Back to Journals » Risk Management and Healthcare Policy » Volume 15
Explore the Relationship Between Short-Term Ambient Air Pollution Exposure and Daily Outpatient Visits for Metabolic Related Fatty Liver
Authors Wang MW ![]() , Sun L, Wen W, Wang J, Wang C, Ni J, Jiang J, Feng ZH
, Sun L, Wen W, Wang J, Wang C, Ni J, Jiang J, Feng ZH ![]() , Cheng YR
, Cheng YR
Received 3 May 2022
Accepted for publication 15 August 2022
Published 19 September 2022 Volume 2022:15 Pages 1751—1759
DOI https://doi.org/10.2147/RMHP.S364270
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mecit Can Emre Simsekler
Ming-Wei Wang,1,* Lixia Sun,2,* Wen Wen,1,* Jie Wang,3 Chun-yi Wang,1 Jie Ni,1 Jing-jie Jiang,1 Zhan-Hui Feng,4 Yong-Ran Cheng5
1Metabolic Disease Center, Affiliated Hospital of Hangzhou Normal University, Hangzhou, People’s Republic of China; 2Zhejiang University of Water Resources and Electric Power, Hangzhou, People’s Republic of China; 3Hangzhou Zhenqi Technology Co., Ltd, Hangzhou, People’s Republic of China; 4Neurological Department, Affiliated Hospital of Guizhou Medical University, Guiyang, People’s Republic of China; 5School of Public Health, Hangzhou Medical College, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhan-Hui Feng; Yong-Ran Cheng, Email [email protected]; [email protected]
Background: Many studies have shown that the pollution of fine particles in the air is related to the incidence of chronic diseases. However, research on air pollution and metabolism-associated fatty liver disease (MAFLD) is limited.
Objective: The purpose of this study was to explore the relationship between short-term ambient air pollution and daily outpatient visits for metabolic-related fatty liver.
Methods: We used a quasi-Poisson regression generalized additive model to stratify analyses by season, age, and gender.
Results: From January 1, 2017, to August 31, 2019, 10,562 confirmed MAFLD outpatient visits were recorded. A 10 μg/m3 increase of fine particular matter (PM10and PM2.5) and NO2 concentrations corresponding with percent change were 0.82 (95% confidence interval [CI], 0.49– 1.15), 0.57 (95% CI, 0.18– 0.98), and 0.86 (95% CI, 0.59– 1.13) elevation in MAFLD outpatient visits. In terms of season, the impact estimates of NO2 and PM2.5% change were 3.55 (95% CI, 1.23– 5.87) and 1.12 (95% CI, 0.78– 1.46) in the hot season and transition season, respectively. Compared with the warm season, the impact estimates of PM10were more significant in the cool season: 2.88 (95% CI, 0.66– 5.10). NO2 has the greatest effect in the transition season, whereas PM10 has the greatest highest effect in the cool and hot seasons. Compared with other pollutants, PM2.5 has the greatest impact in the age stratification, which percent change are 2.69 (95% CI, 0.77– 5.61) and 2.88 (95% CI, 0.37– 6.40) respectively. The impact values of PM2.5 in male and female percent change were 3.60 (95% CI, 0.63– 6.57) and 1.65 (95% CI, 1.05– 2.25), respectively.
Conclusion: This study shows that the air pollutants are related to the number of outpatient visits for MAFLD. The effects of different air pollutants on MAFLD outpatient visits were different by season, ages, and gender.
Keywords: air pollutants, metabolism-associated fatty liver disease, generalized additive model
Introduction
Metabolism-associated fatty liver disease (MAFLD) (formerly known as nonalcoholic fatty liver disease) is the leading cause of liver disease worldwide. Its diagnosis is based on the detection of hepatic steatosis (liver histology, noninvasive biomarkers, or imaging) and the presence of at least one of the three criteria, including clinical evidence of overweight or obesity, type 2 diabetes mellitus, or metabolic dysfunction, such as waist circumference and dyslipidemia or hyperglycemia Studies have shown that the prevalence of MAFLD has increased to a worrying level, creating a huge burden for individuals and the health care system.1,2 In the past 20 years, MAFLD has developed from a relatively unknown disease to the most common chronic liver disease in the world. With rapid changes in lifestyle, the prevalence of MAFLD is considered to be increasing worldwide.3,4 In a model study of eight countries, it was estimated that China’s MAFLD population will increase by 29.1% between 2016 and 2030, reaching 3145.8 million cases.5,6
The World Health Organization analyzed the burden of disease caused by air pollution, finding that more than two million premature deaths each year can be attributed to urban outdoor and indoor air pollution. Four common air pollutants include particulate matter (PM), ozone (O3), nitrogen dioxide (NO2), and sulfur dioxide (SO2).7 The global burden of disease study identified air pollution as the main cause of global burden of disease, especially in developing countries.8,9 Studies have shown that air pollution not only affects respiratory diseases, but also affects acute myocardial infarction, arrhythmia, conjunctivitis, and maletal disorders.10,11
In addition, studies have shown that long-term exposure to PM2.5, PM10, and NO2 is positively associated with the prevalence of the metabolic syndrome.12–14 More and more evidence shows that environmental pollutants such as diesel exhaust particulates, suspended PM, metals, and polychlorinated compounds are important risk factors for the development of MAFLD.15 According to work by Tarantino et al, exposure to ambient air particles with an aerodynamic diameter of 2.5 mm or less (PM2.5) can enhance MAFLD. Therefore, the effect of environmental factors on liver disease has attracted much attention.16 Up to now, some studies on the relationship between fatty liver disease and air pollution have been conducted in animals.17–19 In this study, we performed a quasi-Poisson regression generalized additive model to analyze the relationship between short-term air pollution exposure and fatty liver disease based on outpatient visits to the Affiliated Hospital of Hangzhou Normal University in Hangzhou.
Materials and Methods
Air Pollution and Meteorological Data
Air quality monitoring stations are located in Hangzhou, providing daily values of PM2.5 (μg/m3), PM10 (μg/m3), SO2 (μg/m3), O3 (μg/m3), NO2 (μg/m3), CO (μg/m3), relative humidity (%), and mean temperature (°C). The details of Affiliated Hospital of Hangzhou Normal University and specific air quality monitoring stations are shown in the Figure S1. The daily air pollution parameters and temperatures of Hangzhou between January 1, 2017, and August 31, 2019, were downloaded from the China Meteorological Administration website (http://data.cma.cn/). The daily concentrations are represented 24-hour averages, and the O3 concentration was the maximal 8-hour average from all valid monitoring sites in this study.
Study Population
Data for patients with MAFLD from January 2017 to August 2019 were collected from the outpatient database of Affiliated Hospital of Hangzhou Normal University. Patients diagnosed with MAFLD who attended outpatient visits were included in this study. A MAFLD diagnosis is based on the detection of hepatic steatosis (liver histology, noninvasive biomarkers, or imaging) and the presence of at least one of the three criteria, including clinical evidence of overweight or obesity, type 2 diabetes mellitus, or metabolic dysfunction, such as waist circumference and dyslipidemia or hyperglycemia.20 According to the latest diagnostic standard conditions, the diagnostic program is written with R (The R Foundation R Foundation for Statistical Computing, Vienna, Austria) to re-diagnose the outpatient information recorded in the hospital outpatient database.
In this study, a total of 11,731 outpatient visits, 378 cases of missing information and error were excluded, and 791 cases not living in Hangzhou for a long time were also excluded. Finally, 10,562 outpatient visits with MAFLD were analyzed. The ethics committee of Affiliated Hospital of Hangzhou Normal University approved all the procedures performed in this study, and complied with the Declaration of Helsinki.
Statistical Methods
A generalized additive model (GAM) was used in the statistical analysis to analyze the data. Because daily hospital cases typically followed an over dispersed Poisson distribution, quasi-Poisson regression was used in the GAM.21 Several covariates including natural splines were introduced to control their potential confounding effects. First, a natural cubic regression smoothing function of calendar time with 7 degrees of freedom (df) per year excluded unmeasured long-term and seasonal trends longer than two months. Second, a natural smooth function of the mean temperature (6 df) and relative humidity (3 df) controlled the nonlinear confounding effects of weather conditions. Third, indicator variables were implemented for “day of the week” and public holidays.22 Briefly, the following log-linear GAM was fitted to obtain the estimated pollution log-relative rate β in the selected city:

where  is the expected number of MAFLD outpatient visits at day t; β is the log-related rate of MAFLD associated with a unit increase of air pollutants;
is the expected number of MAFLD outpatient visits at day t; β is the log-related rate of MAFLD associated with a unit increase of air pollutants;  is the pollutant concentrations at day t; DOW is a dummy variable for the day of the week; ns is the natural cubic regression smooth function.
is the pollutant concentrations at day t; DOW is a dummy variable for the day of the week; ns is the natural cubic regression smooth function.
All these cases were stratified by age (<45 and ≥45 years), by Gender (male female) and cool season (November to March), hot season (June to August), and transition season (April, May, September, and October).After establishing the basic model, single-pollutant models were initially used and introduced, a priori, in turn each air pollutant concentration on the concurrent day (lag0). Given that the health effects of ambient air pollutants could last for multiple days, more single lag days were used (lag0, lag1, lag2, lag3, lag4, lag5, and lag6), and the moving average exposure of multiple days (lag01, lag02, lag03, lag04, lag05, lag06, and lag07) were obtained. To verify the stability of the model, two-pollutant models were built to evaluate the stability of effect estimates after adjusting for the co-pollutants. Co-pollutants with a correlation coefficient < 0.7 were added to the two-pollutant model.
The effects are expressed as the percentage of change and 95% CI in daily hospital MAFLD outpatient visits per 10 μg/m3 increase in pollutant concentrations. The statistical tests were two-sided, and the effects with p < 0.05 were considered to be statistically significant. All statistical models were constructed using R software version 3.6.0 (R Foundation for Statistical Computing, version 3.6.1; http://www.Rproject.org) using the MGCV package.
Results
The basic descriptive statistics of the number of outpatient visits, pollutants, and meteorological data are shown in Table 1. From January 1, 2017, to August 31, 2019, 10,562 confirmed outpatient visits were reported. During this period, the average number of cases per day was 8.94, and the number of cases in winter was more than that in summer or transition seasons. During the study period, the daily average concentrations of NO2, SO2, PM10, O3, and PM2.5 were 48.43 µg/m3, 35.89 µg/m3, 56.80 µg/m3, 137.50 µg/m3, and 48.91 μg/m3, respectively. The daily average humidity and temperature were 75.21% and 18.45 °C, respectively.
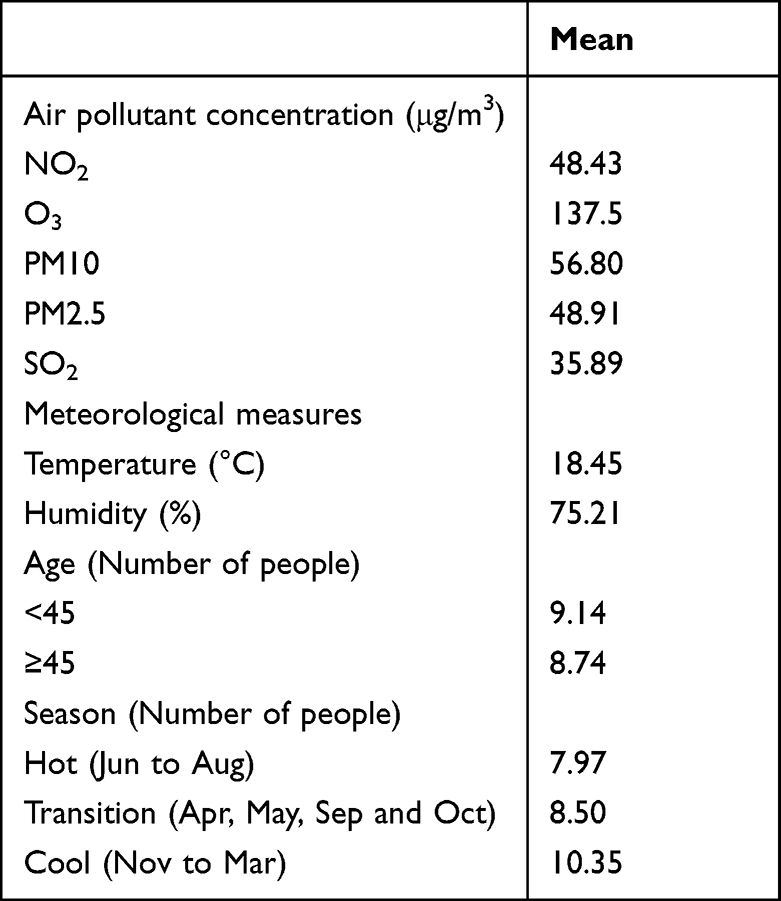 |
Table 1 Summary Statistics of Daily Air Pollutants, Weather Conditions, and Number of Outpatient Visits Caused by MAFLD (N = 10,562) in Hangzhou from 2017.1 to 2019.08 |
Figure 1 shows significant differences among the five different air pollution indicators and number of outpatient visits in three different seasons. The daily air pollution concentration and the number of MAFLD outpatient visits (except O3) are the greatest in the cool season and the lowest in the hot season. The number of outpatient visits is the greatest in hot seasons. The Spearman correlation coefficients of PM2.5, PM10, SO2, and NO2 were 0.68 to 0.95. The maximum 8-hour mean O3 concentration negatively correlated with PM2.5, PM10, SO2, and NO2 (Spearman correlation coefficient ranged from 0.27 to 0.06) (Figure 2).
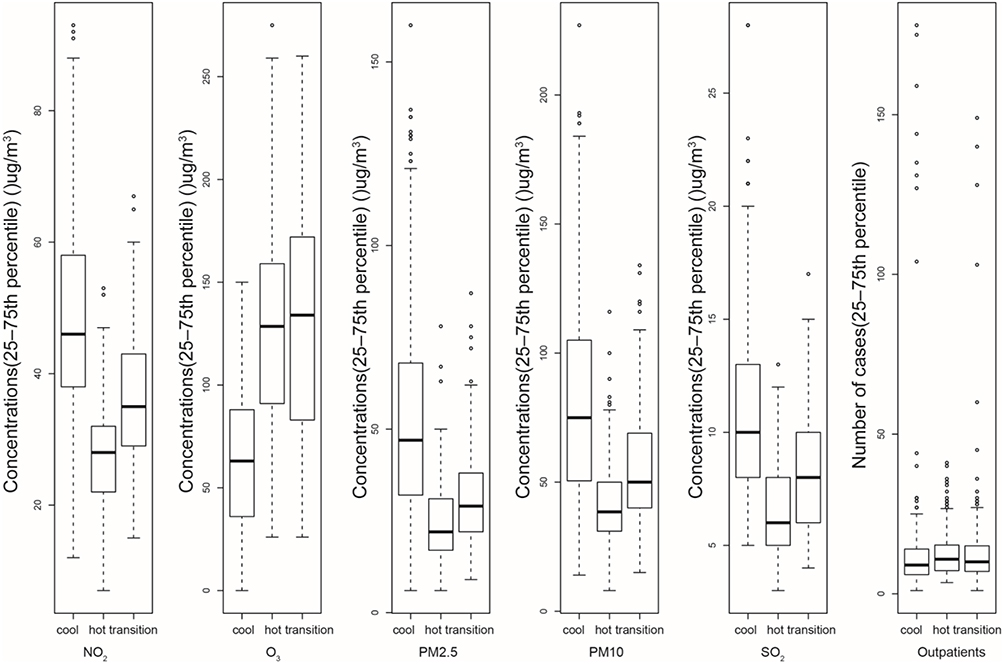 |
Figure 1 Box plots of five air pollutants in the cool, transition, warm seasons and outpatient visits cases. Boxes indicate the interquartile range (25–75th percentile); lines within boxes !indicate medians; whiskers below the boxes represent minimum values; whiskers and dots above the boxes indicate the maximum values. |
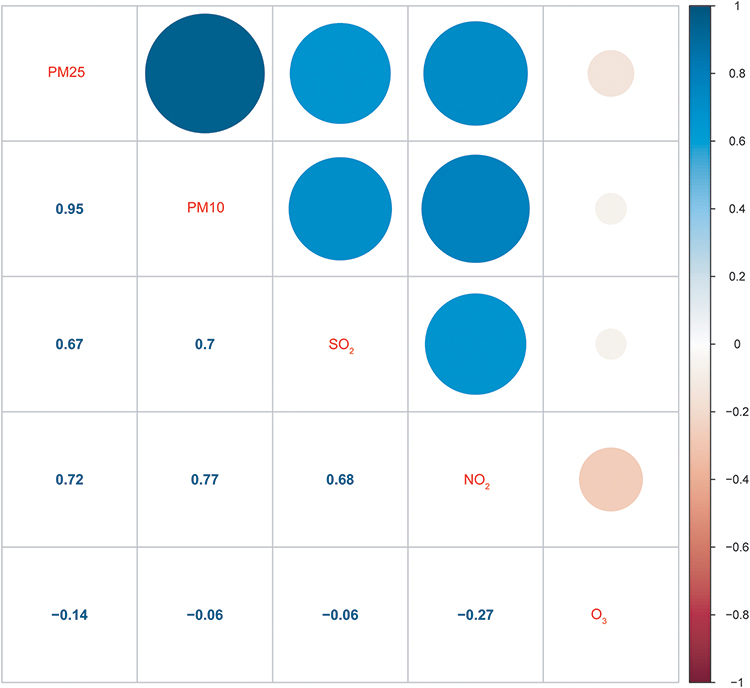 |
Figure 2 NO2, O3, PM10, PM2.5, and SO2 correlation coefficient matrix.(The upper right corner matrix represents the correlation size, the lower left corner matrix is the correlation coefficient, and the right bar is the correlation coefficient contrast color). |
In terms of seasons, the effect of ambient air pollution on the total number of outpatient visits with MAFLD shows significant differences among the three seasons (Table 2). The impact estimates of NO2 and PM2.5 were 3.55 (95% CI, 1.23–5.87) and 1.12 (95% CI, 0.78–1.46) in the transition season, respectively. Compared with the warm season, the impact estimates of PM10 were more significant in the cool season: 2.88 (95% CI, 0.66–5.10). NO2 has the greatest effect in the transition season, whereas PM10 has the greatest effect in the cool and hot seasons. Regarding age, the study shows an increase in the correlation percentage between NO2, PM10, PM2.5, and the total number of outpatient visits with MAFLD varies with age groups. The older the age, the greater the impact estimate. In the two age groups with 45 years as the dividing line, PM2.5 has the highest impact estimate: 2.69 (95% CI, 0.77–5.61) and 2.88 (95% CI, 0.37–6.40), respectively. Regarding gender, compared with females, NO2, PM10, and PM2.5 had a greater impact on males, especially PM2.5. The impact values of PM2.5 in male and female were 3.60 (95% CI, 0.63–6.57) and 1.65 (95% CI, 1.05–2.25), respectively.
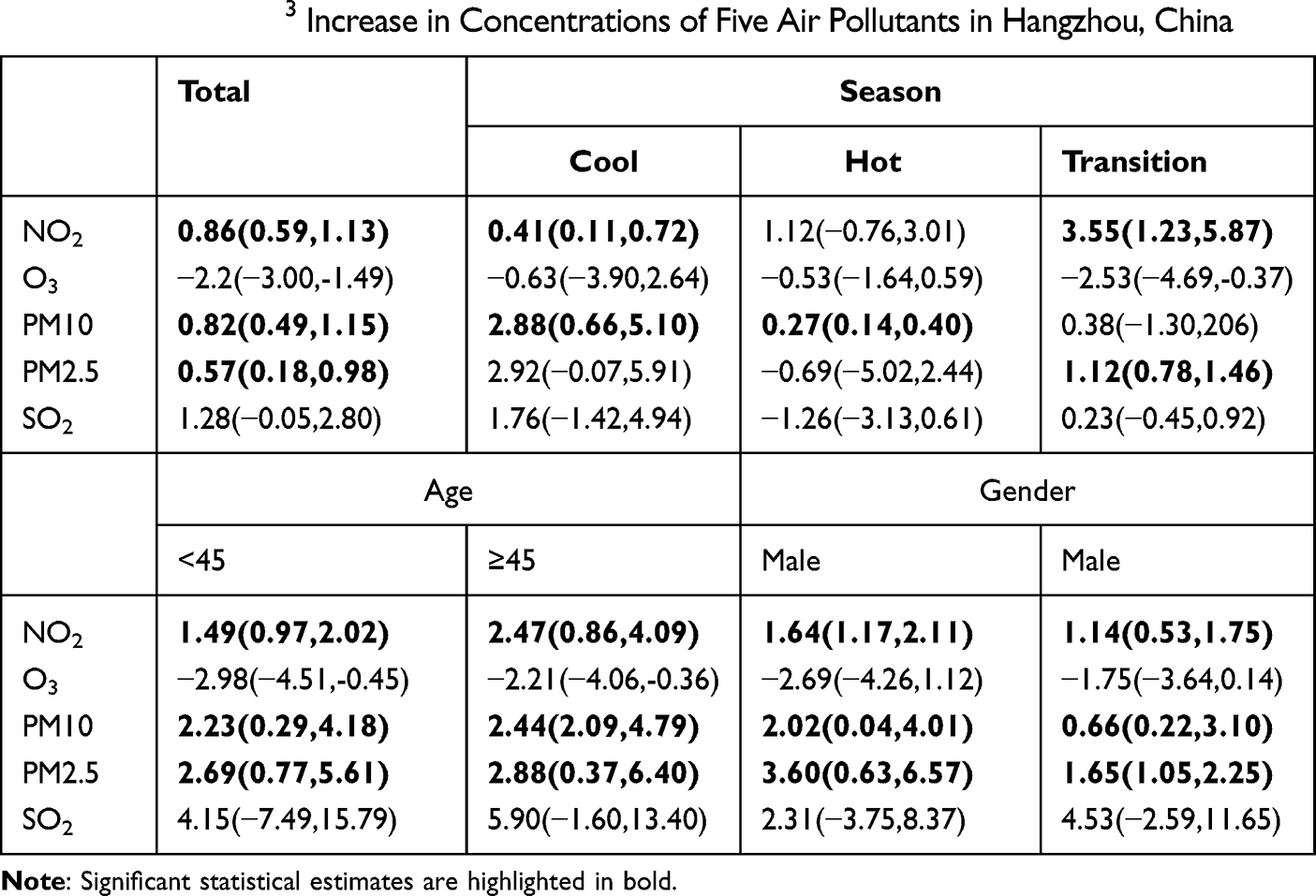 |
Table 2 Percent Change (95% CI) in MAFLD Outpatient Visits Caused by Total, Season, Gender, and Age per 10 μg/m3 Increase in Concentrations of Five Air Pollutants in Hangzhou, China |
Figure 3 shows the results obtained from the single-lag day (lag0–lag6) and cumulative exposure models (lag01–lag07) for the percent increase in MAFLD outpatient visits per 10 μg/m3 increase in pollutants. Statistically significant results were observed at lag 0–4 and 01–07 day for NO2, lag 0 and 01–04 day for PM10, lag 0 and 01–03 day for PM2.5, and lag 01–03 day for SO2. Table 3 shows the results of two-pollutant models using exposure at lag 01. The magnitudes of all five pollutants were stable The effect estimates of NO2, PM10, and PM2.5 pollutants remained statistically significant when adjusting for co-pollutants.
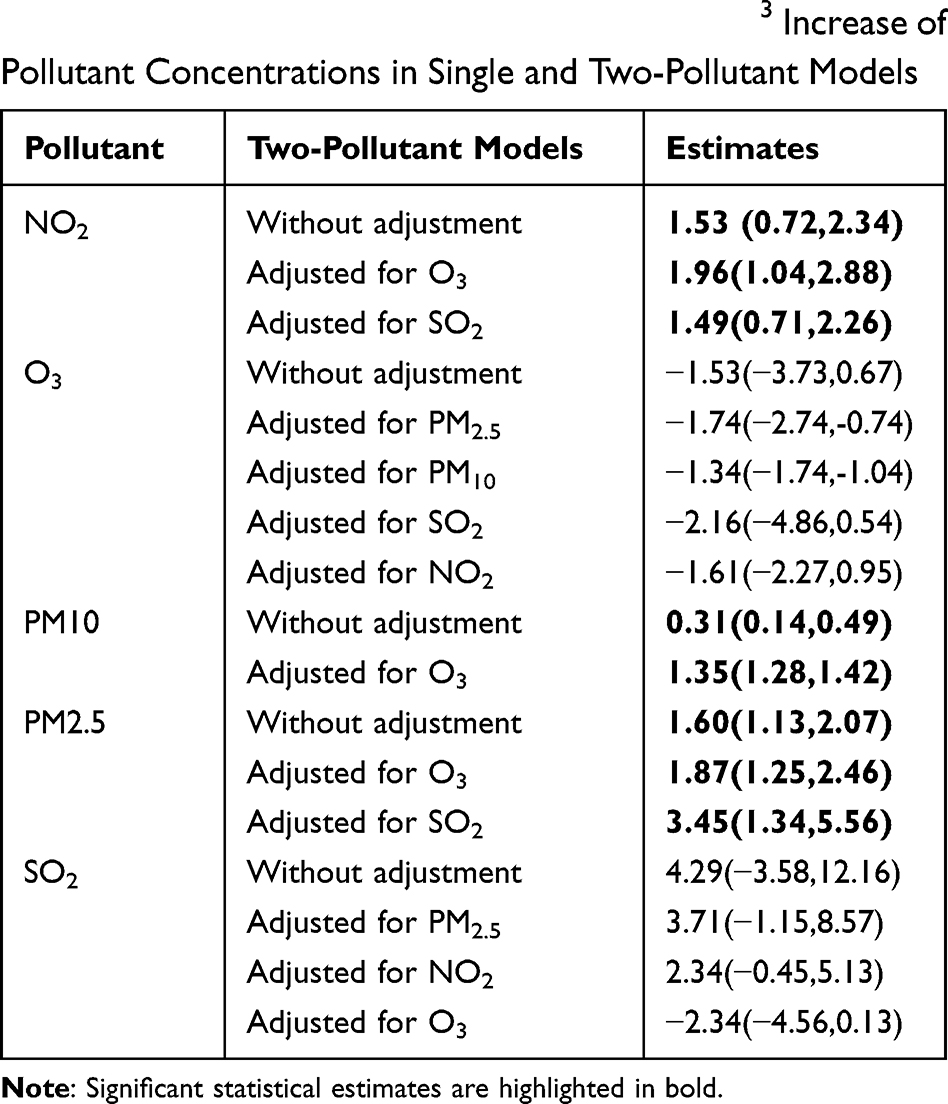 |
Table 3 Percent Change (Mean and 95% Confidence Intervals) of Daily Outpatient Visits Associated with 10 μg/m3 Increase of Pollutant Concentrations in Single and Two-Pollutant Models |
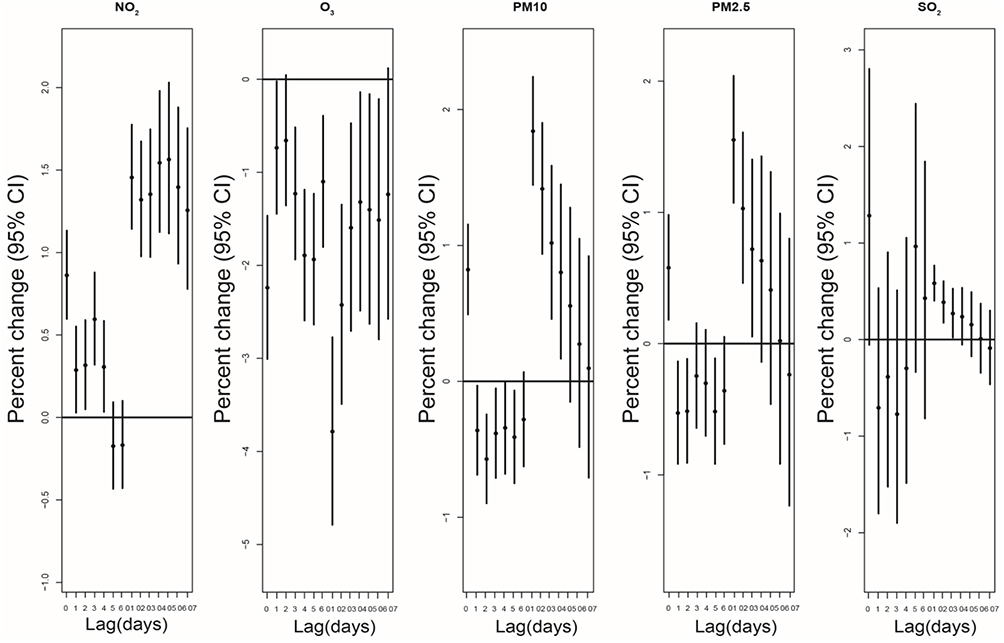 |
Figure 3 Percent increase of MAFLD outpatient visits cases with 10 μg/m3 increase of NO2, O3, PM10, PM2.5, and SO2 in different lag days. |
Discussion
This study shows that the air pollutants in Hangzhou are related to the number of outpatient visits for MAFLD. The effects of different air pollutants on MAFLD outpatient visits were different for different seasons, ages, and genders. The most significant associations of air pollution appeared on single days and the associations in the cumulative exposure models were still positive. Regarding seasonal variations, NO2 showed the greatest effect in the transition season, whereas PM10 had the greatest effect in the cool and hot seasons. The effect of PM10 was more significant in the cool season. Regarding variations with age, in the two age groups with 45 years as the dividing line, PM2.5 has the highest impact estimation: the older the person, the greater the impact. Regarding gender, this study shows that males are more vulnerable to air pollutants, especially PM2.5. Our study shows a significant correlation between the PM in the air and the outpatient visits for MAFLD.
With regard to the pathogenesis of MAFLD, inflammation and oxidative stress caused by the metabolic syndrome are widely considered as the key factors in the pathogenesis of nonalcoholic fatty liver disease.23 In addition, many studies showed that the systemic proinflammatory and oxidative responses induced by air pollutants are associated with the metabolic syndrome.24–27 Therefore, it can be concluded that air pollutants are related to the pathogenesis of MAFLD. Our findings are consistent with this conclusion. In addition to oxidative stress, the activation of Kupffer cells and macrophages, as well as the production of cytokines and chemokines, plays a central role in the progression of MAFLD. Studies have shown that the particles in the air enter the circulation through the alveolar membrane and reach the liver; these fine particles in circulation can then accumulate in the Kupffer cells and induce the secretion of cytokines in Kupffer cells, in turn leading to inflammation and collagen synthesis in hepatic stellate cells.28,29 This study suggests that there are gender differences in the effects of air pollutants on fatty liver disease. Relevant studies indicate that this gender difference can be attributed to the differences in biological characteristics, such as sex hormone levels, body size, lung size, and growth, which may affect the biological transport of environment-derived chemicals.30
In addition, studies have shown that lifestyle such as physical activity patterns and dietary intake may also lead to gender-specific air pollution effects. Compared with girls, boys are more likely to engage in outdoor sports and take in more solid substances,31 and boys participate in more moderate-to-intense sports activities.32 This difference may cause boys to be more vulnerable to air pollution exposure than girls. Regarding the differences in age, previous studies have shown that the elderly are more vulnerable to air pollution than younger people.33,34 However, some studies have reported, that compared with the elderly, young people may be more prone to lipid metabolism disorders.35 In addition, we did not find relevant literature to explain the mechanism of age in the effect of air pollutants on MAFLD; therefore, our conclusion that “the older the age, the greater the impact of air pollutants” should be verified in a larger sample.
This study has some limitations. Potential confounding factors such as body mass index, education level, smoking habits, and drug use history may also have an impact on the relationship between air pollutants and fatty liver disease. Second, we only collected the daily number of outpatient visits from one hospital, which may not represent the overall level of the city.
Conclusion
This study concluded that the number of outpatient visits for MAFLD is related to air pollution exposure. The effects of different air pollutants on MAFLD outpatient visits were different in different seasons, ages, and genders. It suggests that sufficient health counseling about hot temperature exposure and transition seasons should be included in care programs for patients with MAFLD.
Data Sharing Statement
The original data are available on request to Ming-Wei Wang, or at the Affiliated Hospital of Hangzhou Normal University, Hangzhou, 310014, China.
Consent for Publication
Not applicable. All data were supplied and analysed in an anonymous format, without access to personal identifying information.
Acknowledgment
The presented study was Medical and Technology Project of Zhejiang Province (No.2021HY127, No.2020362651, No.2021KY890); Hangzhou science and Technology Bureau fund (No.20191203B96;No.20191203B105); Clinical Research Fund of Zhejiang Medical Association (No.2020ZYC-A13); Hangzhou Health and Family Planning Technology Plan key projects (2017ZD02).
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or critically revising it for important intellectual content; agreed to submit to the current journal; gave final approval for the version to be published; and agreed to be accountable for all aspects of the work.
Disclosure
The authors declare that there is no conflict of interests regarding the publication of this paper.
References
1. Eslam M, Sarin SK, Wong VW, et al. The Asian Pacific Association for the Study of the Liver clinical practice guidelines for the diagnosis and management of metabolic associated fatty liver disease. Hepatol Int. 2020;14:889–919. doi:10.1007/s12072-020-10094-2
2. Wong MCS, Huang JLW, George J, et al. The changing epidemiology of liver diseases in the Asia-Pacific region. Nat Rev Gastroenterol Hepatol. 2019;16:57–73. doi:10.1038/s41575-018-0055-0
3. Sarin SK, Kumar M, Eslam M, et al. Liver diseases in the Asia-Pacific region: a lancet gastroenterology and hepatology commission. Lancet Gastroenterol Hepatol. 2020;5:167–228. doi:10.1016/S2468-1253(19)30342-5
4. Li J, Zou B, Yeo YH, et al. Prevalence, incidence, and outcome of non-alcoholic fatty liver disease in Asia, 1999–2019: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2019;4:389–398. doi:10.1016/S2468-1253(19)30039-1
5. Li H, Guo M, An Z, et al. Prevalence and risk factors of metabolic associated fatty liver disease in Xinxiang, China. Int J Environ Res Public Health. 2020;17:1818. doi:10.3390/ijerph17061818
6. Murray CJ, Ezzati M, Flaxman AD, et al. GBD 2010: design, definitions, and metrics. Lancet. 2012;380:2063–2066. doi:10.1016/S0140-6736(12)61899-6
7. Lee KW, Choi YH, Hwang SH, et al. Outdoor air pollution and pterygium in Korea. J Korean Med Sci. 2017;32:143–150. doi:10.3346/jkms.2017.32.1.143
8. GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388:1659–1724. doi:10.1016/S0140-6736(16)31679-8
9. Cohen AJ, Brauer M, Burnett R, et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the global burden of diseases study 2015. Lancet. 2017;389:1907–1918. doi:10.1016/S0140-6736(17)30505-6
10. Wang MW, Chen J, Cai R. Air quality and acute myocardial infarction in adults during the 2016 Hangzhou G20 summit. Environ Sci Pollut Res Int. 2018;25:9949–9956. doi:10.1007/s11356-017-1136-2
11. Wang M, Chen J, Zhang Z, et al. Associations between air pollution and outpatient visits for arrhythmia in Hangzhou, China. BMC Public Health. 2020;20:1524. doi:10.1186/s12889-020-09628-y
12. Chen J, Cheng Y, Zhou M, et al. Machine learning prediction on number of patients due to conjunctivitis based on air pollutants: a preliminary study. Eur Rev Med Pharmacol Sci. 2020;24:10330–10337. doi:10.26355/eurrev_202010_23380
13. Qiu H, Zhu X, Wang L, et al. Attributable risk of hospital admissions for overall and specific mental disorders due to particulate matter pollution: a time-series study in Chengdu, China. Environ Res. 2019;170:230–237. doi:10.1016/j.envres.2018.12.019
14. Sun S, Yang Q, Zhou Q, et al. Long-term exposure to air pollution, habitual physical activity and risk of non-alcoholic fatty liver disease: a prospective cohort study. Ecotoxicol Environ Saf. 2022;235:113440. doi:10.1016/j.ecoenv.2022.113440
15. Xu H, Chen L, Chen G, et al. China Multi-Ethnic Cohort collaborative g. Exposure to air pollution is associated with an increased risk of metabolic dysfunction-associated fatty liver disease. J Hepatol. 2022;76(3):518–525. doi:10.1016/j.jhep.2021.10.016
16. VoPham T, Kim NJ, Berry K, Mendoza JA, Kaufman JD, Ioannou GN. Pm2.5 air pollution exposure and nonalcoholic fatty liver disease in the nationwide inpatient sample. Environ Res. 2022;213:113611. doi:10.1016/j.envres.2022.113611
17. Yang J, Wei Q, Peng X, Peng X, Yuan J, Hu D. Relationship between Methyl Tertiary Butyl ether exposure and non-alcoholic fatty liver disease: a cross-sectional study among petrol station attendants in Southern China. Int J Environ Res Public Health. 2016;13:946. doi:10.3390/ijerph13100946
18. Tarantino G, Capone D, Finelli C. Exposure to ambient air particulate matter and non-alcoholic fatty liver disease. World J Gastroenterol. 2013;19:3951–3956. doi:10.3748/wjg.v19.i25.3951
19. VoPham T. Environmental risk factors for liver cancer and nonalcoholic fatty liver disease. Curr Epidemiol Rep. 2019;6:50–66. doi:10.1007/s40471-019-0183-2
20. Treviño LS, Katz TA. Endocrine disruptors and developmental origins of nonalcoholic fatty liver disease. Endocrinology. 2018;159:20–31. doi:10.1210/en.2017-00887
21. Deierlein AL, Rock S, Park S. Persistent endocrine-disrupting chemicals and fatty liver disease. Curr Environ Health Rep. 2017;4:439–449. doi:10.1007/s40572-017-0166-8
22. Chen R, Yin P, Meng X, et al. Fine particulate air pollution and daily mortality. A Nationwide analysis in 272 Chinese cities. Am J Respir Crit Care Med. 2017;196:73–81. doi:10.1164/rccm.201609-1862OC
23. Yang C, Chen A, Chen R, et al. Acute effect of ambient air pollution on heart failure in Guangzhou, China. Int J Cardiol. 2014;177:436–441. doi:10.1016/j.ijcard.2014.09.003
24. Li H, Chen R, Meng X, et al. Short-term exposure to ambient air pollution and coronary heart disease mortality in 8 Chinese cities. Int J Cardiol. 2015;197:265–270. doi:10.1016/j.ijcard.2015.06.050
25. Younossi Z, Tacke F, Arrese M, et al. Global perspectives on nonalcoholic fatty liver disease and nonalcoholic steatohepatitis. Hepatology. 2019;69:2672–2682. doi:10.1002/hep.30251
26. Estes C, Anstee QM, Arias-Loste MT, et al. Modeling NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016–2030. J Hepatol. 2018;69:896–904. doi:10.1016/j.jhep.2018.05.036
27. Xu MX, Ge CX, Qin YT, et al. prolonged PM2.5 exposure elevates risk of oxidative stress-driven nonalcoholic fatty liver disease by triggering increase of dyslipidemia. Free Radic Biol Med. 2019;130:542–556. doi:10.1016/j.freeradbiomed.2018.11.016
28. Kelishadi R, Mirghaffari N, Poursafa P, Gidding SS. Lifestyle and environmental factors associated with inflammation, oxidative stress and insulin resistance in children. Atherosclerosis. 2009;203:311–319. doi:10.1016/j.atherosclerosis.2008.06.022
29. cCullough AJ. Pathophysiology of nonalcoholic steatohepatitis. J Clin Gastroenterol. 2006;40(Suppl 1):S17–29.
30. Tan HH, Fiel MI, Sun Q, et al. Kupffer cell activation by ambient air particulate matter exposure may exacerbate non-alcoholic fatty liver disease. J Immunotoxicol. 2009;6:266–275. doi:10.3109/15476910903241704
31. Clougherty JE. A growing role for gender analysis in air pollution epidemiology. Environ Health Perspect. 2010;118:167–176. doi:10.1289/ehp.0900994
32. Cohen DA, McKenzie TL, Sehgal A, Williamson S, Golinelli D, Lurie N. Contribution of public parks to physical activity. Am J Public Health. 2007;97:509–514. doi:10.2105/AJPH.2005.072447
33. Tong L, Li K, Zhou Q. Season, sex and age as modifiers in the association of psychosis morbidity with air pollutants: a rising problem in a Chinese metropolis. Sci Total Environ. 2016;541:928–933. doi:10.1016/j.scitotenv.2015.09.066
34. Song J, Zheng L, Lu M, et al. Acute effects of ambient particulate matter pollution on hospital admissions for mental and behavioral disorders: a time-series study in Shijiazhuang, China. Sci Total Environ. 2018;636:205–211. doi:10.1016/j.scitotenv.2018.04.187
35. Chen HJ, Li GL, Sun A, Peng DS, Zhang WX, Yan YE. Age differences in the relationship between secondhand smoke exposure and risk of metabolic syndrome: a meta-analysis. Int J Environ Res Public Health. 2019;16:1409. doi:10.3390/ijerph16081409
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.