Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Experiences Of Immigrant Parents In Sweden Participating In A Community Assessment And Intervention Program For Preschool Children With Autism
Authors Nilses Å ![]() , Jingrot M
, Jingrot M ![]() , Linnsand P
, Linnsand P ![]() , Gillberg C
, Gillberg C ![]() , Nygren G
, Nygren G ![]()
Received 5 July 2019
Accepted for publication 31 October 2019
Published 6 December 2019 Volume 2019:15 Pages 3397—3410
DOI https://doi.org/10.2147/NDT.S221908
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Åsa Nilses,1 Marianne Jingrot,2 Petra Linnsand,3,4 Christopher Gillberg,3 Gudrun Nygren3,4
1Center for Progress in Children’s Mental Health, Region Vastra Gotaland, Gothenburg, Sweden; 2Research and Development Primary Health Care, Region Vastra Gotaland, Gothenburg, Sweden; 3Gillberg Neuropsychiatry Centre, Institute of Neuroscience and Physiology, Sahlgrenska Academy, Gothenburg University, Gothenburg, Sweden; 4Child and Adolescent Specialist Centre, Angered Hospital, Region Vastra Gotaland, Angered, Sweden
Correspondence: Åsa Nilses
Center for Progress in Children’s Mental Health, Kungsgatan 12, Gothenburg 411 19, Sweden
Tel +46 722 245311
Email [email protected]
Background: Barriers inherent in service systems for autism can hinder parents from getting help for their children, and this is probably especially true for immigrant parents. In order to provide accessible assessment and interventions for preschool children with autism, a multidisciplinary team was established in one district of a Swedish city, with a majority population of immigrants.
Aim: The aim of the present study was to gain knowledge of the parents’ experiences of participating in the community assessment and intervention program.
Methods and procedures: A qualitative study with semi-structured interviews was conducted with parents of 11 children aged 3–5, who had been diagnosed with autism and participated in the community intervention program for at least 1 year. The interviews were recorded and transcribed verbatim, and data were analyzed following a phenomenological hermeneutical method.
Results: The overall meaning of the parents’ narratives was interpreted as “A new way of understanding my child made life more hopeful and more challenging than before”. Their experience was interpreted as a process, captured in the three main themes: ”An overwhelming diagnosis”, “Cooperating with the team”, and “Growing as a parent”.
Conclusion: As lacking knowledge of available resources and support seems to be an important barrier to access services, the results underscore the importance of providing individually tailored services including comprehensive societal support to immigrant families with young children suffering from autism. The study also highlights the importance of addressing the parents’ previous awareness and knowledge of autism early in the assessment process, as well as continually involving parents in the intervention program, and this may enhance parental growth.
Keywords: ASD, autism spectrum disorder, early intervention, migrate, parental experience, qualitative
Introduction
Autism spectrum disorder (ASD) is a serious condition that involves problems with communication and social interaction, as well as restricted and repetitive behavior, according to the diagnostic manual DSM-5.1 The prevalence of ASD is approximately 1%,2,3 but in recent studies, somewhat higher.4 Higher ASD prevalence rates have been reported in immigrant populations, especially in children of mothers who migrated during the child's pre- and perinatal period.5–8
Early diagnosis and interventions for ASD can have a significant impact on the course of the child's continued development,9–11 and a multidisciplinary assessment is essential.12 Neuronal plasticity and indications of “critical and sensitive periods” on the developing brain during early childhood are important premises for early intervention.13
It has been emphasized in several studies that close cooperation with parents as well as parent involvement in early interventions are important for children affected by ASD.14–16
Parents of children with ASD often experience daily life as stressful17–19 and suffer mental health problems to a greater extent than other parents.20,21 Raising a child with autism is described as strenuous and challenging,22 but that it can also lead to personal growth.23 Parents often report barriers to access interventions after the child's diagnostic process.18,19,24,25 Immigrant parents, or parents who are ethnic minorities, tend to delay help-seeking when their children show developmental and/or behavioral problems, compared to nonimmigrant parents.26,27 Possible explanations for this are language barriers and lack of knowledge of available support.27,28 Furthermore, immigrant parents of children affected by ASD and/or other neurodevelopmental disorders are less likely to access health services and usual sources of support compared to nonimmigrant parents.29,30 Thus, it is of great importance to highlight the support needs of immigrant parents and their children.
The public health services in the city of Gothenburg, Sweden, have implemented a screening program provided through Child Health Centers (CHC), to enable early detection of ASD.31 For children with suspected ASD, neuropsychiatric assessments are provided in specialized assessment centers. For children who are diagnosed with ASD, the assessment is followed by an intervention program in yet another separate treatment center. The process of screening, assessment, and intervention in separate locations is perceived as problematic to some parents, such as causing delays in receiving support or uncertainty during transition periods.32,33 Children of parents with inadequate social and economic resources are less equipped to navigate the obstacles in health-care systems, resulting in a greater risk of failure to follow through on referrals or poor attendance and/or adherence.33,34
A community multidisciplinary team for preschool children with neurodevelopmental disorders including ASD was established in one district of the city of Gothenburg. The aim of the program was to provide assessment and individually tailored interventions to children with neurodevelopmental disorders, in their own neighborhood, in order to increase the accessibility and continuity in the health care provided. Another aim was to increase parents' involvement in the interventions. The district is a socioeconomically disadvantaged area, with a majority population of first- and second-generation immigrants, a high percentage of unemployment and a low average income compared to the population of the whole city of Gothenburg.35 The multidisciplinary team offers comprehensive neuropsychiatric assessments, intervention, and support in close cooperation with the child's local health center nurse and preschool staff. Thus, families are able to obtain the services needed without having to be referred to separate and distant treatment centers, thereby minimizing unnecessary barriers in accessing services.
In the district in which the multidisciplinary team was established, there is a Family Center that comprised of a CHC, a Maternity Health-care Center, and an open-access preschool, as well as parent support services provided by the Social Services Agency. The CHC responsible for developmental monitoring of children aged 0–5 years, works closely together with the preschools in the district, because most children in this area, as well as in Sweden in general, attend preschool from the age of 18 months. At this specific CHC, about 1400 children were registered at the time of the study (December 2016). When the staff at the CHC (nurse, pediatrician, and psychologist) identify a child with suspected ASD and/or other neurodevelopmental problems, comprehensive assessment and interventions are provided at the Family Center by the multidisciplinary team (pediatrician, child psychiatrist, developmental psychologist, special education teacher, speech and language pathologist, pediatric nurse, and social worker). The parents are interviewed about the child's developmental and medical history, current clinical symptoms, and social situation. Various assessments are conducted with the child, such as physical developmental examination, hearing test, blood tests, and sometimes other relevant examinations like electroencephalography. Assessments of cognitive, adaptive, and language functions are also performed, as well as an observation at the child's preschool,36 or in the home. If there is an urgent need for treatment, it is initiated parallel to the assessment process. This may include addressing the sleep, feeding or behavioral problems, or the parents' need for family support.
When the clinical diagnosis is determined and communicated to the parents, they are offered counseling by a member of the multidisciplinary team. Comprehensive information and psychoeducational support is provided to both parents and preschool staff, based on the principles of the Early Start Denver Model (ESDM).37,38 According to the ESDM, parents and preschool staff are taught strategies for playing and communicating with the child in everyday activities. A manualized intervention program, delivered on an individual basis, is also introduced, either ESDM,37–39 or a comprehensive program called Intensive Learning for Young Children with Autism.40 This intervention program is based on Applied Behavior Analyses and provides a curriculum where imitation is used as a method to teach social interaction, play, communication, language, and academic skills.41 Both of the intervention programs, aiming to increase the child's social communication and learning skills, are provided through biweekly sessions with the child, the parents, and the preschool staff. The “intensity” of the intervention program is dependent on the extent to which the parents and the preschool staff practice the new skills with the child in between the sessions. In addition to the manualized program, interventions also involve continuously addressing and treating the individual child's coexisting developmental disorders, behavioral problems, and/or medical conditions.
The aim of the study was to gain a deeper understanding of immigrant parents' experiences of having their child diagnosed with ASD and participating in the community intervention program.
Methods
Study Design
A qualitative study was designed, based on semi-structured interviews, to capture the parents' experiences of participating in the community assessment and intervention program.42 In order to fully understand the parents' experiences, the narratives needed to be described and interpreted, and for this purpose, a phenomenological hermeneutical method was chosen.43 According to this method, the focus is on the understandable meaning of human experiences, captured through the individual's narratives. The method is inspired by the hermeneutical theory of interpretation,44 stating that it is possible to gain a deeper understanding of the lived experiences of humans, by differentiating between what a text says and what it is referring to. According to this method, a certain level of preunderstanding is considered useful in the interpretation process. The first author's experience of working in the district as a psychologist at the CHC, in cooperation with the community intervention team, was perceived as a useful kind of preunderstanding. However, during the process of interpretation, the researcher needs to be aware of previous knowledge, ideas, and personal views, in order to stay open-minded, and let the text speak for itself, a process called “bracketing”.43
Data Collection
Interview data were collected using a semi-structured interview guide, developed by the first author, ÅN, together with the second author, MJ (a physiotherapist and researcher experienced in qualitative studies). The interview guide was developed with the purpose of exploring the lived experiences of the parents' participation in the community assessment and intervention program. By outlining the objectives of the study, reviewing the literature and using clinical experience, the interview questions were developed. The interview guide, consisting of open-ended questions covered four main topics, as shown in Supplementary materials, Appendix 1. The responses were explored using follow-up questions, to capture the richness and nuances of the parents' experiences.42 As the main questions were abstract and some parents might find it difficult to provide detailed narratives based on these questions, additional questions were designed to cover different aspects of the main topics.
Altogether 11 interviews were performed, of which the first 2 were conducted by author ÅN, in order to try out the interview guide. Subsequently, interviews were carried out by an external interviewer (a licensed psychologist working with preschool children and their parents in a different area). One parent from each family participated in each interview, except for one of the interviews where both parents chose to participate. The interviews lasted 45–65 mins and were conducted at the local family health center. The interviews were held in Swedish, except for the last two, which were carried out with the help of a professional interpreter. When preparing for the interviews with interpreters, an interpretation agency was contacted with information about the study, and the choice of interpreter was discussed with a coordinator at the agency. Efforts were made to recruit interpreters with substantial experience, and if possible, previous experience with research interviews. The contracted interpreters were thoroughly informed individually prior to the interview, about the aim of the study and interview techniques in qualitative studies.45 All the interviews were audio recorded and subsequently transcribed verbatim by author ÅN.
Data Analysis
The interview texts were interpreted according to the chosen phenomenological hermeneutic method described by Lindseth and Norberg,43 a process consisting of three methodological steps: (1) naïve reading, (2) structural analysis, and (3) comprehensive understanding (interpreted whole). The hermeneutic circle was used as an analytical tool, which refers to a process of moving back and forth between the small parts of the text and the whole empirical material, in order to validate the detailed parts in relation to the whole text, and vice versa. The data analysis was mainly carried out by the first and second authors (ÅN and MJ), in close collaboration and with regular discussions. On several occasions, discussions were held with all authors, as well as in seminars with research colleagues, to ensure reliability and credibility.46
During the naïve reading, the first and second authors read through each of the interview texts several times, in order to get an overall impression and a sense of the material as a whole. It was important for the authors to try to bracket their preunderstanding,43 to be able to read the interviews with an open mind, and yet keep the research questions in focus. During the structural analysis, the authors reread each of the interviews thoroughly, looking for “meaning units”, such as phrases, sentences, or paragraphs that seemed to convey an essential meaning of the lived experience.43 When dividing the text into meaning units, there were some parts that did not seem to be about anything related to the research question, for instance, remarks about the weather. These text parts were taken into consideration during the analysis but did not contribute to the formulation of themes. The meaning units were then condensed into single words or shorter sentences. Each condensed meaning unit was expressed as precisely as possible in everyday words. When all interviews were analyzed and all meaning units were detected, the condensed meaning units were reflected upon with regards to similarities and differences. All condensed meaning units that were similar were further condensed, interpreted, and sometimes abstracted, to form subthemes. Subthemes that described experiences on the same topic were assembled into themes, and the overall meaning, the so-called essence, gradually emerged as the subthemes and themes were continuously reflected upon. During the final step (comprehensive understanding), the interview texts were once again reread several times, with the overall understanding and the validated themes in mind, until the naïve understanding was validated through the structural analysis. This meant that it sometimes was necessary to go back and reflect upon certain subthemes or themes, to discuss and reword those that did not seem to be validated through the naïve understanding. During this last phase, existing research relevant to the findings was also used to highlight the findings of the present study, and the themes emerging from the text were used to discuss research results from other relevant studies.43 Throughout the process of analysis, the software package N-Vivo was used47 to enable structuring and organizing the interview transcripts, meaning units, and emerging subthemes and themes.
Recruitment And Participants
Participants in the present study were parents whose child had been diagnosed with ASD, who had participated regularly in the community intervention program for at least 1 year, born in a foreign country (95% of all parents who took part in the described community intervention program were immigrants). Every family entering the intervention program had been informed about the planned interview study. At the point in time for the study, 16 families met inclusion criteria and were invited to participate in the study by a member of the intervention team. Of those, 15 families expressed interest in taking part and were contacted by the first author who gave further information about the aim of the study. Parents who spoke fluent Swedish were telephoned, and parents who did not speak fluent Swedish were informed during a regular visit at the CHC with the help of an interpreter. Parents who then consented to participate in the study were sent written information about the interview questions that would be asked during the interview and about the voluntary nature of the study. They were informed about their right to end participation at any time without negative consequences for their child's continued treatment.
Parents of 11 children chose to participate in the present study. Parents of the four other children declined to participate when they had received more information about the study, referring to lack of time as the main reason. The interviews were performed during September and October 2016. The age of the parents ranged from 24 to 44 years (mean age 34.5). The parents' years of schooling were as follows: eight had completed high school, three had 2 or more years of higher education (college/university), and one had not completed elementary school (mean years of schooling was 12 years). All parents but one lived together with the child's other parent. The median amount of time since the parents' migration to Sweden was 9 years, with a range between 2 and 30 years. The number of children within each family ranged from 1 to 4. Each of the children, in addition to the ASD diagnosis, met criteria for one or more additional developmental problem, including attention-deficit/hyperactivity disorder (AD/HD), speech and language problems, learning disabilities or intellectual developmental disorder. Participant demographics are summarized in Table 1.
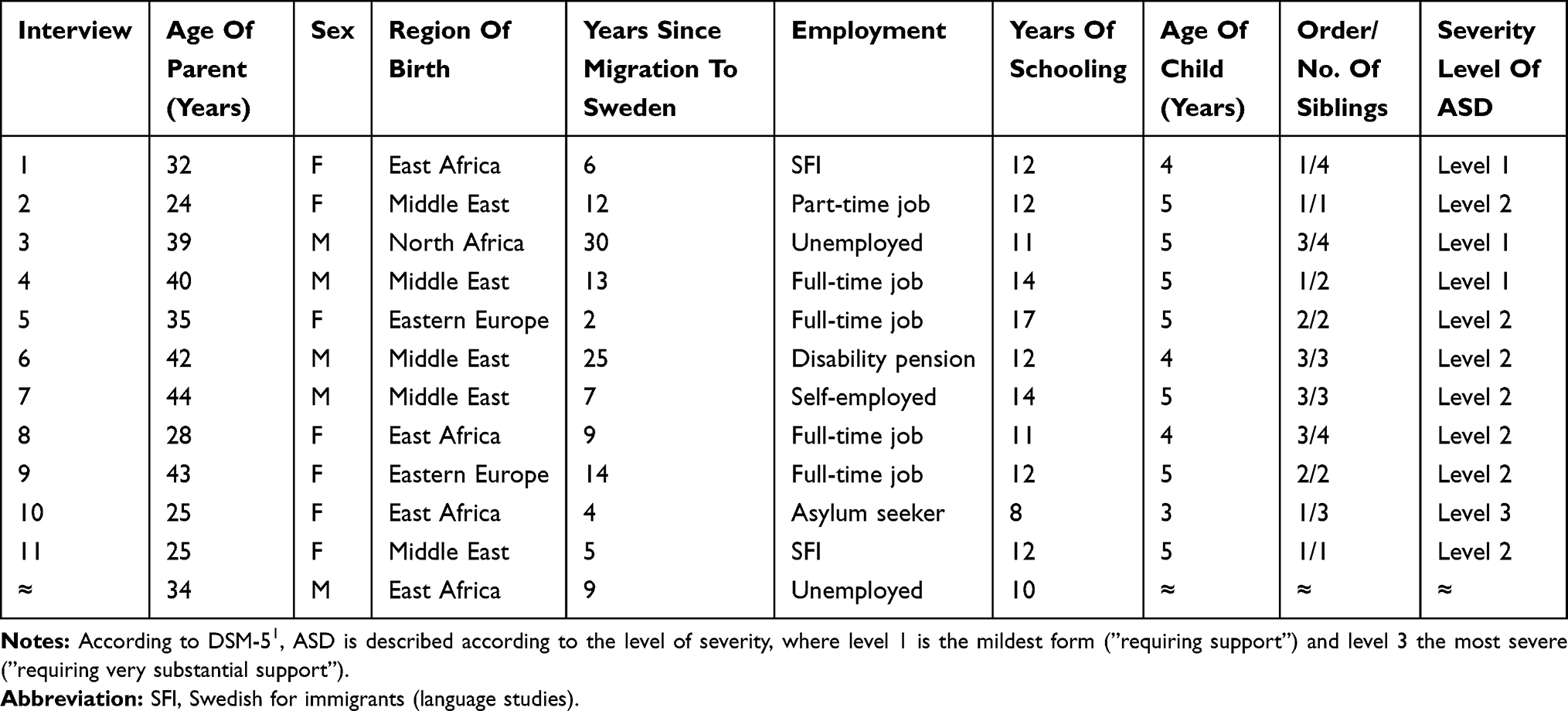 |
Table 1 Demographic Description Of Participating Parents And Their Children (n=11) |
Results
An essence emerged from the analysis of the interview texts, based on three main themes relevant to the aim of the study, is illustrated in Figure 1. Each of the main themes consists of four or five subthemes (see Figure 2), and in the following presentation, subthemes are illustrated by quotes from the interviews, translated into English. Following the quotes, a number in parentheses indicates the order in which the participant was interviewed.
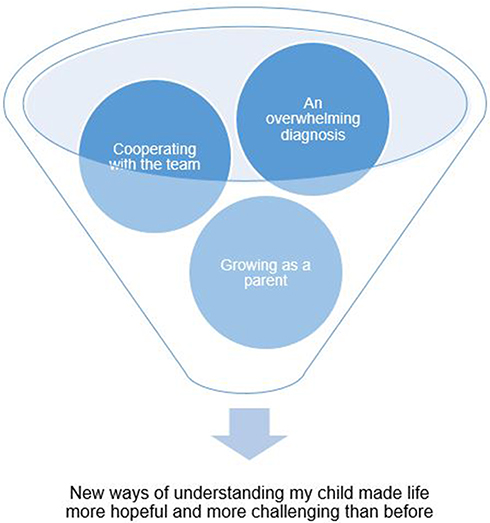 |
Figure 1 Three main themes were interpreted as a process which constitutes the essence of the parents' experiences. |
The essence of the interview themes, new ways of understanding my child made life more hopeful and more challenging than before, was interpreted as a process that parents described going through during their involvement in the child's assessment and intervention program. During the process, parents experienced that they learned more about their child, and for some of the parents this kind of knowledge was completely new. The first main theme, an overwhelming diagnosis, describes the different feelings parents reported going through upon learning about their child's diagnosis. The feeling of understanding their child was perceived as gradually growing stronger as parents became involved in the child's interventions, which is described in the second main theme, cooperating with the team. Taking an active part in the child's interventions was experienced as generating both emotional and practical consequences for the parents, which was interpreted as the third main theme, growing as a parent.
 |
Figure 2 Presentation of the subthemes in each of the main themes. |
An Overwhelming Diagnosis
The first main theme concerns the different emotions and reactions that parents described upon learning about their child's diagnosis. Some parents stated that it was their own initiative to let their child go through the diagnostic process, due to their worries about the child's development and behavior. Others reported that the assessment was initiated by the child's CHC nurse or the preschool staff. Parents were not asked questions about their feelings before the child's assessment; however, they mentioned feeling worried and insecure about what would happen next. For some parents, the diagnosis did not come as a surprise, but instead experienced the diagnosis as a confirmation of their earlier worries. For others, the word autism was completely new, which seemed to make the process of understanding and accepting the diagnosis more difficult.
Dealing With Emotions
Learning about the child's diagnosis triggered emotions that were experienced as difficult to manage. Parents expressed reactions like feeling shocked and alarmed:
No, actually both of us experienced the same kind of shock. Well … I think the mother a bit more maybe. She was crying so much, she was sad all the time … and she still says: it can't be true! (6).
Another emotional reaction commonly described was sadness, and experiencing a period of mourning: ”It felt … I just began to feel really sad.… Firstly because she doesn't speak, secondly because she doesn't listen. So … it just felt really hard, having a child who's different … ” (10). Talking to one's partner was described as a helpful way of dealing with the difficult feelings. Another way of dealing with emotions was turning to a member of the intervention team for counseling, because this was offered to each of the parents after their child received diagnosis.
Never Heard Of Autism
The word autism was experienced as a completely new concept for some parents, and they were faced with a whole new world of knowledge. Parents described how they previously had made their own interpretations of the child's behavior, for instance as a sign of physical problems:
At first I thought he has to see a doctor to have an examination to sort out the problem.… It's something he has … somewhere he's in pain … or suffers from some kind of disease … but I was never aware of any autism. […] That didn't exist in my mind, those kind of diseases … (1)
Another parent recalled making no interpretations at all, just accepting the child's strange behavior: ”Before the assessment, like I said before, I thought X just liked spending time with the mobile phone. But after the assessment, I'm feeling more bothered … or worried … about X's behavior” (10). Parents who reported no previous knowledge of the word autism expressed a need for more information, through individual counseling, during the process of learning about the diagnosis.
Fearing Stigma
Parents expressed fear of telling others about the child's diagnosis. They described being afraid of what other people would think and how they would respond. One example was fear of other's judgement: ”People don't understand … that's why we avoid sitting around and telling others … […] And to be honest, sometimes you shouldn't tell just anybody, because they might go around gossiping … ”(6). Another example was hesitating to tell the extended family about the diagnosis because of their assumed negative preconceptions:
We haven't told the whole family that he has autism. With autism you think such serious things … [I: Mhm … what is it one thinks?] When you say autism people will think he's stupid, or handicapped and so on … with autism you think of really serious diseases. (7)
In summary, the theme fearing stigma was interpreted as being afraid that telling others about the child's diagnosis would cause negative consequences for themselves or their child.
Sense Of Relief
Parents described that learning about of the child's diagnosis, besides the difficult feelings, also gave them a feeling of relief. They expressed that it made life easier to know why their child was behaving differently compared to other children, and how they could manage their child's needs: ”When we started this … after a few meetings, you know … you knew more what it's all about, and somehow this was easier to cope with” (9). Learning about what was causing the child's delayed or different development gave a sense of comprehensibility, and that there was something the parents could do to help their child. Finding out the child's diagnosis was also described as relief from a sense of guilt:
… before I was feeling … I had a feeling of guilt. I thought: why is he like this? Is there something we didn't do well enough? Is there something we did wrong, you understand? I felt guilty.… But now that I know, I … or we … don't feel that way anymore. (2)
Cooperating With The Team
The second main theme describes different aspects of parents' experiences of being involved in the child's intervention program. Several aspects were expressed as facilitating factors, like being able to get in touch with the intervention team easily, meeting the same professionals throughout the assessment and interventions, as well as being thoroughly listened to. Feelings of disappointment were also reported, mainly expressing a need for more frequent and longer sessions with the intervention team.
Feeling Important
During the diagnostic process, and throughout the intervention program, parents met numerous times with the multidisciplinary team. They described the team as attentive and perceptive, making parents feel that their experiences, thoughts, and feelings were important. Parents also expressed being able to adjust the interventions according to their child's capability, for instance, the level of difficulty or the speed of moving forward: “I noticed that when we felt things were going too fast, we told them, that this is too fast for X. Then they adjusted the schedule … ”(5). Together with the child's preschool staff, parents were taught exercises to practice with the child. Feelings of satisfaction were reported, concerning the fact that they as parents were the ones teaching their child new skills, and noticed that it made a difference. Regardless of how frequently parents reported being able to practice the exercises, they expressed joy about making an impact on their child's development.
But at first we didn't know how to do this, but then they began to help us here at the center, how to teach X, to help him develop new skills. They gave us exercises, and gave the same exercises to the preschool … we did this together. We did it here, then at home, and then the same at the preschool, and that makes three, and each helped a bit … and that's how it works (snaps his finger) … it helps. (7)
Being Close
In many aspects, parents described feeling comfortable and satisfied being involved in their child's intervention program. The fact that they were able to come and see the team in the local family center, not having to travel far, was considered important for some of them: “We didn't have to go all the way across the city to see the team. Yeah … that was better for us. Otherwise it would have been hard, both for us, and for X too” (4). Some valued being able to get in contact with the team easily, and schedule meetings on short notice:
In the beginning, I contacted them, or called them, quite often … rather often. More than usual. I asked quite a lot of questions. But now these contacts aren't as frequent. If I feel I need their help, they schedule an interpreter, and we meet with them. (11)
The possibility of meeting the team in a place they were already familiar with was described as important both for the parents and the child. The importance of meeting the same professionals throughout the process, both during the assessment and the subsequent intervention program, was also stated. Parents experienced getting to know the professionals well, which was interpreted as an important part of feeling close and comfortable.
The first time you meet with someone it's always … you feel unsure of what will happen. But then after a while, once you get to know them, the people who are supposed to help you … to help us, you feel more helped … as for me I felt really, really helped. And you feel they're close, and you can talk to them about all the problems you stumble across. (1)
Navigating Service Systems
Having a child with ASD means having to navigate and maintain regular contact with a multitude of different professionals and agencies, such as preschool staff, the Social Services, the National Insurance Office, as well as different public health-care units. Parents talked about the fact that they as immigrants needed more information and support in understanding the public systems of health care and social services:
And another thing … since one is new in this country, one doesn't have a clue of what help there is, you know, and where to turn to for that help. That's a good thing about this place, you can just ask them. (9)
Parents expressed that the support provided by the team was considered helpful. Not only because of the information they received but also because they were supported when establishing contact with new service agencies when needed, like telephoning, setting up a meeting, or being accompanied to the first meeting.
They know which units to turn to, they know where to go … if I'm feeling sick, or if I'm not feeling well, they take you to the place and show you. Like they'll go: Here's what you need, if you want it. You'll feel better.… The social services can help you, and we can help you get in touch with them. So … you can get all the help you wish for, just anything, they're so helpful with children and their parents, really … (1)
Wanting More Support
When asked if there was anything lacking during the child's diagnostic process or the intervention program, parents in general responded that they were satisfied with both the assessment and the intervention program and had no further requirements. Feelings of disappointment were also reported, such as expecting more frequent appointments with the team, or that the sessions had lasted longer:
X doesn't receive as much help as we expected. People we read about receive interventions at least 45 minutes or more every day. We see the team once every second week or sometimes even once a month, that's not enough. (10)
Another example of wanting more support was the expressed frustration about being expected to perform the exercises at home with the child:
We expected … in our heads … a lot, actually. That X would be offered a lot more help, a lot more support. That he would attend a center with experience and knowledge of children with autism, and go there every day. Me or his mom … or ordinary people, we can't understand X that easily. (6)
Growing As A Parent
The third main theme illustrates parents' descriptions of how their parenting was affected by their involvement in the child's intervention program, and some of the perceived consequences. Parents expressed different ways in which their interactions with the child had changed, as well as the relations within the family, as a result of the new ways of understanding the child that they had gradually acquired. They reported both emotional and practical consequences, which are described in the following subthemes.
Interacting With The Child
While the parents continuously acquired knowledge and understanding of the support needs of their child, they also experienced changes in the way they interacted with the child, such as being more proactive and avoiding unnecessary conflicts with the child.
I try to explain things to him, but if he still doesn't want to do the thing I'm asking him to, then it's ok. You shouldn't make a great fuss about things, that's what I've learnt. Have patience. I'm not actually that kind of person. In my childhood and youth, I've always been the kind of person who snaps immediately, kind of. But now that I have this knowledge, I don't any more … (2)
Some parents described that altering the way they interacted with the child contributed to positive changes in their child's behavior:
It was both him and us that had to … agree, we had to understand each other. And I … sometimes he's caught by something … some activity, and doesn't want to leave. But I know now I'm going to have to wait for him. […] … otherwise he's not gonna cooperate. And now it definitely takes less time than before. (5)
Bringing The Family Together
One of the experienced consequences was that the new way of understanding their child increased the couples' ability to cooperate, by sharing responsibilities, and taking turns in managing their child's routines. Parents described that the mutual and growing knowledge about their child strengthened the communication between them:
In a way, we started to sit down and talk to each other: how do we solve this? How do we handle him? To find solutions, find help, to read a lot about autism, and so on.… This has opened a lot of opportunities and pathways for us … (6)
The parents also perceived a strengthening of the family as a whole, and that the interventions had led to a growing feeling of cohesiveness and increased understanding for all members of the family:
I believe that the diagnosis affected our family in a positive way. And another thing, the members of our family affected each other's feelings too, it brought us closer together, you could say. (5)
Organizing Daily Life
Along with the new ways of understanding their child, parents described being able to organize daily life more efficiently. They developed strategies to improve routines and overcome logistic challenges, and reported new parenting skills that made daily life easier:
We make a daily schedule for him, and they make one at the preschool too. We noticed that if we don't make the daily schedule, it doesn't work, he can't manage without it. But when you have a schedule with fixed activities, it works quite well. (11)
Managing daily routines was experienced as a challenge, but examples were given of how these were overcome, through the development of organizational skills enabling leisure time and family activities to be planned more efficiently:
You have a great deal to keep up with at times, but … we try, and it does affect our daily life, it really does. Sometimes we have to consider the whole family's needs, and we have to devote lots of time to plan the extra activities, when we break the normal routines. (3)
A Burden Too Heavy
Daily life with a child affected by ASD was percieved as demanding, and the circumstances sometimes impossible to manage. The child's participation in the intervention program was energy- and time-consuming. Parents expressed that other factors, such as their employment- or housing situation, made it difficult to find time and energy to practice the new skills with the child, as much as they would have wanted to: “It's my situation that's really hard, me and my kids are lodgers in one room, so there's not enough room. Then there's my other kid who cries a lot, it's all just too much for me” (10). Parents who had more than one child often described it difficult to find enough time for their other children. The situation in the family was sometimes complicated for the siblings, who often felt it was unfair that the child with ASD was given more time and attention: “For sure, she [sister] doesn't like it. […] It's really hard to find the time for all of them, and she's not happy about me just taking X to the interventions” (8).
Hoping And Despairing
Throughout the narratives, parents described struggling with conflicting feelings concerning their child with ASD, and their relationship with the child. Some of these thoughts and feelings were experienced as positive, like feelings of wonder and joy watching the child make progress. Parents felt pleased about the child's increased social awareness and enhanced communication skills, and, as a consequence, experienced less worry than previously. “We're not worried any more, never … We were before, when this whole thing started, but these past six months … this past year, our feelings have changed.” (4). Parents expressed feeling more confident in their parenting:
I think that when I have … when I see myself from another angle, like being at work, taking different courses, having so many duties to fulfill, plus the duties as a parent, plus working extra with X … then I realize how much work it actually requires. And it makes me feel stronger, seeing all the things I've accomplished. (5)
The narratives were also filled with sadness and distress concerning the child's difficulties. Parents described feeling constant worry about how the difficulties would affect the child's future life.
I don't know, really, that's what makes me worry the most. This autism of his, how is it going to affect his future? I'm worrying that maybe X will end up in the wrong place … I think about that a lot. (1)
Having to think about future demands and parental responsibilities was perceived as emotionally challenging. To handle difficult thoughts, parents described strategies they had developed, such as taking one day at a time, not planning too far ahead in time, or trying to stay positive:
I'm trying not to see the negative side, and try to think it's all going to work out. Even when it´s really hard. Like things are now, it's really, really tough. But I'm trying to stay positive, and do what I can. I do my best. Then … that's all there is to it. (8)
Discussion
Parents in the present study described going through a process, where the child's assessment and the subsequent intervention program were intertwined, thus not separate experiences. They experienced that their knowledge about ASD gradually grew and transformed into a deeper understanding of their child's needs. The new ways of understanding their child were perceived as triggering both positive and negative consequences, with regard to relationships within the family, as well as the parents' own emotions and well-being. The essence that emerged from the parents' narratives, new ways of understanding my child made life more hopeful and more challenging than before, is in many aspects consistent with results from other qualitative studies exploring experiences of parents caring for a child with ASD.18,19 Parenting a child with ASD has been reported in many studies as carrying with it numerous challenges and difficulties, and is often the source of emotional strain and psychological distress, while at the same time allowing for positive experiences of joy and personal growth.
The aim of the present study was to gain a deeper understanding of immigrant parents' experiences of having their child diagnosed with ASD and participating in a specific community intervention program. One of the main findings in our study, described in the subtheme never heard of autism, concerns the fact that some parents possessed no previous knowledge of the concept of ASD. This lack of knowledge seemed to affect their experience of the child's assessment and intervention program, as the challenge to achieve new knowledge and understanding of their child seemed more time-consuming and demanding. This finding is consistent with a recent qualitative study of Somali parents in the UK.28 However, the sample of parents in the present study is more diverse, as it includes parents born in several regions of the world. Interestingly, those parents who expressed a lack of knowledge of ASD were born in Africa or Middle Eastern countries, whereas parents from Eastern Europe did not. These findings pinpoint the importance of addressing parents' previous knowledge of ASD early in the assessment process, in order to provide adequate and individually tailored support to each family.
Another important finding in our study is described in the subtheme navigating service systems. The perceived difficulty in navigating Swedish support services such as health services, social security services, or available parental support provision may be linked to the parents' immigration background (all but two had arrived in Sweden as adults). This is in line with the experience of Somali parents in the study mentioned previously.28 However, the parents in the current study expressed satisfaction with the support they received from the intervention team in gaining access to services, such as finding information and contacting the services needed.
On the other hand, knowledge about the systems in themselves is not sufficient, which was shown in a previously mentioned study by Carlsson et al,32 conducted in the same city as the present study, but with a study sample consisting mainly of nonimmigrant parents. In the Carlsson et al's32 study, parents did not explicitly express a lack of knowledge about available support systems, but nevertheless perceived navigating the systems as challenging.
As well as being problematic for parents whose child has received a diagnosis, a lack of knowledge of available support systems is a common problem for immigrant parents on a general level, leading to delay in seeking help, and possibly causing underdiagnosis of immigrant or ethnic minority children showing signs of ASD.26,27 Providing information about ASD and other developmental disorders to immigrant parents, in addition to providing accessible assessment and treatment services, is equally important, in order to ensure early intervention.
The current study found that taking an active part in the child's interventions was considered important, and the main theme cooperating with the team describes the parents' experience of being involved in the child's interventions. As the evidence suggests that parental involvement is an important prognostic factor for the success of early behavioral interventions for children with ASD,14,16 this is a positive finding. The subtheme feeling important illustrates how parents described being able to influence their child's interventions. A conclusion made from these results is the need to not only adjust the interventions to suit the children's needs and abilities but also to modulate the interventions in accordance with the parents' resources and the family's life situation, as pointed out by Vivanti et al.15
Our study shows that parents whose children were offered both integrated assessment and interventions by the same local team, and individual support according to their needs, perceived the intervention program as helpful. They appreciated being able to get in touch easily, meeting the team in a location close to their homes, and staying in contact with the same professionals throughout the assessment as well as the subsequent interventions, factors which appeared to provide feelings of comfort and continuity illustrated in the theme being close. Studies have shown that in cases when assessment and intervention are provided in separate locations, parents experience uncertainty during transition periods and delays in receiving support.32,33
The first main theme, an overwhelming diagnosis, shows that emotional reactions experienced by parents upon learning about their child's diagnosis may vary, and that receiving an ASD diagnosis often elicits a range of emotions for parents to deal with. If parents have previously suspected the child's disability, the diagnosis might be experienced as a relief, a conclusion also drawn in a study by Russel and Norwich.48 However, several studies have shown that the child's ASD diagnosis often evokes ambivalent feelings.23,32,49 One reflection made during the analysis of the present study was that parents who did not initiate their child's assessment, but were referred by someone else, might have reacted with more negative emotions than parents who initiated the assessment themselves. Parents in the present study also expressed feeling afraid of telling others about the child's diagnosis, because of fear of meeting judgmental attitudes in family or friends, which is illustrated in the subtheme fearing stigma. The importance of understanding cultural views of ASD, and the need to raise awareness and reduce stigma has been indicated, in order to prevent families from delaying to seek help.28 The parents' previous knowledge of ASD is likely dependent on their country of origin, culture, and educational background, which is yet another reason to explore parents' previous awareness and beliefs of ASD early in the assessment process, in order to reduce the fear of stigmatization.
Parents experienced positive as well as negative consequences while being involved in the community assessment and intervention program, which is described in the third main theme growing as a parent. They expressed a challenging day-to-day life, where time and energy were never sufficient, and a lack of opportunity to regain energy. A constant feeling of insufficiency in regards to meeting the child's needs as well as the rest of the family's needs, seems to be a common source of stress experienced by many parents of children with ASD.19,22 Despite the challenging day-to-day life, parents in the present study described positive experiences, such as learning how to organize daily life in more efficient ways, developing new ways of interacting with their child, and contributing to their child's progress. Feelings of joy and hope for the future were expressed by some parents, which is in accordance with a study by Altiere and von Kluge.23 Another positive consequence experienced by parents was how it affected relationships within the family, outlined in the theme bringing the family together. Results from studies on the impact on the marital relationship for parents raising a child with ASD have been conflicting. Hock et al50 found that the marital relationship was strengthened by the couples' mutual struggle for their child with ASD, while Myers et al51 found that couples in the same situation were challenged in their marital relationship, and that this was a common cause of divorce. In the current study, parents described that their marriage was strengthened. It would be interesting to explore further whether this is linked to the parents' involvement in the community intervention program, or whether there were other factors that explain their experience of a strengthened marital relationship.
More studies are required in order to gain further understanding of immigrant parents' perceptions of early assessment and intervention for children with ASD. The need for individualized assessment and intervention is recognized, as can be seen with the Canadian program described by Sritharan and Koola,52 which, like the intervention program described in the present study, offers a culturally sensitive intervention program to immigrant families of children with ASD.
Strengths And Limitations
As the current study uses qualitative methodology, the variation in background among the sample population, such as years of schooling, time since migration, and regions of birth, presents as a strength. A larger sample of parents might have contributed to still more aspects of parents' lived experiences coming to light, because both children with ASD and immigrant parents are population groups with great diversity. The downside of heterogeneity of the participants is that it limits the conclusions that can be made. However, as a qualitative method was used, generalization of the results cannot be expected. Two of the interviews were conducted through an interpreter, which was considered both a strength and a limitation. The strength being that all parents who were involved in the intervention program were invited to participate in the study. The inclusion of interpreted interviews however confers a risk of losing the parents' own words and narratives. By contracting experienced interpreters to work alongside an interviewer, also experienced in working with an interpreter, our intention was to minimize that risk. The parents in the present study expressed a range of positive experiences of being involved in the local intervention program. One might question whether the fact that the intervention was still ongoing may have affected their truthfulness. However, this was alleviated by the fact that the interviewer was not personally involved in the intervention program.
Conclusion
This study describes the experiences of immigrant parents in Sweden participating in a community assessment and intervention program for preschool children with ASD. Their experiences are partly universal, shared by many parents raising children with ASD in other parts of the world. However, our findings reveal the unique experiences and challenges for this group of parents. Above all, parents in the study described that participating in the community assessment and intervention program, provided close to the families' homes, was experienced as easily accessible and overall helpful. Parents appreciated the support they were provided to lessen the burden of navigating service systems, especially as they experienced a lack of knowledge of available resources as a barrier. This highlights the need for comprehensive societal support for immigrant parents. Due to parents' varying knowledge and preconceptions of ASD, the information and support provided to immigrant parents also need to be adequate and considered early in the assessment process. The study shows that interventions for children with ASD should be individually tailored according to the child's needs as well as the parent's resources and life situation. More research is needed in order to understand the complexity of challenges faced by immigrant parents and their varying needs of support.
Ethics Approval And Informed Consent
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Prior to the beginning of data collection, the study was approved by the Regional Ethics Committee in Gothenburg, Sweden. Written informed consent was obtained from each individual participant included in the study.
Acknowledgments
We would like to express our sincere gratitude to all participating parents for making this study possible. We would also like to thank the previous head of the Central Child Health Care Unit in Gothenburg, Thomas Arvidsson, and the previous head of the Psychologists for Maternal and Child Health Care, Antonia Reuter, for encouragement and support.
Author Contributions
ÅN conceived the study; participated in its design, coordination, collection, and interpretation of data; and drafted the manuscript. MJ participated in the design of the study, the interpretation of data and drafting the manuscript. PL conceived the study and participated in its coordination. CG participated in the design of the study and reviewing the manuscript. GN conceived the study, participated in its design and the literature review. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
2. Coleman M, Gillberg C. The Autisms.
3. Baird G, Simonoff E, Pickles A, et al. Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: the Special Needs and Autism Project (SNAP). Lancet. 2006;368(9531):210–215. doi:10.1016/S0140-6736(06)69041-7
4. Christensen DL, Baio J, Van Naarden Braun K, et al. Prevalence and characteristics of autism spectrum disorder among children aged 8 years - Autism and Developmental Disabilities Monitoring Network, 11 sites, United States, 2012. MMWR Morb Mortal Wkly Rep. 2016;65(3):1–23. doi:10.15585/mmwr.ss6503a1
5. Barnevik-Olsson M, Gillberg C, Fernell E. Prevalence of autism in children of Somali origin living in Stockholm: brief report of an at-risk population. Dev Med Child Neurol. 2010;52(12):1167–1168. doi:10.1111/j.1469-8749.2010.03812.x
6. Crafa D, Warfa N. Maternal migration and autism risk: systematic analysis. Int Rev Psychiatry. 2015;27(1):64–71. doi:10.3109/09540261.2014.995601
7. Fairthorne J, de Klerk N, Leonard HM, Schieve LA, Yeargin-Allsopp M. Maternal race-ethnicity, immigrant status, country of birth, and the odds of a child with autism. Child Neurol Open. 2017;4:1–9. doi:10.1177/2329048X16688125
8. Magnusson C, Rai D, Goodman A, et al. Migration and autism spectrum disorder: population-based study. Br J Psychiatry. 2012;201:109–115. doi:10.1192/bjp.bp.111.095125
9. Barbaro J, Dissanayke C. Autism spectrum disorders in infancy and toddlerhood: a review of the evidence on early signs, early identification tools, and early diagnosis. J Dev Behav Pediatr. 2009;30(5):447–459. doi:10.1097/DBP.0b013e3181ba0f9f
10. Fernell E, Eriksson MA, Gillberg C. Early diagnosis of autism and impact on prognosis: a narrative review. Clin Epidemiol. 2013;5:33–43. doi:10.2147/CLEP.S41714
11. Volkmar FR, Reichow B. Infants and toddlers with autism: the promise and the challenges. Int J Speech Lang Pathol. 2014;16(1):11–14. doi:10.3109/17549507.2013.862859
12. Gillberg C. The ESSENCE in child psychiatry: early symptomatic syndromes eliciting neurodevelopmental clinical examinations. Res Dev Disabil. 2010;31(6):1543–1551. doi:10.1016/j.ridd.2010.06.002
13. Ismail FY, Fatemi A, Johnston MV. Cerebral plasticity: windows of opportunity in the developing brain. Eur J Paediatr Neurol. 2017;21:23–48. doi:10.1016/j.ejpn.2016.07.007
14. Estes A, Vismara L, Mercado C, et al. The impact of parent-delivered intervention on parents of very young children with autism. J Autism Dev Disord. 2014;44(2):353–365. doi:10.1007/s10803-013-1874-z
15. Vivanti G, Prior M, Williams K, Dissanayake C. Predictors of outcomes in autism early intervention: why don’t we know more? Front Pediatr. 2014;2(58):1–10. doi:10.3389/fped.2014.00058
16. Wallace KS, Rogers SJ. Intervening in infancy: implications for autism spectrum disorders. J Child Psychol Psychiatry. 2010;51(12):1300–1320. doi:10.1111/j.1469-7610.2010.02308.x
17. Corcoran J, Berry A, Hill S. The lived experience of US parents of children with autism spectrum disorders: a systematic review and meta-synthesis. J Intellect Disabil. 2015;19(4):356–366. doi:10.1177/1744629515577876
18. DePape A-M, Lindsay S. Parents’ experiences of caring for a child with autism spectrum disorder. Qual Health Res. 2015;25(4):569–583. doi:10.1177/1049732314552455
19. Ooi KL, Ong YS, Jacob SA, Khan TM. A meta-synthesis on parenting a child with autism. Neuropsychiatr Dis Treat. 2016;12:745–762. doi:10.2147/NDT.S100634
20. Bonis S. Stress and parents of children with autism: a review of literature. Issue Ment Health Nurs. 2016;37(3):153–163. doi:10.3109/01612840.2015.1116030
21. Yirmiya N, Shaked M. Psychiatric disorders in parents of children with autism: a metaanalysis. J Child Psychol Psychiatry. 2005;46(1):69–83. doi:10.1111/jcpp.2005.46.issue-1
22. van Tongerloo MAMM, van Wijngaarden PJM, van der Gaag RJ, Lagro-Janssen ALM. Raising a child with an autism spectrum disorder: “If this were a partner relationship, I would have quit ages ago”. Fam Pract. 2015;32:88–93. doi:10.1093/fampra/cmu076
23. Altiere MJ, von Kluge S. Searching for acceptance: challenges encountered while raising a child with autism. J Intellect Dev Disabil. 2009;34(2):142–152. doi:10.1080/13668250902845202
24. Hartley SL, Schultz HM. Support needs of fathers and mothers of children and adolescents with autism spectrum disorder. J Autism Dev Disord. 2015;45:1636–1648.
25. Westman Andersson G, Miniscalco C, Gillberg N. A 6-year follow-up of children assessed for suspected autism spectrum disorder: parents´experiences of society´s support. Neuropsychiatr Dis Treat. 2017;13:1783–1796.
26. Jo H, Schieve LA, Rice CE, et al. Age at autism spectrum disorder (ASD) diagnosis by race, ethnicity, and primary household language among children with special care needs, United States, 2009–2010. Matern Child Health J. 2015;19:1687–1697.
27. Magaña S, Lopez K, Aguinaga A, Morton H. Access to diagnosis and treatment services among Latino children with autism spectrum disorders. Intellect Dev Disabil. 2013;51(3):141–153. doi:10.1352/1934-9556-51.3.141
28. Fox F, Aabe N, Turner K, Redwood S, Rai D. “It was like walking without knowing where I was going”: a qualitative study of autism in a UK Somali migrant community. J Autism Dev Disord. 2017;47:305–315. doi:10.1007/s10803-016-2952-9
29. Broberg M, Norlin D, Nowak H, Starke M. Riktat föräldrastöd: RiFS-projektets slutrapport, en aktionsforskningsansats för att kartlägga behov och förbättra stödet till föräldrar som har barn med funktionsnedsättning [Targeted Parent Support: RiFS Project Final Report, an Action Research Effort to Map Needs and Improve Support for Parents of Children with disabilities]. Gothenburg: FoU i Väst; 2014.
30. Lin S, Yu S, Harwood R. Autism spectrum disorders and developmental disabilities in children from immigrant families in the United States. Pediatrics. 2012;130(2):191–197. doi:10.1542/peds.2012-0900R
31. Nygren G, Sandberg E, Gillstedt F, Ekeroth G, Arvidsson T, Gillberg C. A new screening programme for autism in a general population of Swedish toddlers. Res Dev Disabil. 2012;33:1200–1210. doi:10.1016/j.ridd.2012.02.018
32. Carlsson E, Miniscalco C, Kadesjö B, Laakso K. Negotiating knowledge: parents´ experience of the neuropsychiatric diagnostic process for children with autism. Int J Lang Commun Disord. 2016;1–12.
33. Jimenez ME, Barg FK, Guevara JP, Gerdes M, Fiks AG. Barriers to evaluation for early intervention services: parent and early intervention employee perspectives. Acad Pediatr. 2012;12(6):551–557. doi:10.1016/j.acap.2012.08.006
34. Carr T, Shih W, Lawton K, Lord C, King B, Kasari C. The relationship between treatment attendance, adherence, and outcome in a caregiver-mediated intervention for low-resourced families of young children with autism spectrum disorder. Autism. 2016;20(6):643–652. doi:10.1177/1362361315598634
35. SCB/Gothenburg City Council. Göteborgsbladet 2018. In: Stadsledningskontoret, editor. Gothenburg: Göteborgs Stad; 2018. Available from: http://statistik.goteborg.se/Statistik/Faktablad/Goteborgsbladet/. Accessed March 1, 2019. Swedish.
36. Westman Andersson G, Miniscalco C, Johansson U, Gillberg C. Autism in toddlers: can observation in preschool yield the same information as autism assessment in a specialised clinic? ScientificWorld J. 2013;2013:1–7.
37. Dawson G, Jones EJH, Merkle K, et al. Early behavioral intervention is associated with normalized brain activity in young children with autism. J A Acad Child Adolesc Psychiatry. 2012;51(11):1150–1159. doi:10.1016/j.jaac.2012.08.018
38. Dawson G, Rogers S, Munson J, et al. Randomized, controlled trial of an intervention for toddlers with autism: the Early Start Denver Model. Pediatrics. 2010;125(1):17–23. doi:10.1542/peds.2009-0958
39. Rogers SJ, Dawson G. Early Start Denver Model for Young Children with Autism: Promoting Language, Learning and Engagement. New York: Guilford Publications; 2010.
40. Spjut Jansson B, Lindahl U, Nilsson Rutberg M. Manual för Intensivinlärning för små barn med autism [Manual for Intensive Learning for Young Children with autism]. Gothenburg: Habilitering och Hälsa; 2011.
41. Spjut Jansson B, Miniscalco C, Westerlund J, Kantzer AK, Fernell E, Gillberg C. Children who screen positive for autism at 2.5 years and receive early intervention: a prospective naturalistic 2-year outcome study. Neuropsychiatr Dis Treat. 2016;12:2255–2263. doi:10.2147/NDT.S108899
42. Kvale S, Brinkmann S. InterViews: Learning the Craft of Qualitative Research Interviewing.
43. Lindseth A, Norberg A. A phenomenological hermeneutical method for researching lived experience. Scand J Caring Sci. 2004;18:145–153. doi:10.1111/scs.2004.18.issue-2
44. Ricoeur P. Interpretation Theory: Discourse and the Surplus of Meaning. Fort Worth: Texas Christian University Press; 1976.
45. Björk Brämberg E, Dahlberg K. Interpreters in cross-cultural interviews: a three-way coconstruction of data. Qual Health Res. 2013;23(2):241–247. doi:10.1177/1049732312467705
46. Malterud K. Qualitative research: standards, challenges, and guidelines. Lancet. 2001;358(9280):483–488. doi:10.1016/S0140-6736(01)05627-6
47. Edhlund BM, McDougall AG. NVivo 10 Essentials. Stallarholmen: Form & Kunskap AB; 2013.
48. Russell G, Norwich B. Dilemmas, diagnosis and de-stigmatization: parental perspectives on the diagnosis of autism spectrum disorders. Clin Child Psychol Psychiatry. 2012;17(2):229–245. doi:10.1177/1359104510365203
49. O´Brien M. Ambiguous loss in families of children with autism spectrum disorders. Fam Relat. 2007;56:135–146. doi:10.1111/j.1741-3729.2007.00447.x
50. Hock R, Timm T, Ramisch J. Parenting children with autism spectrum disorders: a crucible for couple relationships. Child Fam Soc Work. 2012;17(4):406–415. doi:10.1111/j.1365-2206.2011.00794.x
51. Myers B, Mackintosh V, Goin-Kochel R. ‘‘My greatest joy and my greatest heart ache:’’ Parents’ own words on how having a child in the autism spectrum has affected their lives and their families’ lives. Res Autism Spectr Disord. 2009;3:670–684. doi:10.1016/j.rasd.2009.01.004
52. Sritharan B, Koola MM. Barriers faced by immigrant families of children with autism: a program to address the challenges. Asian J Psychiatr. 2019;39:53–57. doi:10.1016/j.ajp.2018.11.017
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.