Back to Journals » Journal of Multidisciplinary Healthcare » Volume 11
Exploration of the contexts surrounding the implementation of an intervention supporting return-to-work after breast cancer in a primary care setting: starting point for an intervention development
Authors Bilodeau K ![]() , Tremblay D
, Tremblay D ![]() , Durand MJ
, Durand MJ
Received 30 September 2017
Accepted for publication 19 December 2017
Published 1 February 2018 Volume 2018:11 Pages 75—83
DOI https://doi.org/10.2147/JMDH.S152947
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Karine Bilodeau,1,2 Dominique Tremblay,2,3 Marie-José Durand4,5
1Faculty of Medicine and Health Sciences, Université de Sherbrooke, Longueuil, QC, Canada; 2Hôpital Charles-LeMoyne Research Center, Longueuil, QC, Canada; 3School of Nursing, Faculty of Medicine and Health Sciences, Université de Sherbrooke, Longueuil, QC, Canada; 4School of Rehabilitation, Faculty of Medicine and Health Sciences, Université de Sherbrooke, Longueuil, QC, Canada; 5Centre for Action in Work Disability Prevention and Rehabilitation, Longueuil, QC, Canada
Background: Many recommendations have been made regarding survivorship care provided by teams of primary care professionals. However, the nature of that follow-up, including support for return-to-work (RTW) after cancer, remains largely undefined. As implementation problems are frequently context-related, a pilot study was conducted to describe the contexts, according to Grol and Wensing, in which a new intervention is to be implemented. This pilot study is the first of three steps in intervention development planning.
Method: In-depth semi-structured interviews (n=6) were carried out with stakeholders selected for their knowledgeable perspective of various settings, such as hospitals, primary care, employers, and community-based organizations. Interviews focused on participants’ perceptions of key contextual facilitators and barriers to consider for the deployment of an RTW intervention in a primary care setting. Data from interviews were transcribed and analyzed. A content analysis was performed based on an iterative process.
Results: An intervention supporting the process of RTW in primary care makes sense for participants. Results suggest that important levers are present in organizational, professional, and social settings. However, many barriers, mainly related to organizational settings, have been identified, eg, distribution of tasks for survivor follow-up, continuity of information, and coordination of care between specialized oncology care and general primary care.
Conclusion: To develop and deploy the intervention, recommendations that emerged from this pilot study for overcoming barriers were identified, eg, training (professionals, survivors, and employers), the use of communication tools, and adopting a practice guide for survivor care. The results were also helpful in focusing on the relevance of an intervention supporting the RTW process as a component of primary care for survivors.
Keywords: complex intervention, primary care, cancer survivorship, return-to-work, knowledge translation approach
Background
Over the past few decades, the number of breast cancer (BC) survivors, ie, adults who complete cancer treatment that is of curative intent,1 has climbed steadily, thanks to early screening and major advances in cancer treatment.2 However, survivors face many challenges after completing cancer treatments, including return-to-work (RTW),3 defined as a complex process that involves “work reentry” and “work retention.”4,5 The RTW process is important for some survivors, as resuming one’s working role fosters the continuation of social interactions, self-esteem, financial security, and psychological well-being.6–9 Despite these benefits, it is often difficult for women to RTW and keep working as long as they would like. They face challenges associated with the recurrent effects of the cancer or treatments (eg, fatigue, pain),10 as well as challenges associated with the workplace (eg, lack of support from supervisors and colleagues, lay-offs, stigmatization).11,12 In addition, follow-up care diminishes in intensity during the RTW process once active treatment for BC is completed.13 Some authors have suggested interventions with multiple components (eg, educational, physical, vocational, and psychoeducational activities) and several levels (survivor, health care professional, employer) to address issues related to RTW after cancer.13–16 This type of multifaceted intervention is similar to complex interventions17 in which implementation strongly depends on the setting, in which various stakeholders have multiple, often competing objectives.18 To date, few multilevel interventions (survivor, health care professional, employer) designed to support RTW have been put forward. Considering the many challenges associated with the RTW process, there is reason to believe that these women would benefit from interventions by primary care health care professionals as soon as active treatments end in order to attenuate the impact of side effects and thus facilitate work reentry. A pilot study was performed to provide recommendations for the later development of early intervention supporting RTW after primary care for BC. This pilot study is the first of three steps in intervention development planning. The other steps were exploration of the RTW process of BC survivors and the collaborative creation of the intervention with different stakeholders (eg, BC survivors, health care professionals).
The Medical Research Council notes the importance of suggesting adapted interventions and understanding the context in which they are deployed.17,19 According to Pfadenhauer et al,20 the context is more than a physical location, as it may include roles, interactions and relationships at multiple levels, as well as a set of characteristics and circumstances. A good number of papers emphasize that the characteristics of the context may influence the implementation of the intervention, acting as either barrier or facilitator.21 In oncology care, several promising interventions have not been integrated into primary care practice due to context-related implementation problems. For example, survivorship care plans are seldom used in primary care or specialized care, even though practice guides encourage their use.22 Many barriers to making the survivorship care plan an integral part of existing practice have been reported, including low “buy-in” from primary care professionals23 and the lack of dedicated resources.24,25 There are grounds for believing that similar issues could be raised in the development and implementation of an intervention designed to promote RTW in primary care. For this reason, it is necessary to contextualize the intervention to locate levers and barriers, assign priorities, and attempt to understand their synergy.
As part of the development of an intervention to support RTW for BC survivors in primary care, a pilot study was conducted to improve our understanding of the context for the intervention. An approach inspired by integrated knowledge translation was chosen, as it involves stakeholders to facilitate understanding of the real context.26 In addition, the involvement of stakeholders makes it easier to identify barriers and facilitators, as well as interventions that should be given priority.27
The aim of this pilot study is to describe the contexts, according to Grol and Wensing,28 in which the new intervention is to be implemented. More precisely, the objectives were: 1) to explore the opinions of different stakeholders on the role that primary care could play in supporting the RTW process after BC; and 2) to identify perceived barriers and facilitators to the deployment of this new intervention in a primary care setting in Quebec (Canada).
Framework
Given the complexity of the development of the intervention enhancing RTW, the pilot study was guided by the Knowledge to Action framework26,29 and the barriers and facilitators identified by Grol and Wensing28 related to Improving Patient Care: The Implementation of Change in Health Care. First of all, the Knowledge to Action framework, built on the theory of planned behavior, suggests an iterative and dynamic process of exchanges between researchers and potential knowledge users to facilitate the implementation of meaningful results, in this case an intervention to support RTW. This model suggests that the development of an RTW intervention in primary care integrates available research evidence as well as stakeholders’ knowledge over seven action phases: 1) identifying the problem and selecting knowledge; 2) adapting knowledge to the local context; 3) evaluating factors that present obstacles or contribute to the use of knowledge; 4) selecting, adapting, and implementing interventions that eliminate barriers to the use of knowledge; 5) monitoring the use of knowledge; 6) evaluating results; and 7) creating mechanisms for maintaining the use of knowledge.
Since the various action phases are interconnected in an iterative process, it is possible to document “identifying the problem” and “evaluating favorable factors and barriers” jointly. The contexts identified by Grol and Wensing28 are useful in guiding the description of favorable factors and barriers. The authors state that it is important to identify these factors to be in a position to develop consistent implementation strategies for different contexts: individual health care professionals’ context (eg, skills, attitudes, values, knowledge), the social context (eg, patients’ preferences, expectations, knowledge, needs, attitude and behavior of colleagues, culture in the social network), the organizational context (eg, financial resources, care organization, division of tasks), and the economic and legal context (eg, rules, regulations, laws).
Method
To explore stakeholders’ opinions on the development and implementation of a new intervention, six semi-directed interviews were conducted, using snowball sampling.30 Key informants identified potential participants who were involved in the RTW journey of women who had received treatment for BC in the same geographic region (Quebec, Canada). Participants were to represent oncology care (hospital), community care and services (family medicine unit, nonprofit organization for people with cancer), and employers. The potential participants were contacted by telephone or e-mail to present the project, answer their questions, and validate their interest. Four health care professionals (physicians, nurse, and psychologist), a representative of a community organization, and an occupational health and safety officer from a hospital were recruited (Table 1). All the participants signed consent forms and were told that the data would remain confidential. An interview guide based on items from the reference framework was used to direct the conversation (Box 1). Interviews lasted an average of 35 minutes and were digitally recorded. Interviews were performed in French; a professional translator translated the manuscript from French to English to ensure the quality of the language and the scientific work.
 | Table 1 Sample characteristics |
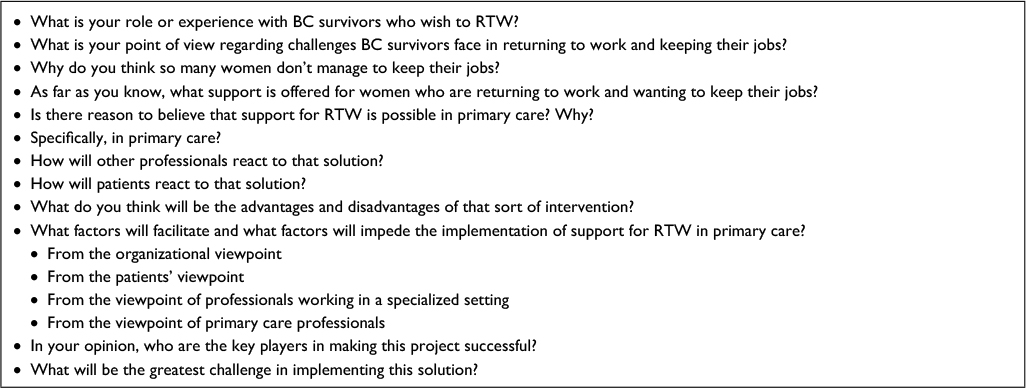 | Box 1 Interview guide |
Data analysis
The transcribed data were put through a qualitative analysis of consistent content and an iterative process including the following activities: condensation, presentation of data, and development and verification of the conclusions.31 According to this process, two coding cycles were performed. The first cycle of structural coding32 was designed to assign specific codes to issues related to the RTW process after a BC diagnosis, as well as the role of primary care in the RTW process, favorable factors, processes, and barriers to implementing the intervention. These data were displayed in a summary table. Participants’ perspectives on the issues emerged. In the second cycle, data were skimmed to identify barriers and facilitators. We used a coding grid based on the barriers and facilitators identified by Grol and Wensing.28 Content analysis summary tables were created to make connections between the barriers and facilitators perceived by participants according to different contexts (organizational, health care professional, social, economic, and legal). QDA Miner v.4.0.11 software was used to manage qualitative data.31 The following measures were taken by the researchers to ensure reliability, validity, and transferability31: 1) the interviews were listened to after each cycle of coding to review the codes and themes to ensure that the results were truly representative of participants’ perspectives; 2) all authors gave feedback to explore differences and refine codes; and 3) the context of this pilot study was documented in a detailed fashion.
Ethical considerations
Ethical approval was obtained from the Office of Research Ethics and Integrity at Ottawa University before the study commenced. All participants signed consent forms and were told that the data would remain confidential. They received a copy of the consent form.
Results
Stakeholders’ perceptions of RTW after BC
Participants from different milieux (eg, community organizations, employers) presented a converging vision of major challenges relating to the process of RTW after cancer. They mentioned that BC survivors had trouble keeping their jobs. Some said that work reentry came too soon, and recurring symptoms of cancer and treatments (eg, fatigue, cognitive difficulties) were barriers to continuing employment. A gap was reported between the survivor’s ability to complete the prescribed tasks and the employer’s expectations in terms of the desired productivity. It was even noted that some BC survivors have to ask for sick leave again due to symptoms of depression or burnout. A participant explained the situation:
They’re often able to achieve good results at work but after two hours [of concentration] they’re exhausted […] it takes a lot of effort […] it takes a lot of compensation strategies for a while […] often the recovery period after treatment is not completed before RTW so they go back to work with gaps right from the start. (Onco_context #2)
Participants explained that accommodations were offered at the beginning of the work reentry process, but very little planning was done to ensure that they could keep working. Here is an example:
A few years ago, RTW wasn’t planned and it felt like the person was coming back to work as if she’d just had a bad cold. In some cases it is still like that, but I think many employers do act in good faith and really try to accommodate the person and plan RTW properly. Where I think there are enormous gaps is [when] RTW is planned but I’m not sure whether they’ve planned properly for the person to keep on working. (Com_context #1)
Participants also agreed that there are limited resources for supporting patients with RTW after BC. While they are on sick leave, BC survivors find it difficult to gain access to resources that are available in hospitals. Community services are underdeveloped for this group:
I’d like to be able to say that there are lots of resources but there aren’t; I think we were all unprepared for treatments becoming increasingly effective […] I think we just weren’t ready. (Com_context #1)
Stakeholders’ perceptions of developing an RTW intervention in primary care
Participants had a positive perception of an intervention in primary care. They believed in the solution and felt that it met patients’ needs in terms of RTW. They found the solution interesting, as it promoted the accessibility of service, continuity of care during RTW, and the involvement of various professionals. Participants explained:
[…] extremely useful, because resources are available in primary care, such as psychologists; for sure it’s the most interesting approach to improve accessibility because it’s always more difficult in a hospital setting […] (Work_context #1)
It’s interesting when here (in a hospital setting) we’re always limited to things relating to oncology […] all the same, we’re going to limit ourselves to cancer after-effects, since you need to have a framework for a given time, but if it was in primary care, I imagine they could cast a wider net. (Onco_context #2)
Findings on participants’ perceptions of facilitators and barriers are presented in various contexts in the following sections (Table 2).
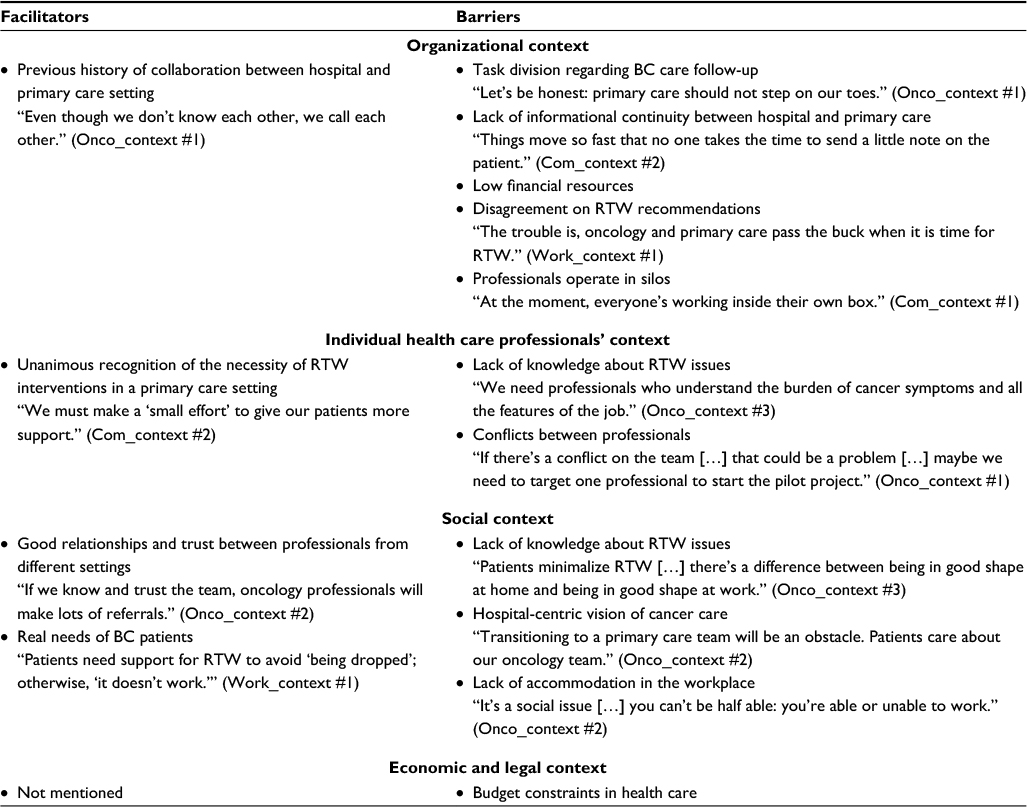 | Table 2 Perceptions of facilitators and barriers Notes: Onco_context: oncology care context; Com_context: community care context; Work_context: employeer context. Interviews were performed in French; a professional translator translated the manuscript from French to English to ensure the quality of the language and the scientific work. Abbreviations: BC, breast cancer; RTW, return-to-work. |
Factors conducive to intervention
In terms of organizational context, participants coming from primary care and oncology reported that they were able to communicate easily with colleagues from these different milieux. According to participants, the presence of this communication seemed to augur well for the development of an RTW intervention in primary care.
As for the individual health care professional context, all the participants agreed on the necessity of putting in place interventions designed to promote RTW in primary care. The proposed intervention is perceived as filling a “practice gap.”
The highest number of facilitating factors was found in the social context. Good relationships and mutual trust between oncology professionals and primary care professionals were reported as being extremely important aspects. This situation will foster the use of services developed for the intervention. It was also reported that the intervention meets a real need for the population of BC survivors. According to participants, women will be more inclined to participate in such an intervention.
Barriers to intervention
When it came to organizational context, many barriers were identified. First of all, participants explained that there was no consensus on the sharing of tasks or the adoption of recommendations for follow-up after BC treatments or on RTW. The sharing of medical activities was raised as a major issue in the context of developing a new intervention that would rally professionals from specialized care and primary care. Participants also mentioned that although there was communication between milieux, various professionals mainly operated in silos. They explained that the last notes dictated are not generally given to family physicians, which makes it hard to have any continuity in terms of information. Participants also doubted the organization’s ability to provide staff and resources for primary care RTW interventions due to the perceived lack of resources in daily practice.
In the individual health care professional context, participants pointed out that many professionals do not know enough about issues surrounding RTW after cancer. They stated that professionals consulted during the intervention should be aware of the problems and challenges related to different types of jobs, the variability of work settings (small or large company), as well as whether there was insurance. One participant also said that there was some conflict between certain members of his work team who had a lot of influence. This situation could limit the participation of key players. The suggestion was made that only one key professional should be targeted as the main contact person in a pilot project.
As for the social context, participants explained that BC survivors downplay RTW issues and do not get enough information on this aspect of surviving cancer. They also reported that BC survivors prefer specialized oncology teams, though the teams may be reluctant to consult in primary care at the end of treatments and may not see the point of dwelling on aspects related to RTW. On the employer’s side, the point was raised that one of the most complex aspects of RTW is the concept of ability to work after cancer treatments. One participant said that the survivor’s ability to resume work changes over time, which means accommodations in the workplace (eg, flextime, review of tasks) will need to continue over a longer period. Some employers’ rigid attitudes to making accommodations can limit the effects of the proposed intervention.
As for the economic and legal context, participants said only that health care budget cuts in recent years could limit the deployment of an RTW intervention in primary care. Primary care resources for the implementation of the intervention could be limited.
Discussion
The integrated knowledge translation approach is helpful in improving our understanding of the local context, existing practices, and relationships between particular stakeholders. The pilot study pinpointed barriers and facilitators to the implementation of an intervention in primary care to support RTW after BC. The results further suggest that participants believe the development of the intervention is achievable and useful. The principal findings and pathways to solutions designed to support the development and deployment of the intervention are discussed in the following paragraphs.
Although the stakeholders came from various milieux, the results of this pilot study documented converging opinions on issues with RTW after BC. Several barriers that had previously been identified in the literature were reported by participants, including early RTW, fatigue, and brain fog.11,33 Issues relating to job retention were also raised by participants (eg, RTW too soon, recurring symptoms still present, insufficient planning for job retention). These issues are important, as they reinforce the idea that RTW after BC requires long-term follow-up by a team of professionals (eg, symptom management), as well as commitment by employers.9,13,33 Employers were identified as key partners in the RTW process who need to be brought in quickly to support RTW and job retention.34 Like health care professionals, participants also explained that it was necessary to inform BC survivors about the challenges of RTW after BC. There are many studies and recommendations on this topic, making it clear that information on survival issues needs to be given out at the end of treatments to ensure quality of care and the transition to primary care.35–38 Finally, these results show the need to develop a multifaceted intervention that rallies people from a range of milieux.
The proposed RTW intervention in primary care was welcomed by the participants, who believe that this context facilitates access to more resources and a diverse range of professionals. The results also suggest that major levers are present in the organizational, professional, and social contexts. For the organizational context, a history of communication between the oncology and primary care teams was perceived as a determining factor. This type of communication seems to be conducive to the deployment of a new intervention. As for the individual health care professional context, the perception that the proposed intervention fills a “practice gap” is an essential element. In terms of social context, participants believe that cancer survivors are predisposed to appreciate an RTW intervention in primary care. The results of our study thus provide confirmation that the proposed intervention is a useful way of compensating for issues experienced by various stakeholders from various contexts.
This pilot study enabled us to identify barriers, primarily regarding the organizational context. Although the various stakeholders were aware of problems with RTW after BC, existing practices and procedures did not appear to have been modified to meet the needs of BC survivors. Our results seem to suggest that care and services were coordinated “by referral.” Participants frequently mentioned that practice took place “in silos” and that communication among various players regarding exchanging information on survivors’ health was poor. Problems with communication between oncology and primary care teams, as well as the absence of clear directives on survivor care, can limit coordination of care,35,39–41 transition of routine follow-up care,24,42 feeling able to trust family physicians to play a more active role with this clientele,43 and survivors having confidence in their primary care team to follow-up posttreatment.1,44,45 Also, these difficulties about coordinating care between primary care and specialized care seem recurrent in the general practice.46 In addition, in terms of social context, participants perceived survivors’ difficulty with obtaining ongoing accommodations in the workplace. According to a recent Canadian study,47 this clientele requires tailor-made accommodations that take into account job demands as well as support available in the workplace and work context.47 It is worth noting that employers have no legal obligations to put in place ongoing accommodations for people who are deemed fit for work,48,49 as is the case for BC survivors. This aspect is extremely important, as it reinforces the idea of intervening at an early stage and providing better information for various professionals on the employer’s legal obligations. There have been reports of survivors minimizing problems related to RTW. This is why it is recommended that survivors, professionals, and employers be informed about this subject.50 In light of these results, recommendations are proposed for different contexts in order to overcome the presence of barriers and focus on identified levers (Table 3).
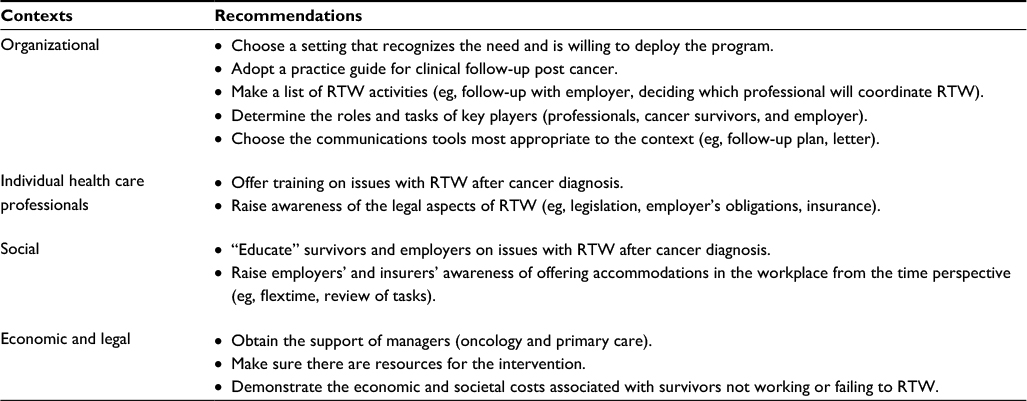 | Table 3 Recommendations for facilitating the development and deployment of the intervention Abbreviation: RTW, return-to-work. |
Strengths and limitations
One strength of this study is the use of varied perspectives from stakeholders from the oncology, community and employer contexts. Thanks to this strategy, favorable factors and potential barriers to developing an intervention related to RTW in primary care have been identified. The application of an integrated knowledge translation approach to support the development and implementation of a complex intervention has proven to be a wise strategy, as it helps to identify the opinions of various stakeholders involved in the RTW journey of women treated for BC. Since this is an exploratory stage in a pilot study, the number of interviews was limited. It should be noted that there are scant data to explain the employer’s context. For this project, the stakeholder who was recruited was a workplace health and safety officer working in a hospital, with a background in nursing science. Perhaps that choice should be reconsidered in a future study to include other workplace settings. Also, to reinforce the transferability of the results, more interviews are needed. We suggest conducting focus groups with representatives from each contexts (oncology, employers, and community). Despite the small number of participants, this pilot study provides some recommendations for a local context as a part of an intervention development strategy. A further note: our results document the specific context of stakeholders in a specific geographical area – the province of Quebec, Canada. Considering these limitations, the results should be interpreted with caution.
Conclusion
The results of this pilot study improve our understanding of the local context in preparing for the development of a complex intervention designed to support RTW after BC. The problem (eg, difficulty with RTW) and the solutions (eg, intervention in primary care) were pinpointed, and recommendations for breaking down the barriers were identified (eg, training, communication tools). In addition, the results focus on the usefulness of an intervention supporting the RTW process as a component of primary care treatment for survivors. Ultimately, the intervention to be developed would need to focus on both creating the conditions to change practices in favor of the intervention and making the intervention an integral part of professional practices and the organization of existing services. Finally, the application of an integrated knowledge translation approach has proven to be useful in formulating pragmatic recommendations that will be applicable to the Canadian clinical context.
Acknowledgment
This study was supported by postdoctoral bursaries from the Fonds de Recherche du Québec- Santé (FRQ-S) and Quebec SPOR-SUPPORT Unit as well as the Quebec Nursing Intervention Network awarded to K Bilodeau.
Disclosure
The authors report no conflicts of interest in this work.
References
Mayer DK, Nasso SF, Earp JA. Defining cancer survivors, their needs, and perspectives on survivorship health care in the USA. Lancet Oncol. 2017;18(1):e11–e18. | ||
DeSantis CE, Lin CC, Mariotto AB, et al. Cancer treatment and survivorship statistics, 2014. Cancer J Clin. 2014;64(4):252–271. | ||
Knobf MT. The transition experience to breast cancer survivorship. Semin Oncol Nurs. 2015;31:178–182. | ||
Schultz IZ, Gatchel RJ. Handbook of Return to Work: From Research to Practice. Vol. 1. New York: Springer; 2015. | ||
Steenstra I, Lee H, de Vroome E, Busse J, Hogg-Johnson S. Comparing current definitions of return to work: a measurement approach. J Occup Rehabil. 2012;22(3):394–400. | ||
Morrison TL, Thomas RL. Survivors’ experiences of return to work following cancer: a photovoice study: expériences vécues par des survivantes à un cancer face à leur retour au travail: Une étude photovoice. Can J Occup Ther. 2014;81(3):163–172. | ||
Nachreiner N, Dagher R, McGovern P, Baker B, Alexander B, Gerberich S. Successful return to work for cancer survivors. AAOHN J. 2007;55:290–295. | ||
Rasmussen DM, Elverdam B. The meaning of work and working life after cancer: an interview study. Psycho-Oncology. 2008;17(12):1232–1238. | ||
Wells M, Williams B, Firnigl D, et al. Supporting ‘work-related goals’ rather than ‘return to work’after cancer? A systematic review and meta-synthesis of 25 qualitative studies. Psycho-Oncology. 2013;22(6):1208–1219. | ||
Duijts SFA, van Egmond MP, Spelten E, van Muijen P, Anema JR, van der Beek AJ. Physical and psychosocial problems in cancer survivors beyond return to work: a systematic review. Psycho-Oncology. 2014;23(5):481–492. | ||
Dorland H, Abma F, Roelen C, Smink J, Ranchor A, Bültmann U. Factors influencing work functioning after cancer diagnosis: a focus group study with cancer survivors and occupational health professionals. Support Care Cancer. 2016;24(1):261–266. | ||
Tiedtke C, Dierckx de Casterlé B, Donceel P, de Rijk A. Workplace support after breast cancer treatment: recognition of vulnerability. Disabil Rehabil. 2015;37(19):1770–1776. | ||
Bilodeau K, Tremblay D, Durand MJ. Exploration of return-to-work interventions for breast cancer patients: a scoping review. Support Care Cancer. 2017;25(6):1993–2007. | ||
Stergiou-Kita M, Grigorovich A, Tseung V, et al. Qualitative meta-synthesis of survivors’ work experiences and the development of strategies to facilitate return to work. J Cancer Survivor. 2014;8(4):1–14. | ||
Wells M, Amir Z, Cox T, et al. Time to act: the challenges of working during and after cancer, initiatives in research and practice. Eur J Oncol Nurs. 2014;18(1):1–2. | ||
Sun Y, Shigaki CL, Armer JM. Return to work among breast cancer survivors: a literature review. Support Care Cancer. 2017;25(3):709–718. | ||
Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M; Medical Research Council Guidance. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ. 2008;337:a1655. | ||
Denis JL, Hébert Y, Langley A, Lozeau D, Trottier LH. Explaining diffusion patterns for complex health care innovations. Health Care Manage Rev. 2002;27(3):60–73. | ||
Moore GF, Audrey S, Barker M, et al. Process evaluation of complex interventions: Medical Research Council Guidance. BMJ. 2015; 350:1–7. | ||
Pfadenhauer LM, Gerhardus A, Mozygemba K, et al. Making sense of complexity in context and implementation: the Context and Implementation of Complex Interventions (CICI) framework. Implement Sci. 2017;12(1):21. | ||
May CR, Johnson M, Finch T. Implementation, context and complexity. Implement Sci. 2016;11(1):141. | ||
Forsythe LP, Parry C, Alfano CM, et al. Use of survivorship care plans in the United States: associations with survivorship care. J Natl Cancer Inst. 2013;105(20):1579–1587. | ||
Salz T, McCabe MS, Onstad EE, et al. Survivorship care plans: is there buy-in from community oncology providers? Cancer. 2014;120(5):722–730. | ||
O’Malley D, Hudson SV, Nekhlyudov L, et al. Learning the landscape: implementation challenges of primary care innovators around cancer survivorship care. J Cancer Survivor. 2017;11(1):13–23. | ||
Hébert J, Fillion L. Development and validation of an individualized survivorship care plan (ISCP) for women with endometrial cancer during the transition of the end of active treatment to the cancer survivorship. Can Oncol Nurs J/Revue canadienne de soins infirmiers en oncologie. 2017;27(1):33–42. | ||
Straus S, Tetroe J, Graham ID. Knowledge Translation in Health Care: Moving from Evidence to Practice. Chichester: John Wiley & Sons; 2013. | ||
Légaré F, Zhang P. Barriers and facilitators. In: Straus S, Tetroe J, Graham ID, editors. Knowledge Translation in Health Care: Moving from Evidence to Practice. 2nd ed. West Sussex: Wiley Blackwell; 2013:121–136. | ||
Grol R, Wensing M. Effective implementation of change in healthcare: a systematic approach. In: Grol R, Wensing M, Eccles M, Davis D, editors. Improving Patient Care: The Implementation of Change in Health Care. Chichester: Wiley Blackwell; 2013:53–54. | ||
Graham ID, Logan J, Harrison MB, et al. Lost in knowledge translation: time for a map? J Contin Educ Health Prof. 2006;26(1):13–24. | ||
Guest G, Namey EE, Mitchell ML. Collecting Qualitative Data: A Field Manual for Applied Research. Thousand Oaks, CA: Sage; 2013. | ||
Miles MB, Saldaña J, Huberman AM. Qualitative Data Analysis: A Methods Sourcebook. 3rd ed. Thousand Oaks, CA: SAGE Publications, Inc; 2014. | ||
Saldaña J. The Coding Manual for Qualitative Researchers. 2nd ed. Thousand Oaks, CA: Sage; 2016. | ||
Stergiou-Kita M, Pritlove C, Holness DL, et al. Am I ready to return to work? Assisting cancer survivors to determine work readiness. J Cancer Survivor. 2016;10(4):1–12. | ||
Schultz IZ, Gatchel RJ. Handbook of Return to Work: From Research to Practice. New York: Springer; 2016. | ||
Jefford M, Kinnane N, Howell P, et al. Implementing novel models of posttreatment care for cancer survivors: enablers, challenges and recommendations. Asia-Pacific J Clin Oncol. 2015;11(4):319–327. | ||
Hewitt M, Ganz PA. From Cancer Patient to Cancer Survivor – Lost in Transition: An American Society of Clinical Oncology and Institute of Medicine Symposium. Washingtion, DC: The National Academies Press; 2005. | ||
McCabe MS, Bhatia S, Oeffinger KC, et al. American Society of Clinical Oncology statement: achieving high-quality cancer survivorship care. J Clin Oncol. 2013;31(5):631–640. | ||
Canadian Partnership Against Cancer. Return to Work Concerns Faced by People Dealing with Cancer and Caregivers: Literature Review and Consultation. Toronto: Canadian Partnership against Cancer; 2012. | ||
Easley J, Miedema B, Carroll JC, et al. Coordination of cancer care between family physicians and cancer specialists Importance of communication. Can Family Phys. 2016;62(10):e608–e615. | ||
Tremblay D, Latreille J, Bilodeau K, et al. Improving the transition from oncology to primary care teams: a case for shared leadership. J Oncol Practice. 2016;12(11):1012–1019. | ||
Easley J, Miedema B, O’Brien M, et al. The role of family physicians in cancer care: perspectives of primary and specialty care providers. Curr Oncol. 2017;24(2):75–80. | ||
Kendell C, Decker K, Groome P, et al. Use of physician services during the survivorship phase: a multi-province study of women diagnosed with breast cancer. Curr Oncol. 2017;24(2):81–89. | ||
Lawrence RA, McLoone JK, Wakefield CE, Cohn RJ. Primary care physicians’ perspectives of their role in cancer care: a systematic review. J Gen Intern Med. 2016;31(10):1–15. | ||
Hudson SV, Miller SM, Hemler J, et al. Adult cancer survivors discuss follow-up in primary care: ‘not what I want, but maybe what I need.’ Ann Family Med. 2012;10(5):418–427. | ||
Franco B, Dharmakulaseelan L, McAndrew A, Bae S, Cheung M, Singh S. The experiences of cancer survivors while transitioning from tertiary to primary care. Curr Oncol. 2016;23(6):378. | ||
Kim B, Lucatorto MA, Hawthorne K, et al. Care coordination between specialty care and primary care: a focus group study of provider perspectives on strong practices and improvement opportunities. J Multidiscip Healthc. 2015;8:47. | ||
Stergiou-Kita M, Pritlove C, van Eerd D, et al. The provision of workplace accommodations following cancer: survivor, provider, and employer perspectives. J Cancer Survivor. 2016;10(3):489–504. | ||
Commission des normes, de l’équité, de la santé et de la sécurité du travail. Act respecting labour standards, its regulations and the National Holiday Act 2017. Available at: https://www.cnt.gouv.qc.ca/en/interpretation-guide/part-i/act-respecting-labour-standards/definitions-sect-1/1/index.html. Accessed January 22, 2018. | ||
Canadian Human Rights Commission. A Guide for Managing the Return to Work. Montreal: Minister of Public Works and Government Services; 2007. | ||
Moskowitz MC, Todd BL, Chen R, Feuerstein M. Function and friction at work: a multidimensional analysis of work outcomes in cancer survivors. J Cancer Survivor. 2014;8(2):173–182. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.