Back to Journals » Integrated Pharmacy Research and Practice » Volume 12
Exploring Changes in Attitudes, Behaviors, and Self-Measured Health Data Through Lifestyle Modification Support by Community Pharmacists: Suito-Ogaki Selfcare (SOS) Trial
Authors Hibino Y, Matsumoto S, Nagase H, Nakamura T, Kato Y, Isomura T, Hori M
Received 15 February 2023
Accepted for publication 17 April 2023
Published 24 April 2023 Volume 2023:12 Pages 87—99
DOI https://doi.org/10.2147/IPRP.S408813
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jonathan Ling
Yasushi Hibino,1 Shohei Matsumoto,2 Hisamitsu Nagase,3 Takamasa Nakamura,4,5 Yoshihito Kato,4,6 Tatsuya Isomura,4,5 Michiko Hori4,7
1Gifu Prefecture Pharmacists Association, Gifu, Japan; 2Ogaki Pharmacists Association, Gifu, Japan; 3Faculty of Pharmacy, Gifu University of Medical Science, Gifu, Japan; 4Japan Selfcare Promotion Association, Tokyo, Japan; 5Clinical Study Support, Inc, Nagoya, Japan; 6Kowa Company, Ltd, Nagoya, Japan; 7SIC Co., Ltd, Tokyo, Japan
Correspondence: Tatsuya Isomura, Japan Selfcare Promotion Association, Showayakubou Bldg. 5F, 3-4-18 Nihonbashi-honcho, Chuo-ku, Tokyo, 103-0023, Japan, Tel +81-3-6271-8941, Fax +81-3-6271-8942, Email [email protected]
Purpose: Contributing to public health by supporting people’s health is the social mission of community pharmacists. This multicenter, prospective case series study aimed to evaluate changes in people’s behavior and health states through community pharmacists’ self-care support for healthy lifestyles.
Methods: The participants were recruited from voluntary adults aged ≥ 20 years who agreed to participate in the study, at community pharmacies in Gifu, Japan, between June and September 2021. Participants self-managed their lifestyles for six months while recording their health data, including blood pressure (BP), daily using devices (home BP monitor, body composition monitor, and activity meter) and a diet-recording app. They received lifestyle modification support at pharmacies at least once per month. Participants’ subjective health status, attitudes, and behavioral changes were evaluated using self-report questionnaires. Due to the exploratory nature of this study, data were primarily analyzed descriptively.
Results: Fifty-four participants aged 20 to 77 (mean age: 49.6 years; female participant proportion: 55.6%) participated in this study. Their mean weekly BP shifted almost horizontally from baseline to week 24 (systolic BP: 118.8 to 121.5 mmHg; diastolic BP: 76.1 to 77.5 mmHg). At six months, 38.9% and 35.2% of the participants reported better overall health and mental health, respectively, than at baseline. Over 85% of the participants became more proactive in improving their lifestyles regarding salt intake, diet, weight loss, and exercise, although drinking and smoking habits were more challenging to change. All the participants reported that they intended to continue to improve their lifestyle.
Conclusion: The participants’ responses suggested that community pharmacists’ support helped increase participants’ health awareness and promote their health-enhancing behaviors. However, its impact on health parameters should be further examined in future studies. More vigorous, tailored self-care support may be worth considering in developing a more effective, community-fitted health/well-being support system in Japan.
Keywords: community pharmacies, self-care, behavioral change, lifestyle modification, blood pressure, Japan
Introduction
With the global increase in life expectancy, accompanied by years of ill health or disability,1 increasing healthy life years (ie, a period without health problems limiting daily life) has become the focus of public health. Notably, a support system that promotes health is essential for increasing healthy life years. In Japan, the super-aging society requires a community-based, integrated care system to ensure that people can live longer and independently in their familiar communities, receiving diverse life support.2 Contributing to public health by supporting the maintenance and improvement of people’s health is a social mission of community pharmacists.3 Therefore, we aspire to build a community-fitted health and well-being support system centered on community pharmacies by promoting health literacy, which will contribute to prolonging healthy life expectancy and revitalizing the entire community.4 Community pharmacists can play an important role in increasing people’s health awareness and supporting positive behavior change in them, which are necessary for health promotion.5
Japan is one of the top countries in the world in terms of longevity.1 However, healthy life expectancy is around ten years (8.73 years in men and 12.06 years in women) shorter than life expectancy.6 Living with diseases or disabilities burdens individuals, their families, and society. It also accelerates the increase in healthcare expenditure, coupled with population aging.7 Therefore, shrinking this gap by prolonging healthy life years is one of the greatest priorities for improving public health and achieving a sustainable social security system in Japan.8
Noncommunicable diseases (NCDs) constitute major causes of unhealthy life years,9 among which hypertension is a leading risk factor for global deaths,10 and its reduction is the global target for the prevention of NCDs.11 Hypertension is also a national health problem in Japan; it is estimated to be prevalent among 43 million people.12 Hypertension is not only the leading risk factor for cardiovascular deaths in Japan,13 but it can also cause other conditions such as renal failure and dementia.12 National Health-Promotion Project in the 21st Century (Health Japan 21 (II)), announced by the Ministry of Health, Labour and Welfare, aims to reduce the average systolic blood pressure (BP) of the entire Japanese population by 4 mmHg within 10 years by promoting antihypertensive measures in terms of such as diet, physical activity, and alcohol drinking.8 The goal of this population strategy is to lower the BP distribution of the entire nation. Lifestyle modifications, often led by healthcare professionals, can significantly reduce BP and are recommended regardless of the BP level.12
Recently, even in Japan, frailty among older adults has received attention as a priority for prolonging healthy life expectancy.14 Social support for individuals’ health promotion may help prevent frailty, positively affecting the physical, psychological, and social aspects of people’s life—the three domains of frailty.15 Frailty substantially increases the risk of disability, long-term care, and death.16 Therefore, its prevention, which should be started earlier instead of targeting only older adults,17 is an important mission of community care for extending healthy life expectancy.18
Facilitating self-care among community residents to contribute to public health is an important role of community pharmacies.19 The effectiveness and challenges of health-promoting interventions by community pharmacists have been well reported, primarily overseas,20–22 but they have recently been explored in Japan as well.23–26 However, inconsistent findings of previous studies20 warrant further research on the effectiveness of pharmacist support for various purposes and methods. Additionally, most previous studies in Japan targeted people at risk for particular conditions;24,26 studies on self-care promotion among people, including healthy individuals, are scarce. Moreover, the reported behavioral changes or improvements in previous studies mainly depended on self-reporting; quantitative assessments using objective measures are rare.26,27 Furthermore, the intervention effects may vary in community settings. Thus, additional studies on community pharmacies’ self-care support using both qualitative and quantitative assessments would provide helpful information for developing a community-fitted health support system by community pharmacies in Japan.
Therefore, this study aimed to explore the impact of community pharmacists’ self-care support for lifestyle modifications on pharmacy visitors’ behaviors and health parameters, particularly BP.
Materials and Methods
Study Design
This multicenter, prospective case series study (Suito-Ogaki selfcare [SOS] trial; UMIN000044881) aimed to observe changes in individuals’ behaviors and health states through lifestyle modification and behavior change support provided by community pharmacists. The study was conducted in community pharmacies in Gifu, Japan, belonging to the Ogaki Pharmacists Association. The participants were recruited from pharmacies between June and September 2021. The target sample size was set to 60 to ensure feasibility (approximately 30 pharmacies would participate in the study, and two persons could be recruited at each pharmacy during the recruitment period). The study was approved by the Academic Research Ethical Review Committee of the Gifu Prefecture Pharmacists Association (approval reference number: 21070501). This study was conducted in accordance with the provisions of the Declaration of Helsinki and the Ethical Guidelines for Medical and Health Research Involving Human Subjects in Japan.
Participants
This study included individuals who met the following inclusion criteria: (1) provided written informed consent, (2) were adults (aged 20 years or older), and (3) were able to manage themselves using devices and smartphone apps at home, according to instructions. People were excluded if they were under treatment for chronic disease and attending physicians did not permit their study participation or if pharmacists judged their participation to be inappropriate. Physicians submitted written permission if their patients were allowed to participate despite hypertension.
Self-Care and Pharmacists’ Lifestyle Modification Support
At enrollment, participants received detailed instructions on how to use the devices and apps (described below) to measure their health data at home. The necessary devices were provided to the participants. The participants managed their lifestyles for six months and recorded their daily health data using devices and apps. They were asked to visit the pharmacy at least once per month to receive lifestyle modification support. During the participants’ visit, pharmacists provided advice on lifestyle modifications regarding salt intake, diet, weight, exercise, alcohol intake, and smoking in reference to the guidelines for the management of hypertension,12 based on self-measured health data. Pharmacists were gathered and instructed on how to provide advice before the study.
Assessments and Measures
Data were collected at the pharmacies or at home. Registration and other data collected at the pharmacies using questionnaires were sent to the study office. The study office kept track of the progress and regularly updated the participating pharmacies accordingly.
Baseline Assessment
At baseline, data on patient attributes (age and sex) and use of antihypertensive agents were collected. Additionally, baseline health state and lifestyle habits were assessed using the Questionnaire for Medical Checkup of Old-Old (QMCOO).28,29 This questionnaire was developed by the Ministry of Health, Labour and Welfare to comprehensively assess the health state of older adults in light of frailty and comprises 15 items covering ten aspects, including overall and mental health state, exercise and fall, and social participation.
Self-Measurements During the Study
During the study, the participants measured and recorded the following data themselves: (1) BP using a home BP monitor (HCR-7501T; OMRON Healthcare Co., Ltd., Kyoto, Japan); (2) weight using a body composition monitor (HBF-227T; OMRON Healthcare); (3) step count using an activity meter (HJA-405T; OMRON Healthcare); and (4) contents of meals using the health app CALO mama Plus (Link & Communication Inc., Tokyo, Japan). Data measured using devices (1) to (3) were transferred to smartphone apps, enabling participants to self-monitor their health data.
CALO mama Plus is a health app for recording health data (diet, exercise, mood, and sleep), and it also provides dietary advice using artificial intelligence. In this study, the app was only used for diet recording. The automated image recognition technique enabled participants to record meals by photography, although manual input or adjustment was also possible.30
The participants were instructed to record BP every morning and night, weight every morning, step count from waking up to bedtime, and diet at every meal. Self-recorded data were stored in the cloud, and the study office sent the data of the respective participants to their pharmacies.
Assessment at Six Months
At the six-month visit, the participants’ health state and lifestyle habits were re-assessed using the QMCOO. Additionally, participants’ attitudes toward lifestyle modification were evaluated using a self-report questionnaire on each lifestyle (salt intake, diet, weight, exercise, alcohol intake, and smoking), interest in lifestyle or health enhancement, and pharmacist support. Participants responded to each item by selecting one of four response choices (yes, somewhat yes, somewhat no, or no).
Finally, pharmacists’ support was qualitatively evaluated by both participants and pharmacists using four questions: (1) whether participants could ask about something they did not understand (whether pharmacists could ask participants about something they did not understand), (2) whether participants felt they were listened to by pharmacists (whether pharmacists felt they could listen to participants), (3) whether the guidance length was appropriate, and (4) whether a trusting relationship with pharmacists (participants) was deepened through lifestyle modification support. Each item had four response choices: yes, somewhat yes, somewhat no, or no.
Statistical Analyses
This study was exploratory in nature, and descriptive statistics were primarily used. For objective health parameters, where appropriate, summary statistics (weekly mean values ± standard deviation [SD]) were calculated using the weekly median value of each participant as their data for the week. Additionally, the number of measurements was counted per device or app.
The results of the self-report questionnaires were summarized descriptively. If available, the responses between baseline and six months (last visit) were cross-tabulated and compared using McNemar’s test or Wilcoxon signed rank test. A two-sided p-value of <0.05 was considered statistically significant. Weighted kappa coefficients, ranging from 0 to 1, were calculated to assess agreement in evaluations of pharmacists’ support between participants and pharmacists. Kappa coefficients were interpreted as follows: values <0.2 represented poor agreement; 0.21–0.40 fair agreement; 0.41–0.60 moderate agreement; 0.61–0.80 good agreement; and 0.81–1.00 very good agreement.31 All analyses were performed using SAS release 9.4 (SAS Institute, Cary, NY, USA).
Results
Participant Characteristics
In total, 54 individuals aged 20–77 years who met the eligibility criteria were enrolled from 21 community pharmacies. The mean age was 49.6 years, and 55.6% were women (Table 1). Nine participants used antihypertensive agents at baseline, of whom one experienced a dose increase during the study period. During the six-month follow-up, no participant dropped out of the study. The participants visited the pharmacy an average of 6.7 times during the follow-up.
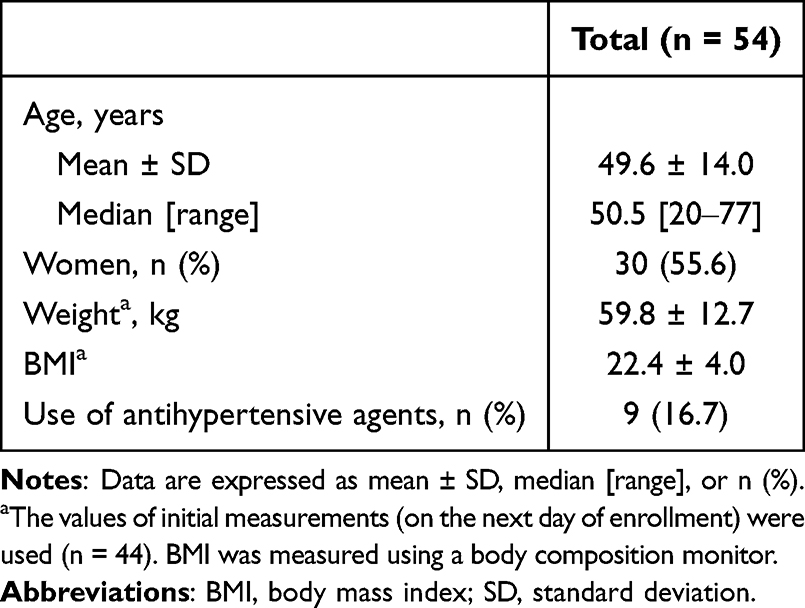 |
Table 1 The Baseline Characteristics of the Participants Recruited for This Study |
Weekly Mean Values of BP and Other Health Parameters
In the overall population (n=54), the weekly mean BP shifted almost horizontally from baseline to week 24 (systolic BP: 118.8 to 121.5 mmHg; diastolic BP: 76.1 to 77.5 mmHg). By the use of antihypertensive medications, a similarly horizontal shift was observed among 45 participants without antihypertensive medications (systolic BP: 115.3 to 118.9 mmHg; diastolic BP: 75.1 to 76.4 mmHg) and eight participants with antihypertensive medications but without dose increase (systolic BP: 130.6 to 131.1 mmHg; diastolic BP: 78.4 to 82.1 mmHg) (Figure 1). Both systolic and diastolic BP declined in one participant with a dose increase in antihypertensive medications, from 165.0 to 138.0 mmHg and from 95.0 to 80.5 mmHg, respectively (Figure 1). The participants measured BP, on average ± SD, 13.7 ± 9.2 times per week, with almost constant frequency throughout the study (Figure 2a).
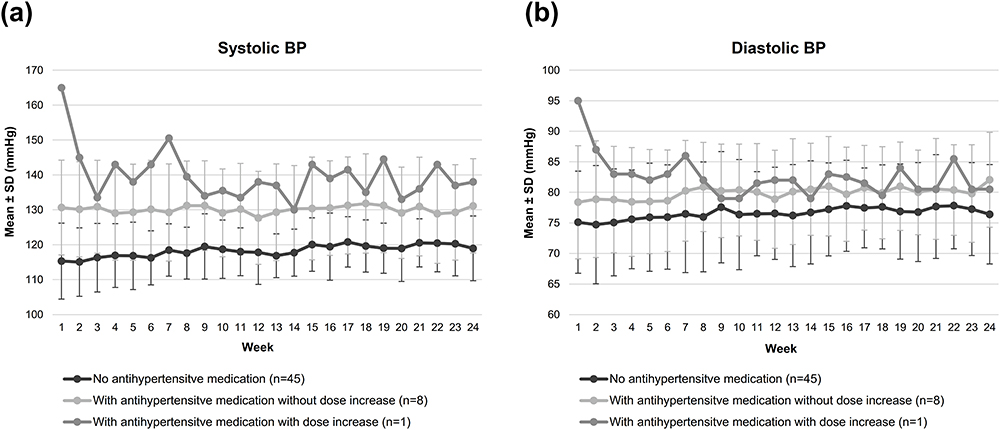 |
Figure 1 Mean weekly BP over the six-month follow-up period (by the use of antihypertensive medications): (a) systolic BP and (b) diastolic BP. Abbreviations: BP, blood pressure; SD, standard deviation. |
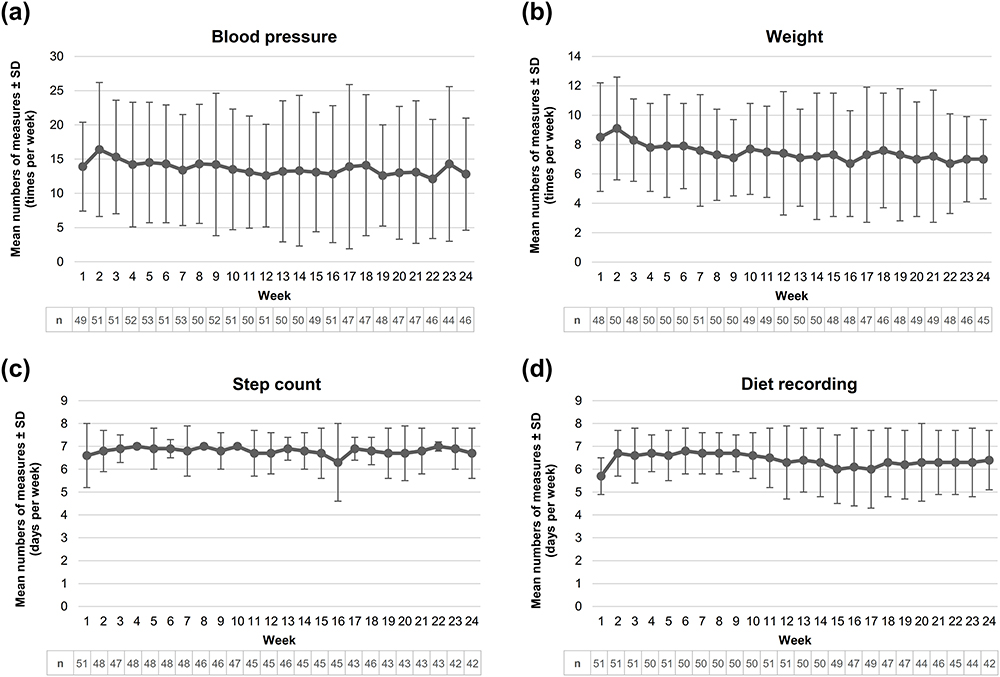 |
Figure 2 Weekly mean numbers of measures of each health parameter over the six-month follow-up period: (a) blood pressure, (b) weight, (c) step count, and (d) diet recording. Abbreviation: SD, standard deviation. |
Figure 3 displays the weekly mean weight, daily step count, and daily calorie intake over six months. There was little change in the weekly mean weight from 61.8 kg at baseline to 60.1 kg at week 24 (Figure 3a). The participants measured their weight, on average, 7.5 ± 3.6 times per week (Figure 2b). The weekly mean daily step count was approximately 4500 until week 16 but then gradually decreased to below 4000 (Figure 3b). The step count was measured, on average, 6.8 ± 0.9 days per week (Figure 2c). The mean daily calorie intake fluctuated weekly, but there was no clear decreasing or increasing trend at roughly around 1600 kcal (Figure 3c). The weekly mean days of diet recording was 6.4 ± 1.3 (Figure 2d).
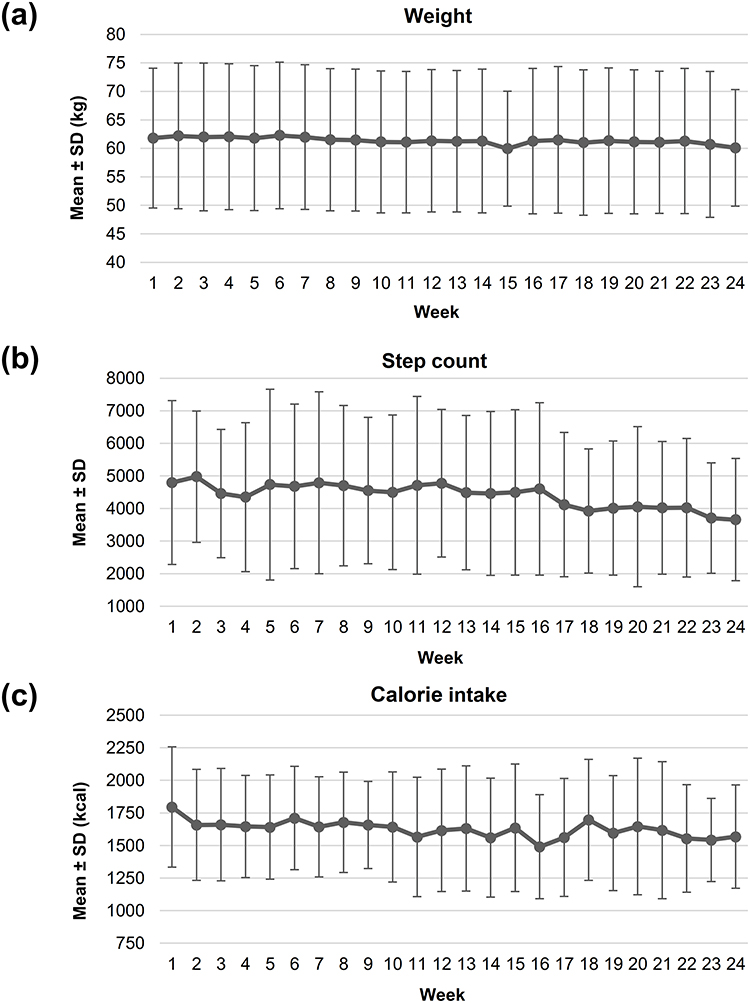 |
Figure 3 Weekly mean values of (a) weight, (b) daily step count, and (c) daily calorie intake over the six-month follow-up period. Abbreviation: SD, standard deviation. |
Self-Reported Health State
Table 2 cross-tabulates the results of QMCOO at baseline and six months. Compared to the baseline, 38.9% and 35.2% rated better overall health and mental health states, respectively, at six months. Sixteen (29.6%) participants became to walk at least once a week, even though they did not have such a walking habit at baseline. The number of participants who reported walking slower than before decreased from 17 (31.5%) at baseline to 6 (11.1%) at six months. Furthermore, 18 (33.3%) participants, who did not report weight loss at baseline, reported losing more than 2 to 3 kg. These five items all showed statistically significant results, with all p-values <0.001. In terms of social aspects, most of the participants already had social participation at baseline, which remained unchanged at six months.
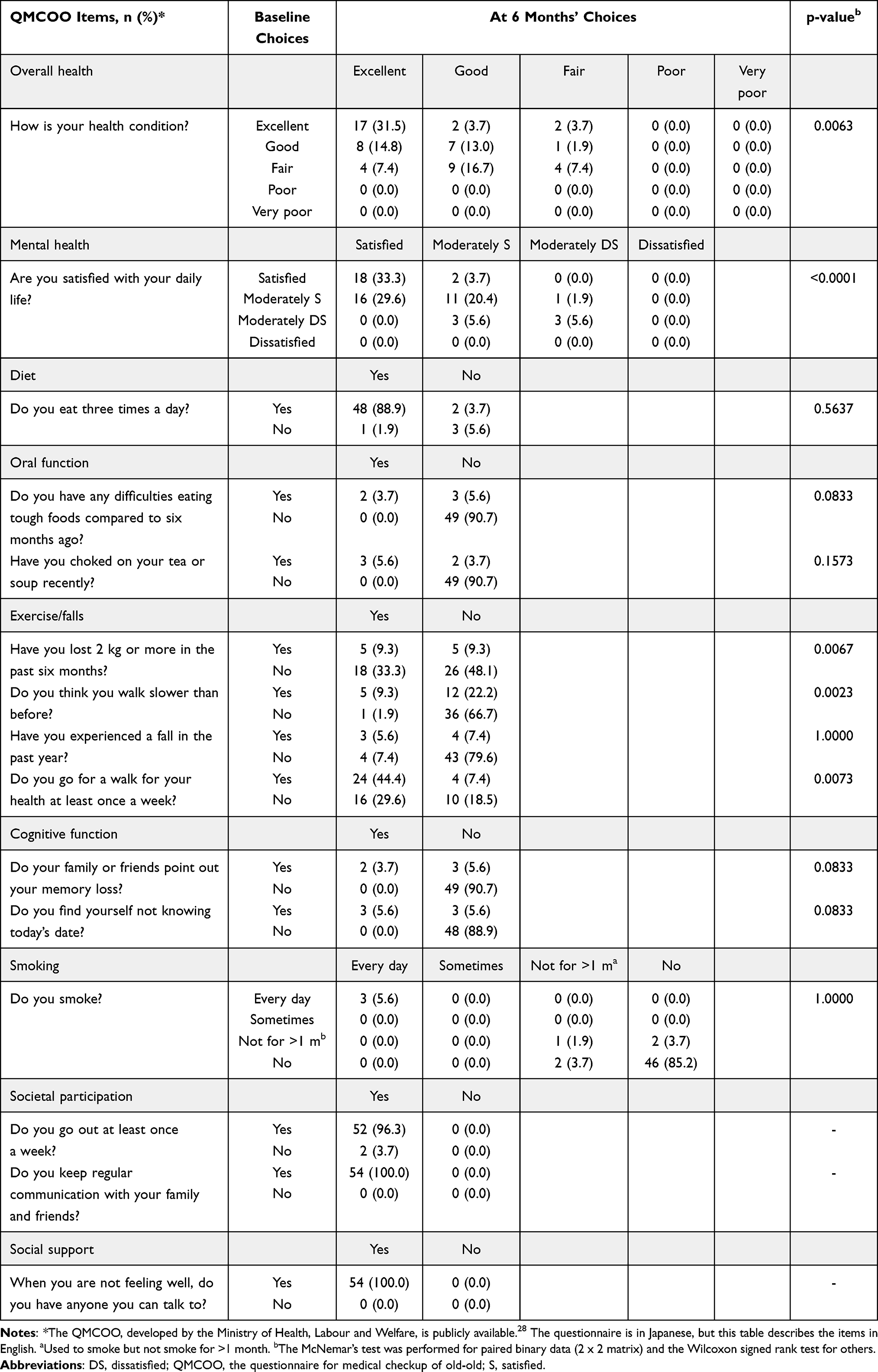 |
Table 2 A Cross-Tabulation of Participant’s Health States and Lifestyle Habits at Baseline and Six Months (n = 54) |
Lifestyle Behaviors
Table 3 summarizes the participants’ attitudes toward lifestyle modifications at the end of the follow-up period. Over 85% of the participants considered that they have become more proactive in improving their lifestyles regarding salt intake, diet, weight loss, and exercise (combined proportion of “yes” and “somewhat yes”: 85.2–96.3%). However, alcohol consumption and smoking habits seemed more challenging to change, with 28.6% and 66.7% of the participants with drinking and smoking habits, respectively, responding “somewhat no” to their behavioral change. All participants answered “yes” or “somewhat yes” to have the intention to continue improving their lifestyles.
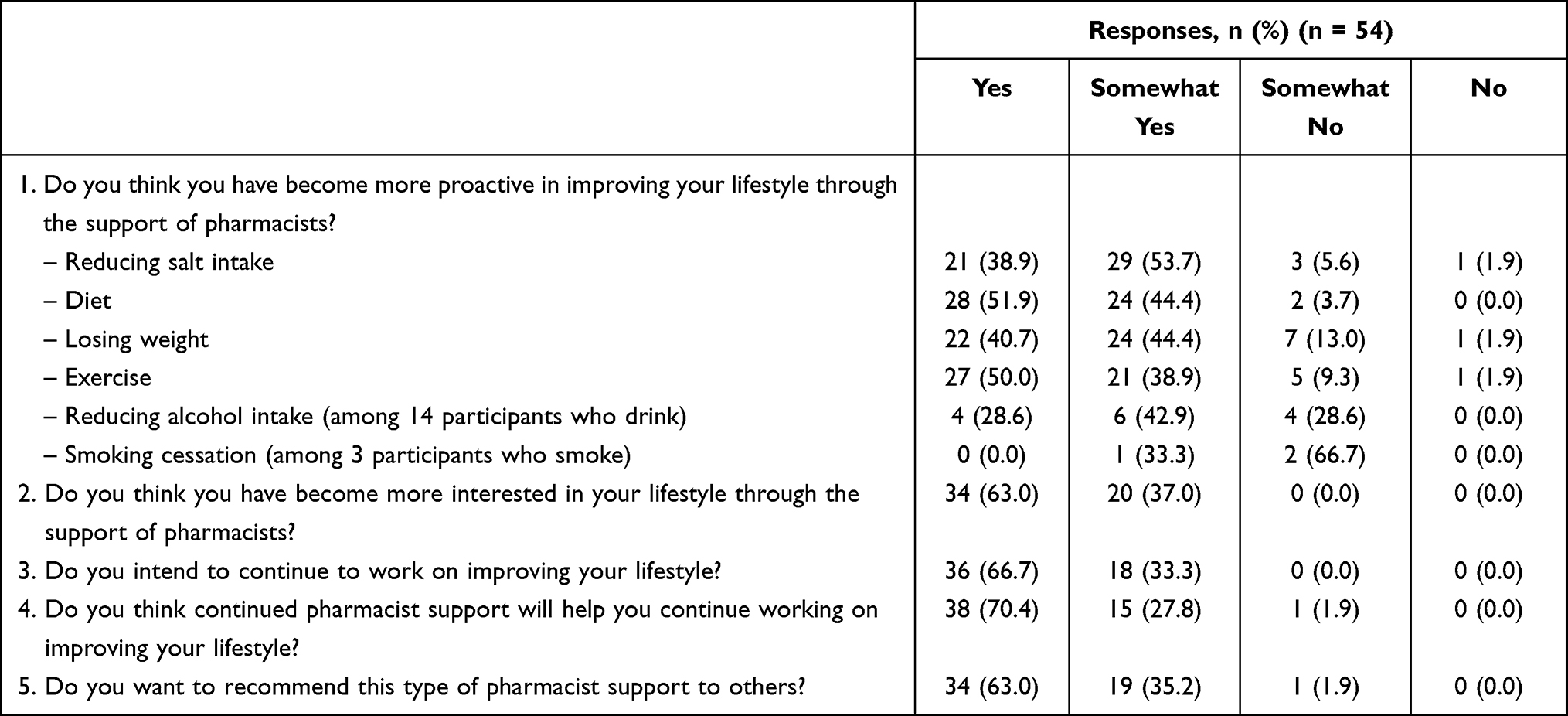 |
Table 3 The Participants’ Perception of Lifestyle Modification at Six Months |
Evaluation of Pharmacists’ Lifestyle Modification Support
Table 4 summarizes the evaluations by the participants and pharmacists of pharmacist support. The participants’ responses were favorable for all four questions. There was no notable discrepancy in trends; the majority (64.8–75.9%) chose the same response choices between the participants and pharmacists. However, overall, pharmacists rated items less positively than participants, resulting in poor to fair agreement between pharmacists and participants (weighted kappa coefficients: 0.01–0.34). Both participants and pharmacists predominantly reported that the trusting relationship had deepened through support (yes: 81.5% and 70.4%; somewhat yes: 18.5% and 24.1%, respectively). However, 12 pharmacists (22.2%) rated lower than the participants, with 3 (5.6%) rating “somewhat no” or “no.”
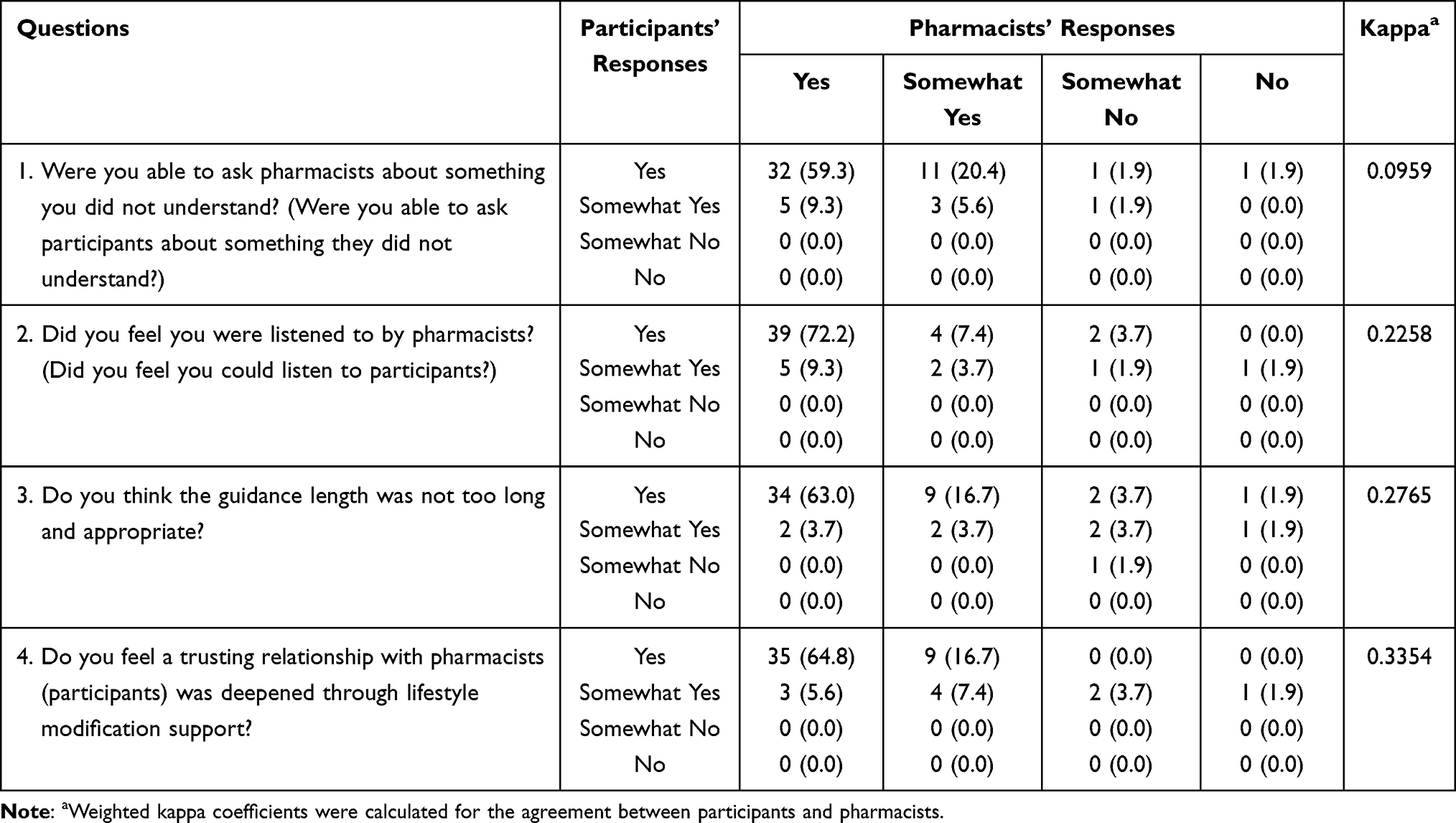 |
Table 4 Evaluation of Pharmacists’ Support from the Perspective of Participants and Pharmacists (n = 54 for Each) |
Illustrative Cases
Here, two illustrative cases of improved health parameters are introduced. The first case was a 58-year-old man with spinal canal stenosis who did not take antihypertensive medication. He was unable to change his lifestyle behaviors before the study, despite his awareness of insufficient exercise. However, in this study, he set his own goals and continued self-care for six months. Consequently, his step count increased, and his systolic BP and weight were reduced. He was satisfied with his participation in this study and reported that it was a good motivation for behavioral change. The other case was a 72-year-old man who did not take antihypertensive medication. He had stomach cancer nine years prior and wanted to increase his weight. He reported that participation in this study increased his interest in dietary habits, which also motivated his wife, leading to an improvement in their dietary balance. Consequently, his caloric intake and weight increased.
Discussion
This study explored whether community pharmacies’ self-care support was feasible for health promotion among community residents. It was not limited to people at a higher risk of lifestyle diseases but included healthy individuals. We observed nearly stable mean BP levels in the study population. However, the participants became more interested in their lifestyles and proactive in their improvement through the support of community pharmacists. The results of this study not only showed the potential of this type of pharmacy support but also provided insights into future improvements.
This study used several digital devices to measure and record health data. Digital devices can help effectively improve lifestyle behaviors,32 involving or enabling behavior change techniques, such as goal setting, self-monitoring, self-motivation, and self-evaluation.33 Healthcare professionals’ feedback constitutes an important element in lifestyle intervention, but they are mostly provided based on people’s self-reports rather than objective data.34 However, in this study, active data tracking enabled pharmacists to provide more accurate, individualized advice based on objective performance data. The availability of such tailored feedback may have somewhat motivated the participants’ continuous engagement in self-measurements, such as twice-a-day BP and daily weight measurements. However, other factors may also have been responsible for such active engagement or high self-care continuation rate (no dropout) in this study, such as better physical and psychological accessibility to community pharmacies than to hospitals or the possibility of seeking social interaction arising from a feeling of loneliness due to the coronavirus pandemic.35
Despite active engagement, the mean values of BP and other parameters remained almost constant over the study period. There was even a decrease in the mean number of steps taken in the later study period. There are several possible explanations for this result. First, this study included many healthy individuals with normal BP and body mass index at baseline. Thus, some may not have targeted a drastic behavioral change but instead pursued maintaining health. Second, seasonal variation in BP may have offset the decline in BP due to lifestyle improvements. There is an inverse association between home BP and temperature, with an approximately 7 mmHg difference between the summer and winter seasons in Japan.36 Since the study started in the summer, the participants would have had higher BP toward the end of the study in winter. However, there was no such increase in BP. Lifestyle modifications may have prevented the seasonal rise in BP to some extent. This seasonal factor may also explain the reduced step count in the later study period, that is, the winter season.37 Given these, our results may not necessarily indicate the insufficient effect of pharmacists’ support. Its impact on health parameters should be further examined in future comparative studies.
Another aspect to consider is that each participant had different motivations and goals. As previously illustrated, some individuals intended to lose weight, but there were also individuals who wished to increase their weight. Some participants may have aimed to improve food balance or increase muscle training; however, such an improvement may not have been adequately captured in our measurements. Thus, even if there were some improvements at the individual level, lumping them together may have obscured improvements in the parameters at the population level. In real-world practice, it is crucial to provide tailored health support considering individual situations, using effective behavior change techniques such as goal setting and action planning.38,39
The participants evaluated pharmacist support positively. Almost all participants reported that they became more proactive in improving their lifestyles, such as salt intake, diet, weight control, and exercise, although changing their smoking and drinking habits appeared to be more challenging. Not only did they become more conscious about each lifestyle habit, but many participants also felt improvement in well-being; more than one in three participants improved their overall health state (38.9%) and mental health state (35.2%) from baseline. Moreover, all the participants responded that they intended to continue improving their lifestyles. In addition to previous reports,23,40 our results demonstrate that community pharmacies have tremendous potential for promoting health and facilitating self-care among community residents.
In line with a previous report,41 the participants in this study appreciated the usefulness of pharmacist support, and almost all reported that they wanted to recommend it to others. Given their potential and people’s demands, these activities of community pharmacies should be facilitated and prevail across Japan. However, there seems to be much room for improvement in such health support programs. For example, devices and apps may pose a hurdle for older adults. Too many devices may be burdensome, hindering continuation, as suggested by the slight decrease in the number of participants who measured step count or recorded diet. Therefore, pharmacists should tailor the method depending on people’s goals and accessibility to devices. It may also be worth establishing a cooperative support system between pharmacies and health device providers.
Public health promotion is essential for achieving a sustainable health system in Japan. Improving people’s health so that citizens can play an active role in improving their own health is the foundation for health promotion among the public, and proper education is essential for its improvement.42 The Japanese government considers communities as the foundation of the health system that should play an important role in health promotion.43 Community pharmacists should play a significant role in public health and health literacy promotion in their communities through education or active involvement in people’s self-care support, as in our attempt.
This study was unique and significant in that it used objective measures in addition to subjective evaluations and was not exclusive to people at high risk of certain conditions. However, it also has certain limitations. First, the generalizability of the results may be limited due to selection bias. For example, participants who voluntarily participated in the study were more likely to be health conscious, which probably underlies their overall active engagement. Second, the self-measured data may not be accurate; participants may have taken repeated measurements or recorded arbitrarily to submit favorable data. Additionally, the overall too-low caloric intake (around 1600 kcal) for the estimated energy requirement of the Japanese44 suggests improper data input, let alone limited accuracy.30 Finally, the lack of a control group restricted us from examining the causal association between self-care and health parameters, which should be determined in future comparative studies. However, this type of exploratory and descriptive study is extremely important to help generate hypotheses to be tested in further analytic research.45,46
Conclusions
The results of this study suggest that community pharmacists’ support helped increase health awareness among pharmacy visitors and promote their health-enhancing behaviors. The participants’ overall well-being improved, and they appreciated the pharmacists’ support. However, its impact on objective parameters should be further examined in future research. Also, more vigorous, tailored self-care support may be worth considering in the future. We believe that the promising results and challenges highlighted in this study will help community pharmacies develop a more practical, effective, and community-fitted health/well-being support system by promoting health literacy in Japan.
Acknowledgments
We thank all the participants and participating pharmacies belonging to the Ogaki Pharmacists Association. Statistical analyses and medical writing support were provided by Clinical Study Support, Inc., with funding from the Japan Selfcare Promotion Association.
Author Contributions
YH, HN, TN, YK, TI, and MH contributed to the conception of the study. YH and SM significantly contributed to the study design, execution, data acquisition, and data analysis/interpretation. YH and SM primarily drafted the manuscript, and the others critically reviewed or revised it. All authors agreed 1) to the journal to which they would submit the manuscript, 2) to the final version of the manuscript for submission, and 3) to take responsibility and be accountable for the contents of the manuscript.
Funding
This study was funded by the Japan Selfcare Promotion Association. The sponsor had no involvement in the study design, data collection and analysis, and preparation of the manuscript.
Disclosure
Takamasa Nakamura is an employee of Clinical Study Support, Inc. Yoshihito Kato is an employee of Kowa Company, Ltd. Tatsuya Isomura is a board member of Clinical Study Support, Inc. Michiko Hori is a board member of SIC Co., Ltd. The other authors have no conflicts of interest to declare.
References
1. World Health Organization. World health statistics 2022: monitoring health for the SDGs, sustainable development goals. Available from: https://www.who.int/data/gho/publications/world-health-statistics.
2. Ministry of Health, Labour and Welfare. Establishing the Community-based Integrated Care System. Available from: https://www.mhlw.go.jp/english/policy/care-welfare/care-welfare-elderly/index.html.
3. Ministry of Health, Labour and Welfare. The State of Health Support Pharmacies. Available from: https://www.mhlw.go.jp/file/05-Shingikai-11121000-Iyakushokuhinkyoku-Soumuka/matome.pdf.
4. Cabinet Office, Government of Japan. Basic Policy on Economic and Fiscal Management and Reform 2022. Available from: https://www5.cao.go.jp/keizai-shimon/kaigi/cabinet/2022/2022_basicpolicies_en.pdf.
5. Prochaska JO, Velicer WF. The transtheoretical model of health behavior change. Am J Health Promot. 1997;12(1):38–48.
6. Ministry of Health, Labour and Welfare. Healthy Life Expectancy in 2019. Available from: https://www.mhlw.go.jp/content/10904750/000872952.pdf.
7. OECD. Fiscal Sustainability of Health Systems: Bridging Health and Finance Perspectives. Paris: OECD Publishing; 2015.
8. Ministry of Health, Labour and Welfare. A Basic Direction for Comprehensive Implementation of National Health Promotion. Available from: https://www.mhlw.go.jp/file/06-Seisakujouhou-10900000-Kenkoukyoku/0000047330.pdf.
9. Benziger CP, Roth GA, Moran AE. The Global Burden of Disease Study and the Preventable Burden of NCD. Glob Heart. 2016;11(4):393–397.
10. World Health Organization. Global NCD target: reduce high blood pressure. Available from: https://apps.who.int/iris/rest/bitstreams/1217190/retrieve.
11. World Health Organization. Global action plan for the prevention and control of noncommunicable diseases 2013–2020. Available from: https://www.who.int/publications/i/item/9789241506236.
12. The Japanese Society of Hypertension. Guidelines for the Management of Hypertension 2019 (JSH 2019). Tokyo: Life Science Publishing; 2019.
13. Ikeda N, Inoue M, Iso H, et al. Adult mortality attributable to preventable risk factors for non-communicable diseases and injuries in Japan: a comparative risk assessment. PLoS Medicine. 2012;9(1):e1001160. doi:10.1371/journal.pmed.1001160
14. Ministry of Health, Labour and Welfare. Plans for Extension of Healthy Life Expectancy. Available from: https://www.mhlw.go.jp/content/12601000/000514142.pdf.
15. Ye L, Elstgeest LEM, Zhang X, Alhambra-Borrás T, Tan SS, Raat H. Factors associated with physical, psychological and social frailty among community-dwelling older persons in Europe: a cross-sectional study of Urban Health Centres Europe (UHCE). BMC Geriatr. 2021;21(1):422.
16. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. 2013;381(9868):752–762.
17. Hanlon P, Nicholl BI, Jani BD, Lee D, McQueenie R, Mair FS. Frailty and pre-frailty in middle-aged and older adults and its association with multimorbidity and mortality: a prospective analysis of 493 737 UK Biobank participants. Lancet Public Health. 2018;3(7):e323–e332.
18. Kojima M, Satake S, Osawa A, Arai H. Management of frailty under COVID-19 pandemic in Japan. Glob Health Med. 2021;3(4):196–202.
19. Rutter P. Role of community pharmacists in patients’ self-care and self-medication. Integr Pharm Res Pract. 2015;4:57–65.
20. Agomo C, Udoh A, Kpokiri E, Osuku-Opio J. Community pharmacists’ contribution to public health: assessing the global evidence base. Pharm J. 2018;10:4.
21. Brown TJ, Todd A, O’Malley CL, et al. Community pharmacy interventions for public health priorities: a systematic review of community pharmacy-delivered smoking, alcohol and weight management interventions. Public Health Res. 2016;4:2.
22. Steed L, Sohanpal R, Todd A, et al. Community pharmacy interventions for health promotion: effects on professional practice and health outcomes. Cochrane Database Syst Rev. 2019;12(12):Cd011207.
23. Suzuki R, Suzuki T, Kikuchi C. Improvements in lifestyle from a lifestyle consecutive self-review at a pharmacy. YAKUGAKU ZASSHI. 2019;139(7):1047–1054.
24. Kikuchi C, Yamaguchi K, Kojima M, et al. Comparative trial of the effects of continuous locomotion training provided at pharmacies: a pilot study. J Pharm Health Care Sci. 2020;6(1):24.
25. Wada Y, Wada Y, Ennyu S, Shimokawa KI, Ishii F. Ability of community pharmacists to promote self-care and self-medication by local residents [I]: improvements in bone mineral density. Drug Discov Ther. 2017;11(1):35–40.
26. Okada H, Onda M, Shoji M, et al. Effects of lifestyle advice provided by pharmacists on blood pressure: the COMmunity Pharmacists ASSist for Blood Pressure (COMPASS-BP) randomized trial. Biosci Trends. 2018;11(6):632–639.
27. Noble K, Brown K, Medina M, et al. Medication adherence and activity patterns underlying uncontrolled hypertension: assessment and recommendations by practicing pharmacists using digital health care. J Am Pharm Assoc. 2016;56(3):310–315.
28. Ministry of Health, Labour and Welfare. Explanation and Notes on the Questionnaire for the Late Elderly. Available from: https://www.mhlw.go.jp/content/000605506.pdf.
29. Satake S, Arai H. Questionnaire for medical checkup of old-old (QMCOO). Geriatr Gerontol Int. 2020;20(10):991–992.
30. Sasaki Y, Sato K, Kobayashi S, Asakura K. Nutrient and Food Group Prediction as Orchestrated by an Automated Image Recognition System in a Smartphone App (CALO mama): validation Study. JMIR Form Res. 2022;6(1):e31875.
31. Altman DG. Practical Statistics for Medical Research.
32. Chatterjee A, Prinz A, Gerdes M, Martinez S. Digital Interventions on Healthy Lifestyle Management: systematic Review. J Med Internet Res. 2021;23(11):e26931.
33. Manzoor A, Ali I, Khokhar S, Hussain N, Sulleman M. Formalization of behavior change theories to accomplish a health behavior. Int J Adv Comput Sci Appl. 2018;9(5):177–182.
34. Bossen D, Bak M, Braam K, et al. Online and Offline Behavior Change Techniques to Promote a Healthy Lifestyle: a Qualitative Study. Int J Environ Res Public Health. 2022;19(1):521.
35. IbashoChat. org., Japan Science and Technology Agency. Survey on People’s Loneliness under COVID-19. Available from: https://www.jst.go.jp/pr/announce/20220224/pdf/20220224.pdf.
36. Iwahori T, Miura K, Obayashi K, et al. Seasonal variation in home blood pressure: findings from nationwide web-based monitoring in Japan. BMJ Open. 2018;8(1):e017351.
37. Yasunaga A, Togo F, Watanabe E, et al. Sex, age, season, and habitual physical activity of older Japanese: the Nakanojo study. J Aging Phys Act. 2008;16(1):3–13.
38. Lenzen SA, Daniëls R, van Bokhoven MA, van der Weijden T, Beurskens A. Disentangling self-management goal setting and action planning: a scoping review. PLoS One. 2017;12(11):e0188822.
39. Samdal GB, Eide GE, Barth T, Williams G, Meland E. Effective behaviour change techniques for physical activity and healthy eating in overweight and obese adults; systematic review and meta-regression analyses. Int J Behav Nutr Phys Act. 2017;14(1):42.
40. Fujita N, Nabetani N, Umemura N, Kikuchi C, Suzuki T. Lifestyle Improvement through Continuous Measurements of Hemoglobin A1c Levels and Lifestyle Checks at the Community Pharmacy in Three Cases. YAKUGAKU ZASSHI. 2016;136(10):1445–1448.
41. Hirota N, Okamura N. Patients’ Attitudes, Awareness, and Opinions About Community Pharmacies in Japan: next Steps for the Health Support Pharmacy System. Integr Pharm Res Pract. 2020;9:243–256.
42. World Health Organization. WHO guideline on self-care interventions for health and well-being, 2022 revision. Available from: https://www.who.int/publications/i/item/9789240052192.
43. Cabinet Secretariat, Office of Healthcare Policy. Global Health Strategy. Available from: https://www.kantei.go.jp/jp/singi/kenkouiryou/senryaku/r040524global_health.pdf.
44. Ministry of Health, Labour and Welfare. Overview of the Dietary Reference Intakes for Japanese (2020). Available from: https://www.mhlw.go.jp/content/10900000/000862500.pdf.
45. Albrecht J, Meves A, Bigby M. Case reports and case series from Lancet had significant impact on medical literature. J Clin Epidemiol. 2005;58(12):1227–1232.
46. Kooistra B, Dijkman B, Einhorn TA, Bhandari M. How to design a good case series. J Bone Joint Surg Am. 2009;91(Suppl 3):21–26.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.