Back to Journals » Patient Preference and Adherence » Volume 18
Exploring Attitudes Toward Pre-Exposure Prophylaxis for HIV Prevention Prior to Implementation Among Female Sex Workers in Malaysia: Results from a Qualitative Study
Authors Foley S, Keene DE, Shrestha R ![]() , Brown SE, Gautam K, Sutherland RA, Maviglia F, Saifi R, Wickersham JA
, Brown SE, Gautam K, Sutherland RA, Maviglia F, Saifi R, Wickersham JA ![]()
Received 27 May 2023
Accepted for publication 8 February 2024
Published 5 April 2024 Volume 2024:18 Pages 797—807
DOI https://doi.org/10.2147/PPA.S413423
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Shaylen Foley,1 Danya E Keene,1 Roman Shrestha,2– 4 Shan-Estelle Brown,5 Kamal Gautam,2 Ryan A Sutherland,3 Francesca Maviglia,3 Rumana Saifi,4 Jeffrey A Wickersham3,4
1Department of Social and Behavioral Sciences, Yale School of Public Health, Yale University, New Haven, CT, USA; 2Department of Allied Health Sciences, University of Connecticut, Storrs, CT, USA; 3Section of Infectious Diseases, Department of Internal Medicine, Yale School of Medicine, Yale University, New Haven, CT, USA; 4Centre of Excellence for Research in AIDS (CERiA), Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia; 5Department of Anthropology, Rollins College, Winter Park, FL, USA
Correspondence: Shaylen Foley, 135 College Street, Suite 323, New Haven, CT, 06510, USA, Tel +419 343-4606, Email [email protected]
Introduction: Pre-exposure prophylaxis (PrEP) is an effective method for prevention of HIV transmission. Female sex workers (FSW) in Malaysia are at substantially increased risk of acquiring HIV compared to the general female population, yet little is known about this population’s current HIV prevention practices or acceptance of PrEP. This study aims to inform the culturally relevant implementation of PrEP through the qualitative exploration of (1) the potential need for PrEP in this population and (2) the factors that determine FSW willingness to use oral PrEP.
Methods: In-depth, semi-structured interviews (n = 30) were conducted with FSW in English, Malay, or Tamil. Transcribed and translated interviews were analyzed using a grounded theory approach.
Results: FSW express positive interest in PrEP but prefer it as a supplement to condoms, not a replacement. Perceived challenges to PrEP use include cost, adherence, and side effects.
Conclusion: The findings suggest that in combination with condom use, PrEP may be an acceptable method of HIV prevention. Effective PrEP rollout may also include condom promotion using a peer-driven model, cost subsidies, and sex work harm reduction and empowerment components.
Keywords: sex work, HIV, pre-exposure prophylaxis, Malaysia
Introduction
Female sex workers (FSW) are disproportionally affected by HIV compared to the general population.1 Compared to the general population, FSW reports having more sex partners and more frequent sexual risk behaviors, putting them at higher risk of both acquiring and transmitting HIV. FSW have been largely underserved in HIV research and practice, particularly with regard to biomedical approaches to prevention.2
Daily oral Pre-Exposure Prophylaxis (PrEP) for HIV prevention offers the opportunity to curb HIV transmission among FSW in a novel way. Intended for HIV-uninfected individuals at high risk, PrEP has been demonstrated to safely and effectively reduce risk of HIV infection in men who have sex with men (MSM), people who inject drugs (PWID), and serodiscordant heterosexual couples.3 Although PrEP has already proven to be effective for preventing HIV in FSW, there is limited research on factors related to its implementation in FSW populations.
Unlike condoms, which are often subject to negotiation between FSW and their clients, PrEP is an HIV prevention tool that can be used easily and discretely by FSW, taking their PrEP dose at a time of day that is convenient and private for them.4 Scale-up of PrEP among sex workers is highly promising because it provides FSW with an additional strategy to reduce their risk of acquiring HIV. Current HIV prevention efforts focus on condom promotion and distribution, yet condom use remains suboptimal. Condom use may be inconsistent due to limited agency, client refusal or coercion, sexual or physical violence, criminalization of carrying condoms, offers of higher payment by clients, and attitudes of non-paying partners.5,6
Research on acceptability of daily oral PrEP among high-risk groups, including FSW, has demonstrated that acceptability is generally high but varies depending on cost, perceived efficacy, and fear of side effects.7–9 However, these studies have predominately relied on survey-based methods and fail to look in-depth at the factors that may shape PrEP acceptability among FSW. Indeed, previous research has found that the most common PrEP acceptability measures may not be great predictors of actual adherence, as they ignore contextual factors such as agency or competing priorities.10 Research demonstrates that FSW decision-making is calculated and often involves juggling a variety of interests, but little is known about factors that might determine FSW willingness to use PrEP. Challenges related to PrEP uptake, adherence, and retention among sex workers11,12 demonstrate the importance of understanding the contextual factors that influence acceptability and adherence.
In order to address this gap, this research draws on qualitative interviews conducted among FSW in Kuala Lumpur to examine PrEP acceptability within the context of participant HIV risk perception and mitigation behaviors. By providing an in-depth understanding of how PrEP decisions are made by women themselves, this analysis can inform implementation of PrEP for HIV prevention among FSW and transgender sex workers (TGSW).
Setting
For two decades after the first confirmed case of HIV was detected in Malaysia in 1986, the epidemic remained largely driven by PWID.13 Across that time, however, Malaysia’s HIV epidemic evolved to become a generalized epidemic, with more than 80% of all new cases in 2021 attributed to sexual transmission.14 Of the estimated 40,000 FSW in Malaysia, an estimated 6.3% are living with HIV.13 In the Klang Valley, which includes the capital city of Kuala Lumpur, HIV prevalence among FSW was even higher at 11.1%.15
Despite advancements in HIV treatment, antiretroviral therapy (ART) coverage remains suboptimal. Recent estimates suggest that only 79% of all PLWH are on ART and only 48% are virally suppressed.16 PLWH may not seek treatment for various reasons, including lack of awareness, financial costs, time constraints, and fear of positive results. In Malaysia, pervasive stigma surrounding HIV compounds the problem, contributing to higher rates of late-stage diagnosis and increased risk of mortality, suggesting the need for more comprehensive prevention approaches.17
Current HIV prevention efforts targeting FSW in Malaysia rely on community-based organizations to distribute condoms, provide education on HIV risk reduction, and offer rapid point-of-care HIV testing.18,19 These outreach efforts have made inroads in expanding access to and use of condoms. Despite this, the high rates of HIV among FSW make it clear that there are significant gaps in HIV prevention and highlight the need for biomedical approaches like PrEP. As access to and use of PrEP is expanded to places like Malaysia, it is crucial that we understand how PrEP is perceived and fits within already adopted HIV prevention strategies among key populations.
Methods
Study Design and Sample
This study draws on qualitative semi-structured interviews with 30 FSW. Participants were eligible if they were female, 18 years of age or older, reported engaging in sex work in the past 30 days, and spoke Malay, English, or Tamil. Participants were provided with information on PrEP that emphasized its appropriateness for uninfected individuals, its high effectiveness, the importance of taking the pill daily, the need for blood tests every 3 months to check HIV status and kidney function, and to monitor sexually transmitted infections (STIs) and pregnancy if not using condoms. Purposive sampling was used to ensure a diverse sample of participants with respect to age and ethnicity. Within age and ethnicity purposive sampling criteria, participants were selected on a first come first serve basis.
Data Collection
Participants were recruited via three local non-governmental organizations located in greater Kuala Lumpur area that provide outreach and education to the sex worker community. Recruitment flyers were distributed digitally (eg, WhatsApp groups and Facebook groups) by NGOs and their outreach workers. Prospective participants were provided a participant information sheet that described the study purpose, procedures, and inclusion criteria and contact details of the study team. Individuals who met the inclusion criteria and expressed interest in participation reached out to the study staff either through phone communication or by visiting the NGO in person. Those who met the inclusion criteria were then scheduled for an interview date and time. Interviews were conducted between June and October. Prior to the beginning of the interview, a facilitator read an information sheet about the study, and participants provided verbal consent to participate. Interviews were audio recorded and involved the participant, principal investigator, and a research assistant able to speak all three languages. All data collected were anonymous. Participants were provided with 50 Malaysia Ringgit (RM) (approximately $13.50 USD) and contact information for local healthcare and social service organizations.
A qualified team of trained local research assistants transcribed and translated interviews into English between August and October 2015. Twenty-three final transcripts contained both Malay and English so that accuracy could be checked (SF), four were transcribed directly into English, and three were translated from Tamil audio files into English. A secure cloud-based website was used to store and share both audio and written files. All participants used a pseudonym to protect their privacy and are used in the present results.
Data Analysis
Analysis of transcript data was based on grounded theory methodology.20 Constant comparisons, which involve comparing pieces of data both within and between files, were used to develop emerging concept.20 Comparison of data was facilitated by an iterative coding process. First, open codes were used to identify key themes (SF, JW). This analysis formed the basis for the development of a codebook (SF), which was used to code the entirety of the interviews using ATLAS.ti software (SF).21 A selection of interviews was independently double-coded by trained research staff and then compared to ensure reliability. Theoretical comparisons were then used to look at interactions between concepts and group codes into themes. During this process, codes were often regrouped in the codebook to reflect the on-going conceptual development (SF, JW, DK, SB). All results are presented with participant pseudonyms.
Ethics Statement
This research was approved by the institutional review boards of Yale University and the University of Malaya. The study adhered to the guidelines outlined in the Declaration of Helsinki. Informed consent was obtained verbally from all participants, as approved by the institutional review boards, from all study participants and included consent to publish anonymized responses.
Results
Participant Characteristics
Characteristics of the sample are reported in Table 1. Participants ranged in age from 21 to 65 years, with an average age of 38. Most participants were of Malay (17/30) or Indian (8/30) ethnicity. Education levels were relatively low, with only 8 of 30 participants having completed Form 5, the equivalent of US high school. History of prior arrest (23/30), lifetime use of alcohol (20/30) or methamphetamines (20/30), positive screens for depression (20/30) and exposure to physical, sexual, or emotional violence in the past 12 months (13/30) were frequent, demonstrating the persistent challenges faced by this population.
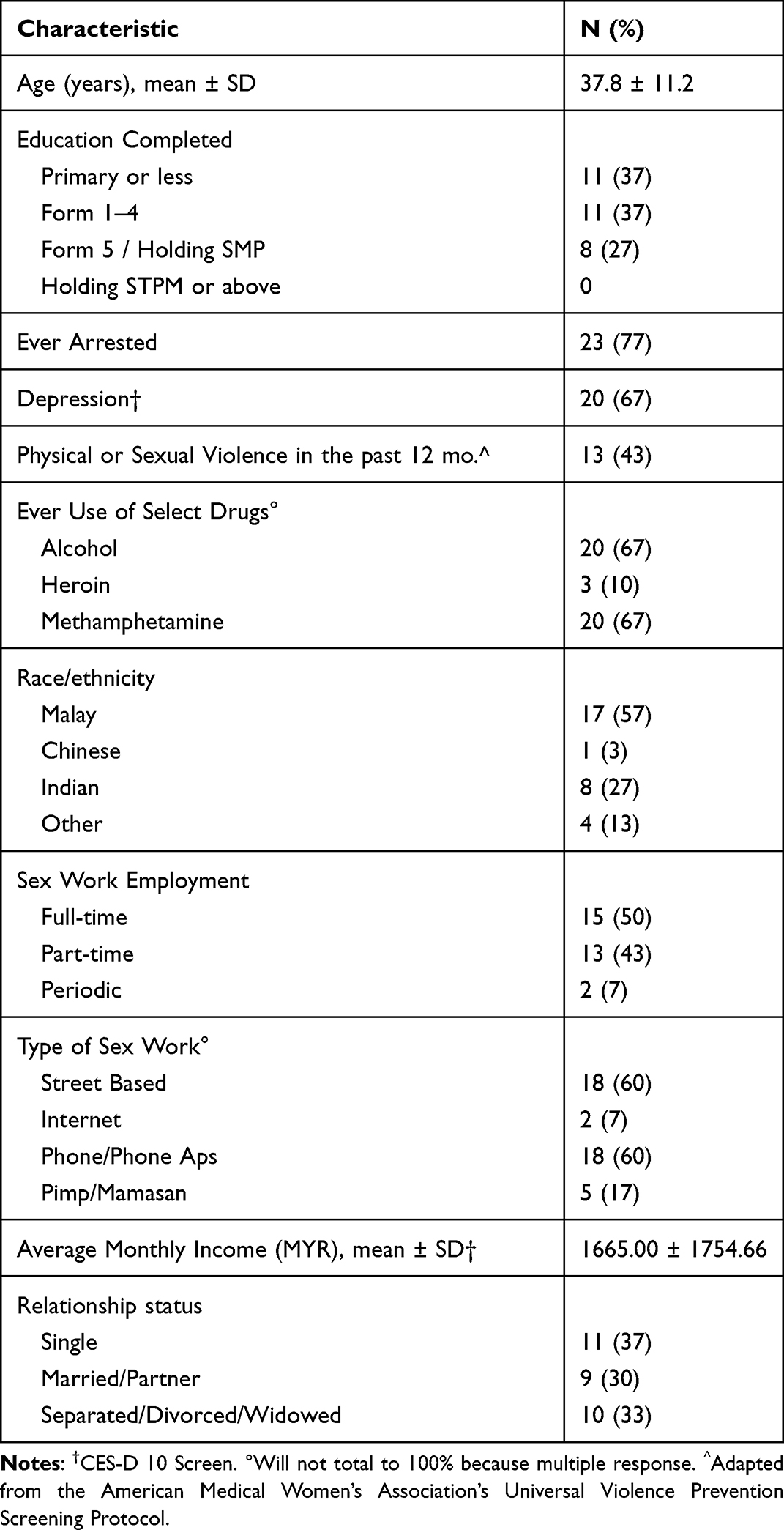 |
Table 1 Description of the Sample (n = 30) |
With regard to sex work, the majority of participants reported doing it full time (15/30) or part time (13/30) and recruiting clients on the street (18/30) or by phone (18/30). A large majority reported having sex with clients over the last six months in hotels (26/30), while some reported meeting at the client’s residence (6/30), the FSW’s home (3/30), or in a brothel (3/30). Average age of initiation into sex work was not asked directly, but a review of the interview transcripts revealed a reported range from age 14 to 39, with an approximate average age of 23.
Thematic Results
The themes that emerged from the data illustrate how Malaysian FSW perceive and respond to HIV risk in their daily lives. These themes also provide insight into their attitudes, beliefs, and perceptions of oral PrEP as an HIV prevention tool. Findings are broken down into three progressive groupings. The first section describes participant attitudes towards HIV and their HIV risk perception. The second section presents how FSW react to their perceived risk by exploring HIV prevention practices and the shortcomings of these methods. These two sections provide context for understanding how PrEP, an HIV prevention tool, fits into the HIV prevention routines employed by FSW at the time of survey. The third section examines how PrEP might address the challenges FSW face, while also detailing the potential limitations of PrEP in this unique population.
PART 1: “Even the Word Can Give Me Goose Bumps”: HIV Risk Perception
HIV risk perception is a salient theme in the interviews, and participants describe high levels of perceived HIV risk. For example, when asked about her thoughts on HIV, one participant called Sami [age 39] reacts by saying: “No, I am afraid of this, HIV, I cannot imagine, even the word can give me goose bumps.” For many participants, this fear is derived from experiences of HIV in their community. Aditi [age 48] elaborates:
I personally had a friend who passed away because of HIV, but she was on drugs. We went for her funeral. No one must ever have this sickness. You can get any other sickness, but not this.
For those like Aditi, there is a clear link between HIV and mortality.
When asked what they know about HIV, most participants knew about transmission from unprotected intercourse and unclean needles. Regardless of this, misinformation about HIV transmission remains. A quote by Nisa [age 30] highlights this:
“Maybe if our friends have it [HIV], [but] we do not know that, right? We can get infected by wounds or cuts, right?”
Another common source of confusion was related to HIV treatment. While most women were aware that there is no cure for HIV, few understand that it can be effectively treated with antiretroviral medications and managed as a chronic illness. These uncertainties expose the realities that exist for this population’s access to accurate prevention information, early diagnosis, and appropriate treatment for HIV.
For many FSW, concerns about HIV were directly related to their experiences with clients. Women described feeling aware of their HIV risk while providing services to clients:
“I am worried if we choose the wrong customer…but I do not know because we cannot tell if the person has HIV or not…I am afraid if I get infected.” [Dina, Age 38]
Coping with this constant fear often involved creative client screening methods. Some FSW attempted to screen clients based on physical or racial profiling, alcohol intoxication or drug use, appearance of the genitals, or other measures. Participants talked about screening clients this way:
“I do not just take [any] customer. I look at them first. If they look okay then I will take them. Sometimes other sex workers just want the money so they take whomever they want. But I am picky; I only take certain customers that look okay.” [Nisa, Age 30]
Client-screening methods like those described above were part of how FSW manage risk, suggesting that FSW are searching for a way to cope with non-disclosure of client disease status. FSW inability to truly screen clients or request disclosure is a primary challenge to HIV prevention in this population and highlights the limitations of risk perception. Understanding HIV risk perception among FSW is important to explaining both the demand for PrEP and how it fits into the lives of this population.
PART 2: “He Did Not Want to Wear a Condom”: Condom Negotiation Practices
Given the HIV risk perception of this population, condoms play an important role in helping FSW prevent HIV. All participants used the male condom with clients. Most described negotiating with clients about wearing condoms. These negotiations happened in two stages, with primary negotiations taking place before going “upstairs” to a private room and secondary negotiations happening once in the room with a client. Shivani [age 57], an older FSW doing sex work to meet her basic needs, described her primary negotiations with clients this way:
“[When] I go to the place where an Indian guy has booked me, I go and automatically ask him, uncle do you have a condom? Oh, it’s okay if you do not have it, but you can buy it at the shop. If he does not move, I go back home. I must have a condom! If he refuses to use the condom then he cannot have it [sex].”
Unfortunately, even with primary negotiations, FSW still described the physical shortcomings of condoms, as well as challenges they face with secondary condom negotiations.
First, participants reported issues with condoms breaking and slipping. Nisa described experiencing a condom break, “Sometimes if I don’t get aroused, I will be dry. So when we have sex…it will burst…‘tup’…” These types of breaks or leaks are concerning for FSW. Annabel [age 38] expressed the anxiety she felt about potential condom breaks and concerns of waiting for three months, as recommended, before being able to undergo an HIV test for sex workers:
“Yes okay, I always use a condom, like I told you before, [but] none of these condoms are good. It can break, sometimes when we use it, it can easily break. Of course, we are worried [about HIV].”
Second, even when condom use was negotiated ahead of time, FSW encountered customers who refused to wear condoms once alone, often leading to additional negotiations. These secondary negotiations were frequently frustrating for FSW. Most participants reported returning client money and leaving without providing services. For example, Husna reported: “I do [face issues with customers wearing condoms] but I force them to use it. If not, I don’t give them my service, it’s like that.” Another participant described how client refusal to wear a condom once in the room violated the rules of her established negotiation process:
“When we enter the room [and] he tells me that he did not want to wear a condom, I will ask him to use it. If he still refuses to wear it, I will give back his money. I will not jeopardize my health…But it was his fault because he did not tell me that he did not want to wear condom during our negotiation. If he goes upstairs of course he knows that we will wear a condom. Except if we agree to do it without a condom during our negotiation downstairs. If not, they cannot force us to do it.” [Dina, age 35]
While Dina and Husna were confident about their ability to decline customers who refuse condoms once in a private setting, that was not the case with all participants. Those participants reporting condomless sex due to clients’ refusal did so in the following situations:
First, a minority of participants describe asking for substantially higher payments from customers in exchange for not using condoms. Sabrina [age 41] elaborates on this, saying:
“Normally if I want to get extra money from them, I allow it…I test the customer, okay, if you want to pay RM 300 (∼USD 81) or you pay me more than RM 150 (∼USD 40) I will allow you to ejaculate inside me.”
Second, another participant reported being more willing to agree to sex without a condom during times of financial difficulty:
If it is an emergency, [and] I do not have any money at all [I will take a client without a condom]…It is challenging for me to get even one customer [sometimes], so I have no choice and take it. I am aware of the risk, but I can only hope for the best. [Sofea, Age 35]
Third, secondary negotiations regularly took place in private spaces that resulted in a loss of agency and an increased level of vulnerability. Nadia [age 41] talked about an experience of sexual violence due to a customer refusing to wear a condom:
“I went through that once…[actually,] it has occurred a few times…I will cry if I feel unsafe and I will reject the customer’s offer. If they still want it and force me until at some point I am terrified, I will do it with him but that will be the first and last time…I will not take him again, [because] I [can] recognize the guy. I will not accept his offer again because he scares me.”
The challenges with condoms discussed in this section, specifically breaks or leaks and ineffective condom negotiations due to financial incentive, financial constraint, or violence, highlight the issues FSW face when trying to protect themselves from HIV. PrEP has the potential to enable FSW to reduce their HIV risk, particularly when other prevention methods failed. . FSW reactions to PrEP are informed by their awareness of the shortcomings of condoms, their sole HIV prevention tool. The next three sections elaborate on FSW reactions to PrEP, starting with interest, followed by perceived barriers to using PrEP.
PART 3: PrEP as a Solution with Limitations
“I Don’t Want to Wait Until I Get the Disease”: PrEP for Preserving Health
Of the 30 women interviewed, none had previously heard of PrEP. Reactions were positive on the whole, with the majority of participants (90%) responding that they would be willing to take PrEP if it were offered to them as a daily pill. Participant statements during interviews reflected this high interest rate. Most participants reported a positive view of PrEP because it provides a way to proactively prevent HIV:
“If you ask my opinion, I do not mind to take the [PrEP] medicine because it is used to prevent the [HIV] disease. If people want to say anything, I can tell them that this is for prevention, I do not want to wait until I get the disease, then it will be too late.” [Nisa, Age 30]
Participants expressed willingness to spend their own money on PrEP because of the perceived preventative benefit. Dinny [age 19] states: “This is for prevention, and I am worried [about HIV], so I will try to buy it.” Aditi [age 48] described how much she would pay for PrEP, saying:
“If you have to buy the medicine for the safety of our health, then we do not have any choice but to buy it. No two ways about it…we will spend so much money for HIV, [that] RM 300 [a participant generated cost equivalent to $81 USD] is nothing. I will buy [it] for myself and take the medication.”
Other participants had expressed interest in PrEP because it served as a means to protect FSW when they had forgotten to use condoms while using drugs:
“I think those injection drug addicts should take this PrEP medication because they are high risk to get the [HIV] disease. Those sex workers who do not use condoms are in the high-risk group as well but most of us know about this. So we use condoms when we have protected sex. But sometimes if we are high on drugs we will forget to wear condoms, right?” [Nur, Age 48]
Positive reactions to PrEP are not limited to preserving the health of participants themselves. Participants also expressed willingness to share information about PrEP with others, particularly friends or partners who were at high-risk of contracting HIV. Husna [age 26] described her willingness to share PrEP for the good of others, saying: “Of course I will recommend it [PrEP] to my friends because it will bring goodness to them.” This desire to share knowledge of PrEP with others is not all-encompassing, but specifically relates to individuals that FSW trust. Sabrina [age 41] explained how she would determine who to tell about PrEP:
“If my friend came to my room, my friend that knows about my [sex] work, [then] it is ok with me [to share information about PrEP]… I cannot share it to family and relatives, this is personal. Personal is personal.”
“I Will Still Use a Condom”: PrEP as a Supplement to Condoms Rather Than a Replacement
While participants expressed enthusiasm about PrEP, their narratives also revealed that they viewed it as a supplement to, rather than a replacement of, condoms. In several interviews women rejected PrEP initially if they thought it required them to give up condoms. Researchers framed PrEP as something that should be used with condoms, but these types of reactions happened anyway. The majority (83%) of participants reported still being willing to take PrEP even if they had to continue using condoms.
Participants described comfort with condom use and the negotiation routines FSW already have. When considering her current negotiation practices in light of PrEP, Farah [age 20] reported that PrEP would not change her existing condom negotiation routine:
“If I take this medicine [PrEP] I will still use a condom. I will not use a condom only with the regular customer because I already make a deal with them by saying that it is alright for them to not wear it. But if I can wear it, I will use it even if I take this medicine so it can give me double protection.”
Participants considered the significance of using condoms alongside the PrEP medication to prevent other STIs and unintended pregnancies. Additionally, participants mention that using a condom helped keep bodily fluids contained, making the sexual experience feel cleaner and more manageable. Nadia [age 41] expressed her fear of not being protected by PrEP alone, stating:
“If I do not wear it [a condom] I will feel like I still can get infected, even if I am on that medication [PrEP] … I do not have to worry about, having baby or…I do not feel like I can get any infection inside … and I do not have to wash regularly. The semen will be in the condom. It is much easier if we wear condom too … it’s much cleaner.”
A minority of those interested in PrEP were interested in the opportunity to forgo condoms with customers. Aditi [age 48] talked about her perspective on condoms and PrEP:
“I will feel secure because I am taking the [PrEP] medication. Moreover my customers will be happy they do not need to use condoms. So the sex workers will be happy to take this medication as their customers do not need any condoms. In whatever way you see women being protected, that is the main thing.”
Challenges to PrEP Implementation
Participants identified several important challenges to PrEP implementation including cost, adherence, and fear of side effects. Many participants expressed concern about how much PrEP will cost and how they will pay for it. Sania [age 48] expressed these concerns saying:
“I listen about this but [I think] it is so expensive. If the sex workers can afford this, they can take it. If the sex workers cannot afford they cannot take it.”
The majority of participants asked the researchers for the price during the interview. Since PrEP was not available in Malaysia at the time of interviews, the interviewers were unable to provide participants with a cost. Participants were still able provide feedback on the importance of cost. An FSW named Hur [age 33] described how important the cost would be to her decision to take the medication, saying:
“I have to see the price first and compare it. If I can afford it, I will buy [it]. But I cannot afford it if the price is more than RM500 [approximately $135 USD]. How can I purchase the medicine [if it costs that much]?”
When asked how much they could afford most FSW cite not being able to pay very much:
“I can afford it if it is about RM10, if it is more than that I do not want it. I cannot afford it. People like me cannot afford to buy this kind of thing. It’s expensive, if the price is RM50, I consider it to be expensive.” [Nadia, Age 41]
In U.S. dollars, RM10 is equivalent to only $2.70. Almost two thirds of the participants reported income at or below the poverty level in Malaysia. FSW that report being able to pay more than Nadia also report a higher income from sex work.
Participants also described challenges to PrEP adherence. Some FSW compared adherence to PrEP to taking other medications. Shelly [age 37] puts it this way: “I need to take my medicine for my blood pressure. So if I can take the medication for high blood pressure, why can’t I take this?” Husna [age 26] compares it to her regularity of having a cigarette: “If we can remember to take our cigarette of course we can remember to take this medicine.” And yet, she also discusses the challenge of establishing routines within the context of her lifestyle, reflecting:
“So that means I take it at the same time every day, like that? To remember that I should take it every day is quite challenging…I am worried that I will forget to take it. Because we do not have a fixed schedule, right? I sleep at anytime.”
Other participants also shared Husna’s concern about the impact of an irregular routine on taking PrEP. Establishing a routine to take medications is something Nur [age 48] reported struggling with previously:
“I am worried that I cannot take it on time. Because I have problems taking my medicine on time. I take it after lunch, or early in the morning. I do not take it on time. So to be disciplined in taking the medicine on time is a problem for me.”
The third primary concern for FSW was the side effects of the medication. Dina shared her concerns this way: “If it has any side effects I will think first before I take it. What kind of side effects [are there], right?”. Many participants responded “yes” when asked directly whether they were concerned about side effects but most struggled to elaborate why.
Lastly, in three of the 30 interviews, participants made it clear that they are not interested in taking PrEP. Shivani [age 57] declined PrEP due to her desire to exit sex work: “I want to quit my job. I don’t want to eat [take] this, I don’t. People who work everyday might be interested.” The other two participants expressed unwillingness to take medication. Sarah [age 55] put it this way: “Old people like us…we don’t want to take any medicine.” These quotations highlight how multiple considerations may impact acceptability of PrEP, particularly among older FSW.
Discussion
Developing an effective response to the HIV epidemic among FSW in Malaysia requires a comprehensive understanding of the potential barriers and facilitators to the successful implementation of PrEP. There is little research on understanding attitudes toward PrEP among FSW in Malaysia using qualitative methods. The present study illustrates how Malaysian FSW hold favorable attitudes toward PrEP and most expressed a high degree of willingness to use PrEP if it were made available to them.
Overall, these results indicate FSW in Malaysia hold positive views of oral PrEP for HIV prevention. Given the challenges associated with negotiating consistent condom use with their clients, it makes sense that FSW might hold favorable attitudes toward PrEP. Participants perceived themselves to be at substantial risk of HIV infection and characterized a combination of strategies they utilize to mitigate this risk, some of them more effective than others. The integration of condoms into their primary negotiations with clients and their prioritizing the use of condoms in secondary negotiations reflects effective and proactive efforts to reduce risk. These findings are similar to studies of FSW in Tanzania22 and elsewhere.8 Screening clients based on appearance and determining whether or not to use condoms based on familiarity may be less effective.
Even when FSW employ effective prevention measures, they still face occupational challenges due to both individual- and structural-level risks, including active alcohol or drug dependencies, physical or sexual violence from clients or intimate partners, police harassment or arrest, and extreme financial or housing insecurity. These gaps in protection are where PrEP has the most potential to benefit FSW. PrEP can provide FSW with security when negotiations fail, condoms are forgotten, break, or slip, or intimate partners expect unprotected sex. While none of the participants were familiar with PrEP prior to engaging in this study, they expressed high willingness to adopt PrEP when it becomes available, describing the appeal of a secondary layer of protection against HIV, after condoms.
A frequently articulated concern is that PrEP will lead to greater sexual risk-taking behavior, commonly called behavioral disinhibition or risk compensation.23 The FSW in this study want to continue using condoms in addition to PrEP because they are familiar with condoms and perceive the physical barrier of condoms as more hygienic. These results support and add to other PrEP acceptability research suggesting that behavioral disinhibition and risk compensation may be less applicable to FSW populations.8,23
Another concern surrounding PrEP is adherence, as poor adherence to daily oral PrEP medication greatly reduces efficacy.24 FSW in the present study reported having previously taken daily oral medications, with many drawing parallels between their experiences with other medications and PrEP. Strong adherence to daily oral medications, however, is often dependent on external life factors – such as stable housing, employment, and transportation. Previous studies of FSW in most countries point to chronic unstable housing and financial insecurity, which may lead to challenges in sustained PrEP adherence.24–26
Lastly, it is important to acknowledge the importance of social status, power, control, and education in the demand for PrEP. Compared to FSW in Britain, health issues are perceived as less important and FSW face fewer challenges with safe work spaces, violence, and control over interactions with clients. PrEP cannot address the root causes of the challenges FSW face in their daily lives.27
Considerations for Implementation and Future Research
Participants in the present study expressed a strong preference for continued condom use, even when taking PrEP, during sex work. This suggests that a successful PrEP intervention must build upon the existing condom promotion activities already in place in the country. There is ongoing support for integrating PrEP with behavioral prevention methods like condom promotion, so this approach follows the literature.6 Additionally, when considering the social and public health factors that contribute to HIV vulnerability among FSW, combination HIV prevention efforts that include evidence-based approaches to empowering FSW should be prioritized.28 Previous research with Malaysian FSW has found high interest and motivation for empowerment-based approaches to HIV prevention, such as microfinance and skills development.29
To address adherence to PrEP and offset the complex challenges faced by FSW, an intervention should also consider providing individuals with assistance developing and maintaining effective adherence practices. High participant buy-in and willingness to share information about PrEP with others, particularly with other high-risk individuals or fellow sex workers, suggests the importance of a peer-led model. Implementation of PrEP should build upon FSW trust in their social network by mobilizing and training local Non-governmental Organization (NGO) outreach staff and peers on PrEP distribution, use, and routine building. Peer-led models for PrEP among other key populations have found considerable success in other Southeast Asian nations, including Thailand and Philippines.30–32
In 2017, oral PrEP for HIV prevention became available in Malaysia, which makes this study applicable and timely for understanding and coordinating PrEP uptake in the coming months or years. There are currently no government subsidies to offset the cost of PrEP, which currently costs between 90 and 120 Malaysian Ringgit ($20–26 USD) for a 30 day supply. Participants in the present study voiced willingness to pay for PrEP, but given the large proportion of FSW living below the poverty level, it is likely to remain inaccessible.
This research provides in-depth interviews to explore PrEP acceptability among FSW in Malaysia, providing a richer perspective than previous research. This research opens the door for the development of socially appropriate PrEP interventions among FSW. This study has some limitations. First, all but two participants were recruited via local NGOs, and it is unknown whether their contact with local NGOs increases their awareness of HIV, access to condoms, and HIV testing relative to other FSW. Lastly, while this research has added to our understanding of PrEP acceptability, any scale-up of PrEP should endeavor to assess how acceptability is linked to actual adherence.
Overall, this research demonstrates that PrEP acceptability among FSW in Malaysia is driven by circumstantial need for additional methods of protection from HIV. In order to fill these gaps in protection, while accounting for the complex environment in which this population operates, these findings suggest that PrEP may be an acceptable method of HIV prevention when implemented in combination with condom promotion efforts, a peer-driven model, cost subsidies, and sex work harm reduction and empowerment components.
Acknowledgments
This research is based on the M.P.H. thesis of the first author (SF). The authors would like to thank participants for their time and stories, the staff from Centre of Excellence for Research in AIDS (CERiA) at the University of Malaya for their support and guidance and the outreach workers and staff at PAMT, SEED, and WAKE for their generous assistance.
Funding
This research was supported by two fellowship grants from Yale Downs International Health Student Travel Fellowship and the Yale Council for Southeast Asia Studies and research grants from the National Institutes of Health (R21AI157857 for JAW and RS; and R34MH130233 for JAW and RS).
Disclosure
Ms Shaylen Foley reports grants from The Downs International Health Student Travel Fellowship, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Baral S, Beyrer C, Muessig K, et al. Burden of HIV among female sex workers in low-income and middle-income countries: a systematic review and meta-analysis. Lancet Infect Dis. 2012;12(7):538–549. doi:10.1016/s1473-3099(12)70066-x
2. Bekker L-G, Johnson L, Cowan F, et al. Combination HIV prevention for female sex workers: what is the evidence? Lancet. 2015;385(9962):72–87. doi:10.1016/s0140-6736(14)60974-0
3. Spinner CD, Boesecke C, Zink A, et al. HIV pre-exposure prophylaxis (PrEP): a review of current knowledge of oral systemic HIV PrEP in humans. Infection. 2016;44(2):151–158. doi:10.1007/s15010-015-0850-2
4. Shannon K, Crago AL, Baral SD, et al. The global response and unmet actions for HIV and sex workers. Lancet. 2018;392(10148):698–710. doi:10.1016/s0140-6736(18)31439-9
5. Conserve DF, Middelkoop K, King G, Bekker LG. Factors Associated with HIV Discussion and Condom Use with Sexual Partners in an Underserved Community in South Africa. J Health Care Poor Underserved. 2016;27(1):131–144. doi:10.1353/hpu.2016.0015
6. Bekker LG, Johnson L, Cowan F, et al. Combination HIV prevention for female sex workers: what is the evidence? Lancet. 2015;385(9962):72–87. doi:10.1016/s0140-6736(14)60974-0
7. Makhakhe NF, Sliep Y, Meyer-Weitz A. ”Whatever is in the ARVs, is Also in the PrEP” Challenges Associated With Oral Pre-exposure Prophylaxis Use Among Female Sex Workers in South Africa. Front Public Health. 2022;10:691729. doi:10.3389/fpubh.2022.691729
8. Giguère K, Béhanzin L, Guédou FA, et al. PrEP Use Among Female Sex Workers: no Evidence for Risk Compensation. J Acquir Immune Defic Syndr. 2019;82(3):257–264. doi:10.1097/qai.0000000000002134
9. Wang Z, Lau JTF, Yang X, et al. Acceptability of Daily Use of Free Oral Pre-exposure Prophylaxis (PrEP) Among Transgender Women Sex Workers in Shenyang, China. AIDS Behav. 2017. doi:10.1007/s10461-017-1869-4
10. Mensch BS, van der Straten A, Katzen LL. Acceptability in microbicide and PrEP trials: current status and a reconceptualization. Curr Opin HIV AIDS. 2012;7(6):534–541. doi:10.1097/COH.0b013e3283590632
11. Ghayda RA, Hong SH, Yang JW, et al. A Review of Pre-Exposure Prophylaxis Adherence among Female Sex Workers. Yonsei Med J. 2020;61(5):349–358. doi:10.3349/ymj.2020.61.5.349
12. van der Straten A, Van Damme L, Haberer JE, Bangsberg DR. Unraveling the divergent results of pre-exposure prophylaxis trials for HIV prevention. AIDS. 2012;26(7):F13–9. doi:10.1097/QAD.0b013e3283522272
13. Ministry of Health Malaysia. The Global AIDS Monitoring Report 2019; 2019.
14. Ministry of Health Malaysia. The Global AIDS Monitoring Report - 2022; 2022.
15. Wickersham JA, Gibson BA, Bazazi AR, et al. Prevalence of Human Immunodeficiency Virus and Sexually Transmitted Infections Among Cisgender and Transgender Women Sex Workers in Greater Kuala Lumpur, Malaysia: results From a Respondent-Driven Sampling Study. Sex Transm Dis. 2017;44(11):663–670. doi:10.1097/olq.0000000000000662
16. Pandey A, Galvani AP. The global burden of HIV and prospects for control. Lancet HIV. 2019;6(12):e809–e11. doi:10.1016/s2352-3018(19)30230-9
17. Tee YC, Earnshaw VA, Altice FL, Jin H, Kamarulzaman A, Wickersham JA. Evaluating Physicians’ Intention to Discriminate Against Patients Living with HIV in Malaysia. AIDS Behav. 2019;23(4):1039–1047. doi:10.1007/s10461-018-2362-4
18. Kim RS, Wickersham JA, Maviglia F, et al. Drivers of HIV self-testing among female sex workers: findings from a multi-state study in Malaysia. Front Med Lausanne. 2023;10:1022746. doi:10.3389/fmed.2023.1022746
19. Pedersen CJ, Wickersham JA, Altice FL, et al. Prevalence and Correlates of Active Amphetamine-Type Stimulant Use Among Female Sex Workers in Malaysia. Front Psychiatry. 2022;13:879479. doi:10.3389/fpsyt.2022.879479
20. C J, S A. Basics of Qualitative Research.
21. ATLAS.ti Scientific Software Development GmbH. ATLAS.ti Windows (version 1.0.24); 2016. Available from: https://atlasti.com.
22. Beckham SW, Mantsios A, Galai N, et al. Acceptability of multiple modalities of pre-exposure prophylaxis (PrEP) among female sex workers in Tanzania: a mixed-methods study. BMJ Open. 2022;12(8):e058611. doi:10.1136/bmjopen-2021-058611
23. Om E, Marshall L, Teljeur C, et al. Oral pre-exposure prophylaxis (PrEP) to prevent HIV: a systematic review and meta-analysis of clinical effectiveness, safety, adherence and risk compensation in all populations. BMJ Open. 2022;12(5):e048478. doi:10.1136/bmjopen-2020-048478
24. Celum C, Hosek S, Tsholwana M, et al. PrEP uptake, persistence, adherence, and effect of retrospective drug level feedback on PrEP adherence among young women in Southern Africa: results from HPTN 082, a randomized controlled trial. PLoS Med. 2021;18(6):e1003670. doi:10.1371/journal.pmed.1003670
25. Mboup A, Diabaté S, Béhanzin L, et al. Determinants of HIV Preexposure Prophylaxis Adherence Among Female Sex Workers in a Demonstration Study in Cotonou, Benin: a Study of Behavioral and Demographic Factors. Sex Transm Dis. 2021;48(8):565–571. doi:10.1097/olq.0000000000001373
26. Longino A, Montano MA, Sanchez H, et al. Increasing PrEP uptake and adherence among MSM and TW sex workers in Lima, Perú: what and whom do different patients trust? AIDS Care. 2020;32(2):255–260. doi:10.1080/09540121.2019.1634787
27. Sanders T. A continuum of risk? The management of health, physical and emotional risks by female sex workers. Sociol Health Illn. 2004;26(5):557–574. doi:10.1111/j.0141-9889.2004.00405.x
28. Beyrer C, Crago A-L, Bekker L-G, et al. An action agenda for HIV and sex workers. Lancet. 2015;385(9964):287–301. doi:10.1016/s0140-6736(14)60933-8
29. Lall P, Shaw SA, Saifi R, et al. Acceptability of a microfinance-based empowerment intervention for transgender and cisgender women sex workers in Greater Kuala Lumpur, Malaysia. J Int AIDS Soc. 2017;20(1):21723. doi:10.7448/ias.20.1.21723
30. Pengnonyang S, Ramautarsing RA, Janyam S, et al. Certification of lay providers to deliver key population-led HIV services in Thailand’s National Healthcare System: lessons learned. J Int AIDS Soc. 2022;25(7):e25965. doi:10.1002/jia2.25965
31. Eustaquio PC, Docken SS, Leyritana KT, Wulandari LPL. HIV care cascade among cisgender men who have sex with men in a key population-led community center in the Philippines. Int J STD AIDS. 2021;32(8):718–728. doi:10.1177/0956462420987435
32. Vannakit R, Andreeva V, Mills S, et al. Fast-tracking the end of HIV in the Asia Pacific region: domestic funding of key population-led and civil society organisations. Lancet HIV. 2020;7(5):e366–e72. doi:10.1016/s2352-3018(20)30077-1
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.