Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Exploring COPD Participants’ Experiences in a Comprehensive Telewellness Program within a Mixed-Disability Cohort: A Qualitative Study
Authors Arora P, Bhatt SP ![]() , Rimmer JH
, Rimmer JH
Received 26 January 2026
Accepted for publication 7 May 2026
Published 29 May 2026 Volume 2026:21 592692
DOI https://doi.org/10.2147/COPD.S592692
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Pooja Arora,1 Surya P Bhatt,2 James H Rimmer3
1Department of Physical Therapy, School of Health Professions, University of Alabama at Birmingham, Birmingham, AL, USA; 2Division of Pulmonary, Allergy and Critical Care Medicine, University of Alabama at Birmingham, Birmingham, AL, USA; 3School of Health Professions, University of Alabama at Birmingham, Birmingham, AL, USA
Correspondence: Pooja Arora, Department of Physical Therapy, School of Health Professions, University of Alabama at Birmingham, Birmingham, AL, USA, Email [email protected]
Background: Telehealth pulmonary rehabilitation (PR) has expanded access to rehabilitation services for individuals with Chronic Obstructive Pulmonary Disease (COPD); however, participation and adherence remain variable. COPD management emphasizes patient-centered approaches that address heterogeneity of this condition. Although telehealth PR has improved access to care, there is a need to better understand how broader telewellness programs can support patient-centered care and improve patient engagement.
Objective: This study aimed to explore how individuals with COPD perceive changes in their physical and psychological health after participation in a generic, group-based telewellness (MENTOR: mindfulness, exercise and nutrition to optimize resilience) program. It further examined how personal and contextual factors influence engagement by identifying barriers and facilitators across five domains (built environment and community context, service delivery, instructional strategies, equipment and technology use, and policy factors) as per Guidelines, Recommendations, and Adaptations Including Disability (GRAIDs) framework. Additionally, we explored the recommendations for enhancing telewellness models for individuals with COPD.
Methods: In-depth semi-structured interviews were conducted with participants (n=15) who completed the program. Transcripts were analyzed using Braun and Clarke’s six-step thematic analysis.
Results: Twelve primary themes were identified. Participants reported improvements in motivation, confidence in physical activity, emotional regulation, and nutrition awareness. The group-based format reduced isolation and fostered peer support. Program engagement was influenced by symptom burden, comorbidities, home environment, social support, and digital literacy. Participants valued supportive instructors, multimodal instructions (verbal, visual, written summaries, live demonstrations), adaptive exercise program, a user-friendly telehealth platform, and program’s holistic nature. Participants emphasized the need for tailored nutrition guidance, technical training for telehealth platform and equipment use, and long-term access to program resources.
Conclusion: A generic, 8-week telewellness program designed for individuals with mobility limitations was acceptable and beneficial for individuals with COPD.
Keywords: chronic obstructive lung disease, COPD, telewellness
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous respiratory condition1 and a leading cause of disability and mortality worldwide, affecting an estimated 400 million individuals globally and approximately 16 million adults in the United States.2 In 2020, COPD prevalence among adults aged 40 years and older was 10.6%.3,4 Beyond respiratory impairment, it is associated with multiple comorbidities, including muscle wasting, poor nutrition, anxiety, depression, and social isolation, all of which contribute to reduced exercise tolerance and diminished quality of life.5–8 A defining feature of COPD is variability in symptoms due to acute exacerbations and disease progression, frequent hospitalizations and multiple comorbidities.9 Given this complexity, COPD management has shifted from traditional single-disease approach toward more personalized, lifestyle-oriented approach that extends beyond symptom management to address broader determinants of health and well-being.10,11 These approaches emphasize self-management to support symptom control, promote accountability, and encourage engagement in healthy lifestyle behaviors.9
Pulmonary rehabilitation (PR), which integrates exercise training, education, and behavior change, is a cornerstone of COPD management.12,13 However, traditional PR programs often prioritize exercise training and insufficiently address other modifiable lifestyle-related risk factors such as physical activity, nutrition, mental health and social participation.14 Furthermore, access to center based PR remains limited due to factors such as poor access, transportation challenges, cost, mobility limitations and lack of perceived benefits of the program and motivation.15
Telehealth PR has emerged as a promising alternative to improve access, particularly following the pandemic; however, participation and adherence remain inconsistent.16 While existing literature has focused on the clinical effectiveness and delivery models of telehealth interventions, there is a need to better understand patient perspectives on telehealth programs, particularly how individuals perceive changes in their health and factors influencing their engagement.17
Individuals with COPD often live with multiple comorbidities that can significantly interfere with their daily functioning. As the disease progresses, these challenges tend to become more pronounced, increasing the risk of disability.18,19 Therefore, programs that address not only disease-specific limitations but also accounting for broader functional challenges such as mobility limitations,20 balance deficits and increased fall risk,21,22 pain,23,24 fatigue,25 sleep disturbance,26 memory and cognitive impairment27 and social isolation28 while incorporating an integrated focus on self-management may provide more comprehensive and meaningful support for individuals ageing with COPD.29 Existing literature identified barriers to engagement in physical activity and effective self-management such as lack of motivation, limited understanding of medication use and benefits, limited access to healthcare providers, memory challenges and lack of adequate guidance, open spaces affected by weather conditions, comorbidities and obesity.30–33
These barriers highlight a need for supportive, accessible and user-friendly interventions. Emerging evidence suggests that involving patients, caregivers, and other stakeholders in the design of interventions through co-design approaches can enhance their relevance, acceptability, and sustainability.34 The co-design approaches facilitate the identification of specific barriers and user needs. Frameworks such as the Guidelines, Recommendations, and Adaptations Including Disability (GRAIDs) provide a structured method to operationalize these insights by guiding adaptations across domains including the built environment, service delivery, instructional strategies, equipment and technology use, and policy factors. Together, co-design and structured adaptation frameworks support the development of interventions that are both patient-centered and responsive to diverse functional and environmental needs.34,35
Most rehabilitation programs are condition-specific, which may limit accessibility and inclusivity for individuals with diverse needs. In addition, current telehealth PR programs often remain limited in scope, with insufficient integration of holistic components such as mindfulness and nutrition, despite their potential role in supporting behavior change and overall well-being. These limitations may restrict the ability of telehealth PR to fully address the multidimensional needs of individuals with COPD.16
To overcome these challenges, more generic programs that are not disease specific but instead target common challenges experienced by individuals with COPD may offer a practical alternative. Such approaches have the potential to improve accessibility, particularly for those who are unable to participate in telehealth PR. For example, Bates et al, evaluated a generic, 6 month, home-based exercise program for older adults and demonstrated significant improvements in balance at both 3 and 6 months among participants with COPD, along with high acceptability and strong recommendation rates (83%).36
Mixed-disability, group-based programs comprising individuals with COPD and other diagnoses may further enhance acceptability by reducing eligibility barriers, fostering peer support, and broadening access to program components and other shared resources. Programs that emphasize holistic wellness, such as comprehensive telewellness programs integrating exercise, mindfulness, nutrition, and health coaching have demonstrated improvements in physical and psychological outcomes among individuals with mobility limitations37,38 and can be further explored in COPD populations. Additionally, structured adaptation approaches such as GRAIDs support the identification of implementation-related challenges and facilitate the development of more accessible and inclusive interventions for individuals with COPD.35
To address these gaps, this qualitative study explores the perceptions and lived experiences of individuals with COPD who participated in an 8 week, generic, group-based telewellness program originally designed for individuals with mobility limitations. This program integrates exercise, nutrition, mindfulness, and health coaching delivered through synchronous group sessions. This study examined participants’ perceptions as well as barriers and facilitators to participation across multiple domains, including the built environment and community context, service delivery, instructional strategies, equipment and technology and policy factors (Definitions of these domains are provided in Supplement 1).
This analysis is informed by the Guidelines, Recommendations, Adaptations Including Disability (GRAIDs) framework, which offers guidance for adapting programs for individuals with disabilities by identifying design and implementation-related challenges.35 Community context was considered alongside the built environment as both may influence participation in online programs.
This study is guided by the following research questions:
- How do individuals with COPD perceive their physical and psychological health, and do these perceptions change after participating in a telewellness program delivered in a group-based format for individuals with mobility limitations (eg, neurological and orthopedic conditions)?
- What challenges do individuals with COPD face while engaging in program sessions (exercise training, mindfulness, nutrition education, and health coaching), including factors related to the built environment and community contexts, service delivery, instructional strategies, use of technology and equipment and policy?
- What facilitators or enablers support participation in the program sessions, and which specific aspects of the built environment and community contexts, service delivery, instructional strategies, use of technology and equipment and policy enhance their engagement with the program components?
- What recommendations and suggestions do individuals with COPD provide to improve the design of telewellness programs to better support their physical and psychological health?
The findings aim to inform the development of more inclusive, patient-centered telewellness models that address the multidimensional needs of individuals living with COPD and support their long-term engagement with health promoting behaviors.
Methods
Study Design
This study used a phenomenological qualitative approach with semi-structured in-depth interviews to explore the lived experiences of individuals with COPD participating in a telewellness program. The program comprised 5 hours per week for 8 weeks of synchronous, group-based sessions including exercise, mindfulness, nutrition, and health coaching, delivered via the HIPAA-compliant platform, ie, HEALTHIE, which supported videoconferencing, educational resources, and secure messaging with instructors (Refer to Supplement 2 for program details). Previous discussion of the program can also be found in the published literature.37–39
In line with Creswell and Poth (2023), a phenomenological approach was appropriate as it emphasizes participants’ stories and how they experience a shared phenomenon within specific contexts.40 A semi-structured interview guide was developed to explore participants’ perceptions and experiences of participating in telewellness program alongside individuals with other types of mobility limitations. Interview questions were designed to specifically probe aspects of the built environment and community contexts, service delivery, instructional strategies, technology and equipment and policy.35
Setting
This study was conducted in collaboration with the National Center on Health, Physical Activity and Disability (NCHPAD), Birmingham, Alabama, and the Division of Pulmonary, Allergy and Critical Care, University of Alabama at Birmingham (UAB), Birmingham, Alabama.
Participants and Sampling
A total of 15 participants were recruited using purposive sampling from a pool of participants who had completed the 8-week program. Recruitment continued until data saturation was reached, defined as the point at which no new topics emerged, and similar issues were repeatedly described across interviews. A recent systematic review reported that studies using a homogenous sample usually reach data saturation with 9–17 participants.41 Fifteen individuals with COPD who met the following eligibility criteria were enrolled: (1) physician-diagnosed COPD with FEV1/FVC ≤ 0.7; (2) willingness to participate in the interview.
The University of Alabama at Birmingham Institutional Review Board provided the approval to conduct this qualitative study (IRB-300012556). This study complies with the Declaration of Helsinki. An informed consent was obtained from all participants for the publication of their deidentified demographic and clinical data for research purpose. The informed consent also included publication of anonymized responses/direct quotes. Table 1 lists the participants characteristics.
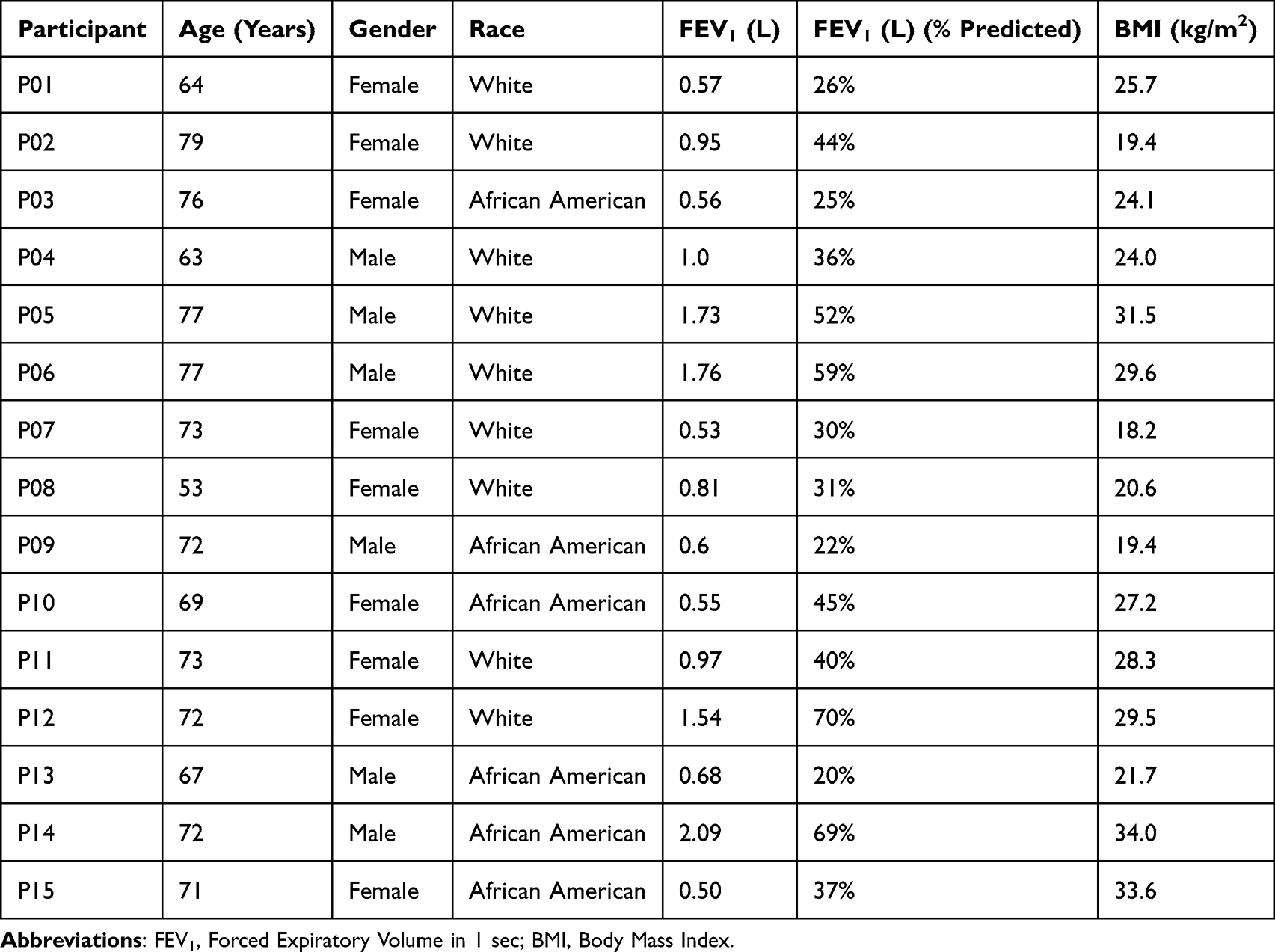 |
Table 1 Participants’ Demographic and Clinical Profiles |
Data Collection
All interviews were conducted via a HIPAA-compliant ZOOM platform, lasting 30–45 minutes, audio-recorded, and transcribed verbatim in English. The researcher took notes and created a summary after each session. All data was de-identified, stored securely in the cloud, and shared with co-researchers via encrypted files to ensure privacy and confidentiality. Participants were de-identified in all transcripts and reports using unique participant identification codes (P01–P15).
Data Analysis
Data were analyzed by two coders using Braun and Clarke’s reflexive thematic analysis, which emphasizes the researchers’ active role in knowledge construction and reflection throughout the process.42 Following six stages, audio recordings and interview notes were first transcribed and repeatedly read to gain familiarity. Initial codes were then generated systematically, followed by the development of potential themes. Themes and codes were reviewed to ensure alignment with the research questions, refined in terms of scope and meaning, and finally, findings were reported. This approach acknowledges how researchers’ perspectives shape theme development and interpretation.
Rigor/Quality of Study
The trustworthiness of this study was ensured by addressing credibility, dependability, transferability, and confirmability.
Credibility
To establish credibility, the researchers carefully examined each transcript, evaluating similarities and differences within each participant’s responses and across all participants. Each interview transcript was analyzed multiple times and inductively reduced to codes. Codes that are conceptually similar or related were then organized into categories. The established codes and categories were then re-examined by researchers experienced in qualitative methods. We also employed triangulation by reviewing and cross-checking the transcribed interviews with written notes taken during the interviews. Two researchers independently analyzed the data and compared their findings to establish an intercoder agreement.40,43
Dependability
Dependability was supported by providing a detailed description of the study purpose, recruitment strategy, data collection procedures, analysis process and research findings, as well as interpretations and discussion. This documentation allows readers to follow the methodological decisions made throughout the study.
Transferability
Transferability was facilitated by reporting participants’ demographic characteristics, study setting, and key details of the online lifestyle wellness program. This contextual information enables readers to evaluate the extent to which the findings may be applicable to other settings or populations.
Confirmability
Confirmability was enhanced through member checking. After the interviews, participants were contacted and invited to review and verify the interviewer’s summary of their experiences to ensure that the interpretations accurately reflected their perspectives.
Results
The mean age (n=15) was 70 ± 6 years, 9 participants were females (60%), the mean FEV1 (% predicted) was 40 ± 0.16.
Twelve themes emerged and were further organized into three overarching categories: (1) personal factors (Table 2), encompassing health beliefs, evolving perceptions of disease over time, and perceived benefits of the online lifestyle wellness program; (2) contextual factors (Table 3), reflecting participants’ experiences of participating in the telewellness program within their built and community environments, including experiences related to service delivery, instruction, equipment/technology, and policy (3) Participants’ recommendations (Table 4).
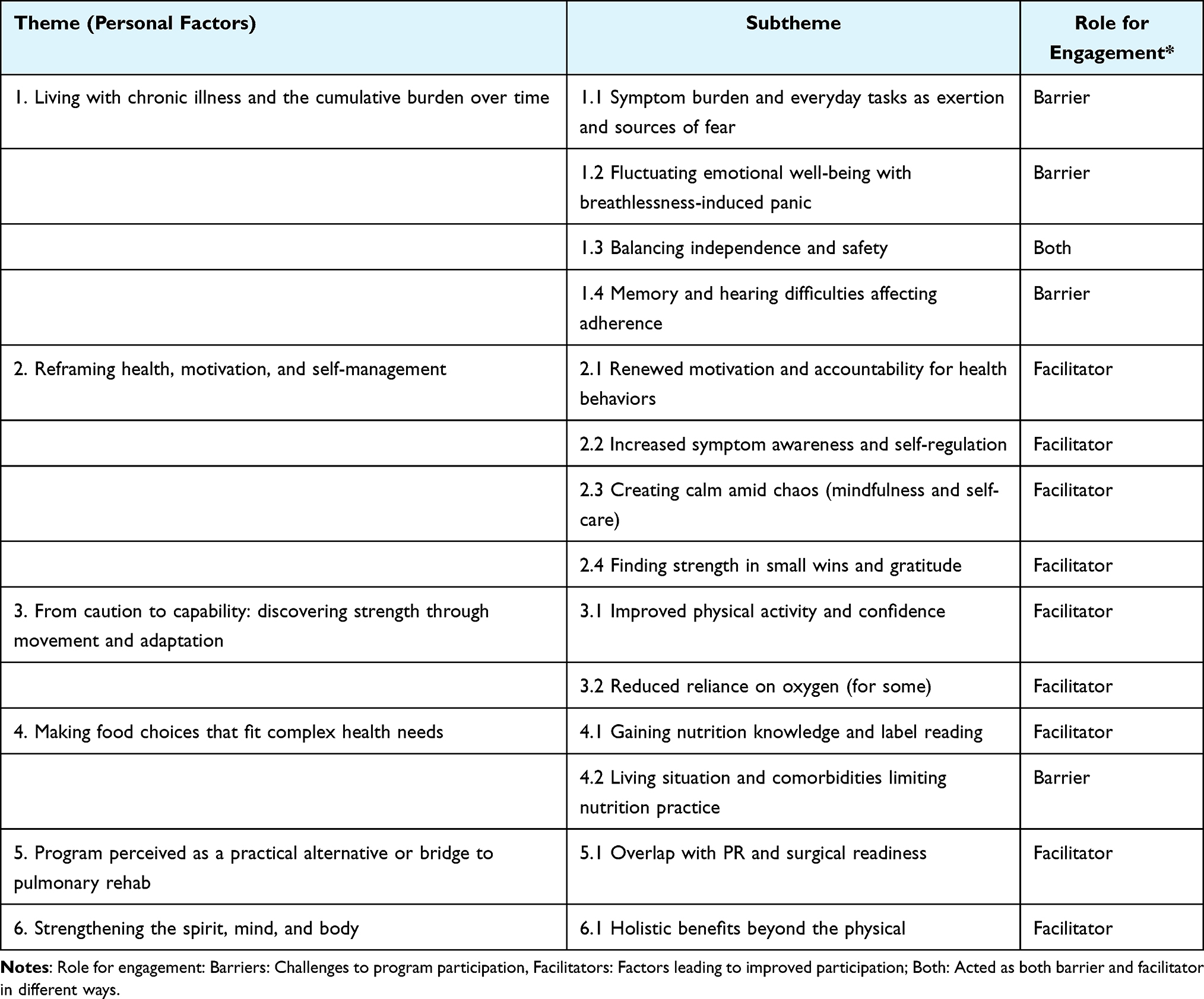 |
Table 2 Personal Factors: Health Beliefs, Changing Perceptions Over Time, Perceived Barriers and Benefits of the Telewellness Program |
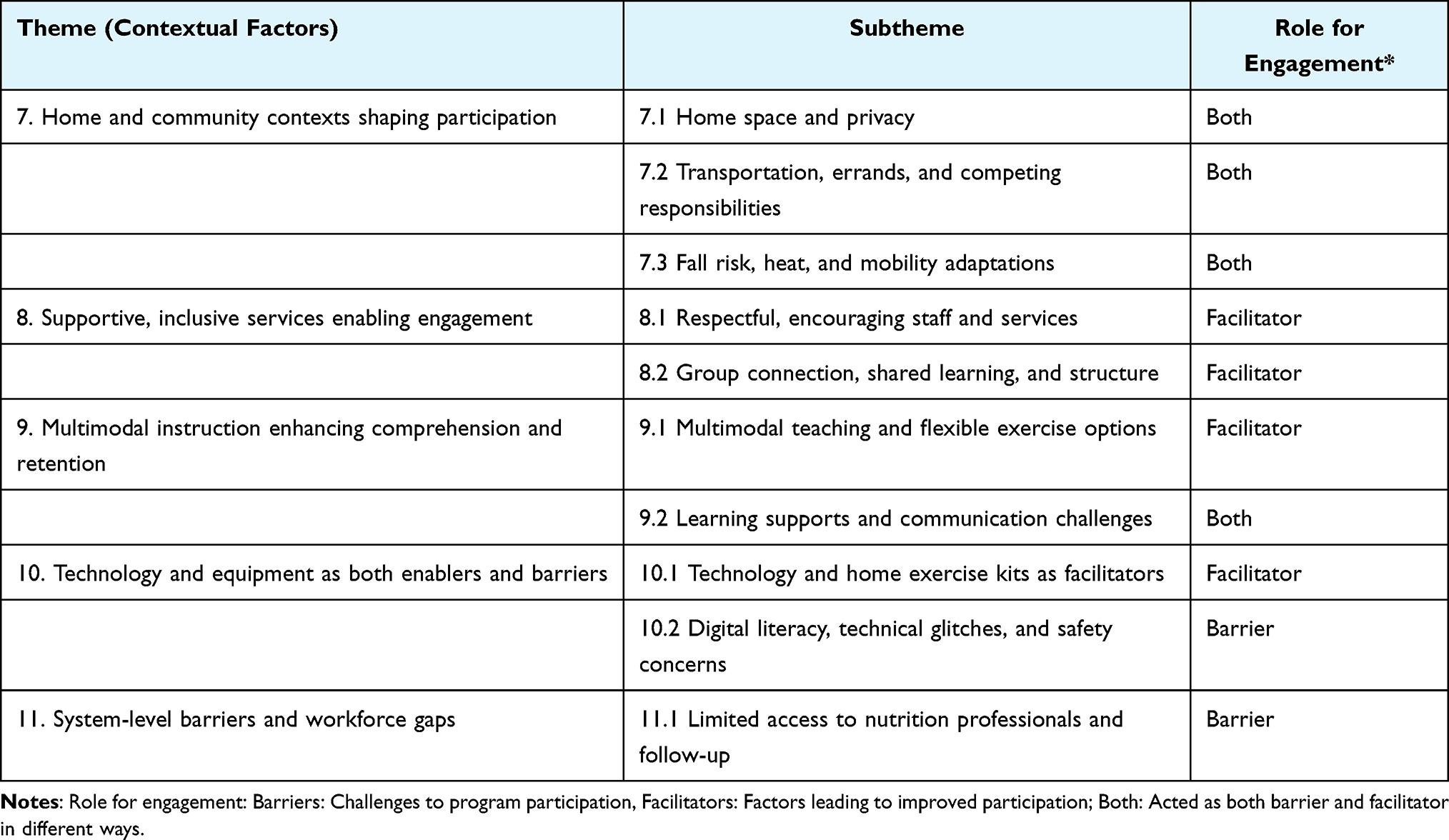 |
Table 3 Contextual Factors: Participants’ Experiences of Participating in Telewellness Program |
 |
Table 4 Participants’ Recommendations for Future COPD-Tailored Telewellness Programs |
Themes and Subthemes (Table 2)
Living with Chronic Illness and the Cumulative Burden Over Time
Participants described living with COPD and its co-existing conditions as a continuous, exhausting effort to manage symptoms and accomplish basic activities of daily living.
Subtheme Symptom Burden and Everyday Tasks as Exertion and Sources of Fear
Participants described symptom burden as pervasive, with routine activities such as showering, cooking, gardening, or moving around the house experienced as exertional tasks that could quickly provoke breathlessness and fatigue. As P10 stated, “You don’t realize how much it takes just to take a shower… I really have to take my time”, while others described similar effort while standing to prepare meals or doing basic chores.
Participants also highlighted a gradual loss of valued activities over time, including hobbies, travel, and regular exercise. As P07 reflected, I used to work in my garden every year. I just cannot do it anymore and described how repeated hospitalizations affected her life “I’ve had so many times where I’ve had to be put in the hospital, I’ve missed family trips”. This load was frequently compounded by multimorbidity and treatment demands. P15 linked obesity, atrial fibrillation, and high blood pressure to additional functional limitations, noting that she “can’t even bend and tie her shoes or stand for long periods”. For others, continuous oxygen use made basic tasks such as cooking harder. Together, these accounts illustrate the functional impact of COPD amplified by co-existing conditions on activities of daily living and previously enjoyable activities.
Subtheme Fluctuating Emotional Well-Being with Breathlessness-Induced Panic
Participants described their emotional state as tightly linked to their breathing, with elevated levels of anxiety when their oxygen levels dropped, or with breathlessness. Several identified a “panic point” around desaturation, with one participant (P01) explaining, “I get anxious when it hits 92 and that’s when I panic”. For some, even the anticipation of breathlessness shaped their day as P11 said “Some days I just dread going outside. it’s going to get me gasping for breath”. Others described episodes where being briefly off oxygen or feeling stressed would trigger a panic until they could calm their breathing. Breathlessness also carried a social and emotional burden; as one participant (P11) shared, “When I get really out of breath, I just feel embarrassed, I don’t want people to see me like that”. Mindfulness strategies introduced in the program were often used in these moments by several participants, with a participant (P02) noting that “using some of the things from the mindfulness class when I get anxious and have panic attacks… has helped”, underscoring how emotional distress, social concerns, and symptom management were deeply intertwined.
Subtheme Balancing Independence and Safety
Participants valued staying independent and “getting out of the house”, but described constantly negotiating how to do so safely. For those dependent on oxygen, even short trips required planning and time limits. As participant (P15) explained,
I can go wherever I need to go. I just can’t stay long, because I’m carrying those little, small oxygen tanks that don’t last but about 15 minutes.
And another participant (P08) described grocery shopping as a targeted in-and-out trip rather than a leisurely activity, as she stated, “I can’t just browse, I have to go in, get what I need and come back”. Participants reported the flexibility of moving around while using a longer cannula but just need to be careful.
Others similarly described trying to resume going out after illness while relying more on oxygen than before or avoiding certain movements and uneven surfaces because of balance problems and fear of falling. One participant (P07) reflected, “There’s a lot of things you become aware of that you got to learn how to do by myself, and not be moving too fast”, capturing the way self-protection and independence were continually weighed against each other. Together, these accounts highlight a continual balancing act between maintaining autonomy and minimizing risk.
Subtheme Memory and Hearing Difficulties Affecting Adherence
Cognitive load, memory problems, hearing difficulties, and fluctuating energy further affected program participation. Some participants with memory challenges reported that they forgot sessions despite wanting to attend, as P11 explained,
I have memory problems… I have trouble remembering things like dates and times… some of the ones I missed, it wasn’t because I didn’t want to attend.
While another participant (P10) reflected, “My memory’s not good like it used to be… the class yesterday, I really forgot”. Hearing problems also interfered with engagement and comprehension, with one participant (P06) noting, “Because of their accent and my hearing problem, it was hard to understand”, and another (P04) adding, “I couldn’t understand the accent, and I have hearing issue on both sides, however having PowerPoints was very helpful”. Collectively, this theme illustrates how intertwined physical, cognitive, and emotional demands shape participants’ day-to-day functioning and capacity to engage with rehabilitation.
Reframing Health, Motivation, and Self-Management
This theme captures how participation in the program encouraged participants to rethink their relationship with their health from feeling overwhelmed or passive to becoming more motivated, and active in managing symptoms, emotions, and daily behaviors.
Renewed Motivation and Accountability for Health Behaviors
Despite living with substantial symptom burden, many participants described the program as a catalyst for re-engaging with their health. Scheduled sessions “got [them] up and moving” on days when they might otherwise have remained sedentary; P01 noted, “It was good for me. It got me up and moving on some days that I probably wouldn’t have”, and P04 emphasized, “I participated and listened to everything, and I’d done everything that I could do there”. P13 framed his ongoing participation as a hopeful trajectory, stating, “I feel like if I keep on this journey with this program… I’m going to be all right… just one day at a time”. These narratives illustrate a renewed sense of accountability and purpose around health behaviors.
Increased Symptom Awareness and Self-Regulation
Participants described becoming more aware of their oxygen levels and more deliberate in pacing their activity, routinely “checking the number” and responding when saturation dropped. As P10 noted, “I checked and it had dropped down to like 89, so I actually had to sit down for a minute”. P15 similarly explained,
I have my little finger thing… I measure [my oxygen] and sometimes I have to wait a minute so it can come back up, because it’ll go down depending on what exercises we’re doing.
Together, these reflections illustrate a growing awareness of personal limits and the need to adjust activity or oxygen flow accordingly.
Creating Calm Amid Chaos (Mindfulness and Self-Care)
Mindfulness and breathing strategies were described as helpful tools to manage panic, anxiety, and feeling “on edge”. P01 shared that “using some of the things from the mindfulness class when I get anxious and have panic attacks… that has helped too”, while P11 noted that “the mindfulness was good as far as helping me to relax”. Participants used these skills outside of class to regain control during distressing moments. P07 reflected that she had a tendency to panic when she was away from her oxygen, but mindfulness and breathing practice taught her “not to panic, but just to learn how to breathe better… till I can get to the oxygen”, helping her to calm both body and mind. P05 similarly described practicing pursed-lip breathing not only for COPD but as a way of “clearing my… mind and body of other things”, emphasizing that the repeated “breathe in through the nose and out through the mouth” routine during mindfulness sessions helped him reset when stress built up. P15 summed up the impact by explaining that in mindfulness class she learned she could
Just sit and relax and not have to worry about how you’re going to do this or that… sometimes I feel like I’m always on edge, but I’m learning to relax because of the mindfulness classes.
Together, these accounts show how mindfulness turned frightening breathless episodes and everyday worries into moments where participants could “calm down” and feel more in control.
Finding Strength in Small Wins and Gratitude
Participants frequently drew motivation from small but meaningful improvements and from comparing their situation to others, which fostered both gratitude and perseverance. P11 reflected that “some people can’t walk… at least I still can get up and walk… that gives me some encouragement to try to get up”, and P10 added that seeing other participants’ challenges made her realize “the problems that I have are kind of miniscule in comparison… it makes me realize I have a lot to be grateful for”. P15 similarly described a similar sense of uplift after exercise: “sometimes I feel five pounds lighter”, and said that on those days “I can go clean the bathroom, or I can clean the kitchen”, tasks she previously lacked the energy to do. P01 and P10 also highlighted the emotional boost of group sessions, noting that “it helps to see that other people… you feel like you’re the only person and now I see that I wasn’t”, and “I’m not alone in this… some people can’t use half of their body, some people can’t walk”. P14 reported that a small improvement in being able to stand longer while cooking as he stated, “I can cook my meal feeling less winded like before and it’s giving me a sense of independence, and I will continue to do more exercises”.
These small physical gains and moments of perspective helped participants reframe their illnesses, cultivating a sense of gratitude and reinforcing their desire to keep engaging with the program.
From Caution to Capability: Discovering Strength Through Movement and Adaptation
This theme reflects how participants shifted from fear and avoidance of exertion toward increasing confidence in their physical abilities, discovering that with adapted exercises, pacing, and support they could safely do more, tolerate activity better, and integrate movement into everyday life.
Improved Physical Activity and Confidence
Across the interviews, participants described a shift from fear of exertion to greater confidence that they could move safely and do more. P01 noted, “I can do a little bit more now around the house without stopping”, while P15 explained that after exercising, she felt she could finally tackle chores she had been avoiding: “before that, I just don’t have the energy to do it… after exercising, I feel like I can do more. I can go clean the bathroom, or I can clean the kitchen”. P04 described a similar trajectory outdoors, saying the program “has motivated me to try to get out and do a little bit more”, including regular walks on trails by the river with his spouse. P05 added that the classes “help me maybe start a new habit where I will continue to do it”, describing feeling better overall.
Together, these accounts show participants moving from protecting themselves from breathlessness to cautiously testing and expanding their activity, supported by adapted exercises, pacing, and instructor reassurance.
Reduced Reliance on Oxygen (for Some)
For a subset of participants, increased activity tolerance translated into perceived improvements in oxygen needs or stability. P05 noted that during and after the program, “my oxygen stays better than before”, suggesting that conditioning allowed him to exercise without as dramatic a drop in saturation. P01, who had previously been “on oxygen 24/7”, described that after completing the program she had progressed to where “some days I don’t. I take it with me when I do go somewhere”, marking a meaningful step toward independence.
Other participants did not report reduced oxygen requirements but still described improvement in breathlessness: P15, for example, remained on high-flow oxygen but explained that after class she “doesn’t feel as winded” as she once did, even when exercising at 8–10 liters. These experiences suggest that for some individuals, telewellness participation may help stabilize oxygen levels or reduce continuous dependence, while for others it primarily improves comfort and endurance at their current prescription.
Making Food Choices That Fit Complex Health Needs
This theme reflects how participants used nutrition education to better understand “what’s good and not”, while simultaneously navigating practical and medical constraints (living alone, cooking with oxygen, multimorbidity) that made it challenging to apply generalized diet advice to their complex, individual health needs.
Gaining Nutrition Knowledge and Label Reading
Participants reported gaining practical nutrition skills, especially around label reading and understanding how specific nutrients relate to their health conditions. P15 explained that through the nutrition classes she was “learning now… to prepare meals that I hope will help me with my obesity… proportioned meals for protein, for fiber, and just preparing good meals”, linking dietary change directly to weight and symptom management. P02 described a new habit of scrutinizing packaging:
I’ve learned how to read labels… to see the amount of sodium and the amount of protein… what’s in what you’re eating… I do that now constantly.
P05 similarly noted, “I learned a lot in the nutrition class, like how to read labels at the grocery store and see what’s good and what’s not”, and emphasized that he now thinks “it’s good for me to be… eating healthy… it affects the rest of my body”. For some, this knowledge resonated with existing clinical training; as P01, a former nurse, put it, “the content was kind of… something I already knew, but… it was good to go back over it again”, reinforcing prior health education and motivating renewed attention to diet.
Living Situation and Comorbidities Limiting Nutrition Practice
Despite these gains, participants highlighted substantial barriers to putting nutrition advice into practice. P09, who lives alone, explained that “since I live alone and don’t cook much, it’s hard to practice”, and added that “cooking is hard because I wear oxygen all the time”, underscoring how fatigue and equipment need complicate the meal preparation.
Others felt that generic weight-loss advice did not align with their goals or comorbidities. P08 noted that “most of the nutrition was geared towards losing weight but with my COPD, I need to gain weight”, while P06, living with stage 4 kidney disease, shared that “a lot of that nutrition stuff didn’t pertain to him… eating a lot of protein, he cannot do that… the dairy, he’s very limited on that”. Another participant reported that she did not like the recipes shared during the program, and those are the kind of foods she does not eat. These accounts illustrate how living alone, continuous oxygen use, multimorbidity (eg, obesity, kidney disease) and cultural food choices can constrain the extent to which participants can translate new knowledge into day-to-day eating, and highlight the need for more individualized, condition-specific guidance.
Program Perceived as a Practical Alternative or Bridge to Pulmonary Rehab
This theme captures how participants viewed the telewellness program as overlapping with key components of pulmonary rehabilitation especially breathing and exercise and, for some, as a practical substitute or “bridge” that could meet therapy or surgical readiness requirements when traditional, in-person pulmonary rehab was unavailable, inaccessible, or not covered.
Overlap with PR and Surgical Readiness
Many participants described the program as overlapping substantially with pulmonary rehabilitation, particularly through its focus on breathing exercises and structured physical training. P12 felt that “most people could possibly find something they could do… but at least some of it [was] geared towards pulmonary rehab type stuff”, emphasizing the PR-like nature of the exercise content. For some, this similarity had concrete implications for surgical care. P11 reported that “this counted as therapy so I could go ahead with surgery”, and P01 elaborated that she
Needed to have pulmonary therapy… to have a surgery that my doctor wanted to provide… and he couldn’t without pulmonary therapy and this was able to… count as pulmonary therapy through UAB.
The absence of program fees and the tele-delivery format made this especially valuable for individuals whose insurance would not cover traditional PR or who could not travel to hospital-based programs.
In this way, the telewellness intervention functioned as a practical alternative or bridge, helping participants meet pre-surgical requirements and access rehabilitation support that might otherwise be out of reach.
Strengthening the Spirit, Mind, and Body
This theme reflects how participants experienced the program as more than exercise, describing it as uplifting and supportive of their emotional, spiritual, and physical well-being, with breathing, mindfulness, and education working together to help them cope with COPD.
Holistic Benefits Beyond the Physical
Participants consistently emphasized that the benefits of the program extended beyond physical, and included emotional, social, and spiritual dimensions of health. P03 described the sessions as “all good, positive advice”. “Uplifting, and… give all of us things to think about, because we have different areas of health. You know, spiritual and mentally and physically”, and P14 concluded that “the breathing, the mindfulness and the exercise… are biggies for the COPD”. P07 similarly highlighted the program’s impact on mood and relationships, explaining that people with health problems “go through so much depression because of their health situations”, and that having a program like this “brought me out of some of that… learning how to eat better, and… just relationships… I just think it’s good”. For some, these holistic benefits intersected with faith and community; P15, for example, continued to attend church services online due to infection concerns, but drew strength from feeling part of both her faith community and the program, noting that seeing others “with other ailments” doing their best helped her feel she could do the same. Across interviews, participants framed the intervention not only as exercise or education but as a telewellness space that nurtured the “spirit, mind, and body” together.
Themes and Subthemes (Table 3)
Home and Community Contexts Shaping Participation
This theme describes how participants’ home environments and community responsibilities both enabled and constrained their ability to attend, focus, and exercise safely during the program.
Home Space and Privacy
Participants described home space as both a barrier and a facilitator for participation. For some, limited room and shared living arrangements made it hard to exercise comfortably: as P10 stated, “I don’t have that much space in my house”, while P14 explained, “Home with more than one… You know, it’s about 6 people in there… It’s like a boarding house”, making it difficult to find privacy to attend the sessions. In contrast, others had ample room to move and set up equipment. P02 noted, “I don’t have a problem with space at all. You know, I have enough room to do what I need to be doing”, and P11 shared, “Most of the exercises I did in the kitchen. I’ve got a pretty big kitchen”. Privacy within these spaces was also important; P01 described that “It was a little hard to concentrate with my granddaughter in the background giggling”, highlighting how noise and interruptions in shared homes could limit focus and comfort during group sessions.
Transportation, Errands, and Competing Responsibilities
Competing responsibilities and travel demands often collided with scheduled sessions, even when motivation was high. P01 recalled, “There were a few times I would have a doctor’s appointment or something come up”, while P14 noted that “Most of the time my appointments coincide with other appointments… groceries, shopping… it conflicted with the time”. At the same time, many emphasized that home-based delivery removed a major barrier, making participation feasible in the first place. P04 reflected, “I think doing it at home was a lot better for me. If I had to go somewhere to do this, I probably wouldn’t have participated”, and P05 similarly shared that “It was online was a big help. If I’d have had to… personally attend these meetings… the way it’s set up, it was no problem at all”. Together, these accounts underscore how the home setting reduced travel burdens but did not fully resolve time pressures and role demands.
Fall Risk and Mobility Adaptations
Fall risk and mobility limitations strongly shaped how participants adapted exercises in their homes. P11 explained, “I can’t get down on the floor and do those types of things once I’m down, I can’t get back up without help”, leading her to avoid certain movements altogether. Others relied on furniture or equipment for stability; P07 shared, “I hold on to the chair when I do the exercises, just to feel safe”, while P09 described needing to use a chair for many activities even though he “had plenty of space”. These adaptations allowed participants to continue engagement with the program.
Supportive, Inclusive Services Enabling Engagement
This theme captures how respectful, skilled staff and inclusive group structures fostered trust, belonging, and sustained engagement.
Respectful, Encouraging Staff and Services
Participants consistently described instructors and staff as caring, non-judgmental, and encouraging. P02 recalled being reassured to pace herself: “He told us if you’re unable to do any of it, just do what you can do… just try to do something during the time”, while P13 summarized, “You know, they’re trying to help me, that’s all they did”. Trust in staff was strengthened by their clinical expertise and clear explanations. P03 remarked, “Each instructor was knowledgeable of that area. They explained and went over things very thoroughly”, and P13 appreciated “a mentor walking you through. Everything you’re trying to do… and what you’re doing will help in that area”. Similarly, P08 noted that an instructor “she kept an eye on, as far as technique… she always emphasized to go at your own pace… if you couldn’t do this part, you can do it this way”. These experiences left participants feeling respected and supported rather than judged or left behind.
Group Connection, Shared Learning, and Structure
Group sessions reduced isolation and created opportunities for shared learning. P13 reflected, “You start thinking it’s just you… and then you hear everyone else, and you realize, okay, I’m not alone in this” and P08 emphasized, “Being in the group showed me I’m not alone and everyone has different limitations, but we’re all dealing with something”. P15 described how peer questions could resonate with her own concerns:
When somebody may ask a question where it’s really related to something that you may have been thinking about, and you can chime in and so we communicated in that way.
P11 appreciated that “She put in some good recipes, and there’s a good rapport with the group… we were able to provide our input”, particularly in nutrition sessions. Regularly scheduled classes also provided a helpful structure; P13 shared, “It was nice having something planned during the day, something to look forward to”. Together, these accounts depict the program as a supportive community, not just a series of classes.
Multimodal Instruction Enhancing Comprehension and Retention
This theme reflects how diverse teaching formats and flexible exercise options supported understanding, while additional learning support helped compensate for hearing and communication challenges.
Multimodal Teaching and Flexible Exercise Options
Participants valued having information delivered in multiple ways, ie, verbally, visually, and through demonstration. P03 noted, “They presented the material… very well to where any participant should have been able to understand”, and P12 added, “If we had questions, they answered them fully and made sure we understood what they were saying”. Visual supports were especially helpful; P13 explained, “Like, seeing the PowerPoint, I learned better that way when I can see it”, and P10 commented that the nutrition component “teaches you about stuff that you shouldn’t eat and how easy it is to prepare a healthy meal… it didn’t even take that long”.
Flexibility in exercise program was also a facilitator to participation. Several participants reported that the option to perform exercises in a seated position enabled them to engage more fully in the exercise sessions. P14 shared, “I like it that I can do the exercises either sitting or standing. I like it that they showed it to us both ways”, while P02 described that “Even when my oxygen dropped, I just switched to sitting and kept going”. P08 emphasized that the instructor “always emphasized to go at your own pace… for the standing and sitting exercises, you were able to alternate between the two”. These multimodal strategies and options allowed participants with different capacities to stay engaged.
Learning Supports and Communication Challenges
Written materials, repetitions, and recordings reinforced learning and helped participants compensate when they missed details. P12 said, “The workbook was really good; I could write notes in it. Sometimes I’d forget an exercise unless I reviewed the video”, and P15 appreciated that “You have an instructor that’s explaining it to you, and you also have a manual you can sit there and read”. When sessions were recorded or videos were shared, participants used them flexibly: “They would send videos that I could follow along with… do the program even if I missed the class of the day, so that was helpful”, P07explained, and P05 said “If I have a question in my mind about something, then I’ll go to the videos”. At the same time, some participants reported that hearing difficulties and understanding accents made content hard to follow. P01 reported, “Because of his accent and my hearing problem, it was hard to understand”, and P02 shared, “I had difficulty understanding the content in health coaching because of the accent however everything was written on power point which made it easier”. These accounts highlight the value of layered supports, ie, captions, clear audio, written materials, and recordings to maximize accessibility.
Technology and Equipment as Both Enablers and Barriers
This theme captures how the telehealth platform and home exercise kit often facilitated participation and confidence, while digital literacy, technical glitches, and safety concerns sometimes limited engagement.
Technology and Home Exercise Kits as Facilitators
For many participants, the virtual format and exercise kit made it easier to join and stay engaged. P05 emphasized, “It was online was a big help. If I’d have had to… personally attend these meetings… the way it’s set up, it was no problem at all”, and P02 reflected, “The remote program was good as I didn’t hao go anywhere and I knew that during COVID with kids attending their classes”. Some felt the app and platform were straightforward; P12 noted, “I’m not… very good on the computer but this app was easy to use and pretty self-explanatory”, while P15 shared, “I’ve been working with computers for a long time. That was my work, so… no, I didn’t have any problems”. Participants also valued the equipment itself; P14 said, “It was a help, a wonderful help. Some of the things I had were old, so it was nice to get something new”, and P07 added, “I liked it all. Receiving all of the equipment was a bonus! I even learned how to use the various equipment in a way that works for me”. These features collectively increased comfort and made exercise feel more accessible at home.
Digital Literacy, Technical Glitches, and Safety Concerns
Some participants reported frustration with technology and equipment, especially early in the program, and noted that a lack of social support further intensified these difficulties. P14 described relying on trial and error: “These computers these days, you just have to play around with it… You know, I know that some of the participants had other people”, and P13 noted that “Well, sometime my, uh, computer froze… but I think that’s this house over here, because there’s so many things hooked up to it”. P13 reflected “I live alone… so I had to figure it out myself. I couldn’t get on the first class, but after that, it went okay”. Age-related digital challenges also emerged; P11 shared, “I’m 72 years old… I’m not real tech savvy and my daughter helped me log into the sessions”.
Participants reported difficulties using the exercise equipment, particularly when instructions for the items provided were unclear. P14 recalled, “Exercise equipment that was sent to me. I don’t know how to use those particular items”. Safety concerns around equipment and oxygen were also prominent. As P10 put it, “The balance disc was good… I’m just a little scared because I might fall”, while P09 explained, “It’s hard dragging the concentrator around when I’m trying to exercise”, and P05 noted, “I have my continuous oxygen flow in my room, and I didn’t use it while exercising in living room. I could’ve used it”. These experiences underscore the need for individualized tech support and safety planning alongside the provision of equipment.
System-Level Barriers and Workforce Gaps
This theme reflects broader system-level barriers, particularly in nutrition services and follow-up with healthcare professionals that constrained participants’ ability to obtain specialized, ongoing support beyond the program.
Limited Access to Nutrition Professionals and Follow-Up
Participants described difficulty accessing dietitians and knowing where to turn with nutrition questions outside the structured sessions. P06 stated, “All the nutritionists are working in hospitals now. You can’t find a new… I found one nutritionist on the internet, and she was in California” indicating both geographic and availability barriers. P02 similarly shared, “I wasn’t able to reach out to the nutritionist… I didn’t know who to call”, highlighting unclear pathways for follow-up support. Others felt that the amount or pacing of nutrition information required more time with a professional; P08 reflected, “Nutrition was a lot of information. That’s just something… I need more time than others”. Collectively, these accounts point to workforce shortages and fragmented systems that hinder sustained, COPD-relevant nutrition care.
Themes and Subthemes (Table 4)
Seeking Sustained, COPD-Relevant Rehab Support
This theme captures participants’ desire for ongoing, COPD-specific rehabilitation and resources, and flexible, tailored tele-rehab models that reflect the diversity of COPD experiences.
Desire for Ongoing, COPD-Specific Support and Resources
Participants expressed a strong wish to continue aspects of the program after its formal end, particularly through recordings and materials they could reuse. P10 suggested, “I think if he recorded them, or we could go back to the mindfulness… that would be helpful, even though we’re not having class anymore”, and P14 shared, “Well, I saved those… I will go back, and that’s what I will use… exercise when this program is over. Those are my intentions”. Several also wanted the program itself to continue; P02 noted, “The program duration and frequency of classes was good. I only missed one or two… time went by so fast, and I wish the program would continue long”. Participants additionally voiced a desire to see more COPD-specific representation. P04 reflected, “I would have liked to have seen a couple more with the COPD… nobody really came up and spoke about having the problems that I have”, and P02 added, “I think it would be good to see more people with COPD. Everyone is doing something… it’s good to know what others are doing to manage their COPD”. These narratives highlight a desire for sustained COPD-focused support that extends beyond time-limited intervention.
Importance of COPD-Specific Pulmonary Rehabilitation Strategies
Participants recognized the value of pulmonary rehabilitation strategies and wanted them more explicitly tailored to COPD. P11 commented, “Some of the things that they do in pulmonary rehab may be beneficial for people with COPD”, suggesting that greater integration of these elements could strengthen the program. P15 emphasized the need for more structured breathing training:
For COPD, having more breathing exercises, where you are taught… exercise, I mean, you’re always told to breathe in, breathe out. But for people with COPD. Some people don’t even know how to breathe.
These reflections underscore a desire for clearly framed, COPD-relevant rehab content, especially around breathing techniques during activity.
Precision Wellness is a Key to Future Research
Participants also highlighted the wide range of needs across the COPD spectrum and called for greater flexibility in how the program is structured. P12 said, “I don’t feel like my COPD is… as bad as some people. So, I can’t speak for them. Um, I’m not on oxygen”, while P11 noted,
Some people are depressed and have a lot of health problems. Some of the sessions would have probably helped them more than they helped me, because most of the time, I’m not depressed.
These comments point to differences in personal goals, symptom severity, mental health, and comorbidities. Participants wanted program design to reflect this variation. P15 suggested, “For all the different things, everybody doesn’t have to attend everything at the same time”, and P08 remarked, “Nutrition was a lot of information. That’s just something that’s something I need more time than others”. P07, whose schedule was unpredictable, explained, “I’m not always sure what the next few weeks will look like, so I’d rather schedule my classes one week at a time”. Together, these perspectives argue for long-term telewellness models that are both structured and flexible, allowing people to select components, adjust intensity, and pace participation in ways that align with their individual health status and life circumstances.
Future Program Adaptation Guidelines
Based on the derived themes and subthemes, we developed a set of participant-informed inclusion recommendations and design adaptations for telewellness programs for individuals with COPD, organized using the Guidelines, Recommendations, and Adaptations Including Disability (GRAIDs) framework (Refer to Table 5).
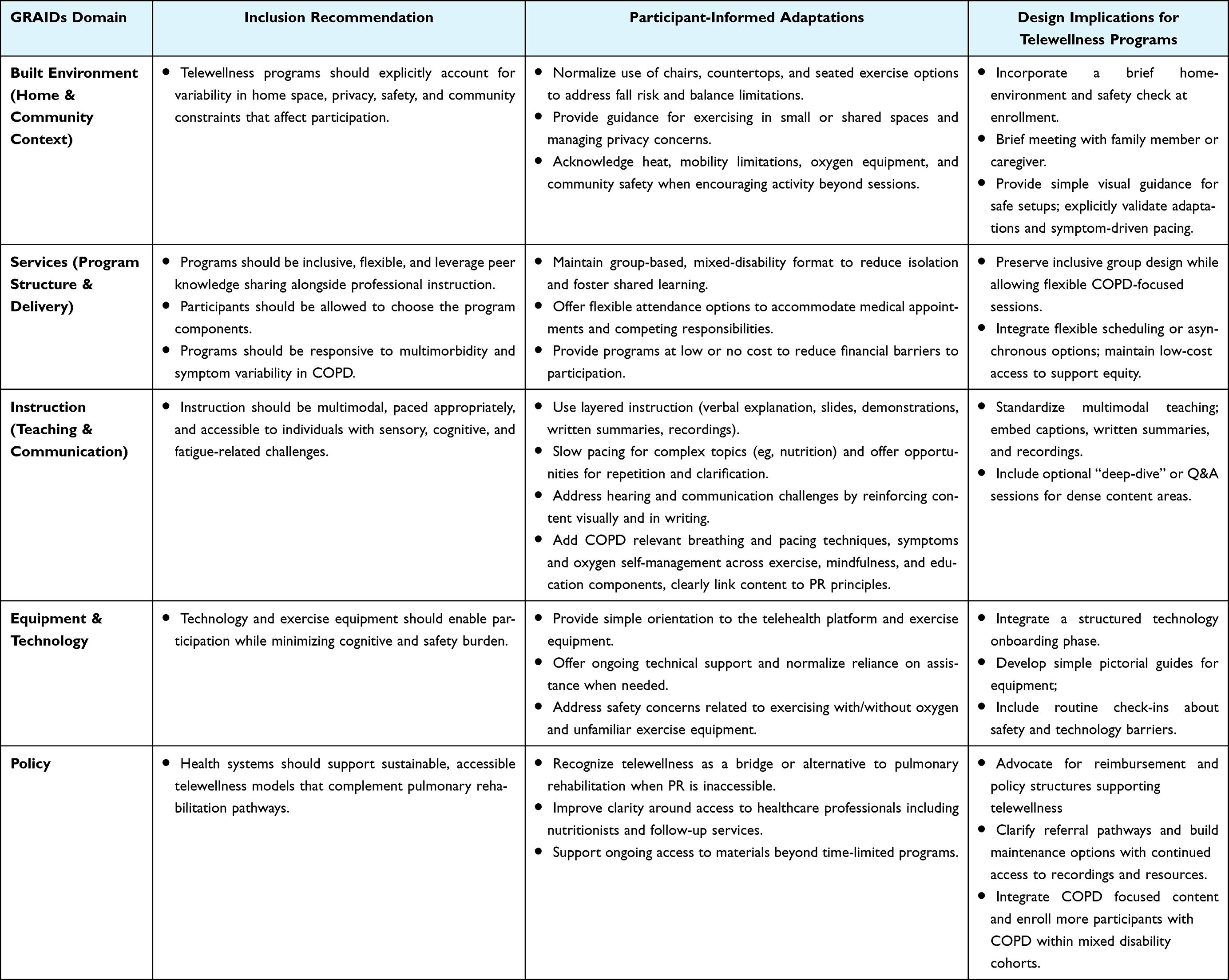 |
Table 5 Participants’ Informed Future Telewellness Program Adaptation Guidelines |
Discussion
This qualitative study provides novel evidence that the generic, telewellness program for individuals with mobility limitations is acceptable and beneficial for individuals with COPD. Participants reported improvements in confidence, physical activity, dyspnea-related anxiety, social isolation, nutritional knowledge, and overall well-being. Participants’ baseline narratives reflected fear of exertion, heightened sensitivity to breathlessness, and perceptions of everyday activities as unsafe or exhausting, often leading to activity avoidance. These findings align with evidence that dyspnea-related fear and catastrophizing are central drivers of physical inactivity, poor pulmonary rehabilitation uptake, and adverse outcomes in COPD.44–46
Participation in the MENTOR program supported a shift from avoidance to cautious engagement by helping participants reframe movement as adaptable and manageable through guided exercise, pacing, breathing techniques, and mindfulness. Mindfulness practices helped participants in managing panic associated with desaturation and restore confidence in their physical capabilities. These findings are consistent with evidence that mindfulness-based interventions (MBI) improve dyspnea, physical activity, symptom management, anxiety and behavioral avoidance.47–49
These results also support the treatable traits framework for COPD care, which emphasizes targeting behavioral, psychological, and extrapulmonary factors alongside airflow limitation.50,51 Lifestyle-based interventions addressing physical activity, weight management, and health behavior change have demonstrated improvements in health outcomes in COPD52–54 and our qualitative findings extend this evidence by demonstrating how participants experience these changes in real-world home settings.
There is growing attention towards personalized and precision-based approaches to treat chronic conditions. Celli et al highlighted a quote by Sir William Osler who said “Care more particularly for the individual patient than for the special features of the disease”55 and a key step in this approach is to identifying personal or contextual factors that influence symptoms and treatment adherence.9 The adapted 4M framework (assessment of medications, mentation, mobility, and morbidities) further reinforces a holistic, person-centered approach to COPD management by addressing modifiable factors such as physical activity, mobility limitations, anxiety, nutrition, and comorbidities to improve overall health outcomes and quality of life.55
The group-based, mixed-disability format played a significant role in shaping participant’s experiences and facilitating behavior change. Sharing sessions with individuals living with diverse disabilities reduced feelings of isolation and reinforced the perception that participants were not alone. Exposure to others with varying mobility limitations and health challenges helped normalize symptoms, foster perspective, and cultivate gratitude and empathy. These findings support the existing literature that sharing experiences with others in similar situations creates security and reduces the feeling of being alone.56
Participants also valued the inclusion of holistic program components, particularly mindfulness, nutrition, and health coaching. Reported benefits included management of anxiety, panic, healthier eating. Several participants reported nutrition-related behavior changes, including improved ability to read food labels and prepare healthier meals within the constraints imposed by limited mobility and lack of social support. This improvement is particularly important as evidence suggests that individuals with COPD face challenges in maintaining adequate nutrition due to dietary habits, limited access to healthy food and comorbidities.57 A recent study reported that nutritional literacy, is an important factor in disease prevention.58
Instructure-led health coaching sessions in our study was reported to be beneficial in providing support to promote positive behavioral changes. These findings align with existing evidence demonstrating that health coaching improves self-management abilities, health-related quality of life and reduce hospital admissions.59–63 These findings suggests that health coaching with structured guidance can address key barriers to program adherence, such as low motivation, psychological burden, and lack of individualized support.30
Several participants reported that home-based program eliminated travel-related barriers and made participation feasible, as they would not have attended center-based programs due to fatigue, mobility limitations, limited transportation, or lack of social support. Despite the benefits of virtual program, participants’ responses reflected that home environment was not uniformly enabling. Limited physical space, shared or crowded housing, background noise, and competing household responsibilities constrained privacy, focus, and movement for some participants. These findings are consistent with previous literature that individuals with COPD have different preferences as some like exercise in outdoor spaces versus controlled air-conditioned environments or benefits of social connections in center-based programs.64
Safety considerations such as fall risk and desaturation required participants to modify exercises by using chairs or countertops, avoiding certain positions, or restricting activity to spaces with continuous oxygen supply. Older adults with COPD are at a higher risk of falls than their healthier peers due to poorer balance, reduced muscle strength and exercise capacity.36 These findings underscore the need for telewellness programs to explicitly address the home environment and to support participants in creating safe exercise space aligned with their circumstances.
Additionally, engagement was intermittently disrupted by competing demands such as medical appointments and essential errands. Participants living alone described an added burden of independently managing meal preparation and grocery shopping, which further affected their ability to engage consistently with the program. These findings reinforce that telehealth is not inherently equitable unless home environments, digital literacy and disability related needs are explicitly addressed.35,65
The service delivery approach emerged as a central mechanism supporting engagement. Participants consistently valued instructors and staff who were respectful, encouraging, and non-judgmental, and who emphasized “doing what you can” rather than performance or perfection. Instructors’ knowledge of chronic conditions enabled them to anticipate limitations, offer appropriate modifications, and respond confidently to safety concerns, which fostered trust and feelings of acceptance regardless of functional ability. Regularly scheduled, group-based sessions provided structure and accountability, as well as something participants looked forward to each week, while creating opportunities for shared learning through the experiences of others living with disabilities. Existing literature support these findings as the participants enrolled in telehealth programs reported the importance of social connections in center-based programs and that inclusion of group-based format would be beneficial in telehealth programs to sustain the motivation.66 In this way, the program functioned as a socially supportive environment, rather than solely as a set of exercises or educational components.
Instructional design and learning support also emerged as key drivers for sustained participation. Multimodal teaching combining clear verbal explanations, PowerPoint slides, live demonstrations, written materials, and reflective journaling supported comprehension and retention, which was particularly important given age-related sensory changes and the cognitive demands of managing multiple chronic conditions. Participants described journaling as a useful tool for reinforcing learning, tracking symptoms and behaviors, and reflecting on progress over time, thereby supporting self-awareness and self-regulation.
Adapted seated and standing exercise options, along with encouragement to modify intensity, enabled participation across a wide range of functional levels and accommodated day-to-day symptom fluctuation. The variety of exercises across the program was reported as beneficial to sustain motivation, which also aligns with findings from previous study where participants’ reported similar daily exercise routine as challenging to their engagement.67 Furthermore, hearing difficulties, challenges understanding certain accents, and the density of some content (particularly nutrition) posed barriers for some participants. These findings underscore the importance of instructions tailored to participants’ needs such as visual supports, written summaries, reflective journaling, slower pacing, and session recordings as standard components of telehealth programs for individuals living with chronic conditions.
Experiences with technology and equipment were similarly mixed. For participants with prior digital experience, the telehealth platform facilitated consistent engagement. For others, limited digital literacy, unstable internet connections, and the need for family assistance to log in or troubleshoot issues reduced independence and sometimes limited participation. These findings are consistent with the barriers listed in the existing literature such as age related issues, lack of equipment, poor network, unfamiliarity with technology.68
Safety concerns related to using some exercise equipment and exercising with oxygen in the home further emphasized the need for clear, individualized safety guidance and ongoing support. A previous study reported that baseline home assessments should include evaluation of exercise equipment, safety protocol for situations such as loss of video or internet connection, use of equipment such as bike, tablet-related issues such as screen pop-ups, and emergency procedures for events such as falls during sessions,69 These findings suggest that digital training and home safety should be treated as core program components.
Overall, participants’ reflections highlighted system-level gaps in telehealth PR and nutrition services. Participants valued the holistic nature of the program, noting that it extended beyond exercise alone. Some described this generic telewellness program as an alternative or “bridge” when telehealth pulmonary rehabilitation (PR) was unavailable, and also as a preparatory therapy prior to lung volume reduction surgery. These situations were often related to loss of insurance benefits or dissatisfaction with existing telehealth PR programs that focused primarily on exercise training.
Participants expressed a desire for more COPD-specific components, including breathing exercises, tailored educational content, and nutrition guidance addressing coexisting conditions such as renal disease, diabetes, obesity, and hypertension. They also emphasized the need for clearer referral pathways and improved access to nutrition specialists. Additionally, participants highlighted the importance of continued access to program recordings, particularly for exercise and mindfulness sessions. This finding is consistent with previous studies demonstrating participants’ desire for ongoing access to program resources and varied exercise options.61
Taken together, these findings suggest that a holistic, group-based, free, mixed-disability telewellness program can be both feasible and impactful for people with COPD when it is supportive, flexible, multimodal, and explicitly designed around the realities of home environments, technology use, and system constraints. Future work can build on these insights to design a tailored COPD telewellness or telerehabilitation model that preserves the strengths of this approach, ie, holistic content, mixed-disability community, and no-cost access while adding more explicit COPD-focused components (breathing and pacing strategies, condition-specific education), home-environment and safety assessments, digital literacy support, and clear pathways to ongoing multidisciplinary care and maintenance options beyond the initial program period.
Limitations
The study findings are based on self-reported experiences and may be influenced by recall bias or social desirability. The interviews were conducted after program completion, and long-term sustainability of perceived benefits could not be assessed. Participant’s experiences reflect those who were able to complete the program and may underrepresent challenges faced by individuals who dropped out early due to factors such as health status, limited digital access and lower digital literacy. Nevertheless, the study provides rich, in-depth insights that can inform the design of future COPD-tailored, precision-based telewellness models.
Conclusion
This qualitative study highlights the promise of a generic, tele-delivered lifestyle wellness program for individuals with COPD, while underscoring the need for personalization to address the heterogeneity of COPD. Participant’s experiences demonstrated that engagement and perceived benefits are shaped not only by symptom burden and functional capacity, but also by comorbidities, home and community environments, digital literacy, social support, and system-level constraints. The mixed-disability, group-based telewellness model provided meaningful access and psychosocial support by reducing isolation and offering structure.
While participants reported benefits from the holistic approach, some emphasized the need for more COPD-specific content, tailored nutrition guidance, and flexible, sustained support. Addressing these gaps through precision-based tailoring, combined with GRAIDs-guided adaptations, may enable the development of scalable, equitable, and patient-centered telewellness models that better reflect the lived realities of people with COPD.
Acknowledgment
We would like to sincerely thank all the participants in this study for participation and valuable insights and feedback.
Funding
Funding for this study was provided by the National Center on Health, Physical Activity and Disability (NCHPAD). NCHPAD is funded by the Centers for Disease Control and Prevention (CDC), National Center on Birth Defects and Developmental Disabilities (NCBDDD), Division of Human Development and Disability, Disability and Health Promotion Branch, Grant #NU27DD000022. Research reported in this publication was also supported by the Eunice Kennedy Shriver National Institute Of Child Health & Human Development of the National Institutes of Health under Award Number P50HD118626.
Disclosure
Dr Surya Bhatt reports personal fees from Apreo, AstraZeneca, Boehringer Ingelheim, Chiesi, Connect Biopharma, Genentech, GSK, Kymera, Merck, Polarean, Sanofi, Regeneron, Uniquity, and Verona Pharma., grants from Apreo, Connect Biopharma, COPD Foundation, Genentech, Nuvaira, Sanofi, and Uniquity, personal fees from Horizon CME, Illuminate Health, Integritas Communications, IntegrityCE, and MedScape, outside the submitted work. The authors report no conflicts of interest in this work.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
References
1. Singh D, Han MK, Bhatt SP, et al. Is disease stability an attainable chronic obstructive pulmonary disease treatment goal? Am J Respir Crit Care Med. 2025;211(3):452–22. doi:10.1164/rccm.202406-1254CI
2. Bhatt SP, Abadi E, Anzueto A, et al. A multidimensional diagnostic approach for chronic obstructive pulmonary disease. JAMA. 2025;333(24):2164–2175. doi:10.1001/jama.2025.7358
3. de Oca MM, Perez-Padilla R, Celli B, et al. The global burden of COPD: epidemiology and effect of prevention strategies. Lancet Respir Med. 2025;13(8):709–724. doi:10.1016/S2213-2600(24)00339-4
4. Calverley PMA, Walker PP. Contemporary concise review 2022: chronic obstructive pulmonary disease. Respirology. 2023;28(5):428–436. doi:10.1111/resp.14489
5. Negewo NA, Gibson PG, McDonald VM. COPD and its comorbidities: impact, measurement and mechanisms. Respirology. 2015;20(8):1160–1171. doi:10.1111/resp.12642
6. Ritchie AI, Wedzicha JA. Definition, causes, pathogenesis, and consequences of chronic obstructive pulmonary disease exacerbations. Clin Chest Med. 2020;41(3):421–438.
7. Yohannes AM, Dransfield MT, Morris PE. The obesity paradox in pulmonary rehabilitation: relevance and implications to clinical practice. J Cardiopulm Rehabil Prev. 2024;44(6):417–424.
8. Gale NS, Albarrati AM, Munnery MM, et al. Frailty: a global measure of the multisystem impact of COPD. Chron Respir Dis. 2018;15(4):347–355. doi:10.1177/1479972317752763
9. Cravo A, Attar D, Freeman D, et al. The importance of self-management in the context of personalized care in COPD. Int J Chron Obstruct Pulmon Dis. 2022;17:231–243. doi:10.2147/COPD.S343108
10. Sandelowsky H, Weinreich UM, Aarli BB, et al. COPD - do the right thing. BMC Fam Pract. 2021;22(1):244. doi:10.1186/s12875-021-01583-w
11. Born CDC, Bhadra R, D’Souza G, et al. Combined lifestyle interventions in the prevention and management of asthma and COPD: a systematic review. Nutrients. 2024;16(10):1515. doi:10.3390/nu16101515
12. Rochester CL, Alison JA, Carlin B, et al. Pulmonary rehabilitation for adults with chronic respiratory disease: an official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2023;208(4):e7–e26. doi:10.1164/rccm.202306-1066ST
13. Wouters EFM, Wouters BBREF, Augustin IML, et al. Personalised pulmonary rehabilitation in COPD. Eur Respir Rev. 2018;27(147):170125. doi:10.1183/16000617.0125-2017
14. Holland AE, Wageck B, Hoffman M, et al. Does pulmonary rehabilitation address treatable traits? A systematic review. Eur Respir Rev. 2022;31(165):220042. doi:10.1183/16000617.0042-2022
15. Bhatt SP, Casaburi R, Mosher CL, et al. Telehealth pulmonary rehabilitation: a call for minimum standards. Am J Respir Crit Care Med. 2024;210(2):145–146. doi:10.1164/rccm.202402-0392VP
16. Arora P, Quach P, Lai B, et al. Advancing telehealth pulmonary rehabilitation for COPD: bridging current practices, individual experiences, and future needs: a scoping review. Respir Care. 2026:19433654251401473. doi:10.1177/19433654251401473
17. Holland AE, Cox NS, Houchen-Wolloff L, et al. Defining modern pulmonary rehabilitation. An Official American Thoracic Society Workshop Report. Ann Am Thorac Soc. 2021;18(5):e12–e29. doi:10.1513/AnnalsATS.202102-146ST
18. Yohannes AM. Disability in patients with COPD. Chest. 2014;145(2):200–202. doi:10.1378/chest.13-1703
19. Witt LJ, Wroblewski KE, Pinto JM, et al. Beyond the lung: geriatric conditions afflict community-dwelling older adults with self-reported chronic obstructive pulmonary disease. Front Med. 2022;9:814606. doi:10.3389/fmed.2022.814606
20. Zhou J, Liu Y, Yang F, et al. Risk factors of sarcopenia in COPD patients: a meta-analysis. Int J Chron Obstruct Pulmon Dis. 2024;19:1613–1622. doi:10.2147/COPD.S456451
21. Hakamy A, Bolton CE, Gibson JE, et al. Risk of fall in patients with COPD. Thorax. 2018;73(11):1079–1080. doi:10.1136/thoraxjnl-2017-211008
22. Nguyen KT, Brooks D, Macedo LG, et al. Balance measures for fall risk screening in community-dwelling older adults with COPD: a longitudinal analysis. Respir Med. 2024;230:107681. doi:10.1016/j.rmed.2024.107681
23. van Dam van Isselt EF, Groenewegen-Sipkema KH, Spruit-van Eijk M, et al. Pain in patients with COPD: a systematic review and meta-analysis. BMJ Open. 2014;4(9):e005898. doi:10.1136/bmjopen-2014-005898
24. Raphaely RA, Mongiardo MA, Goldstein RL, et al. Pain in Veterans with COPD: relationship with physical activity and exercise capacity. BMC Pulm Med. 2021;21(1):238. doi:10.1186/s12890-021-01601-8
25. Ebadi Z, Goërtz YMJ, Van Herck M, et al. The prevalence and related factors of fatigue in patients with COPD: a systematic review. Eur Respir Rev. 2021;30(160):200298. doi:10.1183/16000617.0298-2020
26. Kim I, Kapella MC, Collins EG, et al. Sleep disturbance and next-day physical activity in COPD patients. Geriatr Nurs. 2020;41(6):872–877. doi:10.1016/j.gerinurse.2020.06.010
27. Wang J, Li X, Lei S, et al. Risk of dementia or cognitive impairment in COPD patients: a meta-analysis of cohort studies. Front Aging Neurosci. 2022;14:962562. doi:10.3389/fnagi.2022.962562
28. Suen AO, Iyer AS, Cenzer I, et al. Social isolation and mortality in adults with chronic obstructive pulmonary disease. JAMA Intern Med. 2025;185(1):113–116. doi:10.1001/jamainternmed.2024.5940
29. Adhikari S, Saud B, Yadav PK. Empowering communities: implementing a COPD self-management program in Nepal. Lancet Reg Health Southeast Asia. 2024;29:100469. doi:10.1016/j.lansea.2024.100469
30. O’Toole J, Krishnan M, Riekert K, et al. Understanding barriers to and strategies for medication adherence in COPD: a qualitative study. BMC Pulm Med. 2022;22(1):98. doi:10.1186/s12890-022-01892-5
31. Rafii F, Alinejad-Naeini M, Soleymani babadi A, et al. Facilitators and barriers to self-management in Iranian men with chronic obstructive pulmonary disease: a qualitative study. BMJ Open Respir Res. 2024;11(1). doi:10.1136/bmjresp-2023-002245
32. Chen X, Wen N, Liu J, et al. Self-management and COPD: a qualitative study to explore the perceived barriers and recommendations to improve COPD management using the Information-Motivation-Behavioral skills model. NPJ Prim Care Respir Med. 2025;35(1):34. doi:10.1038/s41533-025-00443-9
33. Martins SM, Adams R, Rodrigues EM, et al. Living with COPD and its psychological effects on participating in community-based physical activity in Brazil: a qualitative study. Findings from the Breathe Well group. NPJ Prim Care Respir Med. 2024;34(1):33. doi:10.1038/s41533-024-00386-7
34. Yadav UN, Lloyd J, Baral KP, et al. Using a co-design process to develop an integrated model of care for delivering self-management intervention to multi-morbid COPD people in rural Nepal. Health Res Policy Syst. 2021;19(1):17. doi:10.1186/s12961-020-00664-z
35. Rimmer JH, Vanderbom KA, Bandini LG, et al. GRAIDs: a framework for closing the gap in the availability of health promotion programs and interventions for people with disabilities. Implement Sci. 2014;9:100. doi:10.1186/s13012-014-0100-5
36. Bates A, Furber S, Gilchrist H, et al. Reducing fall risk in older adults with COPD: pilot study to test the efficacy of a home-based exercise program with virtual care support. Int J Chronic Obstr. 2025;20(1):3175–3186. doi:10.2147/COPD.S502082
37. Rimmer JH, Wilroy J, Galea P, et al. Retrospective evaluation of a pilot eHealth/mHealth telewellness program for people with disabilities: mindfulness, exercise, and nutrition to optimize resilience (MENTOR). Mhealth. 2022;8:15. doi:10.21037/mhealth-21-34
38. Rimmer JH, Young H-J, Bachiashvili V, et al. Enhancements to a telewellness program for people with physical disabilities: mindfulness, exercise, and nutrition to optimize resilience (MENTOR 2.0). Prev Chronic Dis. 2024;21:E02. doi:10.5888/pcd21.230181
39. Ferguson CC, Clina JG, Young H-J, et al. Improvements in nutrition knowledge among adults with physical disabilities: a program evaluation of the mindfulness, exercise, and nutrition to optimize resilience (MENTOR) program 2020–2021. Disabil Health J. 2024;17(2):101577. doi:10.1016/j.dhjo.2023.101577
40. Poth CA. Qualitative Inquiry and Research Design: Choosing Among Five Approaches.
41. Hennink M, Kaiser BN. Sample sizes for saturation in qualitative research: a systematic review of empirical tests. Soc Sci Med. 2022;292:114523. doi:10.1016/j.socscimed.2021.114523
42. CLarke VBV. Using thematic analysis in psychology. Qual Res Psychol. 2008;3(2):77–101.
43. Poth CA. Qualitative Inquiry and Research Design.
44. Peng LC, Xu M, Wang Y, et al. Latent profile analysis of dyspnea-related kinesiophobia in older adults with chronic obstructive pulmonary disease. Heart Lung. 2025;69:241–247. doi:10.1016/j.hrtlng.2024.10.016
45. Hill K, Hug S, Smith A, et al. The role of illness perceptions in dyspnoea-related fear in chronic obstructive pulmonary disease. J Clin Med. 2023;13(1):200. doi:10.3390/jcm13010200
46. Wang J, Bai C, Zhang Z, et al. The relationship between dyspnea-related kinesiophobia and physical activity in people with COPD: cross-sectional survey and mediated moderation analysis. Heart Lung. 2023;59:95–101. doi:10.1016/j.hrtlng.2023.02.007
47. Von Visger TT, Wardlaw K, Li C-S, et al. Associations between mindfulness and symptom severity among adults living with chronic obstructive pulmonary disease (COPD). Heart Lung. 2025;70:163–169. doi:10.1016/j.hrtlng.2024.12.002
48. Tschenett H, Vafai-Tabrizi F, Zwick RH, et al. Digital mindfulness-based intervention for people with COPD - a multicentre pilot and feasibility RCT. Respir Res. 2025;26(1):199. doi:10.1186/s12931-025-03243-4
49. Kraemer KM, Kilgore K, Litrownik D, et al. A web-based mind-body intervention (Mindful Steps) for promoting walking in chronic cardiopulmonary disease: insights from a qualitative study. Glob Adv Integr Med Health. 2023;12:27536130231212169. doi:10.1177/27536130231212169
50. Cardoso J, Ferreira AJ, Guimarães M, et al. Treatable traits in COPD - A proposed approach. Int J Chron Obstruct Pulmon Dis. 2021;16:3167–3182. doi:10.2147/COPD.S330817
51. Agusti A, Gibson PG, McDonald VM. Treatable traits in airway disease: from theory to practice. J Allergy Clin Immunol Pract. 2023;11(3):713–723. doi:10.1016/j.jaip.2023.01.011
52. Au DH, Gleason E, Hunter-Merrill R, et al. Lifestyle intervention and excess weight in Chronic Obstructive Pulmonary Disease (COPD): INSIGHT COPD Randomized Clinical Trial. Ann Am Thorac Soc. 2023;20(12):1743–1751. doi:10.1513/AnnalsATS.202305-458OC
53. Brauwers B, Machado FVC, Beijers RJHCG, et al. Combined exercise training and nutritional interventions or pharmacological treatments to improve exercise capacity and body composition in chronic obstructive pulmonary disease: a narrative review. Nutrients. 2023;15(24):5136. doi:10.3390/nu15245136
54. Ambrosino N, Bertella E. Lifestyle interventions in prevention and comprehensive management of COPD. Breathe. 2018;14(3):186–194. doi:10.1183/20734735.018618
55. Celli BR, Fabbri LM, Yohannes AM, et al. A person-centred clinical approach to the multimorbid patient with COPD. Eur J Intern Med. 2025;140:106424. doi:10.1016/j.ejim.2025.07.020
56. Berglund M, Andersson S, Kjellsdotter A. A feeling of not being alone - Patients’ with COPD experiences of a group-based self-management education with a digital website: a qualitative study. Nurs Open. 2024;11(4):e2153. doi:10.1002/nop2.2153
57. Muellers KA, O’Conor R, Russell AM, et al. Barriers and facilitators of self-management behaviors among patients with chronic obstructive pulmonary disease and chronic comorbidities: a mixed-methods investigation. Chronic Illn. 2024;20(4):605–617. doi:10.1177/17423953231187172
58. Çapar AG, Çetiner EN. Can nutritional literacy be an important barrier for obesity and chronic diseases? Medicine. 2025;104(40):e44464. doi:10.1097/MD.0000000000044464
59. Long H, Howells K, Peters S, et al. Does health coaching improve health-related quality of life and reduce hospital admissions in people with chronic obstructive pulmonary disease? A systematic review and meta-analysis. Br J Health Psychol. 2019;24(3):515–546. doi:10.1111/bjhp.12366
60. Benzo R, McEvoy C. Effect of health coaching delivered by a respiratory therapist or nurse on self-management abilities in severe COPD: analysis of a large randomized study. Respir Care. 2019;64(9):1065–1072. doi:10.4187/respcare.05927
61. Midthun WR, Benzo MV, Ridgeway JL, et al. Understanding the patient experience of home-based pulmonary rehabilitation with health coaching for COPD: a qualitative interview study. Chronic Obstr Pulm Dis. 2023;10(3):224–233. doi:10.15326/jcopdf.2022.0384
62. Benzo RP, Kirsch JL, Hathaway JC, et al. Health coaching in severe COPD after a hospitalization: a qualitative analysis of a large randomized study. Respir Care. 2017;62(11):1403–1411. doi:10.4187/respcare.05574
63. Wang L, Mårtensson J, Zhao Y, Nygårdh A. Experiences of a health coaching self-management program in patients with COPD: a qualitative content analysis. Int J Chron Obstruct Pulmon Dis. 2018;13:1527–1536.
64. Rutherford H, Dale M, Wootton S, et al. Experiences of home-based pulmonary rehabilitation with mhealth and centre-based pulmonary rehabilitation in people with chronic obstructive pulmonary disease: a qualitative study. Health Expect. 2025;28(2):e70181. doi:10.1111/hex.70181
65. Arora P. Advancing telehealth pulmonary rehabilitation for COPD: bridging current practices, individual experiences, and future needs: a scoping review. Respir Care. 2026;10.
66. Krag T, Jørgensen EH, Phanareth K, et al. Experiences with in-person and virtual health care services for people with chronic obstructive pulmonary disease: qualitative study. JMIR Rehabil Assist Technol. 2023;10:e43237. doi:10.2196/43237
67. Lahham A, McDonald CF, Mahal A, et al. Home-based pulmonary rehabilitation for people with COPD: a qualitative study reporting the patient perspective. Chron Respir Dis. 2018;15(2):123–130. doi:10.1177/1479972317729050
68. Chien SY, Wong AM-K, Tseng W, et al. Feasibility and design factors for home-based pulmonary rehabilitation of patients with chronic obstructive pulmonary disease and chronic lung diseases based on a people-object-environment framework: qualitative interview study. JMIR Hum Factors. 2024;11:e51150. doi:10.2196/51150
69. King D, Khan S, Polo J, et al. Optimizing telehealth experience design through usability testing in hispanic American and African American Patient Populations: observational study. JMIR Rehabil Assist Technol. 2020;7(2):e16004. doi:10.2196/16004
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Using Machine Learning to Predict Likelihood and Cause of Readmission After Hospitalization for Chronic Obstructive Pulmonary Disease Exacerbation
Bonomo M, Hermsen MG, Kaskovich S, Hemmrich MJ, Rojas JC, Carey KA, Venable LR, Churpek MM, Press VG
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2701-2709
Published Date: 20 October 2022