Back to Journals » Patient Preference and Adherence » Volume 19
Exploring Patient Satisfaction and Determinants in VIP Outpatient: A SERVQUAL-Based Latent Class Analysis
Authors Wang H, Wang H, Guan S, Li J
Received 31 August 2025
Accepted for publication 18 November 2025
Published 28 November 2025 Volume 2025:19 Pages 3819—3834
DOI https://doi.org/10.2147/PPA.S564293
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ramón Morillo-Verdugo
Huilin Wang,1,2 Hao Wang,1 Sinan Guan,2 Jing Li1
1Outpatient Department of Peking University First Hospital, Beijing, People’s Republic of China; 2School of Nursing, Peking University, Beijing, People’s Republic of China
Correspondence: Jing Li, Outpatient Department of Peking University First Hospital, Xishiku Road, Xicheng District, Beijing, 100034, People’s Republic of China, Tel/Fax +86 010-83572020, Email [email protected]
Objective: To address the diverse needs of patients at different levels, VIP (Very Important Person) outpatient services function as a personalized approach and are of significant importance in the healthcare system. Additionally, patient satisfaction serves as a critical tool for understanding and improving the quality of healthcare services. Therefore, this study aimed to classify VIP outpatients based on satisfaction levels and identified its determinants, hypothesizing that distinct satisfaction segmentations exist and are influenced by several factors.
Methods: A total of 4068 patients who attended the VIP outpatient at a tertiary hospital were enrolled between June and July 2025. The SERVQUAL model was used in this study. Descriptive statistical analyses were conducted and quantitative data were gathered using a 5-point Likert scale tailored to assess patient satisfaction. Latent Class Analysis (LCA) was used to delineate heterogeneous satisfaction groups, while a chi-square test and binary logistic regression were employed to investigate satisfaction levels and potential influencing factors.
Results: Two latent classes were identified using Mplus 8.4: the overall high satisfaction group (73.1%) and the high medical care–low support service group (26.9%). All hypotheses are supported. A total of 49.7% waited less than 30 min before consultation, and 76.4% communicated with the doctor for more than 20 min. Binary logistic regression analysis revealed that the patient source, waiting time before consultation, and length of communication with the doctor were associated factors (all p < 0.05).
Conclusion: For non-local patients registered as outpatients with VIP, priority should be given to addressing their core clinical needs and strengthening doctor–patient interactions. Furthermore, measures such as implementing a cap on registrations and assigning doctor assistants can be introduced to reduce waiting times and extend the length of communication.
Keywords: patient satisfaction, VIP outpatient, SERVQUAL model, latent class analysis
Introduction
As frontline interfaces for healthcare delivery, outpatient systems play a critical role in providing medical services.1 It is estimated that outpatient departments in China handled approximately 9.55 billion patient visits by 2023, reflecting a year-on-year increase of 13.5%.2 Departments such as general clinics, specialty clinics, emergency services, and VIP outpatients are integral components that significantly contribute to outpatient systems.3,4 Within the diversified departments, the VIP outpatients are distinct from the general clinics, which are designed to meet the universal and fundamental medical demands of the general population.5 As a high-end service, it effectively caters to the varying expectations and extends beyond mere convenience—such as assistance with examination scheduling and prioritized access via dedicated channels—to encompass a heightened focus on individualized needs and the efficient and meticulous management of personal health through a higher fee.6,7 This service model is embedded within a macro-policy environment that actively fosters its development. In 2022, the State Council advocated partnerships between social institutions and hospitals to enhance VIP outpatient care, a measure aimed at promoting the growth of this sector and optimizing patient experience.8 To better understand patient experience and advance the growth of VIP outpatient, as a vital indicator for assessing the quality of outpatient care, patient satisfaction accurately reflects patients’ perceptions of service effectiveness and hospital management.9,10 In recent years, studies on satisfaction have increasingly incorporated with important theories that capture multifaceted aspects of patient experience to analyze influencing factors in depth.11,12 The SERVQUAL model represents the foundational theoretical approach.
According to the SERVQUAL model proposed by Parasuraman, service quality is conceptualized through five core dimensions: “tangibles”, “reliability”, “responsiveness”, “assurance”, and “empathy”, which together reflect the interactive customer experience (ICX).13 “Tangibles” refer to the appearance of physical facilities, equipment, and personnel; “reliability” is mainly the ability to fulfill service obligations and promises; “responsiveness” encompasses the willingness to help customers and provide prompt service; “assurance” refers to the courtesy of employees and their ability to inspire trust and confidence; “empathy” represents the provision of caring, individualized attention to customers.13 Analyzing the discrepancy between the target population’s perceived and expected quality through the lens of these five components provides a valuable framework for investigating their behaviors and attitudes, making the SERVQUAL model extensively applied across diverse research contexts.14 Zhao et al15 revealed that “tangibles”, such as technological, organizational, and environmental factors, are critical elements that impact customers’ intention to errand delivery (INED) in business negotiations, thus highlighting their importance in attracting enterprise users. Similarly, Wisutwattanasak et al16 found that health considerations, safety (“tangibles”), and staff service attitude (“empathy”) were key factors in passengers’ choice of rail travel in the post-pandemic era, underscoring their relevance to service quality improvement and passenger satisfaction. Furthermore, the application of the SERVQUAL model is well established in healthcare settings for evaluating patient satisfaction and perceptions of medical services.12 For example, patients with longer hospital stays reported lower satisfaction in both “tangibles” and “reliability” compared to those discharged within two days.12 Another study demonstrated that, using a 25-item satisfaction questionnaire adapted from SERVQUAL, health insurance enrollees exhibited high levels of satisfaction with the “assurance” and “reliability” of care quality.17
Existing research has identified a range of factors influencing patient satisfaction, which can be broadly categorized into clinical and non-clinical support services.18–20 Clinical services primarily refer to the provision of diagnostically valuable activities and their processes within the healthcare system; diagnosis, treatment, attitude, and interaction of medical staff and patients along the clinical pathway are key elements included in this category.21,22 In SERVQUAL model, Kashfi et al23 found that clinical service such as doctors’ behavior, diagnosis, explanation, arrangements, and attitude of medical staff are critical contributors to the dimension of “reliability” and “empathy”. A study conducted in Africa reported similar findings.24 According to the Australian Government Productivity Commission, non-clinical support services mainly refer to a service delivery model focused on the environmental, social, and activity-based determinants of health.25 A favorable environment, infrastructure, and support from auxiliary staff are encompassed within this category, and increasing evidence for the efficacy of non-clinical interventions underlies the World Health Organization’s recent advocacy for such practices in low- and middle-income countries.22,26 Farrokhi et al20 found that non-clinical services, such as the outpatient environment, sanitation, and timely responses from staff, serve as critical explanations for the “tangibles” and “responsiveness” dimensions in the SERVQUAL model. This finding is consistent with earlier observations from a study conducted in Iranian teaching hospitals as well.23 Nevertheless, variations in patient perceptions and behaviors can lead to divergent satisfaction patterns across these categories.27,28 For instance, some patients may report high overall satisfaction, whereas others might express satisfaction with clinical services but identified shortcomings in non-clinical support, and vice versa. Consequently, based on the theory of the SERVQUAL model, it is essential to conduct an in-depth analysis of patient satisfaction across different subgroups to identify contributing factors.
Currently, research on healthcare satisfaction primarily focuses on general outpatients and inpatients, with few studies specifically targeting VIP outpatient.29,30 Additionally, most studies have depended on traditional statistical approaches, such as correlation and regression analyses, implicitly assuming patients as a homogeneous population and culminating in a lack of investigation on the diversity among patients within VIP outpatient settings, particularly advanced analytical techniques, such as LCA, to discern latent subgroups based on satisfaction patterns. Furthermore, the existing studies often lack robust theoretical underpinnings. LCA can effectively elucidate the characteristics and heterogeneity of a target population by delineating distinct latent subgroups. Consequently, to better address multilevel needs, this study investigated patient satisfaction based on the SERVQUA in outpatients with VIP. It aims to: (1) formulate and test hypotheses based on the model. (2) employ LCA to identify latent classes among non-local VIP outpatients based on their satisfaction patterns. (3) determine the key factors differentiating these groups to provide a precise basis for policymaking and targeted quality improvements, thereby enhancing the satisfaction with medical services in VIP outpatients.
Based on the extant literature, we anticipate heterogeneity in patient satisfaction profiles, which can be theorized through the SERVQUAL framework. While some patient subgroups may report uniformly high satisfaction across all dimensions, others are likely to exhibit distinct patterns.13,18 One subgroup may prioritize core clinical services (eg, diagnostic accuracy, doctor-patient communication), leading to high ratings in “reliability” and “empathy” but comparatively lower scores in other areas.22,24 Conversely, another subgroup’s satisfaction may be predominantly influenced by non-clinical support services, where deficiencies in “tangibles” and “responsiveness” frequently lead to notably low overall satisfaction.21,23 Consequently, the following hypotheses are proposed:
H1: There is at least one class that exhibits high levels of satisfaction across the five dimensions. H2: There is at least one class whose satisfaction on the “reliability” and “empathy” dimensions are significantly higher than those on the other dimensions. H3: There is at least one class whose satisfaction on the “tangibles” and “responsiveness” dimensions are significantly lower than those on the other dimensions.
Method
Data and Sample
A cross-sectional study was conducted using the Wenjuanxing platform (a service offering functionality similar to Amazon Mechanical Turk) to recruit participants through simple random sampling. This study was conducted between June and July 2025 in the VIP outpatient department of a tertiary hospital to evaluate patient satisfaction. From the 4215 distributed questionnaires, we successfully collected 4068, yielding a high response rate of 96.51%. According to the inclusion criteria, each patient (1) provided written informed consent and agreed to participate in the study, (2) was treated in the VIP outpatient, and (3) was in a medically stable condition. Patients who (1) had infectious diseases and/or (2) were emergencycases were excluded.
It should be noted that while the single-center nature of this study and its focused two-month data collection period were beneficial for sample homogeneity, they might inherently limit the assessment of seasonal effects and broader institutional applicability.
Measures
Building on prior research,31,32 the items were refined by incorporating expert feedback and aligning them with existing questionnaires in the field. The questionnaire comprised 30 items organized into three dimensions: demographic characteristics, core healthcare process, and satisfaction assessment of the medical experience (Figure S1). Reverse scoring was applied to only one item (“waiting time before consultation”) to standardize the direction of data interpretation and enhance the consistency of analytical outcomes.
The demographic measures included sex, age, patient source, and educational status. Gender was coded as a binary variable: 1 = female, 0 = male; age (units: years) was a continuous variable in years, and we categorized it into three groups: 0–44 = 0; 45–59 = 1, ≥60 = 2; patient source had two categories: local patients = 0; non-local patients = 1; educational attainment was measured as an ordinal variable with three levels: 0 = high school and below, 1 = undergraduate/junior college, and 2 = postgraduate and above.
The core healthcare process dimension encompasses two main aspects: service flow and the examination of the auxiliary department. Service flow includes payment methods, waiting times, and face-to-face communications. Payment method refers to the settlement method of patients’ medical expenses: 0 = no medical insurance and 1 = medical insurance. Waiting time was an indicator of medical efficiency (units: minutes): >60 = 0; 31–60 = 1; ≤30 = 2. The length of communication was a continuous variable (units: minutes), and we preprocessed this variable as ≤20 = 0 and >20 = 1. For the examination of the auxiliary department, respondents indicated whether they had made payments or purchased medication in the outpatient pharmacy or underwent examinations in the clinical laboratory, medical imaging department, ultrasound department, nuclear medicine department, or endoscopy center (no = 0, yes = 1).
The satisfaction assessment system for medical experience comprises 16 items across three dimensions. (1) Doctor–patient interaction: (i) overall satisfaction with waiting time, (ii) satisfaction with behavior of treating doctor, (iii) doctor explained your treatment and respected privacy, (iv) doctor gave some guidance and materials, (v) doctor diagnosed diseases, (vi) doctor explained why and how to use medicine, (vii) doctor advised the examination and treatment plan, and (viii) doctor informed follow-up arrangements. (2) Nursing care: (i) satisfaction with nurses’ behavior, (ii) nurses listening to their questions and problems, and (iii) nurses answering the questions correctly. (3) Environmental service: (i) satisfaction with hospital services and staff, (ii) satisfaction with responsiveness to your needs, (iii) satisfaction with outpatient environment, (iv) satisfaction with outpatient guideposts, and (v) satisfaction with hygiene of the toilet. The satisfaction items were rated on a 5-point Likert scale ranging from 1 (“very dissatisfied”) to 5 (“very satisfied”), with higher scores denoting greater levels of satisfaction.
The questionnaire demonstrated high internal consistency and strong interrelationship among the items, as evidenced by a Cronbach’s alpha coefficient of 0.969, a KMO value of 0.963, and a significant Bartlett’s test of sphericity (χ2 = 6717.92, p < 0.001).
Statistical Analysis
This study initiated a descriptive analysis of the characteristics of the 4068 participants. Subsequently, LCA was performed using Mplus 8.4 to identify distinct satisfaction patterns in VIP outpatients. LCA is a probability model-based statistical approach applied across various fields, such as psychology, sociology, and medical research, which classifies individuals and identifies population heterogeneity primarily according to their distinct response patterns to categorical observed variables.33 Model selection relied on several goodness-of-fit indices: (1) Akaike Information Criterion (AIC), (2) Bayesian Information Criterion (BIC), (3) adjusted Bayesian Information Criterion (aBIC), (4) entropy, (5) Lo-Mendell-Rubin likelihood ratio test (LMR), and (6) bootstrap likelihood ratio test (BLRT).34 It was guided by a combination of the following criteria: (i) statistical fit: a lower BIC value relative to models with fewer classes, accompanied by significant LMRT and BLRT p-values. (ii) classification precision: high entropy values (approaching 1). Entropy ranges from 0 to 1, with values >0.8 indicating >90% classification accuracy. (iii) parsimony and interpretability: the most parsimonious model was ultimately selected, contingent upon all latent classes being substantively meaningful and ensuring result stability. Finally, chi-square tests (SPSS 27.0) were used to assess the associations between variables and class membership. Furthermore, binary logistic regression analysis was conducted to verify the determinants of satisfaction in VIP outpatients. A statistical significance threshold of p < 0.05, was applied for all tests. There were no missing data for any of the variables included in the analysis.
Quality Control
In this study, a team of five researchers collected the data, and all members were required to undergo standardized training prior to administering the survey. Additionally, multiple statistical indices (AIC, BIC, and aBIC) were used to comprehensively evaluate the model-data fit and determine the optimal number of latent classes. Prior to the questionnaire, participants were informed of the purpose of the study and provided informed consent prior to the formal items. They were assured that their data would remain confidential, and that their privacy would be protected. Additionally, to bolster analytical precision and limit information loss, the length of communication was dichotomized at the empirically supported 20-minute threshold, with shorter durations being known in the literature to correlate with informational inadequacy and lower satisfaction.35
Results
Demographic Characteristics of 4605 Patients in VIP Outpatient
A total of 4068 patients were included in this study (Table 1). Of the participants, 59.6% were female. Approximately half of the participants were aged 0–44 (52.6%), local patients (51.8%), covered by health insurance (50.2%), and had undergraduate or junior college education (56.3%). A total of 49.7% reported waiting no more than 30 min before consultation, and 61.8% were very satisfied with waiting time. Most participants (76.4%) communicated with a doctor for < 20 min.
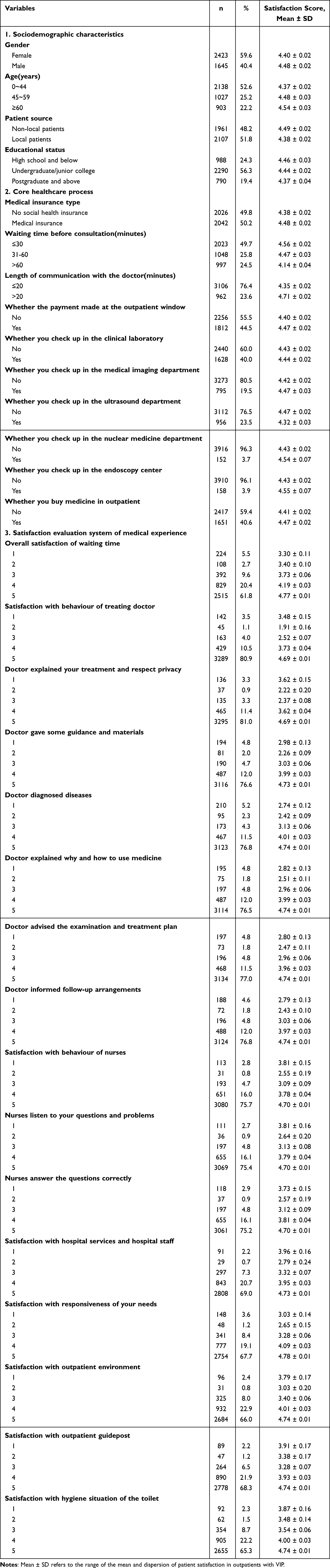 |
Table 1 Descriptive Characteristics and Patient Satisfaction Scores of the Participants (n = 4068) |
Latent Class Analysis of Patient Satisfaction in VIP Outpatient
LCA was used to examine the patterns of VIP outpatient services, commencing with a single-class model and progressively incorporating additional latent classes, ultimately testing five competing models. The results indicated that the two-class solution demonstrated balanced class probabilities and relatively lower BIC value compared to other models, with an entropy value of 0.988, suggesting high classification precision and a superior overall model fit. In contrast, models with more than two classes yielded a non-significant LMRT (p > 0.05) and decreased BIC. Consequently, the two-class model was identified as the optimal solution, with two latent classes comprising 73.1% and 26.9% of the sample (Table 2).
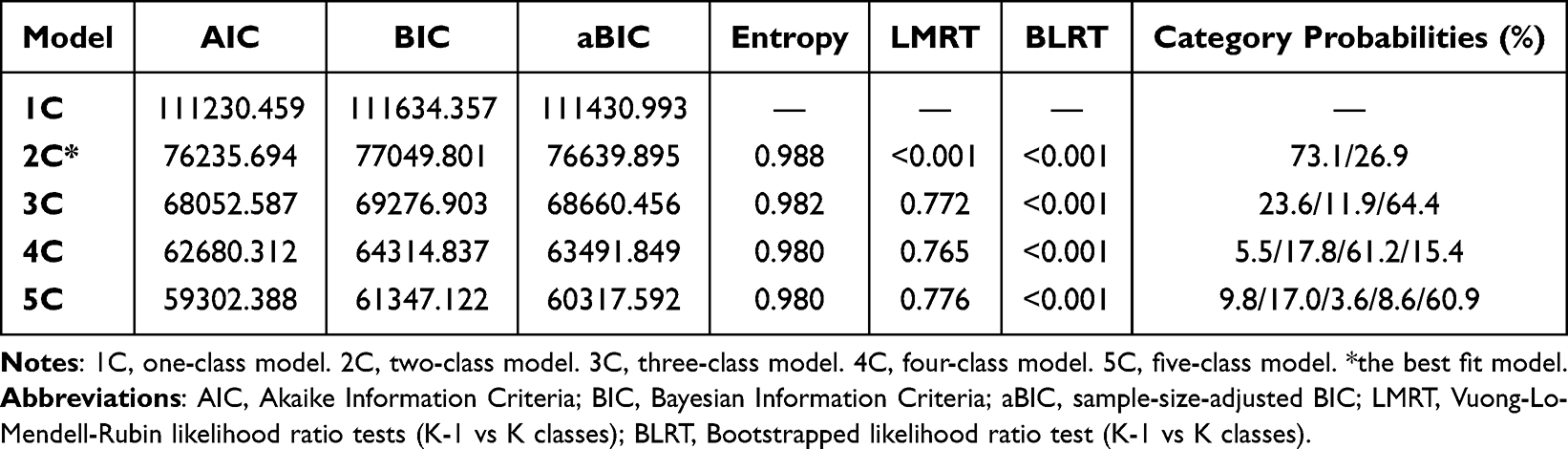 |
Table 2 Fitting Indices of the Latent Class Analysis for Patient Satisfaction in VIP Outpatient |
Identification of Latent Classifications and Verification of Hypotheses
The analysis presented in Figure 1 demonstrated that VIP outpatient satisfaction clusters into two discrete patterns. There were 2975 patients in the first category (top line in Figure 1), accounting for 73.1% of the total. Respondents in this group exhibited the highest scores across all items, indicating a high level of overall satisfaction. Consequently, this category was designated as the “Overall high satisfaction group” (Class 1). Additionally, this pattern of comprehensive satisfaction confirms our initial expectation (Hypothesis 1). The second category, represented by the bottom row in the figure comprised 1093 patients, constituting 26.9% of the sample. The satisfaction level of this group was generally high in terms of the dimension of doctor–patient interaction (Item 2–8) and nursing care (Item 9–11) on a 5-point Likert scale, while the conditional probability of non-clinical support services such as the outpatient environment (Item 13), response of needs (Item 14), outpatient guidepost (Item 15), and hygiene situation of the toilet (Item 16) were at a lower rate. Therefore, this category was named the “High medical care - Low support service group” (Class 1), a finding directly in line with the expectations outlined in Hypothesis 2 and Hypothesis 3.
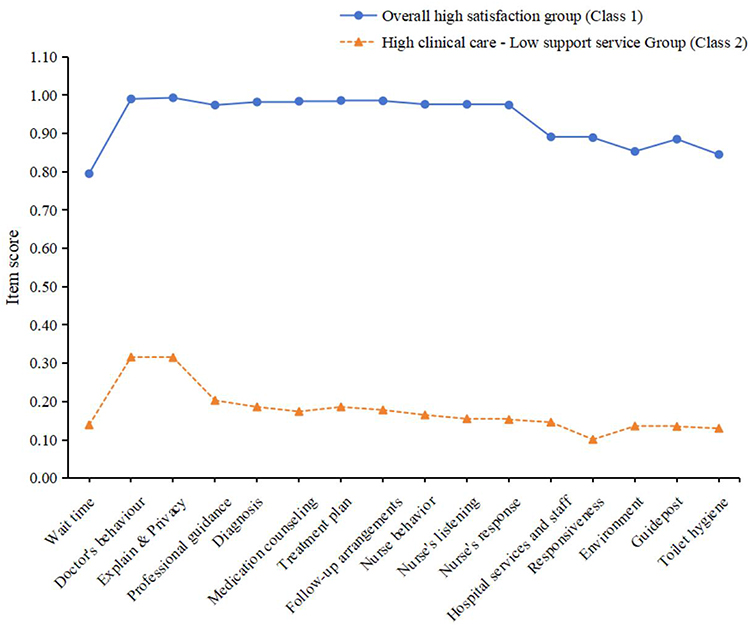 |
Figure 1 Latent Classes of Patient Satisfaction in the VIP Outpatient. Notes: Item labels in the figure correspond to the following full descriptions. Wait time = Item1, Overall satisfaction of waiting time; Doctor’s behaviour = Item2, Satisfaction with behaviour of treating doctor; Explain & Privacy = Item3, Doctor explained your treatment and respect privacy; Professional guidance = Item4, Doctor gave some guidance and materials; Diagnosis = Item5, Doctor diagnosed diseases; Medication counseling = Item6, Doctor explained why and how to use medicine; Treatment plan = Item7, Doctor advised the examination and treatment plan; Follow-up arrangements = Item8, Doctor informed follow-up arrangements; Nurse behavior = Item9, Satisfaction with behaviour of nurses; Nurse’s listening = Item10, Nurses listen to your questions and problems; Nurse’s response = Item11, Nurses answer the questions correctly; Hospital services and staff = Item12, Satisfaction with hospital services and hospital staff; Responsiveness = Item13, Satisfaction with responsiveness of your needs; Environment = Item14, Satisfaction with outpatient environment; Guidepost = Item15, Satisfaction with outpatient guidepost; Toilet hygiene = Item16, Satisfaction with hygiene situation of the toilet. |
Chi-Square Analysis of Patient Satisfaction Between Latent Classes in VIP Outpatient
Table 3 shows that there were statistically significant differences (p < 0.01) among the educational status, patient source, waiting time before consultation, length of communication with the doctor. For gender, age, medical insurance type, whether the payment made at the outpatient window, whether you check up in the clinical laboratory, whether you check up in the medical imaging department, whether you check up in the ultrasound department, whether you check up in the nuclear medicine department, whether you check up in the endoscopy center, and whether you buy medicine in outpatient demonstrating non-significant results (p > 0.05) were excluded in our study.
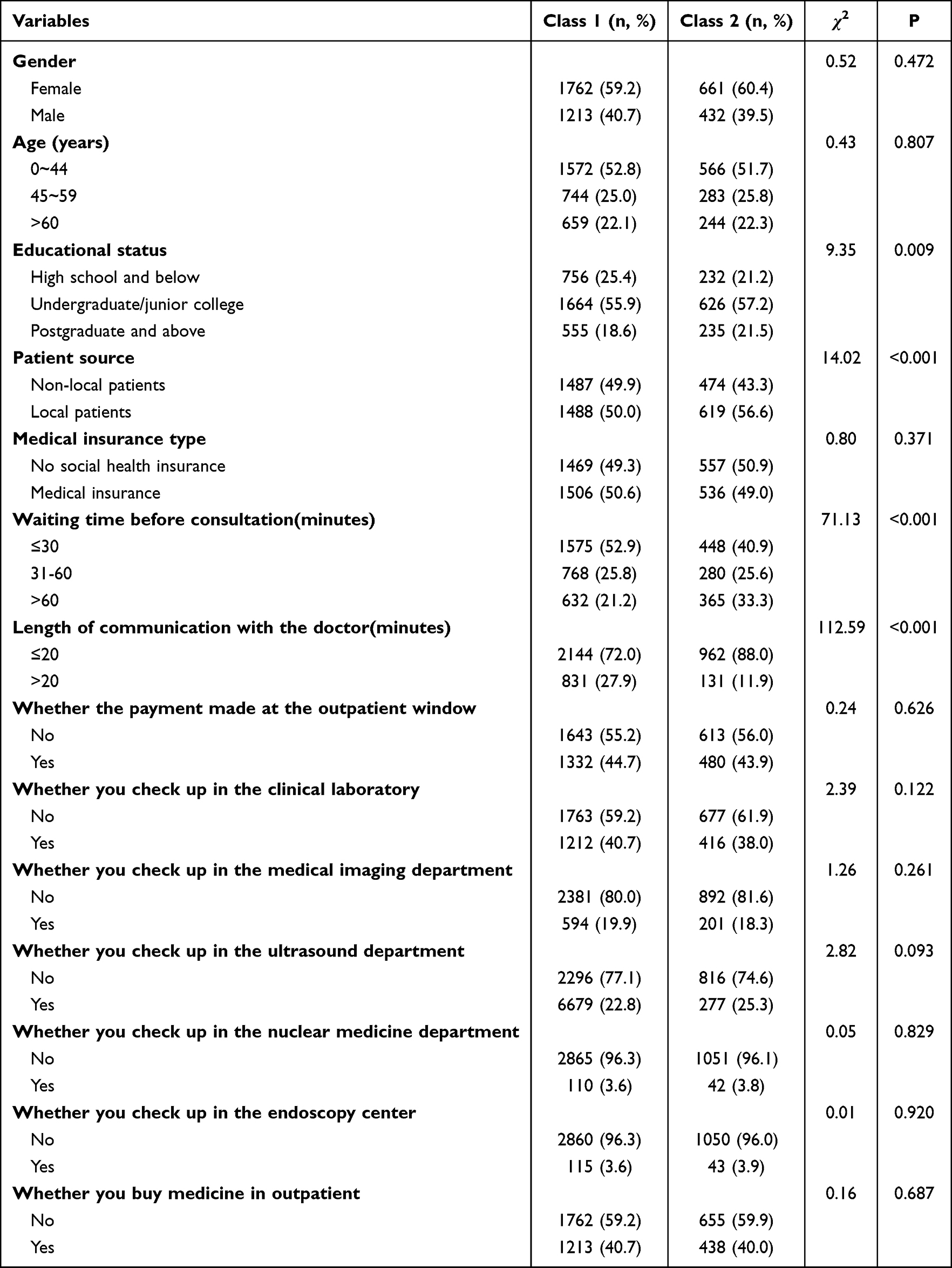 |
Table 3 Association Between Latent Classes and Key Variables in a VIP Outpatient Cohort (n = 4068): A Chi-Square Analysis |
Binary Logistic Regression of Patient Satisfaction in VIP Outpatient
Employing the two distinct patient satisfaction subtypes identified within the VIP outpatient cohort as the dependent variables, all covariates demonstrating statistically significant differences in the chi-square analyses (p < 0.05) were entered as independent variables in a binary logistic regression model. The assignment of the independent variables is presented in Table 4.
 |
Table 4 Variable Assignment |
Considering Class 1 as the reference, Table 5 shows that compared with overall high satisfaction, non-local patients (OR = 0.79, 95% CI: 0.67–0.92), and waiting less than 60 minutes before consultation (OR = 0.43, 95% CI: 0.36–0.51, ≤30; OR = 0.61, 95% CI: 0.50–0.74, 31–60) increased the probability of presenting high satisfaction with clinical care, whereas communicating with the doctor for no more than 20 minutes (OR = 2.94, 95% CI: 2.40–3.61) reduced the likelihood of reporting high satisfaction with clinical care.
 |
Table 5 Associated Factors of Patient Satisfaction in VIP Outpatient: A Binary Logistic Regression Analysis (Class2 vs Class1; n = 4068) |
Sensitivity Analyses
A series of sensitivity analyses were conducted to assess the robustness of the results (detailed in Supplementary Material 1; Tables A1, A2, B1, B2, C; Figure A). First, we evaluated alternative coding schemes for the “Length of communication with the doctor” by changing the cut-point from 20 minutes to 15 and 30 minutes. The results from both the chi-square tests and the binary logistic regression models under these alternative definitions were consistent with the primary analysis and maintained statistical significance. Additionally, a latent class analysis on a 5% reduced sample (≈203 individuals) confirmed the stability of the two-class solution, with nearly identical class profiles and supporting fit indices.
Discussion
For the landscape, unlike general clinics that address fundamental public needs, VIP outpatient care operates as a premium model, meeting diverse patient expectations by integrating operational conveniences with tailored health stewardship.6 This comprehensive, individualized approach is facilitated through a premium fee structure, underscoring a value-based exchange.7 Based on the SERVQUAL model, this study evaluated patient satisfaction among the VIP outpatient at a university hospital. Drawing on first-hand data obtained from Beijing, we identified two distinct latent classes: overall high satisfaction satisfied with every dimension and high clinical care-low support service that valued clinical engagement and nursing practice, but lower non-clinical support. Although 73.1% of patients fell into the high-satisfaction group, a noteworthy category was identified that uncovered notable differences in clinical care and support services among the classes with respect to patient source, waiting time before consultation, and length of communication with the doctor. To conduct an in-depth investigation within this context, this study uncovered distinct categories of patients attending the VIP outpatient and provided a basis for tailored interventions to support decision making.
An interesting finding of this study is that non-local patients reported higher satisfaction with clinical services than those in the overall high satisfaction group. While prior studies may noted this phenomenon, few have explored its causes across patient subgroups.36,37 One plausible explanation is that effective clinical intervention is the primary motivator for non-local patients, which is consistent with earlier interview-based research on patient satisfaction.38 Despite higher baseline costs (eg, transportation, accommodation, and meals), non-local patients willingly incur significant additional expenses for VIP care, implying that local resources may be inadequate for their needs.39,40 Consequently, the primary goal and urgent need of these patients is to obtain high-quality diagnosis, treatment, and doctor-patient communication from the best available doctors, while assigning less importance to support services like guideposts, sanitation, and outpatient environments. Higher satisfaction was observed among these patients when their clinical expectations were met.41 Another key factor is that unfamiliarity with the local healthcare system, combined with illness-related stress and financial burden, often predisposes non-local patients to anxiety and depression, as supported by a Swiss study on medical travelers.42 Therefore, they exhibit a stronger psychological need for doctor–patient interaction regarding their treatment, which serves to reassure them that their efforts and expenses are justified and effective. The specific behaviors and psychological tendencies pose a distinct systemic challenge. This demands that medical providers not only deliver excellent clinical care but also address psychological needs through empathetic, person-centered approaches. It calls for a strategic shift from a standardized model to an insight-driven, adaptive system, characterized by precise resource allocation and sustained by a framework for continuous learning and agile response. Consequently, hospital managers should develop targeted strategies to identify and cater to diverse patient groups. Investing in effective personnel selection and regular training to elevate both technical and interaction skills among medical providers is essential to meet the clinical needs of non-local patients in VIP outpatients. This training equips healthcare providers to employ professional skills such as active listening and emotional validation in clinical consultations, by replacing superficial platitudes like “Don’t worry” with a genuine understanding of concerns, thereby alleviating psychological distress of patients.43
Furthermore, waiting time before consultation emerged as a significant factor in the high clinical care and low support service group. A recommendation from the UK indicated that the optimal waiting time should not exceed 30 minutes.44 In accordance with this suggestion, our study found that non-local patients with shorter waiting times reported higher levels of satisfaction with clinical care, and a protective effect on satisfaction was observed when waits remained under 30 minutes, whereas this association substantially weakened beyond that threshold. Given time constraints and long-distance travel, non-local patients prioritize shorter wait times and empathetic interactions with their doctors, which is consistent with the conclusions drawn by Leive.45 Within the SERVQUAL framework, the dimensions of “reliability” and “responsiveness” emphasize the importance of providers seeing patients at the scheduled time and responding promptly to inquiries, thereby building trust and enhancing service quality and satisfaction. However, the ultimate evaluation depends on the discrepancy between the perceived service performance and prior expectations.46 Owing to the higher financial investment associated with VIP outpatient services, patients often arrive at elevated expectations for their clinical encounter.47 When these expectations are not met, prolonged waiting times may foster a sense of futility regarding the decision to seek care from that provider.48 The paradigm of extended waiting times exemplifies a passive healthcare model that is misaligned with modern demands for augmented services and a positive patient experience, thereby exacerbating supply–demand imbalances. Fundamentally, the solution lies in a proactive shift, leveraging advanced planning and scheduling to streamline operations, enhance efficiency, and advance the premium healthcare service model, which is not just as a logistical target, but as a core tenet of VIP service delivery. Specifically, controlling waiting times can be achieved through operational strategies such as implementing appointment caps, utilizing time-slot scheduling, and redesigning the workflow. A previous study in southwestern Saudi Arabia demonstrated that the introduction of the new Web-Based Medical Appointment System “Mawid” effectively reduced overcrowding and decreased patient waiting times.49 The implementation of this approach has significantly improved medical efficiency and fostered a relatively controlled, low-stress clinical atmosphere that not only alleviates psychological strain on medical providers but also directly elevates patient care quality.
Finally, the length of communication with the doctor was the most influential predictor across different latent classes in VIP outpatient settings. A consultation time greater than 20 minutes can foster a stronger sense of patient endorsement of clinical services, which is consistent with previous studies conducted in Japan that emphasize the decisive effect of doctor-patient communication.50 Research demonstrates that the primary requirement for patients is sufficient time to articulate their treatment perceptions, needs, and expectations to medical staff.37 However, the year-on-year increase in outpatient visits creates high patient volumes that constrain available length of communication, which is corroborated by studies reporting that the average doctor–patient interaction has dwindled to approximately 10 minutes.35 Within the SERVQUAL framework, shorter consultations (<20 min) were linked to the most significant gaps in “empathy” and “responsiveness”, stemming from reported failures in active listening and addressing patient concerns, which fostered care-related skepticism. A study from Pakistan further supports that communication lasting less than 15 minutes often results in superficial interaction and fails to establish a constructive therapeutic relationship.51 Inadequate doctor-patient communication time, which prevents patients from fully expressing their needs, compromises not only satisfaction but also objective healthcare value, leading to risks of misdiagnosis, repeated visits, and poor adherence. Therefore, investing in thorough doctor-patient communication is essential for diagnostic accuracy and patient experience, transcending the fulfillment of service metrics to become a foundational component and an uncompromisable cornerstone of high-quality care. More precisely, this can be achieved by providing doctors with administrative support teams to handle non-clinical tasks, ensuring its provision is a strategic imperative that demands the optimal allocation of high-value clinical human capital, thereby freeing up more time for meaningful doctor-patient communication. Additionally, physicians should adapt communication styles according to patients’ cultural and educational backgrounds to enhance mutual understanding and communication effectiveness. Similarly, the “teach-back” method, listed among the 34 most effective patient education strategies by the US Agency for Healthcare Research and Quality (AHRQ), which leverages patient feedback to accurately assess comprehension and communicative effectiveness, permitting immediate correction and significantly improving communication efficiency, should be adopted.52
This study underscores the methodological value of LCA in patient satisfaction research. By shifting the focus from the average variable relationships captured by traditional statistical models to a person-centered approach, LCA successfully delineated two actionable patient subgroups with distinct satisfaction profiles. This approach moves beyond merely confirming drivers like waiting time and communication to providing hospital administrators with a strategic roadmap for replacing broad initiatives with precisely targeted interventions. Whilst this two-month cross-sectional study in a VIP outpatient offers valuable management insights, its specific context necessitates further validation. It is critical that future research, potentially through multi-center studies, assesses the generalizability of these results across other clinical environments (eg, different wards, general clinics) and even hospitals of varying levels and regions. Moreover, employing longitudinal designs is essential to establish causal relationships between the influencing factors and satisfaction across different subgroups. Such research is fundamental for developing evidence-based improvement strategies among different subgroups in the future.
Limitation
The limitations of this study primarily involve four points. First, the cross-sectional design of this study constrains our capacity to establish causal relationships, allowing only the identification of associations among multiple variables. Subsequent studies should implement longitudinal approaches and latent transition modeling to monitor changes in patient satisfaction over time. Second, this study was confined to a limited set of covariates. Future studies should incorporate additional determinants, such as psychological factors in patients, including perceptions of shared decision making in treatment plans, and explore their underlying mechanisms more thoroughly. Third, because the sample was exclusively drawn from Beijing with a time span of only two months, the findings may not be generalizable to other geographical areas and account for potential seasonal variations in patient flow. Therefore, to improve the robustness of the conclusions, further research should extend the coverage of the survey to the national level and the observation period to expand our findings. Finally, inherently limited by its reliance on self-reported data susceptible to recall bias and its inability to qualitatively explore underlying drivers, this research necessitates future studies that employ patient interviews to elucidate the root causes.
Conclusion
The current investigation employed LCA to categorize patient satisfaction with VIP outpatient services into two distinct classes in Beijing. Aligning with the SERVQUAL framework, our results showed that the “High Medical Care - Low Support Service” group exhibits a distinct alignment with its core dimensions: high scores in “assurance” (eg, doctor–patient interaction) and “empathy” (eg, nursing care), but lower scores in “tangibles” (eg, outpatient guidepost) and “responsiveness” (eg, response of needs). Furthermore, the findings indicate that tailored management strategies should be developed for patients from different geographic sources, and that strengthening the selection and training of doctors in VIP outpatients is essential to meet the core clinical needs of non-local patients. Moreover, controlling waiting time remains a critical operational priority. Lastly, adequate physician assistant staffing alongside effective information exchange is critical for constructive and efficient doctor-patient communication.
Data Sharing Statement
Data is available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethics approval was granted by the Ethics Committee of the Peking University First Hospital (NO. 2025R0051-0002).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Peking University First Hospital Scientific Research Project Fund (2025SF124).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Akin T. Assessing quality of health care in the context of patient satisfaction from patients’ perspective among a physical therapy and rehabilitation unit. BMC Health Serv Res. 2025;25(1). doi:10.1186/s12913-025-12214-w
2. National Health Commission. Statistical bulletin on the development of health care in China in 2023. 2023. Available from: https://www.nhc.gov.cn/guihuaxxs/c100133/202408/0c53d04ede9e4079afff912d71b5131c/files/1734002454304_67772.pdf.
3. McIntosh JT. VIP care: ethical dilemmas and recommendations for nurses. Nurs Ethics. 2020;27(3):809–820. doi:10.1177/0969733019878833
4. Yang Y, Cheng M, Chen N, Yuan L, Wang Z. Do VIP medical services damage efficiency? New evidence of medical institutions’ total factor productivity using Chinese panel data. Front Public Health. 2023;11. doi:10.3389/fpubh.2023.1261804
5. Von Dem Knesebeck O, Klein J. Attitudes towards the dual health insurance system and inequalities in health care in Germany - results of a population survey. BMC Health Serv Res. 2025;25(1). doi:10.1186/s12913-025-12847-x
6. Cleary MI, Murray JM, Michael R, Piper K. Outpatient costing and classification: are we any closer to a national standard for ambulatory classification systems? Med J Australia. 1998;169(S1):S26–S31. doi:10.5694/j.1326-5377.1998.tb123472.x
7. Cleary M. Outpatient costing and classification. Med J Australia. 1999;170(6):286–287. doi:10.5694/j.1326-5377.1999.tb127772.x
8. The State Council of the People’s Republic of China. Notice of the general office of the state council on issuing the national health plan for the 14th five year plan. 2022. Available from: https://www.gov.cn/zhengce/content/2022-05/20/content_5691424.htm?trs=1.
9. Alemu WG, Mwanri L, Due C, Azale T, Ziersch A. Mental health service satisfaction among adults with mental illness attending a psychiatric outpatient clinic: a cross-sectional study. Front Public Health. 2025;13. doi:10.3389/fpubh.2025.1471297
10. Liang H, Xue Y, Zhang Z. Patient satisfaction in China: a national survey of inpatients and outpatients. BMJ Open. 2021;11(9):e049570. doi:10.1136/bmjopen-2021-049570
11. Jonkisz A, Karniej P, Krasowska DM. Meeting patient expectations: assessing medical service and quality of care using the SERVQUAL model in dermatology patients at a single center in Poland. Med Sci Monit. 2023;29. doi:10.12659/msm.941007
12. Cai Y, Liu Y, Liu S, Wang C, Jiang Y. A cross-sectional study on the relationship between length of stay and patient satisfaction based on the SERVQUAL model. Sci Rep. 2025;15(1):5605–5611. doi:10.1038/s41598-025-90176-z
13. Parasuraman AZ, Berry LL, Berry LL. A conceptual model of service quality and its implications for future research. J Mark. 1985;49(4):41–50. doi:10.1177/002224298504900403
14. Wei L, Zhang X, Li H, Wang Y, Lu M, Chai Q. Construction of internet plus wound care service quality evaluation system based on donabedian and SERVQUAL models—A delphi-analytic hierarchy process study. Nurs Health Sci. 2025;27(1). doi:10.1111/nhs.70051
15. Zhao J, Liu Q, Son H, Liu Y. Errand delivery adoption by business users: integrated perceived SERVQUAL model within TOE - TAM model. Res Transp Bus Manag. 2025;59. doi:10.1016/j.rtbm.2025.101313
16. Wisutwattanasak P, Champahom T, Jomnonkwao S, Aryuyo F, Se C, Ratanavaraha V. Examining the impact of service quality on passengers’ intentions to utilize rail transport in the post-pandemic era: an integrated approach of SERVQUAL and health belief model. Behav Sci. 2023;13(10):789–795. doi:10.3390/bs13100789
17. Onyemaechi S, Ezenwaka U, Okeke C, Ibeziakor T, Okuakaji C, Osifala O. Assessing determinants of enrollees’ satisfaction with quality of health services within the state social health insurance scheme: an application of modified SERVQUAL model. Niger J Clin Pract. 2025;28(4):513–524. doi:10.4103/njcp.njcp_562_23
18. McMullan RD, Badgery-Parker T, Li L, Urwin R, Westbrook J. Management and administration and non-clinical services staff experiences of co-worker unprofessional behaviour and their reported speaking-up skills: a survey across seven Australian hospitals. J Health Organ Manag. 2025;1–15. doi:10.1108/jhom-04-2024-0164
19. Saikali LM, Herrera CD, Chen AT, et al. The center for surgical health (CSH). Ann Plast Surg. 2025;94(4S):S390–S394. doi:10.1097/sap.0000000000004285
20. Farrokhi P, Aryankhesal A, Bagherzadeh R, Hashjin AA. Evaluation of outpatient service quality: what do patients and providers think? Int J Healthcare Man. 2023;16(3):394–403. doi:10.1080/20479700.2022.2110195
21. Carmody N, Eikelboom RH, Tegg-Quinn S. Seeking help for tinnitus and satisfaction with healthcare providers including diagnosis, clinical services, and treatment: a scoping review. Eval Health Prof. 2023;46(2):170–193. doi:10.1177/01632787231158402
22. Kinsman T, Reid S, Arnott H. Taking a value based commissioning approach to non-clinical and clinical support services. Aus Health Rev. 2024;48(2):154–159. doi:10.1071/AH23278
23. Kashfi SM, Karimian E, Ravangard R, Mehralian G, Bastani P. Service quality in outpatient teaching hospital pharmacies based on the SERVQUAL model: an assessment in the south of Iran. Int J Pharm Pract. 2022;30(2):153–159. doi:10.1093/ijpp/riac004
24. Asiamah N, Opuni FF, Aggrey M, Adu-Gyamfi K. ADAPTED SERVQUAL: a health service quality scale incorporating indicators of sanitation and hygiene. Qual Man Health C. 2021;30(3):184–193. doi:10.1097/qmh.0000000000000269
25. Productivity Commission. Productivity commission inquiry report: mental health. 2020. Available from: www.pc.gov.au/inquiries/completed/mental-health/report.
26. Keynejad R, Spagnolo J, Thornicroft G. WHO mental health gap action programme (mhGAP) intervention guide: updated systematic review on evidence and impact. Evid-Based Ment Heal. 2021;24(3). doi:10.1136/ebmental-2021-300254
27. Han T, Wei QP, Wang RK, et al. Service quality and patient satisfaction of internet hospitals in China: cross-sectional evaluation with the service quality questionnaire. J Med Internet Res. 2024;26:e55140. doi:10.2196/55140
28. Lu PY, Yang CY, Yao J, Xian MX, Shelley M. Patterns of outpatient service satisfaction among low-income adults in rural China: a latent class analysis. Healthcare. 2022;10(8):1380. doi:10.3390/healthcare10081380
29. Karmacharya BM, Marasini S, Sharma S, et al. Patient satisfaction with the components of the national health insurance program of Nepal: a cross-sectional study. BMC Health Serv Res. 2025;25(1). doi:10.1186/s12913-025-12893-5
30. Alhasan MS, Alahmadi IM, Alhilali HF, et al. Determinants of patient satisfaction among outpatients with chronic illnesses in the region of medina, Saudi Arabia: a cross-sectional study. BMC Health Serv Res. 2025;25(1). doi:10.1186/s12913-025-13116-7
31. Zhou X, He Q, Li Q, Kuang J, Han Y, Chen J. Factors associated with outpatient satisfaction in provincial tertiary hospitals in Nanchang, China: a structural equation modeling approach. Int J Environ Res Pub He. 2022;19(14). doi:10.3390/ijerph19148226
32. Zhou F, Xu C, Sun Y, Meng X. Influencing factors of outpatients’ satisfaction in China a cross-sectional study of 16 public tertiary hospitals. Patient Prefer Adher. 2021;15:1243–1258. doi:10.2147/PPA.S311786
33. Spurk D, Hirschi A, Wang M, et al. Latent profile analysis: a review and “how to” guide of its application within vocational behavior research. J Vocat Behav. 2020;120:103445. doi:10.1016/j.jvb.2020.103445
34. Goldshear JL, Ganesh SS, Borquez A, Gelberg L, Corsi KF, Bluthenthal RN. Material hardship, forced displacement, and negative health outcomes among unhoused people who use drugs in Los Angeles, California and Denver, Colorado: a latent class analysis. BMC Public Health. 2025;25(1). doi:10.1186/s12889-025-21626-6
35. Irving G, Neves AL, Dambha-Miller H, et al. International variations in primary care physician consultation time: a systematic review of 67 countries. BMJ Open. 2017;7(10):e017902. doi:10.17863/CAM.21761
36. Dibba Y, Boima F, Jerome JG, et al. Patient satisfaction and its associated factors in selected primary healthcare facilities in Kono District, Sierra Leone: a cross-sectional study. BMJ Open. 2025;15(4):e093501. doi:10.1136/bmjopen-2024-093501
37. Ke L, Chen JS, Jia J, et al. Outpatients’ satisfaction in the context of 10 years of health-care reform: a cross-sectional study of tertiary hospitals in Shiyan, China. Patient Prefer Adher. 2020;14:191–202. doi:10.2147/ppa.S233472
38. Liu XJ, Lu HS, Wang YN, et al. Factors affecting patient satisfaction with ecdemic medical care: a cross-sectional study in Nanchang, China. Patient Prefer Adher. 2018;12:1373–1382. doi:10.2147/ppa.S167244
39. Pan J, Liu D, Ali S. Patient dissatisfaction in China: what matters. Soc Sci Med. 2015;143:145–153. doi:10.1016/j.socscimed.2015.08.051
40. Liu Y, Skup M, Lin J, Chao J. Impact of non-medical switching on healthcare costs: a claims database analysis. Value Health. 2015;18(3):A252. doi:10.1016/j.jval.2015.03.1465
41. Alamoudi M. Estimating patients’ satisfaction in healthcare sector using multiple regression analysis. Adv Appl Stat. 2025;92(2):273–302. doi:10.17654/0972361725013
42. Burrer A, Spiller TR, Koussemou JM, et al. Psychiatric treatment outcomes of travelers admitted to a psychiatric hospital: a retrospective analysis. Trop Dis Travel Med. 2025;11(1):9–15. doi:10.1186/s40794-024-00244-x
43. Chen XY, Liu C, Yan PP, Wang HL, Xu JJ, Yao K. The impact of doctor-patient communication on patient satisfaction in outpatient settings: implications for medical training and practice. BMC Med Educ. 2025;25(1). doi:10.1186/s12909-025-07433-y
44. Bleustein C, Rothschild DB, Valen A, Valatis E, Schweitzer L, Jones R. Wait times, patient satisfaction scores, and the perception of care. Am J Manag Care. 2014;20(5):393–400.
45. Leive A, David G, Candon M. On resource allocation in health care: the case of concierge medicine. J Health Econ. 2023;90:102776. doi:10.1016/j.jhealeco.2023.102776
46. Chen SL. The evaluation of rural elderly care service quality under group public health management with SERVQUAL model. Curr Psychol. 2025;44(13):12880–12891. doi:10.1007/s12144-025-08086-2
47. Alhawshani S, Khan S. A literature review on the impact of concierge medicine services on individual healthcare. J Family Med Prim Care. 2024;13(6):2183–2186. doi:10.4103/jfmpc.jfmpc_1685_23
48. Nguyen M, Mehrotra A, Malik A, Pandey R. Nexus between generative AI engagement, quality and expectation formation: an application of expectation-confirmation theory. J Enterp Inf Manag. 2025;38(3):798–820. doi:10.1108/jeim-08-2024-0452
49. Mahfouz MS, Ryani MA, Shubair AA, et al. Evaluation of patient satisfaction with the new web-based medical appointment systems “Mawid” at primary health care level in Southwest Saudi Arabia: a cross-sectional study. Cureus. 2023;15(1). doi:10.7759/cureus.34038
50. Xintong Z, Tao X, Shuying W, et al. An evaluation of outpatient satisfaction based on the national standard questionnaire: a satisfaction survey conducted in a tertiary hospital in Shenyang, China. Front Public Health. 2024;12. doi:10.3389/fpubh.2024.1348426
51. Shaikh NQ, Afzal N, Rahim KA, et al. A cross-sectional study to assess patients’ perception of physicians’ communication skills: 15 minutes is what it takes. Patient Educ Couns. 2025;138:109191. doi:10.1016/j.pec.2025.109191
52. Qin YX, Lin Y, Han J, Zhang XX, Li J. Teach back educational model combined with zinc supplementation improves clinical symptoms and immunity in children with asthma. Afr J Reprod Health. 2025;29(5s):43–50. doi:10.29063/ajrh2025/v29i5s.6
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.