Back to Journals » Patient Preference and Adherence » Volume 19
Exploring Health Literacy Needs in Different Stages of Older Patients with COPD: An in-Depth Qualitative Study
Authors Chen C ![]() , Qian Y, Wan G, Zhang Z
, Qian Y, Wan G, Zhang Z
Received 23 July 2025
Accepted for publication 24 October 2025
Published 5 November 2025 Volume 2025:19 Pages 3421—3433
DOI https://doi.org/10.2147/PPA.S550268
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ramón Morillo-Verdugo
Chen Chen,1,* Yinghua Qian,1,* Guangming Wan,1 Zhouji Zhang2
1Department of Nursing, Shanghai Chest Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 200030, People’s Republic of China; 2Department of Integrated Chinese and Western Medicine, Shanghai Chest Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 200030, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhouji Zhang, Department of Integrated Chinese and Western Medicine, Shanghai Chest Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 200030, People’s Republic of China, Email [email protected]
Background: As the incidence and recurrence rates of chronic obstructive pulmonary disease (COPD) among older people continue to rise globally, it is essential to understand the health literacy needs of these patients at various stages of the disease. Health literacy is closely linked to the risk of COPD onset and recurrence. However, there is a notable deficiency in research that specifically addresses the health literacy requirements of this population across different disease stages.
Objective: This study aimed to investigate the health literacy needs of older patients with COPD across various stages of their disease trajectory.
Methods: Utilizing a timing framework, purposive sampling was conducted from July 2023 to March 2024, selecting participants from Shanghai Chest Hospital. Semi-structured in-depth interviews were conducted, and thematic analysis was employed to interpret the data.
Results: A total of 28 participants completed the interviews, comprising 18 males and 10 females. Based on timing theory, these findings identified four themes: 1) Diagnostic period: Limited ability to acquire disease information, psychological support, and change unhealthy lifestyles, 2) Treatment period: therapeutic information support and efficient care, 3) Discharge preparation period: specific health guidance and a promising life plan, 4) Home recovery period: self-management, continuous healthcare support, and balancing self-discipline with external discipline.
Conclusion: The health literacy needs of older patients with COPD varied across different stages of the disease. Healthcare professionals should develop individualized health literacy interventions that are tailored to the specific needs and characteristics of individuals at different stages of their health journey.
Keywords: health literacy, older patients, COPD, qualitative study
Introduction
COPD is a respiratory condition primarily characterized by airflow limitation, which is associated with high morbidity and mortality rates. Surveys indicate that the prevalence of COPD in China is 21.2% among individuals aged 60–69 and 35.5% among those aged 70 and above, demonstrating an increasing trend year by year.1 In addition to respiratory symptoms such as coughing, sputum production, and dyspnea, COPD patients also experience systemic symptoms, including depression, anxiety, and fatigue, which had garnered significant attention.2,3 Studies show that pain is also a notable symptom in COPD patients, with prevalence rates ranging from 21% to 85%.4–6 Pain lead to increased medical expenses,7 exacerbation of dyspnea and fatigue,8,9 adverse effects on sleep quality10 and physical activity,11 and may contribute to the development of depression and anxiety.5
Personal lifestyle is the primary influencing factor in the onset and progression of COPD in older patients.12 The health literacy and self-management abilities of these patients play a decisive role in shaping their personal lifestyles. Health literacy is defined as “the degree to which individuals can obtain, process, and understand the basic health information and services they need to make appropriate health decisions”.13 Studies indicate that unhealthy habits, such as smoking, insufficient physical activity, and elevated stress levels, are contributors to the onset of COPD in older patients.14 Furthermore, a prospective cohort study demonstrates a negative correlation between behavioral habits influenced by health literacy and the risk of developing COPD.15 However, One survey reveals that the overall health literacy level among COPD patients is relatively low.16 COPD, as a prevalent chronic condition, has a treatment objective focused not on “cure” but on “long-term management”. This management encompasses symptom control, prevention of acute exacerbation, maintenance of lung function, enhancement of quality of life, and facilitation of social participation.17 A significant portion of this management is conducted by patients themselves outside of clinical settings. Consequently, it is imperative for patients to sustain a certain level of health literacy over time to achieve optimal management outcomes. It is noteworthy that patients encounter varying health literacy barriers, psychological states, and support expectations at different stages of the disease.18 For instance, the initial diagnosis of COPD may induce psychological shock, while changes in symptoms and an increased need for disease monitoring during treatment heighten patients’ demand for information. Additionally, the complex care skills required for long-term lifestyle adjustments post-discharge further complicate this scenario. Therefore, emphasizing the health literacy of COPD patients at different stages allows for an expansion of the concept from a static notion to a dynamic construct closely intertwined with disease progression and the life course.
The key to improving health literacy lies in scientifically and accurately assessing the individual health literacy needs and developing targeted interventions.19 However, the needs of COPD patients remain largely unexplored, and strengthening patient health education is still the primary means of intervention.20,21 The Timing It Right theory proposed by American scholar Cameron et al suggests that support and needs change over time, and therefore care must adapt to the dynamic needs of patients at different stages.22 The theory divides the disease process into five stages: the diagnostic period, the stable period, the discharge preparation period, the adjustment period, and the adaptation period. It has been effectively applied to the physiological, psychological, support needs, and nursing interventions for patients with acute respiratory distress syndrome23 and stroke.24 This theory is also applicable to patients with COPD, allowing for an examination of the specific health literacy needs at various stages of the disease. The health literacy needs of COPD patients are encompassed within this theoretical framework. Research indicates that during the treatment process, the complexity and rapid progression of COPD can lead to negative emotions, such as anxiety and depression, resulting in a heightened demand for psychological counseling from healthcare professionals.7 A longitudinal study found that the need for guidance on health behaviors remains largely unmet for most COPD patients following discharge, with only minimal improvements observed in their health behavior capabilities.13 Consequently, exploring the health literacy needs of COPD patients at different stages is an essential prerequisite for developing comprehensive intervention plans.
Considering the negative impact of age on cognitive levels, elderly patients may experience a decline in cognitive abilities as they age. This decline can lead to limitations in their understanding and comprehension of professional questions and complex scale items in quantitative questionnaires, making it challenging for them to accurately quantify their self-perceptions and experiences. Furthermore, the socio-economic development trajectory in China has resulted in a generally low educational level among the elderly population, which directly restricts their functional health literacy in accessing, interpreting, evaluating, and applying written health information.25 Traditional quantitative research paradigms exhibit inherent limitations in capturing the complex and implicit experiences of this demographic. Firstly, pre-set closed-ended questions are insufficient for capturing the rich realities that extend beyond the options provided in questionnaires. Secondly, standardized data outputs fail to reveal the underlying emotional motivations, cultural beliefs, and decision-making processes that inform the observed phenomena.26 In this context, the value of qualitative research becomes evident. Qualitative research creates a safe space that encourages free expression in the natural settings familiar to patients, utilizing flexible and open methods such as in-depth interviews and participatory observation. It does not aim for numerical generalizations, instead, it focuses on providing a “thick description” of the patients’ life worlds. This approach unveils how patients understand disease, cope with treatment challenges, interact with the healthcare system, and the individualized contexts and networks of meaning that inform their health decisions.27 Consequently, exploring the specific content of health literacy needs at various stages of COPD from a qualitative perspective is crucial for developing subsequent health literacy intervention programs. This shift enables our support to transition from “what we think patients need” to “what patients themselves feel they need”.
Therefore, this study aimed to investigate the health literacy needs of older patients with COPD across various stages of their disease trajectory.
Method
A descriptive study was conducted, using a qualitative and deductive approach in this work.28 The interview is featured by a semi-structural style in line with the consolidated criteria for reporting qualitative research (COREQ) guideline.29
Participants
The study participants were from Shanghai Chest Hospital. Study enrollment and interviews took place between July 2023 to March 2024. The inclusion criteria were as follows: A diagnosis of COPD was established following spirometric (post-bronchodilator FEV1/FVC < 0.70) and computed tomography (CT) assessments; age ≥ 60 years; language expression and communication are barrier-free. Additionally, patients were required to have stable vital signs, and both patients and their families were informed about the study and signed informed consent forms. The exclusion criteria included: a history of severe mental disorders or psychological disorders; severe impairment of vital organ functions (heart, liver, brain, or kidneys); and the presence of gastrointestinal tumors or other malignant tumors. Patients were also eliminated from the study if they discontinued treatment, abandoned treatment, or died during the treatment period, as well as those who needed to withdraw for personal reasons. The sample size adhered to the principle of data saturation, ie, in three consecutive interviews, no new concepts, categories, or themes related to the core research questions emerged, and the internal variations within the existing themes had been thoroughly explored.26
Based on Timing Theory and taking into account the clinical characteristics of COPD, the treatment stages of COPD had been categorized into four distinct periods: hospitalization for acute exacerbation period (within 24 hours of admission), the hospitalization treatment period, the discharge preparation period (1–2 days prior to discharge), and the home recovery period (3 months post-discharge). The corresponding patient groups for each stage were designated with the letters A, B, C, and D, respectively.
The design of the interview guide for this study was executed in three stages. Initially, the researcher drafted the guide based on the research objectives, relevant literature, consultations with experts, and clinical experience. In the second stage, a pre-interview was conducted with two participants who met the inclusion criteria. Finally, the interview guide was revised in light of the findings from the pre-interview and subsequently confirmed through group discussion. The specific content of the guide is presented in Table 1.
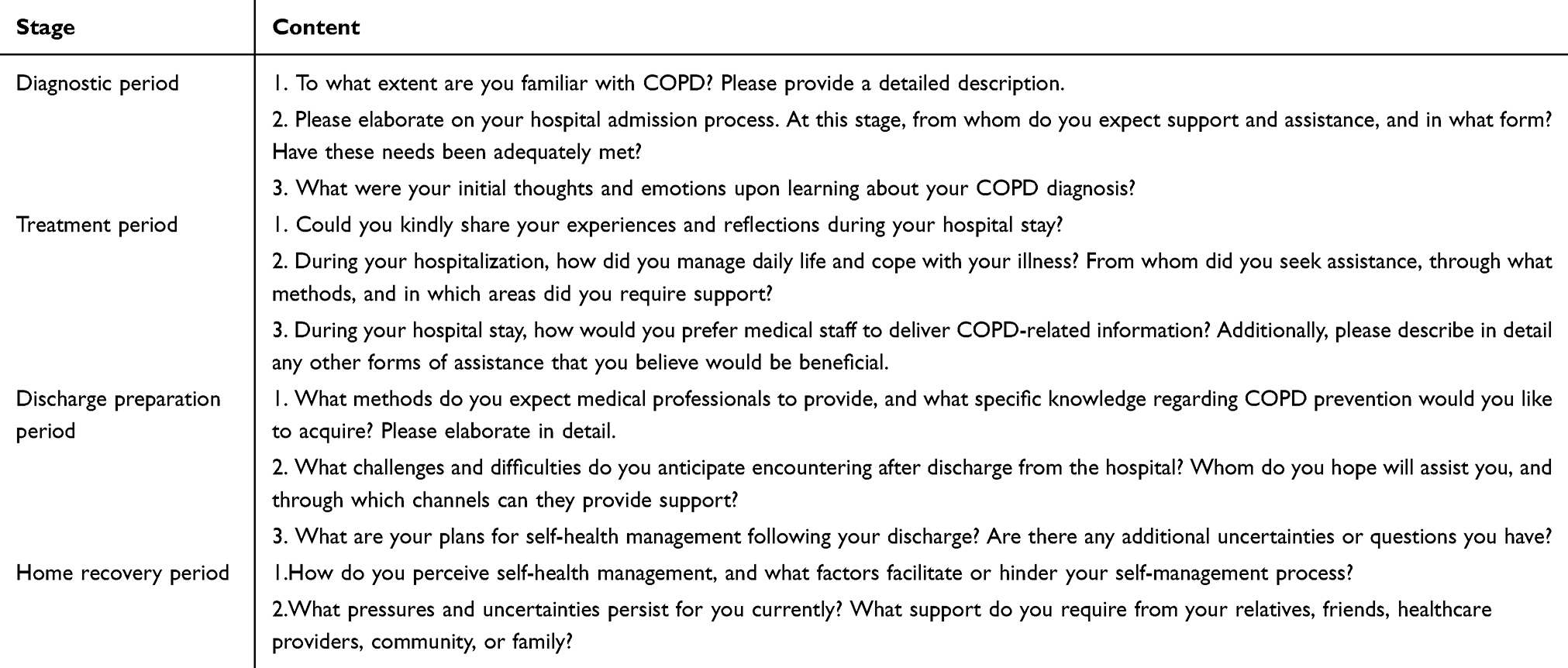 |
Table 1 Interview List |
Data Collection
Participants were categorized into four groups based on their disease diagnosis and treatment stages: 8 participants in the first group, 7 in the second, 6 in the third, and 7 in the fourth. Notably, the interviews for the first three groups were conducted face-to-face during the participants’ hospitalization, while the final group utilized telephone interviews due to the participants’ discharge. The texts from the four interview periods were labeled as A to D, with participants identified using Arabic numerals, such as A1, B1, C1, and D1. The timing and location of the interviews were determined by the participants, typically scheduled in the afternoons when treatments were less frequent; the interview locations were quiet and private teaching rooms. Prior to the interviews, Interviewer provided an explanation of the study’s purpose and significance, as well as the cooperation required from participants during the interview process (including on-site recording and the option to decline answering sensitive questions). Following this, informed consent was obtained from the participants. Each interview began with informal conversations designed to encourage participants to express themselves actively, thereby fostering a relaxed atmosphere. Throughout the interview process, changes in participants’ facial expressions, body language, and verbal responses were meticulously recorded to reveal their true feelings. The interviewer, possessing extensive experience in qualitative research, refrained from overly subjective guidance and suggestive questioning throughout the entire process, thereby maintaining a neutral stance.
Data Analysis
Data analysis was conducted using qualitative content analysis.30 The interview recordings were transcribed into text within 24 hours of the interviews. The transcriptions were reviewed and screened by two researchers. For offline interviews, participants verified the final texts for completeness and accuracy, while for online interviews, the texts were sent to participants electronically for verification. Two researchers independently performed the data analysis, followed by joint discussions. Any discrepancies identified during the analysis were submitted to a third senior researcher and the project leader for adjudication. The specific analysis process is as follows: 1) Clear data preparation; 2) Organization of language units (words, phrases, sentences, or paragraphs); 3) Classification of language units through coding; 4) Evaluation of coding consistency; 5) Extraction of results consistent with the determined themes. The data analysis process was conducted using Nvivo 12 software.
Results
Characteristics of Participants
There was no overlap among the respondents across the four stages, with the number of participants being 8, 7, 6, and 7, respectively, totaling 28 participants, comprising 18 males and 10 females. The general information regarding the respondents was presented in Table 2.
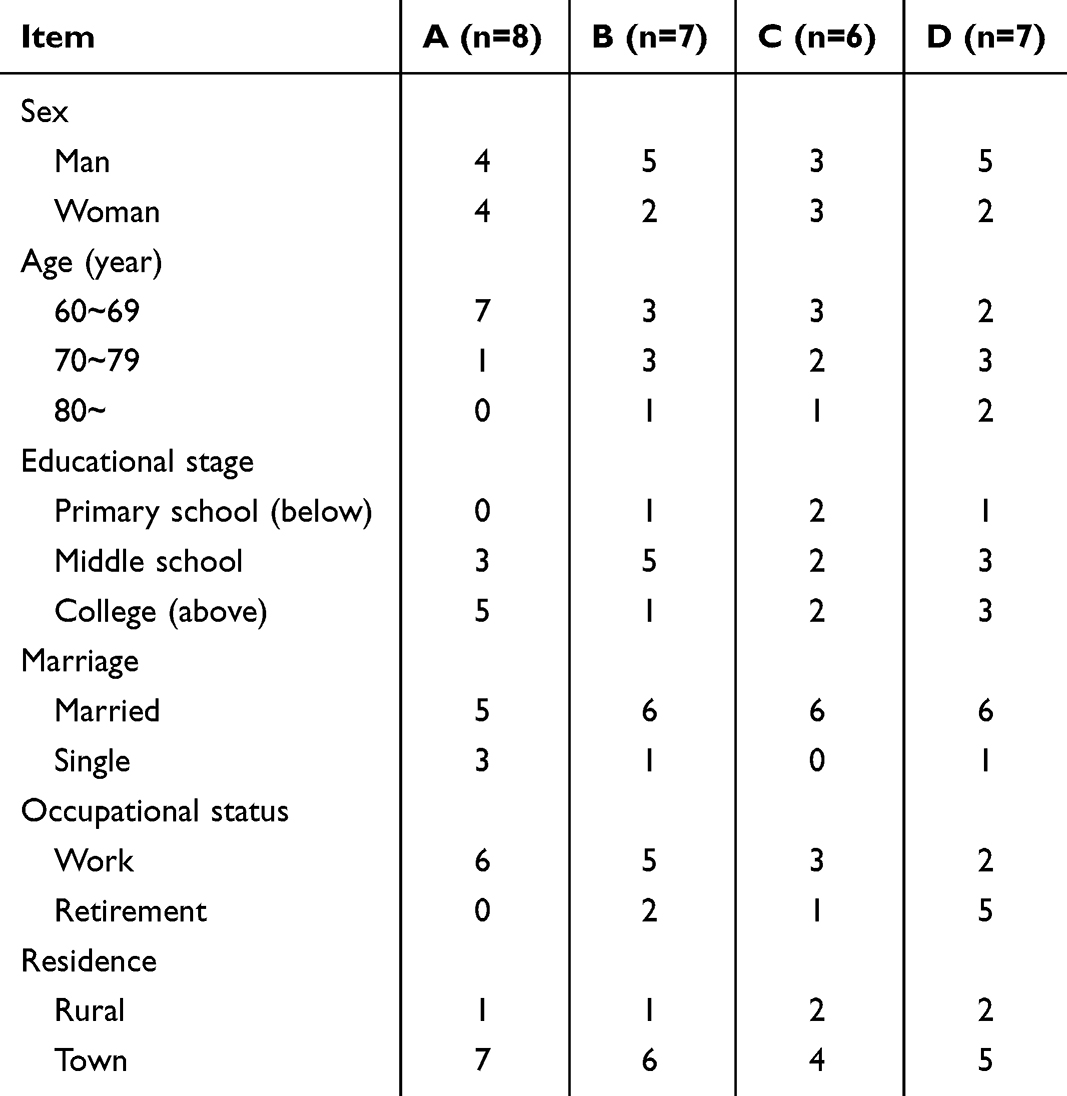 |
Table 2 Characteristics of Interviewee Information |
Theme 1: Hospitalization for Acute Exacerbation Period
Sub-Theme 1.1 Limited Ability to Acquire Disease Information
Most participants were non-medical professionals and therefore lack relevant medical knowledge. Their insufficient understanding of COPD triggers and clinical manifestations increased their uncertainty regarding the disease. After being informed about their condition, participants seek related knowledge through informal channels, such as word of mouth from relatives and friends or online resources, while simultaneously questioning the accuracy of the information they acquire.
A3:I had never heard of COPD before, and none of my relatives or friends have had it. I never thought I would get this disease (sigh).
A5:I have never heard of COPD before. Can high blood lipids also lead to COPD?
A1:The doctor said my COPD was caused by high blood lipids, so I quickly looked it up on Baidu, but I still do not understand how it could be caused, nor do I know if what it says is correct.
A8:Nurse, I have a question. My husband passed away from a chronic lung disease. Is my condition related to his?
Sub-Theme 1.2 Psychological Support
Symptoms such as dyspnea and wheezing were prominently observed. The distress caused by physical pain, coupled with cognitive biased regarding the illness, led participants to experience fluctuating emotions, including fear, anxiety, depression, and restlessness. Effective psychological counseling alleviated these emotional disturbances and enhanced patients’ overall well-being.
A6:Initially, I did not feel much after the doctor informed me of COPD diagnosis; however, upon researching it on Baidu, I was taken aback by the information I discovered.
A7:Having never encountered this illness before, my visit to the hospital filled me with immense fear. Engaging in conversations with doctors and nurses greatly alleviated my anxiety.
Sub-Theme 1.3 Change Unhealthy Lifestyles
Upon hospitalization, participants engaged in self-reflection regarding their previous unhealthy behaviors. After a thorough evaluation, many participants began to implement self-adjustments.
A4:Had I known the extent of the pain I would endure, I would have refrained from excessive alcohol consumption. Additionally, while I have enjoyed greasy foods in the past, I intend to reduce my intake moving forward.
A2:In the past, I could not eat without meat, consumed my meals hastily, had a penchant for cigarettes, and maintained an irregular daily routine. Upon reflection, I realize that my previous lifestyle was profoundly unhealthy. Now that I have been diagnosed with this illness, it is imperative that I initiate significant changes.
Theme 2 Hospitalization for Treatment and Control Period
Sub-Theme 2.1 Therapeutic Information Support
Participants expressed a desire for transparency throughout the treatment process, which allowed them to comprehend the detailed treatment plan and the rationale behind various medical measures. It was crucial for participants to receive timely and accurate information to remain informed and dynamically aware of their health status. This transparency not only enhanced compliance but also fostered shared decision-making.
B1:What I need is timely information: about my tests – their schedule, purpose, and results – and about my medications, like the reasons for taking them or changing them. And the waiting in the ward, when you are left in the dark, that’s what makes you really anxious.
B2:When I check on my phone, the test results are not updated promptly, and the morning rounds are very brief. Sometimes we forget, and the doctor has not told me about the blood test results. Also, I had a CT scan—has there been any improvement?
B4:The doctor said I need to undergo an intervention. I just want to know specifically when it will start. I have been here for several days already.
Sub-Theme 2.2 Effective and Compassionate Care
The support of healthcare professionals was crucial for participants during the diagnosis and treatment of COPD. Participants required the assistance of these professionals to receive expert guidance and advice.
B3:Those rehabilitation exercise programs and breathing techniques would have been unknown to us without the nurses’ guidance!
B5:When I arrived, I was in excruciating pain. The nurse on night rounds noticed that I could not sleep at all, so she called the doctor to administer an injection. She advised me to sit with my legs hugged for a while, and after some time, I felt much better.
B7:Providing detailed guidance on diet, breathing exercises, and medication usage, rather than relying solely on verbal instructions from nurses, would significantly enhance my overall well-being.
Theme 3 Discharge Preparation Period
Sub-Theme 3.1 Specific Health Guidance
Participants expressed that traditional educational methods hindered their mastery of health management knowledge. Participants experienced comorbidities, which led to feelings of confusion regarding future home rehabilitation. Moreover, due to the recurrent nature of COPD, participants had an urgent need to comprehend relevant preventive knowledge prior to discharge.
C1:Just now, the nurse informed me about preventing the recurrence of COPD and maintaining a light diet after returning home. She provided a lot of information, but I did not retain much of it. Nowadays, we cannot do without our phones. It would be beneficial if this information could be delivered to us through a mini-program or similar platform, as it would be more convenient for me to access. I even searched for it online the other day.
C4:As I age, my memory is not what it used to be. Once I return home, I will have to rely on my son. It would be most helpful if you could provide a specific training method, making it easier for us to follow.
Sub-Theme 3.2 A Promising Life Plan
During this phase, participants gradually resume their daily activities. To prevent the deterioration of their condition and the recurrence of COPD, they seek suitable rehabilitation plans and expect specific guidance from healthcare professionals.
C5:What should I eat and do when I return home? Can you provide more specific details?
C2:After discharge, are there any precautions I should take regarding exercise? How should I manage my activities at home?
Theme 4 Home Recovery Period
Sub-Theme 4.1 Self-Management
During the recovery phase of the illness, participants found themselves without the health guidance of medical professionals while at home. They expressed a desire to acquire more knowledge about health care practices that could enhance their immunity and prevent disease recurrence.
D2:Nurse, I still feel a bit weak, I sweat easily, and I have no energy. Some friends have recommended I take Chinese medicine. I also want to take care of myself. Do you have any recommendations?
The recurrence of COPD was associated with unhealthy lifestyle habits. Effective home care required the development of specific self-management skills, which included regular follow-up examinations and scheduled health check-ups.
D1:I understand that I should refuse cigarettes and alcohol, and that I need to maintain a healthy lifestyle, but I find it challenging to implement these changes!
Participants exhibited diverse approaches to self-health management, influenced by factors such as age, economic status, and education levels. Consequently, there was a demand for varied health management methods.
D3:If you could just send my information to the community, I would not have to travel so far for follow-up, or it would be even better if I could do the follow-up online.
Sub-Theme 4.2 Continuous Healthcare Support
After discharge, participants experienced a sense of mental relaxation due to their improved health conditions, but they might lack professional health guidance and supervision, which led to inadequate self-management abilities. To prevent readmissions, post-discharge care support was essential.
D1:Could you create a group for us COPD patients to communicate and keep each other motivated? You could also keep an eye on us and make more phone calls. After discharge, it feels like we are left unattended.
D5:Honestly, the medicine I have been taking for my cough and phlegm is not working that well. On top of that, I am left wondering, if I have side effects from the hormone drugs, who’s going to be there to help me?
Sub-Theme 4.3 Self-Discipline and External Discipline
The modification of detrimental lifestyle habits was linked to the prevention of disease. However, altering long-standing unhealthy behaviors necessitated both strong self-discipline and external support from patients.
D3:I believe the most crucial aspect is self-discipline, but it would be even better if my family members could regularly remind me.
D6:Currently, I do not pay as much attention to my lifestyle, and my family members are sometimes not as attentive as they were when I first returned home. Occasionally, I think that having a cigarette once in a while would not be so serious.
Discussion
The TIR theory was initially developed to capture the supportive needs of family members caring for stroke survivors during critical transitional phases of recovery.31 This theory posited that, over time, patients’ specific supportive needs evolved across distinct phases of illness. In this study, it was employed to investigate the health literacy needs of patients with COPD, revealing that the focus of patients’ health literacy requirements varies at different stages of the disease. The content and nature of these needs also fluctuated across various stages. Specifically, information needs transition from early-stage knowledge regarding disease awareness and treatment to later-stage requirements for detailed guidance on health management and self-care. Emotional needs were particularly pronounced during the diagnostic phase, characterized by a strong desire for professional psychological support. In the treatment phase, the emphasis shifted to the necessity for professional medical and nursing assistance, while the recovery phase highlighted the importance of self-management and guidance on self-discipline and external regulation. Therefore, comprehending the specific health literacy needs of patients at different stages of the disease will enable healthcare professionals to devise scientifically informed interventions, thereby enhancing health literacy levels.
Acute Exacerbation Period: Establishing a Foundation of Health Literacy to Effectively Respond to Acute Crises
This interview revealed that patients diagnosed with COPD exhibited a significant lack of understanding regarding their condition, hindering their ability to grasp comprehensive knowledge about the disease. Patients expressed a strong demand for information related to their illness, which aligned with the findings of Amado CA et al.32 Early fulfillment of patients’ informational needs alleviated anxiety symptoms, reduced psychological stress, diminished uncertainty regarding the disease, and enhanced treatment adherence.33 The Knowledge-Attitude-Practice Theory suggested that changes in individual behavioral motivation were primarily driven by the accumulation of knowledge. A solid understanding of relevant disease and health information fostered the development of correct and positive attitudes and beliefs, ultimately prompting individuals to modify health-damaging behaviors and actively engage in health-promoting activities.34 A profound understanding of related diseases and health information fostered the development of accurate and constructive attitudes and beliefs. This, in turn, motivated individuals to change health-damaging behaviors and participate in health-promoting activities.35 Therefore, upon diagnosis, healthcare professionals should proactively provide patients with essential knowledge about the disease and its potential clinical symptoms, thereby mitigating feelings of panic.
This study found that the acute onset and severe condition of COPD, coupled with high levels of pain, led to varying degrees of negative emotions in patients at different stages. These emotions manifested as despondency, anxiety, depression, and irritability, with more pronounced symptoms observed during the diagnostic period.36 Previous studies had indicated that effective psychological guidance could alleviate negative emotions such as depression and anxiety, enhance self-efficacy, increase compliance with treatment and care, and promote positive changes in patients’ health behaviors.37,38 Therefore, during this critical phase, medical staff should prioritize communication with patients, monitor their emotional changes, conduct psychological assessments and timely interventions, encourage patients to express their thoughts, and provide personalized psychological counseling to alleviate negative emotions. Additionally, it was essential to effectively utilize support from family members and emotional support from nurses as coping resources, thereby enhancing patients’ confidence in their treatment.
The onset and exacerbation of COPD were closely related to unhealthy lifestyle habits.39 Patients began to reassess their behaviors and express motivation to adopt healthier practices following their diagnosis. This stage presented a crucial opportunity for health education, not only to disseminate knowledge but also to cultivate practical literacy skills. Therefore, it was essential to strengthen health education during this phase. Interventions should be based on identifying barriers and facilitators to behavioral change, providing personalized, one-on-one health education.40 The methods of health education should be diverse, incorporating videos, illustrations, brochures, and other necessary resources to enhance comprehension and retention. Expanding the reach of health information through mobile platforms, such as applications, WeChat, and SMS, could further support patients in adopting healthy behaviors.41 These strategies aligned with the multidimensional perspective of health literacy, encompassing functional, interactive, and critical competencies.
Treatment and Inpatient Control Period: Cultivating Decision-Making Abilities Through Systematic Interactions
This study found that the core health literacy needs of participants in both the treatment and stable phases shifted from passive reception to active interaction and critical engagement. Participants expressed a desire to obtain treatment information and engage in shared decision-making during interviews, reflecting their developmental needs for interactive and critical health literacy. Shared decision-making was not only an ethical best practice; the process itself served as a powerful context for cultivating health literacy, as it required patients to understand, evaluate, and articulate their personal preferences.42 This finding had been consistently highlighted in cancer treatment decision research, where decision aids had been shown to effectively enhance patients’ decision readiness and satisfaction.43 At this juncture, nurses assumed a pivotal role as “health literacy mediators”, simplifying complex information through decision aid tools, akin to the strategy of using “question prompt cards” to facilitate doctor-patient communication among older inpatients.44 This study found that participants exhibited an increased demand for compassionate care, underscoring the empowering role of medical empathy in enhancing health literacy. Given the complexity of the condition, the challenges associated with treatment, the prolonged course of the disease, and the uncertainty surrounding treatment outcomes, participants encountered various stressors throughout the treatment process.45 This necessitated that healthcare providers not only enhanced the professionalism of their care but also increased their empathy to foster a sense of warmth among participants, which aligned with the findings of Vincent et al.10 Compassionate communication not only built trust but also directly alleviated the “navigation” burden on patients within complex healthcare systems. Research had confirmed that patients’ perceptions of compassion in care were positively correlated with their self-management confidence.46 The professional support and emotional empathy offered by healthcare providers acted as an essential “scaffold” for patients facing treatment pressures and systemic complexities, significantly bolstering their self-efficacy in managing illness. Establishing a supportive and communicative treatment environment was crucial to ensure that patients are both able and willing to leverage their health literacy.47 Therefore, health literacy interventions at this stage should focus on transforming the treatment environment into a supportive learning and empowerment system, enabling patients to gradually become active participants in their own health management while receiving professional care.
Discharge Preparation Period: Enhancing the Capacity to Navigate Health Transitions Between Hospital Settings and Home Environments
The discharge preparation period represents a critical transitional phase for the migration of health literacy from the hospital setting to the home environment. This study found that participants’ need for specific, personalized health guidance highlighted their difficulty in translating general medical knowledge into personal daily practices—a core challenge at the application level of health literacy.48 This challenge is not unique to COPD. Studies on discharge planning for older fracture patients have identified the lack of personalized home rehabilitation guidance as a significant risk factor for readmission.49 Therefore, healthcare professionals must reassess participants’ health behavior capabilities and lifestyles before discharge. This assessment should include identifying lifestyle and environmental factors and collaboratively developing personalized health management measures with participants to cultivate their “adaptive literacy”, which refers to the ability to adjust health behaviors according to the home environment. Furthermore, participants in this study expressed expectations for a “hopeful life plan”, indicating their desire to rebuild life goals and maintain a sense of hope despite the constraints imposed by illness. The study suggests that establishing long-term support from hospital to home positively affects patients’ access to high-quality continuous care and enhances their health management competencies.50 Digital technology plays a significant role in this process. The interviews revealed that most participants are already familiar with using communication platforms and social software to maintain close contact with healthcare providers. The application of mobile health platforms also provides seamless linkage support for remote health services, such as improving medication adherence and strengthening rehabilitation supervision.51 Effective discharge preparation entails providing patients with comprehensive self-management skills and equipping them with the necessary tools to navigate post-discharge health challenges, in addition to establishing mechanisms for sustained support to ensure a smooth transition to home care.
Home Recovery Period: Achieving Self-Management Through Ongoing Social and Technical Support
This study revealed that participants encountered challenges in self-management and exhibited a lack of self-discipline following discharge. The phenomenon of a significant decline in patient self-efficacy over time post-discharge represented a prevalent issue in the global management of chronic diseases.52 Establishing good behavioral habits and a healthy lifestyle was crucial for preventing the recurrence of COPD. Nevertheless, many patients lacked the necessary self-management skills, struggled to maintain a healthy lifestyle over time, and demonstrated poor self-discipline.53 These factors contributed to adverse behaviors, including self-discontinuation of medication, poor dietary choices, and irregular schedules.54 Traditional interventions placed excessive reliance on patients’ personal willpower (self-discipline) while overlooking the critical importance of creating a supportive environment (external discipline).55 Therefore, it was essential to enhance external supervision by constructing an intelligent management platform that integrated various health behaviors, such as medication adherence, dietary practices, and health monitoring. Additionally, lowering the threshold for health literacy through reminders, feedback, and simplified operations would improve patients’ self-management efficacy. Establishing long-term peer supervision, such as forming patient teams and family accompaniment, along with remote support mechanisms, was crucial for creating a sustainable “external discipline” and enhancing collective efficacy. Furthermore, the promotion of health literacy during the home stay period should transition from a one-way educational approach directed at individual patients to the development of an “empowerment ecosystem”.56 This ecosystem should integrate intelligent tools, social networks, and professional support to assist patients in achieving enduring autonomous health behaviors in real-world settings.57
Limitations
This study was the first to explore the specific needs of older patients with COPD from a qualitative perspective, utilizing the framework of health literacy. It analyzed these needs at crucial time points in the disease trajectory through the lens of timing theory. However, the study has certain limitations. Firstly, as a qualitative study, the findings were inevitably influenced by the researchers’ backgrounds, assumptions, and disciplinary perspectives. Although this study had implemented practices such as independent dual analysis to enhance rigor, the interpretation of data remains a subjective process. Future research should focus on expanding cross-verification of results among team members to further strengthen the credibility of the findings. Secondly, this study conducted interviews with patients at various stages, guided by the TIR theory. While it effectively captured the health literacy needs of patients throughout an extended treatment cycle, it was important to note that the progression of COPD was not always linear, and patients’ subjective experiences might not fully correspond with these stages. For example, even post-discharge, patients might continued to experience significant impacts on their health. This study was not have completely addressed these inconsistencies. Future research should consider incorporating patient-reported outcome measures alongside clinical staging to bridge this gap and provide a more comprehensive understanding. Lastly, given the necessity for long-term care among older patients with COPD, subsequent studies could enhance findings by including interviews with nurses, caregivers, and other relevant stakeholders.
Conclusion
The health literacy needs of older patients with COPD exhibit phase-specific characteristics. During the acute phase, patients demonstrate significant information and emotional needs; in the treatment phase, they require professional support; and post-discharge, their focus shifts to self-management. It is recommended that health literacy interventions be tailored to address the predominant needs of each phase. These programs should provide adequate emotional support, promote patient empowerment and shared decision-making, ensure professional nursing support, and establish remote management and behavior monitoring to reinforce patients’ health behaviors.
Abbreviations
COPD, chronic obstructive pulmonary disease; COREQ, Consolidated criteria for reporting qualitative research; TIR, Timing It Right.
Data Sharing Statement
The data generated and analyzed during the study are not publicly accessible due to ethical considerations and privacy concerns.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki. We affirm that all methods were implemented in compliance with the relevant guidelines and regulations. The research received approval from the Medical Ethics Committee of Shanghai Chest Hospital. Participants were informed about the study, and it was emphasized that their participation was entirely voluntary; they could withdraw from the study at any time without consequence. Subsequently, written informed consent was obtained from all participants. All participants provided informed consent, agreeing to the use of their research data for scientific purposes and the publication of research anonymized responses/direct quotes.
Acknowledgments
We would like to express our heartfelt appreciation to all the patients and nurses who participated in this study for their invaluable contributions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Fundamental Research Funds for the Central Universities (project number YG2021QN130).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
2. Global Strategy for Prevention, Diagnosis and Management of COPD: 2022 Report [EB/OL]. 2022. Available from: https://goldcopd.org/2022-gold-reports-2/.
3. Labaki WW, Rosenberg SR. Chronic obstructive pulmonary disease. Ann Intern Med. 2020;173(3):ITC17–ITC32. doi:10.7326/AITC202008040
4. Lewthwaite H, Williams G, Baldock KL, Williams MT. Systematic review of pain in clinical practice guidelines for management of COPD: a case for including chronic pain? Healthcare. 2019;7(1):15. doi:10.3390/healthcare7010015
5. Tanaka T, Okita M, Jenkins S, Kozu R. Clinical and psychological impact of chronic pain in people with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2022;17:893–903. doi:10.2147/COPD.S359223
6. Clarke SY, Williams MT, Johnston KN, Lee AL. The prevalence and assessment of pain and dyspnoea in acute exacerbations of COPD: a systematic review. Chron Respir Dis. 2022;19:14799731221105518. doi:10.1177/14799731221105518
7. Roberts MH, Mapel DW, Thomson HN. The impact of chronic pain on direct medical utilization and costs in chronic obstructive pulmonary disease. Clinicoecon Outcomes Res. 2015;7:173–184. doi:10.2147/CEOR.S80424
8. Lee AL, Harrison SL, Goldstein RS, Brooks D. Pain and its clinical associations in individuals with COPD: a systematic review. Chest. 2015;147(5):1246–1258. doi:10.1378/chest.14-2690
9. Bentsen SB, Miaskowski C, Cooper BA, et al. Distinct pain profiles in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2018;13:801–811. doi:10.2147/COPD.S150114
10. Xu Q, Wu K, Yang Y, et al. Association between sleep quality and pain intensity in mild patients with COPD: a community study. J Pain Res. 2021;14:2641–2649. doi:10.2147/JPR.S310036
11. Andenæs R, Momyr A, Brekke I. Reporting of pain by people with chronic obstructive pulmonary disease (COPD): comparative results from the HUNT3 population-based survey. BMC Public Health. 2018;18(1):181. doi:10.1186/s12889-018-5094-5
12. Born CDC, Bhadra R, D’Souza G, et al. Combined lifestyle interventions in the prevention and management of asthma and COPD: a systematic review. Nutrients. 2024;16(10):1515. doi:10.3390/nu16101515
13. World Health Organization (WHO): health literacy, the solid facts. 2013. Available from: http://www.euro.who.int/__data/assets/pdf_file/0008/190655/e96854.pdf.
14. Adams RJ, Stocks NP, Wilson DH, et al. Health literacy--a new concept for general practice? Aust Fam Physician. 2009;38(3):144–147.
15. Pang Y, Kartsonaki C, Turnbull I, et al. Metabolic and lifestyle risk factors for acute pancreatitis in Chinese adults: a prospective cohort study of 0.5 million people. PLoS Med. 2018;15(8):e1002618. doi:10.1371/journal.pmed.1002618
16. Poureslami I, FitzGerald JM, Tregobov N, Goldstein RS, Lougheed MD, Gupta S. Health literacy in asthma and chronic obstructive pulmonary disease (COPD) care: a narrative review and future directions. Respir Res. 2022;23(1):361. doi:10.1186/s12931-022-02290-5
17. Lundell S, Pesola UM, Nyberg A, Wadell K. Groping around in the dark for adequate COPD management: a qualitative study on experiences in long-term care. BMC Health Serv Res. 2020;20(1):1025. doi:10.1186/s12913-020-05875-2
18. Frings D, Sykes S, Ojo A, et al. Differences in digital health literacy and future anxiety between health care and other university students in England during the COVID-19 pandemic. BMC Public Health. 2022;22(1):658. doi:10.1186/s12889-022-13087-y
19. Liu YB, Liu L, Li YF, Chen YL. Relationship between health literacy, health-related behaviors and health status: a survey of elderly Chinese. Int J Environ Res Public Health. 2015;12(8):9714–9725. doi:10.3390/ijerph120809714
20. Munigala S, Gardner TB, O’Reilly EM, et al. Understanding pancreatic diseases using animated pancreas patient: informing patients for better health outcomes with visual formats of learning. Pancreas. 2018;47(10):1256–1261. doi:10.1097/MPA.0000000000001178
21. Phillips AE, Faghih M, Drewes AM, et al. Psychiatric comorbidity in patients with chronic pancreatitis associates with pain and reduced quality of life. Am J Gastroenterol. 2020;115(12):2077–2085. doi:10.14309/ajg.0000000000000782
22. Cameron JI, Gignac MA. “Timing It Right”: a conceptual framework for addressing the support needs of family caregivers to stroke survivors from the hospital to the home. Patient Educ Couns. 2008;70(3):305–314. doi:10.1016/j.pec.2007.10.020
23. Lee CM, Herridge MS, Matte A, Cameron JI. Education and support needs during recovery in acute respiratory distress syndrome survivors. Crit Care. 2009;13(5):R153. doi:10.1186/cc8053
24. Ramsay P, Huby G, Rattray J, Salisbury LG, Walsh TS, Kean S. A longitudinal qualitative exploration of healthcare and informal support needs among survivors of critical illness: the RELINQUISH protocol. BMJ Open. 2012;2(4):e001507. doi:10.1136/bmjopen-2012-001507
25. Simon MA, Li Y, Dong X. Levels of health literacy in a community-dwelling population of Chinese older adults. J Gerontol a Biol Sci Med Sci. 2014;69(Suppl 2):S54–S60. doi:10.1093/gerona/glu179
26. Li Y, Li C, Zhou N, et al. Perspectives of nurses and patients on the misplacement of supportive care information for type 2 diabetes mellitus: a qualitative study in China. BMC Nurs. 2025;24(1):123. doi:10.1186/s12912-025-02783-w
27. Zhou H, Wang X, Du R, et al. The work experience of newly recruited male nurses during COVID-19: a qualitative study. Asian Nurs Res. 2021;15(3):203–209. doi:10.1016/j.anr.2021.05.001
28. Bradshaw C, Atkinson S, Doody O. Employing a qualitative description approach in health care research. Glob Qual Nurs Res. 2017;4:2333393617742282. doi:10.1177/2333393617742282
29. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
30. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. doi:10.1016/j.nedt.2003.10.001
31. Su X, Ma S, Yang X, Zhang C, Chen W. Health literacy needs of acute pancreatitis patients during the diagnosis and treatment process under the lens of the timing it right theory: a qualitative study. Patient Prefer Adherence. 2024;18:507–517. doi:10.2147/PPA.S444955
32. Amado CA, Pérez-García C, Tamayo Fernández B, Agüero-Calvo J, Muñoz-Cacho P, Golpe R. Information needs in COPD after an educational programme: influence in exacerbations and admissions. Int J Chron Obstruct Pulmon Dis. 2020;15:2663–2671. doi:10.2147/COPD.S275002
33. Schrijver J, Lenferink A, Brusse-Keizer M, et al. Self-management interventions for people with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2022;1(1):CD002990. doi:10.1002/14651858.CD002990.pub4
34. Qutob RA, Alaryni A, Alammari Y, et al. Knowledge, attitudes, and practices of healthcare providers towards advance directive for COPD patients in Riyadh, Saudi Arabia. Healthcare. 2025;13(7):771. doi:10.3390/healthcare13070771
35. Ghalavand H, Nabiolahi A, Panahi S. Health literacy and motivation to change health behavior among cardiovascular patients. BMC Cardiovasc Disord. 2025;25(1):479. doi:10.1186/s12872-025-04936-w
36. MacLeod M, Papi A, Contoli M, et al. Chronic obstructive pulmonary disease exacerbation fundamentals: diagnosis, treatment, prevention and disease impact. Respirology. 2021;26(6):532–551. doi:10.1111/resp.14041
37. Taylor SJC, Sohanpal R, Steed L, et al. Tailored psychological intervention for anxiety or depression in COPD (TANDEM): a randomised controlled trial. Eur Respir J. 2023;62(5):2300432. doi:10.1183/13993003.00432-2023
38. Volpato E, Farver-Vestergaard I, Brighton LJ, et al. Nonpharmacological management of psychological distress in people with COPD. Eur Respir Rev. 2023;32(167):220170. doi:10.1183/16000617.0170-2022
39. Tokgöz Akyıl F, Tural Önür S, Sökücü S, et al. Lifestyle changes and exacerbation frequency of COPD in times of the pandemic. Turk Thorac J. 2022;23(3):210–217. doi:10.5152/TurkThoracJ.2022.21165
40. Hansen TS, Poulsen I, Nørholm V, Loft MI, Jensen PS. Nutritional support and physical activity intervention programs with a person-centred approach in people with chronic obstructive pulmonary disease: a scoping review. Int J Chron Obstruct Pulmon Dis. 2024;19:2193–2216. doi:10.2147/COPD.S458289
41. Zhou L, Song C, Xu W, Wang R, Zhang W. WeChat-assisted strategies for personalized health management in patients with AECOPD: a randomized controlled trial. PLoS One. 2025;20(8):e0330673. doi:10.1371/journal.pone.0330673
42. Barradell AC, Bourne C, Alkhathlan B, Larkin M, Singh SJ. A qualitative assessment of the pulmonary rehabilitation decision-making needs of patients living with COPD. NPJ Prim Care Respir Med. 2022;32(1):23. doi:10.1038/s41533-022-00285-9
43. Jiang Y, Nuerdawulieti B, Chen Z, et al. Effectiveness of patient decision aid supported shared decision-making intervention in in-person and virtual hybrid pulmonary rehabilitation in older adults with chronic obstructive pulmonary disease: a pilot randomized controlled trial. J Telemed Telecare. 2024;30(10):1532–1542. doi:10.1177/1357633X231156631
44. Padilha JM, Sousa PAF, Pereira FMS. Nursing clinical practice changes to improve self-management in chronic obstructive pulmonary disease. Int Nurs Rev. 2018;65(1):122–130. doi:10.1111/inr.12366
45. Tian X, Yi L, Liu X, et al. Relationship between social support, symptom burden, dyspnea, perceived stress, perceived stigma, coping styles, and psychological distress in patients with stable COPD: a structural equation model. Int J Chron Obstruct Pulmon Dis. 2025;20:2183–2198. doi:10.2147/COPD.S521786
46. Gerber Z, Davidovics Z, Anaki D. The relationship between self-compassion, concern for others, and parental burnout in child’s chronic care management. Mindfulness. 2021;12(12):2920–2928. doi:10.1007/s12671-021-01752-z
47. Phillips TM, Moloney C, Sneath E, et al. Associated factors, assessment, management, and outcomes of patients who present to the emergency department for acute exacerbation of chronic obstructive pulmonary disease: a scoping review. Respir Med. 2022;193:106747. doi:10.1016/j.rmed.2022.106747
48. Corcoran R, Moore Z, Avsar P, et al. Home-based management on hospital re-admission rates in COPD patients: a systematic review. J Adv Nurs. 2024;80(10):3955–3964. doi:10.1111/jan.16168
49. Suominen TH, Edgren J, Salpakoski A, et al. Effects of a home-based physical rehabilitation program on tibial bone structure, density, and strength after hip fracture: a secondary analysis of a randomized controlled trial. JBMR Plus. 2019;3(6):e10175. doi:10.1002/jbm4.10175
50. Lee JA, Choi M, Lee SA, Jiang N. Effective behavioral intervention strategies using mobile health applications for chronic disease management: a systematic review. BMC Med Inform Decis Mak. 2018;18(1):12. doi:10.1186/s12911-018-0591-0
51. Knight-Davidson P, Meshe OF, Jenkins TO, et al. Acceptability of a digital pulmonary rehabilitation app as an adjunct or alternative to usual care for people with chronic lung diseases: a qualitative study of patients’ views and experiences. Chron Respir Dis. 2025;22:14799731251365632. doi:10.1177/14799731251365632
52. Hess Engström A, Flink M, Lindblom S, von Koch L, Ytterberg C. Association between general self-efficacy and health literacy among stroke survivors 1-year post-discharge: a cross-sectional study. Sci Rep. 2024;14(1):7308. doi:10.1038/s41598-024-57738-z
53. Sigurgeirsdottir J, Halldorsdottir S, Arnardottir RH, Gudmundsson G, Bjornsson EH. COPD patients’ experiences, self-reported needs, and needs-driven strategies to cope with self-management. Int J Chron Obstruct Pulmon Dis. 2019;14:1033–1043. doi:10.2147/COPD.S201068
54. Dineen-Griffin S, Garcia-Cardenas V, Williams K, Benrimoj SI. Helping patients help themselves: a systematic review of self-management support strategies in primary health care practice. PLoS One. 2019;14(8):e0220116. doi:10.1371/journal.pone.0220116
55. Al-Homoud M. Older adult supportive environment at home-a case study in Jordan: overall sense of control associated with home modification. Front Public Health. 2024;12:1329315. doi:10.3389/fpubh.2024.1329315
56. Zhang L, Maitinuer A, Lian Z, et al. Home based pulmonary tele-rehabilitation under telemedicine system for COPD: a cohort study. BMC Pulm Med. 2022;22(1):284. doi:10.1186/s12890-022-02077-w
57. Cruz J, Brooks D, Marques A. Home telemonitoring in COPD: a systematic review of methodologies and patients’ adherence. Int J Med Inform. 2014;83(4):249–263. doi:10.1016/j.ijmedinf.2014.01.008
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.