Back to Journals » Vascular Health and Risk Management » Volume 20
Exploring Myocardial Infarction Knowledge, Attitudes, and Practice Among Mogadishu’s Somali Residents
Authors Hassan MO ![]() , Ahmed SA
, Ahmed SA ![]() , Hassan MS
, Hassan MS ![]() , Mohamud MA
, Mohamud MA ![]() , Abdi AE
, Abdi AE ![]()
Received 15 November 2023
Accepted for publication 29 December 2023
Published 3 January 2024 Volume 2024:20 Pages 13—20
DOI https://doi.org/10.2147/VHRM.S448220
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Mohamed Omar Hassan,1 Said Abdirahman Ahmed,1 Mohamed Sheikh Hassan,2 Mohamed Abdullahi Mohamud,1 Ahmed Elmi Abdi1
1Department of Cardiology, Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia; 2Department of Neurology, Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia
Correspondence: Mohamed Omar Hassan, Email [email protected]
Introduction: Myocardial infarction and cardiovascular disease are significant global health issues, particularly in Somalia. The Somali population faces challenges due to armed conflict, limited education, and underdeveloped healthcare infrastructure. Cardiovascular risk factors like diabetes, hypertension, and obesity are prevalent, and Somali people face increased susceptibility.
Methods: This study examined Somalia residents’ perceptions, attitudes, and behaviors towards myocardial infarction using a cross-sectional paper-based questionnaire. The sample consisted of 313 urban residents in Mogadishu, aged 20 and above. The questionnaire was written in Somali and was designed for the demographic. Knowledge, attitude, and practice scores were categorized into two groups, with associations between knowledge, attitude, and practice with sociodemographic and health characteristics assessed using Logistic Regression.
Results: This study analyzed data from A random sample of participants who arrived at the hospital for various reasons regarding their perceptions, attitudes, and responses towards myocardial infarction. The mean age was 42 ± 19 years, with 54% being male and 46% female. Hypertension was the most common comorbidity, followed by dyslipidemia and diabetes. Over half of the respondents had no formal education, and only 3.8% had a smoking history. About 5.7% had a previous history of myocardial infarction. The mean knowledge score was 11.07 ± 0.697, with 53.35% of respondents not knowing enough about myocardial infarction. The majority of the patients showed a favorable attitude, but only a slight majority could recognize symptoms of myocardial infarction. The majority of the patients had inadequate practice and behavior, with 53.6% not practicing regularly or engaging in sports.
Conclusion: The research highlights gaps in Mogadishu’s Somali community’s knowledge and practices regarding myocardial infarction. It emphasizes the need for health education, primary care, and community involvement to improve cardiovascular health awareness and reduce MI incidence.
Keywords: myocardial infarction, Somalia, cardiovascular disease, knowledge, practice
Introduction
Myocardial infarction (MI) and cardiovascular disease (CVD) are prominent global health issues, which also pose a major burden within the Somali population. The Somali population encounters distinct obstacles as a result of the repercussions of armed conflict, limited access to education, and an underdeveloped healthcare infrastructure. Myocardial Infarction (MI), commonly known as a heart attack, is a critical medical condition characterized by the interruption of blood supply to a part of the heart muscle, leading to the death of heart tissue. It is a global health concern with significant variations in knowledge, attitude, and practices in different regions, including Africa and specifically Somalia.
Numerous researches have shed light on the significant frequency of cardiovascular risk factors within Somali communities, encompassing conditions such as diabetes, hypertension, and obesity.1 These identified risk variables are known to play a significant role in the pathogenesis of myocardial infarction (MI) and cardiovascular disease (CVD). Furthermore, it has been observed that Somali immigrants and refugees residing in the United States face an elevated susceptibility to obesity and associated cardiovascular health risks.2 This observation indicates the necessity of implementing specific interventions aimed at addressing these risk factors and enhancing cardiovascular well-being within the Somali population.
While there is limited research specifically focused on MI in Somalia, studies conducted in other African countries and among Somali diaspora populations provide valuable insights into the knowledge, attitudes, and practices regarding these conditions. Furthermore, the prevalence of MI is unknown in Somalia but is presumed to be high.
The influence of socioeconomic factors on the development and management of cardiovascular illnesses is of paramount importance. Research undertaken in the sub-Saharan African region, encompassing adjacent nations such as Ethiopia and Tanzania, has shed light on the influence of low socioeconomic level on cardiovascular risk factors and outcomes.3,4 Understanding and managing cardiovascular illnesses requires a high level of health literacy. For instance, low health literacy has been linked to an increased risk of death in people with end-stage renal disease.5
Attitudes toward healthcare and preventative medicine also have an impact on the treatment of MI. Somali patients are less familiar with preventive healthcare practices and tend to seek medical attention only when they are sick.6 Aside from individual knowledge, attitude, and practice, the healthcare system is also important in preventing myocardial infarction. The value of evidence-based preventative strategies is emphasized in guidelines for the management of acute myocardial infarction.7 This study aims to analyze knowledge, attitudes, and behaviors about myocardial infarction among Mogadishu citizens, focusing on socio-economic issues and health literacy, to address healthcare obstacles and improve cardiovascular health outcomes within the Somali community.
Methods and Materials
Design and Settings
A cross-sectional survey in the form of paper-based questionnaire was prepared for this study and used for data collection from 1 June to 31 August to examine Somalia inhabitants’ Perceptions, Attitudes, and behaviors towards Myocardial Infarction. A random sample of participants who arrived at our hospital Mogadishu Somali Turkish Training and Research Hospital for various reasons were referred to our cardiology clinic for the study, they were greeted by a resident doctor, consent was obtained, and they were supported in understanding and answering the questions.
Participants
People above the age of 20 who came to our hospital and accepted to participate in the study. Somali urban residents of Mogadishu were the intended participants; Somalis living outside of Mogadishu or Somalia were not eligible for this study. A sample of 313 urban residents in Mogadishu were collected. With an approximately 95% confidence level, the margin of error is approximately ±5%.
Questionnaire
The questionnaire utilized was similar to other myocardial infarction questionnaires. It was, however, specifically created for our demographic. The questionnaire was written in Somali, and the writing was clear and concise. The process of creating the questionnaire began with the establishment of precise research goals pertaining to cardiovascular health within the community. The selection of important variables was guided by a review of the literature. The questionnaire was created using language that was considerate of cultural differences and underwent validity testing. Any problems with the clarity and cultural appropriateness of the questions were found and fixed in a pilot study with a diverse sample. As a result, the questionnaire is revised. By giving the updated questionnaire to a subset of participants twice, test-retest reliability is guaranteed. The final version is then utilized to collect data for the primary sample. The data was collected and assisted by a resident doctor who was not involved with any patient care, and the sample was random and was collected from participants who came our hospital for various reasons, whether they had risk factors, previous history of myocardial infarction or simply as a relative of a patient or those who came for a simple check-up. Everyone had an equal chance of being requested to participate for the study.
It takes around 7 minutes to complete the questions, and any query or difficulty in comprehending was cleared by a resident doctor who assisted the patient at every step of the process. Questions included demographic data, such as age, weight, height, education level. Past medical data were also collected, for instance, diabetes or hypertension history, and if there was any previous myocardial infarction. Knowledge, attitude, and practice questions were answered similarly with a binary yes or no, and each response was scored 1 and 0, respectively. In order to assess the reliability of the questionnaire, it was subjected to a pretesting process including a randomly selected sample. No notable language-related challenges were found throughout this procedure.
Statistical Analysis
The study employed IBM SPSS 24 for Windows. For continuous variables, descriptive statistics were reported as mean ± standard deviation (SD), while for other variables, frequencies (%) were employed. The scores of the participants pertaining to knowledge, attitudes, and beliefs were presented and analyzed. The highest attainable scores for knowledge, attitude, and practice were 22, 9, and 7, correspondingly. Moreover, the overall knowledge, attitude and practice scores was categorized into two distinct groups. For example, knowledge was considered to be sufficient for any result above 11, while 11 or less was considered insufficient knowledge. Furthermore, for attitude and practice we similarly scored them into two categories. 5 and less was considered poor attitude, while above was assigned as good attitude. For practice, scores 4 and less were considered inadequate practice, in contrast scores above were acknowledged as adequate practice.
Associations between knowledge, attitude and practice with variable sociodemographic and health characteristics were assessed using Logistic Regression. For every analysis, we employed p < 0.05 to establish statistical significance.
Ethical Consideration
Due to the fact that our hospital is a research hospital an informed consent is obtained from every patient before giving them the questionnaire and assisting them in answering the questions. This study did not disclose any personal information. The study was approved by the research ethics committee of Mogadishu Somali Turkey Training and Research Hospital. The study was performed in line with the principles of the Declaration of Helsinki.
Results
Socio-Demographic Features
In this study the data collected from 313 participants in the hospital for various reasons regarding their perceptions, attitudes, and responses towards myocardial infarction were analyzed. The mean age was 42 ±19 years of age. One hundred and seventy patient (54%) of the subjects were male, and 143 (46%) were female. Hypertension was the most common comorbidity in these subjects 64 (20%), followed by dyslipidemia 41 (13%) and diabetes 36 (11.5%). More than half of the respondents 163 (51%) did not have formal education. Only 12 (3.8%) had smoking history, and 14 (4.4%) had regular practice of Khat chewing. The mean weight of patients was 68±27 kg. Eighteen (5.7%) of the respondents had previous history of myocardial infarction.
Knowledge Results
The mean knowledge score of the participants was 11.07 ± 0.697, with a maximum score of 22. It was discovered that n=167, 53.35% of respondents did not know enough about myocardial infarction using the cut-off criteria (Figure 1). Out of those surveyed, 172 (or 55%) said that a clot-induced arterial blockage was the reason behind the myocardial infarction. Similarly, 187 participants, or 59.7%, acknowledged that MI may be lethal. Additionally, over 50% of the participants were aware that MI typically manifests as chest pain; only 131 (41.9%) were aware that MI might occasionally manifest without chest pain. Only 153 (48.9), 141 (45%), and 141 (45%) of the respondents—or fewer than half—identified hypertension, diabetes, and dyslipidemia as risk factors for MI when questioned about their potential contributions. Sedentary lifestyle was identified as a risk factor by 129 (41.2%) and obesity by 137 (43.8%). Moreover, the majority of participants did not regard weight loss, diabetes management, or hypertension control as helpful in the fight against myocardial infarction and cardiovascular disease. Surprisingly, 205 (65.5%) of our respondents acknowledged that MI is a medical emergency requiring prompt medical intervention. (Table 1)
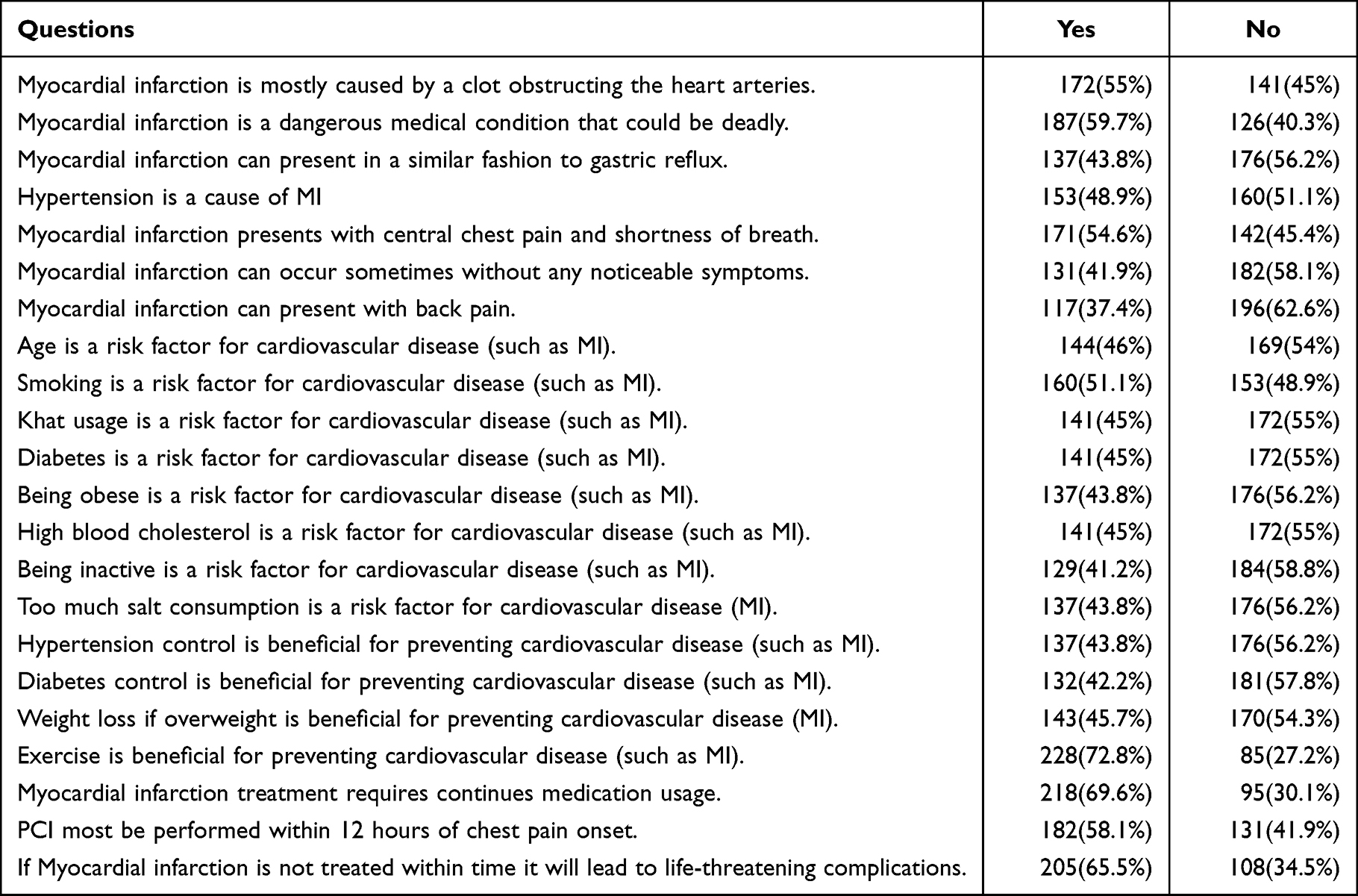 |
Table 1 Reponses to the Knowledge Questions Provided by the Participants, Detailing Their Knowledge About Cardiovascular Disease and Myocardial Infarction |
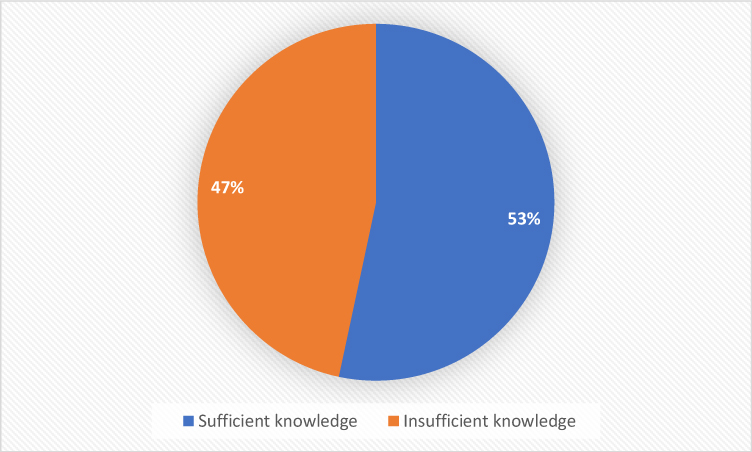 |
Figure 1 Overall knowledge of the study respondents. |
Attitude Results
The mean attitude score of the respondents was 5.086±0.3756. Using cut-off criteria, a slight majority of the patient showed favorable attitude. Almost 168 (53.7%) said they could recognize the symptoms of myocardial infarction. In contrast only 144 (46%) said they can recognize it in others. Furthermore, 154 (49.2%) believed MI is unpreventable, while 201 (64.2%) said they will accept a MI diagnose from a doctor. Lastly, 202 (64.5%) said they are ready to do whatever it takes to lower their risk of myocardial infarction. (Table 2)
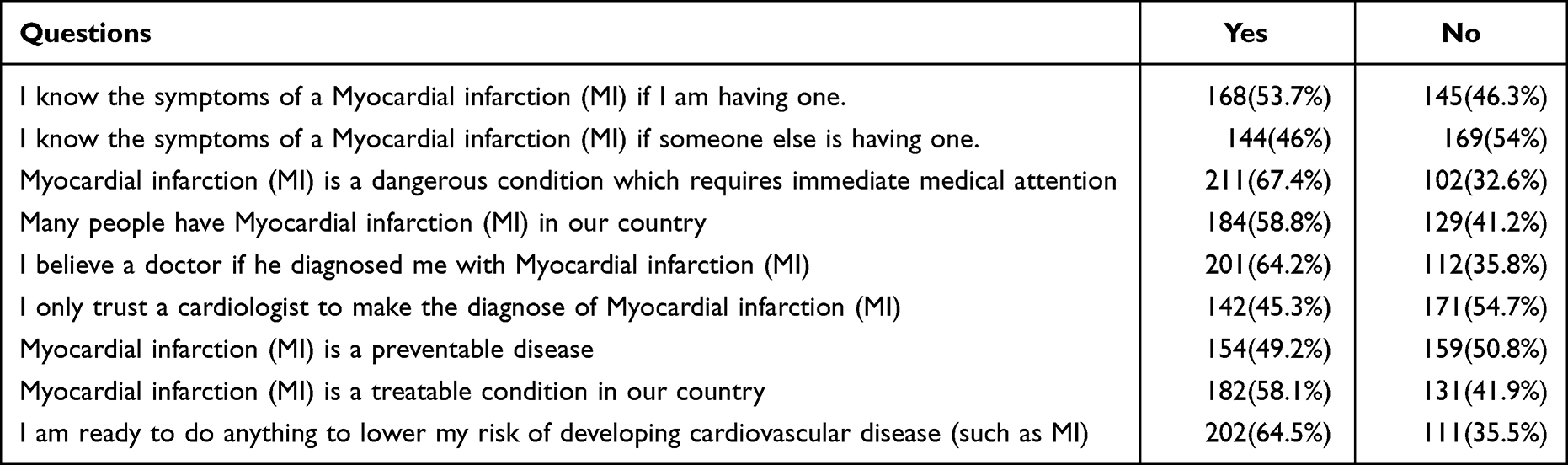 |
Table 2 Reponses to the Attitude Questions Provided by the Participants, Detailing Their Attitude Towards Cardiovascular Disease and Myocardial Infarction |
Practice Results
The practice score average was 3.463259±0.352. Majority of the patient had inadequate practice and behavior according to the cut-off score. 168 (53.6%) of the respondents did not practice regularly or engage in any kind of sport. Only 119 (38%) of those questioned did not regularly check their blood pressure, sugar level or their cholesterol level. Majority of the patient did not also control their salt, sugar and fatty food intake. Noticeably, out of those who had diabetes and hypertension or dyslipidemia more than 75% of them did not comply with their medications. (Table 3)
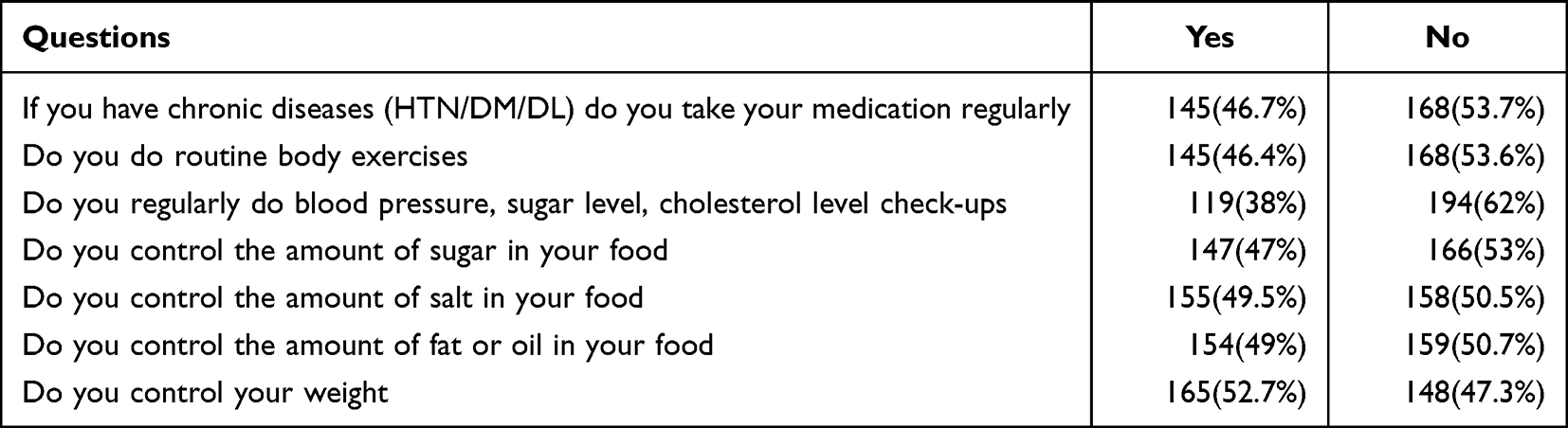 |
Table 3 Reponses to the Practice Questions Provided by the Participants, Detailing Their Behavior Towards Cardiovascular Disease and Myocardial Infarction |
Factors Related to Myocardial Infarction Knowledge, Attitudes, and Practices
In a logistic regression, the following predicator variables such as age, gender, educational status, and a history of diabetes, hypertension, and dyslipidemia were input as variables against the knowledge, attitude and practice scores to be analyzed. With the exception of one group, however, we did not find any significant associations between the various variables and the level of knowledge. It was discovered that participants who were male and had not received any formal education had a higher probability of having a lower knowledge, unfavorable attitude and inadequate practice level (P=<0.05).
Discussion
In this discussion, we will compare Mogadishu’s citizens’ understanding, attitudes, and practices around MI with those of other parts of Africa and the globe. We will also investigate the causes of the differences and provide potential solutions. Numerous researches have looked at various groups’ knowledge, attitudes, and practices about MI. For instance, research carried out in Tanzania discovered that just a small percentage of people there believed they were at risk of MI, and that everyone knew very little about the disease’s symptoms.8 This result was similar to our population findings. The prevalence of MI is rising throughout Africa.9 However, a study that was carried out in three nations—the United States, Australia, and New Zealand—reported similar findings, with 56% of participants knowing enough about ACS symptoms.10 Moreover, MI cases are rising in South Africa which many considers the most developed country in Africa.11 These data show that improved MI prevention, education and management strategies are required in Africa. The relationship between health literacy and the management and prevention of cardiovascular disease is one crucial factor. The scientific statement released by the American Heart Association highlights the basic need of health literacy for both primary and secondary cardiovascular disease prevention.12 Another study also demonstrated that health literacy is connected to healthy behaviors and self-reported health in people with cardiovascular disease, which further validates this.13 These studies emphasize how critical it is to raise health literacy in order to increase understanding and encourage healthy habits related to MI. Somalia is believed to have a low health literacy due to years of civil war and poverty. According to a comprehensive review and meta-analysis by, attitudes toward Myocardial infarction have also been demonstrated to predict attendance at cardiac rehabilitation after an acute myocardial infarction.14 A small majority of our patients showed a favorable attitude towards myocardial infarction. This may be due to a popular perception that heart attack is deadly acute condition in Somali culture. For instance, Patients’ perceptions of their myocardial infarction can differ; according to a study by, some consider it to be an acute heart attack instead of a sign of a long-term illness.15 Effective management of myocardial infarction necessitates a thorough understanding of and implementation of preventative techniques.16 Diabetes mellitus, hypertension, dyslipidemia, and metabolic syndrome are risk factors for myocardial infarction.17,18 Based on the cut-off score, most of our patients exhibited inadequate conduct and practice. 53.6% of the respondents, or 168 people, said they did not play any sport or exercised on a regular basis. Improvements in lifestyle, such as frequent exercise and physical activity, are essential for preventing cardiovascular disease. Physical activity has demonstrated benefits for cardiovascular well-being and can lower the risk of atherosclerotic cardiovascular disease.19 Furthermore, most of the patients with chronic diseases did not comply with their medications in contrast to Seventy percent of hypertensive people in a Tshwane, South Africa research reported complying with treatment, while more than 80% of our hypertensive patients did not comply.20
It is important to think about the effects of telemedicine, mobile technology-based lifestyle in order to improve knowledge and practice. People have seen telemedicine as a possible way to improve health care and practice, especially for people with heart diseases.21 The use of mobile technology and smart devices has shown promise in changing the way people with a high risk of heart disease live, providing a practical way to enhance patient outcomes. These mobile technologies offer a way in which many people with the disease, risk factors or relatives of these groups can be educated.22 Moreover, the internet provides a vast and extensive platform to access an audience of individuals who may have been previously deemed hard to reach. Sharing articles and videos about myocardial infarction can enhance understanding and influence behaviors related to this serious condition. Nevertheless, deceptive information can also be spread online.23 To summarize, effectively addressing knowledge about myocardial infarction (MI) in Mogadishu necessitates implementing customized interventions that take into account cultural subtleties. It is crucial to utilize health literacy and technology to develop efficient strategies for prevention and management.
Limitations of Our Study
In our study we faced several limitations. First, there may be a limit due to the sample size and representativeness. Our study may not have included a representative and varied sample of the Somali population due to restricted access, which could have resulted in selection bias. Second, response bias is introduced by our data collection methods, such as surveys and interviews, as participants may give socially acceptable replies. This could result in an underestimating of bad practices or an overestimation of knowledge and positive attitudes. Another issue with self-reported data is the potential for recollection or social desirability biases, which could skew the responses and effect data quality. Finally, the breadth of our study may be constrained by a lack of funding and time, which could have an impact on the number of participants or data collection locations.
Conclusion
In conclusion, our research highlights the serious gaps in the Somali community of Mogadishu’s knowledge, attitudes, and practices surrounding myocardial infarction (MI). To improve cardiovascular health awareness and management, the results highlight the critical need for focused health education, enhanced primary care, and community involvement. In order to close these gaps and guarantee that prompt and efficient interventions result in a healthier and better-informed Somali population, policymakers and healthcare professionals must work together. This will eventually lessen the incidence of MI in the area.
Author Contributions
Each author contributed significantly to the work reported, whether it was through conception, study design, execution, data acquisition, analysis, and interpretation, or in all of these areas; they all helped draft, revise, or critically review the article; they approved the final version that was published; they all agreed on the journal to which the article was submitted; and they all agreed to take responsibility for the work in its entirety.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mohamed A, Lantz K, Ahmed Y, et al. An assessment of health priorities among a community sample of Somali adults. J Immigrant Minority Health. 2021;24(2):455–460. doi:10.1007/s10903-021-01166-y
2. Njeru J, Wieland M, Okamoto J, et al. Social networks and obesity among Somali immigrants and refugees. BMC Public Health. 2020;20(1). doi:10.1186/s12889-020-8315-7
3. Yuyun M, Sliwa K, Kengne A, Mocumbi A, Bukhman G. Cardiovascular diseases in sub-saharan Africa compared to high-income countries: an epidemiological perspective. Global Heart. 2020;15(1):15. doi:10.5334/gh.403
4. Cappuccio F, Miller M. Cardiovascular disease and hypertension in sub-saharan Africa: burden, risk and interventions. Int Emerg Med. 2016;11(3):299–305. doi:10.1007/s11739-016-1423-9
5. Cavanaugh K, Wingard R, Hakim R, et al. Low health literacy associates with increased mortality in ESRD. J Am Soc Nephrol. 2010;21(11):1979–1985. doi:10.1681/asn.2009111163
6. Pavlish C, Noor S, Brandt J. Somali immigrant women and the American health care system: discordant beliefs, divergent expectations, and silent worries. Soc sci med. 2010;71(2):353–361. doi:10.1016/j.socscimed.2010.04.010
7. Steg P, James S, Atar D, et al. Esc guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Revista Española De Cardiología. 2013;33:548.
8. Hertz J, Madut D, Tesha R, et al. Knowledge of myocardial infarction symptoms and perceptions of self-risk in Tanzania. Am Heart J. 2019;210:69–74. doi:10.1016/j.ahj.2019.01.003
9. Mensah G. Ischaemic heart disease in Africa. Heart. 2008;94(7):836–843. doi:10.1136/hrt.2007.136523
10. Dracup K, McKinley S, Doering LV, et al. Acute coronary syndrome: what do patients know? Arch Internal Med. 2008;168(10):1049–1054. doi:10.1001/archinte.168.10.1049
11. Stassen W, Olsson L, Kurland L. The application of optimisation modelling and geospatial analysis to propose a coronary care network model for patients with ST-elevation myocardial infarction. Afr J Emergency Med. 2020;
12. Magnani J, Mujahid M, Aronow H, et al. Health literacy and cardiovascular disease: fundamental relevance to primary and secondary prevention: a scientific statement from the American heart association. Circulation. 2018;138(2). doi:10.1161/CIR.0000000000000579
13. Aaby A, Friis K, Christensen B, Rowlands G, Maindal H. Health literacy is associated with health behaviour and self-reported health: a large population-based study in individuals with cardiovascular disease. Eur J Preventive Cardiol. 2017;24:1880.
14. French D, Cooper A, Weinman J. Illness perceptions predict attendance at cardiac rehabilitation following acute myocardial infarction: a systematic review with meta-analysis. J Psychosomatic Res. 2006;61(6):757–767. doi:10.1016/j.jpsychores.2006.07.029
15. Brink E, Karlson B, Hallberg L. Readjustment 5 months after a first‐time myocardial infarction: reorienting the active self. Journal of Advanced Nursing. 2006;53(4):403–411. doi:10.1111/j.1365-2648.2006.03737.x
16. Adhikari A, Bhandari B. Awareness and practice of prevention of myocardial infarction among hypertensive patients: cross sectional study in a tertiary cardiac centre of Nepal. Nepalese Heart J. 2017;14(1):25–28. doi:10.3126/njh.v14i1
17. Uppin A, Badiger R, Sharma G, Soni R, Parne S, Maddiri P. Assessment of incidence rate and prognosis of metabolic syndrome among acute myocardial infarction: a longitudinal study. Int J Adv Med. 2020;7(2):267. doi:10.18203/2349-3933.ijam20200077
18. Shepherd J, Cobbe S, Ford I, et al. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. N Engl J Med. 1995;333(20):1301–1308. doi:10.1056/nejm19951116
19. Thompson P, Buchner D, Piña I, et al. Exercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease. Circulation. 2003;107(24):3109–3116. doi:10.1161/01.cir.0000075
20. Mafutha G, Wright S. Compliance or non-compliance of hypertensive adults to hypertension management at three primary healthcare day clinics in Tshwane. Curationis. 2013;36(1). doi:10.4102/curationis.v36i1.52
21. Hayıroğlu M. Telemedicine: current concepts and future perceptions. Anatolian J Cardiol. 2019. doi:10.14744/anatoljcardiol.2019.12525
22. Tekkeşin A, Hayıroğlu M, Çinier G, et al. Lifestyle intervention using mobile technology and smart devices in patients with high cardiovascular risk: a pragmatic randomised clinical trial. Atherosclerosis. 2021;319:21–27. doi:10.1016/j.atherosclerosis.2020.12.020
23. Hayıroğlu Mİ, Çinier G, Keser N, et al. Evaluation of websites reached using Google in the modern digital era related to approach to cholesterol. Turk Kardiyol Dern Ars. 2020;48(6):576–584. doi:10.5543/tkda.2020.40306
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Assessment of Knowledge, Practice, and Associated Factors Towards Airway and Breathing Management Among Nurses Working in the Emergency Departments of Selected Public Hospitals in Addis Ababa, Ethiopia: A Cross-Sectional Study
Nigatu M, Debebe F, Tuli W
Open Access Emergency Medicine 2022, 14:235-247
Published Date: 27 May 2022
Knowledge and Practice of Wound Care and Associated Factors among Nurses Working in South Wollo Zone Government Hospitals, Ethiopia
Tegegne B, Yimam F, Mengesha Yalew Z, Wuhib M, Mekonnen L, Asmamaw Yitayew Y, Ademe S, Tsegaye D, Eshetie Y, Chanie M
Chronic Wound Care Management and Research 2022, 9:1-11
Published Date: 20 July 2022
Knowledge, Attitudes, and Practices Regarding Ergonomic Hazards Among Healthcare Workers in a Saudi Government Hospital

ALHazim SS, Al-Otaibi ST, Herzallah NH
Journal of Multidisciplinary Healthcare 2022, 15:1771-1778
Published Date: 24 August 2022
Self-Medication Prevalence and Factors Associated with Knowledge and Attitude Towards Self-Medication Among Undergraduate Health Science Students at GAMBY Medical and Business College, Bahir Dar, Ethiopia
Siraj EA, Yayehrad AT, Kassaw AT, Kassahun D, Solomon E, Abdela H, Gizachew G, Awoke E
Patient Preference and Adherence 2022, 16:3157-3172
Published Date: 5 December 2022
Current Perspectives, Practices, and Barriers Faced by Community Pharmacists Regarding Pharmaceutical Care Services for Diabetes Mellitus in the United Arab Emirates
Jairoun AA, Al-Hemyari SS, Shahwan M, Jairoun SA, Alorfi NM, Zyoud SH, Suliman AA, Shahwan MK, Alnuaimi G, Shahwan M, Al-Qirim T, El-Dahiyat F
Journal of Multidisciplinary Healthcare 2024, 17:2563-2576
Published Date: 23 May 2024