Back to Journals » Journal of Pain Research » Volume 11
Exploring patients’ experiences of the whiplash injury-recovery process – a meta-synthesis
Authors Söderlund A ![]() , Nordgren L
, Nordgren L ![]() , Sterling M, Stålnacke BM
, Sterling M, Stålnacke BM ![]()
Received 4 December 2017
Accepted for publication 17 April 2018
Published 29 June 2018 Volume 2018:11 Pages 1263—1271
DOI https://doi.org/10.2147/JPR.S158807
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Anne Söderlund,1 Lena Nordgren,2,3 Michele Sterling,4,5 Britt-Marie Stålnacke6–8
1Department of Physiotherapy, School of Health, Care and Social Welfare, Mälardalen University, Västerås, Sweden; 2Center for Clinical Research Sörmland (CKFD), Uppsala University, Eskilstuna, Sweden; 3Department of Public Health and Caring Sciences, Uppsala University, Uppsala, Sweden; 4Recover Injury Research Centre, NHMRC Centre of Research Excellence in Road Traffic Injury, The University of Queensland, Herston, QLD, Australia; 5Menzies Health Institute Queensland, Griffith University, Brisbane, QLD, Australia; 6Department of Community Medicine and Rehabilitation, Rehabilitation Medicine, Umeå University, Sweden; 7Department of Clinical Sciences, Karolinska Institute, Stockholm, Sweden; 8Department of Rehabilitation Medicine, Danderyd Hospital, Stockholm, Sweden
Purpose: The aim of this study was to conduct a meta-synthesis to analyze qualitative research findings and thereby understand patients’ experiences of whiplash-associated disorders (WAD) and the injury-recovery process.
Materials and methods: A qualitative meta-synthesis, which is an interpretive integration of existing qualitative findings, was performed. The databases PubMed, PsychINFO, Scopus, and Web of Science were searched. The Critical Assessment Skills Programme was used to assess the quality of the included studies.
Results: Four studies were included. The synthesis resulted in several codes, 6 categories, and 3 themes (distancing from normalcy, self-efficacy in controlling the life situation after the injury, and readjustment and acceptance) that described the participants’ pain beliefs, their WAD-related life situation and their future expectations and acceptance. Changes in self-image were difficult to cope with and likely led to perceived stigmatization. Struggling with feelings of loss of control appeared to lead to low confidence and insecurity. Focusing on increasing knowledge and understanding the pain and its consequences were believed to lead to better strategies for handling the situation. Furthermore, recapturing life roles, including returning to work, was challenging, but an optimistic outlook reinforced symptom improvements and contributed to feelings of happiness.
Conclusion: The results of the present study provide a comprehensive understanding of patients’ complex, multifaceted experiences of WAD, and the injury-recovery process. The findings can guide us in the development of new ways to evaluate and manage WAD. The results also indicate that a more patient-centered approach is needed to determine the depth and breadth of each patient’s problems.
Keywords: whiplash-associated disorders, control, self-efficacy, happiness, life situation
Introduction
The process of designing next-generation outcomes and management methods to better meet the needs of patients with whiplash-associated disorders (WAD) must involve a broader approach than is currently used. Because the outcome measures and management methods used for WAD are mostly based on studies at group level using standard measures but not based on an individual’s specific needs, it is important to explore the experiences of patients with WAD during the process from injury to recovery.
In the context of WAD, there is no accepted standardized definition for recovery. Sterling et al1 defined the prognosis for clinical recovery by identifying 3 pathways through a trajectory-modeling analysis in which the prognostic factor was the severity of the initial pain-related disability (mild, moderate, or severe) measured at the group level and using standard measures. However, at the individual level, patients themselves most likely define recovery differently depending on their life situation. Thus, patients’ thoughts regarding the injury-recovery process could be significant for their symptom management.
Efforts to manage WAD in current practice still struggle to find the most effective ways to solve pain- and disability-related problems during the recovery process. Exercise as a management method has been studied and is recommended extensively to facilitate recovery, as described in a recent systematic review.2 However, the conclusion of that review was that there was no evidence that general exercise interventions led to long-term improvements.2 Patient education3 and advice4 are often used, either alone or in combination with other methods, to stimulate recovery from WAD. However, the evidence for education is equivocal, and related trials have shown small effects.3 The difficulties of finding effective treatment and management strategies for WAD might be due to the complexity of the disorder and a great variation of pain-related problems between individuals, which clinicians and researchers have not fully comprehended. To complement current practice, we must understand patients’ experiences of WAD and determine what patients believe would support their recovery process.
The situation is similar for the outcomes used in the WAD context. Quantifying patients’ perceptions of their WAD-related life situation is not easy. As a basis for determining what to measure and where to direct the management and treatment,5,6 the biopsychosocial model plays an important role in the WAD context. However, when only the biopsychosocial model is used, there is no guarantee that patients’ perceptions of their WAD-related life situation will be addressed and targeted during evaluation and management. A description of patients’ perceptions of their neck pain and how they experience the process from injury to recovery7,8 is important for modernizing the management of WAD. Thus, the aim of this study was to conduct a meta-synthesis to analyze qualitative research findings and thereby understand patients’ experiences of WAD and the injury-recovery process.
Materials and methods
Design
A qualitative meta-synthesis was applied. Meta-synthesis is defined being as an interpretive integration of existing published qualitative findings.9
Data sources
The PubMed, PsychINFO, Scopus, and Web of Science databases were independently searched. Additionally, the reference lists of the included studies were manually screened to complement the database search. The following keywords were used in the indicated combinations: whiplash, whiplash associated disorders, WAD, expectations or beliefs, recovery, qualitative or phenomenography, and focus group or interview. The search was performed in June 2017, and the range of publication dates was not limited.
The inclusion criteria were as follows: qualitative original studies, reported in the English language, the sample comprised participants with WAD, data collected via individual interviews or via a combination of individual interviews and focus groups, and the results relevant to the aim of this meta-synthesis. The titles and abstracts were screened, and the full text of studies that fulfilled the inclusion criteria was evaluated.
Data extraction and quality assessment
Data were extracted by the first author and cross-checked by the other authors independently. The Critical Assessment Skills Programme (CASP) was used to assess the quality of the included studies.10 The CASP has been used extensively in previous qualitative reviews.11–13 The CASP includes 10 statements (see Table 1) with the response alternatives yes/no/can’t tell. All authors independently assessed the quality of the included studies to increase trustworthiness. Disagreements were resolved by consensus discussions among the authors.
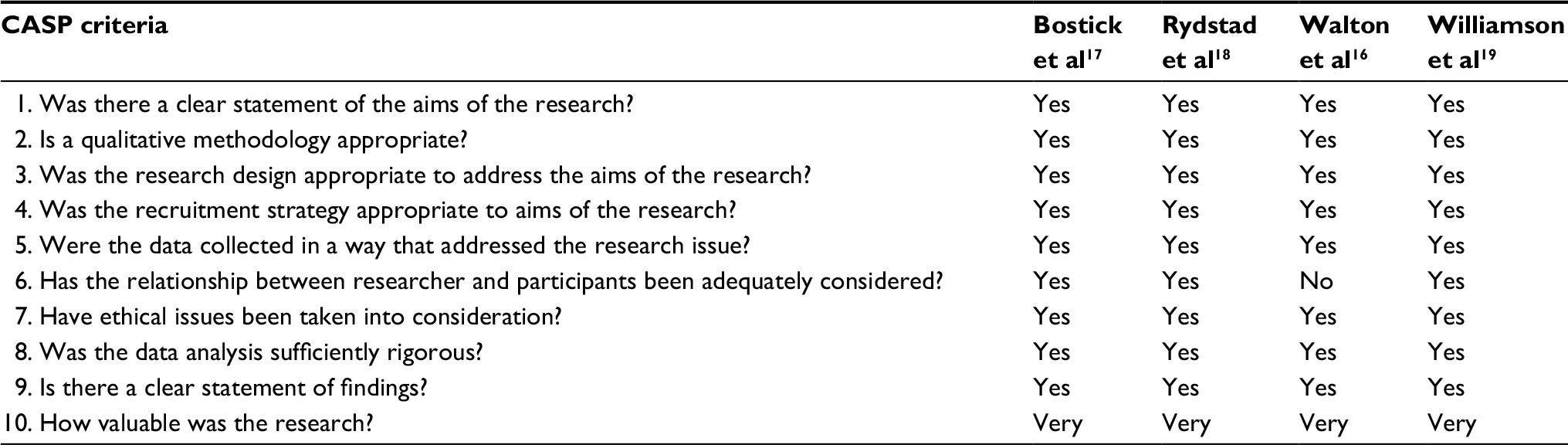 | Table 1 The quality assessment by Critical Appraisal Skills Program (CASP) criteria; response options are Yes/No/Can’t tell Note: Reproduced from Critical Appraisal Skills Programme (CASP) Qualitative Checklist. [online] Available at: www.casp-uk.net.10 |
Data synthesis and analysis
We applied the principles for analysis as recommended by Sandelowski and Barroso9 and Walsh and Downe.14 First, we tabulated the key findings from each study. Second, the quality of the studies was assessed using the CASP statements.10 Third, by reading and re-reading the results of the included studies, we attempted to capture all the relevant descriptors from the original text before synthesizing these finding into the results. Fourth, we used reciprocal translation, which aims to translate the included studies’ findings one at a time into categories that the next study’s findings can confirm or extend while allowing space for divergent and deviant data to refute the identified categories and add new categories. Finally, we synthesized the categories into themes, thus elucidating more refined meanings than each study alone could identify.
Trustworthiness of the meta-synthesis authors
The authors of this meta-synthesis are all senior researchers. All but one (LN) has extensive clinical and research experience in WAD-related health problems. All the authors have experience in qualitative research, but LN has a particularly extensive and varied experience with different qualitative designs and analysis methods. All the authors are well aware of the possible problems that reflexivity and preconceptions15 could cause in this type of study, and all authors reflected on these issues during the meta-analysis process.
Results
A total of 57 studies were identified in the first stage, and 4 studies were ultimately eligible for inclusion in this meta-synthesis. Figure 1 presents the study identification process. In total, 81 individuals with WAD were interviewed in the studies; see Table 2 for more details.
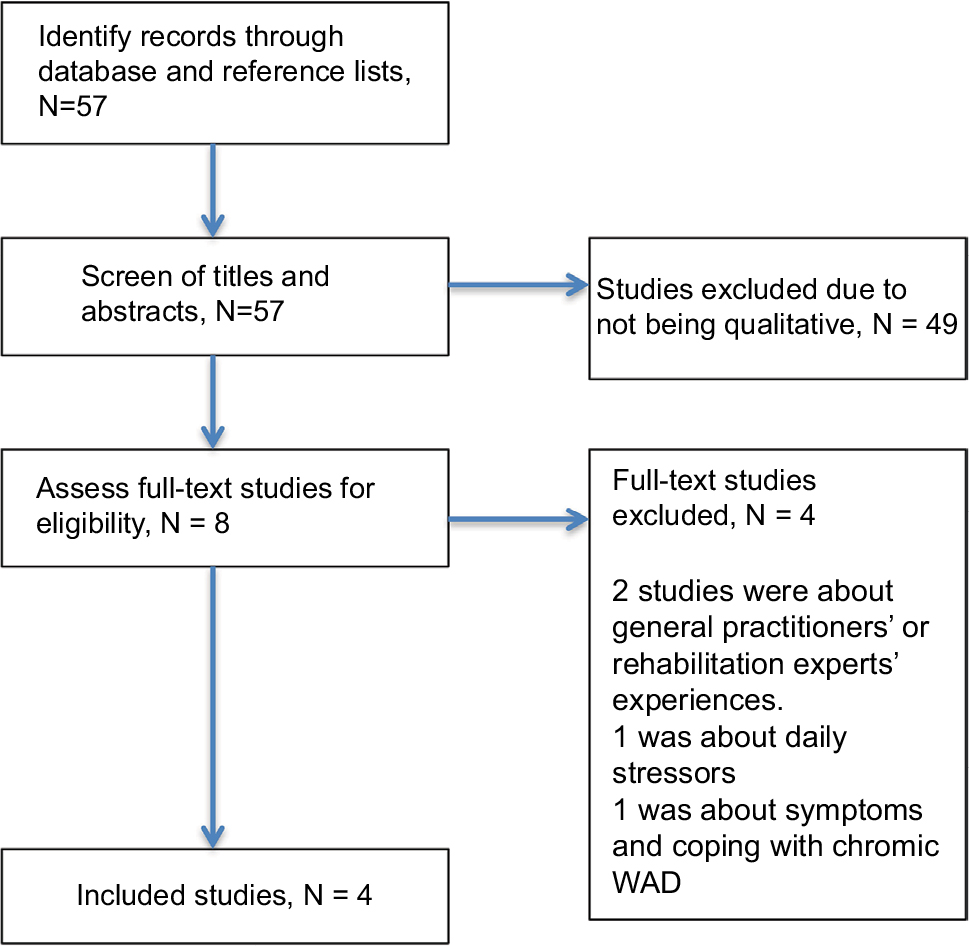 | Figure 1 PRISMA flow diagram Abbreviations: PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; WAD, whiplash-associated disorders. |
 | Table 2 Characteristics and key findings of the included studies Abbreviation: WAD, whiplash-associated disorders. |
The results of the quality assessment of the included studies are presented in Table 1.
The synthesis resulted in 29 codes, 6 categories, and 3 themes. The themes were “distancing from normalcy, self-efficacy in controlling the life situation after the injury, and readjustment and acceptance”. The themes, categories, and codes are presented in Table 3.
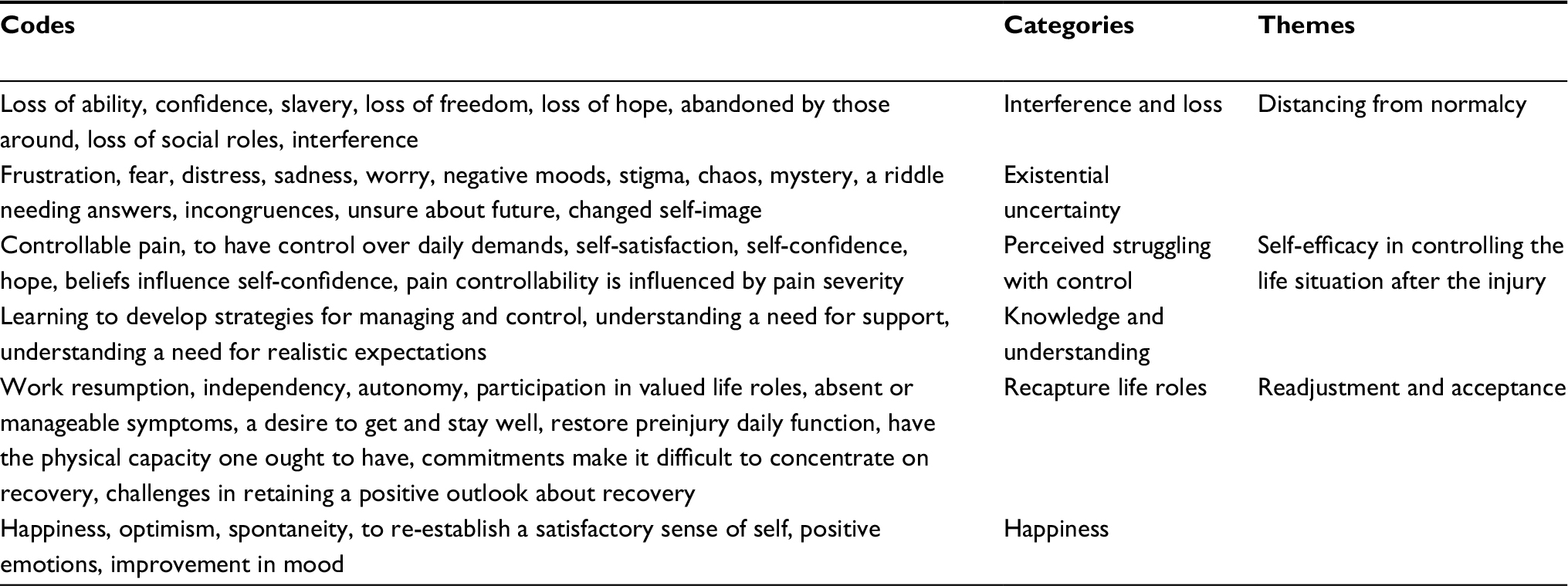 | Table 3 The synthesized themes and categories from the initial findings in the included studies, shortened to codes Note: Categories describe meaning and content of the codes, and themes synthesize the meaning and content of categories. |
Distancing from normalcy
Interference and loss
The participants talked about pain and other symptoms interfering with their lives and about the loss of hope, ability, social roles, autonomy, and spontaneity. The participants also noted that it was difficult to continue exercising even though they believed exercise was beneficial. The participants believed that they had lost the physical capacity they had before the injury,16 and they felt sad and helpless about all physical, psychological, and social losses that were consequences of WAD.16,17 The participants sought to resume the normalcy,17 autonomy, and spontaneity of life experienced before the accident.16
Existential uncertainty
WAD changed the participants’ self-image,18 and the participants felt that their previous self-image was difficult to re-establish.16 The changes in self-image likely contributed to the participants’ existential uncertainty and feelings of being stigmatized.17,18 The participants felt that other individuals without WAD and pain labeled them negatively because there was no visible evidence of their pain.17 The invisibility of pain also contributed to the participants’ belief that others thought they were malingering.17
Self-efficacy in controlling the life situation after the injury
Perceived struggling with control
The participants struggled with their confidence in their ability to control their pain and daily life. Low perceived control appeared to lead to low confidence and insecurity regarding the ability to manage injury-related problems and the future.19 In contrast, perceived positive outcomes of treatment contributed to increased perceived control.17 Additionally, support from health care staff and significant others was an important part of being able to control the situation.18,19 At the same time, some participants believed that they needed to take responsibility for the situation themselves to increase their ability to control it.19
The perceived severity,17 manageability,16 and realistic expectations19 of symptom development also influenced the participants’ feelings of control. Severe symptoms were difficult to tolerate and manage and decreased the participants’ beliefs and confidence regarding their ability to control the situation. The participants did not always know what worsened pain and other WAD-related symptoms. The participants tried to determine how to control their situation but did not often succeed. Consequently, their confidence in their ability to manage pain and participate in daily activities decreased.
Knowledge and understanding
Knowledge of how medication, pain, and other symptoms were associated was believed to make the situation more understandable and could lead to the development of better strategies for coping with the situation.17,18 Additionally, an understanding of the pain was believed to contribute to its elimination. However, when the expectations of recovery were not fulfilled quickly enough, confusion and conflicting thoughts about outcomes arose.17 The participants needed to prioritize different commitments according to how they believed their pain and other symptoms would be aggravated.19 Knowledge about and experiences of participation in physical activity were perceived to be beneficial,18 although physical activity was not always easy to prioritize.19
Readjustment and acceptance
Recapture life roles
Returning to work was perceived as a challenging outcome.18 The combination of expectations regarding recovery and daily experiences of fluctuating symptoms decreased the participants’ confidence concerning the future19 and their return to work.18 Supportive health care staff, colleagues, and employers were of great importance in increasing the participants’ confidence in their ability to return to work. Perceived work-related stress and aggravated symptoms decreased their confidence in their ability to return to work, while different adaptations of working conditions and acceptance of their own physical and psychological limitations increased the participants’ confidence regarding return to work.18
Happiness
The participants talked about the importance of being optimistic despite the pain and other symptoms,17 and their optimism was reinforced by perceived symptom improvements.19 They believed that an optimistic outlook on life would help improve their situation.17 Striving for normalcy aroused positive emotions such as hope18 and happiness.17 Additionally, emotional improvement was interpreted as getting better even when the pain and other symptoms did not necessarily decrease.16
Discussion
This meta-synthesis of patients’ experiences of WAD and the injury-recovery process resulted in 3 themes – 1) distancing from normalcy, 2) self-efficacy in controlling the life situation after the injury, and 3) readjustment and acceptance – describing the participants’ beliefs regarding pain, their WAD-related life situation and their future expectations and acceptance related to the recovery process. The content of the 3 themes, which improves our understanding of the complexity of WAD, can be summarized as follows (the numbers refer to the respective themes indicated above): (1) Patients’ perceived feelings of not being their “usual self” when pain and other symptoms interfered with activities and social contacts were strong. (1) The changed self-image was difficult to cope with and likely led to perceptions of stigmatization. (2) Struggling with feelings of a loss of control appeared to lead to low confidence and insecurity. (2) Thus, reinforcing participants’ self-efficacy in taking control over pain and daily activities emerged as important. (2) A focus on increasing knowledge and understanding the pain and its consequences was believed to lead to better strategies for handling the situation during the recovery process. Furthermore, (3) resuming life roles, including returning to work, was challenging, but being (3) optimistic reinforced symptom improvements and contributed to feelings of happiness.
Existential uncertainty and recovery expectations in recovery process
Holm et al20 and Söderlund et al21 concluded that recovery expectations are important in the prognosis of WAD. Furthermore, these studies showed an association between disability20 or engagement in activities21 and recovery expectations. Those with low expectations were more likely to report high disability20 and low engagement in activities.21 In the current synthesis, one of the emerging categories was existential uncertainty, which consisted of codes such as distress, worry, stigma, chaos, unsure about the future, and changed self-image. These cognitions and emotions are likely to contribute to recovery expectations during the recovery process. Holm et al20 stated that interventions should be targeted to recovery expectations to be beneficial. However, we might need to identify not only recovery expectations but also the components of the recovery expectations concept and then design intervention around the components that are problematic to the patient.21–23
Chronic WAD has been shown to be predicted by initial high pain intensity, coping styles, depression, fear of movement,24–29 and catastrophizing.17,27,28,30,31 Several categories indicated by our results mirrored the predictors, which could be important to the recovery process, found in previous quantitative studies.
The existential uncertainty category consisted of codes such as feelings of fear, sadness, worry, and negative moods, among others. However, the category also contained codes such as stigma, chaos and mystery, which could contribute to catastrophizing; moreover, all of these codes could contribute negatively to the recovery process. Bring et al32 studied coping patterns in patients with acute WAD. The authors concluded that on days with high physical and psychological distress, the patients reported a high degree of catastrophizing.32
Beliefs of being stigmatized, perceiving chaos in daily life, and believing that one’s situation is a mystery or a riddle that requires answers demand different methodological actions from those currently being used in the evaluation and treatment of WAD. These beliefs may not have been addressed effectively in the current management of WAD and thus may not effectively support the recovery process.
Control and self-efficacy in recovery process
The perception of struggling with control was one of the categories in the theme “self-efficacy in controlling the life situation after the injury”. This category consisted of codes related to control, controllable pain, and having control over daily demands but also self-satisfaction, self-confidence, hope, and beliefs that influence self-confidence. These results could be interpreted as indication that we must identify various areas where perceived control is an issue when evaluating the life situation of patients with WAD. We must also identify the meanings and the levels of self-satisfaction, self-confidence, and perceived feelings of hope to offer better tailored treatments for supporting the recovery process. The codes in the perceived struggling with control category also suggest that there is a strong need for coping strategies that affect perceived control over pain and activities, as demonstrated previously.33
Furthermore, the knowledge and understanding category included codes related to learning to develop strategies for control and self-management and understanding the need for realistic expectations, indicating important factors to consider in the treatment of WAD. This finding is in line with recent guidelines in which educating through advice as part of treatment has been recommended.4 However, because evidence of education as an effective treatment strategy remains equivocal, and considering the present results regarding desired topics for gaining knowledge (e.g., strategies for control), there is a need to consider what content knowledge-enhancing education should involve for these patients from an individual’s point of view.
Poor self-efficacy in activities is a strong predictor of long-term disability.26,29,34,35 Functional self-efficacy and catastrophizing had large direct effects on disability, and self-efficacy had the larger effect of these 2 variables.29 In 1 study, patients who had high self-efficacy in activities at inclusion reported lower disability at a 3-month follow-up compared with those who reported low initial self-efficacy.34 The theme “self-efficacy in controlling the life situation after the injury” supported the importance of self-efficacy and emotions and beliefs in relation to increasing or decreasing self-efficacy, as captured in previous studies. In contrast, the content of the theme “distancing from normalcy” and the related category interference and loss suggest that there are factors that can decrease one’s self-efficacy in managing the WAD-related situation. To date, there has been little or no effort to systematically evaluate and manage the beliefs and emotions in the context of WAD. The closest attempts have involved measuring and increasing self-efficacy beliefs and perceived control over pain. Much remains to be accomplished to better support the recovery process.
Life roles and acceptance in recovery process
The recapture life roles category in the theme “Readjustment and acceptance” further described possible significant factors contributing to patients’ beliefs in their capacity to handle the situation, i.e., a desire to get and stay well, resume preinjury daily functioning, have the expected physical capacity, handle commitments that make it difficult to concentrate on recovery, and the challenges in retaining a positive outlook regarding recovery.
Approximately 50% of patients with WAD have long-term symptoms after their injury,1,24 and a large proportion are reported to have poor quality of life.36 Additionally, 13–50% are unable to work or participate fully in their daily activities.37 The category recapture life roles describes the importance of resuming work, gaining independence and autonomy, and participating in valued life roles. Patients with WAD are in the middle of their lives, a period when work and participation in life are highly valued. Additionally, these results indicate that better management strategies are needed to support return to work and daily life in general.
The category happiness described existing positive beliefs and emotions, such as optimism, spontaneity, re-establish a satisfactory sense of self, positive emotions, and improvement in mood, that are important to capture in evaluation and support during management. The happiness category is likely related to the concept of acceptance and thus possibly indicates the possible importance of acceptance and commitment therapy, where psychological inflexibility is targeted, as one of the treatment strategies in WAD supporting the recovery process.38
We need new ideas for designing evaluation and management methods for the recovery process for patients with WAD.39 Our results can be a starting point for the development of more individualized methods that support recovery better than the current methods do. For example, the 3 recovery pathways suggested by Sterling et al1 could be complemented with the results of the present study and possibly applied in clinical practice at the individual level.
Strengths and limitations
The strengths of the study lie in its credibility, trustworthiness, and auditability. The credibility of data handling is important in meta-synthesis,14 meaning that the data remain true to their source. In our study, the codes are clearly recognizable in the included studies, thus implying high credibility. Trustworthiness is another important methodological issue. In our study, all the authors, who are senior researchers, independently checked each step of the analysis, implying high trustworthiness. Thus, we believe that our analysis and the results are both credible and trustworthy. Furthermore, to enhance auditability,9,14 we have transparently documented each phase of the meta-analysis, from search to synthesis. Another important methodological issue in qualitative research is transferability, i.e., whether the findings can be transferred to new settings.40 The present findings are in line with those of previous qualitative studies, e.g., those investigating the life situation of people living with another chronic condition.41
The number of included studies might be considered a limitation affecting the trustworthiness of the results. However, we conducted an intensive search of studies that was not limited in terms of publication year and found only 4 relevant papers. Several repeated searches of databases and reference lists yielded the same 4 studies, which we ultimately included. In qualitative studies, the sample size should not be so large that it aggravates the intensive analysis required. Ethically, it is also important to listen to patients’ voices without delay to facilitate improved management of WAD in the future. The participants in the included studies also repeatedly talked about similar topics, thus providing confirmation that enhances the trustworthiness of our results. We believe that our results generally mirror the beliefs of patients with WAD.
It should be noted that in the study by Williamson et al,19 only the findings for their first aim were included as their second aim lay beyond the focus of this meta-synthesis.
The quality of the studies could be a limitation. Specifically, 1 study failed the quality evaluation. However, as Sandelowski et al42 wrote: “In general, studies should not be excluded for reasons of quality, because […] there are wide variations in conceptions of the good, and in quality criteria”. Thus, we decided to include the low-quality study.
Conclusion
The results of the present study with its 3 themes (distancing from normalcy, self-efficacy in controlling the life situation after the injury, and readjustment and acceptance) and the large variation in the contents (codes) of the themes provide a more comprehensive understanding of the complexity of WAD; patients’ complex, multifaceted experiences of WAD; and the injury-recovery process. The results can guide the development of new ways to evaluate and manage WAD. These results also indicate that there is great demand for an approach based on individuals’ specific needs to determine the depth of problems and how to support the recovery process.
Disclosure
The authors report no conflicts of interest in this work.
References
Sterling M, Hendrikz J, Kenardy J. Compensation claim lodgement and health outcome developmental trajectories following whiplash injury: a prospective study. Pain. 2010;150(1):22–28. | ||
Griffin A, Leaver A, Moloney N. General exercise does not improve long-term pain and disability in individuals with whiplash-associated disorders: a systematic review. J Orthop Sports Phys Ther. 2017;47(7):472–480. | ||
Rebbeck T. The role of exercise and patient education in the noninvasive management of whiplash. J Orthop Sports Phys Ther. 2017;47(7):481–491. | ||
Bussières AE, Stewart G, Al-Zoubi F, et al. The treatment of neck pain-associated disorders and whiplash-associated disorders: a clinical practice guideline. J Manipulative Physiol Ther. 2016;39(8):523.e527–564.e527. | ||
Borrell-Carrió F, Suchman A, Epstein R. The biopsychosocial model 25 years later: principles, practice, and scientific inquiry. Ann Fam Med. 2004;2(6):576–582. | ||
Henningsen P. Still modern? Developing the biopsychosocialmodel for the 21st century. J Psychosom Res. 2015;79:362–363. | ||
Mead N, Bower P. Patient-centredness: a conceptual framework and review of the empirical literature. Soc Sci Med. 2000;51:1087–1110. | ||
Randall K, McEwen I. Writing patient-centered functional goals. Phy Ther. 2000;80(12):1197–1203. | ||
Sandelowski M, Barroso J. Handbook for Synthesizing Qualitative Research. New York: Springer Publishing Company; 2007. | ||
http://www.casp-uk.net/ [homepage on the Internet]. Critical Appraisal Skills Programme (CASP). Better Value Healthcare Ltd; 2017. Accessed 1 July, 2017. | ||
Synnott A, O’Keeffe M, Bunzli S, Dankaerts W, O’Sullivan P, O’Sullivan K. Physiotherapists may stigmatise or feel unprepared to treat people with low back pain and psychosocial factors that influence recovery: a systematic review. J Physiother. 2015;61:68–76. | ||
Kelly G, Blake C, Power C, O’Keeffe D, Fullen B. The association between chronic low back pain and sleep: a systematic review. Clin J Pain. 2011;27:169–181. | ||
Fullen B, Baxter G, O’Donovan B, Doody C, Daly L, Hurley D. Doctors’ attitudes and beliefs regarding acute low back pain management: a systematic review. Pain. 2008;136:388–396. | ||
Walsh D, Downe S. Meta-synthesis method for qualitative research: a literature review. J Adv Nurs. 2005;50(2):204–211. | ||
Malterud K. Qualitative research: standards, challenges, and guidelines. Lancet. 2001;358(9280):483–488. | ||
Walton DM, Macdermid JC, Taylor T, ICON. What does ‘recovery’ mean to people with neck pain? Results of a descriptive thematic analysis. Open Orthop J. 2013;7:420–427. | ||
Bostick GP, Brown CA, Carroll LJ, Gross DP. If they can put a man on the moon, they should be able to fix a neck injury: a mixed-method study characterizing and explaining pain beliefs about WAD. Disabil Rehabil. 2012;34(19):1617–1632. | ||
Rydstad M, Schult ML, Lofgren M. Whiplash patients’ experience of a multimodal rehabilitation programme and its usefulness one year later. Disabil Rehabil. 2010;32(22):1810–1818. | ||
Williamson E, Nichols V, Lamb SE. “If I can get over that, I can get over anything” – understanding how individuals with acute whiplash disorders form beliefs about pain and recovery: a qualitative study. Physiotherapy. 2015;101(2):178–186. | ||
Holm LW, Carroll LJ, Cassidy JD, Skillgate E, Ahlbom A. Expectations for recovery important in the prognosis of whiplash injuries. PLoS Med. 2008;5(5):e105. | ||
Söderlund A, Löfgren M, Stålnacke BM. Predictors before and after multimodal rehabilitation for pain acceptance and engagement in activities at a 1-year follow-up for patients with whiplash-associated disorders (WAD) – a study based on the Swedish Quality Registry for Pain Rehabilitation (SQRP). Spine J. Epub 2017 Nov 16. | ||
Beaton D, Tarasuk V, Katz J, Wright J, Bombardier C. “Are you better?” A qualitative study of the meaning of recovery. Arthritis Rheumatol. 2001;45:270–279. | ||
Ottosson C, Pettersson H, Johansson S, Nyren O, Ponzer S. Association between self-perceived recovery and the SF-36 after minor musculoskeletal injuries. Qual Life Res. 2007;16:217–226. | ||
Carroll L, Holm L, Hogg-Johnson S, et al. Course and prognostic factors for neck pain in whiplash-associated disorders (WAD): results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. J Manipulative Physiol Ther. 2009;32(Suppl 2):S97–S107. | ||
Carroll LJ, Ferrari R, Cassidy D, Cote P. Coping and recovery in whiplash-associated disorders: early use of passive coping strategies is associated with slower recovery of neck pain and pain-related disability. Clin J Pain. 2014;30(1):1–8. | ||
Sandborgh M, Johansson A-C, Söderlund A. The relation between the Fear-Avoidance Model and constructs from the Social Cognitive Theory in acute WAD. Pain Res Manag. 2016;2016:8281926. | ||
Söderlund A, Lindberg P. Coping as a mediating factor between self-efficacy and disability in Whiplash Associated Disorders (WAD). J Whiplash Relat Disord. 2002;1(2):25–37. | ||
Söderlund A, Lindberg P. Whiplash Associated Disorders – predicting disability from a process-oriented perspective on coping. Clin Rehabil. 2003;17(1):101–107. | ||
Söderlund A, Sandborgh M, Johansson A-C. Is the self-efficacy and catastrophizing in pain related disability mediated by control over pain and ability to decrease pain in whiplash-associated disorders? Physiother Theory Pract. 2017;33(5):376–385. | ||
Adams H, Ellis T, Stanish W, Sullivan M. Psychosocial factors related to return to work following rehabilitation of whiplash injuries. J Occup Rehabil. 2007;17:305–315. | ||
Casey PP, Feyer AM, Cameron ID. Course of recovery for whiplash associated disorders in a compensation setting. Injury. 2015;46(11):2118–2129. | ||
Bring A, Bring J, Söderlund A, Wasteson E, Asenlöf P. Coping patterns and their relation to daily activity, worries, depressed mood, and pain intensity in acute whiplash-associated disorders. Int J Behav Med. 2013;20(2):293–303. | ||
Angst F, Gantenbein A, Lehmann S, et al. Multidimensional associative factors for improvement in pain, function, and working capacity after rehabilitation of whiplash associated disorder: a prognostic, prospective outcome study. BMC Musculoskelet Disord. 2014;15:130. | ||
Söderlund A, Lindberg P. Cognitive behavioural components in physiotherapy management of chronic Whiplash Associated Disorders (WAD) – a randomised group study. Physiother Theory Pract. 2001;17:229–238. | ||
Söderlund A, Åsenlöf P. The mediating role of self-efficacy expectations and fear of movement and (re)injury beliefs in two samples of acute pain. Disabil Rehabil. 2010;32(25):2118–2126. | ||
Tournier C, Hours M, Charnay P, Chossegros L, Tardy H. Five years after the accident, whiplash casualties still have poorer quality of life in the physical domain than other mildly injured casualties: analysis of the ESPARR cohort. BMC Public Health. 2016;16:13. | ||
Scholten-Peeters G, Verhagen A, Bekkering G, et al. Prognostic factors of whiplash-associated disorders: a systematic review of prospective cohort studies. Pain. 2003;104:303–322. | ||
Wicksell RK, Olsson GL, Hayes SC. Psychological flexibility as a mediator of improvement in Acceptance and Commitment Therapy for patients with chronic pain following whiplash. Eur J Pain. 2010;14(10):1059.e1–1059.e11. | ||
Jull G, Söderlund A, Stemper B, et al. Toward optimal early management after whiplahs injury to lessen the rate of transition to chronicity. Spine (Phil Pa 1976). 2011;36(25 Suppl):S335–S342. | ||
Finfgeld-Connett D. Generalizability and transferability of meta-synthesis research findings. J Adv Nurs. 2010;66(2):246–254. | ||
Nordgren L, Asp M, Fagerberg I. Living with moderate-severe chronic heart failure as a middle-aged person. Qual Health Res. 2007;17(1):4–13. | ||
Sandelowski M, Docherty S, Emden C. Qualitative metasynthesis: issues and techniques. Res Nurs Health. 1997;20(4):365–371. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.