Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 14
Experiences and Perceptions on Community Client-Led ART Delivery (CCLADS) Model of Antiretroviral (ART) Delivery: Patients’ and Providers’ Perspectives in South Western Uganda
Authors Kasande M ![]() , Taremwa M, Tusimiirwe H, Lamulatu K, Amanyire M, Nakidde G
, Taremwa M, Tusimiirwe H, Lamulatu K, Amanyire M, Nakidde G ![]() , Kabami J
, Kabami J ![]()
Received 23 August 2022
Accepted for publication 11 November 2022
Published 18 November 2022 Volume 2022:14 Pages 539—551
DOI https://doi.org/10.2147/HIV.S387190
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Meble Kasande,1 Michael Taremwa,1 Happiness Tusimiirwe,1 Kabiite Lamulatu,1 Mark Amanyire,1 Gladys Nakidde,1 Jane Kabami1– 3
1Faculty of Nursing and Health Sciences, Bishop Stuart University, Mbarara city, Uganda; 2Department of Nursing, Kabale University School of Medicine, Kabale, Uganda; 3Infectious Diseases Research Collaboration, Kampala, Uganda
Correspondence: Jane Kabami, Tel +256706315810, Email [email protected]
Purpose: Community Client-Led ART Delivery groups (CCLADS) were introduced as part of the differentiated service delivery models in 2017 to better serve growing number of HIV patients and reduce unnecessary burden on the HIV care delivery system. However, there is limited evidence on the exact patients’ and care providers’ experiences and perceptions regarding the CCLADS model of ART delivery. We therefore aimed to explore the experiences and perceptions on CCLADS model from the patient and provider perspectives.
Participants and Methods: A descriptive qualitative study was conducted at two ART clinics in Southwestern Uganda. We conducted in-depth interviews (IDI) to get a deeper understanding of the patient and providers’ perspective regarding the model. Responses from participants were recorded using audio recorders and were translated and transcribed. We used thematic approach to analyze the data.
Results: A total of 20 in depth interviews were conducted, with providers, CCLAD leaders and Adults Living with HIV (ALHIV) to assess the experiences and perceptions to participation among People Living with HIV (PLHIV) enrolled in CCLADS and the care providers. Key themes included benefits, limitations, experiences and perceptions of CCLADS. Benefits to ALHIV included: Longer refills, reduced transport costs, receive drugs in time, peer advice; to providers: time saving, less tiresome and reduced congestion at facility. Barriers included: stigma, limited outreaches, failure to comply. Patients perceived the model positively (cost effective, improved quality care, no missed appointment where as others were negative (blood samples not taken like before). Experiences also included enough time, learnt some activities and good adherence.
Conclusion: Participation in the CCLADS groups provides several benefits to the patient including reduced transport, longer refills and good adherence. Stigma remains a challenge to CCLADS participation, which requires innovative and collaborative strategies from Ministry of Health (MOH) and implementation partners to address in order to sustain CCLADS participation.
Keywords: CCLADs, community client led ART delivery models, participation, adult HIV people
Introduction
Sub-Saharan Africa is one of the most burdened regions with HIV/AIDS, and ART service delivery puts a lot of pressure on the health system. Among the 38.9 million people living with HIV globally in 2021, 62% were accessing lifesaving Antiretroviral Therapy (ART) and 53% are virally suppressed.1,2 In the Same year (2018), Uganda registered an estimated 1.4 million people who were living with HIV, 1,190,000 (72%) of who were accessing ART and the viral load suppression was at 64.1,2 This heavy burden of disease translates into higher cost of care, patient congestion, and long waiting times at the health centers.3
The World Health Organization (WHO) recommended differentiated HIV service delivery as a novel evidence based strategy to reduce congestion at the facility ART clinic, promote meaningful involvement of People Living with HIV (PLWHIV), and to enhance patients’ self-management.4,5 The differentiated delivery models included Community Client-Led ART Delivery Groups (CCLADs), Community Drug Distribution Points (CDDPs), Facility-Based Groups (FBGs), and Facility-Based Individual Management (FBIM).6–8 In Uganda CCLADs have been implemented as one of the differentiated service delivery (DSD) model since 2017 by the ministry of health.1,4 This is a client centered approach to improve on the quality of care through provision of ART delivery while acknowledging specific drivers and barriers to empower patients to manage their disease with the support of the health system.9–14
Each CCLAD group consists of between 4 and 8 HIV positive patients who come from the same community with a group leader who must have been consistently on ART, selected by the health care provider. The collection of ART regimens at each refill for all the group members from the facility is done by only one member who then it’s the group leader who distributes to the others.
HIV differentiated care might be influenced by many factors such as stigma, quality of care among health workers and transport among others.15 These may affect, retention in care for many patients leading to loss to follow up, defaulting ART and eventually failing to achieve viral load suppression.16 However, there is little research about the benefits and limitations to participation in order to maximize the benefits of CCLADS.17,18 We assessed these benefits and barriers to participation in Community Client Led ART Delivery (CCLAD) groups among adult patients who are enrolled in CCLADs in two high volume facilities from two districts in South-Western Uganda. The findings from this study are critical in addressing critical barriers to participation by designing innovative and collaborative strategies in order to sustain CCLADS participation and its optimal benefits.
Materials and Methods
Study Design and Setting
This was a descriptive qualitative study conducted among adult HIV patients enrolled in CCLADS, health workers and CCLAD leaders in Bushenyi and Rubirizi Health Centre (HC) IVS in south western Uganda enrolled in CCLADS. Bushenyi Health Centre IV is located in Bushenyi district, approximately 300km from Kampala, Uganda’s capital, and about 75km from Mbarara, western Uganda. Rugazi Health Centre IV, is located in Rubirizi district, also in Western Uganda, approximately, 97km from Mbarara. In Uganda, Health Centre IV facilities serve a catchment population of over 100,000 people, headed by a medical officer and serve as a referral centre for lower level facilities from HC III and below. They offer all services with a fully functioning HIV clinic with approximately 1500 HIV positive active clients registered.
Geographically, these Health Centres are located in districts with one of the highest HIV prevalence (Bushenyi; 6.8% and Rubirizi; 7.1%) (Ministry of Health, Uganda, 2021) which is higher than the national prevalence of 5.5% (UPHIA Report, 2020). In addition, the two HCIVs have been implementing CCLADs model since 2018.
The CCLDs model enrolls stable patients following a detailed health education talk by responsible workers. These explain the advantages, disadvantages and how these models operate. So, those who admit to join form groups of 4–8 people and chose a CCLAD leader who has disclosed their status to everyone and is no longer stigmatized by their status. The group members alternate the responsibility of going for ART refills and after that they gather at a selected place, distribute their ART and share peer advice and encouragement to each other to improve ART adherence.
Study Population and Sample Size
We collected data from adult HIV patients aged 18 to 65 years receiving HIV care and treatment from the two health centre fours (IVs) of Bushenyi and Rugazi. We included adults who were considered stable “patients receiving ART for at least a year with no HIV comorbidities” and also enrolled in CCLADS. We conducted a total of 20 in-depth interviews on participants; 8 interviews on CCLAD leaders, 8 interviews on patients and 4 interviews on providers. This was considered a sufficient sample and saturation was reached.
Data Collection Procedures
We developed interview guides using information from previous studies. We pretested our semi structured interview guides at Mbarara municipal Health Centre IV and this helped us in adjusting and modifying on the questions developed to suit the context and objectives of the study. All patients provided informed consent to participate in the study, Interview guides were used for the data collection. A total of 20 participants were purposively selected to participate in the in-depth interviews and data was collected using research assistants for a period of 2 months from May to July 2021. All the IDIs were audio recorded by the research assistants and later transcribed and translated verbatim into meaningful transcripts.
We conducted in-depth interviews (IDI) to get a deeper understanding and explore the experiences and perceptions regarding the CCLADS from the patient and provider perspective. We used interview guides to interview participants who were involved in CCLADs. We specifically conducted in-depth interviews (IDIs) due to the sensitivity of the study population, since there still exists social and internal stigma among the victims and this would limit free interaction if at all we opted for focus groups. IDIs helped us to gain a deeper understanding on the benefits, limitations, and perceptions of CCLADs engagement and participation from the perspective of both the patients and providers.
Interaction with the Participants
We worked with health providers in the HIV clinics to generate a list of all HIV patients enrolled in the CCLAD model of ART delivery. We reached out to these adult HIV participants in the ART clinics through phone calls. Those who responded were given appointments and were consented to participate in the study. We also interviewed other patients were had come to the clinics on their routine clinic visit day. All participants enrolled in the study provided a verbal and written informed consent to participate in the study. privacy was ensured by using private rooms for the interviews, participation was voluntary and no names or any patient identifiers were used during the interviews, neither are they used anywhere during the publication process.
Data Management and Analysis
All the interviews were audio recorded and transcribed verbatim by the research assistants who conducted the interviews. We read through the transcripts while listening to the recording, correcting errors, anonymizing the data (eg, names, places) and inserting notations for pauses, laughter and punctuations. Field notes were used to include the nonverbal or contextual issues. Coding was manually done grouping similar quotes together under the broad themes (benefits, limitations and improvement in quality of care identifying the similarities and differences revealed through the participants’ narratives, eliminating duplicates, and ensuring inclusion of data from different sources.
We selected direct quotes that we thought were representative of the participant’s views and included them in the results. This was done by listening to the audio recordings of all participants and identifying those that were repetitive, and the number of respondents who expressed similar ideas, examining their level of emphasis and tone of voice. Overall, we followed four major steps and was largely iterative process. The first step involved data familiarization through multiple readings of interview transcripts. The second step entailed generating a coding framework. Codes were inductively generated from the interview transcripts. The third stage was that of abstracting the coded data into thematic categories and lastly making meaning out of the different codes and themes.
Ethical Consideration
Ethical clearance and approval were provided by the Ethical Review Committee of Mbarara University of Science and Technology and Ugandan National Council on Science and Technology. Voluntary written informed consent was obtained from all participants for participation in the study. This study was conducted in accordance with the declaration of Helsinki. The research team also sought permission from the faculty of nursing and health sciences, department of nursing sciences of Bishop Stuart University. We also sought administrative clearance from the district health officers and in charges of the participating facilities of Rugazi and Bushenyi Health Centre IVs to allow the process of data collection within the study facilities. In addition, the confidentiality of participants was maintained by removing patient identifiers from the questionnaire and keeping the filled data secure.
Results
A total of 20 in-depth interviews were conducted exploring experiences and perceptions associated with CCLADS participation and retention in care. We interviewed 4 health providers, 6 CCLADS leaders and 10 patients to gain a deeper understanding on their participation and engagement but also their perceptions on CCLADS. There was an equal participation (8) at 50% of both female and male patients, 3 male providers and one female. The mean age of the participants was 43 and there was a standard deviation of 15.47. Participants who had attained primary level of education were more at 50%, 28% had no formal education and were involved in farming since 57.1% were peasants. 28.6% of the participants who participated in the study were married (Table 1).
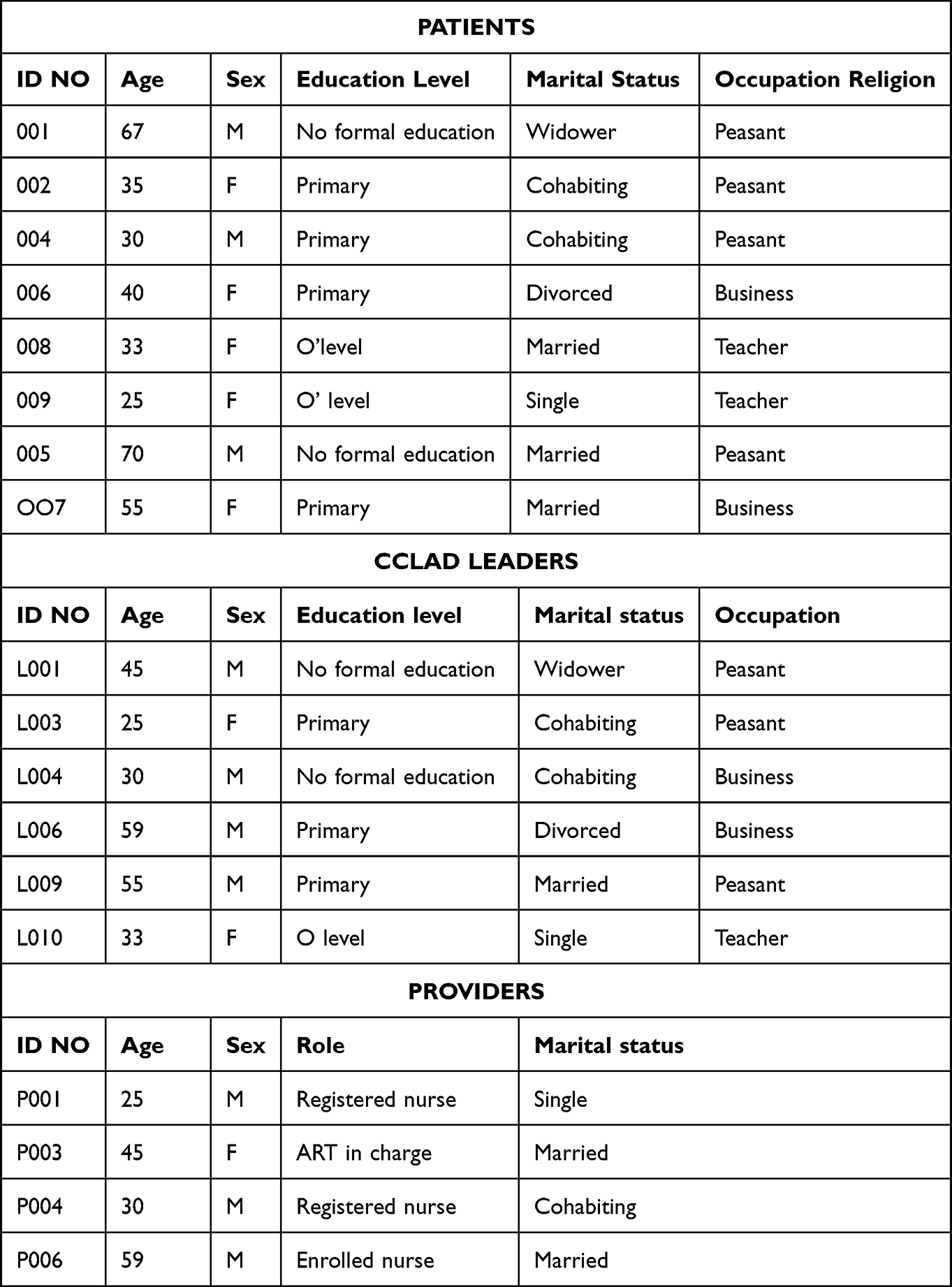 |
Table 1 Socio-Demographic Characteristics of Adult HIV Patients in CCLADs and Their Providers |
From the results, two major themes emerged from participant experiences; a) Benefits of CCLADS participation with subthemes of benefits to participants and benefits to providers including longer refills to the patients and reduced congestion at the facilities; b) Limitations to CCLADs participation with stigma as a subtheme and; c) Improved Quality of Care.
Several benefits were highlighted by both the patients and providers. They included: longer ART refills, reduced transport costs, receiving drugs in time, reduced congestion at facility, advice from health workers and fellow group members and special consideration at the facility.
On the other hand, they also faced some limitations to participation in the CCLADs like stigma among the group members, reduced drug stocks, longer duration during clinic days, Lack of transport to the facility, no materials like bags and patient’s failure to comply which would cause poor retention in care. The participants also mentioned some of the things that would be preventing other HIV stable members to enroll in CCLADs and mainly stigma emerged. Regarding the perceptions of participants towards CCLADs, one major theme of improved quality of care emerged from the data collected.
Theme 1: Benefits of Participation in the CCLADS
Subtheme 1: Benefits to Participants
The patients shared their experiences and benefits that they had had ever since they enrolled to CCLADs as follows;
Longer Refills for the CCLAD Members
The providers said that the CCLAD members are given longer refills since they are stable clients and this reduces frequenting at the facility on clinic days and the patients were happy to stay home and do their activities.
We give them 5-6 months refill depending on the stock levels. And by the way that was also a motivator, because clients in groups are given longer refills compared to those on clinic based model since they have no co morbidity and they are adhering well to ART p007.
In addition, the patients also said that it was helpful since they would take long without going to the facility which saves on their time and transport costs.
We are given a longer refill than before when we were still picking our drugs individually, we are now given a 3 months refill 003.
People Save Their Time for Doing Other Activities
Patients explained how being in CCLADS benefited them in a way that they could keep doing their work and still get their medication. This is mainly because on the clinic day, members keep rotating and it takes time to go to the facility.
The benefits I got, Time! Managing to do my works because when your colleague goes to pick for you medicine at the hospital and you stay at home, there is something useful you can do at home. For example I rear hens when I don’t go to the hospital for like a period of three months because someone else is collecting the medicine, I also do other things like going to my garden so I make sure I use the time productively, that’s one L010R.
Reduced Transport Costs to the Facility
Patients said that these CCLADs reduced on the transport cost in a way that they no longer spend a lot of money since they all contribute less money for only one person’
Also on transport, members have been relieved, because if one was using 10,000 shillings before, he/she now uses just 1000 shillings to contribute to the member’s transport who will be going to the clinic RL003.
You know when I was still picking my drugs from the clinic, I would spend about 7000 shilling on transport. And so from our training we were briefed how we would start contributing just 1000-2000 shillings for a member to pick for us our medication. So generally the model is cost effective 006.
Received Drugs in Time
The CCLADs model enabled the patients to receive timely drugs since they would always be when remaining with a few pills at the time of the next drug refill in order to retain them in care. The patients also added that they were receiving medications in time.
You know I always keep checking in the drug packs of all my members, and so when the pills reduce to like a balance of 1-2 pills, then that’s when I go to the clinic for a refill. I make it a point to go to the clinic before all pills are finished 007L.
Social Support
Patients reported that they were given counseling back at the hospital which encouraged them and they felt providers were thinking about them and during meetings; they give advice to themselves concerning personal issues.
For instance we advise members never to take their daily pills before eating something, and also to drink enough water. So generally, CCLAD group model is the best for HIV care delivery L003.
I cannot lie to you about our health providers, they welcome us well, and they always want to listen to our complaints, they also do the necessary counseling, you real feel that they want us to live longer 008.
Patients and providers also think that the model has helped to support patients who would otherwise not make it to the facility for their refills.
That time whenever you would be feeling weak, you would miss going to the clinic for your refill, unlike now when another member can help to pick for you drugs, whenever other members are not in position to 005.
Learnt Some Activities in the Group
Patients have learnt so many things like writing because to go the facility, you have to know how to read what is on the document, so they always train each other on different activities.
When we were starting those groups, some of the clients did not know how to write their names, but all members of our group now can read and write. Members have also developed a self-esteem, no more stigma p009.
Subtheme 2: Benefits to the Providers
From the experiences of providers as they implement the CCLADS model, they reported some benefits during care delivery.
Reduced Congestion at Facility
Our clients always confess that they have been saved from frequenting the facility because the clinic used to be so busy on every clinic visit, and that’s they would be delayed before they could be served.
When the patient numbers reduce, you have time to document, you also have enough time to talk and listen to the clients, because most patients have many health issues like Opportunistic Infections (OIs) among other infections p005.
Since all the people do not come to the facility at the same time on the clinic day, there is no longer congestion at the facility. Only one representative comes to the clinic and picks drugs on behalf of all CCLAD members.
We used to have overcrowding of clients on every HIV clinic day, but now that is no longer experienced. The clients themselves also tell us how they were relieved of transport costs, since they now can come to the clinic once in a year and one at a time p007.
Enough Time for the Health Providers
Providers say they are given more time since they now work on few patients compared to the ones they would work on before these had joined the CCLADS so they easily work on the few patients who are available.
When the patient numbers reduce, you have time to document, you also have enough time to talk and listen to the clients, because most patients have many health issues like Opportunistic Infections (OIs) among other infections p005.
Theme 2: Limitations to Participation in the CCLADS,
The different providers, leaders and the patients talked about the different limitations that they faced while participating in in the CCLADS.
Subtheme 1: Stigma
CCLAD leaders said that some of the group members did not want to go pick the medications when it was their turn to pick the drugs for other group members because they did not want people to see them picking drugs hence knowing them as positive HIV patients
The only challenge we have so far is stigma, as we gather up as group members in one place to pick our drugs or for any other health service, are always talked about in the community as people living with HIV 006.
In addition, some members lack confidence to disclose their status to their partners and this affects their care and they may end up leaving the model because they fear gathering in the group as they can be seen and identified by family and community members.
Before I was well enlightened, I got a man whom I actually have a child of 7 years with, so I had to hide him my HIV status. But after some time, I decided to go back to the clinic, I explained how I had dropped out of care, and then the providers reinstated me 001L.
Fear to Be Seen and Known by Community Members
Different clients shared what would be preventing adult HIV patients to join CCLADs. Most patients feared to be seen by community members and preferred not to be part of the CCLADS. From the interviews, Patients in CCLADs always gather up in one place for meetings or even when picking drugs, some of the group members tend to expose themselves and people in the community begin talking about them as people living with HIV which causes stigma to others who would like to join CCLADs.
Some people don’t like being known as people living with HIV, that’s why they fear groups because they think they will be exposed 009.
Reduced Drug Stocks at the Health Facilities
Sometimes the drugs are not enough at the health facility and yet some patients should be given for a six-month refill which would not be available for all the members and so the providers give them few drugs which will make them return to the facility earlier than they are supposed to return.
When CCLAD model came in the drug refills increased up to 3–6 months, and so the challenge comes when we do not have enough drug stocks P005.
Reduced Income Levels Among the Patients
As the group operates, they are supposed to solicit the money for transport however some members at the time of picking drugs, they fail to raise the money they are supposed to be contributing and this becomes hard for CCLAD leader to gather required money and meet the costs to reach the facility.
The challenge that we have in the group is lack of transport to the clinic, sometimes a member fails to raise even 100 shillings and I end up walking to the facility to pick drugs L003R.
the challenge that we have in the group is lack of transport to the clinic, sometimes a member fails to raise even 100 shillings and I end up walking to the facility to pick drugs L003R.
Lack of Materials Like Bags Where to Carry Drugs from
The providers said that normally they should pack the drugs a day before the patients come to the facility but that is not possible since they do not have those bags
You know we are supposed to pack drugs a day before the clinic day, but since we do not have where to pack those drugs, we have to wait for the clients to first come, so that we use the bags they will have come with. You can see we still have a gap there, since we cannot prepare to serve our clients in advance p004.
The same issue was talked about by the patients themselves that they actually lack bags where to carry drugs from since the numbers are many and the tins are also many.
We only improvise by borrowing a bag from friends, and the challenge that comes with that is that the person who gives the bag keeps inquisitive of what you would want to use the bag for. you know it’s hard now to carry over 15 tins of drugs 006.
Failure to Comply When Invited to the Facility
Since they are already in CCLADS and members have picked their drugs, they do not find reasons for them to respond when called by the providers like in cases of viral checkups. This is a challenge because at some point they will be virally suppressed and will be dropped out of CCLADS.
You know that disappoints me is when we are all invited at the clinic by the providers, but my other group members other than my wife fail to comply. It actually shows me that such people do not love themselves; they only need me to love them instead. They always think they are punishing government when instead they are punishing themselves L010.
Lack of Confidentiality
Some members in the group cannot keep quiet about what is happening when they meet, so they always go to other people talking about all the information that has been shared. Therefore, if a person had plans to join CCLADS, it would be difficult for them knowing that everyone will know about them.
There is when you find you’re in a group and one has rumor and when you leave they ask him what you were doing there and he says they were distributing medicines for HIV/AIDS and you find that he has spread the rumors 002.
Geographical Location of the Health Facility
Providers reported that people being near the hospital, it would not be ideal for them to join groups since its easy for them to reach the hospital without difficulty.
At some point it has improved retention, but only that we have very few clients so far that are in CCALD groups. Our catchment area here being town, people prefer to come for their drugs by themselves p004.
Theme 3: Improved Quality of Care
Since people who pick drugs are few, the quality of care provided is better than before when many HIV patients could congest at the facility and the providers work tirelessly without resting.
All clients in groups are happy with the model, they talk about how they no longer delay in the line for their refills, they are also happy that they no long spend on coming to the clinic so frequently, that they have now saved that money that would have been for transport p009.
Group leaders felt like the model had also improved on ART adherence among the patients enrolled in those CCLADS.
The group members have always been warned that whoever does not suppress will be chased away from the group. More so those clients who drink alcohol we do caution them to stop or they would be chased away from the group too, and by the way those clients do need to be warned and they eventually change for better adherence p005.
Clients felt good about the model this was reported by the providers and how the model has really helped them since it was implemented.
………because this model helped us last year when COVID-19 was at its highest pick. Since during that period there were transport challenges, therefore members of different groups would contribute money for transport, and they would give it to one person to pick for them drugs. So the retention remained un-interrupted, we therefore give credit to the CCLAD groups p004.
Patients say they no longer fear people to know them as people living with HIV so when they are attending the meetings, they do not find it stigmatizing in any way.
When HIV clients are still under clinic based, they tend to hide their HIV status from the community, but with groups, clients always meet more often in their groups which exposes them, and this tends to wipe away stigma p005.
another patient also said that,
We do not care if people get to know our status, we got used to our situation of being HIV positive, so even if other people in the community get to know 007L.
Discussion
This study assessed the providers and patients experiences and perceptions on participation in the CCLADS model in south western Uganda. The results were discussed following three major themes: From participant experiences; a) Benefits of CCLADS participation with subthemes of benefits to participants and benefits to providers including longer refills to the patients and reduced congestion at the facilities and; b) Limitations to CCLADs participation with stigma and one major theme of improved quality of care from participants’ perceptions.
Benefits of CCLADS Participation to Patients and Providers
Adequate time with the health provider was a satisfying experience reported because health providers have few patients to work on. Providers say they are given more time to focus on patient concerns without pressure since they now work on few patients compared to the ones they would work on before joining the CCLADS. It is known that patients are more satisfied with health care services overall when adequately given attention and their needs are met resulting in better health and psychological outcomes.19
It was noted that CCLADs model is time saving, patients take longer refills, they incur reduced transport costs, receive drugs in time, yet there is reduced congestion at facility. Similar findings were reported by Kintu hence more time to meet patient needs and improved care at the facility.21 The reduced congestion at facility is further supported by Kizito’s study that confirmed that longer waiting hours at the facility were highly associated with decision to join the CCLADS26 and the report from Jaffar which reported that health facility-based models are less appreciated and hinder patients from their uptake.27
Our study further revealed that patients no longer walk long distances and they receive encouragement advice from colleagues which is in agreement with Prust’s study in Malawi where patients reported reduced travel times and less congestion at health facilities.22 In addition, the CCLADS model has been reported to increase male involvement as reported by Kushemererwa.23 This is so important to patient motivation to stay in care, adhere to treatment and hence better health outcomes as also foreseen by WHO in the effort to increase the patients on treatment and to achieve viral load suppression in the UNAIDS 95-95-95 goal by 2030.24,25
The CCLADs further relieved patients from the high transport costs spent while coming at the facility since the amount of money they spend was not much as compared to the money spent before they joined CCLADs. This also reported from various related studies.21,23,26 In addition, patients receive drugs in time and this helps them not spend any day without taking the drug. The providers said that they always give the CCLAD members the drugs even when they are remaining with a few in their tins.
Longer refills of 5 to 6 months depending on drug stocks for the CCLAD members have been reported to significantly reduce the rate of frequent visits to the facility and to improve adherence outcomes to ART.5 Group leaders felt like the model had also improved on ART adherence among the patients enrolled in CCLADS thus improving the quality of life. These findings are in line with those from Dakum’s study that concluded that community ART treatments are associated with adherence and treatment outcomes.33
Special consideration at the facility was one of the major benefits experienced by CCLADs. CCLAD members are given first priority when they come to the facility and their blood samples are taken where they are tested for how they are faring with the viral load and this encourages them to have the morale to continuously pick the drugs for other members in CCLAD. Similarly, Brown et al in their study to assess factors predictive of successful retention in care of HIV positive men, it was realized that ART delivery systems are instrumental in decreasing logistical barriers to HIV care, support of flexible treatment environments, and accelerated linkage to care which is very crucial in ART treatment programs.28 In the same way, the CCLADs, one of the ART delivery system, eases linkage to care through special considerations of the members hence well motivated to collect drugs for others and to give important feedback to the facility.
These benefits also tally with Tom Decroo et al’s study, “Community-based antiretroviral therapy programs can overcome barriers to retention of patients and decongest health services in sub-Saharan Africa” who highlighted that these models provided cost effectiveness and sustainability of these patients in CCLADs and therefore these would improve drug accessibility, adherence, treatment outcomes29,30 and their retention in care31,32
Since all the people do not come to the facility on the clinic day, clients no longer congest the facility hence no longer experience delay at the clinic. Pascal Geldsetzer further stated that CCLADs have improved ART retention by reducing the time burden to the health workers.20 In addition, ART home delivery shortens waiting times and improve quality of care for even those in facility-based care by decongesting ART clinics, a good experience for health providers having more time to address patient concerns and needs.
Limitations to Participation in CCLADs
On the other hand, stigma among the CCLAD members where some of them fear to be seen and known by the group members as HIV patients was a major limitation reported. This is similar to a study done in Malawi where stigma still remained a major concern.34 Kizito’s study further emphasized that some patients still have not fully disclosed their status which prevents them from freely going to the meeting points to collect their refills associating it to lack of confidentiality.26
Different clients shared what would be preventing adult HIV patients to join CCLADs where stigma was more prominent and this made members prefer not to be part of the CCLADS. From the interviews, patients in CCLADs always gather up in one place for meetings or even when picking drugs, some of the group members tend to expose themselves and people in the community begin talking about them as people living with HIV which causes stigma to others who would like to join CCLADs which showed lack of confidentiality34. Also reduced drug stocks at the facility, leading to shorter refills which eventually make the CCLAD members frequent the facility and eventually causing missed appointments by some members. Timely and adequate health facility planning to make drug requisitions and orders is paramount to combat this critical issue while building confidence among CCLADs on the sustainability of the drug supply chain.
Participants’ Perceptions of Quality of Care at the Facility
Quality of care was perceived to be improved based on the fact that people who pick drugs are few, the quality of care provided is better than before when many HIV patients could congest at the facility and the providers work tirelessly without resting. Providers getting time to attend to patients concerns and needs is fundamental to satisfying their needs hence highly rating the care received.19
Stigma of patients in CCLADS was perceived by participants to be minimized. Patients said they no longer feared people to know them as people living with HIV. However, supporting studies to this cause were limited. The reduced stigma could be attributed to the health education talks to prepare them psychologically to help and support each other to make their access to health care easy and satisfying. So that, they see each other as one, with a common problem that has a common solution. People are reluctant to visit the facility due to the challenges with health facility-based care. With the CCLAD models, most patients felt relaxed with the ever-provided health care services and at times they tend not to respond when they are called by health workers.
The perception towards the CCLADs model was generally good for both the patients and the health workers. There was a reported Positive feeling as clients felt good about the model this was reported by the providers and they appreciated that the model has really helped them since it was implemented and patients feel comfortable about it. This is most likely due to the realized benefits to both the patients as well as the providers.
Study Limitations
The study being qualitative has limited generalizability of findings to a larger population. However, we were confident about the findings of the study because we were able to reach saturation; the in-depth qualitative inquiry gave a detailed understanding of both the patients’ and providers experiences, positive and negatives hence availing a broader understanding of their perspective to facilitate improved service delivery. We recommend a future mixed study in a larger study setting to increase generalizability.
Conclusion and Recommendations
The CCLADS ART delivery model is a highly appreciated model by both providers and patients involved. Positive experiences (benefits to both patients and providers) and negative experiences (limitations) were realized. Participants’ perceptions of improved quality of care were reported key findings.
We recommend continued flow of information in ART clinics using various means to increase awareness on the CCLADS model and its benefits to achieve optimal participation.
Abbreviations
CCLAD, Community Client Art Delivery Models; ART, Antiretroviral Therapy; HIV, Human Immunodeficiency Virus; HC IV, health centre IV; ALHIV, Adults Living with HIV.
Ethics and Consent for Participation Publication
We received Ethical approval from Mbarara University IRB before conducting any data collections under the reference MUREC 1/7. All participants involved in this study signed a written informed consent form that allowed them to participate in the study and also authorized to publish the data after meaningful analysis. Consent forms were translated to the local language understood by participants. All participation was voluntary. All participant data was de-identified for confidentiality issues and avoiding unintentional disclosures.
Acknowledgments
We thankfully acknowledge the administrative support we received from the two health facilities of Bushenyi HC IV and Rugazi HCIV, where this study was conducted. We thank our study participants for accepting to take part in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Research reported in this publication was supported by the Fogarty International Center (US Department of State’s Office of the US Global AIDS Coordinator and Health Diplomacy [S/GAC] and the President’s Emergency Plan for AIDS Relief [PEPFAR]) of the National Institutes of Health under Award Number R25TW011210. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Barnabas RV, Szpiro AA, van Rooyen H., et al. Community-based antiretroviral therapy versus standard clinic-based services for HIV in South Africa and Uganda (DO ART): a randomised trial. Lancet Global Health. 2020;8(10):e1305–e1315. doi:10.1016/S2214-109X(20)30313-2
2. Bain LE, Nkoke C, Noubiap JJN. UNAIDS 90–90–90 targets to end the AIDS epidemic by 2020 are not realistic: comment on “Can the UNAIDS 90–90–90 target be achieved? A systematic analysis of national HIV treatment cascades”. BMJ Global Health. 2017;2(2):e000227. doi:10.1136/bmjgh-2016-000227
3. Sikazwe I, Eshun-Wilson I, Sikombe K, et al. Retention and viral suppression in a cohort of HIV patients on antiretroviral therapy in Zambia: regionally representative estimates using a multistage-sampling-based approach. PLoS Med. 2019;16(5):e1002811. doi:10.1371/journal.pmed.1002811
4. Grimsrud A, Bygrave H, Doherty M, et al. Reimagining HIV service delivery: the role of differentiated care from prevention to suppression. J Int AIDS Soc. 2016;19(1):21484. doi:10.7448/IAS.19.1.21484
5. Sanwo O, Persaud NE, Nwaokoro P, et al. Differentiated service delivery models among PLHIV in Akwa Ibom and Cross River States, Nigeria during the COVID-19 pandemic: descriptive analysis of programmatic data. J Int AIDS Soc. 2021;24:e25820.
6. Vandendyck M, Motsamai M, Mubanga M. Community-based ART resulted in excellent retention and can leverage community em-powerment in rural Lesotho, a mixed method study. AIDS Res Treat Open J. 2015;2(2):44–50. doi:10.17140/HARTOJ-2-107
7. Kandasami S, Shobiye H, Fakoya A, et al. Can changes in service delivery models improve program quality and efficiency? A closer look at HIV programs in Kenya and Uganda. J Acquired Immune Deficiency Syndromes. 2019;81(5):533. doi:10.1097/QAI.0000000000002064
8. Hagey JM, Li X, Barr-Walker J, et al. Differentiated HIV care in sub-Saharan Africa: a scoping review to inform antiretroviral therapy provision for stable HIV-infected individuals in Kenya. AIDS Care. 2018;30(12):1477–1487. doi:10.1080/09540121.2018.1500995
9. Levi J, Raymond A, Pozniak A, Vernazza P, Kohler P, Hill A. Can the UNAIDS 90- 90-90 target be reached. Vancouver, Canada: International AIDS Society; 2015.
10. Hill A, Pozniak A. HIV treatment cascades: how can all countries reach the UNAIDS 90–90–90 target? Aids. 2015;29(18):2523–2525. doi:10.1097/QAD.0000000000000864
11. Geoffrey F, Nicoletta N, Chirowa F, et al. The effectiveness and cost-effectiveness of 3- vs. 6-monthly dispensing of antiretroviral treatment (ART) for stable HIV patients in community ART-refill groups in Zimbabwe: study protocol for a pragmatic, cluster-randomized trial. BMC. 2018;19:548.
12. Nachega JB, Adetokunboh O, Uthman OA, et al. Community-Based Interventions to Improve and Sustain Antiretroviral Therapy Adherence, Retention in HIV Care and Clinical Outcomes in Low- and Middle-Income Countries for Achieving the UNAIDS 90- 90-90Targets. Curr HIV/AIDS Rep. 2016;13:241–255. doi:10.1007/s11904-016-0325-9
13. Decroo T, Telfer B, Dores CD, et al. Effect of Community ART Groups on retention-in-care among patients on ART in Tete Province, Mozambique: a cohort study. BMJ open. 2017;8:e016800.
14. Pellecchia U, Baert S, Nundwe S, et al. ”We are part of a family”. Benefits and limitations of community ART groups (CAGs) in Thyolo, Malawi: a qualitative study. J Int AIDS Soc. 2017;1:21374.
15. Ehrenkranz P, Grimsrud A, Holmes CB, Preko P, Rabkin M. Expanding the vision for differentiated service delivery: a call for more inclusive and truly patient-centered care for people living with HIV. J Acquired Immune Deficiency Syndromes. 2021;86(2):147. doi:10.1097/QAI.0000000000002549
16. Pulido Tarquino IA, Venables E, de Amaral Fidelis JM, Giuliani R, Decroo T. ”I take my pills every day, but then it goes up, goes down. I don’t know what’s going on”: perceptions of HIV virological failure in a rural context in Mozambique. A qualitative research study. PLoS One. 2019;14(6):e0218364. doi:10.1371/journal.pone.0218364
17. Haynes RB, McDonald HP, Garg A, Montague P. Interventions for helping patients to follow prescriptions for medications. Cochrane Database of Systematic Reviews. 2002.
18. Zakumumpa H, Rujumba J, Kwiringira J, Katureebe C, Spicer N. Understanding implementation barriers in the national scale-up of differentiated ART delivery in Uganda. BMC Health Serv Res. 2020;20(1):1–16. doi:10.1186/s12913-020-5069-y
19. Kuipers SJ, Cramm JM, Nieboer AP. The importance of patient-centered care and co-creation of care for satisfaction with care and physical and social well-being of patients with multi-morbidity in the primary care setting Research volume. BMC Health Services. 19;2019.
20. Geldsetzer P, Francis JM, Ulenga N, et al. The impact of community health worker-led home delivery of antiretroviral therapy on virological suppression: a non-inferiority cluster-randomized health systems trial in Dar es Salaam, Tanzania. BMC Health Serv Res. 2017;17(1):160. doi:10.1186/s12913-017-2032-7
21. Kintu. AM, Ssewanyana AM, Kyagambiddwa T. Exploring drivers and barriers to the utilization of community client-led ART delivery model in South-Western Uganda: patients’ and health workers’ experiences. BMC Health Serv Res. 2021;20(1):1129. doi:10.1186/s12913-021-07105-9
22. Prust ML, Banda CK, Callahan K, et al. Patient and health worker experiences of differentiated models of care for stable HIV patients in Malawi: a qualitative study. PLoS One. 2018;13(7):e0196498. doi:10.1371/journal.pone.0196498
23. Kushemererwa J, Muwanguzi M, Atukunda EC, et al. Barriers and facilitators of male engagement in Community Client-Led Antiretroviral therapy Delivery groups (CCLADS) for HIV care and treatment in Southwestern Uganda: a qualitative study. BMC Health Services. 2022;2:87.
24. Ehrenkranz A, Rosen S, Boulle A, et al. The revolving door of HIV care: revising the service delivery cascade to achieve the UNAIDS 95- 95-95 goals. PLoS Med. 2021;18(5):e1003651. doi:10.1371/journal.pmed.1003651
25. UNAIDS. Global HIV Statistics FACT SHEET; 2022.
26. Kizito O, Sabiti L. Factors associated with uptake of community client-led ART delivery model at Mulago adult HIV clinic _ Mulago National Referral Hospital. Cogent Med. 2021;8:875.
27. Muwanguzi M. Rates of virological failure in patients treated in a home-based versus a facility-based HIV-care model in Jinja, southeast Uganda: a cluster-randomised equivalence trial. Lanchet. 2010;1:210.
28. Brown. MG. Factors predictive of successful retention in care among HIV-infected men in a universal test and-treat setting in Uganda and Kenya: a mixed methods analysis. PLoS One. 2019;14(1):e0210126.
29. Isabirye R. Barriers and Facilitators of Art Adherence AmongHiv Positive Patients in Community Client-led ArtDelivery Groups at Lira Regional Referral Hospital. Res Square. 2021;1:86.
30. Byansi W, Nabunya P, Muwanga J. The relationship between life satisfaction, personal health, quality of life, and medication adherence among adolescents living with HIV in southwestern Uganda. J Public Health. 2021;9:1–8.
31. Bock P, Gunst C, Maschilla L, et al. Retention in care and factors critical for effectively implementing antiretroviral adherence clubs in a rural district in South Africa. J Int AIDS Soc. 2019;22(10):e25396. doi:10.1002/jia2.25396
32. Decroo T, Kaelen S, van den Boogaard W, et al. Community-based antiretroviral therapy programs can overcome barriers to retention of patients and decongest health services in sub-Saharan Africa: a systematic review. Int Health. 2013;5:169–179. doi:10.1093/inthealth/iht016
33. Dakum P. Effect of community antiretroviral therapy on treatment outcomes among stable antiretroviral therapy patients in Nigeria: a quasi experimental study. PLoS One. 2021;8:e0250345.
34. Sande O, Burtscher D, Kathumba D, Tweya H, Phiri S, Gugsa S. Patient and nurse perspectives of a nurse-led community-based model of HIV care delivery in Malawi: a qualitative study. BMC Public Health. 2020;20(1):685. doi:10.1186/s12889-020-08721-6
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.