")
Back to Journals » Journal of Experimental Pharmacology » Volume 12
Experimental and Investigational Pharmacotherapy for Psoriatic Arthritis: Drugs of the Future
Authors Navarini L, Currado D, Costa L , Tasso M, Chimenti MS , Caso F
Received 9 September 2020
Accepted for publication 24 October 2020
Published 16 November 2020 Volume 2020:12 Pages 487—502
DOI https://doi.org/10.2147/JEP.S265633
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Uwe Wollina
Luca Navarini,1,* Damiano Currado,1,* Luisa Costa,2 Marco Tasso,2 Maria Sole Chimenti,3 Francesco Caso2
1Unit of Rheumatology, Immunology and Clinical Medicine, Università Campus Bio-Medico Di Roma, Rome, Italy; 2Rheumatology Unit, Department of Clinical Medicine and Surgery, School of Medicine and Surgery, University of Naples Federico II, Naples, Italy; 3Rheumatology, Allergology and Clinical Immunology, Department of Systems Medicine, University of Rome Tor Vergata, Rome, Italy
*These authors contributed equally to this work
Correspondence: Francesco Caso
Rheumatology Unit, Department of Clinical Medicine and Surgery, School of Medicine and Surgery, University of Naples Federico II, Via Pansini 5, Naples 80131, Italy
Tel +39 081 7463773
Fax +39 081 5463445
Email [email protected]
Abstract: In recent years, different studies have shown in psoriatic arthritis (PsA), the pathogenetic role of multiple cytokines other than tumor necrosis factor-α, such as interleukin-17 (IL-17), and IL-23 and dysfunction of Janus kinase (JAK)-signal family pathway. These molecules also represent the target of recently developed biologic (bDMARDs) and targeted synthetic disease modifying antirheumatic drugs (DMARDs) (tsDMARDs) currently investigated in several Phase II and III randomized controlled trials (RCTs). This review examines the therapeutic efficacy and safety of most recent developed IL-17, IL-23 and JAK inhibitors and highlights how these new PsA therapies are going to revolutionize the management of PsA in the next few years. Ongoing RCTs of these molecules in PsA are also described. Available literature on new anti-IL-17 and anti-IL-23 agents and JAK inhibitors demonstrates the potential role of these molecules as effective therapeutic strategies across multiple PsA clinical domains, along with an acceptable tolerability and safety profile, thus expanding the treatment options available for PsA patients. Of note, other molecules are under investigation, and among those, potential therapeutic strategies seem to be represented by single antibodies blocking simultaneously two cytokines, the agents inhibiting mammalian target of rapamycin (mTOR), receptor retinoic acid receptor-related orphan receptor gamma (RORγt), A3 adenosine receptor (A3 AR), and K+ channel voltage channel inhibitors. Remarkable progress has been made in PsA pharmacotherapy, and novel bDMARDs targeting IL17A and tsDMARDs (JAK-inhibitors) represent promising therapies. More clinical trials are needed to better characterize the efficacy and safety profile of these therapeutic agents in PsA treatment.
Keywords: bDMARDs, filgotinib, IL-17 inhibitors, IL-23 inhibitors, JAK-inhibitors, psoriatic arthritis, tofacitinib, tsDMARDs, upadacitinib
Introduction
Psoriatic arthritis (PsA) is a chronic inflammatory arthropathy associated with psoriasis and/or its familiarity. The disease affects the joints, entheses and periarticular structures, usually with an onset age around the fourth decade equally in men and women.1 PsA induces also non-musculoskeletal inflammatory manifestations,2 involving gut (inflammatory bowel disease) and eyes (uveitis),3–5 and comorbidities, such as obesity, metabolic syndrome (MetS), diabetes, hypertension, cardiovascular (CV) disease, and osteoporosis which impact significantly on patients’ quality of life (QoL).6–13
PsA aetiology remains still unknown, but pathogenetic models suggest a complex interaction between multiple genetic (ie, HLA-B*27 and HLA-C*0602 alleles), environmental (ie, infections, biomechanical stress or trauma) and immunologic factors (ie, T helper lymphocyte subsets), able to start and sustain underlining PsA inflammatory mechanisms.14,15
PsA clinical manifestations can be heterogenous, characterized by a predominant axial (psoriatic spondylitis) or peripheral involvement.16,17 On the basis of the distribution of peripheral articular involvement, this phenotype can be distinguished as asymmetric oligoarthritis, peripheral polyarthritis, distal interphalangeal (DIP) joint arthritis, and the rare arthritis mutilans’.18 Enthesitis and dactylitis represent two clinical hallmarks of the disease. The first one may be observed in up to half of PsA patients and frequently at lower limbs, mainly involving Achilles tendon or plantar fascia.19,20 Dactylitis, a painful swelling of one or more entire fingers, is represented by an extrasynovial and tenosynovial sheath compartment inflammation, and can occur in up to 40% of PsA cases.21–24
Joint X-Rays are useful for demonstrating articular damage and staging damage progression over the times. Radiological findings are mainly characterized by juxta-articular erosions, osteolysis phenomena and, mostly in advanced phases, new bone formation.25–28
Imaging techniques, such as Magnetic Resonance Imaging (MRI) and ultrasound (US) combined with power Doppler (PD), can be helpful to detect early and active articular and periarticular inflammatory lesions.29–33
In the above half of PsA patients, serum inflammatory markers, such as erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) are increased, and usually Rheumatoid Factor (RF) and anti-citrullinated peptide antibodies (ACPAs) are negative.34,35
The diagnosis of the disease relies on the presence of concomitant or past psoriasis and/or familial history of psoriasis in a first- or second-degree relative, mainly when combined with inflammatory axial involvement, dactylitis and enthesitis, and/or peripheral arthritis.36,37
Management and Follow-Up of Psoriatic Arthritis
The follow-up of the disease can be performed by measures that evaluate the involvement of skin [namely, Psoriasis Area Severity Index (PASI) or Body Surface Area (BSA) and Nail Psoriasis Severity Index (NAPSI)], axial skeleton [namely, Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and Bath Ankylosing Spondylitis Functional Index (BASFI)], entheseal and articular involvement (namely, Leeds Dactylitis Index (LDI), tender entheseal count (TEC), swollen and tender joints count (SJC and TJC). Other domains such as patient’s reported outcomes (PROs), QOL and pain should be evaluated routinely. Combination of single measures results in several composite indices that evaluate disease activity, such as the Composite Psoriatic Disease Activity Index (CPDAI), Psoriatic Arthritis Disease Activity Score (PASDAS), Disease Activity Index for Psoriatic Arthritis (DAPSA).38,39 The contemporaneous achievement of five of the following seven criteria defines a minimal disease activity (MDA) status: TJC ≤ 1; SJC ≤ 1; PASI ≤ 1 or BSA ≤ 3%; patient pain visual analog score (VAS) ≤ 15; patient global disease activity VAS ≤ 20; Health Assessment Questionnaire Disability Index (HAQ-DI) ≤ 0.5; tender entheseal points ≤ 1.39–41 American College of Rheumatology (ACR) criteria and the Disease Activity Score for 28 joints (DAS28) represent outcome measures mostly used in clinical trials.41,42
The Group for Research and Assessment of Psoriatic Arthritis (GRAPPA) highlights the key role of early diagnosis in order to address quickly an effective therapy. Further, GRAPPA recommends achieving disease remission or, alternatively, lowest possible level of disease activity and improvement of functional status. GRAPPA suggests initiating a treatment based on clinical domain involvement (eg, enthesitis, dactylitis, axial disease, peripheral arthritis) by standard and expedited regimens.43
The European League Against Rheumatism (EULAR) provides an algorithm recommending stepwise therapy based on disease severity. EULAR recommends cycles of nonsteroidal anti-inflammatory drugs (NSAIDs) and/or intraarticular steroid injections, when these are appropriate, to relieve musculoskeletal symptoms. Conventional synthetic DMARDs (csDMARDs), first methotrexate (MTX), or in case of its contraindications sulfasalazine (SSZ) or leflunomide (LFN), should be reserved for those with peripheral arthritis and increased serum levels of ESR and/or CRP. Patients who do not respond to csDMARDs may be switched to bDMARDs, such as inhibitors of Tumor Necrosis Factor-α (TNFis) agents or to anti-IL-17/or anti-IL12/23 agents in case of contraindication to TNFis.44
The American Academy of Rheumatology (ACR)/National Psoriasis Foundation (NPF) guidelines recommend the use of anti-TNF agents over csDMARDs and the Phosphodiesterase-4 inhibitor (PDE4i), apremilast (APR), for treatment-naïve severe patients. csDMARDs, apremilast and TNFis are generally recommended over biologics other than TNFis.45 bDMARDs monotherapy should be preferred to combination with csDMARDs, unless contraindicated.45 For active PsA, despite the treatment with TNFis, a second anti-TNF agent should be preferred.45 In case of adverse events with TNFis or primary TNFis failure, it is suggested to switch to a non-TNF bDMARD.45 In case of failure to TNFis monotherapy, it is suggested the use of IL-17 inhibitors over IL-12/23 inhibitors, or the JAKi, tofacitinib.45 In case of failure to IL-17 inhibitors, it is suggested to switch to IL-12/23 inhibitors rather than to add MTX.45 In PsA patients showing a concomitant IBD, IL-12/23 inhibitors represent valid therapeutic strategies.45
Similarities and differences between these three sets of recommendations are summarized in Table 1.
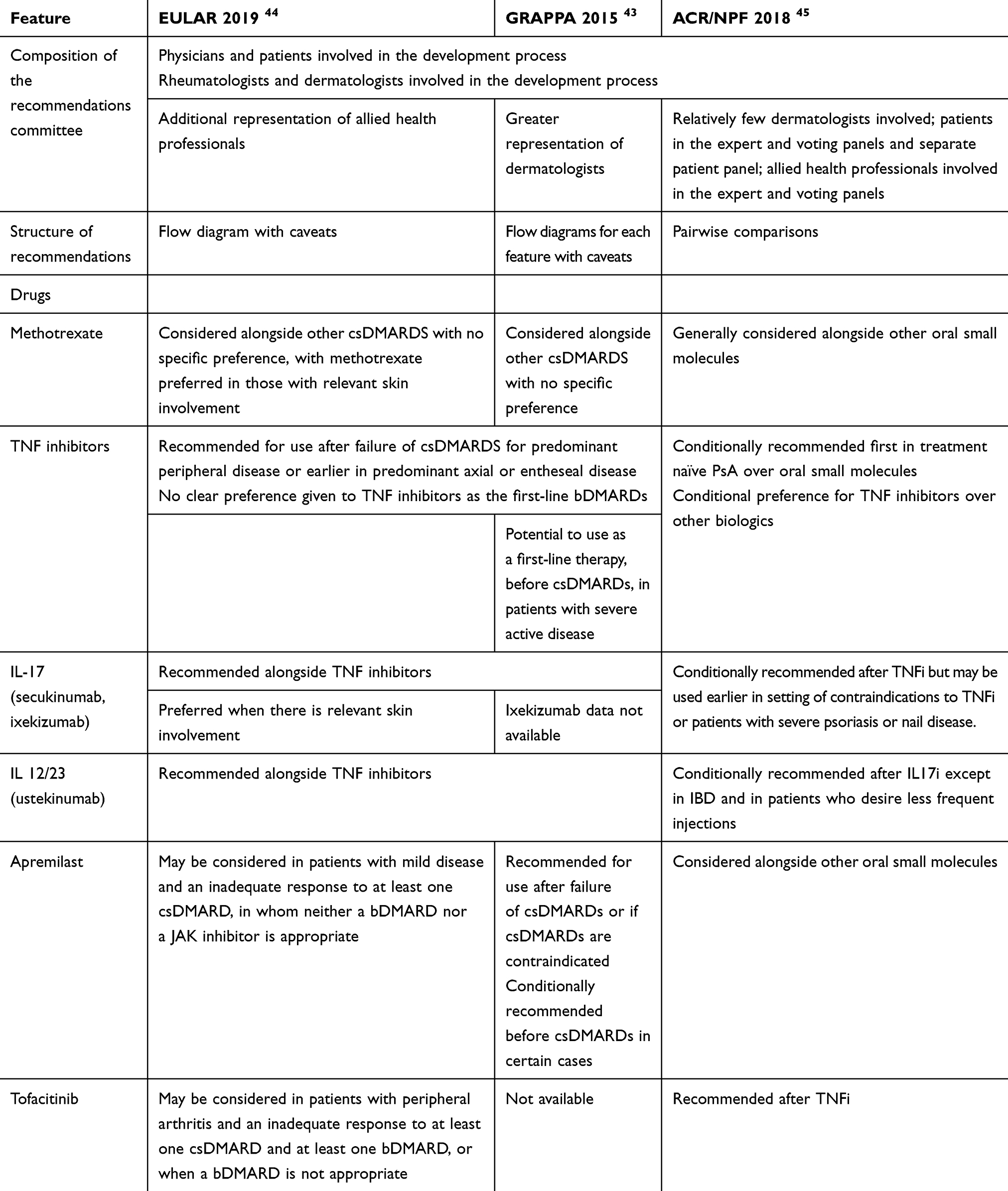 |
Table 1 EULAR 2019, GRAPPA 2015 and ACR/NPF 2018 Recommendations for the Management of PsA: Similarities and Differences |
Nonpharmacological therapy, such as physical and occupational therapy, weight loss, and smoking cessation, may ameliorate disease.45 It is also clearly important a multidisciplinary approach to assess comorbidities and encourage shared decision-making.43
Overall, bDMARDs are highly effective across all multiple clinical domains of PsA.46–48
In particular, in the last two decades, bDMARDs targeting selectively inflammatory cytokines, such as TNF [namely, adalimumab (ADA), certolizumab-pegol (CTZ), etanercept (ETN), golimumab (GOL), and infliximab (IFX)], interleukin (IL)-12/23, ustekinumab (UST) and IL-17A, secukinumab (SEC) and ixekizumab (IXE), have revolutionized therapy in PsA, as they are effective in improving symptoms and signs and inhibiting radiographic disease progression. Moreover, bDMARDs are safe if associated with an appropriate pre-treatment screening and strict follow-up.49–61
In recent years, the tsDMARD, APR, which inhibits the synthesis of multiple pro-inflammatory cytokines and modulates the release of anti-inflammatory molecules, has expanded therapeutic strategies for PsA.53 Of note, more recently, promising therapies are under investigation in several phase II and III clinical trials, such as agents targeting IL-17, IL-23, and the Janus Kinase inhibitors (JAKis). Inhibitors of the kinase mammalian target of rapamycin (mTOR), receptor retinoic acid receptor-related orphan receptor gamma (RORγt) inhibitors, CF101, a selective agonist with high affinity to the A3 adenosine receptor (A3 AR), and K+ channel voltage channel inhibitors represent molecules actually in the early phase of investigation. 62, 63,64
Novel IL-17 Inhibitors
Recently, advances in the role of IL-17 in PsA pathogenesis, and especially in the pathogenesis of enthesitis and dactylitis, have led to the development of therapeutic agents that target this proinflammatory molecule. Many evidences have demonstrated the positive effects of SEC and IXE in PsA.53,62–64
SEC is a recombinant, fully human monoclonal IgG1/kappa antibody targeting human IL-17A, and its efficacy and safety have been reported across a series of trials, FUTURE 1–5.65–68
SEC 300 mg and 150 mg have been reported to have a quite acceptable safety profile and to provide sustained improvements in signs and symptoms and to inhibit radiographic structural progression in active PsA patients over time.66–68 IXE, another monoclonal antibody against IL-17A, is approved for the treatment of PsA.69–71 IXE significantly improved skin symptoms, health-related QoL and work productivity in bDMARDs-naïve patients with active PsA.70 IXE 80 mg every 2 weeks or every 4 weeks after a 160-mg starting dose treatment (the latter currently used in clinical practice) demonstrated sustained efficacy in key PsA domains.71
Brodalumab (BRO), a human anti-IL-17 receptor A (IL-17RA) monoclonal antibody, shows a peculiar mechanism of action inhibiting not only IL-17A but also the activity of other members of the IL-17 family, including interleukin-17F, interleukin-17A/F, and interleukin-17E.72 BRO is Food and Drug Administration (FDA) approved for moderate-to-severe psoriasis treatment, but not for PsA. BRO, at the dosage of 210 mg subcutaneously (SC) at weeks 0, 1, 2, and then every 2 weeks, demonstrated a favorable safety profile and the most frequent Adverse Events (AEs) are represented by nasopharyngitis, upper respiratory tract infection, neutrophil count decrease and headache.63
In a Phase II, randomized, double-blind, placebo-controlled study (ClinicalTrials.gov number, NCT01516957) involving 168 PsA patients, BRO (at the dosage of 140 or 280 mg SC, on day 1 and at week 1, 2, and then every 2 weeks) significantly improved response rates among patients at 12 weeks; the primary endpoint, which was represented by ACR20 response, was achieved by 37% of the patients receiving BRO 140 mg (p=0.03) and by 39% of the patients receiving BRO 280 mg (p=0.02), whilst in the placebo group ACR20 was achieved by 18% of the patients. Moreover, ACR50 response was achieved in 14% of enrolled subjects whereas in only 4% of subjects belonging to the placebo group.72 In the open extension study, ACR50 response was achieved in 33% of patients who continued their participation in the clinical study and started BRO at the dosage of 280 mg every 2 weeks.72
BRO has been also investigated in two recently terminated, double-blind, placebo-controlled, Phase III trials, AMVISION-1 (NCT02029495) and AMVISION-2 (NCT02024646). These trials enrolled 962 adult patients with active PsA (≥3 SJC and ≥3 TJC) despite prior cs- and bDMARDs, randomized to receive placebo, BRO140 mg or BRO 210 mg every 2 weeks.73,74 In a pooled analysis of AMVISION-1 and AMVISION-2 trials, at week 24, a higher rate of patients treated with BRO achieved ACR20 response, which was the primary endpoints, compared to placebo (210 mg: 55% [95% CI: 48%–61%]; 140 mg: 51% [95% CI: 45%–57%]) vs PBO 24% [95% CI: 19%–30%]; P = 0.0001).75
Another therapeutic approach under investigation in PsA is represented by the dual neutralization of IL-17A and IL-17F, by the selective humanized monoclonal antibody Bimekizumab (BMK).76
The BE ACTIVE study (Trial number NCT02969525), a randomised, double-blind, placebo-controlled phase IIb trial, in which the primary endpoint was the proportion of patients with at least ACR50 improvement at week 12 and which involved 206 patients, showed that BMK was associated with significant joint improvement compared with placebo, with an acceptable safety profile.76 More in particular, in this trial, patients were randomly assigned (1:1:1:1:1) to placebo (n: 42), and 41 to each of the four BMK groups (16 mg BMK, 160 mg BMK, 160 mg BMK with a one-off 320 mg loading dose, or 320 mg BMK, administered as subcutaneous injections every 4 weeks).76 After 12 weeks, patients assigned to the placebo and 16 mg BMK groups were randomly reassigned (1:1) to either 160 mg or 320 mg BMK, and all other patients continued their originally assigned dose up to 48 weeks.76 Both BMK doses of 16 mg and 160 mg (with or without a 320 mg loading dose) were significantly associated with improvements in ACR50 compared with placebo, with an acceptable safety profile. Furthermore, most of AEs were mild or moderate. Serious treatment-emergent AEs occurred in eight of patients on BMK and no deaths or cases of inflammatory bowel disease were reported.76
BE COMPLETE77 and BE OPTIMAL78 are two double-blind, placebo-controlled, phase III clinical trials, currently recruiting, aiming at characterizing the clinical efficacy (ACR50 response at week 16), safety and tolerability of BMK administered SC compared with placebo (both trials) and with ADA (only BE OPTIMAL), respectively.
At present, research is also focusing on strategies blocking simultaneously IL-17A and TNF-α with a single antibody. This is the case of ABT-122 (Remtolumab), a TNF-α and IL-17A-targeted dual variable domain IgG1antibody. This drug has been investigated in a 12-week double-blind, parallel-group Phase II study involving 240 PsA active patients who have an inadequate response to MTX. The primary endpoint was represented by ACR20 response.79 In this trial, PsA patients were randomized to receive ABT-122 (120 or 240 mg every week), ADA (40 mg every other week), or placebo. This study showed that ABT-122 had an efficacy and safety profile that was comparable to, and not differentiated from, ADA over a 12-week treatment course in PsA patients. In particular, ABT-122 demonstrated to be superior to placebo but not superior to ADA regarding ACR20 response (primary endpoint). Nevertheless, ABT-122 was superior to Adalimumab regarding ACR50/70 and PASI75 responses for the 240 mg dosage, while other secondary endpoints such as low disease activity or clinical remission based on DAS28, CRP and PASI90 responses were similar for ABT-122 both at 120 and 240 mg every week as compared to ADA.79 Frequencies of treatment-emergent AEs, including infections, were similar across all treatment groups. No serious infections or systemic hypersensitivity reactions were reported with ABT-122.79 Main data derived from Phase III RCTs of anti-IL-17 agents under investigation in PsA are reported in Table 2.
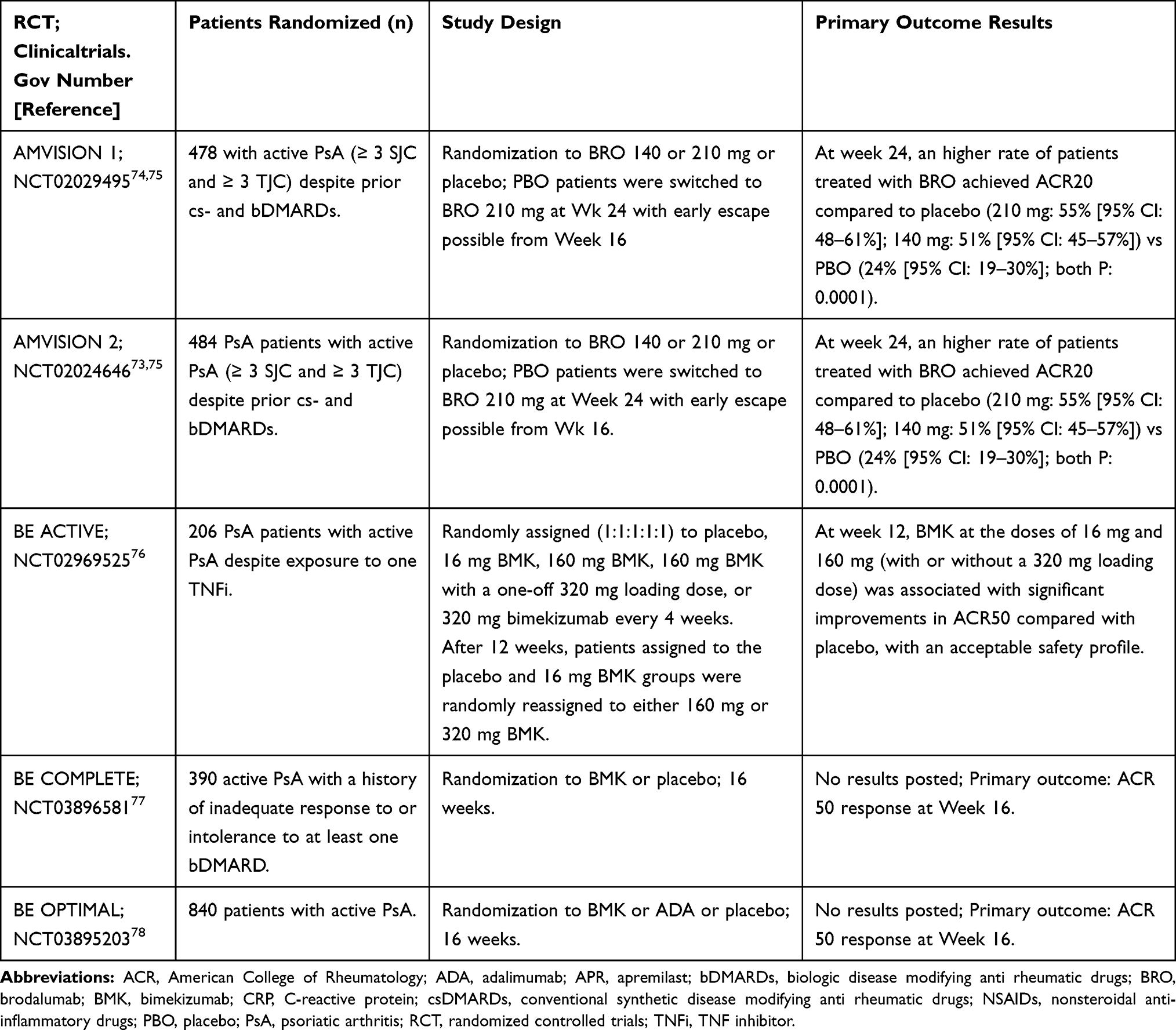 |
Table 2 Main Data Derived from Phase III Randomized Controlled Trials of New Anti-Interleukin (IL)-17 Agents Under Investigation in Psoriatic Arthritis |
IL-23 Inhibitors
In recent years, erosive and osteoproductive phenomena and bone remodeling in PsA, sustained by multiple cytokines, but mainly by the interplay between IL-23 and IL-17, have represented a main research focus in Psoriatic Disease (PsD).53,62–64
Several evidences have reported the key role of the proinflammatory cytokine, IL-23, a member of the IL-12 family, in PsD pathogenesis. IL-23 is a heterodimer composed of two combined subunits, p40, which is shared by IL-23 and IL-12, and p19, which is shared by IL-23 and IL-39. IL-23 drives the expansion and function of pathogenic Th-17 cells. Overexpression of IL-23 and consequent overproduction of Th17 cytokines (IL-17 and IL-22) mediate the development of psoriatic plaque, synovitis, joint erosion, enthesitis and new bone formation. IL-23 represents a therapeutic target in PsA and UST, an antibody against p40 subunit has been the first bDMARD targeting this cytokine approved for PsA treatment.53,63,64,80
More recently, three new antibodies against the p19 subunit of IL-23, Guselkumab (GSK), Tildrakizumab (TIL) and Risankizumab (RSK), have been developed. These bDMARDs have been approved by FDA for moderate-to-severe plaque psoriasis and they are now under investigation in phase II/III RCTs for PsA.53,63,64,80
In a recent randomised, double-blind, placebo-controlled, Phase 2a clinical trial (ClinicalTrials.gov registration number: NCT02319759) involving 149 patients with active PsA (≥3 TJC and ≥3 SJC) and plaque psoriasis (at least 3% BSA), who had an inadequate response or intolerance to standard treatments, GSK significantly improved signs and symptoms of PsA as compared with placebo with regard with the primary endpoint which was represented by the ACR20 response and was well tolerated during 44 weeks of treatment.81 In this study, 100 patients were randomized to GSK and 49 to placebo (2:1). Thirty-five percent of patients in placebo group and 10% of patients in GSK group were eligible for an early escape to the anti-IL12/23 antibody, UST, at week 16. Twenty nine (59%) of 49 patients in the placebo group crossed over and received GSK at week 24.81 Six percent of 49 patients in the placebo group, 3% of 29 patients who crossed over from placebo to GSK, and 6% of 100 patients in the GSK group discontinued study treatment before week 44.81 Fifty-eight percent of 100 patients in the GSK group and 18% of 49 patients in the placebo group achieved an ACR20 response at week 24 (percentage difference 39.7% [95% CI 25.3–54.1]; p<0·0001). Between week 0 and week 24, 36% of patients in the GSK group and 33% of 49 patients in placebo group reported at least one adverse event. For both groups, the most frequent adverse event was infection. The prevalence of adverse events between week 0 and week 56 in GSK-treated patients (51 [40%] of 129) indicated no disproportional increase with longer GSK exposure. No deaths occurred.81
Additional two phase III clinical trials, DISCOVER-1 (ClinicalTrials.gov Number Registration: NCT03162796) and DISCOVER-2 (ClinicalTrials.gov Number Registration: NCT03158285), have focused their attention on GSK efficacy and safety in PsA.82,83
In DISCOVER-1, which involved patients who were either biologic-naïve or have been previously treated with up to two TNFis, the improvement in peripheral arthritis at week 24 was significantly higher among patients on GSK than among those on placebo.82 DISCOVER-1 is a multicenter, double-blind, randomized, placebo-controlled, Phase 3 clinical trial that enrolled adult patients with active PsA (≥3 SJC and ≥3 TJC; and CRP ≥0.3 mg/dL) despite treatment. The 381 patients enrolled in DISCOVER-1 were randomly assigned to subcutaneous GSK 100 mg every 4 weeks, GSK 100 mg at weeks 0, 4, then every 8 weeks, or matching placebo. The primary endpoint was ACR20 at week 24. Significant greater proportions of patients achieved an ACR20 response at week 24 (primary outcome) in the GSK group than in the placebo group with percentage differences versus placebo of 37% (95% CI 26–48) for the GSK every 4 weeks group and 30% (19–41) for the GSK every 8 weeks group (both p<0.0001).82
DISCOVER-2, which enrolled 741 patients, was larger than DISCOVER-1, involved only patients bDMARDs – naïve and compared the treatment with GSK with placebo with regard to the primary endpoint which was represented by ACR20 response. The results of DISCOVER-2 are quite promising. In particular, a significantly greater proportions of patients on GSK every 4 weeks (156 [64%] of 245 [95% CI 57–70]) and every 8 weeks (159 [64%] of 248 [58–70]) achieved an ACR20 response at week 24 than in the placebo group (81 [33%] of 246 [27–39]) (percentage differences vs placebo 31% [95% CI 22–39]).83
At present, a GSK Phase 3b clinical study in PsA patients with inadequate response to TNFis (COSMOS) is enrolling (ClinicalTrials.gov: NCT03796858).84 The study comprises two arms: 1) experimental Group 1, in which participants will receive GSK 100 mg SC injection at Weeks 0, 4, 12, 20, 28, 36, and 44 and placebo SC at Week 24. At Week 16, participants who meet the early escape criteria and receive placebo at Week 16 will be treated with GSK at Week 20, and then GSK every 8 weeks (q8w); 2) Experimental Group 2 in which participants will receive placebo SC injection at Weeks 0, 4, 12, and 20, and will crossover to receive GSK 100 mg SC injection at Weeks 24, 28, 36, and 44. At Week 16, participants who meet the early escape criteria and receive GSK at Week 16 will be treated with GSK at week 20, then GSK every 8 weeks.84 The study will evaluate as primary outcome measure the percentage of participants who achieve an ACR 20 Response at Week 24; secondary outcome measures are: change from baseline in Health Assessment Questionnaire-Disability Index (HAQ-DI) Score at Week 24; percentage of participants who achieve an ACR 50 response at week 24; change from baseline in 36-Item Short Form Health Survey (SF-36) physical component summary (PCS) score at Week 24.84
Another anti-interleukin-23p19 monoclonal antibody, Tildrakizumab (TIL) (SUNPG1623), is now going through a Phase 2b (ClinicalTrials.gov: NCT02980692)85 and/or phase III trials in order to assess its efficacy (ACR 20 response at Week 24) and safety in subjects with active PsA naïve (INSPIRE 2; ClinicalTrials.gov: NCT04314531)86 or with prior exposure to anti-TNF agents (INSPIRE 1; ClinicalTrials.gov: NCT04314544).87
The anti-IL-23 humanized IgG1 monoclonal antibody, Risankizumab (RZB), is under investigation for PsA treatment in two Phase 3, randomized, double-blind, studies, KEEPsAKE 1 (ClinicalTrials.gov: NCT03675308) and KEEPsAKE 2 (ClinicalTrials.gov: NCT03671148). These will evaluate safety and efficacy of RZB in subjects with active PsA with history of inadequate response to or intolerance to at least one csDMARDs and bDMARDS, respectively, and the primary outcome will be an ACR20 response at week 24.88,89
Some of the results on RZB are already available. Indeed, data from a double-blind, parallel-design, dose-ranging Phase 2 study in 185 patients with active PsA have showed the achievement of ACR20 response at Week 16 (primary endpoint) in the groups of patients treated with RZB at different dosages (RZB 150 mg at weeks 0, 4, 8, 12, and 16 [Arm 1], 150 mg at weeks 0, 4, and 16 [Arm 2], 150 mg at weeks 0 and 12 [Arm 3], 75 mg single dose at weeks 0 [Arm 4]) when compared with placebo (PBO, Arm 5). Furthermore, RZB-treated patients (pooled across all RZB arms) showed evidence for inhibition of radiographic progression. RZB was well tolerated with no new or unexpected safety findings; the most common AE was infection but no cases of tuberculosis (TB) were reported.90
IL-23 inhibitors show some advantages over the IL-17 inhibitors represented by IL-17 upstream deactivation, leading to reduction of downstream pro-inflammatory cascades, and reduction of candidiasis risk.63,64,79,80 Main data derived from Phase III RCTs of anti-IL-17 agents under investigation in PsA are reported in Table 3.
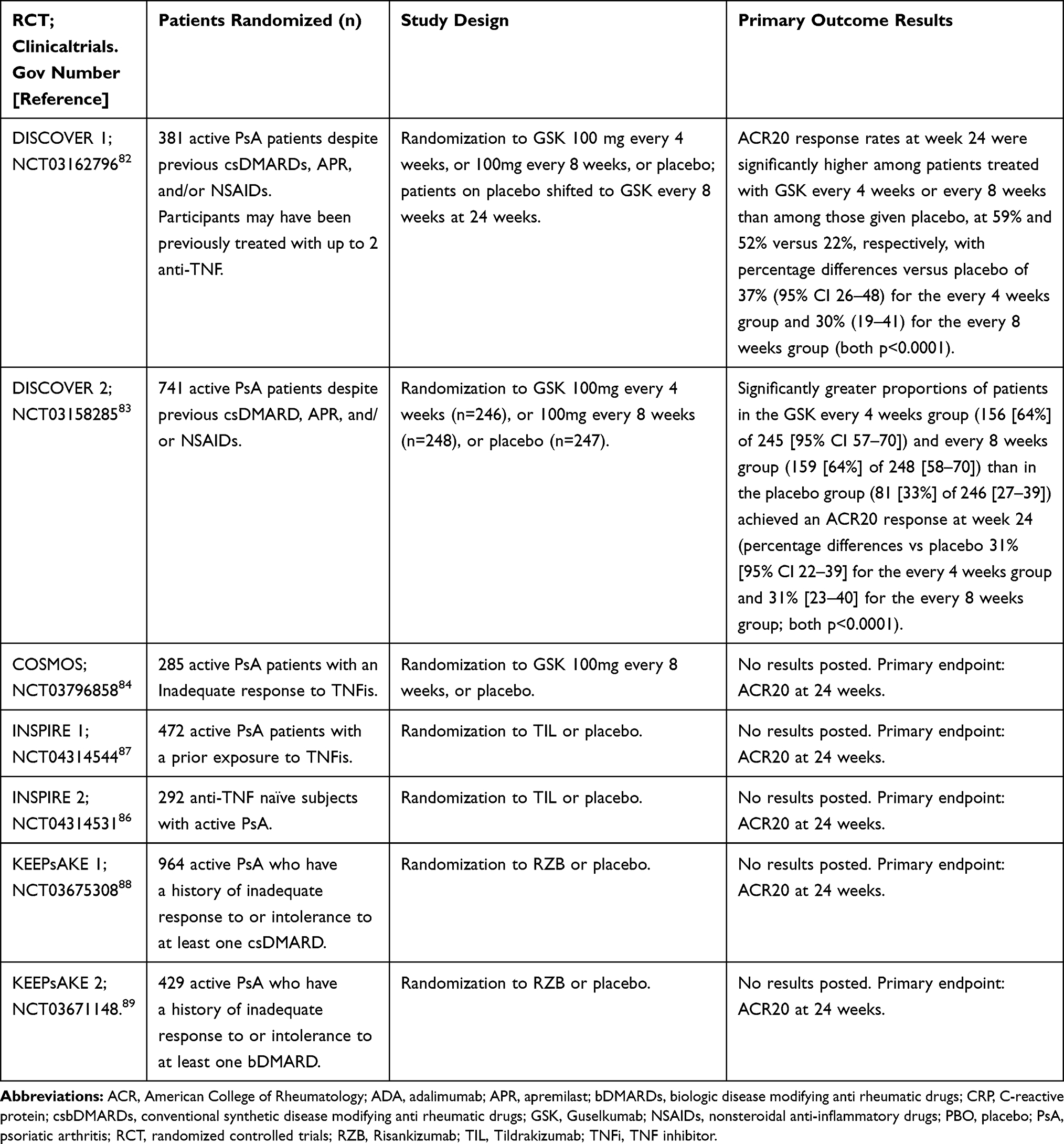 |
Table 3 Main Data Derived from Phase III Randomized Controlled Trials of Anti-Interleukin (IL)-23 Agents Under Investigation in Psoriatic Arthritis |
JAK Inhibitors
The activation of genes codifying for pro-inflammatory cytokines involved in PsA pathogenesis, such as TNFα, IL1β, IL-6, IL-23, and IL-17, is mediated by JAK/signal transducers (JAK1-3 and tyrosine kinase 2, TYK2) and Signal Transducers and Activators of Transcription 1–5a/b, 6 (STAT1-5a/b, 6) intracellular pathways.91–94
The tyrosine kinases belonging to JAK family include four members: JAK1, JAK2, JAK3 and tyrosine kinase 2 (TYK2).95–101 In this context, JAK-inhibitors (JAKi), some of them already approved for the treatment of Rheumatoid Arthritis, are emerging as promising therapeutic strategies for PsA, by targeting all JAKs or different JAK combinations.95–101
Tofacitinib is an oral inhibitor of JAK1 and JAK-3, approved at the dosage of 5 mg twice daily (BID), in combination with MTX for moderate-to-severe active PsA in adults who had inadequate response or intolerance to csDMARDs.102,103 This drug is characterized by several advantages, mainly represented by a fast onset of action, oral administration, and short half-life. Reduction of dosage at 5 mg once a day is recommended in subjects with moderate or severe renal and hepatic impairment and in patients on drugs inhibiting CYP2C19 and/or CYP3A4.104
In PsA, the efficacy and safety of tofacitinib were assessed for the first time by a Japanese 52-week RCT (clinicaltrials.gov NCT01519089).105 This study enrolled 94 adult patients with moderate-to-severe PsA (n=12) and/or psoriasis patients (n=87), which were randomized to receive tofacitinib 5 or 10 mg BID for initial 16 weeks.105 The primary endpoint for patients with PsA was ACR20 response. At week 16, all patients received open‐label tofacitinib 10 mg BID for 4 weeks, and then to week 52, tofacitinib dosage was adjusted to 5 or 10 mg BID.105 Tofacitinib showed efficacy in achieving ACR20 response in all the enrolled subjects. Furthermore, 75% and 87.5% of the patients on tofacitinib 5 mg and 10 mg BID achieved ACR50, respectively, and 50% and 62.5% of the patients on tofacitinib 5 mg and 10 mg BID achieved ACR 70 response.105
Efficacy and safety of tofacitinib have been evaluated in other two randomized, multicentric, double-blind, placebo-controlled phase III clinical trials, which enrolled 800 adult patients with active PsA and either an inadequate response to ≥1 csDMARD and TNFis-naïve (Oral Psoriatic Arthritis triaL (OPAL) Broaden) (ClinicalTrials. Gov: NCT01877668); or had an inadequate response to ≥1 TNFi (Oral Psoriatic Arthritis triaL (OPAL) Beyond) (ClinicalTrials. Gov: NCT01882439).106,107
In both trials, primary end-points were the percentage of patients with improvement in ACR20 and the change from baseline score in the HAQ-DI (scores range from 0 to 3, with higher scores indicating greater disability) at 3-month follow-up compared to placebo.106,107
In the OPAL Broaden program PsA patients (n:422) were randomized to receive tofacitinib 5 mg BID (n = 107), tofacitinib 10 mg BID (n = 104), ADA 40 mg once every 2 weeks (n = 106), and placebo. At month 3, all patients on placebo were treated with tofacitinib 5 mg or 10 mg BID.106 A significantly higher ACR20 response rate was observed in patients on tofacitinib (tofacitinib 5 mg: 50%; tofacitinib 10 mg: 61%) when compared with placebo (placebo: 33%).106 At month 3, the patients on tofacitinib 5 mg or 10 mg BID showed also a significantly higher response rate versus placebo with regard to ACR50 (tofacitinib 5 mg: 28%; tofacitinib: 10 mg 40%; and placebo: 10%) and ACR70 (tofacitinib 5 mg: 17%; tofacitinib 10 mg: 14%; and placebo: 5%) (P≤0.05).106 Of note, patients on tofacitinib showed an early improvement (2 weeks) from baseline in ACR20 response.106 Also, the other primary endpoint (change from baseline in Health Assessment Questionnaire-Disability Index (HAQ-DI)) at month 3 showed significant improvement in patients on tofacitinib 5 or 10 mg BID vs placebo (tofacitinib 5 mg −0.35, tofacitinib 10 mg −0.40 and placebo −0.18 with p≤0.05).106 Furthermore, at month 3, a significant greater proportion of patients on tofacitinib achieved PASI75 response when compared to placebo.106 Significant improvements in HAQ-DI, TJC, SJC, psoriasis, enthesitis and dactylitis were observed for tofacitinib 5 or 10 mg BID at month 3 compared to placebo and these beneficial effects lasted up to 6 months.108 Furthermore, results from an OPAL Broaden sub-analysis demonstrated that, at Month 3, patients receiving tofacitinib 5 mg BID and 10 mg BID have significant improvements in patient-reported outcomes (PROs), fatigue and QoL when compared with placebo (p≤0.05).109 Two OPAL Broaden post-hoc analysis showed positive effects of tofacitinib on radiographic outcomes, with mean changes from baseline through month 12 in erosion and joint space narrowing scores, as evaluated by van der Heijde-modified total Sharp score (mTSS).110 Furthermore, at month 12, >90% of the patients on tofacitinib met the criteria for articular radiographic non-progression in the joints. Nevertheless, minimal changes in radiographic outcomes regardless of CRP levels were observed.111
The OPAL Beyond trial enrolled 394 patients which were randomized to receive tofacitinib 5 mg BID (132 patients), tofacitinib 10 mg BID (132 patients), and placebo (131 patients), the latter group then shifting to tofacitinib either 5 mg (66 patients) or 10 mg BID (65 patients) at month 3.107 At month 3, a significant higher proportion of patient achieving ACR 20 response and favourable mean changes from baseline in HAQ-DI scores (primary outcomes) were observed, when both the tofacitinib groups were compared with the placebo one.107 As in the OPAL Broaden trial, also in the OPAL Beyond study, early improvement (2 weeks) from baseline in ACR20 response was demonstrated in patients on tofacitinib.107
Further, OPAL Balance (ClinicalTrials.gov identifier: NCT01976364), a long-term extension (LTE) study for assessing the long-term use of tofacitinib in 686 PsA Patients from OPAL Broaden and OPAL Beyond showed that its efficacy is maintained over time (30 months).112
With regard to tofacitinib safety, the majority of AEs are mild-moderate and the most common are nasopharyngitis, upper respiratory tract infection, headache and gastrointestinal disorders (diarrhoea, nausea, vomiting, constipation). In OPAL Balance, the incidence rate for specific AEs were: all (non-serious and serious) herpes zoster, 1.7; serious infections, 0.9; opportunistic infections, 0.3 (all disseminated/multi-dermatomal herpes zoster); malignancies excluding non-melanoma skin cancer (NMSC), 0.8; NMSC, 1.0; major adverse cardiovascular events, 0.3; pulmonary embolisms, 0.1; and arterial thromboembolisms, 0.4.112
Other JAKis are currently under investigation in phase 2 or phase 3 RCTs in PsA. For several of those, such as the oral JAK inhibitor with selectivity for JAK1, filgotinib, some data are already available.113
EQUATOR is the first randomized, double-blind, placebo-controlled phase II trial to investigate filgotinib in PsA as compared with placebo with regard to ACR20 (primary endpoint).113 This study explored efficacy and safety in 131 adult PsA patients with ≥5 SJC and ≥5 TJC and insufficient response or intolerance to at least one csDMARD. These patients were randomized to filgotinib 200 mg (n: 65) or placebo (n: 66) orally once daily for 16 weeks (stratified by concomitant csDMARDs and previous TNFis therapy).113 Data from EQUATOR demonstrated an improvement of disease activity, physical functioning, fatigue and pain, in PsA subjects on filgotinib 200 mg once-daily compared to placebo. Particularly, 80% of patients on filgotinib and 33% on placebo achieved ACR20 at week 16 (treatment difference 47%, p < 0.0001). ACR50 and ACR70 responses at Week 16 were also significantly higher for patients receiving filgotinib compared to patients treated with placebo. The study also found greater improvement of peripheral arthritis, enthesitis and psoriasis as measured by MDA and PASI 75, and showed significant improvements in psoriatic arthritis-related pain intensity at week 1 and in HAQ-DI at week 2 (105).113 Ninety-two percent of patients in the filgotinib group completed the study. Filgotinib proved to be acceptably safe with at least one AE, mainly represented by nasopharyngitis and headache, occurring in 57% of treated patients, without statistical significance in comparison with the placebo group (AEs frequency: 59%).113
Efficacy (primary endpoint: ACR20 response at Week 12) and safety of filgotinib at the dosage of 100 mg and 200 mg is currently under investigation in PENGUIN Phase 3 program in about 1400 active PsA patients both naive to bDMARDs (PENGUIN 1)114 or who have an inadequate response or are intolerant to bDMARDs (PENGUIN 2).115
Upadacitinib, (UPA), another JAK1 inhibitor approved by FDA for treatment of Rheumatoid Arthritis (RA), is under investigation in two PsA Phase III RCTs. The first trial (SELECT-PsA 1) compares the efficacy and safety of upadacitinib with placebo and ADA in 1705 adult patients with active PsA who have had an inadequate response to at least 1 csDMARDs;116,117 the second one (SELECT-PsA 2) compares upadacitinib to placebo in 641 PsA patients with inadequate response to at least one bDMARD.118,119
Preliminary results from the SELECT-1 cohort showed that from Week 2 of treatment UPA 15 mg or 30 mg once daily showed efficacy in improving articular symptoms, psoriasis, physical function, pain, and fatigue and in inhibiting radiographic progression. At Week 12, UPA 15 mg or 30 mg once daily were non-inferior to ADA with regard to ACR20 response, whilst UPA 30 mg showed its superiority as compared with ADA. Greater percentages of patients treated with UPA as compared with patients treated with placebo achieved stringent measures of disease control (such as MDA, ACR50 and ACR70 responses).116,117
In SELECT-2 cohort, UPA 15 mg and UPA 30 mg demonstrated significant improvements across different PsA domains including joint and skin signs and symptoms as compared with placebo at week 24, with an interesting improvement starting from Week 2. A greater percentage of patients treated with UPA achieved MDA and ACR50 and ACR70 responses. In SELECT-PsA1 and 2 programs, the incidence of serious infections and cardiovascular events seems to be lower in patients treated with UPSA.117,119
There are other tsDMARDs under investigation for PsA treatment. BMS-986165 is an oral agent blocking a nonreceptor tyrosine kinase 2 (TYK2) with high selectivity, modulating IL-12, IL-23, and type I IFNs immune-inflammatory response.120–122
A trial with BMS-986165 is ongoing for evaluating the safety and efficacy of two different dosages of this molecule compared with placebo in active PsA patients.123
Main data derived from Phase III RCTs of JAKis under investigation in PsA are reported in Table 4.
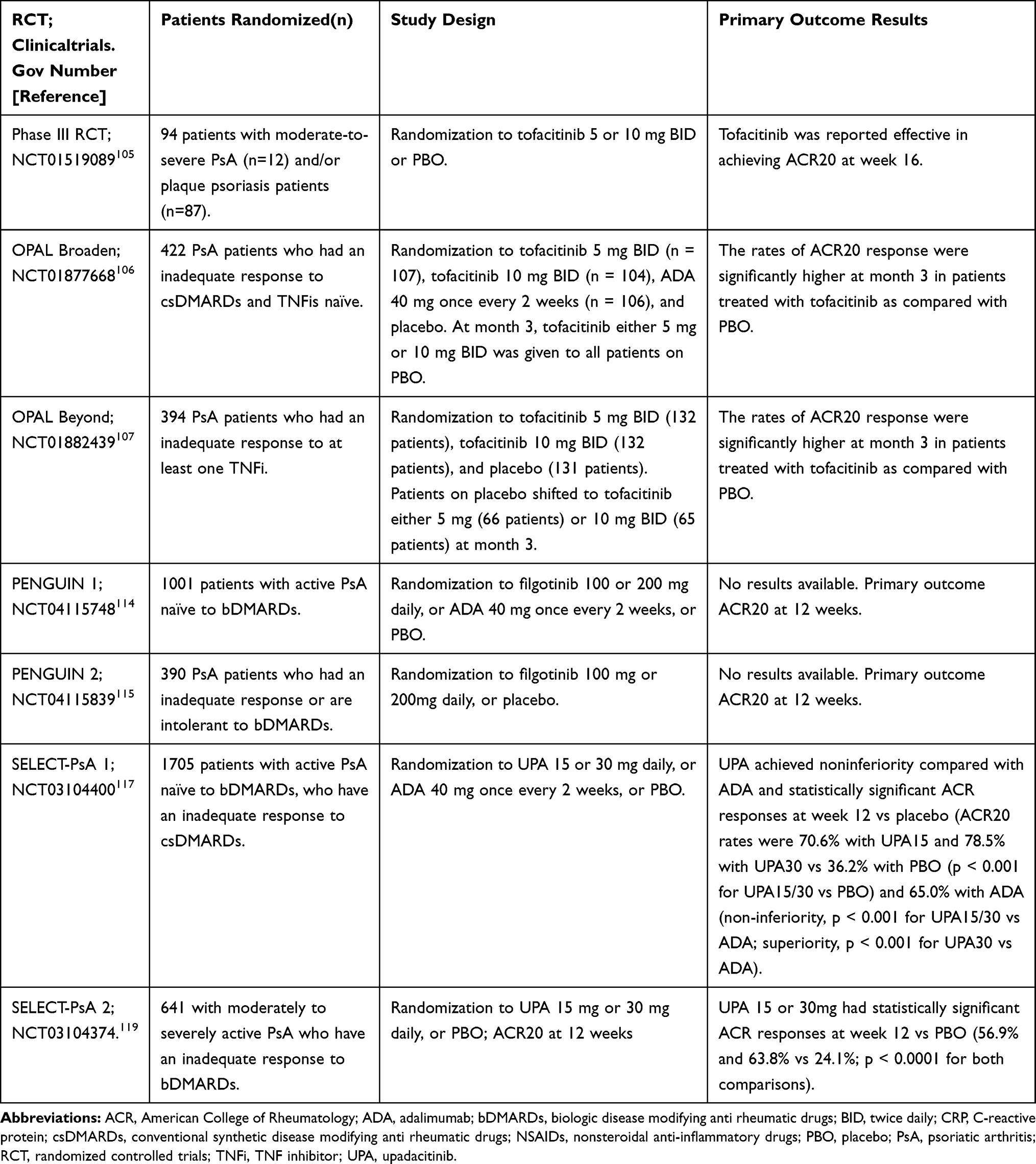 |
Table 4 Main Data Derived from Phase III Randomized Controlled Trials of JAK Inhibitors Under Investigation in Psoriatic Arthritis |
Other Investigational Molecules
Recently, the kinase mammalian target of rapamycin (mTOR), which is regulated by several growth factors (such as nerve growth factor (NGF) and platelet-derived growth factor (PDGF)) and cytokines (IL-17 and IL-22) has emerged as a key contributor in the control of psoriatic epidermal and synovial homeostasis.80,124–127
The inhibition of mTOR signaling pathway by blocking the upstream dual kinases of the signaling pathway, protein kinase B (AKT) or phosphatidylinositol 3-kinase (PI3K), has been suggested as a potential therapy for PsD.80,124–127
Furthermore, the nuclear receptor retinoic acid receptor-related orphan receptor gamma (RORγ or RORc) is a key transcription factor for the pro-inflammatory cytokines’ synthesis, including IL-17.128,129
A RORγt inhibitor, VTP-43742, is currently under investigation in a Phase II trial for psoriasis and seems a promising therapeutic strategy for psoriasis and PsA.130
The Gi protein-associated receptor A3 adenosine receptor (A3AR), over-expressed in inflammatory cells and involved in the regulation of mitogen-activated protein kinase (MAPK) pathways, represents a potential therapeutic target for the treatment of PsA.131
In particular, CF101, a selective agonist with high affinity to the A3AR, has been found to be safe and well-tolerated in all preclinical and human clinical studies and showed promising results in PsO and RA.132–134 Potassium (K+) channel voltage channel inhibitors seem to represent another potential therapy with promising effects for PsA.80 These molecules inhibit K + channels which are overexpressed in psoriatic skin and synovium and induce lymphocytes proliferation and activation.135 Several K+ channels inhibitors such as the Kv1.3 inhibitor, PAP-1 are under investigation in PsD.135–137
Conclusion
In PsA, innate and acquired immune mechanisms contribute to a complex pathogenesis and multifaceted phenotype.
In the last two decades, a deeper knowledge of pathogenic mechanisms of the disease have been pivotal for addressing tailored therapeutic strategies, allowing the introduction of bDMARDs, at first anti-TNF-α agents, and more recently, of APR, IL12/23is, and IL-17is.
Of note, recent improvements in the understanding of IL-17 pathway enabled the development of additional inhibitors, such as BRO63,72–75 and BMK,76–78 currently approved for psoriasis and showing promising results in Phase II and III RCTs.
It should be also mentioned the key role of the overexpression of IL-23 and IL-23-induced Th17 cytokines (IL-17 and IL-22) in the pathogenesis of psoriatic plaque, synovitis, joint erosion, enthesitis and new bone formation. Therefore, IL-23 inhibition represents a further promising strategy for the treatment of PsA. Currently, three antibodies blocking the p19 subunit of IL-23, GSK, TIL and RSK, approved for moderate to severe plaque psoriasis, are now under investigation in phase II/III PsA RCTs.63,64,79,80
The advent of therapeutic agents neutralizing more than one cytokine (TNF-α and IL-17), such as ABT-122 (Remtolumab), seems somewhat promising because of their ability of contemporaneous blocking multiple pathogenic pathways. However, studies on dual cytokines’ neutralization remain still scarce.79
Of note, ongoing research is focusing on JAKis (tofacitinib, filgotinib and upadacitinib), which are able to block different pathogenic pathways, are further enriching the opportunities to treat PsA. 105–106,113,117,119
JAKis have shown an acceptable safety profile and efficacy with a fast onset of action in PsA clinical trials, improving PsA symptoms, PROs and QoL. Furthermore, their oral administration seems to lead to a better therapeutic compliance as compared to SC and intravenous bDMARDs.105,106,113,117,119 More recently, new targets represented by A3AR, mTOR, RORγt, and K+ channel voltage channels are emerging, but further studies are needed for clarifying the efficacy and safety of these agents in PsA.80 In the near future, further studies on less-explored cytokines and intracellular pathways could lead to the expansion of PsA therapeutic armamentarium, with an increased possibility of a more tailored and personalized therapy. Moreover, in the next few years, a greater attention on the different domains of PsA beyond peripheral arthritis should be paid in clinical trials. However, although preliminary Phase II and III trials results are promising, further studies are required to better characterize the efficacy and safety profile of these therapeutic agents in PsA treatment.
Funding
No funding supported the paper.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chimenti MS, Caso F, Alivernini S, et al. Amplifying the concept of psoriatic arthritis: the role of autoimmunity in systemic psoriatic disease. Autoimmun Rev. 2019;18(6):565–575. doi:10.1016/j.autrev.2018.11.007
2. Scarpa R, Caso F, Costa L, et al. Psoriatic disease: clinical staging. J Rheumatol. 2015;93:24–26.
3. Chimenti MS, Perricone C, Novelli L, et al. Interaction between microbiome and host genetics in psoriatic arthritis. Autoimmun Rev. 2018;17:276–283.
4. Lambert JR, Wright V. Eye inflammation in psoriatic arthritis. Ann Rheum Dis. 1976;35:354–356.
5. Chimenti MS, Triggianese P, Salandri G, et al. A Multimodal Eye Assessment in Psoriatic Arthritis Patients sine Psoriasis: evidence for a Potential Association with Systemic Inflammation. J Clin Med. 2020;9:719.
6. Navarini L, Sperti M, Currado D, et al. A machine-learning approach to cardiovascular risk prediction in psoriatic arthritis. Rheumatology. 2020;59:1767–1769.
7. Navarini L, Margiotta DPE, Costa L, et al. Performance and calibration of the algorithm ASSIGN in predicting cardiovascular disease in Italian patients with psoriatic arthritis. Clin Rheumatol. 2019;38:971–976.
8. Navarini L, Margiotta DPE, Caso F, et al. Performances of five risk algorithms in predicting cardiovascular events in patients with Psoriatic Arthritis: an Italian bicentric study. PLoS One. 2018;13:10.
9. Costa L, Caso F, D’Elia L, et al. Psoriatic arthritis is associated with increased arterial stiffness in the absence of known cardiovascular risk factors: a case control study. Clin Rheumatol. 2012;31:711–715.
10. Caso F, Navarini L, Carubbi F, et al. Mediterranean diet and Psoriatic Arthritis activity: a multicenter cross-sectional study. Rheumatol Int. 2020;40(6):951–958. doi:10.1007/s00296-019-04458-7
11. Costa L, Caso F, Ramonda R, et al. Metabolic syndrome and its relationship with the achievement of minimal disease activity state in psoriatic arthritis patients: an observational study. Immunol Res. 2014;61:147–153. doi:10.1007/s12026-014-8595-z
12. Caso F, Chimenti MS, Navarini L, et al. Metabolic Syndrome and psoriatic arthritis: considerations for the clinician. Expert Rev Clin Immunol. 2020;16(4):409–420. doi:10.1080/1744666X.2020.1740593
13. Caso F, Del Puente A, Oliviero F, et al. Metabolic Syndrome in Psoriatic Arthritis: The Interplay with Cutaneous Involvement. Evidences from Literature and a Recent Cross-Sectional Study. Vol. 37. Springer London: Clinical Rheumatology; 2018:579–586.
14. Caso F, Costa L, Chimenti MS, Navarini L, Punzi L. Pathogenesis of Psoriatic Arthritis. Crit Rev Immunol. 2019;39:361–377.
15. Caso F, Costa L, Nucera V, et al. From Autoinflammation to Autoimmunity: Old and Recent Findings. Vol. 37. Springer London: Clinical Rheumatology; 2018:2305–2321.
16. Moll JMH, Wright V. Psoriatic arthritis. Semin Arthritis Rheum. 1973;3(1):55–78.
17. Scarpa R, Caso F, Costa L, et al. Psoriatic Disease 10 Years Later. J Rheumatol. 2017;44(9):1298–1301.
18. Caso F, Costa L, Peluso R, Del Puente A, Scarpa R. Psoriatic Arthritis. In: Mosaic of Autoimmunity. Academic Press; 2019:527–540.
19. Kehl AS, Corr M, Weisman MH. Review: enthesitis: new Insights Into Pathogenesis, Diagnostic Modalities, and Treatment. Arthritis Rheumatol. 2016;68(2):312–322.
20. Rossini M, Epis OM, Tinazzi I, et al. Role of the IL-23 pathway in the pathogenesis and treatment of enthesitis in psoriatic arthritis.Expert. Opin Biol Ther. 2020;20(7):787–798.
21. Kaeley GS, Eder L, Aydin SZ, Gutierrez M, Bakewell C. Dactylitis: A hallmark of psoriatic arthritis. Semin Arthritis Rheum. 2018;48(2):263–273.
22. Girolimetto N, Costa L, Mancarella L, et al. Symptomatic psoriatic dactylitis is associated with ultrasound determined extra-synovial inflammatory features and shorter disease duration. Clin Rheumatol. 2019;38(3):903–911.
23. Girolimetto N, MacChioni P, Tinazzi I, et al. Ultrasonographic evidence of predominance of acute extracapsular and chronic intrasynovial patterns in 100 cases of psoriatic hand dactylitis. J Rheumatol. 2020;47:227–233.
24. Brockbank JE, Stein M, Schentag CT, Gladman DD. Dactylitis in psoriatic arthritis: A marker for disease severity? Ann Rheum Dis. 2005;64:188–190.
25. Napolitano M, Caso F, Scarpa R, et al. Psoriatic arthritis and psoriasis: differential diagnosis. Clin Rheumatol. 2016;35(8):1893–1901.
26. Soscia E, Scarpa R, Cimmino MA, et al. Magnetic resonance imaging of nail unit in psoriatic arthritis. J Rheumatol Suppl. 2009;83:42–45.
27. Soscia E, Sirignano C, Catalano O, et al. New developments in magnetic resonance imaging of the nail unit. J Rheumatt Alol Suppl. 2012;89:49–53.
28. Gladman DD, Antoni C, Mease P, Clegg DO, Nash P. Psoriatic arthritis: epidemiology, clinical features, course, and outcome. Ann Rheum Dis. 2005;64:ii14–7.
29. Ficjan A, Husic R, Gretler J, et al. Ultrasound composite scores for the assessment of inflammatory and structural pathologies in Psoriatic Arthritis (PsASon-Score). Arthritis Res Ther. 2014;16:1.
30. Tan AL, Fukuba E, Halliday NA, et al. High-resolution MRI assessment of Dactylitis in psoriatic arthritis shows flexor tendon pulley and sheath-related enthesitis. Ann Rheum Dis. 2015;74(1):185–189.
31. D’Agostino MA, Aegerter P, Bechara K, et al. How to diagnose spondyloarthritis early? Accuracy of peripheral enthesitis detection by power Doppler ultrasonography. Ann Rheum Dis. 2011;70(8):1433–1440.
32. Sudoł-Szopińska I, Pracoń G. Diagnostic imaging of psoriatic arthritis. Part II: magnetic resonance imaging and ultrasonography. J Ultrason. 2016;16(65):163–174.
33. Wiell C, Szkudlarek M, Hasselquist M, et al. Ultrasonography, magnetic resonance imaging, radiography, and clinical assessment of inflammatory and destructive changes in fingers and toes of patients with psoriatic arthritis. Arthritis Res Ther. 2007;9(6):R119.
34. Giacomelli R, Afeltra A, Alunno A, et al. Guidelines for biomarkers in autoimmune rheumatic diseases - evidence based analysis. Autoimmun Rev. 2019;18(1):93–106.
35. Caso F, Costa L, Atteno M, et al. Simple clinical indicators for early psoriatic arthritis detection. Springerplus. 2014;3:1–3.
36. Tillett W, Costa L, Jadon D, et al. The ClASsification for Psoriatic ARthritis (CASPAR) criteria - A retrospective feasibility, sensitivity, and specificity study. J Rheumatol. 2012;39(1):154–156.
37. Caso F, Tasso M, Chimenti MS, et al. Late-Onset and Elderly Psoriatic Arthritis: clinical Aspects and Management. Drugs Aging. 2019;36(10):909–925.
38. Tucker LJ, Coates LC, Helliwell PS. Assessing Disease Activity in Psoriatic Arthritis: A Literature Review. Rheumatol Ther. 2019;6(1):23–32.
39. Mease PJ. Measures of psoriatic arthritis: tender and Swollen Joint Assessment, Psoriasis Area and Severity Index (PASI), Nail Psoriasis Severity Index (NAPSI), Modified Nail Psoriasis Severity Index (mNAPSI), Mander/Newcastle Enthesitis Index (MEI), Leeds Enthesitis Index (LEI), Spondyloarthritis Research Consortium of Canada (SPARCC), Maastricht Ankylosing Spondylitis Enthesis Score (MASES), Leeds Dactylitis Index (LDI), Patient Global for Psoriatic Arthritis, Dermatology Life Quality Index (DLQI), Psoriatic Arthritis Quality of Life (PsAQOL), Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F), Psoriatic Arthritis Response Criteria (PsARC), Psoriatic Arthritis Joint Activity Index (PsAJAI), Disease Activity in Psoriatic Arthritis (DAPSA), and Composite Psoriatic Disease Activity Index (CPDAI). Arthritis Care Res (Hoboken). 2011;63:S64–85.
40. Scarpa R, Spondyloarthritis: CF. Which composite measures to use in psoriatic arthritis? Nat Rev Rheumatol. 2018;14(3):125–126.
41. Ritchlin CT, Colbert RA, Gladman DD. Psoriatic Arthritis. N Engl J Med. 2017;376(10):957–970.
42. Helliwell PS, Deodhar A, Gottlieb AB, et al. Composite Measures of Disease Activity in Psoriatic Arthritis: comparative Instrument Performance Based on the Efficacy of Guselkumab in an Interventional Phase 2 Trial. Arthritis Care Res (Hoboken). 2019. doi:10.1002/acr.24046
43. Coates LC, Kavanaugh A, Mease PJ, et al. Group for Research and Assessment of Psoriasis and Psoriatic Arthritis 2015 Treatment Recommendations for Psoriatic Arthritis. Arthritis Rheumatol. 2016;68(5):1060–1071.
44. Gossec L, Baraliakos X, Kerschbaumer A, et al. EULAR recommendations for the management of psoriatic arthritis with pharmacological therapies: 2019 update. Ann Rheum Dis. 2020;79(6):700–712.
45. Singh JA, Guyatt G, Ogdie A, et al. Special Article: 2018 American College of Rheumatology/National Psoriasis Foundation Guideline for the Treatment of Psoriatic Arthritis. Arthritis Care Res. 2019;71(1):2–29.
46. Scarpa R, Costa L, Atteno M, Caso F, Lubrano E. Treatment Options: NSAIDs and DMARDs. In: Advances in the Management of Psoriatic Arthritis. 2013:63–70.
47. Atzeni F, Caso F, Costa L, Sarzi-Puttini P, Masala IF. Conventional and biological DMARDs in systemic rheumatic diseases: perioperative risk/benefit management. Handbook of systemic autoimmune diseases. Surg Rheumatic Musculoskeletal Dis. 2018;161–182.
48. Caso F, Costa L, Del Puente A, et al. Pharmacological treatment of spondyloarthritis: exploring the effectiveness of nonsteroidal anti-inflammatory drugs, traditional disease-modifying antirheumatic drugs and biological therapies. Ther Adv Chronic Dis. 2015;6:328–338.
49. Caso F, Lubrano E, Del Puente A, et al. Progress in understanding and utilizing TNF-α inhibition for the treatment of psoriatic arthritis. Expert Rev Clin Immunol. 2016;12(3):315–331.
50. D’Angelo S, Cantini F, Ramonda R, et al. Effectiveness of Adalimumab for the Treatment of Psoriatic Arthritis: an Italian Real-Life Retrospective Study. Front Pharmacol. 2019;10:1497.
51. Megna M, Balato A, Napolitano M, et al. Psoriatic disease treatment nowadays: unmet needs among the “jungle of biologic drugs and small molecules”. Clin Rheumatol. 2018;37(7):1739–1741.
52. Scarpa R, Costa L, Atteno M, et al. Psoriatic arthritis: advances in pharmacotherapy based on molecular target. Expert Opin Pharmacother. 2013;14(17):2311–2313.
53. Caso F, Del Puente A, Peluso R, et al. Emerging drugs for psoriatic arthritis. Expert Opin Emerg Drugs. 2016;21(1):69–79.
54. Costa L, Caso F, Del Puente A, Di Minno MND, Peluso R, Scarpa R. Incidence of malignancies in a cohort of psoriatic arthritis patients taking traditional disease modifying antirheumatic drug and tumor necrosis factor inhibitor therapy: an observational study. J Rheumatol. 2016;43(12):2149–2154.
55. Atteno M, Costa L, Matarese A, et al. The use of TNF-α blockers in psoriatic arthritis patients with latent tuberculosis infection. Clin Rheumatol. 2014;33(4):543–547.
56. Caso F, Cantarini L, Morisco F, et al. Current evidence in the field of the management with TNF-α inhibitors in psoriatic arthritis and concomitant hepatitis C virus infection. Expert Opin Biol Ther. 2015;15(5):641–650.
57. Costa L, Caso F, Atteno M, et al. Long-term safety of anti-TNF-α in PsA patients with concomitant HCV infection: a retrospective observational multicenter study on 15 patients. Clin Rheumatol. 2014;33(2):273–276.
58. Caso F, Costa L, Del Puente A, Scarpa R. Psoriatic arthritis and TNF inhibitors: advances on effectiveness and toxicity. Expert Opin Biol Ther. 2015;15(1):1–2.
59. Costa L, Perricone C, Chimenti MS, et al. Switching Between Biological Treatments in Psoriatic Arthritis: A Review of the Evidence. Drugs R D. 2017;17(4):509–522.
60. Chimenti MS, Ortolan A, Lorenzin M, et al. Effectiveness and safety of ustekinumab in naïve or TNF-inhibitors failure psoriatic arthritis patients: a 24-month prospective multicentric study. Clin Rheumatol. 2018;37(2):397–405.
61. Navarini L, Costa L, Tasso M, et al. Retention rates and identification of factors associated with anti-TNFα, anti-IL17, and anti-IL12/23R agents discontinuation in psoriatic arthritis patients: results from a real-world clinical setting. Clin Rheumatol. 2020;39(9):2663–2670.
62. Chimenti MS, Triggianese P, De Martino E, et al. An update on pathogenesis of psoriatic arthritis and potential therapeutic targets. Expert Rev Clin Immunol. 2019;15(8):823–836.
63. Sakkas LI, Zafiriou E, Bogdanos DP. Mini Review: new Treatments in Psoriatic Arthritis. Focus on the IL-23/17 Axis. Front Pharmacol. 2019;10:872.
64. Maguire S, Sengupta R, The OF. Future of Axial Spondyloathritis Treatment. Rheum Dis Clin North Am. 2020;46(2):357–365.
65. Coates LC, Mease PJ, Gossec L, et al. Minimal Disease Activity Among Active Psoriatic Arthritis Patients Treated With Secukinumab: 2-Year Results From a Multicenter, Randomized, Double-Blind, Parallel-Group, Placebo-Controlled Phase III Study. Arthritis Care Res (Hoboken). 2018;70(10):1529–1535.
66. McInnes IB, Mease PJ, Ritchlin CT, et al. Secukinumab sustains improvement in signs and symptoms of psoriatic arthritis: 2 year results from the phase 3 FUTURE 2 study. Rheumatology. 2017;56(11):1993–2003.
67. Mease P, van der Heijde D, Landewé R, et al. Secukinumab improves active psoriatic arthritis symptoms and inhibits radiographic progression: primary results from the randomised, double-blind, phase III FUTURE 5 study. Ann Rheum Dis. 2018;77(6):890–897.
68. Nash P, Mease PJ, McInnes IB, et al. FUTURE 3 study group. Efficacy and safety of secukinumab administration by autoinjector in patients with psoriatic arthritis: results from a randomized, placebo-controlled trial (FUTURE 3). Arthritis Res Ther. 2018;20(1):47.
69. Mease PJ, Smolen JS, Behrens F, et al. SPIRIT H2H study group. A head-to-head comparison of the efficacy and safety of ixekizumab and adalimumab in biological-naïve patients with active psoriatic arthritis: 24-week results of a randomised, open-label, blinded-assessor trial. Ann Rheum Dis. 2020;79(1):123–131.
70. Gottlieb AB, Strand V, Kishimoto M, et al. Ixekizumab improves patient-reported outcomes up to 52 weeks in bDMARD-naïve patients with active psoriatic arthritis (SPIRIT-P1). Rheumatology. 2018;57(10):1777–1788.
71. van der Heijde D, Gladman DD, Kishimoto M, et al. Efficacy and Safety of Ixekizumab in Patients with Active Psoriatic Arthritis: 52-week Results from a Phase III Study (SPIRIT-P1). J Rheumatol. 2018;45(3):367–377.
72. Mease PJ, Genovese MC, Greenwald MW, et al. Brodalumab, an anti-IL17RA monoclonal antibody, in psoriatic arthritis. N Engl J Med. 2014;370(24):2295–2306.
73. ClinicalTrials.gov. Identifier: NCT02024646
74. ClinicalTrials.gov. Identifier: NCT02029495
75. Brodalumab in psoriatic arthritis (PsA). 24-week results from the phase III AMVISON-1 and −2 trials. J Am Acad Dermatol. 2019;81(4):AB28.
76. Ritchlin CT, Kavanaugh A, Merola JF, et al. Bimekizumab in patients with active psoriatic arthritis: results from a 48-week, randomised, double-blind, placebo-controlled, dose-ranging phase 2b trial. Lancet. 2020;395(10222):427–440.
77. ClinicalTrials.gov. Identifier: NCT03896581
78. ClinicalTrials.gov. Identifier: NCT03895203
79. Mease PJ, Genovese MC, Weinblatt ME, et al. Phase II Study of ABT-122, a Tumor Necrosis Factor- and Interleukin-17A-Targeted Dual Variable Domain Immunoglobulin, in Patients With Psoriatic Arthritis With an Inadequate Response to Methotrexate. Arthritis Rheumatol. 2018;70(11):1778–1789.
80. Toussi A, Maverakis N, Le ST, et al. Updated therapies for the management of psoriatic arthritis. Clin Immunol. 2020;108536.
81. Deodhar A, Gottlieb AB, Boehncke WH, et al. Efficacy and safety of Guselkumab in patients with active psoriatic arthritis: a randomised, double-blind, placebo-controlled, phase 2 study. Lancet. 2018;391(10136):2213–2224.
82. Deodhar A, Helliwell PS, Boehncke WH, et al. Guselkumab in patients with active psoriatic arthritis who were biologic-naive or had previously received TNFα inhibitor treatment (DISCOVER-1): a double-blind, randomised, placebo-controlled phase 3 trial. Lancet. 2020;395(10230):1115–1125.
83. Mease PJ, Rahman P, Gottlieb AB, et al. Guselkumab in biologic-naive patients with active psoriatic arthritis (DISCOVER-2): a double-blind, randomised, placebo-controlled phase 3 trial. Lancet. 2020;395(10230):1126–1136.
84. ClinicalTrials.gov. Identifier: NCT03796858
85. ClinicalTrials.gov. Identifier: NCT02980692
86. ClinicalTrials.gov. Identifier: NCT04314531
87. ClinicalTrials.gov. Identifier: NCT04314544
88. ClinicalTrials.gov. Identifier: NCT03675308
89. ClinicalTrials.gov. Identifier: NCT03671148
90. Mease PJ, Kellner H, Morita A, et al. OP0307 Efficacy and safety of Risankizumab, a selective il-23p19 inhibitor, in patients with active psoriatic arthritis over 24 weeks: results from a phase 2 trial. Ann Rheum Dis. 2018;77(2):200–201.
91. Fiocco U, Martini V, Accordi B, et al. Ex Vivo Signaling Protein Mapping in T Lymphocytes in the Psoriatic Arthritis Joints. J Rheumatol Suppl. 2015;93:48–52.
92. Fiocco U, Martini V, Accordi B, et al. Transcriptional network profile on synovial fluid T cells in psoriatic arthritis. Clin Rheumatol. 2015;34(9):1571–1580.
93. Fiocco U, Accordi B, Martini V, et al. JAK/STAT/PKCδ molecular pathways in synovial fluid T lymphocytes reflect the in vivo T helper-17 expansion in psoriatic arthritis. Immunol Res. 2014;58(1):61–69.
94. Gao W, McGarry T, Orr C, et al. Tofacitinib regulates synovial inflammation in psoriatic arthritis, inhibiting STAT activation and induction of negative feedback inhibitors. Ann Rheum Dis. 2016;75:311–315.
95. Hodge JA, Kawabata TT, Krishnaswami S, et al. The mechanism of action of tofacitinib - an oral Janus kinase inhibitor for the treatment of rheumatoid arthritis. Clin Exp Rheumatol. 2016;34(2):318–328.
96. Berekmeri A, Mahmood F, Wittmann M, Helliwell P. Tofacitinib for the treatment of psoriasis and psoriatic arthritis. Expert Rev Clin Immunol. 2018;14(9):719–730.
97. Chimenti MS, Perricone C, Conigliaro P, et al. Tackling the autoimmune side in Spondyloarthritis: A systematic review. Autoimmun Rev. 2020:102648. doi:10.1016/j.autrev.2020.102648
98. Caso F, Navarini L, Ruscitti P, et al. Targeted synthetic pharmacotherapy for psoriatic arthritis: state of the art. Expert Opin Pharmacother. 2020;21(7):785–796.
99. Costa L, Del Puente A, Peluso R, et al. Small molecule therapy for managing moderate to severe psoriatic arthritis. Expert Opin Pharmacother. 2017;18(15):1557–1567.
100. Chiricozzi A, Saraceno R, Novelli L, et al. Small molecules and antibodies for the treatment of psoriasis: a patent review (2010-2015). Expert Opin Ther Pat. 2016;26(7):757–766. doi:10.1080/13543776.2016.1192129
101. Chimenti MS, D’Antonio A, Conigliaro P, et al. An Update for the Clinician on Biologics for the Treatment of Psoriatic Arthritis. Biologics. 2020;14:53–75.
102. Paik J, Deeks ED. Tofacitinib: A Review in Psoriatic Arthritis. Drugs. 2019;79(6):655–663. doi:10.1007/s40265-019-01091-3
103. Jamilloux Y, El Jammal T, Vuitton L, et al. JAK inhibitors for the treatment of autoimmune and inflammatory diseases. Autoimmun Rev. 2019;18(11):102390. doi:10.1016/j.autrev.2019.102390
104. Song GG, Lee YH. Comparison of the Efficacy and Safety of Tofacitinib and Apremilast in Patients with Active Psoriatic Arthritis: A Bayesian Network Meta-Analysis of Randomized Controlled Trials. Clin Drug Investig. 2019;39(5):421–428. doi:10.1007/s40261-019-00765-w
105. Asahina A, Etoh T, Igarashi A, et al. Oral tofacitinib efficacy, safety and tolerability in Japanese patients with moderate to severe plaque psoriasis and psoriatic arthritis: A randomized, double-blind, phase 3 study. J Dermatol. 2016;43(8):869–880. doi:10.1111/1346-8138.13258
106. Mease P, Hall S, FitzGerald O, et al. Tofacitinib or adalimumab versus placebo for psoriatic arthritis. N Engl J Med. 2017;377(16):1537–1550. doi:10.1056/NEJMoa1615975
107. Gladman D, Rigby W, Azevedo VF, et al. Tofacitinib for psoriatic arthritis in patients with an inadequate response to TNF inhibitors. N Engl J Med. 2017;377(16):1525–1536. doi:10.1056/NEJMoa1615977
108. Nash P, Coates LC, Fleischmann R, et al. Efficacy of Tofacitinib for the Treatment of Psoriatic Arthritis: pooled Analysis of Two Phase 3 Studies. Rheumatol Ther. 2018;5(2):567–582. doi:10.1007/s40744-018-0131-5
109. Strand V, De Vlam K, Covarrubias-Cobos JA, et al. Effect of tofacitinib on patient-reported outcomes in patients with active psoriatic arthritis and an inadequate response to tumour necrosis factor inhibitors in the Phase III, randomised controlled trial: OPAL beyond. RMD Open. 2019;5:1.
110. Strand V, De Vlam K, Covarrubias-Cobos JA, et al. Tofacitinib or adalimumab versus placebo: patient-reported outcomes from OPAL Broaden – A phase III study of active psoriatic arthritis in patients with an inadequate response to conventional synthetic disease-modifying antirheumatic drugs. RMD Open. 2019;5:1.
111. Van Der Heijde D, Gladman DD, FitzGerald O, et al. Radiographic progression according to baseline C-reactive protein levels and other risk factors in psoriatic arthritis treated with tofacitinib or adalimumab. J Rheumatol. 2019;46(9):1089–1096. doi:10.3899/jrheum.180971
112. Nash P, Coates LC, Kivitz AJ, et al. Safety and Efficacy of Tofacitinib in Patients with Active Psoriatic Arthritis: interim Analysis of OPAL Balance, an Open-Label, Long-Term Extension Study. Rheumatol Ther. 2020;7(3):553–580. doi:10.1007/s40744-020-00209-4
113. Mease P, Coates LC, Helliwell PS, et al. Efficacy and safety of filgotinib, a selective Janus kinase 1 inhibitor, in patients with active psoriatic arthritis (EQUATOR): results from a randomised, placebo-controlled, phase 2 trial. Lancet. 2018;392(10162):2367–2377. doi:10.1016/S0140-6736(18)32483-8
114. ClinicalTrials.gov. Identifier: NCT04115748
115. ClinicalTrials.gov. Identifier: NCT04115839
116. ClinicalTrials.gov. Identifier: NCT03104400.
117. Mcinnes I, Anderson J, Magrey M, et al. Efficacy and safety of upadacitinib versus placebo and adalimumab in patients with active psoriatic arthritis and inadequate response to non-biologic disease-modifying anti-rheumatic drugs (SELECT-PSA-1): a double-blind, randomized controlled phase 3 trial. Ann Rheum Dis. 2020;79(1):12–13.
118. ClinicalTrials.gov. Identifier: NCT03104374
119. Genovese MC, Lertratanakul A, Anderson J, et al. Efficacy and safety of upadacitinib in patients with active psoriatic arthritis and inadequate response to biologic disease-modifying anti-rheumatic drugs (SELECT-PSA-2): a double-blind, randomized controlled phase 3 trial. Ann Rheum Dis Ann Rheum Dis. 2020;79(1):139.
120. Burke JR, Cheng L, Gillooly KM, et al. Autoimmune pathways in mice and humans are blocked by pharmacological stabilization of the TYK2 pseudokinase domain. Sci Transl Med. 2019;11(502):eaaw1736. doi:10.1126/scitranslmed.aaw1736
121. Velazquez L, Fellous M, Stark GR, et al. A protein tyrosine kinase in the interferon alpha/beta signaling pathway. Cell. 1992;70(2):313–322. doi:10.1016/0092-8674(92)90105-L
122. Karaghiosoff M, Steinborn R, Kovarik P, et al. Central role for type I interferons and Tyk2 in lipopolysaccharide-induced endotoxin shock. Nat Immunol. 2003;4(5):471–477. doi:10.1038/ni910
123. ClinicalTrials.gov. Identifier: NCT03881059
124. Buerger C. Epidermal mTORC1 Signaling Contributes to the Pathogenesis of Psoriasis and Could Serve as a Therapeutic Target. Front Immunol. 2018;9:2786. doi:10.3389/fimmu.2018.02786
125. Reitamo S, Spuls P, Sassolas B, et al. Griffiths CE Sirolimus European Psoriasis Study Group. Efficacy of sirolimus (rapamycin) administered concomitantly with a subtherapeutic dose of cyclosporin in the treatment of severe psoriasis: A randomized controlled trial. Br J Dermatol. 2001;145(3):438–445. doi:10.1046/j.1365-2133.2001.04376.x
126. Buerger C, Malisiewicz B, Eiser A, Hardt K, Boehncke WH. Mammalian target of rapamycin and its downstream signalling components are activated in psoriatic skin. Br J Dermatol. 2013;169(1):156–159. doi:10.1111/bjd.12271
127. Raychaudhuri SK, Raychaudhuri SP. mTOR Signaling Cascade in Psoriatic Disease: double Kinase mTOR Inhibitor a Novel Therapeutic Target. Indian J Dermatol. 2014;59(1):67–70.
128. Pandya VB, Kumar S, Sachchidanand SR, Sharma RC, Desai RC. Combating Autoimmune Diseases With Retinoic Acid Receptor-Related Orphan Receptor-γ (RORγ or RORc) Inhibitors: hits and Misses. J Med Chem. 2018;61(24):10976–10995. doi:10.1021/acs.jmedchem.8b00588
129. Guendisch U, Weiss J, Ecoeur F, et al. Pharmacological inhibition of RORγt suppresses the Th17 pathway and alleviates arthritis in vivo. PLoS One. 2017;12(11):e0188391. doi:10.1371/journal.pone.0188391
130. Gege C. RORγt inhibitors as potential back-ups for the phase II candidate VTP-43742 from Vitae Pharmaceuticals: patent evaluation of WO2016061160 and US20160122345. Expert Opin Ther Pat. 2017;27(1):1–8. doi:10.1080/13543776.2017.1262350
131. Jacobson KA, Merighi S, Varani K, et al. A3 adenosine receptors as modulators of inflammation: from medicinal chemistry to therapy. Med Res Rev. 2018;38(4):1031–1072.
132. David M, Gospodinov DK, Gheorghe N, et al. Treatment of plaque-type psoriasis with oral CF101: data from a phase II/III multicenter, randomized, controlled trial. J Drugs Dermatol. 2016;15:931–938.
133. Silverman MH, Strand V, Markovits D, et al. Clinical evidence for utilization of the A3 adenosine receptor as a target to treat rheumatoid arthritis: data from a phase II clinical trial. J Rheumatol. 2008;35(1):41–48.172.
134. van Troostenburg AR, Clark EV, Carey WD, et al. Tolerability, pharmacokinetics and concentration-dependent hemodynamic effects of oral CF101, an A3 adenosine receptor agonist, in healthy young men. Int J Clin Pharmacol Ther. 2004;42(10):534–542.
135. Kundu-Raychaudhuri S, Chen YJ, Wulff H, Raychaudhuri SP. Kv1.3 in Psoriatic Disease: PAP-1, a small molecule inhibitor of Kv1.3 is effective in the SCID mouse psoriasis – xenograft model. J Autoimmun. 2014;55:63–72.
136. Feske S, Wulff H, Skolnik EY. Ion channels in innate and adaptive immunity. Annu Rev Immunol. 2015;33:291–353.
137. Toussirot E. New treatment options and emerging drugs for axial spondyloarthritis: biological and targeted synthetic agents. Expert Opin Pharmacother. 2017;18:275–282.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.