Back to Journals » Patient Preference and Adherence » Volume 19
Experiences of Immunoglobulin Therapy for Those with a Confirmed Diagnosis of Chronic Inflammatory Demyelinating Polyneuropathy: A Mixed-Methods Study with a Qualitative Patient Perspective Focus
Authors Hubsch A ![]() , Cashmore SJ
, Cashmore SJ ![]() , Mallick R, Gibbons B
, Mallick R, Gibbons B
Received 24 July 2025
Accepted for publication 1 December 2025
Published 12 December 2025 Volume 2025:19 Pages 3999—4019
DOI https://doi.org/10.2147/PPA.S543188
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Alphonse Hubsch,1 Sarah-Jane Cashmore,2 Rajiv Mallick,3 Ben Gibbons2
1CSL Behring, Bern, Switzerland; 2Bryter Inc., New York, NY, USA; 3Risk Sharing Solutions, Phoenixville, PA, USA
Correspondence: Sarah-Jane Cashmore, Bryter Inc., 433 Broadway, New York, NY, 10013, USA, Email [email protected]
Introduction: This survey aimed to characterize the patient experience with disease and immunoglobulin (Ig) treatment including quality-of-life in those with a neurologist-confirmed diagnosis of Chronic Inflammatory Demyelinating Polyneuropathy (CIDP).
Methods: CIDP patients (n=42) from the United States (n=31) and Europe (n=11) with Ig treatment experience completed an online 20-minute questionnaire, followed by virtual 60-minute in-depth interviews. Interviews were recorded, transcribed verbatim, and analyzed using NVIVO 12 qualitative data analysis software.
Results: Patients reported substantial delays between initial symptoms and CIDP diagnosis (median 2 years, range 0– 15 years), and a profound impact of disease across physical, social, and psychological domains. Physical impact included inability to perform everyday tasks such as household chores and need to utilize assistive devices (eg walkers, wheelchairs). Patients reported substantially reduced social and leisure activities, and associated emotional impact due to social isolation and loss of independence, especially loss of driving ability. The majority retired and/or went on disability within a year of CIDP diagnosis. Notwithstanding some delays in initiating Ig treatment, both Intravenous Immunoglobulin (IVIG) and Subcutaneous Immunoglobulin (SCIG) were generally perceived as highly effective with 69% of patients reporting vast improvements in physical function, including renewed strength, restored ability to walk and perform everyday tasks, and reduced pain. SCIG patients (24%) expressed a preference for SCIG due to its ease of use and minimal disruption to daily life. Overall, 36% of patients reported their physicians ceased their Ig therapy, reduced dose or dosing frequency upon CIDP symptom improvement, with 33% of those patients subsequently worsening, but recovering upon returning to the original dose. Patients expressed a desire for continuing Ig treatment due to fear of disrupting its benefits.
Conclusion: Patients reported substantial impact of CIDP across physical, social, emotional and employment-related domains. Patients reported being highly satisfied with Ig therapy and committed to continuing treatment.
Keywords: SCIG, IVIG, infusion burden, immunoglobulin therapy, Ig, quality of life
Introduction
Chronic inflammatory demyelinating polyneuropathy (CIDP) is the most common chronic immune-mediated inflammatory polyneuropathy, characterized by a disordered immune response to the peripheral nerves.1–3 In the United States, the estimated annual incidence of CIDP is 1.6 per 100,000 people, while the prevalence has been estimated at 8.9 per 100,000 people.4,5 The pathophysiology of CIDP is yet to be fully elucidated and is widely acknowledged to be multifactorial.6 CIDP is characterized by generally symmetrical proximal limb weakness by and sensory symptoms with a slow onset.1,2,7,8 The European Academy of Neurology/Peripheral Nerve Society (EAN/PNS) criteria for CIDP specifies clinical progression for more than 2 months and electrodiagnostic evidence of peripheral nerve demyelination; response to immunosuppressive or immune-modulating therapies, imaging, cerebrospinal fluid analysis and nerve biopsy can provide supportive evidence.9
Patients will typically present with worse quality of life, physical function, and disability as the disease progresses.9–11 One study found that only 27% CIDP patients were professionally active and 40% had difficulty with physical functions such as walking.12 A Serbian study of CIDP patients found a marked reduction in quality of life, particularly in relation to physical domains but also mental domains, including motor function, severe fatigue, depression, and unemployment.13 A population-based CIDP study found that 75.6% had disability in their upper limbs, only 41.5% could walk independently, 26.8% needed unilateral support, and a minority needed bilateral support or a wheelchair.14
Prompt diagnosis and treatment initiation before the disease progresses can avoid high levels of disability and irreversible axonal damage and therefore help maintain patients’ quality of life.13,16 Therapy goals focus on improvement and relapse-free maintenance preventing worsening muscle function and disability.17 Typical first-line treatments for CIDP include immunoglobulin, plasma exchange, and corticosteroids.4,9,18 Immunosuppressant or other immunomodulatory agents may be prescribed when first-line treatments are inadequate, including azathioprine, cyclophosphamide, ciclosporin, and methotrexate.18 Immunosuppressant treatments are associated with an increased risk of infections and an increased risk of certain malignancies.19
For immunoglobulin treatment, the initial dose is usually 2 g/kg, intravenously (IVIG) over two to five days followed by 1 g/kg at 3 week intervals. Eftimov 2013 reviewed IVIG treatment in CIDP (8) RTCs, 322 participants:19–26. The review found that within 6 weeks of IVIG treatment onset there was clinically significant improvement in disability (as determined and defined by the trial authors respectively). Another study considered all systematic reviews of randomized controlled trials of any treatment for any form of CIDP (5 trials, 269 participants) and found intravenous immunoglobulin produced more short-term improvement in disability than placebo.17
SCIG is an alternative to IVIG, with comparable long‐term efficacy in CIDP,27–29 however it provides greater convenience with the ability to self-administer at home. In patients with immunodeficiencies, SCIG is associated with improved health-related quality of life (HRQL) and treatment satisfaction versus IVIG30–37 and more stable serum IgG levels.38 There is a lower incidence of systemic adverse events with SCIG compared to IVIG both in patients with immunodeficiency38 and CIDP.28,29,39 Local‐site reactions are more common with SCIG than IVIG, but these are mostly well‐tolerated and abate with subsequent infusions.27,40,41 CIDP patients opting for SCIG may prefer this due to the independence and flexibility associated with self‐infusion, whereas IVIG preference may be a result of familiarity and reliance on a healthcare professional for infusions.27,42,43 Almasri et al39 conducted a meta-analysis that included 22 studies with data from approximately 1400 CIDP patients, and found a strong preference for SCIG due to its convenience and practicality, as well as significant improvements in functional outcomes, reduced adverse events, and better quality of life compared to IVIG.
Immunoglobulin therapies have been shown to maintain health status, quality of life44 and remission in CIDP patients.21,45,46 However, even on therapy a proportion of CIDP patients relapse.21,43 Further, whilst immunoglobulin treatment has therapeutic benefits to CIDP patients, it is also known for adverse events, which may be transient or long-lasting. Serious adverse events are rare, and include severe skin reactions, venous thrombosis, kidney failure, and hemolytic anemia.47 However, IVIG is most associated with mild-moderate symptoms including headache, nausea, rash, or influenza‐like symptoms17 (Eftimov 2013). The Oaklander 2017 systematic review of randomized controlled trials (5 trials, 269 participants) concluded adverse events were more common with IVIG than placebo.
This study investigated CIDP patient perspectives on quality-of-life impact and benefit of immunoglobulin therapy. This study expands on prior research which primarily focused on physical symptoms and functional limitations. It aims to offer a more holistic view of the patient experience and highlight opportunities to improve patient-centered care.
Materials and Methods
Survey
The research was conducted from March 2024 to August 2024 in accordance with privacy and data protection codes of conduct. The survey stage recruited 31 patients with CIDP from the USA, and 11 patients with CIDP from Europe (UK, France, Germany). The survey comprised a 20-minute online questionnaire.
The survey aimed to characterize Ig in CIDP treatment to understand and quantify the quality-of-life impact of IVIG and SCIG. To do this, the survey included a range of different question types, including: pre-coded (multiple choice) questions, dichotomous (yes/no) questions and rating scales as well as open-ended responses.
Specifically, the questionnaire included standardized scales to quantify CIDP-specific activities and social participation, the Inflammatory Rasch-built Overall Disability Scale (I-RODS),48 as well as scales to assess overall symptom and functional status: Patient Acceptable Symptom Scale (PASS),49 Patient-Reported Outcome Measurement Information System (PROMIS) Physical Function (PF) Short Form (SF)-11a,50 and the Work Productivity and Activity Impairment General Health (WPAI-GH).51 Results of these standardized scales were calculated according to guidelines and scoring instructions provided in the respective manuals/ handbooks for each tool.
Several strategies were employed to mitigate potential biases in survey responses. Participants were recruited from multiple sources to ensure a diverse and representative sample of CIDP patients across the USA and Europe. The survey was carefully designed to avoid leading or suggestive language. Participants were assured of the anonymity and confidentiality of their responses, which encouraged honest and unbiased reporting of their experiences. The survey focused on recent experiences and current treatment regimens to reduce the potential for recall bias.
The survey data were intended to provide descriptive context rather than to draw definitive comparisons or conclusions, and statistical significance was not assessed due to small sample size. Means, medians, and ranges were calculated where appropriate to aid descriptive results. Therefore, the findings are exploratory in nature.
In-Depth Interviews
After survey completion and proof of diagnosis confirmed, these same 42 patients were interviewed for the qualitative stage. Data were analyzed using NVivo 12,52 a qualitative data analysis software. The interviews were transcribed verbatim and imported into NVivo. A thematic analysis was conducted, where initial codes were generated and then grouped into broader themes (Supplementary Materials Table S1). NVivo’s query functions, such as word frequency, matrix coding, and text search, were employed to identify patterns and relationships within the data.
The process followed Braun and Clarke’s six-phase framework for thematic analysis.53 First, all interview transcripts were read and re-read to ensure immersion in the data. A line-by-line analysis of the transcripts was then performed, generating initial codes. Codes were developed inductively, based on the content of the data, and were not pre-determined. Criteria for code inclusion were based on relevance to the research objectives, such as patient-reported impacts of CIDP, experiences with Ig therapy, and treatment preferences. The initial codes were reviewed and grouped into categories based on similarities and patterns. These categories were further refined into overarching themes. Subthemes were developed within each theme to capture more specific aspects of the data. To ensure the reliability of the coding process, all of the transcripts were double-coded by a second or third researcher. Discrepancies in coding were discussed and resolved through consensus, and the coding framework was refined accordingly. Data saturation was reached after analyzing 42 transcripts, as no new themes or subthemes emerged during the final stages of coding. An individual patient level “saturation table” was created in order to track this. The final themes and subthemes were reviewed to ensure they accurately represented the data and aligned with the study objectives.
Study Cohort and Exclusion Criteria
The 42 patients with CIDP (USA n=31, Europe (UK, France, and Germany) n=11) were recruited via a mixed-method approach using specialist research panels and recruitment, digital outreach via patient associations and physician referrals. All patients were validated through written confirmation from their physicians of diagnostic tests being completed to provide their formal diagnosis of CIDP. Only patients who answered all survey questions were included.
Respondents were asked a series of screening questions to confirm that they were eligible (Figure 1) to take part: all patients must have been over the age of 18; must have had at least one of the following tests for CIDP: nerve conduction, EMG, lumbar puncture, nerve biopsy; must have been officially diagnosed with CIDP by a physician; a neurologist or neuromuscular specialist must have either made the formal CIDP diagnosis or currently manage their CIDP; must have (currently or in the past) used IVIG or Hizentra® SCIG; must have used their SCIG for one month minimum or IVIG for 3 months minimum. After survey completion, those who screened-in were further asked to provide medical proof of their diagnosis, in the form of a letter from their treating physician or test results confirming CIDP. A mix of current IVIG users, current SCIG users, and lapsed IVIG/SCIG users were recruited. Patients were recruited to ensure a diverse sample in terms of time since diagnosis, ranging from recently diagnosed (2 years or less) to those diagnosed over 12 years ago. While no hard quotas were set for specific time categories, efforts were made to achieve a broad representation of patient experiences across different stages of the disease. Minimal SCIG users were recruited compared to IVIG in order to prevent bias in the sample towards patients preferring SCIG. In total, 190 patients were screened, with 42 enrolled in the study. Rejected terms (consent/industry affiliation) (n=72) and proof of diagnosis not provided (n=40) were the two main reasons for exclusion. A large proportion of those excluded for lack of proof of diagnosis were due to a misunderstanding of those with similar conditions, eg Guillain–Barré syndrome/Acute Inflammatory Demyelinating Polyneuropathy (AIDP).
 |
Figure 1 Recruitment of Chronic Inflammatory Demyelinating Polyneuropathy (CIDP) patients in USA and Europe. |
Results
Respondent Characteristics
In total, 42 patients with CIDP were enrolled in the study. Respondent characteristics are summarized in Table 1 (further information provided in Supplementary Materials Table S2). Almost half respondents were in the 46–64 age category (48%). There were more female patients (67%) in the total cohort than male (33%). Two thirds of respondents were either on disability or retired, and two thirds utilized assistive devices in their everyday life. Twenty-six patients were currently receiving IVIG, 10 were currently receiving SCIG, and 6 were lapsed Ig users. For PROMIS PF SF-11a, a t-score of 50 corresponds to the general population mean (SD of 10). Thirty-six % had a t-score between 21 and 33 (indicative of severe limitations in physical functioning), 43% had a t-score between 34 and 44 (mild to moderate impairment), and 21% had a t-score between 45 and 58 (within average range of impairment).
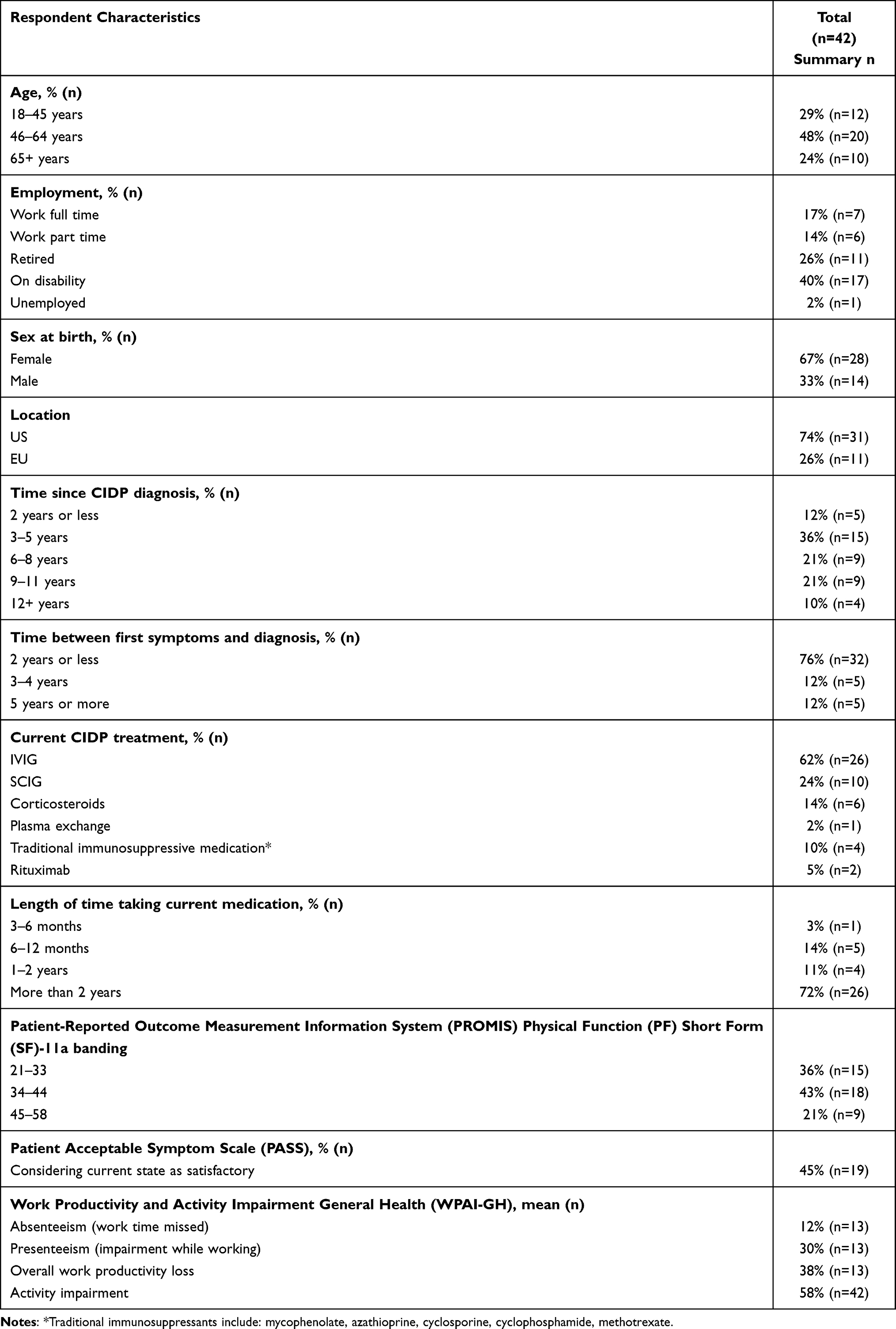 |
Table 1 CIDP Patient Characteristics |
Survey
Numbness of the hands or feet, tingling, and weakness in the hands were most commonly reported symptoms of CIDP (Figure 2A). Forty-five percent of the total cohort rated their current state as satisfactory using the PASS tool, however only 17% of lapsed Ig users rated their current state as satisfactory. CIDP was reported with a wide range of serious symptoms that affected physical function; loss of balance/co-ordination (60%), pain (48%), fatigue (38%), and weakness in hands/fingers (31%) were the most important reported current symptoms to obtain relief from through medication (Figure 2B).
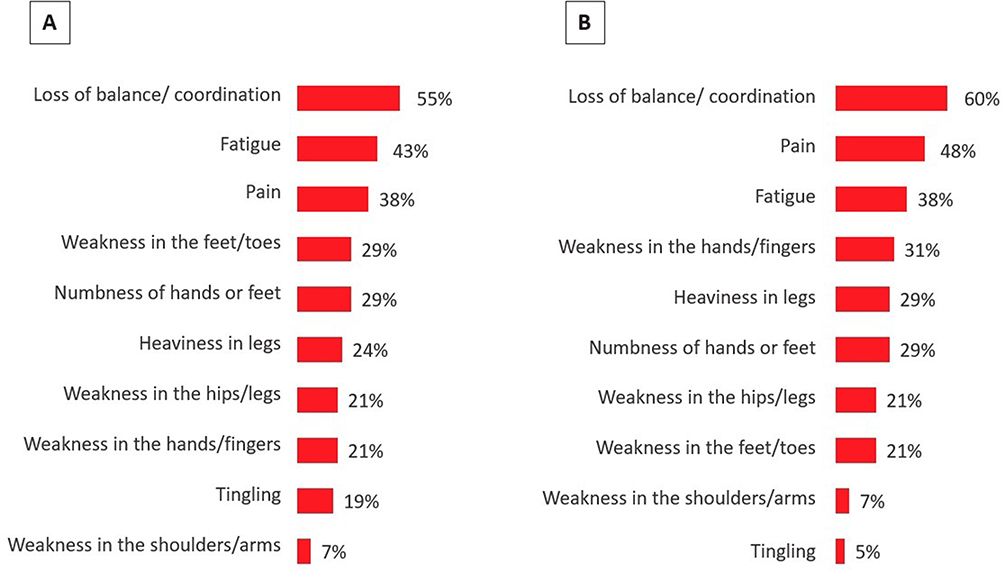 |
Figure 2 Percentage of respondents (A) ever experiencing each CIDP symptom, and (B) reporting most important current symptoms to obtain relief through medication. |
Evaluation of I-RODS revealed that even the simplest activities, ie, those with lowest item weighting on this Rasch-ordered scale, such as washing the upper body, reading a newspaper or book, or going to the toilet were not possible to perform without difficulty for 29–38% of patients (Figure 3A). The median I-RODS score was 55/100 (IQR 33), with clusters around centiles 31–40, 51–60, and 71–80 (Figure 3B).
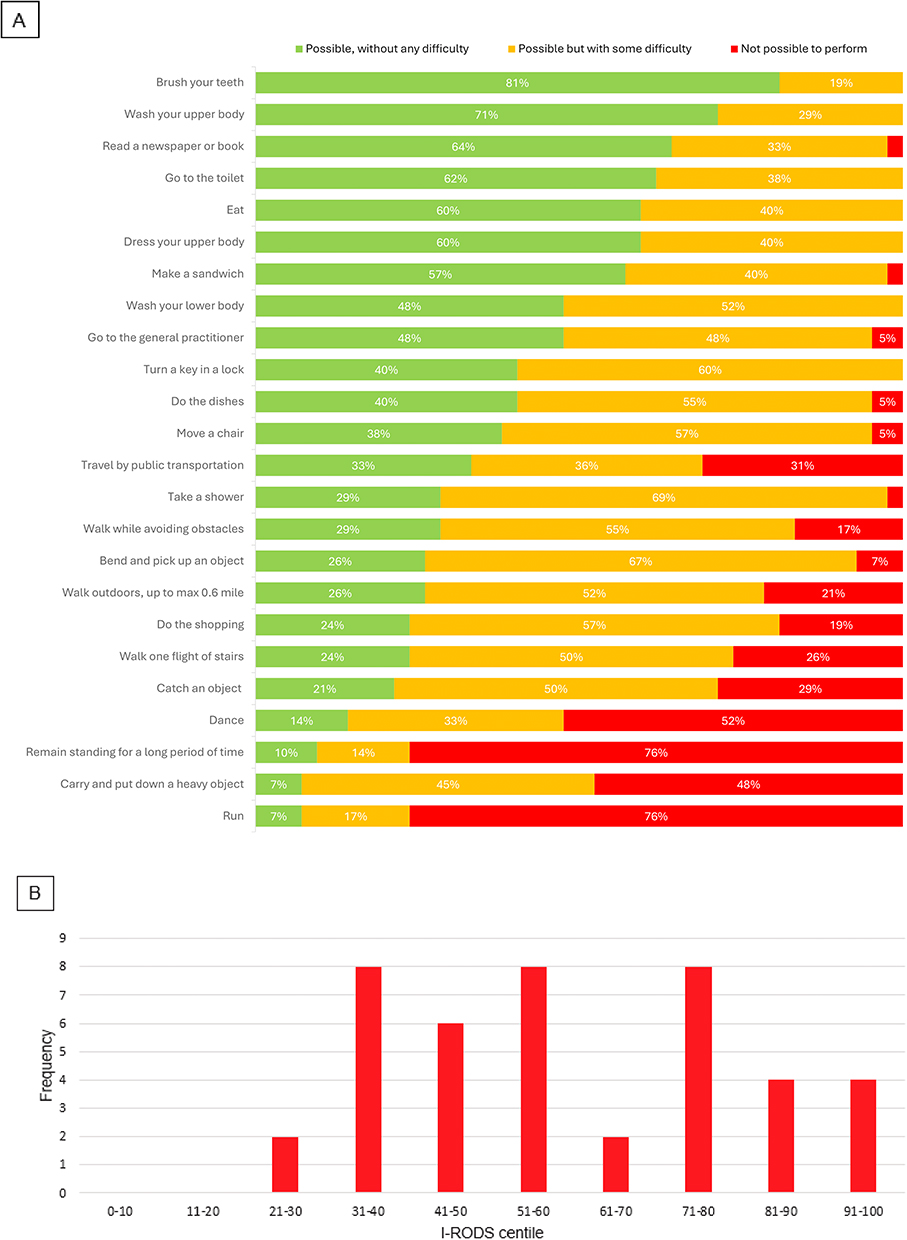 |
Figure 3 (A) Percentage of respondents scoring each activity as “possible, without difficulty” without the help of others or special equipment, (B) Inflammatory Rasch-built Overall Disability Scale (I-RODS) centile scores by frequency. |
For those who were working, the Work Productivity and Activity Impairment (WPAI) mean score for impairment while working due to CIDP is 30% (Figure 4A). A fifth of working patients missed work due to CIDP-associated problems in the past seven days, of which 14% missed 26 or more working hours (Figure 4B).
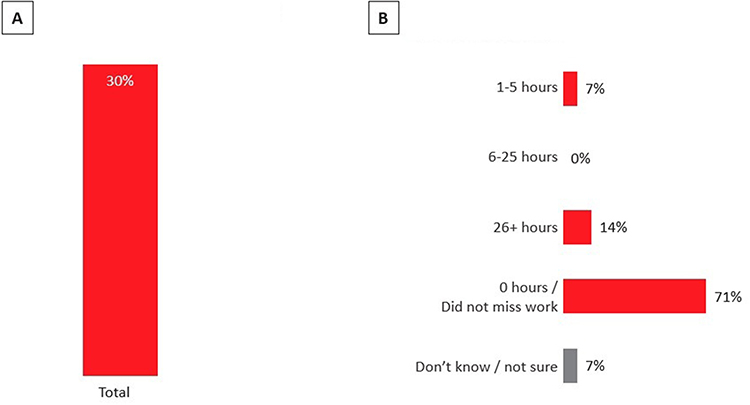 |
Figure 4 For those who work (n=14) (A) Percentage impairment while working due to CIDP (Work Productivity and Activity Impairment General Health (WPAI-GH) mean scores), (B) Hours missed from work due to problems associated with CIDP during past seven days. |
On a structured 5-point scale, 31% of respondents agreed that their close relationships are always or often strained due to CIDP, 38% agreed that they always or often felt isolated or alone, and 50% agreed that they were always or often embarrassed that they can no longer do things they used to do (Figure 5).
 |
Figure 5 Percentage of respondents rating the emotional effect that CIDP has on their life. |
The vast majority of patients (69%) reported significant improvements in physical function with initiation of IG therapy, such as increased strength and ability to walk and raise arms, reduced pain, and stabilization of their condition (Figure 6A). About 74% of patients reported their current status of symptoms is stable, with another 5% whose symptoms continue to improve (Figure 6B).
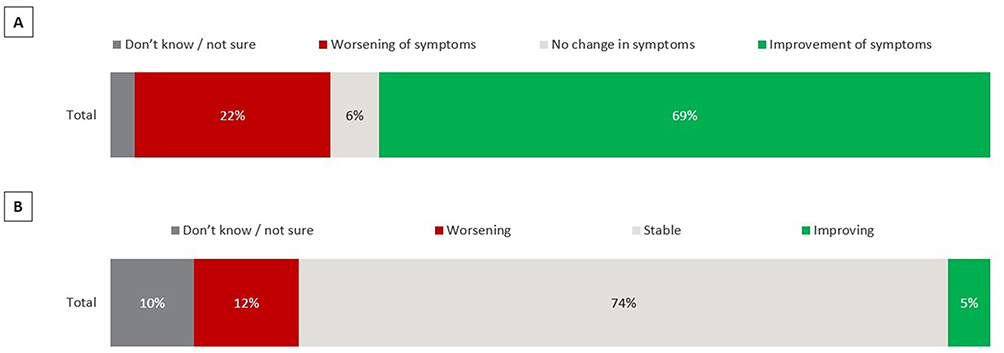 |
Figure 6 (A) Symptom experience since first being on current treatment, (B) Current status of CIDP symptoms. |
IVIG users reported a mean number of 2.2 days per month on which they received infusions. SCIG users reported a mean number of 4.3 days per month (Figure 7). However, the administration time for each infusion was significantly shorter for SCIG than the several hours required for IVIG infusion.
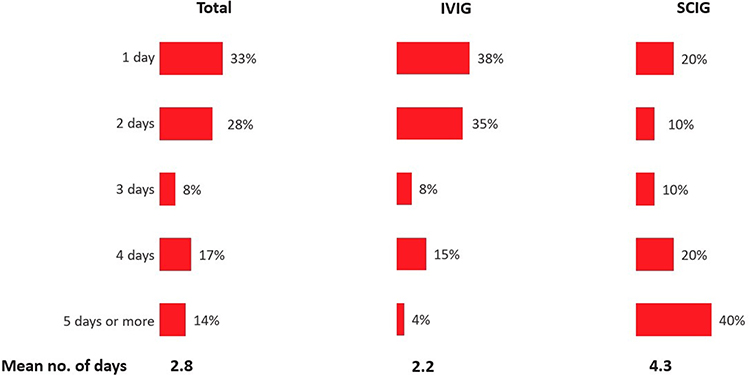 |
Figure 7 Days per month each immunoglobulin treatment required for total respondents, IVIG users, and SCIG users. |
Thirty-six % of patients noted that their Ig treatment was either discontinued or their dose lowered after stabilization of their symptoms. Of those patients, 1/3 (n=3) reported they then deteriorated (Figure 8). However, these patients had further adjustments and stabilized.
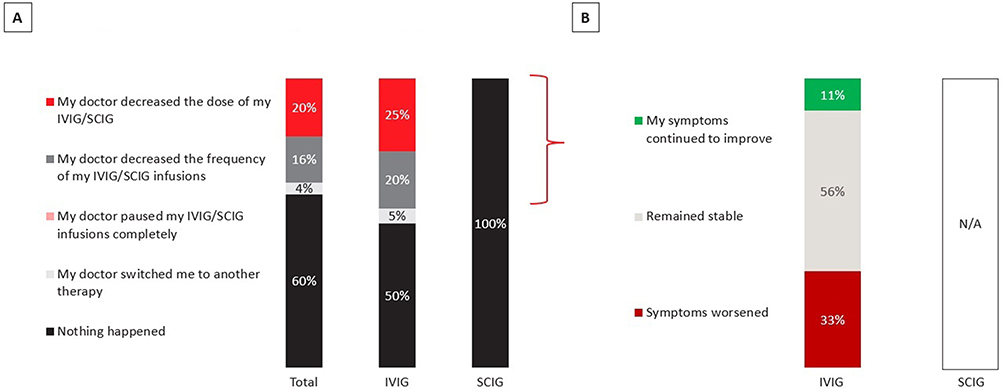 |
Figure 8 Percentage of respondents who had an improvement in their symptoms after starting Ig (A) HCP reaction to the improvement of symptoms (Total n=25; IVIG n=20, SCIG n=5), (B) Change in symptoms for those who had a decrease in dose/frequency of infusion or paused infusions (Total n=9; IVIG n=9, SCIG n=0). |
Thematic Analysis
The initial coding involved line-by-line analysis of the transcripts, resulting in 82 initial codes. These codes were then reviewed and grouped into 21 categories based on similarities and patterns. Through iterative analysis and refinement, four major overarching themes emerged: (1) Impact of CIDP, (2) Ig therapy impact, (3) patient reported adjustments to Ig dosing and treatment continuation following symptom stabilization, (4) future wishes to continue Ig treatment related to fear of deterioration. A summary table of themes can be found in Table 2.
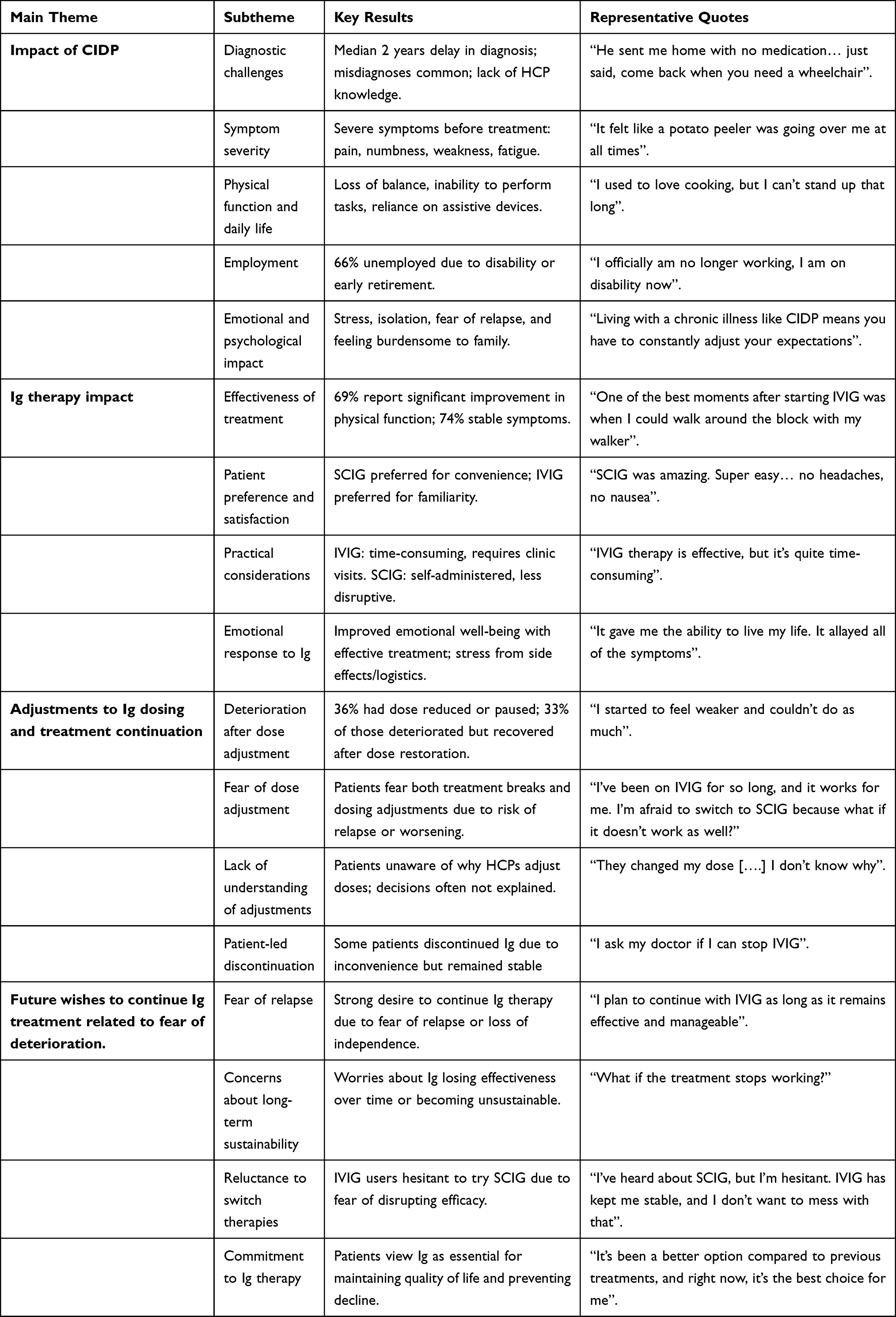 |
Table 2 Summary of Key Themes, Subthemes, Results and Patient Quotes |
Impact of CIDP
Patients mentioned physical, social, and psychological impacts of CIDP. Figure 9 presents a thematic model illustrating the relationships between the identified themes relating to IG impact as self-reported by the patients. Thematic analysis of the transcripts revealed CIDP has a severe impact on patients’ lives, and patients reported that their symptoms are responsible for these life changes.
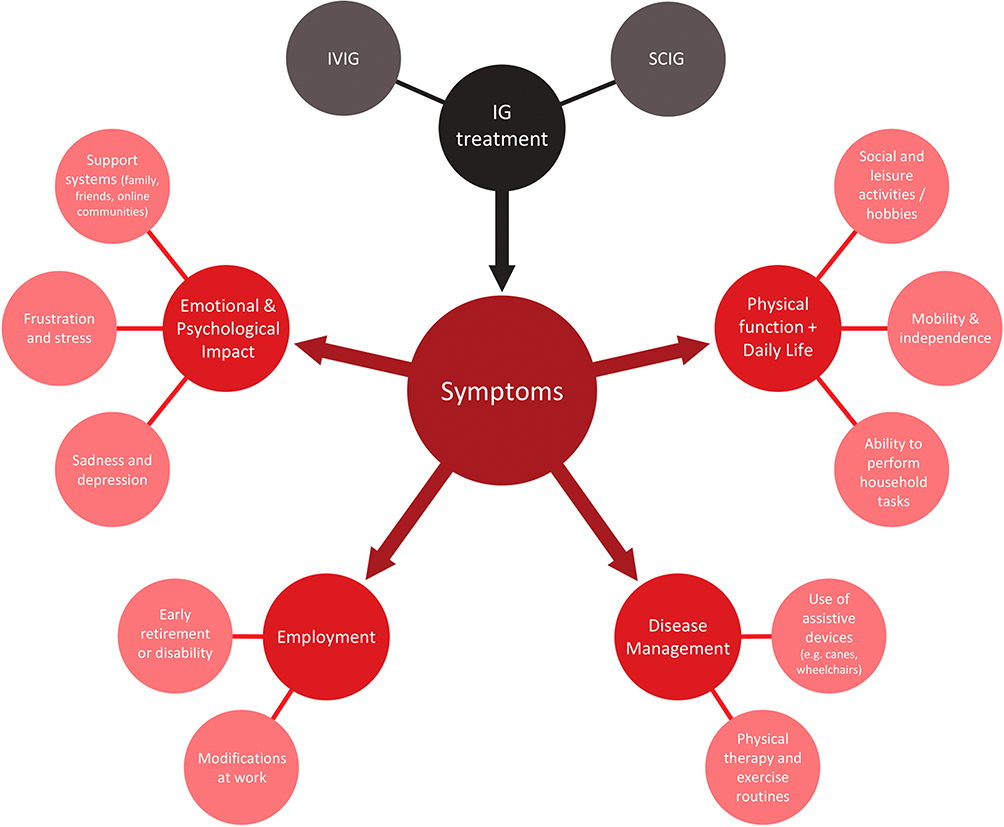 |
Figure 9 A thematic model illustrating the patient reported impacts of CIDP as they relate to IG treatment. Note: Thematic analysis based on patient narratives. |
Diagnostic Challenges
Patients reported how diagnosing CIDP could be a lengthy and complex process. There were reportedly several years between onset of first symptoms and CIDP diagnosis, with this cohort waiting a median of 2 years (range 0–15 years). Diagnosis journey was reported to be often characterized by initial misdiagnoses and the necessity for multiple medical consultations and tests. One of the themes that emerged was that patients felt that doctors were not knowledgeable enough on the condition, with some patients who supplemented medical professional opinion with their own online research.
On misdiagnosis and feelings of neglect, a female SCIG user from the US stated:
We did the EMG and the nerve conduction testing and [my doctor] even went as far as to take a muscle biopsy, and somehow this man came up with SMA as my diagnosis. He basically told me that I would be in a wheelchair by the time I’m 18, and to come back when I needed him… He sent me home with no medication of any sort and just said, come back when you need a wheelchair.
Disappointment, anger, and depression were commonly reported expressions of feeling of HCP neglect: A male SCIG user from the US stated:
[My doctor] has not contacted me to see how I have been doing on the SCIG, if I’ve improved, if I’ve declined, nothing. I have not heard a peep out of him. I’m really very disappointed and actually very angry. I know I’m not his only patient, but I feel like I completely fell off the planet as far as this doctor’s concerned.
These feelings of neglect were reported in all countries of our cohort. A male IVIG user from France stated:
It’s going to be three months now they’ve been looking for a neurologist. At the moment, a doctor for lungs signs off on my Ig treatment, but he told me, ‘That’s the last time, I don’t have the right to sign treatments that aren’t from my specialty. We have to find a neurologist, and if you don’t have a neurologist, I don’t know what we will do’. So, that’s it, I’m in total vagueness for now.
Symptom Severity
Thematic analysis revealed that the impacts of CIDP stem from its debilitating symptoms. Prior to diagnosis, patients frequently recounted a gradual onset of symptoms which collectively contributed to a progressive decline in physical function. Severity of symptoms was reported to be significantly worse before starting IG treatment compared to after, and part of the satisfaction with IG therapy came from the fact that symptoms were often extremely severe at the time of diagnosis.
A female IVIG user from the US discussed her severe symptoms before starting Ig therapy:
I was about a day or two away from being on a ventilator, so it was a 10 out of 10 for severity… the pain was unbelievable. I could hardly handle having any clothing on me or blankets at the hospital… it was excruciating. It just felt like a potato peeler was going over me at all times.
A male IVIG user from the US stated:
I remember the onset of my symptoms vividly. It was like a sudden storm that swept through my body, leaving me paralyzed and uncertain of what the future held.
Physical Function and Daily Life
That CIDP imposes significant physical constraints, affecting patients’ ability to perform everyday tasks, emerged as a key theme. Many individuals reported challenges in executing household chores, such as cooking and cleaning, due to diminished strength and dexterity. Unprompted, loss of driving ability was mentioned frequently by respondents.
Representative of the symptom burden, a female IVIG user from the US noted:
I used to love baking, I used to love cooking, but I can’t stand up that long. I can sit and do it, but it’s not the same. Plus the fine motor skills, I’m not good with a knife anymore.
A female IVIG user from France stated how CIDP limited their ability to engage in household tasks:
When I really reach the end of the infusion’s effects, then it’s catastrophic, I have a big fatigue coming, I see it, when I want to cook, I struggle enormously to cut. And the problem is that I’m someone very hyper and I want to continue living like I was before…I get tired enormously.
Two thirds of the cohort were not employed, due to either disability or early retirement resulting from CIDP symptoms. Most patients who went on disability did so within a year of their CIDP diagnosis. Some had to modify their job roles due to symptoms.
A male SCIG user from the US had to give up a job he was passionate about:
With the CIDP I’ve become immobile, and I am in a wheelchair, so it made things difficult because I was a choreographer. That was my love and my passion and that is the one thing that has been taken away from me. I officially am no longer working, I am on disability now.
A female IVIG user from the US describes modifications to their job as a result of CIDP symptoms:
I am a Certified Nursing Assistant, I have my license. I must let my bosses know I can’t be with anybody that needs walking assistance because I can’t support them the way that they need. At one time it become an issue where I was actually written up for calling out of work so much.
Emotional and Psychological Impact of CIDP
The emotional and psychological toll of CIDP was substantial; patients reported experiencing stress and frustration due to their inability to perform tasks independently and living with a fear of relapse. They reported their support systems, including family and friends, played a role in providing emotional support and practical assistance, helping patients cope with the psychological challenges of living with CIDP. However, caregivers typically were the patient’s spouse or adult children, and some patients reported feeling burdensome to their families.
A female IVIG user from Germany discussed living in fear of relapse:
I think the hardest part is the psychological burden. Living with a chronic illness like CIDP means you have to constantly adjust your expectations and deal with the fear of relapse. It’s not just the physical limitations, it’s the mental toll it takes on you.
CIDP’s impact on mobility and energy levels can limit participation in social and leisure activities, leading to social isolation. Respondents reported their loss of driving ability hindered their ability to perform errands and social outings. Patients often expressed concerns about their future, particularly regarding their ability to maintain independence and engage in meaningful activities.
A male IVIG user from the UK spoke about isolation caused by the emotional impact of CIDP:
I’m quite an outgoing person, but I became very withdrawn. And because of the weakness in my legs during that first summer [after diagnosis], it almost stopped me from going out. It was almost like having had the lockdown and all the effects of that. I wasn’t going out at all, socializing, partly because I didn’t feel like it, because of how I felt mentally. Your mind starts playing tricks with you, you start to get extremely worried.
Disease Management
Effective management of CIDP involves a multifaceted approach. Patients often utilize assistive devices, such as canes and wheelchairs, to maintain mobility and independence. Only one fifth of respondents have never used assistive devices, with 62% currently using them due to CIDP.
A female SCIG user from the US described her wheelchair use:
I can walk independently to an extent. I can’t walk if it’s grocery shopping, I have to be the one that pushes the cart. If it’s an airport, I still have to use my wheelchair. I either have to use my wheelchair typically, or I have to sit a lot.
A male IVIG user from France uses a cane:
I use a standard cane to help me walk. It’s not always easy, but it allows me to get around and do things.
Ig Therapy Impact on Quality of Life
Ig is credited with improving quality of life through relief of CIDP symptoms. While both IVIG and SCIG are seen as being highly efficacious, SCIG is seen as more convenient.
The majority of patients in all countries were treated promptly. The US experienced delays in a minority of patients (5/31 having had a delay of 1 or more years), whereas all EU patients began IG within a year of diagnosis. Germany was the fastest with all patients starting treatment immediately after diagnosis.
Effectiveness of Ig Treatment
Both IVIG and SCIG are generally perceived as effective in managing CIDP symptoms. Some had a considerable improvement in physical function since beginning treatment. The degree of effectiveness can vary, with some patients experiencing more significant benefits than others, and a small subset lapsing Ig treatment.
A female IVIG user from Germany went from wheelchair bound to walking independently:
One of the best moments after starting IVIG was when I could walk around the block with my walker. It felt like a huge victory after being wheelchair-bound for so long. Another high point was going to the supermarket without any mobility aids. These small victories mean a lot and give me hope.
The survey included only a very small number of patients (n=4) who lapsed Ig treatment due to a lack of efficacy. All continued to deteriorate on Ig and were discontinued by their HCPs. Of these four patients, two tried IVIG only and two tried both IVIG and SCIG. Only one experienced any positive effect of Ig on their symptoms initially, but it was mild, and efficacy declined until it no longer had any effect on their symptoms.
Patient Preference and Satisfaction
Satisfaction was closely linked to the perceived effectiveness and convenience of the treatment. Both IVIG and SCIG are rated highly by patients overall (both rated an average of 6 on a 7 point scale, with 1 being not at all satisfied and 7 being completely satisfied). Patients remain committed to Ig due to its efficacy. Many patients express a preference for SCIG due to its ease of use and minimal disruption to daily life, however not all IVIG patients are eligible to receive SCIG. Some patients are averse to the idea of the self-administered needles of SCIG.
A female SCIG user from the US discussed her commitment to SCIG despite her aversion to needles:
While I hate taking it, I really can’t knock it. It does what it’s supposed to do when I take it the way I’m supposed to, and it doesn’t give me the really bad headaches the way that the IVIG did.
A female lapsed user of SCIG and IVIG from the US discussed her preference for SCIG:
SCIG was my savior… SCIG was amazing. Super easy. I can’t say enough good things. Honestly convenient. I think the best thing about SCIG, there were no headaches. There was no nausea. All the things that I had when I had IVIG, I didn’t have, and I didn’t have that roller coaster, that crash.
Corticosteroids were used as an initial treatment or in combination with Ig therapies for some of the patients. Patients held negative views on steroids overall and frequently reported concerns about the long-term side effects. Side effects patients experienced included: weight gain, mood swings, insomnia, bone density loss, risk of infections, hypertension. The majority of patients who tried steroids also reported a lack of efficacy.
A female IVIG user from the US discussed her wariness of steroids due to potential side effects:
When I first started doing IVIG, they did a steroid treatment, and I was freaked out about that because of the side effects of steroids. So that was discontinued pretty quickly, just because my doctor also agreed it wasn’t a long-term solution at that time. It was just the once and I didn’t notice any improvement.
Plasmapheresis was less commonly used by patients and was typically reserved for cases where Ig treatments are ineffective (lapsed users). There was a common desire amongst patients for improved treatment options that offer greater efficacy with fewer side effects and less disruption to daily life.
Practical Considerations
The logistics of Ig treatment, including scheduling and frequency, were recurring considerations for patients. IVIG was often described by patients as time-consuming and usually requires travel to an infusion center, where it is administered by healthcare professionals. They reported this can be disruptive to daily life, as it involves long sessions and recovery time. Often IVIG patients reported planning their week around infusions.
A male IVIG user from Germany discussed the time considerations of the treatment:
The IVIG therapy is effective, but it’s quite time-consuming. It requires frequent visits to the clinic, and each session takes several hours, which can be exhausting.
Patients reported often struggling to balance treatment schedules with their personal and professional lives. IVIG was occasionally mentioned in the context of delaying household tasks, as patients are not able to walk around when receiving their infusions. Financial and insurance issues were also reported to impact treatment decisions, some IVIG users reported having to switch brands. Patients reported that SCIG offers greater convenience than IVIG, as it is self-administered at home and takes significantly less time, allowing for less interference with daily routines.
Emotional and Psychological Impact of Ig
The emotional response to Ig treatment was closely tied to its perceived effectiveness and the burden of administration. Successful management of symptoms through Ig treatment was reported to lead to improved emotional well-being. Conversely, side effects and the logistical challenges of treatment was reported to contribute to stress and frustration.
A female IVIG user from the US expressed her very positive feelings for Ig:
It gave me the ability to live my life. It allayed all of the symptoms. It gave me back my energy. It gave me back my life.
Patient Reported Adjustments to Ig Dosing and Treatment Continuation Following Symptom Stabilization
Patients were largely unaware of why their HCPs made treatment decisions such as changing doses or treatment pauses. Some recalled dose adjustments when they first started IVIG to optimize tolerance, but they were unaware of the details of this. They had more awareness of changes to their treatments due to adverse events or insurance changes, but not regarding symptom management. Exact dosing schemes were not collected, as patients were generally unaware of the specifics of their Ig regimens. In the interviews, all the current Ig users reported they are currently stable and have not experienced deterioration since dosing was optimized, other than the known factor of wear-off between doses that occurs with IVIG but not SCIG.
One third of lapsed users were mild CIDP cases who had improvement and stabilized on IVIG. Their discontinuation was patient-led; they requested their HCPs discontinue IVIG due to the inconvenience and discomfort of the treatment and remained stable upon discontinuation. Both spoke positively of the efficacy of Ig, crediting it for their stabilization, and noted they would try it again in the instance of a future deterioration.
Future Wishes to Continue Ig Treatment Related to Fear of Deterioration
Most patients expressed a strong desire to continue Ig therapy, driven by its efficacy and a fear of symptom deterioration if treatment were discontinued. Some patients expressed concerns about the long-term sustainability of it, citing fears of “relapse” with the treatment losing effectiveness over time. Fears include losing their ability to live independently and quality of life. Many described Ig therapy as essential for maintaining their current level of functioning and preventing further decline.
A female IVIG user from the US stated:
I plan to continue with IVIG as long as it remains effective and manageable. It’s been a better option compared to previous treatments, and right now, it’s the best choice for me.
Many patients were averse to treatment breaks due to fears of deterioration. They did not understand the need for a treatment break if the Ig was efficacious and tolerable and often reported they would go against the recommendations of healthcare professionals to take breaks.
A male SCIG user from Germany discussed his wariness of treatment breaks:
I would always continue taking it. The doctors actually recommend from time to time to take a break, but why should I stop? It’s an authorized medication that, if I take it regularly, I won’t have any deterioration.
The fear of deterioration was so strong that, despite the benefits of SCIG, some IVIG users were wary of trying SCIG in case the change will disrupt the Ig’s efficacy.
A female IVIG user from the US stated:
I’ve been on IVIG for so long, and it works for me. I’m afraid to switch to SCIG because what if it doesn’t work as well? I don’t want to risk a relapse.
Another female IVIG user from the US expressed the same concerns:
I’ve heard about SCIG, but I’m hesitant. IVIG has kept me stable, and I don’t want to mess with that. What if SCIG doesn’t work the same way?
Discussion
Many patients with CIDP are not satisfied with the care they receive. Diagnosis is long and arduous, characterized by misdiagnosis leading to delays in treatment and declining physical function. Frequently several physicians will be seen before diagnosis is finally confirmed. Patients have reported being hospitalized before physicians took their concerns seriously and tested them for CIDP. Even post-diagnosis, patients often feel ignored by healthcare professionals, and may struggle to make appointments or feel listened to by their doctors. The multinational CIDP survey conducted by Querol et al54 found a shorter median diagnostic delay of 6 months (IQR 3–12 months) compared to the median diagnostic delay of 2 years in this study, possibly due to differences in study populations or healthcare systems. However, the conclusions were the same regarding a lengthy diagnosis journey and many experiencing initial misdiagnosis. Incorporating standardized diagnostic criteria and early referral to neuromuscular specialists will help address the diagnostic delays.
The major impacts of CIDP stem from the debilitating effect on physical function. Decline in the ability to walk independently, use their hands and arms, and fatigue, all result in difficulties carrying out household tasks, hobbies, and their jobs. This results in increased reliance on family members to fill the role and take on these household tasks. In this cohort, 43% of patients reported having ever experienced fatigue, and Querol et al54 found FACIT fatigue scores of 35.0 (suggesting significant fatigue). Two thirds of the cohort were not employed, due to either disability or early retirement resulting from physical function impairment from CIDP. Similarly, in a large global survey, 44% of patients with likely CIDP reported stopping work due to symptoms.55 For some patients, the use of wheelchairs and other assistive devices led to increased isolation in the home. Therefore, physical function is their primary concern, and a treatment’s efficacy in this regard would be the primary motivator for patients and physicians. The median I-RODS score was 55 for this cohort, slightly lower than the median score of 62.5 found in Querol et al54 and the median score of 67 found in Peric et al,56 but all indicate moderate disability. The average PROMIS, PASS, or WPAI scores for CIDP patients have not been systematically reported in the published literature to date.
Patients self-assess their severity of CIDP based on their symptoms- their physical function, pain levels, and fatigue levels. Patients reported that, by contrast, their HCPs do not elicit patient reported ability to conduct tasks of daily living, such as ability to raise arms/hands, and perform household tasks, when assessing their CIDP severity. Instead, HCPs perform strength and reflex tests, though do sometimes ask about ability to walk. Although the measures differ, CIDP severity and treatment efficacy are still ultimately assessed using measures of physical function, with patients very rarely asked how they are emotional feeling. A more holistic approach can better capture the true burden of CIDP and guide treatment decisions. Beyond reflex and strength tests, clinicians could evaluate patients’ ability to perform daily tasks and their emotional well-being. Integrating mental health support into CIDP care, such as counseling or support groups, can help patients cope with these challenges and improve their overall well-being.
In general, most Ig patients remain committed to Ig due to its efficacy. Fear of relapse also contributes to strong commitment to Ig. All the SCIG patients in the cohort had first tried IVIG; those patients expressed a preference for SCIG due to its convenience and shorter infusion times. It also does not have a common issue with IVIG that the effects begin to wear off before the next treatment dose. On the other hand, some patients on IVIG were reluctant to try SCIG, due to fears of disrupting efficacy. Patients held very negative perceptions of alternative treatment options, such as corticosteroids, plasmapheresis, and immunosuppressants, due to their side effects and long-term issues that may result from them. Healthcare providers should consider patient preferences, lifestyle, and treatment goals when selecting between IVIG and SCIG. For patients who will remain on IVIG, strategies to minimize the burden of frequent clinic visits, such as home infusion programs, should be explored. Furthermore, comprehensive education on the benefits and administration of SCIG to address patient concerns will enhance shared decision-making in those who are eligible to switch to subcutaneous treatment.
Patients with CIDP are generally highly satisfied with Ig therapy due to its efficacy and the lack of alternative treatment options. However, 36% of patients reported that their Ig treatment was either discontinued or their dose reduced after symptom stabilization. Among these, one-third experienced deterioration but restabilized upon dose increases, while only a few ceased Ig therapy completely after achieving remission. This highlights the importance of exercising caution with dose reductions or treatment cessation, as these adjustments carry a risk of deterioration in some patients. Reluctance to alter a treatment perceived as effective may also act as a barrier to treatment optimization, emphasizing the need for careful monitoring and individualized treatment plans. Healthcare professionals should engage in shared decision-making with patients, ensuring they understand the rationale for treatment changes and the potential risks of discontinuation. Transparent and empathetic communication is essential to alleviate patient fears, which often stem from their reliance on Ig therapy to maintain physical function and quality of life.
This study focused on patient-reported experiences with dose adjustments and their perceived impact on symptoms but did not collect exact dosing data, limiting detailed analysis of dose-response relationships. High-dose immunoglobulin therapy has been associated with higher response rates and clinical improvement, with minimal increases in serious adverse events.57–62 These findings support the clinical utility of high-dose regimens in selected patients, particularly those with active or relapsing disease. However, as recommended by the European Academy of Neurology/Peripheral Nerve Society,8 the minimal effective dose should be sought in every patient to ensure individualized care and responsible use of healthcare resources. Ig therapy is costly and globally limited in supply, underscoring the importance of dose optimization. Future research should investigate the long-term outcomes and cost-effectiveness of different dosing regimens to inform evidence-based recommendations. Incorporating patient-reported outcomes into routine clinical assessments may further align treatment decisions with individual patient priorities, such as maintaining independence and minimizing disruptions to daily life.
Although a cohort of lapsed users were recruited, the recruitment strategy for this study required participants to have received at least one month of SCIG or three months of IVIG treatment, which may have introduced a selection bias favoring patients who responded to Ig therapy. This criterion was implemented to ensure that participants had sufficient experience with Ig treatment to provide meaningful insights into its impact on their quality of life and symptom management. However, this approach may have excluded patients who discontinued treatment early, potentially skewing the satisfaction findings toward more favorable outcomes. As a result, the generalizability of the findings, particularly regarding treatment satisfaction, may be limited to patients who tolerate and respond to Ig therapy. Future studies should aim to include a broader range of patients, including those who discontinued treatment, to provide a more comprehensive understanding of patient experiences with Ig therapy.
Future research should explore strategies to address patient concerns or fear of relapse, which may hinder their treatment optimization. This can be done through education, patient support groups, and shared decision-making in CIDP management. Qualitative research focusing on patient-provider communication could identify best practices for discussing treatment changes in a way that reduces fear and enhances patient confidence. Developing decision aids tailored to CIDP patients, which present treatment options and their implications in an accessible format, may also support more informed and collaborative decision-making. No single PRO instrument fully captures all relevant aspects of patient experience in CIDP, and further validation of disease-specific tools is needed.
While prior research has largely concentrated on the physical symptoms and functional limitations of CIDP, this study explored the perspectives of CIDP patients regarding the quality-of-life impacts and benefits of immunoglobulin therapy, broadened the scope of the patient journey. By examining themes such as diagnostic challenges, experiences with Ig treatments, and long-term disease management, this study provides a more holistic understanding of the lived experiences of individuals with CIDP.
Limitations
The present investigation is a survey among patients with CIDP having received treatment with IVIG or SCIG. The selection of patients having received Ig therapy for a least some time may have resulted in a selection bias towards patients who respond well to Ig therapy. Results reflect the patients’ perception and recall bias may be present in patient-reported outcomes. Further, objective clinical data was not available to validate perceptions. The cross-sectional study design inherently limits its causal inferences. The sample size limits statistical power, and the data is exploratory in nature. Results should not be extrapolated to a broader population. Exact dosing data was not collected, which prevents a detailed analysis of dose-response relationships. While we aimed to recruit a diverse sample of patients with varying durations since CIDP diagnosis, we did not set specific quotas for each time category. As a result, the distribution of patients across different stages of the disease was not controlled. This may limit the ability to draw conclusions about how disease progression specifically influences patient experiences and treatment perceptions.
Conclusion
The findings underscore the need for improved patient-centered care, including better communication between patients and healthcare providers. CIDP affects multiple aspects of the patients’ lives, and they relate each of these back to their symptoms. When assessing both the severity of their CIDP and the effectiveness of treatment, patients relate these to the severity of the symptoms they experience. Interviewed patients were highly satisfied with Ig, and patients were committed to IVIG due to fears of disrupting efficacy despite the benefits of SCIG.
Ethics
Centralized ethics committee Pearl IRB reviewed this study protocol and granted an exemption prior to study start (2024-0212). The guidelines outlined in the Declaration of Helsinki were followed in this study.
Participants were informed about the confidentiality and data protection policy at the beginning of the online screener. The research complied with local data protection in each country and was carried out within the codes of conduct of the Market Research Society (MRS), the British Healthcare Business Intelligence Association (BHBIA), and the European Pharmaceutical Market Research Association (EphMRA).
Informed consent (recorded) was obtained from the study participants at the beginning of the online screener and again at start of interview. Written informed consent (electronically via online platform) was obtained from the study participants at the beginning of the online screener. The information was shown on the first pages of the online survey, where they were given the option to consent and proceed with the survey or decline and close the survey. Only after consenting did they begin the study screener. Consent was recorded for each participant. Before the interview began, the consent information (same as from screener) was repeated, and consent was verbally confirmed a second time (video recorded). Consent explicitly included publication of anonymized results.
The study sponsor (CSL Behring) was not involved in data collection or analysis, which was conducted independently by Bryter to mitigate bias. The sponsor gave input into the study design and reviewed the manuscript drafts. Appropriate data analysis was conducted to mitigate bias/competing interests.
Acknowledgments
The authors gratefully acknowledge Bryter Inc, an independent market research company that carried out interviews, analyzed the data, and prepared the report. We would like to thank CSL Behring for providing an unrestricted grant for funding this research. The abstract of this paper was presented at the Peripheral Nerve Society 2025 Annual Meeting as a poster presentation with interim findings. The poster’s abstract was published in “PNS 2025 Annual Meeting Abstract Supplement” in the Peripheral Nerve Society Journal.
Disclosure
AH is a full-time employee of CSL Behring, and RM was an employee of CSL Behring at the time of study development. SJC and BG are full-time employees of Bryter Inc, and BG holds shares in its parent company Bryter Ltd. The authors report no other conflicts of interest in this work.
References
1. Dalakas MC, Medscape. Advances in the diagnosis, pathogenesis and treatment of CIDP. Nat Rev Neurol. 2011;7(9):507–517. doi:10.1038/nrneurol.2011.121
2. Mathey EK, Park SB, Hughes RA, et al. Chronic inflammatory demyelinating polyradiculoneuropathy: from pathology to phenotype. J Neurol Neurosurg Psychiatry. 2015;86(9):973–985. doi:10.1136/jnnp-2014-309697
3. Nobile-Orazio E, Gallia F, Terenghi F, Bianco M. Comparing treatment options for chronic inflammatory neuropathies and choosing the right treatment plan. Expert Rev Neurother. 2017;17(8):755–765. doi:10.1080/14737175.2017.1340832
4. Lehmann HC, Burke D, Kuwabara S. Chronic inflammatory demyelinating polyneuropathy: update on diagnosis, immunopathogenesis and treatment. J Neurol Neurosurg. 2019;90:981–987. doi:10.1136/jnnp-2019-320314
5. Laughlin RS, Dyck PJ, Melton LJ, Leibson C, Ransom J, Dyck PJ. Incidence and prevalence of CIDP and the association of diabetes mellitus. Neurology. 2009;73:39–45. doi:10.1212/WNL.0b013e3181aaea47
6. Cutellè C, De Lorenzo A, Doneddu PE, et al. Cytokines and chemokines in patients with chronic inflammatory demyelinating polyradiculoneuropathy and multifocal motor neuropathy: a systematic review. J Peripher Nerv Syst. 2024;29:124–134. doi:10.1111/jns.12622
7. Ayrignac X, Viala K, Koutlidis RM, et al. Sensory chronic inflammatory demyelinating polyneuropathy: an under-recognized entity? Muscle Nerve. 2013;48(5):727–732. doi:10.1002/mus.23821
8. Viala K, Maisonobe T, Stojkovic T, et al. A current view of the diagnosis, clinical variants, response to treatment and prognosis of chronic inflammatory demyelinating polyradiculoneuropathy. J Peripher Nerv Syst. 2010;15(1):50–56. doi:10.1111/j.1529-8027.2010.00251.x
9. Van den Bergh PYK, van Doorn PA, Hadden RDM, et al. European Academy of Neurology/Peripheral Nerve Society guideline on diagnosis and treatment of chronic inflammatory demyelinating polyradiculoneuropathy: report of a joint Task Force-Second revision. J Peripher Nerv Syst. 2021;26(3):242–268. doi:10.1111/jns.12455
10. Cocito D, Paolasso I, Antonini G, et al. A nationwide retrospective analysis on the effect of immune therapies in patients with chronic inflammatory demyelinating polyradiculoneuropathy. Eur J Neurol. 2010;17:289–294. doi:10.1111/j.1468-1331.2009.02802.x
11. Lunn MP, Manji H, Choudhary PP, Hughes RA, Thomas PK. Chronic inflammatory demyelinating polyradiculoneuropathy: a prevalence study in south east England. J Neurol Neurosurg Psychiatry. 1999;66:677–680. doi:10.1136/jnnp.66.5.677
12. Merkies IS, Hughes RA, Donofrio P, et al. Understanding the consequences of chronic inflammatory demyelinating polyradiculoneuropathy from impairments to activity and participation restrictions and reduced quality of life: the ICE study. J Peripher Nerv Syst. 2010;15:208–215. doi:10.1111/j.1529-8027.2010.00274.x
13. Santos PL, Almeida-Ribeiro GA, Silva DM, Marques Junior W, Barreira AA. Chronic inflammatory demyelinating polyneuropathy: quality of life, sociodemographic profile and physical complaints. Arq Neuropsiquiatr. 2014;72:179–183. doi:10.1590/0004-282X20130232
14. Bozovic I, Kacar A, Peric S, et al. Quality of life predictors in patients with chronic inflammatory demyelinating polyradiculoneuropathy. J Neurol. 2017;264(12):2481–2486. doi:10.1007/s00415-017-8658-x
15. Mahdi‐Rogers M. The Epidemiology and Treatment of Chronic Acquired Neuropathies [MD Thesis]. London, UK: London University; 2010.
16. Dyck PJB, Tracy JA. History, diagnosis, and management of chronic inflammatory demyelinating polyradiculoneuropathy. Mayo Clin Proc. 2018;93:777–793. doi:10.1016/j.mayocp.2018.03.026
17. Kuitwaard K, Fokkink WR, Brusse E, et al. Maintenance IV immunoglobulin treatment in chronic inflammatory demyelinating polyradiculoneuropathy. J Peripher Nerv Syst. 2017;22:425–432. doi:10.1111/jns.12242
18. Oaklander AL, Lunn MP, Hughes RA, van Schaik IN, Frost C, Chalk CH. Treatments for chronic inflammatory demyelinating polyradiculoneuropathy (CIDP): an overview of systematic reviews. Cochrane Database Syst Rev. 2017;1(1):CD010369. PMID: 28084646; PMCID: PMC5468847. doi:10.1002/14651858.CD010369.pub2
19. Glaubitz S, Zeng R, Schmidt J. New insights into the treatment of myositis. Ther Adv Musculoskelet Dis. 2020;12:1759720X19886494. PMID: 31949477; PMCID: PMC6950531. doi:10.1177/1759720X19886494
20. Hahn AF, Bolton CF, Zochodne D, Feasby TE. Intravenous immunoglobulin treatment in chronic inflammatory demyelinating polyneuropathy: a double‐blind, placebo‐controlled, cross‐over study. Brain. 1996;119(Pt 4):
21. Hughes R, Bensa S, Willison HJ, et al. Randomized controlled trial of intravenous immunoglobulin versus oral prednisolone in chronic inflammatory demyelinating polyradiculoneuropathy. Ann Neurol. 2001;50(2):
22. Hughes RA, Donofrio P, Bril V, et al. Intravenous immune globulin (10% caprylate-chromatography purified) for the treatment of chronic inflammatory demyelinating polyradiculoneuropathy (ICE study): a randomised placebo-controlled trial. Lancet Neurol. 2008;7:136–144. doi:10.1016/s1474-4422(07)70329-0
23. Mendell JR, Barohn RJ, Freimer ML, et al. Randomized controlled trial of IVIG in untreated chronic inflammatory demyelinating polyradiculoneuropathy. Neurology. 2001;56(4):
24. Nobile‐Orazio E, Cocito D, Jann S, et al. Intravenous immunoglobulin versus intravenous methylprednisolone for chronic inflammatory demyelinating polyradiculoneuropathy: a randomised controlled trial. Lancet Neurol. 2012;11(6):
25. Thompson N, Choudhary P, Hughes RA, Quinlivan RM. A novel trial design to study the effect of intravenous immunoglobulin in chronic inflammatory demyelinating polyradiculoneuropathy. J Neurol. 1996;243(3):
26. Dyck PJ, Litchy WJ, Kratz KM, et al. A plasma exchange versus immune globulin infusion trial in chronic inflammatory demyelinating polyradiculoneuropathy. Annals of Neurology. 1994;36(6):838–845.
27. Vermeulen M, van Doorn PA, Brand A, Strengers PF, Jennekens FG, Busch HF. Intravenous immunoglobulin treatment in patients with chronic inflammatory demyelinating polyneuropathy: a double blind, placebo controlled study. J Neurol Neurosurg. 1993;56(1):
28. Goyal NA, Karam C, Sheikh KA, Dimachkie MM. Subcutaneous immunoglobulin treatment for chronic inflammatory demyelinating polyneuropathy. Muscle Nerve. 2021;64(3):243–254. PMID: 34260074; PMCID: PMC8457117. doi:10.1002/mus.27356
29. Racosta JM, Sposato LA, Kimpinski K. Subcutaneous versus intravenous immunoglobulin for chronic autoimmune neuropathies: a meta‐analysis. Muscle Nerve. 2017;55:802–809. doi:10.1002/mus.25409
30. Ramzi A, Maya S, Balousha N, et al. Subcutaneous immunoglobulins (SCIG) for chronic inflammatory demyelinating polyneuropathy (CIDP): a comprehensive systematic review of clinical studies and meta-analysis. Neurol Sci. 2024;2024:1–18. doi:10.1007/s10072-024-07640-3
31. Espanol T, Prevot J, Drabwell J, Sondhi S, Olding L. Improving current immunoglobulin therapy for patients with primary immunodeficiency: quality of life and views on treatment. Patient Prefer Adherence. 2014;8:621–629. PMID: 24833896; PMCID: PMC4014377. doi:10.2147/PPA.S60771
32. Gardulf A, Borte M, Ochs HD, Nicolay U; Vivaglobin Clinical Study Group. Prognostic factors for health-related quality of life in adults and children with primary antibody deficiencies receiving SCIG home therapy. Clin Immunol. 2008;126(1):81–88. PMID: 17964220. doi:10.1016/j.clim.2007.06.009
33. Gardulf A, Nicolay U, Math D, et al. Children and adults with primary antibody deficiencies gain quality of life by subcutaneous IgG self-infusions at home. J Allergy Clin Immunol. 2004;114(4):936–942. doi:10.1016/j.jaci.2004.06.053
34. Hagan JB, Fasano MB, Spector S, et al. Efficacy and safety of a new 20% immunoglobulin preparation for subcutaneous administration, IgPro20, in patients with primary immunodeficiency. J Clin Immunol. 2010;30(5):734–745. doi:10.1007/s10875-010-9423-4
35. Jolles S, Borte M, Nelson RP, et al. Long-term efficacy, safety, and tolerability of HIZENTRA® for treatment of primary immunodeficiency disease. Clin Immunol. 2014;150(2):161–169. doi:10.1016/j.clim.2013.10.008
36. Mallick R, Jolles S, Kanegane H, Agbor-Tarh D, Rojavin M. Treatment satisfaction with subcutaneous immunoglobulin replacement therapy in patients with primary immunodeficiency: a pooled analysis of Six HIZENTRA® Studies. J Clin Immunol. 2018;38:886–897. doi:10.1007/s10875-018-0562-3
37. Mallick R, Solomon G, Bassett P, Zhang X, Patel P, Lepeshkina O. Immunoglobulin replacement therapy in patients with immunodeficiencies: impact of infusion method on patient-reported outcomes. Allergy Asthma Clin Immunol. 2022;18(1):110. doi:10.1186/s13223-022-00746-3
38. Nicolay U, Haag S, Eichmann F, Herget S, Spruck D, Gardulf A. Measuring treatment satisfaction in patients with primary immunodeficiency diseases receiving lifelong immunoglobulin replacement therapy. Qual Life Res. 2005;14(7):1683–1691. PMID: 16119180. doi:10.1007/s11136-005-1746-x
39. Kobrynski L. Subcutaneous immunoglobulin therapy: a new option for patients with primary immunodeficiency diseases. Biologics. 2012;6:277–287. doi:10.2147/BTT.S25188
40. Almasri A, Bril V, Katzberg H. Quality of life in patients with chronic inflammatory demyelinating neuropathies treated with subcutaneous immunoglobulin. Can J Neurol Sci. 2025:1–7. PMID: 40891262. doi:10.1017/cjn.2025.10416
41. Duhem C, Dicato MA, Ries F. Side‐effects of intravenous immune globulins. Clin Exp Immunol. 1994;97(Suppl 1):
42. Duhem C, Dicato MA, Ries F. Side-effects of intravenous immune globulins. Clin Exp Immunol. 1994;97 Suppl 1(Suppl 1):79–83.
43. Cocito D, Peci E, Torrieri MC, Clerico M. Subcutaneous immunoglobulin in chronic inflammatory demyelinating polyneuropathy: a historical perspective. J Clin Med. 2023;12(22):6961. PMID: 38002576; PMCID: PMC10671960. doi:10.3390/jcm12226961
44. Van Schaik IN, Bril V, van Geloven N, et al. Subcutaneous immunoglobulin for maintenance treatment in chronic inflammatory demyelinating polyneuropathy (PATH): a randomised, double-blind, placebo-controlled, Phase 3 trial. Lancet Neurol. 2018;17:35–46. doi:10.1016/s1474-4422(17)30378-2
45. Hartung HP, Mallick R, Bril V, et al. Patient-reported outcomes with subcutaneous immunoglobulin in chronic inflammatory demyelinating polyneuropathy: the PATH study. Eur J Neurol. 2020;27:196–203. doi:10.1111/ene.14056
46. Léger JM, De bleecker JL, Sommer C, et al. Efficacy and safety of Privigen(®) in patients with chronic inflammatory demyelinating polyneuropathy: results of a prospective, single-arm, open-label Phase III study (the PRIMA study). J Peripher Nerv Syst. 2013;18:130–140. doi:10.1111/jns5.12017
47. Eftimov F, Winer JB, Vermeulen M, de Haan R, van Schaik IN Intravenous immunoglobulin for chronic inflammatory demyelinating polyradiculoneuropathy. Cochrane Database Syst Rev. 2013;12:CD001797. doi:10.1002/14651858
48. Merkies IS, Bril V, Dalakas MC, et al. Health-related quality-of-life improvements in CIDP with immune globulin IV 10%: the ICE Study. Neurology. 2009;72:1337–1344. doi:10.1212/WNL.0b013e3181a0fd80
49. Van Nes SI, Vanhoutte EK, van Doorn PA, et al. Rasch-built Overall Disability Scale (R-ODS) for immune-mediated peripheral neuropathies. Neurology. 2011;76(4):337–345. doi:10.1212/WNL.0b013e318208824b
50. Maksymowych WP, Gooch K, Dougados M, et al. Thresholds of patient-reported outcomes that define the patient acceptable symptom state in ankylosing spondylitis vary over time and by treatment and patient characteristics. Arthritis Care Res. 2010;62(6):826–834. doi:10.1002/acr.20131
51. Rose M, Bjorner JB, Becker J, Fries JF, Ware JE. Evaluation of a preliminary physical function item bank supports the expected advantages of the Patient-Reported Outcomes Measurement Information System (PROMIS). J Clin Epidemiol. 2008;61:17–33. doi:10.1016/j.jclinepi.2006.06.025
52. Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. PharmacoEconomics. 1993;4:353–365. doi:10.2165/00019053-199304050-00006
53. QSR International Pty Ltd. NVIVO (Version 12) [Computer software]. 2018.
54. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
55. Querol L, Rinaldi S, Borsi A, et al. Real-world multinational survey of chronic inflammatory demyelinating polyneuropathy: disease characteristics and therapeutic landscape. J Peripher Nerv Syst. 2025;30(3):e70047. PMID: 40826893; PMCID: PMC12361836. doi:10.1111/jns.70047
56. Allen JA, Butler L, Levine T, Haudrich A. A global survey of disease burden in patients who carry a diagnosis of chronic inflammatory demyelinating polyneuropathy. Adv Ther. 2021;38(1):316–328. Erratum in: Adv Ther. 2021;38(2):1364–1367. doi:10.1007/s12325-020-01586-6. PMID: 33113101; PMCID: PMC7854453. doi:10.1007/s12325-020-01540-6
57. Peric S, Bozovic I, Pruppers MHJ, et al. Validation of the Serbian version of inflammatory Rasch-built overall disability scale in patients with chronic inflammatory demyelinating polyradiculoneuropathy. J Peripher Nerv Syst. 2019;24(3):260–267. PMID: 31397933. doi:10.1111/jns.12343
58. Conti F, Moratti M, Leonardi L, et al. Anti-inflammatory and immunomodulatory effect of high-dose immunoglobulins in children: from approved indications to off-label use. Cells. 2023;12(19):2417. PMID: 37830631; PMCID: PMC10572613. doi:10.3390/cells12192417
59. Cornblath DR, van Doorn PA, Hartung HP, et al; ProCID Investigators. Randomized trial of three IVIG doses for treating chronic inflammatory demyelinating polyneuropathy. Brain. 2022;145(3):887–896. PMID: 35038723; PMCID: PMC9050528. doi:10.1093/brain/awab422
60. Kapoor M, Reilly MM, Manji H, Lunn MP, Aisling S, Carr. Dramatic clinical response to ultra-high dose IVIG in otherwise treatment resistant inflammatory neuropathies. Int J Neurosci. 2022;132(4):352–361. PMID: 32842835. doi:10.1080/00207454.2020.1815733
61. Kuwabara S, Mori M, Misawa S, et al; Glovenin-I CIDP Study Group. Intravenous immunoglobulin for maintenance treatment of chronic inflammatory demyelinating polyneuropathy: a multicentre, open-label, 52-week phase III trial. J Neurol Neurosurg Psychiatry. 2017;88(10):832–838. PMID: 28768822; PMCID: PMC5629934. doi:10.1136/jnnp-2017-316427
62. Seino Y, Nakamura T, Hirohata M, Kawarabayashi T, Okushima T, Shoji M. Severe chronic inflammatory demyelinating polyneuropathy ameliorated following high-dose (3 g/kg) intravenous immunoglobulin therapy. Intern Med. 2019;58(6):855–859. PMID: 30449785; PMCID: PMC6465009. doi:10.2169/internalmedicine.1723-18
63. Terhoeven P, Seybold J, Utz KS, Nickel FT, Lee DH, Linker RA. Longer-term effects of intravenous immunoglobulin treatment in chronic inflammatory demyelinating polyneuropathy: who benefits? J Neurol Sci. 2020;419:117169. PMID: 33035867. doi:10.1016/j.jns.2020.117169
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.