Back to Journals » International Journal of Women's Health » Volume 18
Exploration of Acupoint Compatibility Patterns in Acupuncture Treatment for Infertility Based on Data Mining
Authors Liu J, Zhang J, Li H ![]() , Yuan Z
, Yuan Z ![]() , Liu J, Jia W, Sun Y, Wang X
, Liu J, Jia W, Sun Y, Wang X ![]() , She Y
, She Y
Received 7 December 2025
Accepted for publication 3 March 2026
Published 12 March 2026 Volume 2026:18 578082
DOI https://doi.org/10.2147/IJWH.S578082
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Jun Liu,1,2,* Juncha Zhang,1,2,* Haiping Li,1,* Zichun Yuan,3 Jiaxin Liu,1 Weiwei Jia,1 Yi Sun,1 Xuesong Wang,4 Yanfen She1,2
1College of Acupuncture-Moxibustion and Massage, Hebei University of Chinese Medicine, Shijiazhuang, Hebei, People’s Republic of China; 2Hebei International Joint Research Center for Dominant Diseases in Chinese Medicine and Acupuncture, Hebei University of Chinese Medicine, Shijiazhuang, Hebei, People’s Republic of China; 3Department of Graduate School, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 4Center for Rehabilitation Medicine, Rehabilitation & Sports Medicine Research Institute of Zhejiang Province, Zhejiang Provincial People’s Hospital (Affiliated People’s Hospital), Hangzhou Medical College, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xuesong Wang, Center for Rehabilitation Medicine, Rehabilitation & Sports Medicine Research Institute of Zhejiang Province, Zhejiang Provincial People’s Hospital (Affiliated People’s Hospital), Hangzhou Medical College, No. 158 Shangtang Road, Gongshu District, Hangzhou, Zhejiang, 310000, People’s Republic of China, Tel +8618271838070, Email [email protected] Yanfen She, College of Acupuncture-Moxibustion and Massage,Hebei University of Chinese Medicine, No. 3 Xingyuan Road, Luquan District, Shijiazhuang, Hebei, 050200, People’s Republic of China, Tel +8615833955088, Email [email protected]
Objective: This study aimed to explore the compatibility rules of acupoint selection in acupuncture treatment for infertility using data mining techniques.
Methods: Randomized controlled trials (RCTs)on acupuncture treatment for infertility were retrieved from the China National Knowledge Infrastructure, Wanfang Data Knowledge Service Platform, VIP Chinese Journal Service Platform, Chinese Biomedical Literature Database, PubMed, Embase, Web of Science, and Cochrane Library up to September 22, 2024. The frequency of acupoint use, meridian attribution, selection of specific points, and acupoint association rules in the treatment of polycystic ovary syndrome-related infertility, diminished ovarian reserve related infertility, and unexplained infertility were analyzed using R language. Cytoscape was employed to visualize acupoint associations and disease-acupoint co-occurrence networks.
Results: A total of 220 prescriptions for infertility were included, covering 92 acupoints with an overall frequency of 3,653 uses. The top three frequently used acupoints were Guanyuan (CV4), Sanyinjiao (SP6), Zigong (EX-CA1). The most frequently involved meridians were the Conception Vessel, the Spleen Meridian of Foot-Taiyin, and the Stomach Meridian of Foot-Yangming. The specific acupoint usage frequency from high to low was Front Mu points, Five-shu points, and Yuan-primary points. Network analysis indicated that the core acupoint group consisted of CV4, SP6, Zusanli (ST36), EX-CA1, Qihai (CV6), Baihui (GV20), Xuehai (SP10), Shenshu (BL23), Ganshu (BL18), Guilai (ST29), Zhongji (CV3), Taichong (LR3), Taixi (KI3), Zhongwan (CV12), Tianshu (ST25). The overall therapeutic principle focused on regulating the Flush Vessel and Conception Vessel and harmonizing qi and blood.
Conclusion: This study provides valuable insights for the clinical selection of acupoint combinations in the acupuncture treatment of infertility, offering directions for optimizing acupoint strategies in clinical practice.
Keywords: infertility, acupuncture, acupoints, association rules, data mining
Introduction
Infertility is defined as the inability to conceive after 12 months or more of regular, unprotected sexual intercourse, or the inability to achieve pregnancy again after a previous pregnancy despite more than 12 months of unprotected intercourse.1,2 With the rapid development of modern society, environmental factors and work-related stress have contributed to a rising prevalence of infertility.3 In 2002, the World Health Organization (WHO) estimated that approximately 80 million people worldwide suffered from infertility, and nearly 25% of couples of reproductive age experience infertility problems,4 with female factors accounting for about 40% of cases.5 The prevalence of infertility varies around the world, 21–22% of Iranian women suffer from primary infertility,6 11.5–15.7% in Canada,7 12.5% in the United Kingdom,8 and a relatively high prevalence of 25% among women of reproductive age in China.9 The WHO has defined infertility as a reproductive system disorder and recognized it as a global public health issue.10,11 Causes of infertility include ovarian dysfunction, tubal abnormalities, and endometrial disorders,12 which can result in enormous psychological, physical, and financial burdens, leading in some cases to anxiety and depression.13
The main causes of female infertility include ovulatory disorders, pelvic factors and some unexplained infertility. Conventional therapy for infertility involves drug treatment (clomiphene and gonadotropin-releasing hormone analogs) and assisted reproductive techniques (such as in vitro fertilization, hormonal stimulation, and intracytoplasmic sperm injection).14 Conventional treatments typically involve medications, such as clomiphene and gonadotropin-releasing hormone analogs. However, these treatments are often expensive, imposing financial burdens on patients,15 and they carry risks such as ovarian hyperstimulation syndrome, impaired endometrial receptivity, bleeding, infection, and diminished ovarian reserve, increasing the likelihood of adverse pregnancy outcomes.16
Acupuncture, a complementary and alternative therapy, has been used in the treatment of infertility since ancient times. As early as the Han dynasty, the classic Zhenjiu Jiayi Jing (Systematic Classic of Acupuncture and Moxibustion) by Huangfu Mi recorded acupuncture prescriptions for infertility, stating: “For women without children and with lower abdominal pain, needle Qichong point.” Modern studies indicate that approximately 29% of patients with infertility have used complementary and alternative therapies, and 22% have specifically tried acupuncture.17 In 1999, researchers first demonstrated that acupuncture significantly improves fertility, pregnancy rates, and live birth rates.18 Subsequently, a substantial body of evidence has confirmed the efficacy of acupuncture in improving pregnancy outcomes, increasing live birth rates, and reducing stress, anxiety, and depression levels in infertile patients.19–21 Acupuncture and moxibustion are widely regarded as effective adjunctive therapies for infertility. However, significant inconsistency persists in the literature regarding their efficacy. A study involving over 800 infertile women in Australia and New Zealand reported no significant clinical difference between active acupuncture and sham acupuncture.22 The notable variation in reported success rates across different studies may be attributable to differences in acupoint selection, treatment duration, and the design of sham acupuncture controls. Among these factors, acupoint compatibility is considered one of the most critical determinants of therapeutic efficacy. Optimizing acupoint selection has therefore long been a focal point and challenge in clinical acupuncture practice. Currently, acupoint selection is mainly guided by traditional Chinese medicine (TCM) theory and clinical experience, but considerable differences in acupoint choice exist across studies. For example, a data mining study on moxibustion for infertility found that Guanyuan (CV4), Shenque (CV8), and Zigong (EX-CA1) were among the most frequently used points.23 A bibliometric analysis showed that 73.5% of acupuncture studies for infertility followed fixed-point selection protocols, yet the specific basis for selecting these combinations remains unclear.24 Although numerous acupoints are employed in infertility treatment, few studies have systematically explored which combinations are most commonly used or most effective, limiting the standardization and broad application of acupuncture for infertility. To address this gap, the present study systematically screened RCTs on acupuncture treatment for infertility from eight Chinese and international databases to analyze patterns of acupoint usage and compatibility, with the aim of providing evidence-based guidance for clinical practice.
Materials and Methods
Literature Search
The search databases were China National Knowledge Infrastructure, Wan fang Data, Chinese Scientific Journal Database, China Biology Medicine, PubMed, Embase, Web of Science, and Cochrane Library. The search covered all records up to September 22, 2024. The search was conducted using a combination of subject terms and free words. The keywords included acupuncture, moxibustion, electroacupuncture, warm-needle moxibustion, scalp acupuncture, fire needle, infertility, ovulatory dysfunction infertility, tubal infertility, polycystic ovary syndrome infertility, hyperprolactinemia infertility, luteal phase defect infertility, premature ovarian insufficiency infertility, premature ovarian failure infertility, diminished ovarian reserve infertility, poor ovarian response infertility, anovulatory abnormal uterine bleeding infertility, luteinized unruptured follicle syndrome infertility, and endometriosis infertility. The language was limited to articles published in Chinese or English. The detailed search strategy is provided in Appendix 1.
Inclusion Criteria
(1) Study type: Clinical randomized controlled trials (RCTs) explicitly for acupuncture or electroacupuncture in the treatment of infertility; (2) Study population: Patients diagnosed with infertility, regardless of age or disease duration; (3) Intervention in the experimental group: Acupuncture or electroacupuncture alone, or in combination with other therapies such as Chinese herbal medicine, auricular point pressing, moxibustion, Western medications, or embryo transplantation techniques; (4) Clear documentation of the acupuncture prescription and acupoint combinations; (5) Outcome indicators demonstrating the efficacy of acupuncture or electroacupuncture alone or in combination, including but not limited to conception rate, pregnancy rate, and live birth rate.
Exclusion Criteria
- Only the earliest published article was retained in cases of duplicate publications;
- Studies utilizing personal experience points, Dong’s extraordinary points, or other points not belonging to the fourteen meridians or extraordinary points were excluded;
- Studies in which both groups (or more than two groups) received acupuncture or electroacupuncture interventions.
Literature Screening
Firstly, the retrieved literature was imported into Endnote to merge the data, and after merging and de-emphasizing the included literature to read the title and abstract content for initial screening, remove the type of study, the research object does not meet the literature, and then by reading the full text content for fine screening, and finally imported into Excel 2019 software to organize the details, including the author, title, periodicals, name of the disease, interventions, acupoints prescription, outcome indicators, and clinical efficacy. The above screening process was carried out by two researchers individually, and when there was inconsistency, a third researcher made the decision to screen and merge the two datasets.
Data Entry and Standardization
According to the World Health Organization’s Standard “Acupuncture Point Location in the Western Pacific Region”,25 the ‘Chinese National Standards for Acupoint Nomenclature and Location (GB/T 12346–2021),26 the “Nomenclature and location of extra points in common use” (GB/T 40997–2021),27 and the International Classification of Diseases 11th Revision,28 two researchers standardized the disease and acupoint names in the Excel data. Any discrepancies were resolved by a third researcher.
Quality Assessment
In order to ensure the reliability and accuracy of the study results, the literature quality was scored using a modified version of the Jadad scoring scale,29 which mainly contains four entries, namely, random sequence generation, randomization concealment, blinding, and withdrawal and exit, with 0–3 being classified as a low-quality clinical trial, and 4–7 being classified as a high-quality clinical trial. Furthermore, based on the Peking University Core Journal Catalogue (2023 Edition), the Chinese Science and Technology Core Journal Catalogue (2024 Edition, Social Sciences Volume), the Directory of Journals Selected for the Chinese Science and Technology Journal Excellence Action Plan, and the Chinese Science Citation Database Source Journal List (2023–2024), the included studies were assigned values according to the type of journal in which they were published. General journals were assigned 1 point, core science and technology journals were assigned 2 points, journals listed in the Chinese Science Citation Database (CSCD) and Chinese core journals were assigned 3 points, and SCI journals were assigned 4 points. The acupoint prescriptions were then weighted according to the journal-type scores.
Statistical Analysis
First, R language was used to analyze the frequency of acupoint use, meridian distribution, and use of specific acupoints. Then, the Apriori algorithm in IBM SPSS Modeler 18.0 was employed to identify acupoint association rules, with minimum support set at 20% and minimum confidence at 90%. Effective association rules extracted from the data were visualized using Cytoscape 3.9.0 to illustrate the relationships between acupoints and their roles in infertility treatment.
Results
Literature Search results
A total of 4,395 relevant articles were identified through the initial search. After deduplication, 2,723 articles remained. Following title and abstract screening, 1,063 articles were selected for full-text review. After excluding studies with ineligible study types or interventions, 596 articles were retained. Articles with a Jadad score above 3 were further selected, resulting in 283 high-quality articles. The detailed screening process is illustrated in Figure 1.The included types of infertility encompassed 13 categories: polycystic ovary syndrome (PCOS) related infertility, diminished ovarian reserve (DOR) related infertility, luteinized unruptured follicle syndrome (LUFS) related infertility, tubal obstruction (TO) related infertility, thin endometrium (TE) related infertility, unexplained infertility (UI), chronic adnexitis (CA) related infertility, poor follicular development (PFD), immune (IM) related infertility, luteal phase defect (LPD) related infertility, endometriosis (EMs) related infertility, and idiopathic hyperprolactinemia (IH) related infertility (Figure 2). Among these, the top three most frequently included types were PCOS infertility, DOR infertility, and UI, accounting for a total of 220 articles (72.85%). Therefore, the acupuncture prescriptions extracted from these three categories were used for subsequent analysis.
 |
Figure 1 Flow chart for literature screening of randomized controlled trials of acupuncture for various types of infertility. |
 |
Figure 2 Number and distribution of randomized controlled trials of acupuncture in the treatment of various types of infertility. Abbreviations: zPCOS, polycystic ovary syndrome related infertility; DOR, diminished ovarian reserve related infertility; LUFS, luteinized unruptured follicle syndrome infertility; TO, tubal obstruction related infertility; TE, thin endometrium related infertility; UI, unexplained infertility; CA, chronic adnexitis related infertility; PFD, poor follicular development related infertility; IM, immune related infertility; LPD, luteal phase defect related infertility; EMs, endometriosis related infertility; IH, idiopathic hyperprolactinemia related infertility. |
Analysis of Acupoint Usage Patterns in Acupuncture for Infertility
Frequency Analysis of the Use of Acupuncture Points
The acupoint prescriptions were extracted from the three aforementioned infertility-related studies, and weighted according to the tier of the journals in which they were published. Ultimately, a total of 220 prescriptions involving 92 acupoints were included. The cumulative frequency of acupoint usage was 3,653 times. Among these, the top 10 most frequently used acupoints for acupuncture treatment of infertility were Guanyuan (CV4), Sanyinjiao (SP6), Zigong (EX-CA1), Zusanli (ST36), Qihai (CV6), Zhongji (CV3), Taichong (LR3), Shenshu (BL23), Taixi (KI3), and Baihui (GV20), with a combined usage frequency of 2,182 times (Table 1).
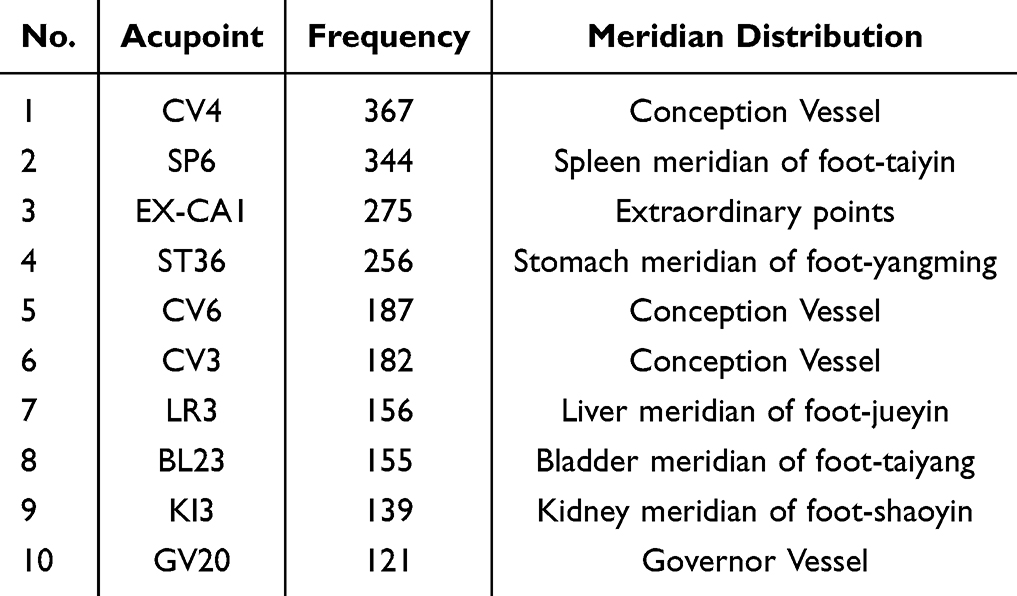 |
Table 1 Frequent Use of Acupuncture Points for the Treatment of Infertility |
Analysis of Meridian Affiliation of Acupoints
Through the analysis of meridian affiliation of the acupoints in the 220 prescriptions, it was found that the acupoints used in acupuncture treatment for infertility are widely distributed across the twelve regular meridians, the conception vessel and governor vessel, and extraordinary points. The meridians with the highest frequency of acupoint affiliation are the conception vessel (8 acupoints, with a usage frequency of 23.71%), the spleen meridian of foot-taiyin (8 acupoints, with a usage frequency of 15.16%), and the stomach meridian of foot-yangming (13 acupoints, with a usage frequency of 14.54%) (Table 2). Acupuncture treatment for infertility commonly involves the selection of acupoints from the conception vessel, the spleen meridian of foot-taiyin, and the stomach meridian of foot-yangming.
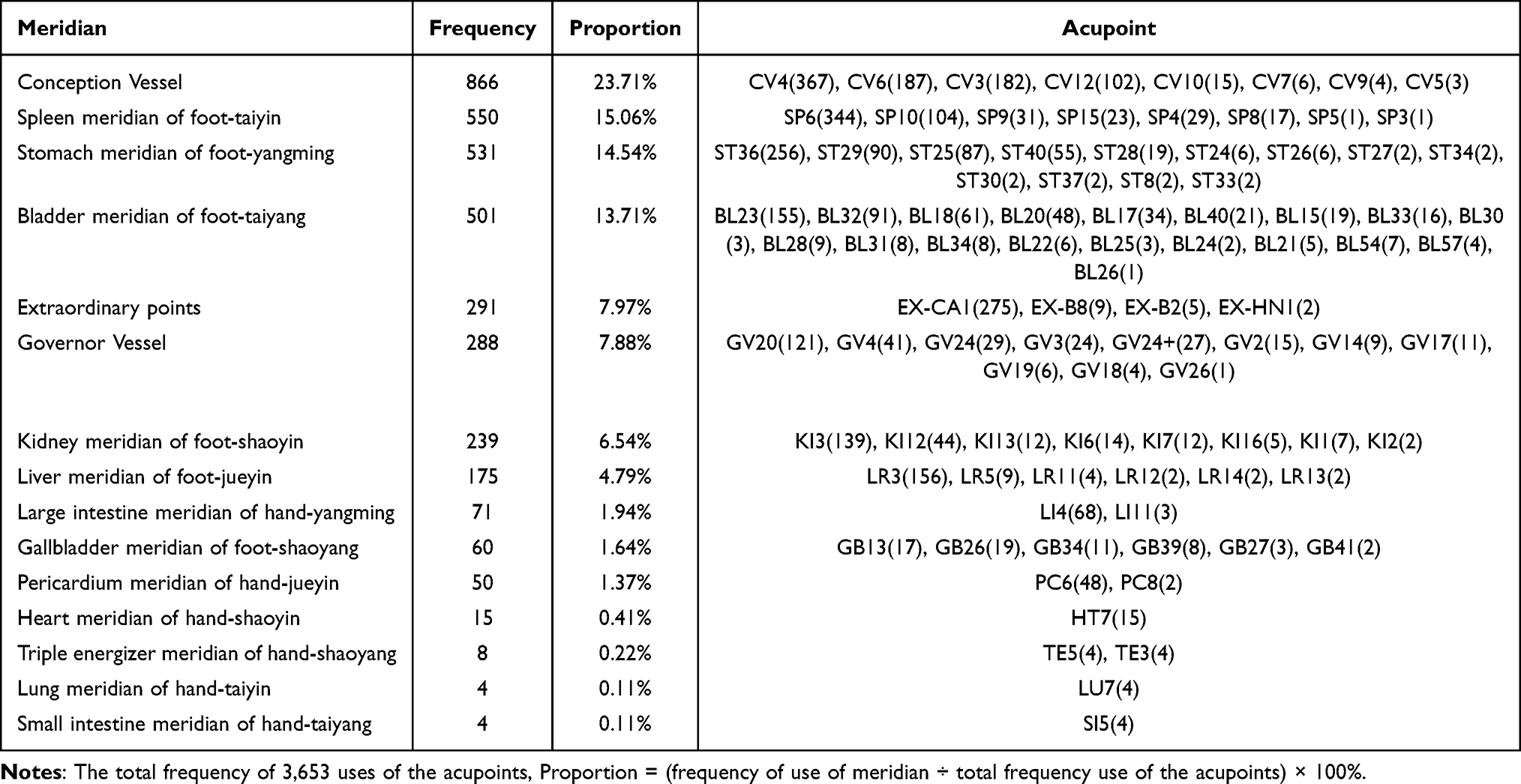 |
Table 2 Frequent Use of Meridian Application for the Treatment of Infertility |
Specific Point Analysis
The utilization of specific acupoints in the 220 prescriptions was summarized. In the acupuncture treatment of infertility, specific acupoints such as the Eight confluent points, Five Shu Points, Yuan-primary points, and Back Shu points were employed, with a total frequency of 2,805 times. Among these, acupoints like Zusanli (ST36), Neiguan (PC6), and Zhongwan (CV12) belong to multiple categories of specific acupoints. After excluding duplicate acupoints, a total of 44 distinct acupoints remained, with a frequency of 2,004 times. The usage frequency of Front Mu points was 26.56%, involving 7 acupoints such as CV4, CV3, and CV12; the usage frequency of Five Shu points was 23.78%, involving 17 acupoints such as ST36, LR3, and KI3; the usage frequency of Source Points was 13.51%, involving 5 acupoints such as LR3, KI3, and Hegu (LI4) (Table 3). In order to further analyze the attribution of high-frequency specific points, three types of high-frequency specific points for clinical treatment of infertility (Front-Mu points, Five Shu points, and Yuan-primary points) were selected for analysis (Figure 3).
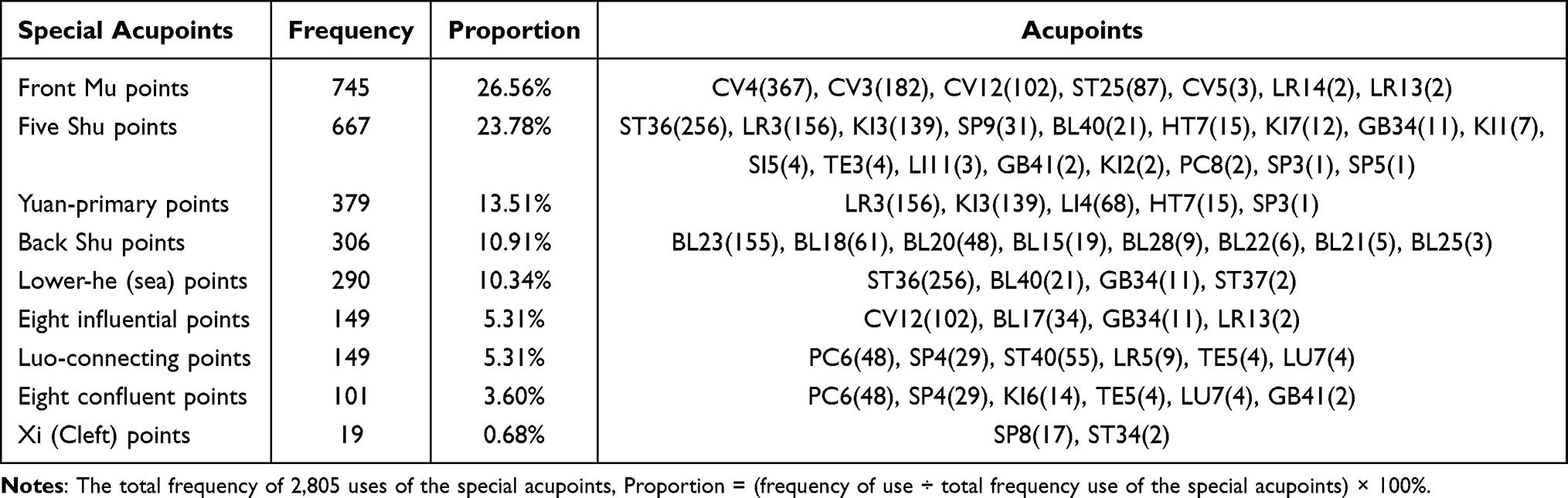 |
Table 3 Frequent Use of Special Acupoints Application for the Treatment of Infertility |
 |
Figure 3 Relationship between high-frequency specific acupoints and meridians in randomized controlled trials of acupuncture treatment for infertility. |
Analysis of Association Rules Between Acupoints and Infertility
Acupoint association rules refer to the analysis of the compatibility relationships between acupoints through data mining methods, in order to reveal the usage patterns and combination methods of acupoints in the treatment of specific diseases. Support, confidence, and lift are three important indicators in association rule analysis, which can be used to measure the validity and significance of the rules. Support is used to measure the frequency of occurrence of acupoints in association rules. Confidence reflects the probability of two points appearing at the same time. Lift indicates the correlation between two points in an association rule, with Lift>1 and higher indicating higher positive correlation, Lift<1 and lower indicating higher negative correlation, and Lift=1 indicating no correlation.
(1) In the analysis of acupoint-acupoint association patterns, the Apriori algorithm was employed to generate permutations and combinations of the included acupoint prescriptions. The minimum support was set at 20%, the minimum confidence was set at 90%, and lift is greater than 1, with each rule comprising at least two acupoints.30 This approach identified high-confidence acupoint combinations, resulting in a total of 24 association rules (Table 4). A visual analysis of the acupoint association patterns was also conducted (Figure 4). The results indicated that the combination of SP6 and CV4 exhibited the highest confidence level. When SP6 was selected, there was a 92.09% likelihood of also selecting CV4. The co-occurrence frequency of these two acupoints was 80.45%, with a Lift value of 1.05, which is greater than 1. This indicates that the combination of SP6 and CV4 constitutes a strong and effective association rule. Additionally, other notable association rules were identified, such as the combinations of EX-CA1 and CV4, ST36 and SP6, and ST36 and CV4, all of which demonstrated high support, confidence, and Lift values.
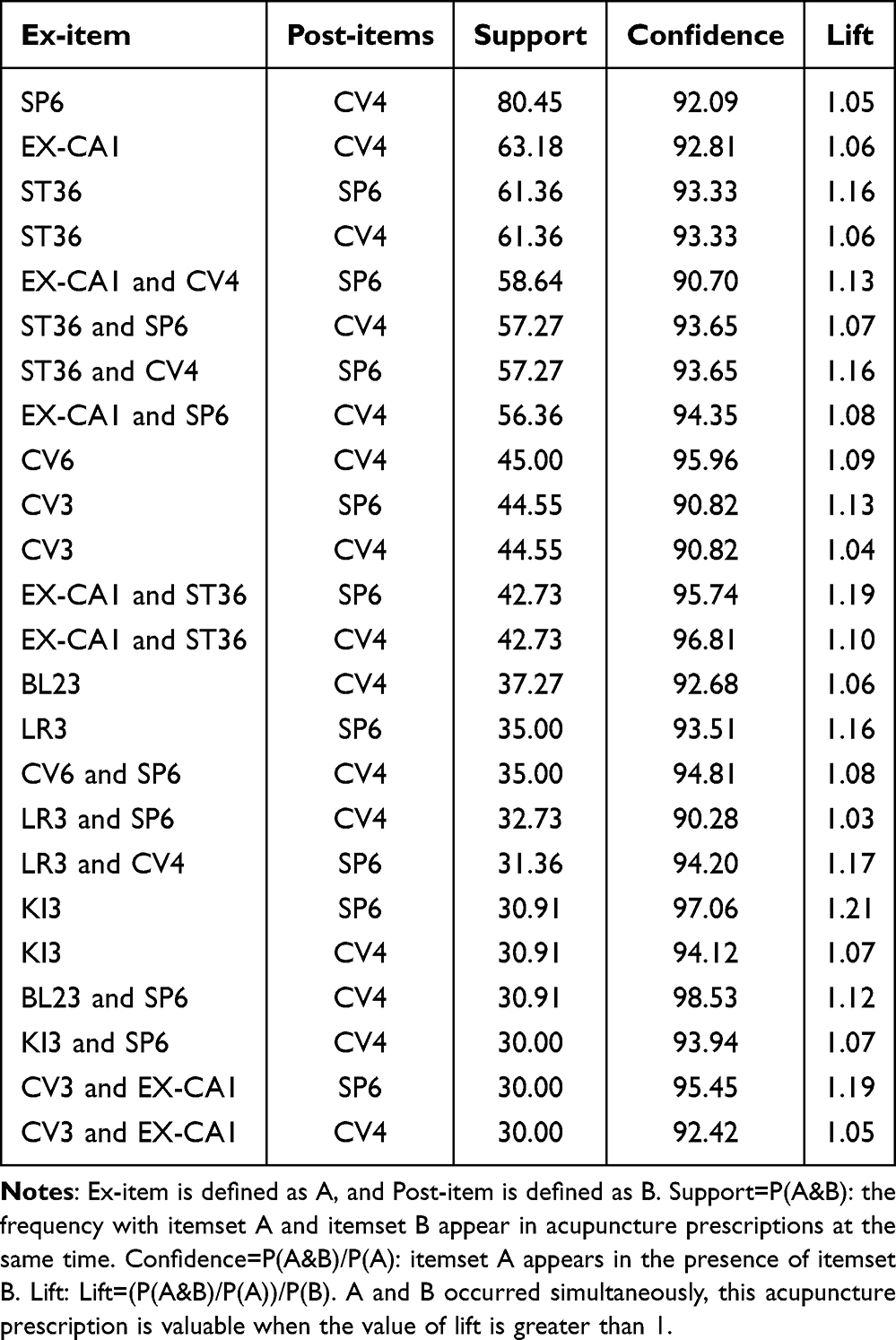 |
Table 4 Association Rules of Acupoints for Infertility Treatment |
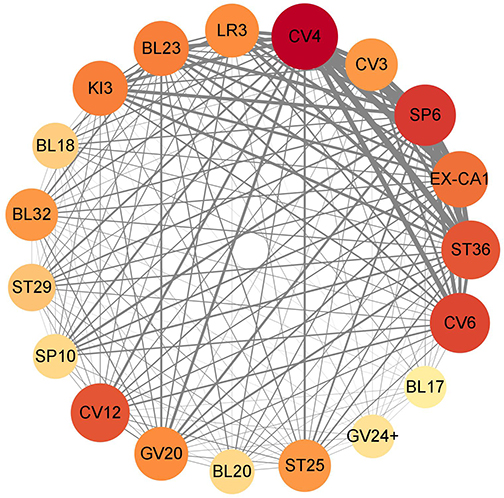 |
Figure 4 Acupuncture for infertility randomized controlled trial literature point association network. The larger the area of acupoint nodes, the higher the usage frequency; the thicker the lines representing network interaction relationships, the stronger the correlation between acupoints. |
(2) Analysis of association rules between diseases and acupoints
Acupoints with frequencies above the mean were selected to construct co-occurrence networks for the three most common infertility types: PCOS-related infertility, DOR-related infertility, and UI (Figure 5). The results indicated that CV4, SP6, ST36, and EX-CA1 are highly associated with all three types of infertility and have higher weights. CV6, GV20, Xuehai (SP10), BL23, Ganshu (BL18), Guilai (ST29), CV3, LR3, KI3, CV12, and Tianshu (ST25) are also used in the treatment of all three types of infertility but with relatively lower weights. In UI related infertility treatment, LI4, PC6, Ciliao (BL32), Pishu (BL20), and Fenglong (ST40) are frequently combined. In PCOS-related infertility, BL20, ST40, and GV4 are often used as supplementary acupoints. In OI-related infertility treatment, LI4, Dahe (KI12), and BL32 are commonly combined. In acupuncture treatment for different types of infertility, a core acupoint cluster is formed, including CV4, SP6, ST36, EX-CA1, CV6, GV20, SP10, BL23, BL18, ST29, CV3, LR3, KI3, CV12, and ST25. Subsequently, other specific acupoints are selected and combined based on the different pathophysiological mechanisms and meridian involvement of the diseases.
 |
Figure 5 Co-occurrence network of acupuncture points for common infertility treatment. The larger the area of acupoint nodes, the higher the usage frequency; the thicker the lines representing network interaction relationships, the stronger the correlation between acupoints. |
Discussion
This study included 596 infertility-related articles, among which the top three most commonly studied infertility types were PCOS-related infertility, DOR-related infertility, and UI, totaling 220 articles. The results showed that the most frequently used acupoints in acupuncture treatment for infertility were CV4, SP6, and EX-CA1, with the most frequently involved meridians being the Conception Vessel, followed by the Spleen Meridian of Foot-Taiyin and the Stomach Meridian of Foot-Yangming. Among specific acupoints, Front-Mu points have the highest usage frequency, followed by Five Shu points, Yuan-primary points, and Back Shu points. The combination of SP6 and CV4 is the most commonly used acupoint pairing in the treatment of infertility. In the core acupoint network, CV4, SP6, ST36, EX-CA1, CV6, GV20, SP10, BL23, BL18, ST29, CV3, LR3, KI3, CV12, and ST25 formed the central cluster for treating infertility.
Female infertility is a complex and refractory reproductive disorder with multiple pathogenic factors and mechanisms. Modern studies suggest that acupuncture stimulation at acupoints can regulate the neuro-endocrine-immune network, immune cells, and inflammatory mediators, exerting bidirectional regulatory effects.31 Acupuncture holds positive clinical significance and has been widely applied in infertility management.32 Research has shown that acupuncture may improve infertility outcomes through various mechanisms, including regulating the uterine microenvironment, improving endometrial receptivity, enhancing ovarian function, relieving tubal blockage, and promoting ovulation,33–35 and clinical studies have confirmed its efficacy and safety.36,37
PCOS is one of the most common endocrine disorders among women of reproductive age, affecting 5–10% of females aged 12 to 45 years and representing a leading cause of female infertility.38,39 Elevated luteinizing hormone (LH)/follicle-stimulating hormone (FSH) ratios in PCOS disrupt follicular recruitment, selection, dominance, and ovulation, leading to infertility. Acupuncture offers multi-target, multi-level comprehensive regulation, improving ovarian function, modulating the hypothalamic-pituitary-ovarian axis, correcting endocrine imbalances, enhancing endometrial receptivity, and promoting follicular rupture and ovulation.40 DOR is due to the decrease in the number and/or quality of oocytes, resulting in the lack of ovarian function and the decline in fertility. It is a significant cause of infertility. Despite substantial global efforts to control this condition, no definitive treatment has been established. However, studies have demonstrated that acupuncture or electroacupuncture can enhance ovarian blood flow, regulate the reproductive endocrine system, and improve ovarian function in women with DOR.41 Acupuncture has also been shown to achieve therapeutic effects comparable to those of estrogen in the treatment of DOR.42 In the evidence-based guidelines for UI issued by the European Society of Human Reproduction and Embryology (ESHRE) in 2023, unexplained infertility refers to couples whose partners are ≤40 years old, have regular sexual life, and the female has obviously normal ovarian function, fallopian tubes, uterus, cervix and pelvis, and the male has normal testicular function, genitourinary anatomy and ejaculation,43 ovulation induction combined with artificial insemination is the first-line treatment for UI.44 Studies have demonstrated that acupuncture can improve pregnancy success by increasing uterine blood flow, improving endometrial receptivity and reducing stress levels, and can significantly improve pregnancy rates in women with UI.45–47
The study found that CV4, SP6, and EX-CA1 were the most frequently used acupoints. The most frequently involved meridian is the conception vessel, followed by the spleen meridian of foot-taiyin and the stomach meridian of foot-yangming. CV4 is located on the conception vessel. As one of the eight extra meridians, the conception vessel originates in the uterus and is primarily responsible for regulating the functions of the uterus, hence its traditional designation as the “Sea of Yin Meridians” and its significant role in gynecological functions such as menstruation, pregnancy, and childbirth.48 In traditional Chinese medicine, spleen and stomach deficiency is often considered an important etiological factor in infertility.49 Deficiency of the spleen and stomach can lead to blood deficiency in the thoroughfare and conception vessel meridians, resulting in malnourishment of the uterine vessels and an inability to retain sperm for conception.50 SP6 belongs to the foot-taiyin spleen meridian, and the foot-taiyin spleen meridian and foot-yangming stomach meridian are dependent on each other in terms of surface and interior, elevation and conjunction, and the two directly affect the functions of the spleen and the stomach,51 therefore, acupuncture points of the foot-taiyin spleen meridian and foot-yangming stomach meridian can provide a material basis for the onset of menstruation and the cultivation of fetus gestation.52 EX-CA1 is an extraordinary point outside the regular meridians, shares similar nerve segment distributions with the uterus and ovaries, modulating the hypothalamic-pituitary-gonadal axis to improve pregnancy rates.53
Specific points, particularly Front-Mu points, Five Shu points, Yuan-primary points, and Back Shu points, are widely applied. Front-Mu points are acupoints where the qi (ie, vital energy) of the zang-fu organs (heart, liver, spleen, lung, and kidney) is infused into the chest and abdomen, and they play a role in harmonizing the zang-fu organs and regulating qi and blood For example, CV4, the Front-Mu point of the small intestine, can harmonize the thoroughfare and conception vessel and warm the uterus in the treatment of infertility,54 CV3 the Front-Mu point of the bladder, has the effects of nourishing essence, strengthening the foundation, warming the uterus, and regulating menstruation. Modern studies have shown that the CV4 and CV3 are anatomically located in the same or adjacent segment of the spinal cord as the uterus. Acupoint stimulation can inhibit the release of prostaglandin, relieve uterine smooth muscle spasm, and improve ovarian function.55 The application of specific acupoints such as Five Shu points, Yuan-primary points, and Back Shu points reflects the TCM principle of syndrome differentiation and treatment based on zang-fu organ theory. Infertility is often caused by factors such as kidney deficiency, liver depression, and phlegm-dampness, which lead to disharmony of the thoroughfare and conception vessel meridians, with the pathological locations frequently involving the liver, spleen, and kidney.56 Among the Five Shu points, except for the He(sea) point of the triple energizer meridian, the others are located below the elbows and knees, distributed in the root and fundamental parts of the body, and are used to treat related diseases of the trunk and zang-fu organs. For example, acupuncture at ST36 has the effects of strengthening the spleen and stomach and promoting the production of qi and blood.57,58 Yuan-primary points as the locations where the original qi of the zang-fu organs is infused, passes through, and resides, play a role in regulating the functions of the zang-fu organs. For example, LR3 and KI3 can soothe the liver, tonify the kidney, activate blood circulation, and regulate menstruation.59 Back-Shu points, located on the bladder meridian of foot-taiyang, are connected to the qi and blood of the five zang organs (heart, liver, spleen, lung, and kidney), six fu organs (gallbladder, stomach, large intestine, small intestine, urinary bladder, triple burner), and the twelve regular meridians. Acupuncture at BL23 can tonify the kidney and nourish essence, thereby promoting conception. In addition, in the clinical treatment of infertility, specific acupoint combinations are followed. For example, the combination of LR3 and Ligou (LR5) represents the pairing of a source point and a connecting point, with one being exterior and the other interior, which can effectively soothe the liver, relieve depression, and harmonize qi and blood. The combination of Pangguangshu (BL28), BL18, and BL20 with CV4 and CV3 forms a Shu-Mu point pairing, which can effectively harmonize the zang-fu organs, unblock the meridians, warm yang, and eliminate phlegm. This helps to ensure the normal circulation of qi and blood and the replenishment of the thoroughfare and conception vessel blood sea, thereby achieving the therapeutic effect of treating infertility.60
The combination of SP6 and CV4 is currently the most frequently used acupoint pairing in the treatment of infertility. SP6 is located on the spleen meridian of foot-taiyin and serves as the intersection point of the spleen meridian of foot-taiyin, kidney, meridian of foot-shaoyin, and liver meridian of foot-jueyin. It has the functions of nourishing qi and blood and balancing yin and yang. CV4 is located on the conception vessel and is the Front-Mu point of the small intestine, as well as the intersection point of the kidney meridian of foot-shaoyin, spleen meridian of foot-taiyin, liver meridian of foot-jueyin, and the conception vessel. It has the effects of warming and promoting the circulation of qi and blood, and tonifying the kidney and consolidating essence. When combined, these two acupoints can regulate the thoroughfare and conception vessel, promote the transformation of kidney yin and yang, and fundamentally restore the normal physiological functions of the “kidney-tiangui-thoroughfare and conception vessel-uterus” reproductive axis.61 Acupuncture at the SP6 and CV4 combination can exert therapeutic effects on infertility through multiple targets and pathways. Acupuncture at this combination can significantly reduce the pulsatility index (PI) and resistance index (RI) in patients with DOR, thereby improving ovarian function.62 It can also lower serum LH levels and the LH/FSH ratio, and improve reproductive hormone levels and ovarian development in a PCOS rat model.63 Additionally, it can promote ovulation and menstruation in PCOS patients, reduce serum androgen levels, and Improve its clinical pregnancy rate and live birth rate.64 In clinical practice, the SP6 and CV4 combination is often supplemented with other acupoints such as EX-CA1, ST36, CV6, and LR3.
The core acupoint association network related to infertility reveals that the acupoints “CV4, SP6, ST36, EX-CA1, CV6, GV20, SP10, BL23, BL18, ST29, CV3, LR3, KI3, CV12, and ST25” constitute the core acupoint cluster for acupuncture treatment of infertility. Modern research suggests that infertility is caused by the disharmony of the thoroughfare and conception vessel, and treatment should focus on the conception and governor vessels.65 This core acupoint cluster reflects the TCM therapeutic principles of regulating the thoroughfare and conception vessel, consolidating kidney essence, and supporting fetal development. Furthermore, from the perspective of TCM, acupoint selection should be based on syndrome differentiation. The occurrence of infertility is mainly closely related to the liver, spleen and kidney. Different infertility syndromes have the same high-correlation acupoint correspondence – different diseases are treated in the same way. For example, PCOS-related infertility often presents with symptoms such as menstrual irregularities, acne, obesity, and is frequently accompanied by anxiety and depression. Treatment should emphasize activating blood circulation to regulate menstruation and strengthening the spleen to resolve dampness.66,67 Additional acupoints such as BL20, ST40, and Mingmen (GV4) are often used to enhance the effects of strengthening the spleen, tonifying the kidney, and resolving dampness. DOR-related infertility is characterized by functional changes in the ovaries.68 The syndrome types are often complex, involving both deficiency and excess. Treatment should focus on balancing tonification and purgation, and acupoints such as LI4, BL32, and KI12 be used to nourish essence and blood and promote the circulation of qi and blood.69 Assisted reproduction pays more attention to tonifying the kidneys and transporting the spleen, regulating qi and activating blood, and is often paired with acupoints such as PC6, LI4, BL32, BL20, and ST40,70,71 in order to detoxify the liver and tranquilize the heart, and to better promote conception.72 In summary, acupuncture treatment for different types of infertility commonly adheres to the primary therapeutic principles of regulating the thoroughfare and conception vessel and promoting the free flow of qi and blood, supplemented by acupoints corresponding to the affected zang-fu organs and meridians to enhance therapeutic efficacy.
This study employed data mining across eight major databases, applying rigorous quality control using the Jadad scale and weighting prescriptions by journal rank, enhancing the reliability and clinical relevance of the results compared to previous data mining studies.73–75 However, limitations remain. Most included studies were from China, reflecting predominantly Asian patient samples, and many studies on acupuncture combined with ART lacked detailed etiological classification, limiting fine-grained analysis. Additionally, current clinical trials on acupuncture for infertility lack standardization and consistency.
Conclusion
This study identified CV4, SP6, EX-CA1, ST36, CV6, CV3, LR3, BL23, KI3, and GV20 as the most commonly used acupoints in acupuncture treatment for infertility. The Conception Vessel, Spleen meridian of foot-taiyin, and Stomach meridian of foot-yangming were the more frequently selected meridians compared to the others. Among specific points, Front-Mu points, Five Shu points, and Yuan-primary points were most commonly used, with SP6-CV4 identified as the most prevalent acupoint combination. These findings provide strong evidence-based support for optimizing acupoint selection in acupuncture for infertility, offering particular guidance for junior practitioners and laying the groundwork for exploring differential efficacy of acupoint combinations. While theoretically valuable, these discoveries require more in-depth validation through prospective clinical research to ultimately translate into more precise and effective clinical treatment solutions.
Availability of Supporting Data
The data supporting the findings of this study are available from the corresponding author Yanfen She ([email protected]) upon reasonable request.
Ethics Approval and Consent to Participate
Ethics approval and consent to participate are not required due to this work is carried out on published data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study funds are derived from the National Natural Science Foundation of China (No. 82474395), the Graduate Innovation Projects of Hebei University of Chinese Medicine (No. XCXZZBS2025029), the Hebei Province Yan Zhao Golden Talent Platform Key Talent Program (No.HJZD202505) and the Project of the Traditional Chinese Medicine Administration Bureau of Hebei Province (No.2025424).
Disclosure
All authors declare that they have no potential conflicts of interest for this work.
References
1. Medicine PCotASfR. Definitions of infertility and recurrent pregnancy loss: a committee opinion. Fertil Steril. 2013;99(1):63. doi:10.1016/j.fertnstert.2012.09.023
2. Zijiang C, Jiayin L, Hefeng H, Jie Q. Infertility diagnosis guidelines. Chinese J Obstet Gynecol. 2019;(08):505–15.
3. Feng J, Wu Q, Liang Y, Liang Y, Bin Q. Epidemiological characteristics of infertility, 1990–2021, and 15-year forecasts: an analysis based on the global burden of disease study 2021. Reprod Health. 2025;22(1):26. doi:10.1186/s12978-025-01966-7
4. Z D, Z Z, L R, et al. Consultation and treatment behaviour of infertile couples in China: a population-based study. Reprod Biomed Online. 2019;38(6):917–925. doi:10.1016/j.rbmo.2018.11.034
5. Koroma L, Stewart L. Infertility: evaluation and initial management. J Midwifery Womens Health. 2012;57(6):614–621. doi:10.1111/j.1542-2011.2012.00241.x
6. Kazem M, Ali A. An overview of the epidemiology of primary infertility in Iran. J Reprod Infertil. 2009;10(3):213–216.
7. Bushnik T, Cook JL, Yuzpe AA, Tough S, Collins J. Estimating the prevalence of infertility in Canada. Hum Reprod. 2012;27(3):738–746. doi:10.1093/humrep/der465
8. Datta J, Palmer MJ, Tanton C, et al. Prevalence of infertility and help seeking among 15 000 women and men. Hum Reprod. 2016;31(9):2108–2118. doi:10.1093/humrep/dew123
9. Zhou Z, Zheng D, Wu H, et al. Epidemiology of infertility in China: a population-based study. BJOG. 2018;125(4):432–441. doi:10.1111/1471-0528.14966
10. Mascarenhas MN, Flaxman SR, Boerma T, Vanderpoel S, Stevens GA, Low N. National, regional, and global trends in infertility prevalence since 1990: a systematic analysis of 277 health surveys. PLoS Med. 2012;9(12):e1001356. doi:10.1371/journal.pmed.1001356
11. Boivin J, Bunting L, Collins JA, Nygren KG. International estimates of infertility prevalence and treatment-seeking: potential need and demand for infertility medical care. Hum Reprod. 2007;22(6):1506–1512. doi:10.1093/humrep/dem046
12. Pourakbari R, Ahmadi H, Yousefi M, Aghebati-Maleki L. Cell therapy in female infertility-related diseases: emphasis on recurrent miscarriage and repeated implantation failure. Life Sci. 2020;378:118181. doi:10.1016/j.lfs.2020.118181
13. Zegers-Hochschild F, Adamson GD, de Mouzon J, et al. International Committee for Monitoring Assisted Reproductive Technology (ICMART) and the World Health Organization (WHO) revised glossary of ART terminology, 2009. Fertil Steril. 2009;92(5):1520–1524. doi:10.1016/j.fertnstert.2009.09.009
14. Lindsay TJ, Vitrikas KR. Evaluation and treatment of infertility. Am Fam Physician. 2015;91(5):308–314.
15. He M, Sun X. Research progress on assisted reproductive technology effects on pregnancy outcomes and women’s long-term health. Chinese J Reproduct Contracept. 2021;41(3):6.
16. Tan Y, Huang Z. Thinking of integrative medical diagnosis and treatment for ovulatory disorder infertility. Chinese J Integrate Trad Western Med. 2019;39(05):521–524.
17. Smith JF, Eisenberg ML, Millstein SG, et al. The use of complementary and alternative fertility treatment in couples seeking fertility care: data from a prospective cohort in the United States. Fertil Steril. 2010;93(7):2169–2174. doi:10.1016/j.fertnstert.2010.02.054
18. Stener-Victorin E, Waldenström U, Nilsson L, Wikland M, Janson PO. A prospective randomized study of electro-acupuncture versus alfentanil as anaesthesia during oocyte aspiration in in-vitro fertilization. Hum Reprod. 1999;14(10):2480–2484. doi:10.1093/humrep/14.10.2480
19. Westergaard LG, Mao Q, Krogslund M, Sandrini S, Lenz S, Grinsted J. Acupuncture on the day of embryo transfer significantly improves the reproductive outcome in infertile women: a prospective, randomized trial. Fertil Steril. 2006;85(5):1341–1346. doi:10.1016/j.fertnstert.2005.08.070
20. Pastore LM, Williams CD, Jenkins J, Patrie JT. True and sham acupuncture produced similar frequency of ovulation and improved LH to FSH ratios in women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2011;96(10):3143–3150. doi:10.1210/jc.2011-1126
21. Bovey M, Lorenc A, Robinson N. Extent of acupuncture practice for infertility in the United Kingdom: experiences and perceptions of the practitioners. Fertil Steril. 2010;94(7):2569–2573. doi:10.1016/j.fertnstert.2010.03.072
22. Xian Z, Soo LM, Smith CA, et al. Effects of acupuncture during in vitro fertilization or intracytoplasmic sperm injection: an updated systematic review and meta-analysis. Eur J Int Med. 2018;23:S1876382018306188.
23. Xiaoxue L, Jian W, Yigong F, Xiaohua Y, Bingyu P, Anqi L. Exploration of the clinical application of moxibustion in the treatment of infertility based on data mining technology. Yunnan J Trad Chin Med Mater Med. 2024;45(01):66–73.
24. Tian Z, Zhang C, Liao X, et al. Trends in acupuncture for infertility: a scoping review with bibliometric and visual analysis. Front Endocrinol. 2024;15:1351281. doi:10.3389/fendo.2024.1351281
25. World Health Organization. Regional Office for the Western P. WHO Standard Acupuncture Point Locations in the Western Pacific Region. Manila: WHO Regional Office for the Western Pacific; 2008.
26. Institute Of Acupuncture And Moxibustion. Nomenclature and Location of Meridian Points. State Aministration for Market Regulation; Strandardization administration; 2021.
27. Institute Of Acupuncture And Moxibustion. Nomenclature and Location of Extra Points in Common Use. State Aministration for Market Regulation; Strandardization administration; 2021.
28. World Health Organization. ICD-11 revision. Available from: https://icd.who.int/en.
29. Oremus M, Wolfson C, Perrault A, Demers L, Momoli F, Moride Y. Interrater reliability of the modified Jadad quality scale for systematic reviews of Alzheimer’s disease drug trials. Dement Geriatr Cogn Disord. 2001;12(3):232–236. doi:10.1159/000051263
30. Liu R, Liang L, Huang H, Zeng Z, Sun J. Rehabilitation effects of acupuncture on the diaphragmatic dysfunction in respiratory insufficiency: a systematic review and meta-analysis. Complement Ther Med. 2024;87:103105. doi:10.1016/j.ctim.2024.103105
31. Naik S, Bouladoux N, Linehan JL, et al. Commensal–dendritic-cell interaction specifies a unique protective skin immune signature. Nature. 2015;520(7545):104–108. doi:10.1038/nature14052
32. Li M, Liu Y, Wang H, Zheng S, Deng Y, Li Y. The effects of acupuncture on pregnancy outcomes of recurrent implantation failure: a systematic review and meta-analysis. Evid Based Complement Alternat Med. 2021;2021:6661235. doi:10.1155/2021/6661235
33. Zhao J, Wang L, Li Y. Electroacupuncture alleviates the inflammatory response via effects on M1 and M2 macrophages after spinal cord injury. Acupunct Med. 2017;35(3):224–230. doi:10.1136/acupmed-2016-011107
34. Chen X, He H, Long B, et al. Acupuncture regulates the apoptosis of ovarian granulosa cells in polycystic ovarian syndrome-related abnormal follicular development through LncMEG3-mediated inhibition of miR-21-3p. Biol Res. 2023;56(1):31. doi:10.1186/s40659-023-00441-6
35. Ye Y, Zhou -C-C, Hu H-Q, Fukuzawa I, Zhang H-L. Underlying mechanisms of acupuncture therapy on polycystic ovary syndrome: evidences from animal and clinical studies. Front Endocrinol. 2022;13:1035929. doi:10.3389/fendo.2022.1035929
36. Yang J, Lu Y, Zhang Y, Zhou C, Liang Q, Liang T. Acupuncture combined with gonadotropin-releasing hormone agonists improves endometrial receptivity and pregnancy outcome in patients with recurrent implantation failure of in vitro fertilization-embryo transfer. J Assist Reprod Genet. 2024;41(8):2185–2192. doi:10.1007/s10815-024-03140-7
37. Quan K, Yu C, Wen X, Lin Q, Wang N, Ma H. Acupuncture as treatment for female infertility: a systematic review and meta-analysis of randomized controlled trials. Evid Based Complement Alternat Med. 2022;2022:3595033. doi:10.1155/2022/3595033
38. Sheehan MT. Polycystic ovarian syndrome: diagnosis and management. Clin Med Res. 2004;2(1):13–27. doi:10.3121/cmr.2.1.13
39. Teede H, Deeks A, Moran L. Polycystic ovary syndrome: a complex condition with psychological, reproductive and metabolic manifestations that impacts on health across the lifespan. BMC Med. 2010;8(1):41. doi:10.1186/1741-7015-8-41
40. Zhao M, Liang R. A randomized single-blind clinical controlled study on the use of electroacupuncture for ovulation induction in polycystic ovary syndrome. Prac Clin J Integrated Trad Chinese Western Med. 2014;14(8):66–68.
41. Wang L, Zhang Y, Jia H. Research advances in the mechanism of acupuncture treatment for premature ovarian failure in recent 10 years. Shanghai J Acupunct Moxibust. 2017;36(3):361–364.
42. Zhang Y, Yu B, Chen J, et al. Effects of acupuncture on PI3K/Akt/mTOR signaling pathway in rats with premature ovarian failure. Zhongguo zhen jiu. 2015;35(1):53–58.
43. Romualdi D, Ata B, Bhattacharya S, et al. Evidence-based guideline: unexplained infertility†. Hum Reprod. 2023;38(10):1881–1890. doi:10.1093/humrep/dead150
44. Tjon-Kon-Fat RI, Tajik P, Zafarmand MH, et al. IVF or IUI as first-line treatment in unexplained subfertility: the conundrum of treatment selection markers. Hum Reprod. 2017;32(5):1028–1032. doi:10.1093/humrep/dex037
45. Calhaz-Jorge C, De Geyter C, Kupka MS, et al. Assisted reproductive technology in Europe, 2013: results generated from European registers by ESHRE†. Hum Reprod. 2017;32(10):1957–1973. doi:10.1093/humrep/dex264
46. Kushnir VA, Barad DH, Albertini DF, Darmon SK, Gleicher N. Systematic review of worldwide trends in assisted reproductive technology 2004–2013. Reprod Biol Endocrinol. 2017;15(1):6. doi:10.1186/s12958-016-0225-2
47. Guven PG, Cayir Y, Borekci B. Effectiveness of acupuncture on pregnancy success rates for women undergoing in vitro fertilization: a randomized controlled trial. Taiwan J Obstet Gynecol. 2020;59(2):282–286. doi:10.1016/j.tjog.2020.01.018
48. Huang Y, Li Y, Yang Y, Li M, Cai L. Analysis on medication law for differential diagnostics of treating gynecological diseases from “Chong-Ren” by CAI Lian-xiang. Chin J Inf Traditional Chin Med. 2017;24(03):91–95.
49. Bai M, Wang T, Li Y, Zhang Y, Wang J, Wang Q. Discussion the thinking of TCM constitution on treatment of infertility based on FU Qing-zhu Nvke. China J Tradition Chinese Med Pharm. 2019;34(08):3388–3391.
50. Li R, Du X, Wu X. Treatment of Infertility from Spleen and Stomach. Clin J Trad Chinese Med. 2021;33(08):1465–1468.
51. Huang Q, Xu H. Treatments of infertility in unicornuate uterus with premature ovarian insufficiency from the perspective of regulating the “pivot”. Guangming J Chinese Med. 2024;39(13):2689–2692.
52. Yuan C, Liu M, Yi J. A survey of gynecological diseases in Sisheng Xinyuan. Tianjin J Traditional Chin Med. 2020;37(11):1265–1267.
53. Liu Y, Zhong F, Shi W, Zhang W. Application of point Zigong to gynecological diseases and its modern theoretical basis. Shanghai J Acupunct Moxibust. 2015;34(04):364–366.
54. Chang G, Feng G. A shallow analysis of clinical practice of guanyuan acupoint in great compendium of acupuncture and moxibustion. Chinese and Foreign Med Res. 2022;20(12):177–180.
55. Kou R, Zou Y, Zhang J. Discussion of biological effects of moxibustion at Guanyuan (CV 4) and its influence factors. Zhongguo zhen jiu. 2016;36(12):1273–1277. doi:10.13703/j.0255-2930.2016.12.013
56. Zhong X, Xu L. Experience in treating diminished ovarian reserve based on Fu Qingzhu’s theories of “regulating menstruation” and “promoting fertility”. J Basic Chinese Med. 2024;30(04):709–712.
57. Zhang R, Wang X, Wang X. Analysis of the law of TCM acupoint selection and prescription medication in IVF-ET. Clin J Trad Chinese Med. 2020;32(11):2114–2121.
58. Zhu X, He P, Ma Z, Luo C. Analysis of acupoint selection of gynecopathy in Zisheng classic of acupuncture and moxibustion. Chin J Ethnomedicine Ethnopharm. 2023;32(09):107–114.
59. Liu J, He H, Chen C, Tan T. Analysis of clinical application of Taichong point in great compendium of acupuncture and moxibustion. China Modern Medicine. 2024;31(11):92–96.
60. Wu Z, Chai C, Meng L, Chen S, Gneg H, Wang C. Clinical study on the treatment of polycystic ovary syndrome with acupuncture using Shu-Mu (Back-Shu and Front-Mu) point combination. J Li-shizhen Trad Chinese Med. 2024;35(07):1685–1687.
61. Wu C, Huang Q, Xie C, Yang G, Zhang C. Literature metrology study on acupuncture and moxibustion in treatment of infertility based on randomized controlled trials. Acad J Shanghai Univ Trad Chinese Med. 2022;36(04):84–91.
62. Bi F, Yan Y, Ma J, Liang X, Chu M. Effects of acupuncture Guanyuan-Sanyin on ovarian reserve function and ovarian blood perfusion in patients with DOR. J Rare Uncommon Dis. 2024;31(01):95–96.
63. Zhou J, Zhang X, Yu M, Lu S, Chen X. Effect of transcutaneuos acupoint electrostimulation on serum sex hormone levels and expression of ovarian steroid hormone metabolic enzymes in polycystic ovary syndrome rats. Zhen Ci Yan Jiu. 2016;41(1):11–17.
64. Xing LW, Liu F, Dong QZ, et al. Efficacy observation of staged acupuncture and moxibustion therapy based on the theory of ‘thorough fare vessel being sea of blood’ on frozen-thawed embryo transfer in patients with polycystic ovary syndrome. China J Tradition Chinese Med Pharm. 2022;5(37):2755–8.
65. Huang L, Chen S. Curative effect of acupuncture for coordinating Chong-Ren and strengthening kidney combined with Yigong Yangpao decoction on small follicular ovulation infertility and its effect on the function of the hypothalamus-pituitary-ovarian axis. Mod J Integr Traditional Chinese Western Med. 2021;30(02):160–3+203.
66. Yan X, Wang L, Guo Y, Liu Y, Ding R. Meta analysis on prevalence of anxiety and depression of patients with polycystic ovary syndromen in China. Chin Med Herald. 2022;19(27):92–96.
67. Chen R, Liu Y, Wang Q, Kong X, Jin F, Mo T. Clinical experience in the treatment of ovulatory dysfunction-related infertility in polycystic ovary syndrome. J China Japan Friendship Hospital. 2023;37(01):44–46.
68. Veitia RA. Primary ovarian insufficiency, meiosis and DNA repair. Biomed J. 2020;43(2):115–123. doi:10.1016/j.bj.2020.03.005
69. Zu Q, Song X, Zhang C. Experience of acupuncture,medicinal,and moxibustion in treating infertility of premature ovarian insufficiency. China’s Naturopathy. 2023;31(09):51–55.
70. Xu X, Lv M, Jiang Z, et al. Research progress of acupuncture therapy assisting in IVE-ET. J Clin Acupunct Moxibust. 2019;35(10):102–105.
71. Hu R, Zhang C, Song Y, Zhang M, Huang G, Dong H. Review of clinical application of acupuncture and moxibustion in different patient groups in terms of assisted reproduction technology. J Clin Acupunct Moxibust. 2022;38(12):83–88.
72. Chen S, Deng Y, Huang X, et al. The experience of integrative acupuncture and moxibustion in assisted reproduction: a phased approach of “one needle, two Moxa, three consolidation”. Global Trad Chinese Med. 2023;16(09):1867–1869.
73. Ong SS, Tang T, Xu L, et al. Research on the mechanism of core acupoints in electroacupuncture for functional constipation based on data mining and network acupuncture. Front Med Lausanne. 2024;11:1482066. doi:10.3389/fmed.2024.1482066
74. Xue Q, Huang S, Liu LX, et al. Efficacy and dispensing patterns of TCM-acupuncture combinations in vascular dementia treatment: a meta-analysis and data mining analysis. Am J Transl Res. 2024;16(11):6187–6207. doi:10.62347/ZYCW4830
75. He Y, Wu Y, Li X. Analysis of acupoint selection and combinations in acupuncture treatment of migraine: a protocol for data mining. J Pain Res. 2024;17:4149–4157. doi:10.2147/JPR.S489296
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Analysis of Acupoint Selection and Combinations in Acupuncture Treatment of Carpal Tunnel Syndrome: A Protocol for Data Mining
He Y, Miao F, Fan Y, Zhang F, Yang P, Zhao X, Wang M, He C, He J
Journal of Pain Research 2023, 16:1941-1948
Published Date: 7 June 2023
Analysis of Acupoint Selection and Combinations in Acupuncture Treatment of Piriformis Syndrome: A Protocol for Data Mining
He Y, Miao F, Fan Y, He J, Zhang F, Wang Z, Wu Y, Zhao Y, Yang P
Journal of Pain Research 2023, 16:3265-3272
Published Date: 28 September 2023
Acupoint Selection in Postoperative Ophthalmic Pain Management: A Data Mining Protocol
Wang J, Yang F, Wang X, Pang F
Journal of Pain Research 2024, 17:903-909
Published Date: 5 March 2024
A Data Mining Study for Analysis of Acupoint Selection and Combinations in Acupuncture Treatment of Carpal Tunnel Syndrome
He Y, Miao F, He C, Fan Y, Zhang F, Yang P, Wang M, He J
Journal of Pain Research 2024, 17:1153-1170
Published Date: 18 March 2024
Exploration of the Application Rules and Clinical Significance of Acupoints in Acupuncture Treatment of Migraine Based on Data Mining
He Y, Wang X, Liu M, Li L, Han T, Wu Y, Li X
Journal of Pain Research 2025, 18:3049-3067
Published Date: 18 June 2025