")
Back to Journals » Patient Preference and Adherence » Volume 17
Experience of Disease Acceptance in Chinese Patients with Newly Diagnosed Crohn’s Disease: A Descriptive Qualitative Study
Authors Wang Y , Liu J , Zhou Y
Received 9 July 2023
Accepted for publication 3 October 2023
Published 11 October 2023 Volume 2023:17 Pages 2523—2534
DOI https://doi.org/10.2147/PPA.S429663
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Ying Wang,* Jinghan Liu,* Yunxian Zhou
School of Nursing, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yunxian Zhou, School of Nursing, Zhejiang Chinese Medical University, 548 Binwen Road, Binjiang District, Hangzhou, Zhejiang, 310053, People’s Republic of China, Tel +86 571 86633121, Fax +86 571 86613674, Email [email protected]
Background: High levels of disease acceptance are important predictors of improved psychological well-being, treatment outcomes, and enhanced quality of life. Relatively few studies have focused on the process of disease acceptance in patients with Crohn’s disease (CD), particularly those who are newly diagnosed.
Purpose: To explore the disease acceptance process in newly diagnosed CD patients.
Patients and Methods: A descriptive qualitative approach was employed. Sixteen CD patients from 2 tertiary hospitals in Hangzhou, Zhejiang were recruited through purposive sampling using a maximum variation strategy. Semi-structured interviews were conducted. The interviews were transcribed verbatim and analysed using conventional content analysis.
Results: Five phases of the psychosocial process of the “acceptance journey” of newly diagnosed CD patients emerged from the data analysis: (1) praying for the illness to not be CD; (2) not being able to accept CD; (3) having to accept CD; (4) knowing that CD should be acceptable; and (5) starting to accept CD. Patients at the stage of “starting to accept CD” are more proactive and motivated to face the disease, and their overall acceptance of the disease is higher than that of the previous stages. However, by the end of the interview, 2 patients remained at the stage of “having to accept CD”, and 3 patients remained at the stage of “knowing that CD should be acceptable”. Two patients entered the stage of “starting to accept CD” and then reverted back to one of the previous stages.
Conclusion: The “acceptance journey” of newly diagnosed CD patients is dynamic, individual and reversible. Traditional Chinese cultural values such as respect for authority, the philosophy of wu-wei and family responsibility contribute to the acceptance of CD in Chinese patients. Hence, there is a need to provide early and culturally tailored psychological support or interventions according to the stages of acceptance.
Keywords: Crohn’s disease, conventional content analysis, disease acceptance, inflammatory bowel disease, qualitative study
Introduction
Disease acceptance is a multidimensional concept. Initially, it was defined as acceptance of loss.1 This definition was further developed as a willingness to be present with one’s illness-related thoughts, feelings, and bodily sensations without judging or making unnecessary attempts to control the disease.2 In the context of chronic illness, acceptance is defined as an awareness of the need to adapt to chronic illness, to tolerate the unpredictable and uncontrollable nature of the illness, to stop battling bodily discomfort, to actively refocus on other aspects of daily life and to integrate chronic illness into one’s life.2 From a psychological adjustment perspective, acceptance is primarily about adapting to the potential limitations and difficulties caused by the illness, maintaining an optimistic attitude, positively perceiving the benefits of the illness and restarting an active life.3 Disease acceptance is an important part of the illness process and a key factor in patients’ psychosocial adjustment, and high levels of disease acceptance promote better adjustment to illness and are important predictors of improved psychological well-being, treatment outcomes and enhanced quality of life.4–6 For patients with chronic diseases, illness can persist for a lifetime, and accepting the disease is not easy.
Crohn’s disease (CD) is a chronic nonspecific bowel disease that belongs to the same category of inflammatory bowel disease (IBD) as ulcerative colitis (UC). The disease is recurrent and lifelong, and patients often suffer from symptoms such as diarrhea and mucopurulent bloody stool. Treatments such as hormonal therapy and nasogastric feeding bring about changes in self-image, dietary restrictions and reduced social participation, and the high costs of disease treatment impose psychological stress on patients.7–9 This seriously affects patients’ physical and mental health and quality of life and generates a heavy economic burden for individuals, families and society. The prevalence of individuals with IBD in the Western world is expected to be as high as 1% in 2030.10 The incidence of IBD in newly industrialized countries is lower than that in the Western world; however, the rate of the rise in IBD incidence is considerably higher.11 It is expected that China will have more than 1.5 million IBD cases by 2025.12
To date, relatively few studies have focused on illness acceptance in patients with IBD. A study of UC patients showed a moderate level of disease acceptance as evaluated by the Acceptance of Illness Scale.13 The 6-item acceptance subscale of the Illness Cognition Questionnaire has also been used to assess illness acceptance among IBD patients.14 Factors influencing disease acceptance in patients with chronic diseases include demographic and disease characteristics, psychological resilience, stigma, and cognitive emotion regulation.2–6,13,15 UC patients with higher education who were professionally active and treated conservatively accepted their disease better.13 IBD patients experiencing loss reported lower illness acceptance than those experiencing resilience and thriving.15 A qualitative study showed that through downwards social comparison, some patients developed a mindset that they were not alone, and they derived confidence from the positive mental outlook of others in similar situations, which promoted their acceptance of a patient identity.16 A longitudinal qualitative study explored the phases of acceptability of symptoms in newly diagnosed CD patients.17 In addition, a supportive environment may act as a catalyst for patient acceptance of the disease. Young adults with IBD and stoma, after an initial phase of anger, began to travel along a predictable path of acceptance and growth as patient education and support services were strengthened and the experiences of stoma management increased.18
Despite these studies, there are still some gaps in the literature. First, studies of factors influencing disease acceptance in IBD patients have mainly focused on demographic and disease characteristics, whereas the process of disease acceptance is dynamic and complex and is not limited to these factors. Second, qualitative studies have explored the experiences of CD patients with a disease course of more than six months or symptom experience of newly diagnosed CD patients, but there is a lack of studies focusing specifically on the disease acceptance of newly diagnosed CD patients. The newly diagnosed stage is an important stage with significant physical and psychological changes in CD patients, and acceptance at this time is the beginning of the patient’s positive coping with the disease, which deserves special attention. Thus, this study aimed to investigate the experiences and perceptions of the disease acceptance process in newly diagnosed CD patients. It can not only provide a reference for early targeted psychological interventions but also lay a foundation for subsequent studies.
Methods
Design
This article presents work that is a subset of a larger longitudinal research project in which the posttraumatic growth of Chinese patients with newly diagnosed CD was studied. A descriptive qualitative approach was employed in the study based on naturalistic inquiry, which does not presuppose variables and theoretical assumptions but uses everyday language to directly describe the experiences of participants or present an event.19 This form of inquiry tends to obtain the most direct and essential answers to the concerns of practitioners or policy makers and helps researchers analyse a phenomenon to obtain more realistic and objective results.20
Participants and Sampling
Between November 2021 and March 2022, participants were recruited from 2 tertiary hospitals in Hangzhou, Zhejiang, China. Purposive sampling and a maximum variation strategy were used to select participants who were information rich and good at expressing themselves. The inclusion criteria were as follows: (1) patients diagnosed with CD based on the Chinese criteria released in 2018;21 (2) patients diagnosed in the last approximately 3 months; (3) patients aged ≥18 years old; and (4) patients who were able to talk freely and clearly. Patients who had serious life-threatening diseases or mental illnesses were excluded.
The sample size was based on data saturation. In this study, when the number of participants reached 14, no new themes emerged from the data analysis; then, 2 more participants were included, and no new information emerged. Therefore, the data were considered to have reached thematic saturation. Finally, 16 semi-structured interviews were conducted. The details of the participants’ demographics and clinical characteristics are shown in Table 1.
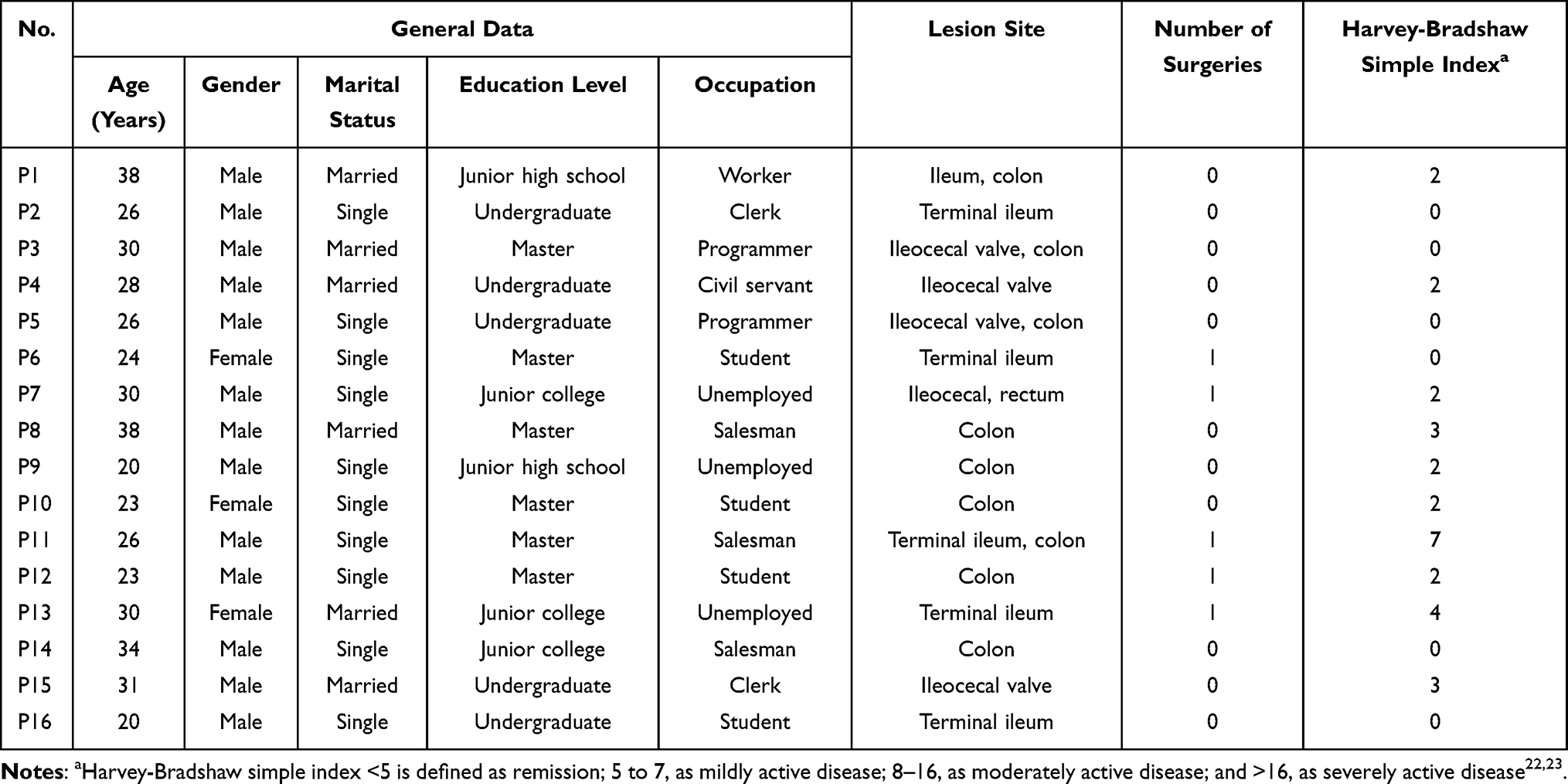 |
Table 1 Study Participants’ Demographics and Clinical Characteristics (n=16) |
Data Collection
A female postgraduate nursing student (JL) conducted semi-structured interviews with the guidance of YZ. YZ is a female PhD qualitative expert who works at a nursing school. The interview sites included outpatient waiting areas (9 participants), wards (4 participants), cafes (1 participant), and parks (1 participant); 1 interview was conducted via telephone. We did not initially aim to frame the interview around the concept of acceptance. The initial interview questions were broadly designed to encourage the collection of more information, such as (1) “Can you tell me about your experience of being diagnosed with CD?” (2) “What was your reaction to the diagnosis of CD?” (3) “How did you perceive CD after diagnosis?” During the interviews, participants were encouraged to express themselves freely in an effort to gather accurate and comprehensive information about their psychological experience; the researcher remained neutral during the interviews, listened carefully to the participants, and clarified any ambiguities. As data collection and analysis advanced, the interview questions became more focused on exploring the themes that emerged from the previous interviews. The order and wording of the questions were adjusted according to the situation without attempting to elicit certain responses or imply meaning. Nonverbal information such as the participants’ expressions, pauses, voice, tone and body language were observed and recorded. The interviews lasted from 27 to 67 minutes.
Data Analysis
After an interview was completed, the researchers transcribed the audio recordings verbatim within 24 hours, and the transcribed data were then checked for accuracy. Data were analysed concurrently with data collection using conventional content analysis by the researchers (YW, JL and YZ). YW is a female PhD candidate who had comprehensive experience in qualitative studies. All the researchers had volunteered for the China Crohn’s & Colitis Foundation, were familiar with the treatment and care of CD, and had frequent contact with CD patients. First, the researchers were immersed in the data to gain a sense of the data as a whole. Second, important ideas and concepts in the data were marked and open coded. Third, similar and related codes were grouped to form themes and subthemes. Finally, themes, subthemes, and codes were defined, and corresponding excerpt examples were identified from the data. To improve the quality of the data analysis, two researchers (YW and JL) analysed the data simultaneously and compared their analyses afterwards, and YZ performed quality control throughout the study. Disagreements in coding and categorization were discussed in a timely manner.
Ethical Considerations
The study complied with the Declaration of Helsinki and was approved by the Ethics Committee of Zhejiang Chinese Medical University (20211217-2). The researchers obtained written informed consent from all participants, including publication of the anonymized responses. Participants were free to withdraw at any time without penalty. The collected data were well kept, and only the research team had access. The researchers carefully managed their relationships with the participants.
Rigour
Three methods were used to maintain rigor in this study. First, credibility was established through peer debriefings in which the researchers consulted with one another to address any ambiguities or disagreements on methodological issues or data analysis. Second, the researchers informed the participants about the themes and subthemes of the study and confirmed whether they had the same feelings or experiences. Third, the researchers kept a reflective journal to identify ideas and assumptions about the research experience and to explore how personal characteristics influenced the interaction between researchers and participants and the construction of the results.
Results
This study explored the experiences and feelings of newly diagnosed CD patients (from suspected CD to 3 months after CD diagnosis) during the disease acceptance process. Five phases of the psychosocial process emerged from the data analysis. It is referred to as the “acceptance journey” of newly diagnosed CD patients and is illustrated in Figure 1. Arrows are used to illustrate the transition from the previous phase to the next phase. The dashed arrows show that not all participants could reach the last two stages, while the dashed arrows in the opposite direction indicate that some participants returned to a previous stage for some reason.
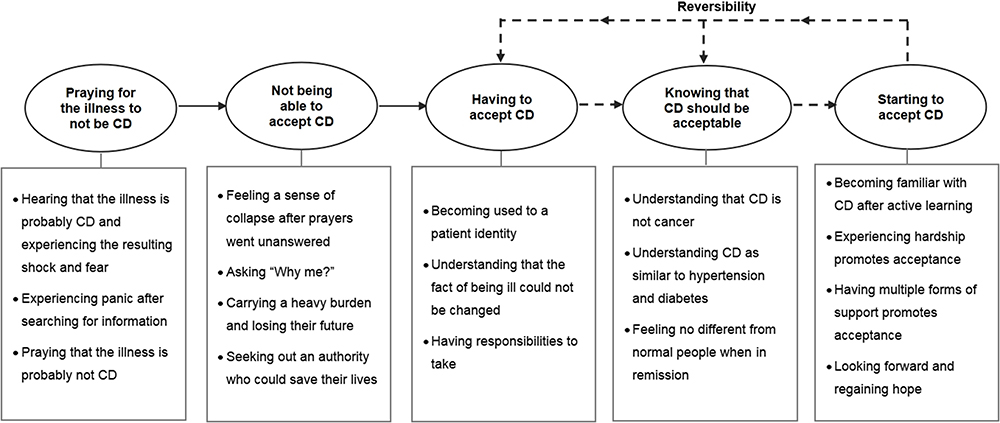 |
Figure 1 The “acceptance journey” of newly diagnosed Crohn’s disease (CD) patients. |
Phase 1: Praying for the Illness to Not Be CD
The diagnosis of CD lacks a gold standard and requires a combination of clinical manifestations, laboratory tests, endoscopy, imaging and pathological histology for exclusionary diagnosis and comprehensive analysis. Therefore, there is a relatively long “waiting period” between the first suspicion of CD and the definitive diagnosis. During this time, emotional changes caused by disease information began, but formal care was not accessible. The “waiting period” for different patients in this study ranged from 5 days to 7 months.
Hearing That the Illness is Probably CD and Experiencing the Resulting Shock and Fear
When a doctor informed patients that they might have CD, the first reaction of 13 patients was a feeling of shock and/or fear. As indicated by the data analysis, the incidence of CD in China is relatively low, and CD is thus an extremely unfamiliar disease among Chinese people. In addition, patients often have gastrointestinal symptoms, perianal abscesses or anal fistulas before seeking medical care, which makes them think that they may have more common conditions such as gastroenteritis or haemorrhoids.
At first, I did not know about it and thought it was a particularly rare disease that no one had ever heard of. (P2)
The name sounded scary, and I got scared because I had not heard of it at all. I immediately called the work unit and said I am going to quit, that I was suspected of having a very serious illness (elevated tone). (P7)
The remaining three participants did not show significant shock and/or fear upon learning of the suspected diagnosis because they had been exposed to CD before or did not realize the severity of CD.
Experiencing Panic After Searching for Information
Faced with an unfamiliar diagnosis, the patients began to use their usual search engines, such as Baidu (the largest Chinese search engine) and Xiaohongshu (a popular social mobile application in China), to search for information about CD on their own. Twelve of them clearly described that the descriptions of CD they found on the internet included the terms “green cancer (a metaphor for CD, indicating that CD is incurable although not fatal)”, “incurable”, “nasal feeding”, “enterostomy”, and “possible canceration”, which made them transition from shock to profound fear. It is evident that the early description of the disease directly influenced the patients’ emotional response and perception of CD.
I searched for the disease, and the results showed “green cancer”. This is too serious. I kind of loss confidence to read further. (P2)
Praying That the Illness is Probably Not CD
Faced with the severe disease descriptions found on the internet, the patients instinctively rejected the suspected diagnosis of CD and then prayed that they might not have CD. Six of the patients described that they wished they had been misdiagnosed by their doctors and prayed that they did not have CD. Three of the patients browsed the information and learned that the two most common types of IBD were CD and UC, and they felt that CD was more serious than UC; therefore, they preferred to have UC rather than CD. The patients developed a temporary psychological defense and protected themselves through denial and prayer.
I am just very apprehensive anyway because there’s still that thought in my mind that it could be a misdiagnosis by our local doctor or something. (P6)
Phase 2: Not Being Able to Accept CD
After the confirmed diagnosis, the patients found that their prayers had not been answered, and their psychological defence instantly collapsed when the doctor announced the diagnosis of CD.
Feeling a Sense of Collapse After Prayers Went Unanswered
When the aforementioned psychological defence of denial and prayer was instantly shattered by the diagnosis, 11 patients had relatively strong emotional reactions, including 2 female patients who “cried on the spot” and 9 patients who explained that they felt like “the sky was falling”, that they were “devastated”, that they “did not expect it (the diagnosis) to be so serious”, and that “bad luck comes to those who suffer”.
I felt like that the sky was falling (bitter laugh). (P1)
The remaining 5 patients had relatively mild emotional reactions at the time of diagnosis. One of them had a five-year history of psoriasis, which was now well controlled; this patient believed that both CD and psoriasis were chronic diseases that could be controlled, and he noted, “I had psychological preparation when I had psoriasis”. Two patients had been troubled by abdominal pain and diarrhoea for many years, but the real cause was never found due to various factors, so this diagnosis made them feel “relieved”. The other two patients were glad that they had been diagnosed early and that their condition was not severe.
Asking “Why Me?”
The patients were puzzled about the diagnosis and asked themselves, “Why me?” Considering the time before their illness, the participants thought that they had a regular life, that they were healthy, and even that they had a superb physique, so they wondered why they suffered from this “rare disease”. They wondered how they had become one of the few who were chosen by fate. The patients could not explain this to themselves and felt baffled.
There are few CD patients in China, so why me? I am the one being chosen to suffer from CD among tens of thousands. (P10)
Carrying a Heavy Burden and Losing Their Future
The patients began to experience various negative emotions and often looked at problems negatively and one-sidedly, perceiving that CD was a “big burden (P1)” or a “big situation (P3)” in their life and thinking that they would “have to fight with CD for the rest of their lives (P4)”. One patient noted, “I feel sorry for my family (P3)”, and some patients even pessimistically complained that “all of a sudden there is no future (P6)” or that “their lives have no hope (P7)”.
First, we are ordinary working-class people, and our rhythm of work and life will be disrupted after having this disease that cannot be cured. Second, it is also a great pressure on income. Therefore, I carried a big burden inside when I was newly diagnosed. (P1)
Seeking Out an Authority Who Could Save Their Lives
Patients and their families placed hope in medical authorities because they believed that CD was not an ordinary disease and because they were affected by negative emotions. All 16 patients looked for IBD authorities and compared experts in this field through various channels.
(After having gone to 4 hospitals) I think the treatment plan from doctor A is pretty good, and I can accept it. She draws charts for me to explain the CD. I asked her if she suggested that I use vedolizumab, and she said, “I would use it if I were you”. I felt that she could perceive it from the patient’s point of view, and I was quite moved because she was able to provide me with some psychological support. (P2)
Phase 3: Having to Accept CD
As treatment was ongoing, repeated medical visits forced the patients to gradually become accustomed to being a patient.
Becoming Used to a Patient Identity
The interviews in this study were conducted approximately within 3 months after CD diagnose. The frequency of visits during this period was high. The patient identity was constantly reinforced by repeated hospital visits.
I have been hospitalized four or five times since my diagnosis. I am used to staying in the hospital. Running to the hospital every day is quite normal for me. (P13)
Understanding That the Fact of Being Ill Could Not Be Changed
Faced with physical symptoms such as abdominal pain, diarrhoea, and fatigue as well as repeated follow-ups and the acknowledgement that the whole ward was full of CD patients, the patients became increasingly aware that the illness could not be changed. The participants’ tone revealed a sense of resignation: “I’m already like this”, “I can’t change it”, “It’s useless to refuse”, “I can only try to adapt”, and “I can only accept it”.
This is unavoidable. My life and work are certainly being affected, and the impact is certainly not small, so we can only try to adapt to it and find ways to solve it later. (P8)
The patients’ narratives show that they did not give up regarding the disease and themselves. They chose their own way to face the present situation.
Having Responsibilities to Take
In China, the peak incidence of CD occurs in young and middle-aged people. After diagnosis and treatment in the early stage, the patients gradually returned to their previous context of family, work or study. Ten patients expressed a deep sense of family responsibility, as they were the main provider in the family. In addition, the patients had to face work or study pressure. The sense of responsibility and real-life pressure forced the patients to accept CD.
I have a family with children and the elderly. If I cannot pull myself together, what about other people in my family? What about my family if I cannot adjust myself? I have to learn to accept it. (P13)
Phase 4: Knowing That CD Should Be Acceptable
With an increasing amount of information about the disease and improvement of the disease condition, the patients’ perception of CD became more comprehensive and objective. A series of cognitive shifts and mental reconstructions prompted the patients to stop rejecting their CD diagnosis and to believe that CD should be acceptable.
Understanding That CD is Not Cancer
The patients’ initial perception of CD as cancer mainly came from the internet description of CD as a “green cancer”. Those sensitive terms, such as “cancer”, could easily attract the attention of newly diagnosed patients and lead to increased panic. However, as their perceptions and mindsets changed, the patients’ attention began to shift from the word “cancer” to the important adjective “green”. Nine patients reported that CD, although incurable, is a benign disease and not a real cancer.
CD is manageable; it is not directly fatal. CD is not untreatable as before. As long as it is not cancer, I do not think it is a big problem. (P15)
Understanding CD as Similar to Hypertension and Diabetes
CD is still not a familiar disease to the Chinese public. Therefore, when the patients learned about the characteristics of CD, they tried to analogize it to a more familiar disease. In this way, CD could be more acceptable to the patients. Four patients in this study compared CD to hypertension and diabetes.
It’s just necessary to take regular medication, similar to chronic diseases like hypertension and diabetes. So when I think of it that way, I relax a little bit, I feel okay, and I am not so resistant and afraid of this. (P3)
Feeling No Different from Normal People When in Remission
Six patients were in remission after preliminary treatment. Additionally, newly diagnosed patients had relatively few complications, so the patients truly felt no difference between themselves and normal people when they were in remission.
In addition to regular injections, I almost forget that I am a patient. CD seems to have little influence on me lately, nor does it hurt or itch; basically, I was only reminded of the disease while eating. (P6)
Phase 5: Starting to Accept CD
With more active learning and the use of support, patients begin to look to the future and regain hope, which is in great contrast to the phase of not being able to accept CD, in which the patient carries a heavy burden and has a sense of loss regarding the future. Those who have experienced some hardships and had multiple forms of support are more likely to reach this phase.
Becoming Familiar with CD After Active Learning
Ignorance can lead to panic and delayed acceptance. When patients begin to learn more actively and deeply, it indicates their desire to approach CD further and try to manage it, which are positive signs of beginning to accept CD. Eight patients in this study mentioned the process of active learning.
I just tried to do everything I could, watching videos on patient education, reading some literature on the internet, and following information in patient groups. Then, I tried to choose a more acceptable treatment method provided by my doctor. (P8)
Experiencing Hardship Promotes Acceptance
When faced with CD, many newly diagnosed patients (n=9) tended to associate it with their life experiences, especially their experiences of overcoming hardships, to help them reduce stress and build confidence so that they could better accept CD.
I almost had an accident when I was learning to fly previously. It was very dangerous, and the wind was very strong at that time. I thought I was going to die (laughs). But it was okay later on; the operation was successful, and I survived. I experienced a few more such things. Now I can accept CD more calmly. (P2 used to be a civilian pilot)
Having Multiple Forms of Support Promotes Acceptance
The patients were surrounded by different resources and had different perceptions of people, things, objects, and events related to the disease. These different resources and perceptions all contributed to the patients’ acceptance of CD to different degrees. Each participant had at least one of these supports: family member (n=9), medical and nursing staff (n=8), wardmate (n=7), medical/commercial insurance (n=5), and related institution (n=3).
My wife said it is OK that we lead a poor life. We should first have a good mindset and take care of the illness. We can earn money later on. My pressure was decreased at once. (P1)
At that time, there was a meeting at the China Crohn’s & Colitis Foundation, and I was told that the future is promising. I thought that the future is promising is a good term. It increased my hope. (P10)
Looking Forward and Regaining Hope
Those patients with effective disease management and/or good psychological adjustment (n=10) started to look forward to the future and regain hope. Some patients compared facing CD to being in a “race” or “running with weight”, others began to “face CD head-on”, and still others looked forwards to “new drugs bringing more hope”.
CD is like weight bearing, right? When you run with weights, you get a little tired, but you can still keep running. (P2)
I went to the window, pulled open the curtains, the sun came through, I was particularly impressed with this scene. I suddenly thought, “Why don’t I give myself some hope? Why can’t I get over this?” “Hey, maybe it is a turning point”. I felt I needed to face it head-on. (P3)
In summary, patients at the stage of “starting to accept CD” were more proactive and motivated to face the disease, and their overall acceptance of CD was higher than that in the previous stages. However, not all patients were able to reach this stage. By the end of the interview, 2 patients remained at the stage of “having to accept CD”, and 3 patients remained at the stage of “knowing that CD should be acceptable”. Two patients showed a reversible change in their acceptance journey. They entered the stage of “starting to accept CD” and then reverted back to one of the previous stages. Thus, the “acceptance journey” of newly diagnosed CD patients is dynamic, individual and reversible, and it is not unidirectional or linear.
Discussion
This study focused on patients who had been diagnosed with CD in the last approximately 3 months, and it identified five phases of the “acceptance journey”: praying for the illness to not be CD; not being able to accept CD; having to accept CD; knowing that CD should be acceptable; and starting to accept CD. Another study involving newly diagnosed CD patients also revealed three phases of symptom acceptability: difficult to accept, have to accept and be able to accept.17 Although there are some similarities between the two studies, ours is different in the following aspects. First, Chen’s study focused on the acceptability of symptoms only, whereas our study addressed a broader concept of disease acceptance. Second, the research design and participants differed between the two studies. Chen’s study employed a longitudinal qualitative design and recruited newly diagnosed CD patients, following them for 3, 6 and 12 months post-diagnosis. In contrast, our study utilized a descriptive qualitative approach, and our participants were CD patients diagnosed in the last approximately 3 months. Consequently, Chen’s findings reached the phase of “be able to accept” while ours ended with “starting to accept CD”. Third, in Chen’s study, the starting point of acceptance was “difficult to accept”, while in our study, it began with “praying for the illness to not be CD”. This aligns with the “waiting period” between the first suspicion of CD and the definitive diagnosis, a period rarely mentioned in previous literature but crucial to the “acceptance journey” of this population.
Our study provides some detailed insights into the acceptance process of newly diagnosed CD patients. CD is unique in that patients experience a relatively long “waiting period” before diagnosis, and previous studies have paid less attention to the psychological changes in patients during this period. Many patients expressed anxiety prior to arriving at a diagnosis and often could not access the care that they needed until they received a formal diagnosis.24 During the waiting period, almost all participants turned to internet search platforms for information about the disease. Research has shown that a higher percentage of internet information originates from commercial organizations or pharmaceutical companies, and their sources may be inaccurate or even misleading.25 There are also some internet reports that purposely use exaggerated headlines to gain clicks and advertising fees, while their content is based on unofficial resources and lacks quality.26 When patients still knew little about CD, they were in a state of shock and panic. At this time, emotionally charged words such as “green cancer”, “incurable” and “possible cancer” from online sources were noted and exaggerated by patients, which is evidenced by the subtheme “experiencing panic after searching for information”. This can be explained by the “focusing illusion” in cognitive psychology, which describes how patients focus on the negative effects of the disease during the initial stages of the disease, overestimating the harm of the disease and underestimating their own abilities, resulting in cognitive distortions and negative emotions.27 It is important that health care professionals not ignore the waiting period and that they try to provide concise and correct information about the disease at an early stage. This can alleviate the negative emotions of patients and lay the foundation for subsequent acceptance of CD.
With the final diagnosis of CD, most patients felt that “the sky was falling” and that they had fallen into an abyss, crying out helplessly, “Who will save me?” Influenced by traditional culture, Chinese people prefer and respect authority.28 The immediate coping strategy for them was to “seek out an authority”. At this time, the patient not only faced physical distress but also suffered a substantial psychological impact. Therefore, they had a dual expectation when they sought authority. They expected that the “authority” must be a professional and knowledgeable doctor and could provide the best treatment plan to save them from the “abyss”. They also expected the “authority” to provide them with a large amount of psychological support.29 It is clear that “professional skill” and “kindheartedness” were two expectations patients had. These details enrich our understanding of newly diagnosed patients’ behaviour in seeking medical care. It is suggested that health care providers pay attention to the panic and helplessness of CD patients in the early stages of diagnosis while providing professional medical services and trying to convey confidence and strength to patients.30
As time passed, the patients realized that the fact of being ill could not be changed, which revealed a sense of resignation. However, the patients did not leave the illness to chance. They chose their own way to face the present. This fits well with the Taoist concept of “wu-wei” in China; “wu” means “not” or “non”, and “wei” means “action”, “striving” or “straining”.31 That is, “wu-wei” is a natural way of being in the moment that flows with the circumstances. An apt and often used metaphor is that of water and how it behaves. Water flows to naturally fill whatever shape of container in which it resides. Water does not strive for one direction or resist another direction but rather spontaneously flows with and adapts to the world around it.32,33 In this study, “wu-wei” can be understood as patients facing CD more naturally and spontaneously rather than striving to fight or control CD directly at a particular stage. It should be pointed out that an approach based on the concept of “wu-wei” does not imply a passive response of doing nothing; rather, the concept of “wu-wei” frees patients from the negative mood of not accepting the disease and then provides the possibility and basis to seek new changes later. As the Tao Te Ching (the philosophical works of Lao Tzu) says, “Do nothing and everything is done”. From this cultural and philosophical perspective, health care providers can deeply comprehend the disease acceptance process.
The subtheme “having responsibilities to take” belongs to the theme of “having to accept CD”, which also reflects distinctive Chinese cultural characteristics. The newly diagnosed patients in this study were ages 20 to 38 years old, which coincides with the peak of the onset of CD. This age range is also the prime time for starting a family. Self-perceived responsibility is an important factor that motivates patients to accept CD, especially family responsibility (which was mentioned by 10 participants). Taking on family responsibility is a traditional virtue in China, as a collectivist culture. Confucianism views a person as a part of a family with interdependent responsibilities and expectations.34 Thus, many patients, after experiencing strong emotional swings in the early stages of “not being able to accept CD”, began to reflect, driven by a sense of responsibility. One participant (P13) mentioned that there were old and young members in her family, and if she could not pull herself together, she would not be able to take on family responsibilities; therefore, she could only try to accept CD. Another participant (P3) realized that it would be “irresponsible” for him to communicate negative emotions to his family members, so he decided to adjust his emotions and compensated by subsequently taking care of his wife and daughter. The family responsibility that motivates patients to accept CD reflects the characteristic influence of Confucianism in Chinese culture, a finding that has rarely been reported in other related studies. Given the scope of Confucianism’s influence on culture in East Asia, health care professionals in these regions could draw on a sense of family responsibility to promote patient acceptance of CD when appropriate.
After 2–3 months of consultation and treatment, the patients’ disease was controlled to a certain degree. They had more interaction with health care providers and peer patients and gained more support from them. Therefore, they had more channels to access information, and they gradually changed from the usual search engines to more specialized channels, such as professional medical websites, information provided by the IBD health care team, books, and papers. These prompted CD patients to re-examine the disease, which allowed them to undergo a transition: from the initial stage of being horrified and regarding CD as a “green cancer” to the belief that CD, although incurable, is a benign disease and “not cancer”. Patients moved on to a later stage of comparing CD to hypertension and diabetes and, finally, to the stage of understanding that patients who suffer from CD are not different from normal people when they are in remission. These cognitive shifts reflect the dynamic nature of the disease acceptance journey for patients with CD. However, the study also found that the journey of acceptance is individual and reversible, with some patients stagnating at one stage or even regressing to a previous stage for some reason. This is largely because people with CD live with ongoing unpredictability and uncertainty. Thus, acceptance of the disease may mean acceptance of multiple, shifting versions of “normality”.35,36 Given the dynamic and reversible nature of early disease acceptance, health care professionals should provide targeted psychological interventions to promote a steady rise in disease acceptance.
Limitations
This study had some limitations. First, the participants were from developed provinces in eastern China and were mostly men with relatively high education levels, which may limit the generalizability of the results. Second, although the researchers kept a reflective journal, bias from the researchers cannot be absolutely ruled out. Third, data saturation is a relative concept, and although it was reached in our study, the findings might be enriched with further interviews.
Conclusion
The “acceptance journey” of newly diagnosed CD patients consists of five phases: “praying for the illness to not be CD”, “not being able to accept CD”, “having to accept CD”, “knowing that CD should be acceptable” and “starting to accept CD”. This process is dynamic, individual and reversible. In addition, traditional Chinese cultural values such as respect for authority, the philosophy of wu-wei and family responsibility contribute to the acceptance of CD in Chinese patients. Hence, there is a need to provide early and culturally tailored psychological support or interventions according to the stages of acceptance for CD patients. In the future, longitudinal qualitative studies could be used to further explore the disease acceptance process of patients beyond 3 months of CD diagnosis.
Abbreviation
CD, Crohn’s disease.
Data Sharing Statement
The data generated and/or analysed during the current study are not publicly available due to ethical issues but are available from the corresponding author or first authors on reasonable request.
Acknowledgments
We are grateful to the 16 participants who generously shared their time, experience, and stories in this study.
Author Contributions
All authors made significant contributions to the work reported, including the concept, study design, execution, acquisition of data, analysis and interpretation. All took part in drafting, revising or critically reviewing the article, and gave final approval of the version to be published. Authors agreed on the journal to which the article has been submitted and to take responsibility and be accountable for the contents of the article.
Funding
This project was funded by the Basic Public Welfare Research Program of Zhejiang Province [grant numbers: LGF21C090001]. The funder had no role in the design, conduct, or writing of this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dembo T, Leviton GL, Wright BA. Adjustment to misfortune: a problem of social-psychological rehabilitation. Rehabil Psychol. 1975;22(1):i–iv, 1–100. doi:10.1037/h0090832
2. McCracken LM, Eccleston C. Coping or acceptance: what to do about chronic pain? Pain. 2003;105(1–2):197–204. doi:10.1016/s0304-3959(03)00202-1
3. Zauszniewski JA, McDonald PE, Krafcik K, Chung C, Dobratz MC, Downe-Wamboldt B. Acceptance, cognitions, and resourcefulness in women with diabetes. West J Nurs Res. 2002;24(7):728–43; discussion 744–50. doi:10.1177/019394502762476951
4. Kołtuniuk A, Rosińczuk J. The levels of depression, anxiety, acceptance of illness, and medication adherence in patients with multiple sclerosis - descriptive and correlational study. Int J Med Sci. 2021;18(1):216–225. doi:10.7150/ijms.51172
5. Qiu C, Zhang X, Zang X, Zhao Y. Acceptance of illness mediate the effects of health literacy on self-management behaviour. Eur J Cardiovasc Nurs. 2020;19(5):411–420. doi:10.1177/1474515119885240
6. Sadeghiazar S, Mobasseri K, Gholizadeh L, et al. Illness acceptance, medication adherence and the quality of life in patients with heart failure: a path analysis of a conceptual model. Appl Nurs Res. 2022;65:151583. doi:10.1016/j.apnr.2022.151583
7. Fourie S, Jackson D, Aveyard H. Living with inflammatory bowel disease: a review of qualitative research studies. Int J Nurs Stud. 2018;87:149–156. doi:10.1016/j.ijnurstu.2018.07.017
8. Ruan J, Wu L, Zhou Y. Experiences of body image changes in Chinese patients living with inflammatory bowel disease: a descriptive qualitative study. Asian Nurs Res. 2020;14(4):196–205. doi:10.1016/j.anr.2020.07.006
9. Luo XP, Mao R, Chen BL, et al. Over-reaching beyond disease activity: the influence of anxiety and medical economic burden on health-related quality of life in patients with inflammatory bowel disease. Patient Prefer Adherence. 2016;11:23–31. doi:10.2147/PPA.S118589
10. Kaplan GG, Windsor JW. The four epidemiological stages in the global evolution of inflammatory bowel disease. Nat Rev Gastroenterol Hepatol. 2021;18(1):56–66. doi:10.1038/s41575-020-00360-x
11. Ng SC, Kaplan GG, Tang W, et al. Population density and risk of inflammatory bowel disease: a prospective population-based study in 13 countries or regions in Asia-Pacific. Am J Gastroenterol. 2019;114(1):107–115. doi:10.1038/s41395-018-0233-2
12. Kaplan GG. The global burden of IBD: from 2015 to 2025. Nat Rev Gastroenterol Hepatol. 2015;12(12):720–727. doi:10.1038/nrgastro.2015.150
13. Chrobak-Bień J, Gawor A, Paplaczyk M, et al. The influence of socio-demographic and clinical factors on the process of acceptance of the disease among patients with ulcerative colitis. Pol Przegl Chir. 2018;90(6):1–5. doi:10.5604/01.3001.0012.1753
14. Sirois FM, Hirsch JK. A longitudinal study of the profiles of psychological thriving, resilience, and loss in people with inflammatory bowel disease. British J Health Psychol. 2017; 22(4):920–939. doi:10.1111/bjhp.12262
15. Evers AW, Kraaimaat FW, van Lankveld W, et al. Beyond unfavorable thinking: the illness cognition questionnaire for chronic diseases. J Consult Clin Psychol. 2001;69(6):1026–1036. doi:10.1037/0022-006X.69.6.1026
16. Ruan J, Zhou Y. Regaining normality: a grounded theory study of the illness experiences of Chinese patients living with Crohn’s disease. Int J Nurs Stud. 2019;93:87–96. doi:10.1016/j.ijnurstu.2019.02.015
17. Chen L, Zhou Y. The symptom experience of newly diagnosed Chinese patients with Crohn’s disease: a longitudinal qualitative study. J Adv Nurs. 2023;79(10):3824–3836. doi:10.1111/jan.15721
18. Horgan L, Richards H, Joy A. The young adult male’s perception of life with inflammatory bowel disease and a stoma: a qualitative examination. J Clin Psychol Med Settings. 2020;27(3):560–571. doi:10.1007/s10880-019-09695-3
19. Sullivan-Bolyai S, Bova C, Harper D. Developing and refining interventions in persons with health disparities: the use of qualitative description. Nurs Outlook. 2005;53(3):127–133. doi:10.1016/j.outlook.2005.03.005
20. Neergaard MA, Olesen F, Andersen RS, et al. Qualitative description - The poor cousin of health research? BMC Med Res Methodol. 2009;9(1):52. doi:10.1186/1471-2288-9-52
21. Inflammatory Bowel Disease Group, Chinese Society of Gastroenterology, Chinese Medical Association. Chinese consensus on diagnosis and treatment in inflammatory bowel disease (2018, Beijing). J Dig Dis. 2021;22(6):298–317. doi:10.1111/1751-2980.12994
22. Harvey RF, Bradshaw JM. A simple index of Crohn’s-disease activity. Lancet. 1980;1(8167):514. doi:10.1016/s0140-6736(80)92767-1
23. Best WR. Predicting the Crohn’s disease activity index from the Harvey-Bradshaw Index. Inflamm Bowel Dis. 2006;12(4):304–310. doi:10.1097/01.MIB.0000215091.77492.2a
24. Mirza RM, MacKean G, Shaffer SR, et al. Patient experiences in the management of inflammatory Bowel disease: a qualitative study. J Can Assoc Gastroenterol. 2022;5(6):261–270. doi:10.1093/jcag/gwac014
25. Kurowski JA, Bewtra M, Kodish E, Lashner B. Reducing the spread of internet misinformation in IBD: ethics and responsibility. Inflamm Bowel Dis. 2021;27(6):960–962. doi:10.1093/ibd/izaa335
26. Zhang X, Ghorbani AA. An overview of online fake news: characterization, detection, and discussion. Inf Process Manag. 2020;57(2):102025. doi:10.1016/j.ipm.2019.03.004
27. Peeters Y, Vliet Vlieland TP, Stiggelbout AM. Focusing illusion, adaptation and EQ-5D health state descriptions: the difference between patients and public. Health Expect. 2012;15(4):367–378. doi:10.1111/j.1369-7625.2011.00667.x
28. Guo F, Hanley T. Adapting cognitive behavioral therapy to meet the needs of Chinese clients: opportunities and challenges. Psy Ch J. 2015;4(2):55–65. doi:10.1002/pchj.75
29. Norton BA, Thomas R, Lomax KG, Dudley-Brown S. Patient perspectives on the impact of Crohn’s disease: results from group interviews. Patient Prefer Adherence. 2012;6:509–520. doi:10.2147/PPA.S32690
30. Ma S. Nurses should recognise that focusing only on the resolution of physical symptoms may not be enough to overcome the psychosocial implications of living with a chronic disease. Evid Based Nurs. 2021;24(1):6. doi:10.1136/ebnurs-2019-103245
31. Watts A. The Way of Zen. New York: Pantheon; 1957.
32. Banner M. Wu-Wei: concept analysis of a conceptual paradox. Issues Ment Health Nurs. 2018;39(4):304–310. doi:10.1080/01612840.2017.1398792
33. Barrett NF. Wuwei and Flow: comparative Reflections on Spirituality, Transcendence, and Skill in the Zhuangzi. Philos East West. 2011;61(4):679–706. doi:10.1353/pew.2011.0051
34. Park M, Chesla C. Revisiting Confucianism as a conceptual framework for Asian family study. J Fam Nurs. 2007;13(3):293–311. doi:10.1177/1074840707304400
35. Byron C, Cornally N, Burton A, Savage E. Challenges of living with and managing inflammatory bowel disease: a meta-synthesis of patients’ experiences. J Clin Nurs. 2020;29(3–4):305–319. doi:10.1111/jocn.15080
36. Muse K, Johnson E, David AL. A feeling of otherness: a qualitative research synthesis exploring the lived experiences of stigma in individuals with inflammatory bowel disease. Int J Environ Res Public Health. 2021;18(15):8038. doi:10.3390/ijerph18158038
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.