Back to Journals » Risk Management and Healthcare Policy » Volume 15
Exploring Blood Donation Challenges and Mobilization Mechanisms in North China During the COVID-19 Pandemic: A Qualitative Study
Received 30 April 2022
Accepted for publication 7 August 2022
Published 27 August 2022 Volume 2022:15 Pages 1593—1605
DOI https://doi.org/10.2147/RMHP.S372945
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Haiyan Qu
Zhuo Wang,1,2 Hejian Wang1
1School of Social and Behavioral Sciences, Nanjing University, Nanjing, People’s Republic of China; 2The National Police University for Criminal Justice, Hebei, People’s Republic of China
Correspondence: Zhuo Wang, School of Social and Behavioral Sciences, Nanjing University, Nanjing, People’s Republic of China, Tel +86 15062263226, Email [email protected]
Purpose: The coronavirus disease 2019 (COVID-19) pandemic disrupted the supply of blood globally, resulting in numerous studies focusing on the challenges in maintaining blood supply, and the responses to it, in countries with a mixed blood donation model. This study explored blood donation challenges and mobilization mechanisms in North China, which employs a non-remunerative donation model, during the COVID-19 pandemic’s first wave.
Materials and Methods: A qualitative approach was adopted to investigate blood donation practices in Chengde from April to June 2020. Data were collected from eight blood donors, six potential donors, three blood donation station leaders, and two government officials, through semi-structured interviews.
Results: The major challenge for blood supply was decreased blood donations, owing to lockdown restrictions, and individual and familial apprehensions. Mobilization mechanisms included bureaucratic and ideological mobilization. However, although group blood donation alleviates the pressure on supply chains during emergencies, it is detrimental to the cultivation of civic engagement in the long run.
Conclusion: This study contributes to the understanding of how countries with uncompensated blood donation models respond to public health emergencies. It suggests that striking a balance between the society’s and the state’s perception of blood donation would allow the state to incorporate the different “voices” of society, and devise an inclusive blood donation policy.
Keywords: global health, health policy, COVID-19, blood shortage, qualitative research
Introduction
In March 2021, the World Health Organization (WHO) declared the coronavirus disease 2019 (COVID-19) a global pandemic.1 Consequently, countries worldwide declined not only in their economic development but also in health care services due to unprecedented challenges like difficulties in maintaining blood supply.2,3 Some countries had to close their blood donation centers.4 In the face of these circumstances, many countries changed their blood supply policy, such as by introducing eligibility criteria for blood donors.5,6 The long incubation period of the COVID-19 virus and the presence of asymptomatic carriers poses considerable challenges in recruiting blood donors.7 Previous studies have suggested that disasters provide an opportunity for increasing blood supply.8–11 However, the COVID-19 pandemic led to a plunge in the blood supply in several countries.3,4,12–14 In response to the inadequate blood supply, hospitals implemented measures like postponing elective and nonemergency surgeries.12,15,16 To prevent the disease from spreading further, patients with chronic diseases were advised to use telemedicine, with deaths occurring due to the inability to access medical care on time.17 While previous studies elucidate the problems and social impact of blood shortages in countries with mixed donation models, they do not focus adequately on the challenges faced by countries with uncompensated blood donation models.
In the face of serious blood supply challenges during the COVID-19 pandemic, several studies have focused on the causes of blood supply shortages in various countries and their coping strategies. On the one hand, the government implemented an embargo for effectively preventing the virus from spreading.18 The implementation of such strict social policies led to the cancellation of blood collection activities, thereby pressurizing the blood supply chain.16,19,20 On the other hand, individuals were reluctant to participate in voluntary, unpaid blood donations for fear of contracting the virus.21–23 In response to the dramatic decline in blood supply, some countries sought to facilitate blood donation through measures like increasing mobile blood collection drives,24,25 and using social media platforms to mobilize individuals.26–28 Other countries addressed blood shortages by establishing a national information technology infrastructure to connect all blood operators and included hospitals in the reporting structure.29,30 However, while these studies are rich in listing specific strategies of countries with mixed blood donation models, they do not consider blood donation mobilization mechanisms in countries with uncompensated blood donation models.
This study explored the challenges faced by North China’s blood donation and mobilization mechanisms during the first wave of the COVID-19 pandemic to fill the theoretical gap in addressing the blood supply issues in such countries during major public health crises. North China was chosen in this study because of its typical blood donation model, having implemented a 100% voluntary, non-remunerative blood donation policy since 1998. In addition, because this study obtains data from a specific field, it might provide lessons to countries with a no-cost blood donation policy regarding handling blood supply shortages. The study focuses on the following questions: (i) What were the blood supply-related challenges in North China, which has a 100% voluntary, non-remunerative blood donation policy, during the first wave of the COVID-19 pandemic? (ii) Which blood donation mobilization mechanisms did North China use to respond to the blood supply shortage caused by the COVID-19 pandemic?
Materials and Methods
Various research methods have been applied to study the impact of the COVID-19 pandemic on blood supply.3,7,31 The health policy field most often uses qualitative research designs because quantitative research does not allow for in-depth analysis of a policy’s development process or social impact.32 Moreover, generic qualitative research methods require less inferential interpretation than rooted theory, ethnography, and narrative research.33 The present study used a generic qualitative research approach as its focus was on specific actions, rather than a simple set of numbers, and dynamic processes of the target empirical phenomena.34 Further, a qualitative approach facilitates in-depth exploration of the social meaning underlying the targeted empirical phenomenon.35 However, although qualitative methods better explain the typicality of a research subject, they are not as representative as quantitative methods, which also require less time. Nonetheless, quantitative methods cannot explain the specific details of the action process.36 Considering this study’s focus on determining North China’s challenges to blood supply and the mobilization mechanisms of blood donation during the pandemic, we opted for a qualitative research approach.
Research Site
Following the principles of importance and representativeness in academic research, we selected the city of Chengde as our research site. As a typical blood donation mobilization site in North China, Chengde is representative of other cities with similar characteristics in terms of blood donation mobilization in response to emergencies. It is adjacent to the national capital Beijing and is its most important supplier of interprovincial blood resources for redeployment. In addition, Chengde was the first region in Hebei Province to implement the blood donation policy advocated by the state. Since 1998, it has accumulated rich experience in blood donation mobilization. During the COVID-19 pandemic, local mobilization activities were carried out effectively, and 80,000 mL of red blood cells and 50,000 mL of plasma were successfully collected for Wuhan, the most severely affected city in 2020.
Further, the choice of research site was based on the need to fill theoretical gaps and develop new theories.37 Existing literature has rarely focused on blood donation mobilization in small cities in countries with a 100% voluntary, non-remunerative blood donation policy. Choosing Chengde helps shed light on the state of blood supply and mobilization mechanisms under such a donation system during emergencies, thereby contributing to research on both health policy and social mobilization. Finally, by selecting Chengde, we could ensure that our theoretical objectives matched with the case subjects.38 We were impressed by the valuable role of bureaucratic and ideological mobilization in Chengde’s blood donation process and the readily available data.
Participants
Any qualitative study requires a sample size of 12 or more respondents to ensure reliability.39 We determined that a sample size of 19 individuals was feasible and sufficient for exploring our research questions. The participants comprised eight blood donors, six potential donors, three blood bank leaders, and two government officials. The donors and potential donors were selected to understand their reasons for participating or not participating in blood donation operations during the COVID-19 pandemic. The blood donors in this study were those whose physical health condition met the Chinese blood donation standards, who were between 18 and 60 years old, and who had already donated 200 mL, or 300 mL or 400 mL of blood during COVID-19. We chose to interview blood donors of different occupations, genders and ages in order to highlight the representation of blood donors. Potential donors are mainly those who are in good health and meet the Chinese blood donation standards, are between the ages of 18 and 60, and have not yet participated in blood donation during COVID-19. We took into account the diversity of potential blood donor types and interviewed potential donors who received macro-, meso-, and micro-factors separately. Blood bank leaders were selected to understand the impact of public health emergencies on the local blood supply, and how blood donation mobilization was conducted. We chose these people based on the criteria that they have been working in this blood bank for more than 10 years. Not only do they have a good understanding of blood donation in the city at different times, but also they are responsible for different tasks, such as blood supply and demand distribution work, blood collection safety work and blood donation mobilization work. Blood donation mobilization in North China is usually associated with the bureaucratic operation of the government, so we interviewed 2 government officials associated with blood donation mobilization to understand how they worked with blood donation stations to address the inadequate blood supply during a pandemic. The leaders of the blood banks in this study were from the same blood bank, and the government officials were all in direct business with the staff of that blood bank. Therefore, we applied a purposive sampling method to achieve a deeper understanding of the study population through richer, multifaceted data.35 Table 1 summarizes the participant’s demographic characteristics. A total of 19 interviews were conducted: 42.10% (n = 8) with blood donors, 31.57% (n = 6) with potential donors, 15.78% (n = 3) with blood bank leaders, and 10.52% (n = 2) with government officials. Overall, 31.57% of participants (n = 6) identified as female and 68.43% as male (n = 13).
 |
Table 1 Participant Characteristics |
Data Collection
The interview format comprised open-ended questions. During data collection, we used a semi-structured interview method to ensure consistent collection of information on the research topic, namely blood supply and donation mobilization in North China during COVID-19, and to avoid collecting scattered or irrelevant information.40 It also allowed the interviewees to respond flexibly and express their thoughts and feelings completely.41 To clarify whether our interview design was effective in collecting the required information and to have an accurate idea of the amount of interview time needed, a pilot survey was conducted prior to the formal interviews. Relevant information was collected through face-to-face interviews, as well as cell phones and the WeChat app, on two different occasions, from April to June (interview protocol is shown in Table 2). In each case, we communicated with the interviewees in advance and obtained informed consent, and we made audio recordings to facilitate transcription and analysis. To ensure accurate information, we checked the transcriptions word-for-word against the recordings.
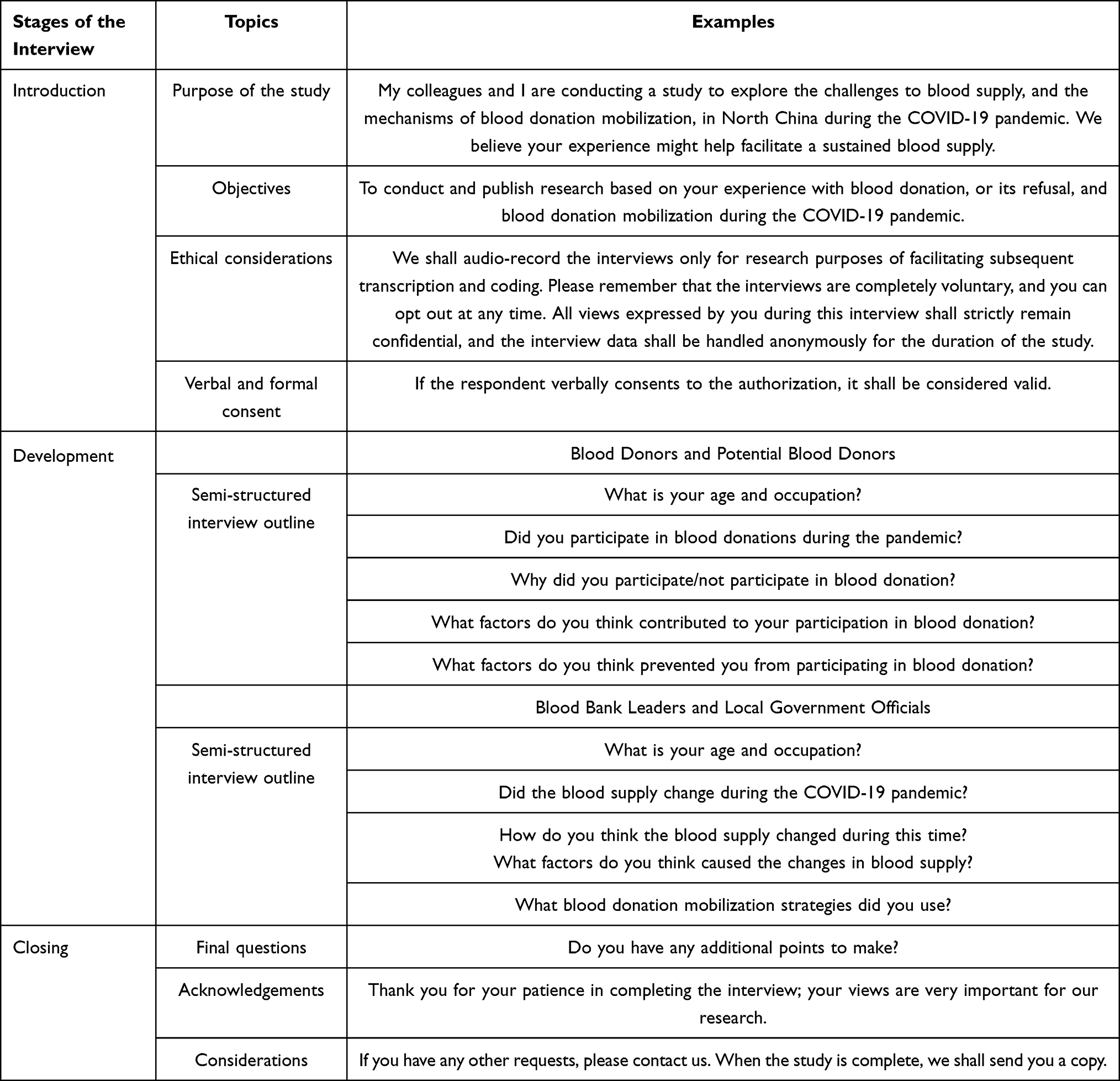 |
Table 2 Interview Protocol |
Data Analysis
The collected data were analyzed using thematic analysis, a method used to identify important research themes.42 This method was selected because: (i) it provides an entry point for qualitative research, allowing researchers to scientifically analyze qualitative data relevant to the research questions through systematic coding,43 and (ii) it identifies and makes sense of patterns of meaning across a dataset.44 We read the transcribed interviews carefully and created inductive codes. These were then combined with deductive codes from the literature to create the final list of codes. We followed the procedures for conducting qualitative data analysis. Prior to conducting the thematic analysis, each author thoroughly read the transcription. There are two coders in this study. NVivo 11 was used to code and organize the data. During the analysis, the first researcher grouped the data we had collected and explored patterns between the data. Excerpts from the collated interview data were linked to the inductive codes, based on which the themes and sub-themes of this study were derived (Figure 1). Data were presented in a narrative format and interpreted based on the researcher’s interpretation. Independently validated by the second researcher, thus ensuring that the data analysis followed the principles of triangulation validation.
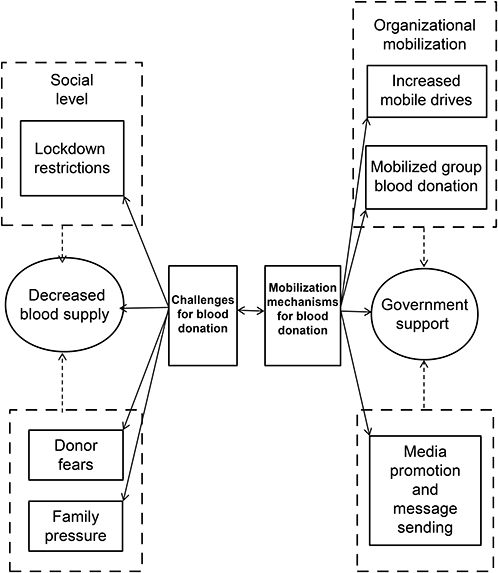 |
Figure 1 Blood supply-related challenges and mobilization mechanisms in North China. |
Ethical Considerations
We reported on determination of sample size, all data exclusions, all manipulations, and all measures employed in the study. This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Nanjing University (approval number: [SS02]; approval date: March 3, 2020). All participants were informed in advance that participation was voluntary. Their consent was obtained to record the interviews.
Results
Their ages ranged from 21 to 60 years old. Qualitative analysis revealed two main themes, summarized in Table 3.
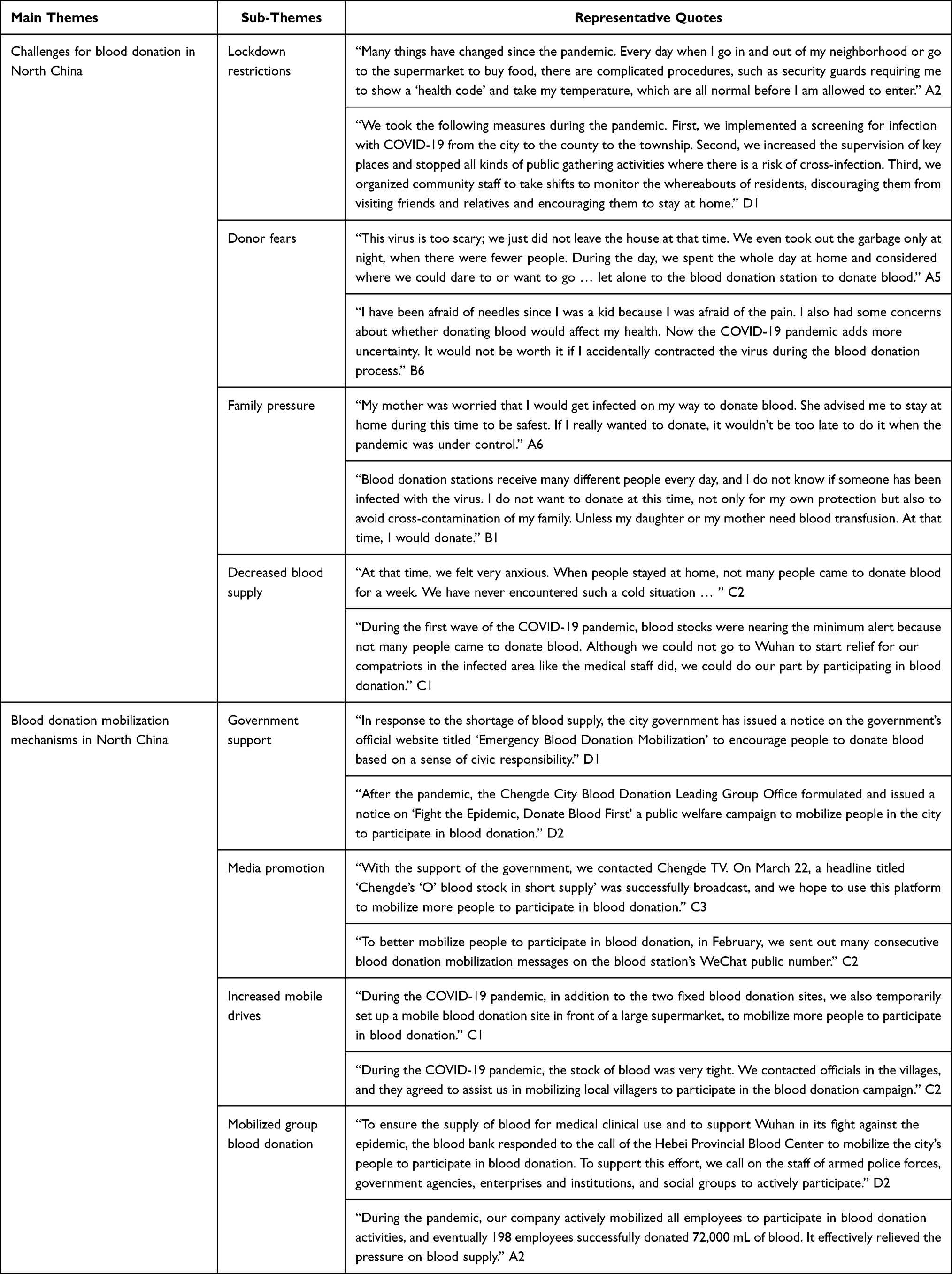 |
Table 3 Main-Themes, Sub-Themes, and Representative Quotes |
Theme 1: Challenges to Blood Donation in North China
This theme covers the challenges to blood supply faced by North China during the COVID-19 pandemic. Our results show that the COVID-19 pandemic had a significant impact at both social and individual levels. At the social level, it led to a social policy of lockdown restrictions, making it difficult for individuals to move freely and participate in blood donation stations. At the individual level, it increased the fear of getting infected with the virus as a result of donating blood. In addition, some families were reluctant to let members go out and participate in social affairs (including blood donation) for the sake of the entire family’s safety. Influenced by these factors, blood donors and potential donors reduced their participation in blood donations during the pandemic. This resulted in a decrease in blood supply in North China compared to the pre-pandemic period.
Sub-Theme 1.1 Lockdown Restrictions
Most participants reported that the first wave of the pandemic disrupted their lives and rhythm of work. At the personal level, changes in everyday life included strict entry and exit procedures in the neighborhoods, and the need to wear masks and measure body temperature when shopping at the supermarket. At the social level, lockdown policies for containing the spread of the virus led the government to close many public places, including social and recreational venues. Although the government’s implementation of a strict lockdown policy contained the spread of the virus, it simultaneously decreased social mobility. One of the blood bank leaders highlighted a direct result, that when people went out less, the number of blood donations plummeted in comparison to the same period in the past:
At that time, we were really anxious. When people were at home hiding from the virus, that’s when we were out on the street looking left and right! We were really looking forward to having people come to donate blood. But unfortunately, there was no movement ….We have never been so worried, and we were always on tenterhooks. (C1)
Sub-Theme 1.2 Donor Fears
Some participants said that the COVID-19 pandemic had a negative impact on their participation in blood donation. The majority of those who had donated blood in the past now feared contracting the virus on the way to, or during, the blood donation process. Most potential donors were afraid of the pain and worried about blood donation’s consequences for their health. The new risks brought about by the pandemic made them even more reluctant to donate blood. In fact, in addition to the fear of contracting the virus, potential donors believed that the incentives for donating blood were inadequate:
It costs time and transportation to donate blood, but we are not reasonably compensated for these costs after we donate. Obviously, donating blood is an irrational thing for me to do, so why should I do it? (B5)
Sub-Theme 1.3 Family Pressure
Several interviewees, including blood donors and potential donors, stated that their families were reluctant about their going out socially during the pandemic, including for donating blood. One blood donor noted that his parents had advised him to stop going out to participate in blood donations for the time being for the sake of his safety; he could resume when the pandemic subsided. Potential donors stated that they would donate blood only if their friends or relatives need a clinical transfusion. One of the potential donors reported that her husband did not agree with her participation in the blood drive from a cost-benefit perspective.
My husband told me that he had participated in group blood donation organized by the company he worked for. He had accumulated more than 1000 mL of blood in recent years, which was enough for meeting the preferential conditions for family members’ clinical transfusion needs for some time to come. He believed that during a pandemic, there was no other benefit of participating in blood donation than the risk of getting infected. (B4)
The quantitative standard of 1000 mL mentioned above is part of the “Hebei Province Blood Donation and Clinical Blood Reporting (Refund) Standards” issued by Hebei Province, which clearly states in Articles 9 and 10 that blood donation is beneficial not just to donors themselves but also to their spouses and immediate family members.
9. If a blood donor donates less than 1000 mL of blood, he or she shall be refunded three times the amount of blood donated, and his or her spouse and immediate family members shall be entitled to “free blood equivalent to the amount of blood donated”, the cost of which shall be calculated separately for himself or herself and the person concerned.
10. Those who donate up to 1000 mL of blood shall be entitled to unlimited free blood for life and shall be reimbursed according to the actual amount of blood used in the clinic; the spouse and immediate family members of the donor shall be reimbursed according to the amount of blood donated by them.
The present study found another interesting phenomenon. Some repeat blood donors, although discouraged by their families, continued donating blood in secret and hid this from their family members.
Whenever I donate blood, I am afraid to let my family know for fear that they will worry. Especially my elderly mother, who said it was a time of pandemic, and it was not safe outside, including in blood donation stations. She told me to go out less and have as little contact with others as possible to avoid catching the virus. Her words made sense, so I did wait and see for a while, not leaving to donate blood at the height of the pandemic. It was only after I found out that the pandemic was not so serious that I went to donate blood. But even now, she does not know that I donated blood because I have not told her. (A7)
Sub-Theme 1.4 Decreased Blood Supply
In this study, a local government official stated that the COVID-19 pandemic further pressured an already fragile blood supply system and further exacerbated the public health crisis. Blood supplies declined from the same period prior to the pandemic:
The sudden drop in blood supply in 2020 was a special case, wherein people did not come out much in the first six months during the COVID-19 pandemic. Under the dual pressure of losing repeat donors and not adding new ones, the blood supply decreased by 30% compared to the same period prior to the pandemic, and blood donations in 2020 were at their lowest level in the past five years. (D2)
Theme 2: Blood Donation Mobilization Mechanism in North China
This theme covers the mobilization mechanisms for blood donation in North China during the first wave of the pandemic. At the ideological level, the government used public service announcements to promote the significance of blood donation and sent text messages to citizens to mobilize them to actively participate in street blood donations. At the organizational level, on the one hand, the government called on all their city units to mobilize their employees to participate in street blood donation. On the other hand, blood banks initiated mobile blood donation drives to facilitate greater participation in blood donation.
Sub-Theme 2.1 Government Support
As the pandemic subsided, the government introduced certain relevant policies to encourage cooperation among various sectors by enhancing the promotion, mobilization and organization of blood donation. For example, in March 2020, North China’s National Health Commission issued a circular on the “Further Implementation of Scientific Prevention and Control of Precise Policy Zoning and Grading Requirements for Blood Protection during the Epidemic,45 which included the following:
City central blood donation stations should further optimize the blood donation process, improve the blood donation environment, and strictly manage the disinfection of blood donation sites and blood collection vehicles to protect the rights and interests of blood donors, as well as the safety of blood donation. When possible, cities will be ready to coordinate telephone appointments for group blood donations from all counties (cities and districts), municipalities, and units in the city, communicate and coordinate with the organizations of each unit in a timely manner, reasonably arrange the blood collection plan, adopt batch collection, avoid concentrations of personnel, and guarantee the safe and orderly implementation of group blood donation activities. (D1)
Sub-Theme 2.2 Media Promotion and Message Sending
Through their social media accounts, provincial epidemic prevention centers sent recruitment text messages to the community, thereby expanding the scope of blood donor recruitment. These messages did encourage some people to participate. One blood donor stated:
It is our duty and immense honor to save people in distress. In school, I have always been interested in teaching my students to be socially responsible. After seeing the blood donation PSA, I did not hesitate to come and donate blood. Because I believe that leading by example is the best education. (A1)
Sub-Theme 2.3 Increased Mobile Drives
In response to the shortage of blood supply, blood banks increased the number of mobile blood donation drives to collect more blood efficiently. At the same time, the blood donation stations expanded their activities to rural areas, mobilizing farmers for blood donation. In addition, to eliminate people’s fears, one blood bank leader said they had implemented some new measures:
Considering that some blood donors were concerned about the blood donation environment in the blood banks, during the pandemic, our blood bank designed and implemented safety testing sessions, such as on-site temperature measurement for blood donors, requiring all personnel entering the blood banks to wear masks, increasing the frequency of cleaning the blood bank environment, and providing free disinfectant for donors to disinfect themselves, among other services. (C3)
Sub-Theme 2.4 Mobilized Group Blood Donation
To alleviate the pressure of blood supply shortage, the Chengde City administration strongly supported the blood donation mobilization efforts of the blood donation stations. Together with the blood donation stations, it called on employees to participate in group blood donations at the organizational level throughout the city. Several companies responded quickly and mobilized many employees to participate in group blood donations. The cooperation of various departments contributed to the success of group blood donation. One government employee said:
During the COVID-19 pandemic, with the cooperation of various departments, the number of group blood donations continued to increase, effectively increasing the blood supply. First, the government took the lead to build a platform for the cooperation between various unit organizations. Second, blood donation stations constructed an effective blood collection environment while conducting blood supply monitoring and establishing an early warning mechanism for low blood supply. Finally, other units needed to cooperate with blood donation stations and organize their members to participate in group blood donation when necessary to replenish the stock of blood donation stations in time. (C2)
Discussion
The challenges to blood supply caused by COVID-19 and the response strategies have been widely discussed.31,46,47 Existing studies mostly constitute descriptive studies of blood supply and coping strategies, and thus lack analysis of the blood supply and mobilization process in blood donation.7,15,20 Moreover, they primarily focus on countries with mixed blood donation policies21,48 and overlook countries with a 100% non-remunerative blood donation policy. The purpose of this study was to explore the challenges to blood supply and mechanisms for blood donation mobilization in North China during the COVID-19 pandemic; this allows a better understanding of how blood supply was impacted by public health emergencies in countries with a 100% non-remunerative blood donation policy and relatively effective blood donation mobilization strategies. The present study obtained intriguing findings about how group blood donation was encouraged in North China during the COVID-19 pandemic to alleviate the pressure on blood supply chains when individual participation was insufficient. This is quite a rare practice across the world. Group blood donation involved donor recruitment according to certain specific Chinese characteristics.49 Furthermore, this study provides a basis for future revisions of blood donation policies. To the best of our knowledge, this is the first empirical study that examines the mobilization mechanism of blood donation in North China during a pandemic from a sociological perspective.
Our findings revealed two aspects that significantly impacted the blood supply chain. First, at the societal level, the government’s imposition of lockdown restrictions limited individuals’ free access to public places. It has been similarly argued that governmental interventions such as mass lockdowns and curbing mass gatherings during the early stages of COVID-19 led to the suspension of voluntary blood donation camps.19,50 Second, at the individual level, people’s fear of the virus and family caused individuals to postpone blood donation. A similar study also found that 93.3% of individuals surveyed in the Eastern Mediterranean region believed that public fear had contributed to a decrease in donations.14 As a result of both these factors, North China’s blood supply declined as compared to the same period before the pandemic.
In response to the blood shortage, people were mobilized to donate blood at two levels. First, at the ideological level, blood banks encouraged people to participate in blood donation by issuing public service announcements and sending blood demand information to the public. Some studies have highlighted that an official information source has a greater influence on participants’ intentions behind donation than an unofficial source51 and that social media publicity motivates more people to donate blood.52 Second, at the organizational level, the government and blood banks worked together to mobilize the city’s organizations and their employees to participate in group blood donations. In addition, blood banks facilitated increased participation by increasing the number of mobile blood collection points. Studies have also noted that increased investment in mobile blood donation drives during the pandemic eased the pressure on the blood supply chain.2,25 In fact, such mobilization mechanisms are inseparable from government support in North China.
The effectiveness of group blood donation in ensuring stable blood supply during a pandemic is worth noting; however, adopting this mobilization model implies the introduction of bureaucracy into the practice of blood donation. In the long run, group blood donations do not foster the spirit of volunteerism among citizens. While some group donors donate blood because they are pressured by the group,53,54 others do it to receive disguised paid rewards from their organization (year-end performance points, promotion opportunities, etc.).55 This suggests that many group donors do not donate blood due to altruistic motives.
In addition, some potential donors in the present study indicated that they would donate blood voluntarily only if their family members needed it. Thus, a follow-up study would need to address whether it makes sense to eliminate group blood donation. Furthermore, in North China, potential donors have diverse perceptions of the nature of blood,56–58 with some considering it as a gift of life,59,60 others as a tie between family members,61,62 and still others as an exchangeable resource.63,64 Such varied points of view thus favor a mixed model of blood donation that incorporates non-remunerative, family substitution, and paid donations. In contrast, the government views blood only as a gift of life, promoting the non-remunerative donation model and delegitimizing the family substitution and paid donation models. This has led many potential donors to refuse donating blood. Therefore, we believe it is necessary to examine both the state and society’s perceptions of blood and strike a balance between the two to expand blood supply by including as many potential donors as possible. In addition, improving practices like testing techniques and blood collection organization management would provide a more consistent supply of safer blood, which would not only help protect the freedom to donate blood but also ensure that the blood received by patients meets quality standards.
However, this study does have certain limitations. First, a limitation of our study is that Chengde is not a representative of cities in Chinese. Although it is well represent of North China, we did not interview blood donors, potential donors, blood bank leaders, and government officials in other regions of North China (eg, Guangzhou, Shanghai, etc.). It would be valuable to investigate our question in a more diverse sample. Second, the results cannot be generalized because the sample size was limited to 19 respondents. Additionally, to gain a deeper understanding of the challenges to maintaining blood supply and of the blood donation mobilization mechanisms in North China during COVID-19, interviews must be conducted in other provinces. Further, we used only qualitative research methods; to demonstrate the overall impact of the COVID-19 pandemic on blood supply in North China in a multidimensional manner, follow-up studies should combine quantitative and qualitative methods. This would facilitate more in-depth investigation and triangulation and improve reliability. Additionally, as the COVID-19 pandemic becomes less pervasive, future studies could consider revising blood donation mobilization policies. Although we focused on blood supply-related challenges and coping mechanisms in North China only, future studies could include other countries with a 100% non-remunerative blood donation policy and compare their similarities and differences.
Conclusion
The findings of this study indicate that the challenges to blood supply include donors’ fears, family pressure and policies restricting free movement, all of which combined during the COVID-19 pandemic to cause a decline in North China’s blood supply, as compared to the previous year. In response to these challenges, the government introduced new policies and engaged in nationwide ideological and organizational mobilization to reverse the decline. Group blood donations, while providing a more stable source of blood in the aftermath of public health emergencies, do not encourage the spirit of civic engagement. Many group blood donors are driven by extrinsic factors like group pressure or organizational rewards rather than the intrinsic motivation to actively care for others. In addition, this study found that the state sees blood donation only as a “gift of life”, in contrast to the multiple social understandings of the nature of blood (“gift of life”, “tie of relationship”, “exchangeable resources”). The state’s cultural perception of the “gift of life” corresponds to the non-remunerative blood donation mode, while society’s cultural perception corresponds to the co-existence of the non-remunerative, family substitution, and paid blood donation models. When the state and society do not agree on the nature of blood, there is a mismatch between blood donation practices and mobilization models. This mismatch is not conducive for fostering people’s freedom to donate blood according to their perceptions of the nature of blood. That is, it would not be possible to fully realize the potential of blood supply for all of society. Future revisions of the blood donation policy should include the different voices of society to promote a sustainable blood supply.
Data Sharing Statement
The data supporting this study’s findings are available on request from the corresponding author. The data are not publicly available due to privacy and ethical considerations.
Informed Consent
Written informed consent has been obtained from the participant(s) to publish this paper.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Nanjing University (Approval number: [SS02]; Date of Approval: [20200320]).
Acknowledgments
We would like to thank Professor Chen Youhua for his advice, as well as Editage (www.editage.cn) for English language editing.
Funding
This work was supported by the National Social Science Fund of China [grant number: 17ASH002].
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO. WHO Director-General’s opening remarks at the media briefing on COVID-19 – 8 March 2021. Available from: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-The-media-briefing-on-covid-19-8-march-2021.
2. Yahia AIO. Management of blood supply and demand during the COVID-19 pandemic in King Abdullah Hospital, Bisha, Saudi Arabia. Transfus Apher Sci. 2020;59:102836. doi:10.1016/j.transci.2020.102836
3. Loua A, Kasilo OMJ, Nikiema JB, Sougou AS, Kniazkov S, Annan EA. Impact of the COVID-19 pandemic on blood supply and demand in the WHO African region. Vox Sang. 2021;116:774–784. doi:10.1111/vox.13071
4. Shander A, Goobie SM, Warner MA, et al. Essential role of patient blood management in a pandemic: a call for action. Anesth Analg. 2020;131:74–85. doi:10.1213/ANE.0000000000004844
5. Park C, Gellman C, O’Brien M, et al. Blood donation and COVID-19: reconsidering the 3-month deferral policy for gay, bisexual, transgender, and other men who have sex with men. Am J Public Health. 2021;111:247–252. doi:10.2105/AJPH.2020.305974
6. Bermúdez-Forero MI, Soto-Viáfara JA, Gardeazábal-Acuña PA, Anzola-Samudio DA, García-Otálora MA. Effect of the first year of COVID-19 pandemic on the collection and use of blood components in Colombia monitored through the National Haemovigilance System. Transfus Med. 2021;31:421–430. doi:10.1111/tme.12828
7. Stanworth SJ, New HV, Apelseth TO, et al. Effects of the COVID-19 pandemic on supply and use of blood for transfusion. Lancet Haematol. 2020;7:e756–e764. doi:10.1016/S2352-3026(20)30186-1
8. Glynn SA, Busch MP, Schreiber GB, et al. NHLBI REDS Study Group. Effect of a national disaster on blood supply and safety – the September 11 experience. JAMA. 2003;289:2246–2253. doi:10.1001/jama.289.17.2246
9. Kasraian L. National disasters in Iran and blood donation: bam earthquake experience. Iran Red Crescent Med J. 2010;12:316–318.
10. Guo N, Wang J, Ness P, et al. First-time donors responding to a national disaster may be an untapped resource for the blood centre. Vox Sang. 2012;102(4):338–344. doi:10.1111/j.1423-0410.2011.01557.x
11. Sass RG. Toward a more stable blood supply: charitable incentives, donation rates, and the experience of September 11. Am J Bioeth. 2013;13:38–45. doi:10.1080/15265161.2013.781703
12. Pagano MB, Hess JR, Tsang HC, et al. Prepare to adapt: blood supply and transfusion support during the first 2 weeks of the 2019 novel coronavirus (COVID-19) pandemic affecting Washington State. Transfusion. 2020;60:908–911. doi:10.1111/trf.15789
13. Wang YJ, Han W, Pan L, et al. Impact of COVID-19 on Blood Centres in Zhejiang Province China. Vox Sang. 2020;115:502–506. doi:10.1111/vox.12931
14. Al-Riyami AZ, Abdella YE, Badawi MA, et al. The impact of COVID-19 pandemic on blood supplies and transfusion services in eastern Mediterranean region. Transfus Clin Biol. 2021;28:16–24. doi:10.1016/j.tracli.2020.11.002
15. Miskeen E, Omer Yahia AI, Eljack TB, Karar HK. The impact of COVID-19 pandemic on blood transfusion services: a perspective from health professionals and donors. J Multidiscip Healthc. 2021;14:3063–3071. doi:10.2147/JMDH.S337039
16. Delabranche X, Kientz D, Tacquard C. Impact of COVID-19 and lockdown regarding blood transfusion. Transfusion. 2021;61:2327–2335. doi:10.1111/trf.16422
17. Sabetkish N, Rahmani A. The overall impact of COVID-19 on healthcare during the pandemic: a multidisciplinary point of view. Health Sci Rep. 2021;4:e386. doi:10.1002/hsr2.386
18. Greer SL, Jarman H, Falkenbach M. Social policy as an integral component of pandemic response: learning from COVID-19 in Brazil, Germany, India and the United States. Glob Public Health. 2021;16:1209–1222. doi:10.1080/17441692.2021.1916831
19. Raturi M, Kusum A. The blood supply management amid the COVID-19 outbreak. Transfus Clin Biol. 2020;27:147–151. doi:10.1016/j.tracli.2020.04.002
20. Pandey HC, Coshic P. Blood supply management in times of SARS-CoV-2 pandemic – challenges, strategies adopted, and the lessons learned from the experience of a hospital-based blood centre. Vox Sang. 2021;116:497–503. doi:10.1111/vox.13019
21. Ogar CO, Okoroiwu HU, Obeagu EI, Etura JE, Abunimye DA. Assessment of blood supply and usage pre- and during COVID-19 pandemic: a lesson from non-voluntary donation. Transfus Clin Biol. 2021;28:68–72. doi:10.1016/j.tracli.2020.10.004
22. Chandler T, Neumann-Böhme S, Sabat I, et al. Blood donation in times of crisis: early insight into the impact of COVID-19 on blood donors and their motivation to donate across European countries. Vox Sang. 2021;116:1031–1041. doi:10.1111/vox.13103
23. Tripathi PP, Kumawat V, Patidar GK. Donor’s perspectives on blood donation during Covid-19 pandemic. Indian J Hematol Blood Transfus. 2021;1–10. doi:10.1007/s12288-021-01504-y
24. Miah M. Study of blood donation campaign communication methods and attributes of donors: a data analytics approach. Int J Healthc Manag. 2022;15:17–27. doi:10.1080/20479700.2020.1836725
25. Oreh AC, Irechukwu C, Biyama F, et al. C.O.V.I.D.-19 Impact on Nigeria’s national blood service commission - lessons for low- and middle-income countries (LMICs). Niger Postgrad Med J. 2022;29:6–12. doi:10.4103/npmj.npmj_720_21
26. Alomari E, Katib I, Albeshri A, Mehmood RCOVID-19. Detecting government pandemic measures and public concerns from Twitter Arabic data using distributed machine learning. Int J Environ Res Public Health. 2021;18:34. doi:10.3390/ijerph18010282
27. Silva-Malta MCF, Rodrigues DOW, Chaves DG, et al. Impact of COVID-19 in the attendance of blood donors and production on a Brazilian blood centres. Transfus Med. 2021;31:206–212. doi:10.1111/tme.12733
28. Kandasamy D, Shastry S, Chenna D, Mohan G. COVID-19 Pandemic and blood transfusion services: the impact, response and preparedness experience of a tertiary care blood center in southern Karnataka, India. Hematol Transfus Cell Ther. 2022;44:17–25. doi:10.1016/j.htct.2021.09.019
29. Menitove JE, Reik RA, Cohn CS, Young PP, Fredrick J. Needed resiliency improvements for the national blood supply. Transfusion. 2021;61:2772–2774. doi:10.1111/trf.16611
30. Kim HO. Current state of blood management services in Korea. Ann Lab Med. 2022;42:306–313. doi:10.3343/alm.2022.42.3.306
31. Almalki S, Asseri M, Khawaji Y, et al. Awareness about coronavirus (COVID-19) and challenges for blood services among potential blood donors. Transfus Apher Sci. 2021;60:103211. doi:10.1016/j.transci.2021.103211
32. Sofaer S. Qualitative methods: what are they and why use them? Health Serv Res. 1999;34:1101–1118.
33. Neergaard MA, Olesen F, Andersen RS, Sondergaard J. Qualitative description – the poor cousin of health research? BMC Med Res Methodol. 2009;9:52. doi:10.1186/1471-2288-9-52
34. Tracy SJ. Qualitative quality: eight ‘Big-Tent’ criteria for excellent qualitative research. Qual Inq. 2010;16:837–851. doi:10.1177/1077800410383121
35. Sandelowski M. Using qualitative research. Qual Health Res. 2004;14:1366–1386. doi:10.1177/1049732304269672
36. Sale JEM, Lohfeld LH, Brazil K. Revisiting the quantitative-qualitative debate: implications for mixed-methods research. Qual Quant. 2002;36:43–53. doi:10.1023/A:1014301607592
37. Crouch M, McKenzie H. The logic of small samples in interview-based qualitative research. Soc Sci Inf Sci Soc. 2006;45:483–499. doi:10.1177/0539018406069584
38. Coyne IT. Sampling in qualitative research. purposeful and theoretical sampling; merging or clear boundaries? J Adv Nurs. 1997;26:623–630. doi:10.1046/j.1365-2648.1997.t01-25-00999.x
39. Guest G, Bunce A, Johnson L. How many interviews are enough? An experiment with data saturation and variability. Field Methods. 2006;18:59–82. doi:10.1177/1525822X05279903
40. Kallio H, Pietilä AM, Johnson M, Kangasniemi M. Systematic methodological review: developing a framework for a qualitative semi-structured interview guide. J Adv Nurs. 2016;72:2954–2965. doi:10.1111/jan.13031
41. DiCicco-Bloom B, Crabtree BF. The qualitative research interview. Med Educ. 2006;40:314–321. doi:10.1111/j.1365-2929.2006.02418.x
42. Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis: striving to meet the trustworthiness criteria. Int J Qual Methods. 2017;16:13. doi:10.1177/1609406917733847
43. Vaismoradi M, Turunen H, Bondas T. Content analysis and thematic analysis: implications for conducting a qualitative descriptive study. Nurs Health Sci. 2013;15:398–405. doi:10.1111/nhs.12048
44. Braun V, Clarke V. One size fits all? What counts as quality practice in (reflexive) thematic analysis? Qual Res Psychol. 2021;18:328–352. doi:10.1080/14780887.2020.1769238
45. National Health Commission. Further Implementation of Scientific Prevention and Control of Precise Policy Zoning and Grading Requirements for Blood Protection during the Epidemic; 2020. Available from: www.nhc.gov.cn/yzygj/s7658/202003/37690667ce01461bbe62947d6185886e.shtml.
46. Barnes LS, Al-Riyami AZ, Ipe TS, Bloch EM, Sibinga CS, Eichbaum QG. AABB Global transfusion forum. COVID-19 and the impact on blood availability and transfusion practices in low- and middle-income countries. Transfusion. 2022;62:336–345. doi:10.1111/trf.16798
47. Ngo A, Masel D, Cahill C, Blumberg N, Refaai MA. Blood banking and transfusion medicine challenges during the COVID-19 pandemic. Clin Lab Med. 2020;40:587–601. doi:10.1016/j.cll.2020.08.013
48. Barrett CL. Primary healthcare practitioners and patient blood management in Africa in the time of coronavirus disease 2019: safeguarding the blood supply. Afr J Prim Health Care Fam Med. 2020;12:e1–e3. doi:10.4102/phcfm.v12i1.2457
49. Yin YH, Li CQ, Liu Z. Blood donation in China: sustaining efforts and challenges in achieving safety and availability. Transfusion. 2015;55:2523–2530. doi:10.1111/trf.13130
50. Basavarajegowda A, Bajpai M, Arora S, Maheshwari A, Dua S, Sahoo D. Survey based cross-sectional study to analyse the variation of practices at blood centres during COVID-19 pandemic in India. Transfus Apher Sci. 2021;60:103131. doi:10.1016/j.transci.2021.103131
51. Wang WH, Li S, Li J, The WY. COVID-19 Pandemic changes the nudging effect of social information on individuals’ blood donation intention. Front Psychol. 2021;12:736002. doi:10.3389/fpsyg.2021.736002
52. Sümnig A, Feig M, Greinacher A, Thiele T. The role of social media for blood donor motivation and recruitment. Transfusion. 2018;58:2257–2259. doi:10.1111/trf.14823
53. Erwin K, Adams V, Le P. Glorious deeds: work unit blood donation and postsocialist desires in urban China. Body Soc. 2009;15:51–70. doi:10.1177/1357034X09103437
54. Guan Y. When Voluntary donations meet the state monopoly: understanding blood shortages in China. China Q. 2018;236:1111–1130. doi:10.1017/S0305741018001327
55. Ou-Yang J, Bei CH, He B, Rong X. Factors influencing blood donation: a cross-sectional survey in Guangzhou, China. Transfus Med. 2017;27:256–267. doi:10.1111/tme.12410
56. Shi L, Wang J, Liu Z, et al. Blood donor management in China. Transfus Med Hemother. 2014;41:273–282. doi:10.1159/000365425
57. Misje AH, Bosnes V, Gåsdal O, Heier HE. Motivation, recruitment and retention of voluntary non-remunerated blood donors: a survey-based questionnaire study. Vox Sang. 2005;89:236–244. doi:10.1111/j.1423-0410.2005.00706.x
58. Marantidou O, Loukopoulou L, Zervou E, et al. Factors that motivate and hinder blood donation in Greece. Transfus Med. 2007;17:443–450. doi:10.1111/j.1365-3148.2007.00797.x
59. Zhang LF, Yao M, Liu H, Zheng S. The effect of functional motivation on future intention to donate blood: moderating role of the blood donor’s stage. Int J Environ Res Public Health. 2021;18:11. doi:10.3390/ijerph18179115
60. Titmuss R. The Gift Relationship: From Human Blood to Social Policy, London. Vol. 12. Allen & Unwin; 1970:38–44.
61. Allain JP. Current approaches to increase blood donations in resource-limited countries. Transfus Med. 2019;29:297–310. doi:10.1111/tme.12629
62. Yaqoob M, Muneeb A, Babar H. Motivation, misconception and myths related to voluntary blood donation. Indo Am J Pharm Sci. 2018;5:9730–9735.
63. Rodriguez Del Pozo PR. Paying donors and the ethics of blood supply. J Med Ethics. 1994;20:31–35. doi:10.1136/jme.20.1.31
64. Arrow KJ. Gifts and exchanges. Philos Public Aff. 1972;1:343–362.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.