering or supervising the rhGH injection on a daily basis and had a sufficient command of the English language. Any parent/caregiver with an indication of cognitive impairment was excluded. Eligible parent/caregivers were provided with an information pack [participant information sheet and participant consent form] via email and invited to participate in the study. Written informed consent was obtained from each participant prior to the interview.
Materials
A semi-structured interview topic guide was developed by the researcher [SG], largely informed by the findings of a previous systematic review,22 discussions with experienced pediatric clinical nurse specialists and input from the Patient Experience Team at Guy’s and St. Thomas’ NHS Foundation Trust (Supplementary Table 1). The topic guide sought to ask questions relating to parental knowledge and understanding of their child’s condition and treatment; living with the condition and the daily management of treatment; the physical, social, and psychological impact of GHD and rhGH treatment; the quality of healthcare communication and support, in addition to treatment adherence.
Data Collection
Data were collected via 14 in-depth telephone interviews. Each telephone interview was conducted by the first author [SG] and audio-recorded using an encrypted digital audio-recording device, with permission of the respondents. The duration time of interviews ranged between 24 and 102 minutes. Data collection continued until no new information relevant to the topic of interest was observed, suggesting theoretical data saturation was attained.
Theoretical and Analytical Approach
The analytical orientation was pre-determined by prior knowledge from a recently conducted systematic review22 and previous comparable literature.35–39 The analyst’s interpretation within the current thematic analysis was guided by a specific focus on the research objective to specifically explore the potentially modifiable factors that influence treatment non-adherence amongst parents/caregivers of children with GHD, although the analyst was open to new contextual ideas and concepts within the raw data. The intention of the analyst was to explore and integrate the diverse views, perspectives, and experiences of the participants and comprehensively report the semantic reality of participants.
Data Analysis
Interviews were independently processed, managed, and analyzed by SG. The interviews were transcribed verbatim and imported onto the qualitative data analysis software NVivo, QSR International Pty Ltd. (2018). All data were anonymized, preserving confidentiality. A rigorous thematic approach was applied to the data, in line with the qualitative approach of Braun and Clarke (2006).42 The data were manually coded; initial ideas and repeated patterns of meaning were formed through the recursive immersion and familiarization of the dataset. Preliminary coding schemes were systematically formulated and organized into provisional subthemes to reflect emerging themes. Codes and subthemes were continuously challenged, discarded, and revised, as potential themes evolved throughout the analytical process. To ensure the reliability and validity of the analyses, codes, and themes were independently cross-checked by two co-researchers [JW and VA]. Any reviewer discrepancies or inconsistencies were resolved by consensus. Overarching themes were further refined to reflect the patterns and relationships evident in the data as a whole. The overview of the main themes, subthemes, and codes, with illustrative quotes is presented in Supplementary Table 3.
Results
Participants
A total of 15 parent/caregiver participants were interviewed [P14 and P15 were parent/caregivers of the same child] (see Table 1). Of the sample group, the mean age of the participants was 46 years, ranging from 34 to 58 years and 93% were female. Amongst the children of the sample group, 64% were male. The youngest child was reported to be 4 years 11 months and the oldest, 10 years 8 months. The length of time on rhGH treatment varied between 2 months and 6 years. The sample group characteristics are detailed in Table 1.
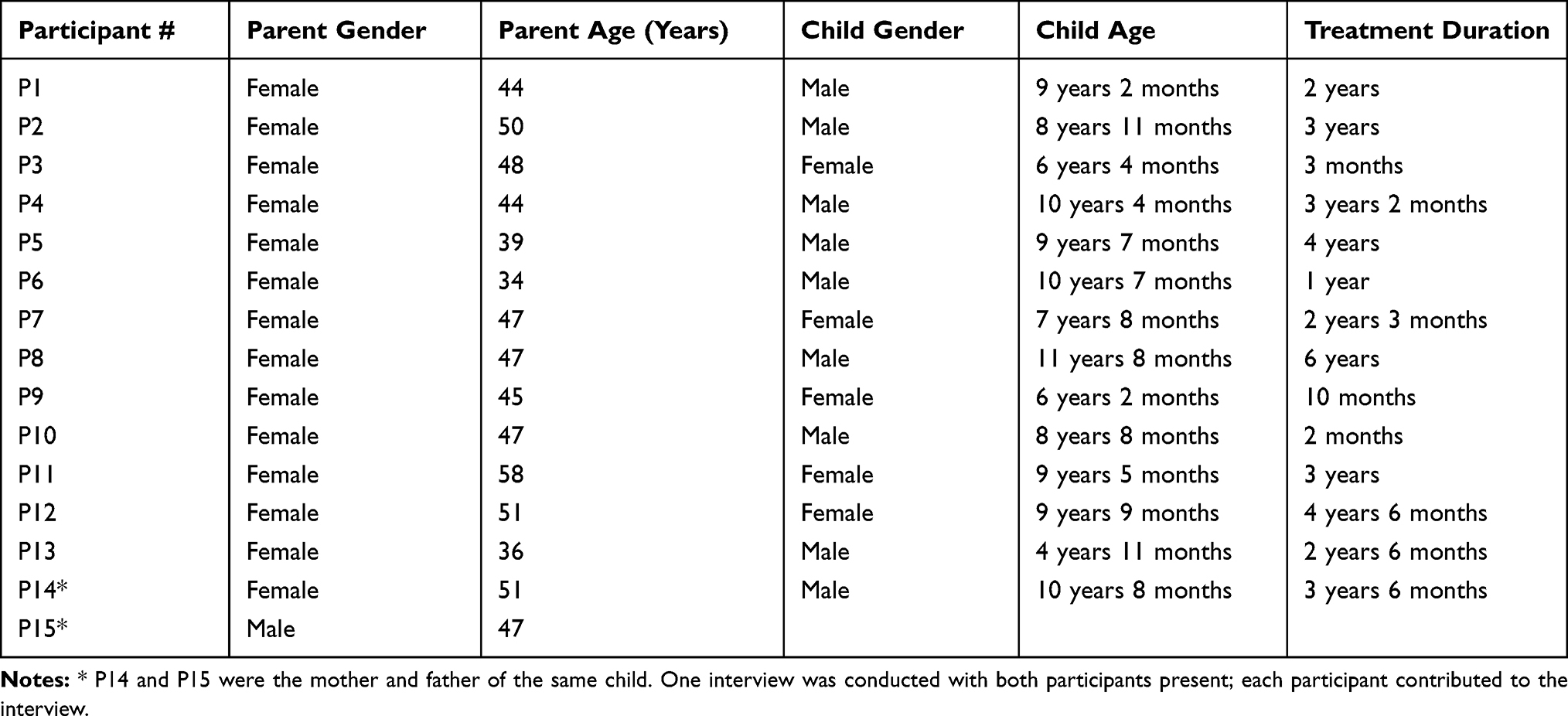 |
Table 1 Sample Characteristics |
Themes
Four core themes and 12 sub-themes derived from the data, as potentially modifiable factors that influence the way in which growth hormone treatment is used: 1) Device Burdens, 2) Treatment Considerations 3) Logistical Interferences and 4) Interpersonal Influences. The summary table of themes is presented in Supplementary Table 2.
Theme 1: Device Burdens
Participants highlighted the burdens experienced during the administration process, which centered around the mechanism of delivery.
Device Issues
Whilst most participants reported to have chosen their own injection device, numerous technical challenges with the device features were described, particularly when preparing or reconstituting the device. Difficulties to administer the injection due to the logistical complexities of the device caused frustration for many participants.
I mean, the other thing that was difficult with our one we use and probably the drawback of it, is that it can be a bit awkward to hold, because you have to hold it, you have to hold it with one hand, so you have to get your finger ready and your thumb on top of the button to push because it is quite stiff, which is quite tricky to do, and you have to have your hand round to click the button, so I mean, it’s quite tricky to push down, you really have to push hard, so it’s difficult. P8 - Mother, 47
Administration Technique
A number of participants reported to struggle with the administration process, in particular, the technical handling of the device, recognizing it to be complicated and confusing. The uneasiness with their poor technique and the negative impact that this had on the administration of rhGH treatment was underlined by participants. Lacking the necessary administration skill, according to the participants, led to unwarranted mistakes being made when attempting the injection, which led to elevated levels of stress for both the participant and child.
It’s really confusing with the pen that we use, you have to pull it back to pull the needle up and sometimes … and a couple of times we’ve found we’ve forgotten to do that and then you end up sticking them with the needle, or you go to press the button and then it hasn’t worked and you got to do it again, so there’s all of that and then you get really stressed. P8 - Mother, 47
Discomfort and Pain from Injection
A number of participants drew attention to the physical discomfort and pain that their children experienced as a result of the injection. Descriptions centered around soreness, bleeding, and bruising. Some participants reported this to be a regular occurrence, others, as more intermittent. Irrespective of the frequency, the incidental consequence of the injection was a source of apprehension for the participants.
He still finds it quite painful, the injection … yesterday was a bit painful for him … sometimes it bleeds as well. P1 - Mother, 44.
Theme 2: Treatment Considerations
Participants shared their personal evaluative concerns which they held about their child’s prescribed rhGH treatment.
Administration Anxieties
Administering the rhGH injection on a daily basis was often linked by participants to feelings of worry and trepidation. The injection process, according to a number of participants was viewed as a daunting and stressful task; some participants disliked handling and using needles, some were worried that they were not administering the dose or managing the treatment correctly and others were anxious about the duty of having to complete the responsibility on a daily basis.
When it comes to, actually giving the injection, I’m worried that I have to give it every day and it has to be repeated. P9 - Mother, 45
You’re nervous about doing it and doing it right. P14 - Mother, 51
Moreover, several participants verbalized that they had experienced feelings of guilt when administering the injection, particularly when they felt they were inflicting pain on their child.
I don’t like doing it, especially when he says that sometimes it does hurt and I just feel horrible …. P1 - Mother, 44
Treatment Concerns
While many participants acknowledged the importance of the treatment for their child, personal fears and uncertainties regarding the treatment were also communicated. Concerns surrounding the side effects of treatment included: the potential side effects that participants had been directly informed about by their HCP, for example, headaches, tumors, etc., as well as the observed side effects which were deemed by the participants as causal by the treatment, for example, early onset of puberty, growing pains, etc.
There was a period of time when she was really struggling walking. She’s growing so quickly that her muscles aren’t working properly and for me, it was perfectly clear that it was the growth hormone. P7 - Mother, 47
In addition, a number of participants expressed conflicted feelings about the benefits of the treatment and the potential long-term adverse consequences for their child. Many questioned their child’s future well-being and quality of life as young adults, as a result of receiving treatment. A lack of understanding of their child’s treatment pathway and the undetermined implications reared a sense of worry and uncertainty for the participants.
It’s pretty scary, you know what I mean? You do, you do, worry that, you know, when they’re in their thirties, that something we did now, turns into a problem, right? You know, we can’t hide from that. P14 - Mother, 51
Feelings of dissatisfaction in relation to their child’s growth response and the effectiveness of the treatment were also cited as concerns by a small number of participants. Using information provided by the HCP and/or social media as reference points, participants had felt that their child’s growth and development were slower than what was expected, resulting in feelings of disappointment and frustration.
From the outset, when you look at pictures of other kids on these sorts of sites, on the Facebook page, and the amount of growth, the difference, it’s sort of astounding in 6 months. It wasn’t like that with X, not at all. P1 - Mother, 44
Theme 3: Logistical Interferences
The challenges of balancing the treatment regimen with the demands of a busy family or social life were highlighted as an issue for many participants.
Inconvenience of Treatment Regimen
A number of participants reported that managing their child’s rhGH treatment interfered with aspects of their family and social life. The requirement to stop or interrupt their daily activities to accommodate the treatment was described by some participants as inconvenient.
It’s an inconvenience, you know. P2 - Mother, 50
As rhGH treatment is recommended by HCPs to be administered in the evening, in order to imitate the normal secretion pattern of human growth hormone, the bedtime routine was reported several times by participants to have been largely impacted, particularly when there were siblings within the family. Participants expressed their frustration at the inopportune dose timing.
It’s just another complication and also if you’ve got other kids and younger kids, their time is particularly full-time, so you’re trying to get your other kids into bed, or stay in bed or whatever and your older kids are doing homework or whatever, so it’s a tricky time and then to deal with a distraught child at that time is quite hard, so it’s a shame really that it has to be so late. We were told that the later he has it before bed, the more effective it will be, so yeah, that was another issue. P8 - Mother, 47
Disruption to Treatment Regimen and Scheduling Issues
Participants identified several lifestyle activities that had interfered with the established treatment routine, for example, when traveling or partaking in social engagements. According to participants, the difficulty to plan, schedule, and undertake the logistics of administration when away from the home environment, had in turn, led to missed rhGH doses.
We travel somewhere and we come back late and the children have fallen asleep in the car, at 9 or 10pm and we transfer them from the car to bed. Very often in that situation, we choose not to give her her injection because she’s half asleep and it would be traumatic. P7 - Mother, 47
Furthermore, participants noted that disruption to the treatment administration occurred when the child specifically was away from the home environment, for example, on school trips or overnight sleepovers. This interference equally created organizational difficulties, thus disturbing the established injection routine.
We just find that, for slightly different reasons, when he’s on school trips or we’re not there, it is difficult and probably is the only time we take a slight view to miss it for a couple of nights. P14 - Mother, 51
Several participants reported that the daily treatment routine was further interrupted during times of illness, for example, when their child suffered with a headache or stomach-ache, etc. As the administration process became practically difficult during this time, this would impel the participant to alter the treatment, as was prescribed.
Well to be honest, there are occasions, we’ll occasionally skip the dose if X is not feeling very well and if she is having an off day or she is feeling unwell and off school, sometimes I will to be honest, I’ll skip the dose. P9 - Mother, 45
Forgetting to Administer Injection
Whilst several participants stated that they forgot to administer their child’s injection inadvertently, “It’s just accidental that we forget.” P9 - Mother, 45, many other participants asserted that forgetting to administer their child’s injection was caused primarily by the disruption to their usual nightly routine, for example, when preoccupied with social engagements or traveling.
On holiday, we forget that first night and then half-way through the holiday, we forget again. It’s so … it’s such a habit thing, it’s such a routine thing that as soon as you break them, it’s easy to forget. P7 - Mother, 47
Theme 4: Interpersonal Influences
Interpersonal relationships were discussed by the participants, in addition to the effect that these interactions had on their personal experiences and management of GHD and rhGH treatment.
Challenge to Administer Injection to Child
Participants described the difficulties that they had experienced when attempting to administer the treatment, largely due to their child’s reluctance, unwillingness, and/or refusal of the injection. According to participants, their child’s aversion towards the treatment stemmed from their nervousness of the needle and/or the pain associated with the injection, both real and anticipated. A number of participants had reflected on the stressful administration process, describing it as “a battle” P1 - Mother, 44, P5 - Mother, 39, and “a nightmare” P5 - Mother, 39. This negative interaction between parent/caregiver and their child resulted in deferred rhGH doses and directly contributed towards feelings of concern towards the adjustment to treatment.
We had several weeks where it was horrendous. I mean, I was crying, he was crying. It was terrible … he was upset and fighting me, that was a real low point, I’ll be honest with you. P1 - Mother, 44
Lack of HCP Information Input
HCPs were another key interpersonal influence cited amongst participants. Despite initial discussions with their HCP regarding the nature of their child’s condition, it was frequently verbalized that participants had felt, on reflection, that they were not well informed and the information that they had received was minimal and vague. Knowledge and understanding gaps increased participants’ ambiguity about their child’s condition and medical pathway.
The doctors were vague, very vague …. with the consultant, when you’re trying to understand about what went wrong, there was vagueness, no clear answers. P7 - Mother, 47
Lack of Knowledge and Understanding of the Condition
Furthermore, the majority of participants acknowledged their insufficient level of knowledge and understanding of their child’s condition and medical journey, for example, the cause or the consequences of the condition. According to participants, this awareness led to feelings of uncertainty, when endeavoring to manage their child’s condition.
It’s really difficult, because you know, we don’t really know and the hospital doesn’t really know and you are kind of feeling your way through it. P8 - Mother, 47
Poor HCP-Parent/Caregiver Communication
In addressing the quality of their interaction with their healthcare professional, a number of participants had expressed feeling frustrated and unsupported as the result of the poor communication received within their consultations. Criticism was directed at the consultants, in particular, by a number of participants, as they had felt at times, their concerns and uncertainties regarding their child’s condition and/or treatment had not been listened to or acknowledged.
You know how arrogant some consultants can be, and that I found, yeah, that, I found quite difficult, because at least it should be an open dialogue. P7 - Mother, 47
Moreover, several participants had reported to feeling dismissed or intimidated on occasion by members of the clinical team, especially when they had attempted to raise a condition or treatment-related concern in their bi-annual consultation.
They often have that attitude of parents being a burden. P7 - Mother, 47
Issues concerning the interpersonal interaction between the parent/caregiver and the HCPs had, as a result, led many participants to be increasingly reluctant to discuss their worries or express their concerns within their consultations.
I know what it’s like to feel intimidated by your doctor …you don’t feel like you can ask a question and then you take away this treatment and you don’t feel like you can ring up to ask a question. P6 - Mother, 34
Discussion
With previous evidence highlighting that up to 71% of growth hormone deficient children and their families are non-adherent to treatment as prescribed,22 the aim of our exploratory qualitative study was to gain a detailed insight into the potentially modifiable factors which influence and inform the way in which rhGH treatment is used. Four core themes derived from the thematic analysis of the data, which encapsulated the parents’/caregivers’ perceptions and experiences of GHD and rhGH treatment: 1) Device Burdens, 2) Treatment Considerations, 3) Logistical Interferences, and 4) Interpersonal Influences.
Within our study, participants highlighted the physical burdens experienced during the administration process, focusing primarily on the burdens of the device. As has been reported in previous qualitative literature,35,37,38 participants reported to experiencing complications with the device features, difficulties with the technical handling of the device, and tensions with the physical consequence of the injection for their child, namely the pain and discomfort. These burdens, in turn, had been a source of frustration and apprehension for the participants, thus in turn, impacting upon their treatment behavior. While participants generally expressed strong beliefs about the necessity of the treatment, they all communicated personal concern(s) of the treatment. Concerns about treatment centered primarily around: the worry and guilt surrounding the administration, the fear of side effects, and the long-term implications, as well as the dissatisfaction to its effectiveness, which aligns with previous descriptive work.35–38 Participants’ concerns were often linked to feelings of uncertainty, thus making treatment management a continual challenge. The challenges of balancing the treatment regimen with other aspects of family or social life were also highlighted as an issue for many participants. Participants reported encountering unanticipated technical and organizational challenges, whilst managing their child’s treatment on a daily basis. In line with prior studies,36–38 interferences such as family travel, school events, social engagements, illness, and the need to interrupt their own daily activities to accommodate the treatment, had a negative impact upon the established treatment schedule and thus treatment adherence, as these logistical interferences, often led to delayed, missed, or forgotten doses. The impact of interpersonal relationships on the management of GHD and rhGH treatment is consistent with the findings of earlier studies.36,37 Participants described the challenges that they faced, when attempting to administer the daily treatment to their child, obtain the necessary information from their HCPs; and to be heard, understood, and valued within their consultations. These negative interactions directly contributed to feelings of anxiety and frustration for many participants, thus exacerbating concern towards the adjustment to treatment.
The broad range of factors found within our study concurs fully with the wider literature, which has identified factors associated with non-adherence to rhGH treatment,1,2,5,11,12 specifically amongst pediatric GHD,4,7,8,15,40,41 and in particular, to several qualitative studies which have explored the perspectives of parents/caregivers of children receiving rhGH treatment.35–38
This study presents an in-depth description of the wide range of potentially modifiable factors that influence low levels of treatment adherence amongst this population. In order to explore treatment non-adherence further and provide an overview of the determining factors, a novel and unique approach was implemented to our findings; the 12 potentially modifiable factors [subthemes] found to influence adherence to rhGH treatment amongst pediatric GHD were mapped and categorized according to the components of the COM-B (capability, opportunity, motivation – behavior) framework (see Table 2). The theoretical framework, with reference to previous and existing theories of behavior, conceptualizes, and categorizes the wide range of drivers of treatment non-adherence.43 Using an established theoretical framework to manage the factors found to influence treatment non-adherence within this exploratory study is a key strength as it can, in turn, be used to guide the development of targeted, evidence-based strategies, to better support treatment adherence amongst pediatric growth hormone deficiency.44
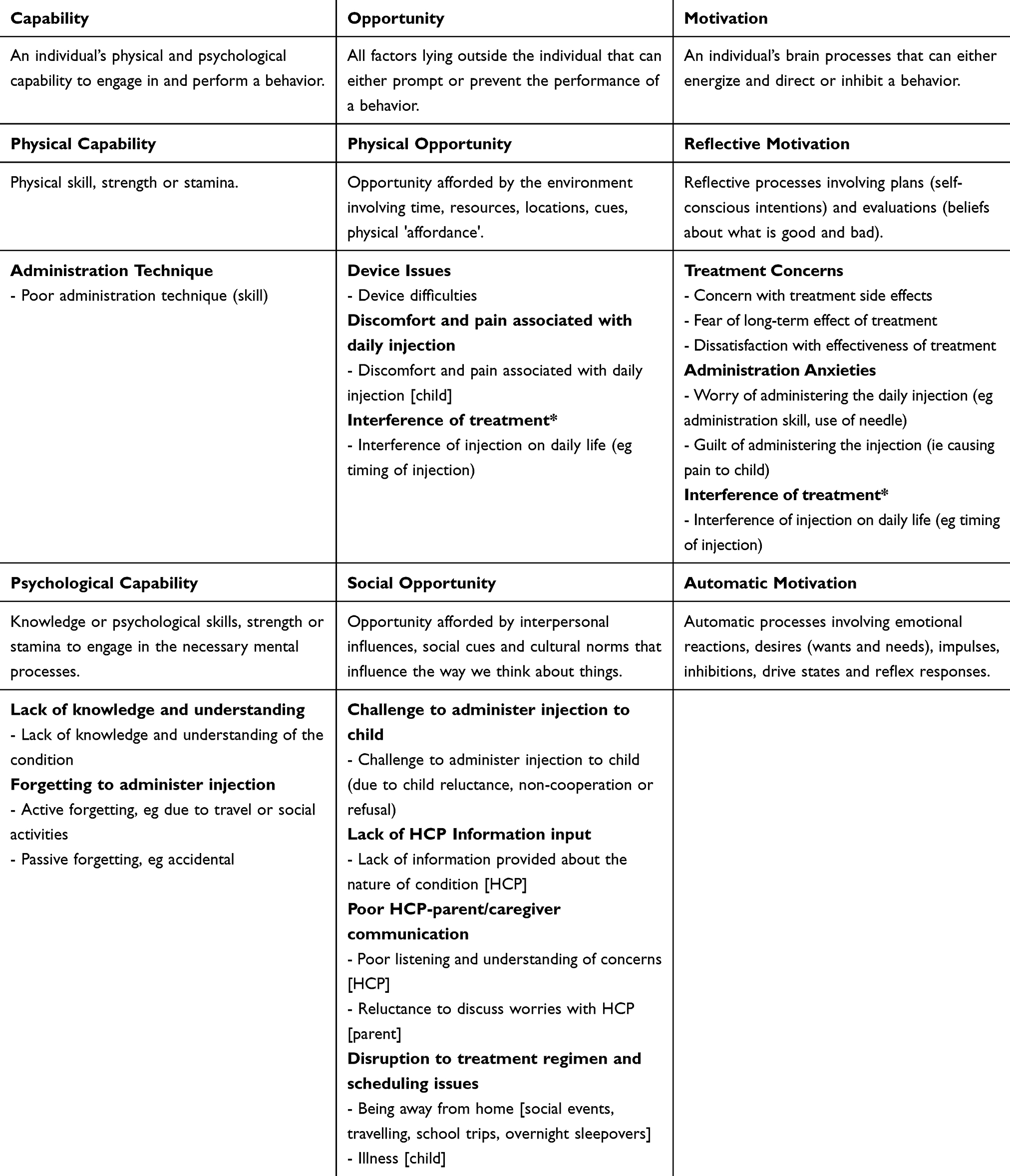 |
Table 2 Themes Mapped Onto the COM-B Framework as Potentially Modifiable Determinants of Non-Adherence to rhGH Treatment Amongst Pediatric GHD |
Limitations
Although several important themes were found within our study, there were some limitations within our sample and methodology. Firstly, our findings are limited by the use of a small purposively selected sample, therefore creating a level of ambiguity regarding the generalizability of the data. Secondly, our analytical process was largely guided by existing assumptions and conducted through the systematic method of locating responses to a defined research focus, rather than via the purely inductive exploration of the raw data. Due to this top-down approach, important aspects of the data, such as the facilitators of treatment adherence were unaccounted for. To further contribute towards the work supporting the use of rhGH treatment, it is recommended that where possible, future research in this area should explore the factors related to good treatment adherence.
Conclusion
Our exploratory study presents an in-depth description of the wide range of potentially modifiable factors that influence treatment non-adherence amongst this population. These findings can be used to inform and promote the development of targeted, adherence-focused interventions, to support growth hormone deficient children and their families and optimize the use of prescribed rhGH treatment within endocrine clinical practice.
Ethics Approval and Informed Consent
UK ethical approval was granted by the North East – Newcastle & North Tyneside Research Ethics Committee (ref. 20/NE/0035). Written informed consent was obtained prior to each interview. All participants have given written informed consent to publish their case (with anonymity).
Acknowledgment
The study forms part of a wider PhD research project which is funded by Merck Serono Ltd.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The study has been funded by Merck Serono Ltd. via an unrestricted educational grant. The funding organization has not played any role in the preparation of data or the manuscript, nor in the decision to submit the manuscript for publication.
Disclosure
Professor John Weinman received an unrestricted educational grant from Merck Serono Ltd., which funded the research reported in this paper. Professor John Weinman has also received fees from Merck Serono Ltd., for conference presentations. The authors report no other conflicts of interest in this work.
References
1. Fisher BG, Acerini CL. Understanding the growth hormone therapy adherence paradigm: a systematic review. Horm Res Paediatr. 2013;79(4):189–196. doi:10.1159/000350251
2. Haverkamp F, Johansson L, Dumas H, et al. Observations of nonadherence to recombinant human growth hormone therapy in clinical practice. Clin Ther. 2008;30(2):307–316. doi:10.1016/j.clinthera.2008.02.017
3. Neilson NV, Flynn O, Kuntze CN, et al. Medicines adherence: involving patients in decisions about prescribed medicines and supporting adherence full guideline. 2009; Available from: www.rcgp.org.uk.
4. Hartmann K, Ittner J, Müller-Rossberg E, et al. Growth hormone treatment adherence in prepubertal and pubertal children with different growth disorders. Horm Res Paediatr. 2013;80(1):1–5. doi:10.1159/000351800
5. Mohseni S, Heydari Z, Qorbani M, Radfar M. Adherence to growth hormone therapy in children and its potential barriers. J Pediatr Endocrinol Metab. 2018;31(1):13–20. doi:10.1515/jpem-2017-0157
6. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–497. doi:10.1056/NEJMra050100
7. Aydın B, Aycan Z, Şıklar Z, et al. Adherence to growth hormone therapy: results of a multicenter study. Endocr Pract. 2014;20(1):46–51. doi:10.4158/EP13194.OR
8. Lass N, Reinehr T. Low treatment adherence in pubertal children treated with thyroxin or growth hormone. Horm Res Paediatr. 2015;84(4):240–247. doi:10.1159/000437305
9. Dumas H, Panayiotopoulos P, Parker D, Pongpairochana V. Understanding and meeting the needs of those using growth hormone injection devices. BMC Endocr Disord. 2006;6(1):5. doi:10.1186/1472-6823-6-5
10. Reh CS, Geffner ME. Somatotropin in the treatment of growth hormone deficiency and turner syndrome in pediatric patients: a review. Clin Pharmacol. 2010;2:111–122. doi:http://doi.10.2147/CPAA.S6525
11. Bagnasco F, Di Iorgi N, Roveda A, et al. Prevalence and correlates of adherence in children and adolescents treated with growth hormone: a multicenter italian study. Endocr Pract. 2017;23(8):929–941. doi:10.4158/EP171786.OR
12. Kremidas D, Wisniewski T, Divino VM, et al. Administration burden associated with recombinant human growth hormone treatment: perspectives of patients and caregivers. J Pediatr Nurs. 2013;28(1):55–63. doi:10.1016/j.pedn.2011.12.006
13. Oyarzabal M, Aliaga M, Chueca M, Echarte G, Ulied A. Multicentre survey on compliance with growth hormone therapy: what can be improved? Acta Paediatr. 1998;87(4):387–391. doi:10.1111/j.1651-2227.1998.tb01464.x
14. Human growth hormone (somatropin) for the treatment of growth failure in children guidance and guidelines. NICE; 2010. Available from https://www.nice.org.uk/guidance/ta188.
15. Cutfield WS, Derraik JGB, Gunn AJ, et al. Non-compliance with growth hormone treatment in children is common and impairs linear growth. PLoS One. 2011;6(1): e16223.
16. Polak M, Blair J, Kotnik P, Pournara E, Pedersen BT, Rohrer TR. Early growth hormone treatment start in childhood growth hormone deficiency improves near adult height: analysis from NordiNet® international outcome study. Eur J Endocrinol. 2017;177(5):421–429. doi:10.1530/EJE-16-1024
17. Sabaté E, World Health Organization. Adherence to Long-Term Therapies: Evidence for Action. World Health Organization; 2003:194.
18. Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73(5):691–705. doi:10.1111/j.1365-2125.2012.04167.x
19. Bozzola M, Pagani S, Iughetti L, Maffeis C, Bozzola E, Meazza C. Adherence to growth hormone therapy: a practical approach. Horm Res Paediatr. 2014;81(5):331–335. doi:10.1159/000357975
20. Koledova E, Stoyanov G, Ovbude L, Davies PSW. Adherence and long-term growth outcomes: results from the easypodTM connect observational study (ECOS) in paediatric patients with growth disorders. Endocr Connect. 2018;7(8):914–923. doi:10.1530/EC-18-0172
21. Khan R, Socha-Dietrich K. Investing in medication adherence improves health outcomes and health system efficiency: adherence to medicines for diabetes, hypertension, and hyperlipidaemia. OECD Health Work Pap. 2018;(105). doi:10.1787/8178962c-en
22. Graham S, Weinman J, Auyeung V. Identifying potentially modifiable factors associated with treatment non-adherence in paediatric growth hormone deficiency: a systematic review. Horm Res Paediatr. 2018;90(4):1–7. doi:10.1159/000493211
23. Haverkamp F, Gasteyger C. A review of biopsychosocial strategies to prevent and overcome early-recognized poor adherence in growth hormone therapy of children. J Med Econ. 2011;14(4):448–457. doi:10.3111/13696998.2011.590829
24. Kardas P, Lewek P, Matyjaszczyk M. Determinants of patient adherence: a review of systematic reviews. Front Pharmacol. 2013;4:91. doi:10.3389/fphar.2013.00091
25. Mathes T, Jaschinski T, Pieper D. Adherence influencing factors – a systematic review of systematic reviews. Arch Public Health. 2014;72(1):37. doi:10.1186/2049-3258-72-37
26. De Pedro S, Murillo M, Salinas I, et al. Variability in adherence to rhGH treatment: socioeconomic causes and effect on children’s growth. Growth Horm IGF Res. 2016;26:32–35. doi:10.1016/j.ghir.2015.12.002
27. Gács G, Hosszu E. The effect of socio-economic conditions on the time of diagnosis and compliance during treatment in growth hormone deficiency. Acta Paediatr Hung. 1991;31(2):215–221.
28. Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47(6):555–567. doi:10.1016/S0022-3999(99)00057-4.
29. Weinman J, Graham S, Canfield M, et al. The intentional non-adherence scale (INAS): initial development and validation. J Psychosom Res. 2018;115:110–116. doi:10.1016/j.jpsychores.2018.10.010
30. Weinman J, Petrie KJ. Illness perceptions: a new paradigm for psychosomatics? J Psychosom Res. 1997;42(2):113–116. doi:10.1016/S0022-3999(96)00294-2
31. Horne R, Chapman SCE, Parham R, Freemantle N, Forbes A, Cooper V. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: a meta-analytic review of the necessity-concerns framework. Xia Y, editor. PLoS One. 2013;8(12):e80633.
32. Petrie KJ, Weinman J. Why illness perceptions matter. Clin Med. 2006;6(6):536–539. doi:10.7861/clinmedicine.6-6-536
33. Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception questionnaire. J Psychosom Res. 2006;60(6):631–637. doi:10.1016/j.jpsychores.2005.10.020
34. Matsui DM. Drug compliance in pediatrics. Clinical and research issues. Pediatr Clin North Am. 1997;44(1):1–14. doi:10.1016/S0031-3955(05)70459-4
35. van Dongen N, Kaptein AA. Parents’ views on growth hormone treatment for their children: psychosocial issues. Patient Prefer Adherence. 2012;6:547–553. doi:10.2147/PPA.S33157
36. Marini MG, Chesi P, Mazzanti L, et al. Stories of experiences of care for growth hormone deficiency: the CRESCERE project. Future Sci OA. 2016;2(1):
37. Alsaigh R, Coyne I. Mothers’ experiences of caring for children receiving growth hormone treatment. J Pediatr Nurs. 2019;49(1):e63–73. doi:10.1016/j.pedn.2019.09.005
38. Brod M, Højbjerre L, Alolga SL, Beck JF, Wilkinson L, Rasmussen MH. Understanding treatment burden for children treated for growth hormone deficiency. Patient. 2017;10(5):653–666.
39. Brod M, Alolga SL, Beck JF, Wilkinson L, Højbjerre L, Rasmussen MH. Understanding burden of illness for child growth hormone deficiency. Qual Life Res. 2017;26(7):1673–1686. doi:10.1007/s11136-017-1529-1
40. Rosenfeld R, Bakker B. Compliance and persistence in pediatric and adult patients receiving growth hormone therapy. Endocr Pract. 2008;14(2):143–154. doi:10.4158/EP.14.2.143
41. Kapoor RR, Burke SA, Sparrow SE, et al. Monitoring of concordance in growth hormone therapy. Arch Dis Child. 2008;93(2):147–148. doi:10.1136/adc.2006.114249
42. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
43. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6(1):42. doi:10.1186/1748-5908-6-42
44. Jackson C, Eliasson L, Barber N, Weinman J. Applying COM-B to medication adherence. Eur Health Psychol. 2014;16(1):7–17.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.