Back to Journals » Risk Management and Healthcare Policy » Volume 14
Experience and Perceptions of Changes in the Living Environment by Older People Losing Their Autonomy: A Qualitative Study in the Caribbean
Authors Chammem R, Domi S, Della Vecchia C, Gilbert T ![]() , Schott AM
, Schott AM ![]()
Received 21 October 2020
Accepted for publication 23 December 2020
Published 22 February 2021 Volume 2021:14 Pages 743—756
DOI https://doi.org/10.2147/RMHP.S287382
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Rita Chammem,1,2 Serge Domi,2 Claire Della Vecchia,1 Thomas Gilbert,1,3 Anne-Marie Schott1,3
1University of Claude Bernard Lyon 1, HESPER Laboratory, Lyon, EA 7425, France; 2CRIFONDO, Caribbean Renaissance Initiative, Département de Gérontologie, Martinique, France; 3Hospices Civils De Lyon, Pôle De Santé Publique, Public Health, Lyon, France
Correspondence: Rita Chammem
Laboratoire HESPER, Université Claude Bernard Lyon 1, Site Rockefeller, 8 Avenue Rockefeller, Lyon, 69008, France
Tel +33 676813256
Email [email protected]
Rationale: Although the literature recognizes the importance of older individuals’ subjective perceptions about their living environments, past studies on the subject have been primarily restricted to nursing home settings.
Objective: This study aimed to better understand the experiences, perceptions, coping mechanisms, and needs of older people living in Martinique who had to modify their living environment because of a decline of autonomy.
Design: Qualitative study using content analysis.
Methods: Semi-structured one-on-one interviews were conducted with older people living in three different types of environment i) at home with professional support, ii) in a foster care family, iii) in a nursing home. Interviews were conducted until data saturation was reached. A conventional content analysis approach was used.
Results: Thirty-four participants were interviewed. Subjects perceived ageing as a factor leading to changes in their living environment. However, they did not spontaneously evoke their functional/structural impairments nor their activity limitations as if the change of living environment could reduce the perceived loss of autonomy by maintaining an acceptable participation. Participants mostly experienced change as both inevitable and as a relief as it took them out of isolation and domestic hardship. This reaction was somewhat facilitated by spiritual beliefs as the changes were interpreted as the will of spiritual forces. Family and social relationships appeared to be more important determinants of participants’ perception of changes in living environment than was health status. We found differences between the three groups regarding familial relationship, fear of death, acceptance of change, and unmet needs. Unmet needs were particularly expressed by those living in foster care. The concept of “feeling at home”, which emerged as essential for all participants, was lacking in foster care families.
Conclusion: Perceived autonomy, including not only functional/structural impairments, but also, social interactions, should be carefully considered when developing support services for older individuals.
Keywords: older people, nursing home, autonomy, quality of life, foster care family
Introduction
France currently has the 5th largest aging population in Europe (18.8% versus 18.9% in Europe in 2016),1 mainly due to the increased life expectancy2 and aging of the baby boom generation.3 In the French overseas regions, demographic transition is particularly rapid. While Martinique was one of the youngest French regions 15 years ago, it is now among the top three oldest regions. By 2030, one third of its population will be 65 or older.4 The unexpectedly rapid increase in the proportion of older individuals currently occurring in Martinique is due to the combination of five factors: 1) decline in birth rate, 2) increase in life expectancy, 3) aging of the baby boom generation, 4) youth emigration due to lack of resources and work opportunities,5,6 and 5) natives returning to Martinique for retirement.7 The region was unprepared for such a situation, and the challenges are compounded by the precarious economic environment. Indeed, almost 30% of individuals over 60 in Martinique are beneficiaries of the governmental solidarity allowance (awarded to older people without income), versus 3.4% in metropolitan France.8 The increase of life expectancy is associated with a high burden of chronic diseases (particularly diabetes, hypertension, and cardiovascular diseases), functional disabilities, neurocognitive disorders,9–13 and related healthcare costs.14–16
The demographic transition in Martinique is accompanied by a societal evolution in the family structure. In the past, older adults shared the family home with their descendants who, in return, provided care and support in the form of intergenerational solidarity.17 Today, families tend to be smaller due to the increase of single-parent families (20% vs 8% in Metropolitan France)18 and the migration of young people.19 Moreover, it is mainly the women (daughter, daughter-in-law, wife, granddaughter) who bear the burden of caring for older parents who have decreased autonomy. However, their role as caregivers is increasingly impacted by their professional activities.20–22 Finally, the average age of caregivers is also increasing, and it is not uncommon for them to be impacted by disabilities themselves.23
There is a strong need to improve the care and support options for the aging population in this territory.24 Furthermore, public institutions and nursing homes which, in Martinique, were reserved for older people of lower socio-economic status who experienced neglect, are becoming essential for all older individuals losing their autonomy.25
The International Classification of Functioning, Disability and Health (ICF) proposed by the WHO in 2001 defined two dimensions of declining autonomy and dependency. The first level concerns the biomedical factors and associated impairments, and also, includes functional disabilities leading to activity limitations and the notion of participation restriction. The second dimension takes into account the interactions of the individuals with their environments and includes different contextual factors.26
The two main public responses to aging individuals’ decline in autonomy are the formalization of home care support or changes in living environments. The latter can include institutions such as nursing homes and independent residences, or alternatives such as foster care families. Formal home care refers to professional support aimed at helping older individuals perform daily life activities (meals on wheels, health care workers, housekeepers). Foster care refers to a model of “homelike” residential care, where individuals who have obtained formal approval from a regional council host and take care of older patients in their own home for a fee.
In this study, we chose to define loss of autonomy as the inability to continue managing daily life alone necessitating a change in lifestyle and/or living environment.
Public policies and medico-social services created to address older peoples’ loss of autonomy have primarily focused on the individual’s functional capacities and level of disability.27 However, the perceptions of older individuals themselves have rarely been investigated. In addition, previous research has mostly focused on objective health status as the main determinant of the quality of life of older people. However, the importance of older individuals’ subjective perceptions is increasingly being recognized.28–31 Quality of life is conceived as a measure of the perceived gap between the individual’s real situation and their aspirations.32 This implies taking better account of patients’ perceptions and their aspirations in order to enable services to be genuinely adapted to their expectations and facilitate their acceptance. Qualitative methods provide a particularly useful approach to appropriately understand individuals’ perceptions. Therefore, these methods can help provide new knowledge and identify factors to improve the older person’s quality of life.33
Our objectives were to measure the participants’ experience and perceptions about their change in living environment due to a loss of autonomy, the way they coped with it, and the needs they expressed.
Methods
Study Design
In Martinique, the institutions that are most commonly used to provide care for aging individuals are the nursing home and the foster care family. In 2018, there were approximately 92,000 people over the age of 60e,34 8 home nursing services (SSIAD, ie, Services de Soins Infirmiers), 30 nursing homes and 65 foster care families in Martinique.35
In this qualitative study, we sought to study the experiences and explore the personal themes and needs expressed by the older individuals in order to improve the quality of care and health provided to them as a response to their loss of autonomy. Qualitative studies are useful in that they provide new knowledge that is complementary to quantitative health care data. Qualitative studies also help us to identify potentially modifiable factors to improve the autonomy of older people.
We used one-on-one semi-structured interviews to elicit older peoples’ perceptions36 about three different types of changes of living environment they experienced because of their loss of autonomy: (1) remaining at home with professional support services; (2) living in a foster care family; (3) living in a nursing home. In our study, these 3 groups were considered to have a loss of autonomy.
We followed the COREQ checklist (COnsolidated criteria for Reporting Qualitative research) for reporting our results (Appendix. 1). 3,37 3 The study was reported using these 32-item checklist (Table 1).
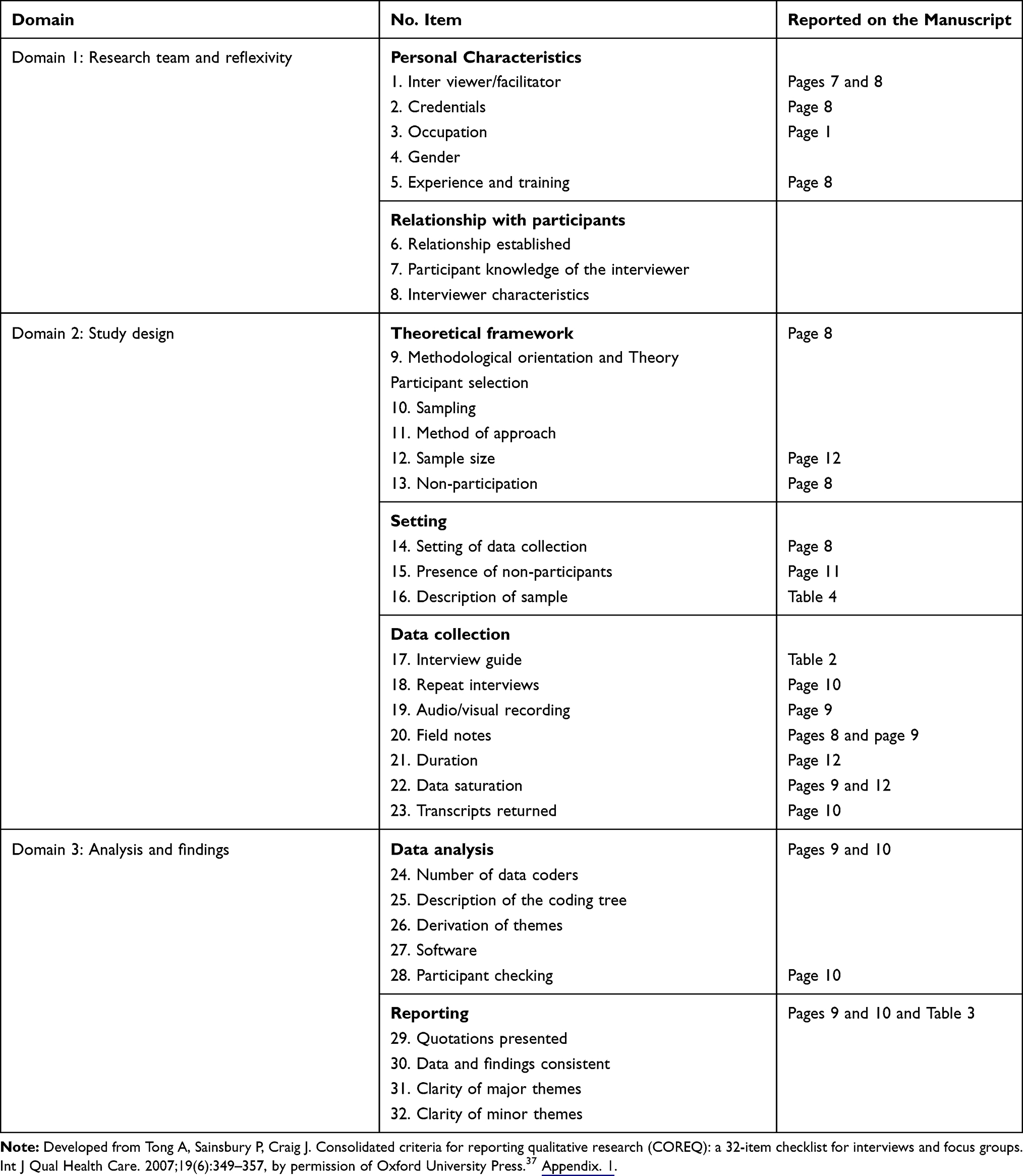 |
Table 1 Study Reported Using COREQ Criteria |
Participants
One nursing home, one SSIAD and the association in charge of foster care families participated in the study. The nursing home and the ambulatory nursing care service are amongst the oldest in the region. Given their geographical location and their significant capacity, they accommodate a very varied population from all over the island (from different municipalities) and thus may be considered as reasonably representative of the general population. Participants were identified through different key informers depending on the mode of living. For individuals living in foster care families, the association in charge of this organization provided a list of potential participants. For those living at home with professional care services, the SSIAD of the city of Lamentin (the second biggest city in Martinique) selected a list of people who met the inclusion criteria. For those who lived in a nursing home, the occupational therapist of this institution selected a list of residents with a Mini Mental States (MMS) score >23. Accordingly, the key informers (ie, the association in charge of foster care, the SSIAD or the occupational therapist, respectively) asked to the eligible participants whether they agreed to be contacted by the researchers and systematically accompanied the researcher for the first contact.
The inclusion criteria for participants were: i) receiving professional care services at home (ie, meal delivery, formal care, SSIAD), or living in foster care family or in a nursing home. ii) being 65 years of age or older, with no major cognitive impairment (MMS >23), iii) speak French and iii) agreeing to participate. To ensure a diversity of situations we purposively sampled respondents based on age, sex, length of time since the change, socio-cultural level, old place of residence, number of children, and marital status. A non-probabilistic sampling procedure consisting of selecting participants considered to be typical of the target population (“reasoned sampling”) was carried out. Only 2 participants refused to participate, one from the nursing home and the other from a foster care family.
Data Collection
Before the interview period, a semi-structured interview guide was created (Table 2) using a framework developed by the project group members. The group included a public health physician and a social psychologist based in metropolitan France as well a Doctor of Sociology and a PhD student in health sciences with a background in sociology and qualitative research, who were based in Lamentin, Martinique. The first 5 interviews were conducted together by the Health sciences PhD student (RC) and the sociologist (SD), who has strong experience working with the target population. Further interviews were conducted by RC alone. Interviews were conducted with an open attitude, using an exploratory approach. They began with a broad question about the experience of the living environment
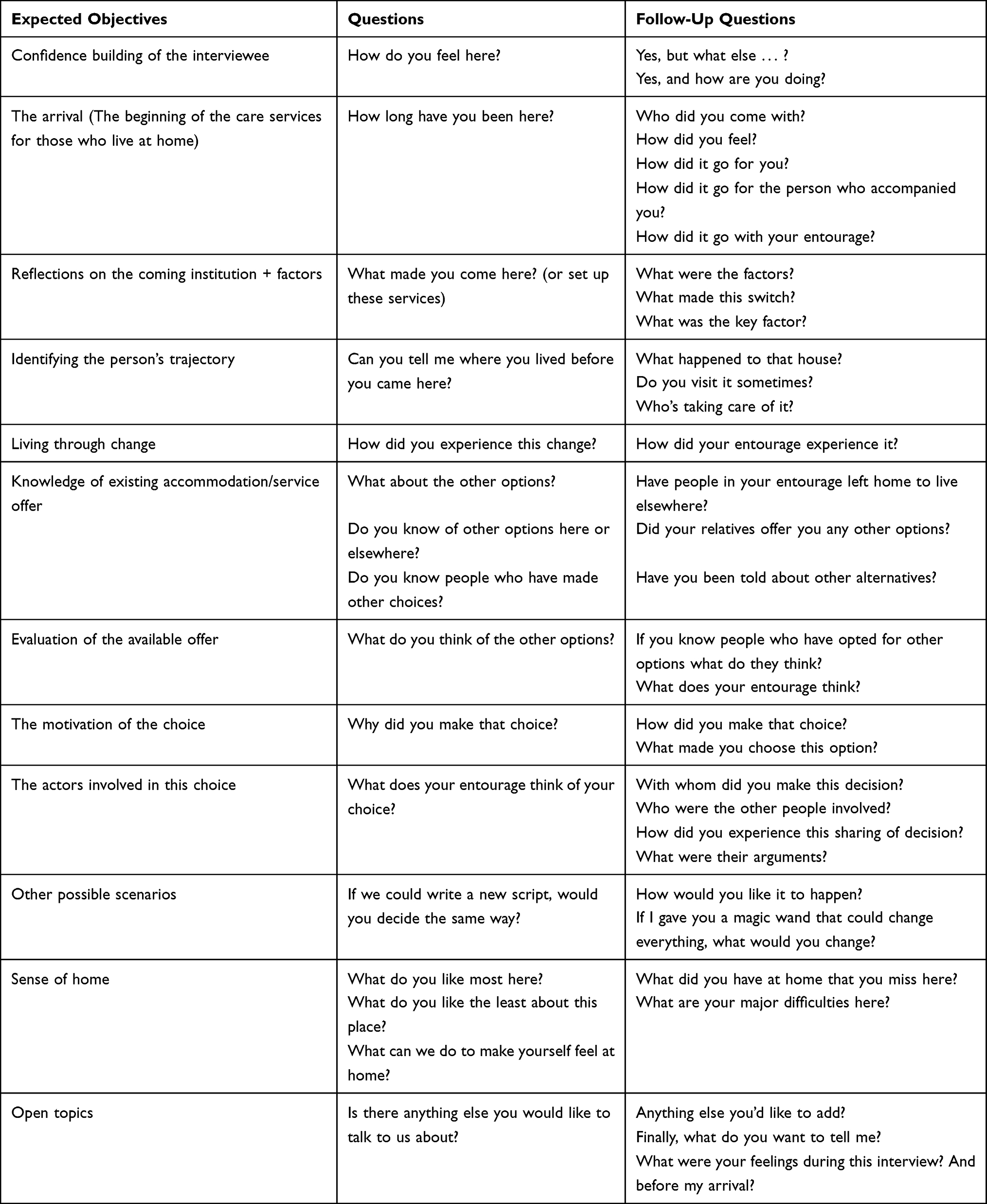 |
Table 2 Semi-Structured Interview Guide |
We would like to exchange with you about your life since you asked for home services/began living with the foster care family/entered this institution, about the reasons that led you to these changes, and how you experienced these changes.
Researchers used rephrasing and probing questions throughout the interview to guide and encourage participants to talk about different elements of their experience and their perceptions.38 With the permission of the participants, interviews were voice recorded using a digital recorder and then fully transcribed.
The interviews were carried out until data saturation, which was reached when the reading of the interviews did not reveal any new elements.39–41
Data Analysis
Interviews were recoded and transcribed anonymously. In order to become familiarized with the content, identify key topics and ensure an in-depth overall understanding of the content, all transcribed interviews were reviewed by RC and SD in an interactive process. Then, RC and SD analyzed texts independently using the conventional content analysis approach. This analysis is a systematic method of generating new knowledge about perceptions and feelings.42 This step requires going back and forth between every interview across the different codes and themes and their relationships. A data-driven thematic analysis was conducted using the verbatim transcriptions of the interviews, ie, an inductive approach without a theoretical framework to guide the analysis.43 According to the methodology previously published by Dahlgren et al, researchers sought to identify the underlying meaning of the transcribed texts, and then regrouped the parts of the text with similar meaning into paragraphs.44 Then, the paragraphs were divided into units, which were further categorized into sub-themes based on comparable content. The sub-themes were then combined into meaningful themes. After researchers had independently carried out this thematic encoding of the data, they compared notes and discussed disparities until consensus was reached. The two researchers shared their emerging themes and improved their comprehension through discussions with the research project team. All researchers checked the accuracy and clarity of themes and concepts. The research team then collaborated to create Table 3, which shows the final codes names, the sub-themes and themes to provide clear information on the content of the analysis.
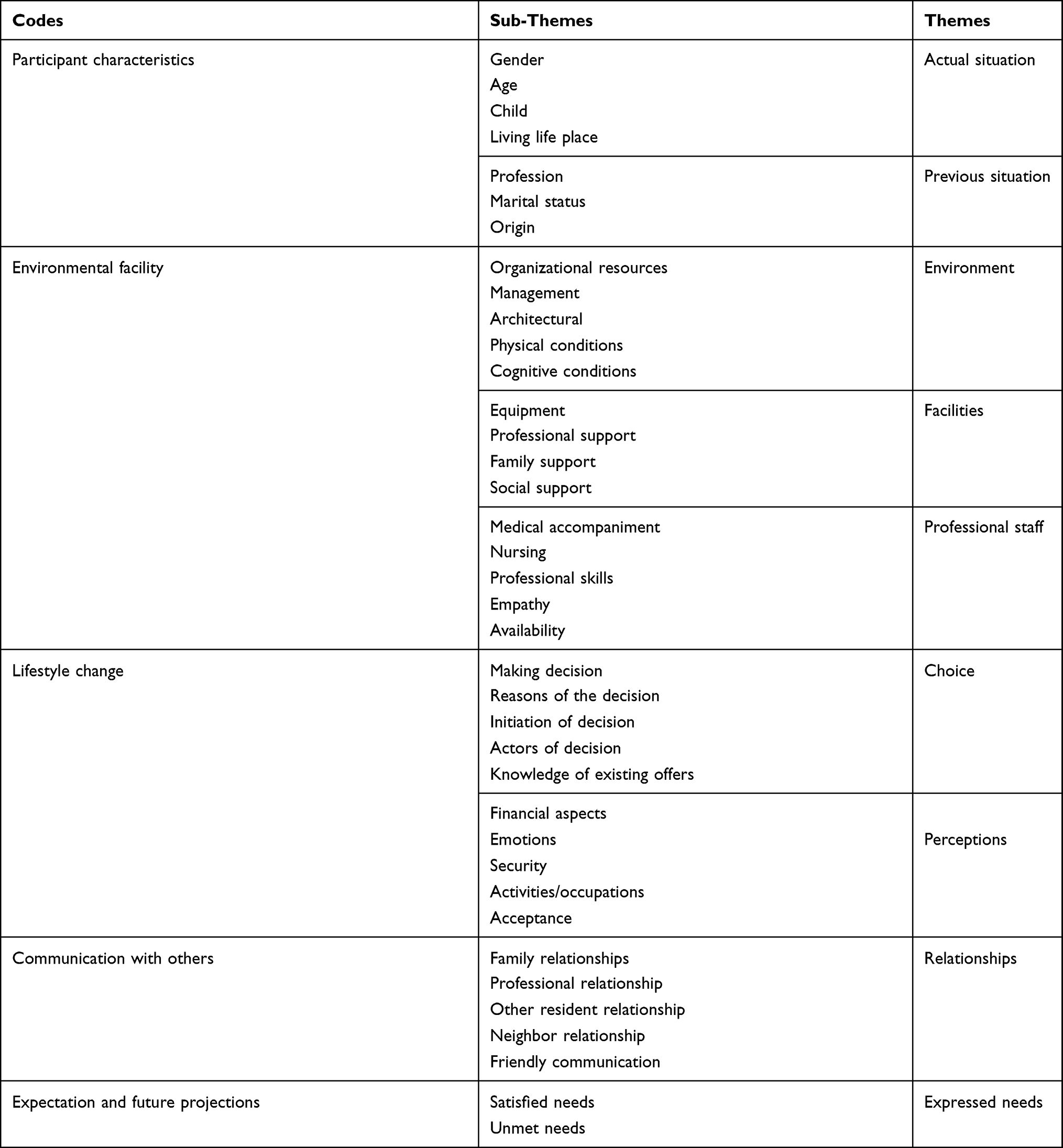 |
Table 3 Codes, Sub-Themes and Themes |
Rigour
We used Lincoln and Guba’s criterion to ensure trustworthiness (credibility, transferability, dependability and confirmability).45 Conclusions of the study analysis were ensured by several techniques to try to reduce bias. Firstly, we confirmed the data source by conducting voice-recorded interview with neutral attitude, and using a full interview transcript. Secondly, data were analyzed separately by two researchers from different disciplines and places within the research laboratory. Then, researchers examined the themes without any prior information or personal bias. Finally, analysis was discussed by all of the researchers. We did not validate written transcribed interviews with the participants because we had not asked for a specific ethics approval to contact participants again after the study. Furthermore, the interviews sometimes brought up painful memories, and we considered making these individuals live these moments again to be potentially harmful. Nevertheless, during the interviews, the researchers made sure to repeat their questions and rephrase the participant answers several times to ensure mutual understanding of the meaning of the questions and answers.
Regulatory Proceeding and Ethics
This study was conducted in accordance with the Declaration of Helsinki. RC gave participants a full explanation of the research project, its objectives, the voluntary nature of participation, the possibility of halting participation at any time without any consequences, the confidentiality of their answers and the way of anonymously handling data 15 days prior to the interview so they could consider their participation.
RC also explained that they should read the information and consent form before agreeing to participate, and that they could be helped if needed. Researchers scheduled the interview appointment at a time and place that was convenient to the participant.
At the beginning of each interview, participants were asked to consent to being audio recorded and to the publication of anonymized responses. Interviews started after the interviewees gave verbal oral consent. Confidentiality was assured by conducting interviews alone with the participants, and not providing any information that participants shared with the other interviewees, professionals or foster family members. All interviews were conducted in a sensitive and non-judgmental way. The study was approved by the Ethics Institutional Review Board of the French Institute of medical research (INSERM) which registered with the flowing identification: IRB00003888, IORG0003254, FWA00005831 and the National Commission on data protection (CNIL).
Results
The interviews lasted an average of 45 minutes, and were held in a place chosen by the participants (usually terrace, living room, or bedroom).
The following themes were identified: perceived causes leading to the change of living environment (with 2 sub-themes: loss of autonomy, and familial relationships); perceived reasons for the choice of living environment, adaptation to change, satisfaction and fulfilled/unmet needs with the living environment.
Characterization of the Older People
Based on data saturation, 34 older adults (20 women and 14 men) were interviewed, with a mean age of 82 years. Among those, nine were living at home with professional care services (mean age 86 years), most often with a relative, 13 were living in a foster care family in different municipalities (mean age 84 years), and 12 were living in a nursing home (mean age 84 years). Most participants had children. Participants’ sociodemographic characteristics are presented in Table 4.
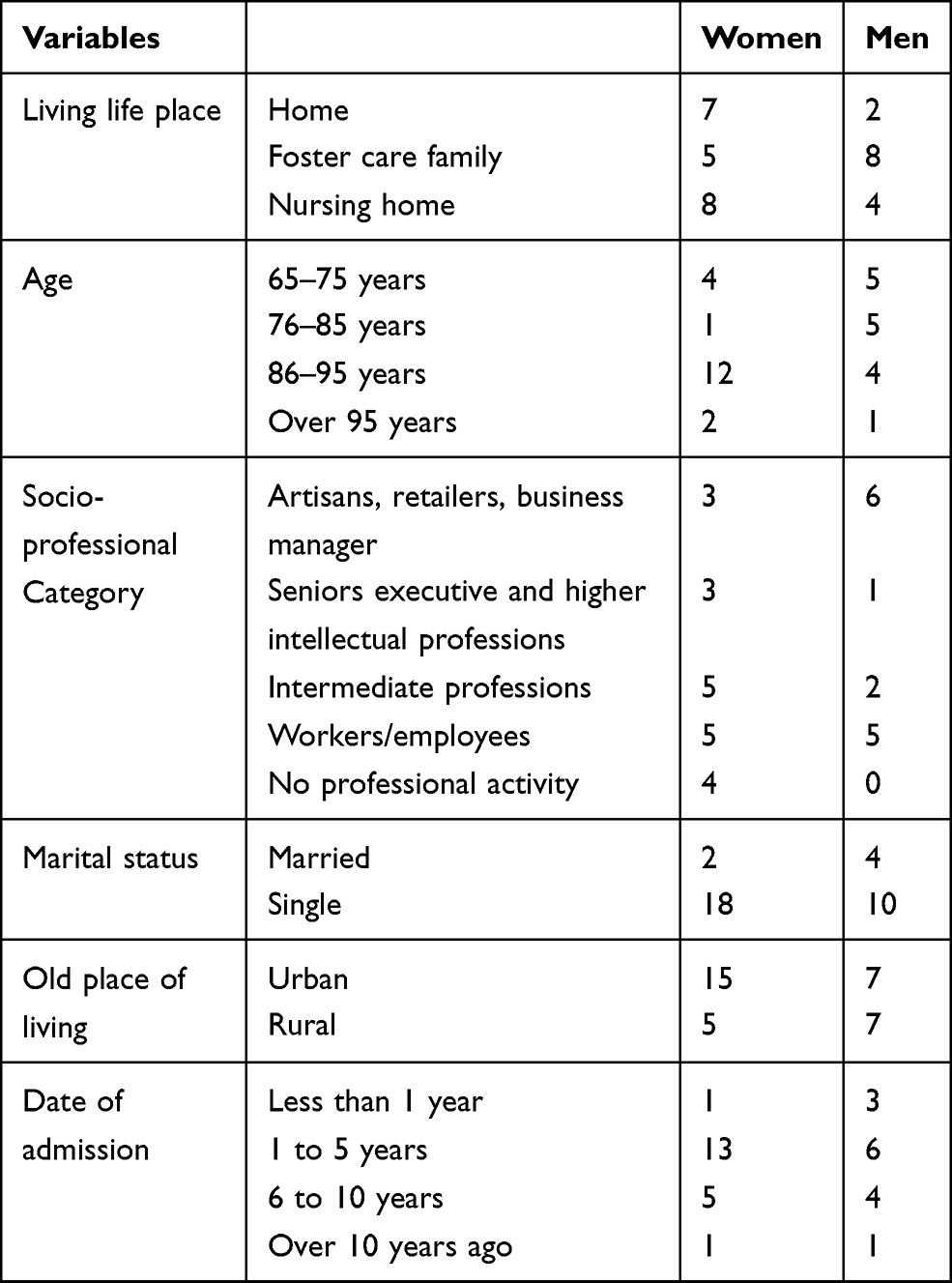 |
Table 4 Participant’s Sociodemographic Characteristics |
Although we did not seek to collect medical data related to the participants’ health status, as requested by the Ethics Institutional Review Board of INSERM, we were given data related to the subjects’ medical conditions. These data revealed that the participants with similar medical conditions, including diabetes, cardiovascular disease, stroke, depression, deafness, blindness, and physical handicaps, were included in the three groups. Therefore, we concluded that the health status of the participants was relatively comparable across the three groups.
Perceived Causes Leading to the Change of Lifestyle and/or Living Environment
Perception of Loss of Autonomy by Older People
For all participants, age progression was a factor leading to the change of living environment; “it’s the age that pushed me”.
“It’s age, you don’t have the means to live as before, you don’t have the means to endure life as before, to continue to have responsibilities”. (Institution).
However, they did not spontaneously evoke their functional and structural impairments nor their activity limitations caused by aging and/or chronic disease. Chronic disease and decreased physical autonomy did not seem to be experienced as a trauma, but as a situation that need to be managed.
I have been sick for a long-time because of my heart, so my children bring the food for me sometimes, then when I feel well, I do it myself, I go out for medical appointments. (At home with services)
Depending on their living environment, participants differed in their understanding of the notion of “loss of autonomy”, which according to the ICF model, is close to participation restriction. Those who stayed at home with professional support evoked the progressive loss of functional autonomy without discomfort while discussing the difficulties associated with managing daily life. Those in foster care family did not speak spontaneously of their loss of functional autonomy. Instead, they spoke of a “feeling of insecurity”, “loneliness”, and “confusion” as a reason for changing their living environment. Those living in the nursing home indirectly evoked their loss of autonomy as a reason for adopting a “preventive” approach to, “delay the loss of autonomy”. Once they were in the institution, the loss of functional autonomy was no longer a concern.
Staying in a house alone, being worried, locked up, you’re scared by everything you hear and you see on TV. This is not a good thing, so we try to find a solution.
Familial Relationships
Older people living at home with services generally reported good relationships with their entourage: “A lot of people come to visit me”, “we laugh together”. They actively participated in organizing their daily life: “I have things to do”, “I don’t have time”. Older adults living in foster families had usually experienced family discomfort and conflicts, especially with siblings (such as inheritance problems) before changing their living environment. “They put me here because I’m embarrassing”. In this context, the occurrence of a brutal event affecting the person (eg, domestic “accident” or “hospitalization”), or his/her environment (“after the hurricane, the house was damaged”), was often the final cause that triggered the change. For those in a nursing home, even if it was a long thought process, the triggering event was often the break-up of the family who left “to metropolitan France”, “to Guadeloupe”, “to Guyana” and the dispersion of members of the community “neighbors have moved” because of economic necessity (to “find a job”, “build elsewhere”, “join my husband”).
Perceived Factors Related to Interactions with the Living Environment
Family and/or environmental ties appeared to be the main determinants of the perception of change, whereas health status did not seem to be strongly associated with the decision to change environments. When financial aspects were evoked, most of the interviewees found it difficult to give details about their income regardless of their living environment. Financial factors may have been a determinant of the initial choice, but once this choice was made, it seemed this was no longer within their purview. The people who stayed at home had to change their lifestyle, integrating the essential support through services. This choice was mostly considered natural and logical: “I am in my house”, “I like home”.
“I’m in my house. I paid for it, it’s to stay in it”.
The possible entry into a nursing home was neither mentioned nor envisaged; “no way”, “It does not suit me”, “for people with no family”. Globally, they had a poor and fragmentary knowledge on existing structures; “I don’t know them”. Two main determinants of this choice were the nature of the family relationship and the status of the owner; “my house is mine” vs tenant; “if I had my house”.
For those living in foster care families, the choice seemed to have been mostly influenced by factors such as the need not to be too far from where they used to live (district, municipality), and the feeling that being in a foster care family would be “closer” to their previous “home”, and that they would be better taken care of (“just three people here”) than in nursing homes.
“She takes good care of all the people, … the people who have already been in this family, … We get along, she is nice”.
However, none acknowledged a personal, thoughtful and deliberate choice even if they did not complain. They felt the decision was not theirs; “sisters”, “neighbors”, “social worker” and the foster care family presented itself as a solution in haste or urgency.
For those who were in a nursing home, the choice was related to a strong sense of prevention. They did not want to take the risk of losing their autonomy at home; “help extend my autonomy”, “you shouldn’t wait until you are really exhausted” and feared managing the environment at home; “lack of security”, “fear”, “isolation”, “difficulty of tasks”.
We come here because that’s precisely it, to perhaps help us to delay the loss of autonomy, to be able to bear the rest of our lives a little more easily, to avoid the most difficult moments. (Institution)
We noted for the three groups, an important reference to “children”, “brothers”, “sisters”, “nephews”, “nieces” or even to “neighbors” or relatives in their interview responses. These persons were somehow involved in their choice; “my sisters have chosen for me”, “my neighbors have decided”, “my nephew who dropped me off” and more broadly in managing their lives; “my sisters are taking me out”, “my sister is taking care of my home”. This involvement also helped the older person to confront these changes and articulate “break-up” and “continuity”; “I am not alone”, “everyone comes as before”, “they call me”.
I didn’t want to end up blind at home, here I am with visually impaired people and other blind people, it helps me to put things into perspective and better accept the day when I will be blind. (Institution)
“I wanted to come here, to enjoy before losing all of my strength, and not being able to do anything, also to adapt, to learn to accept”. (Institution).
“They wanted to put me in a rescue situation, … so I wouldn’t be left alone at home, to feed myself”. (Foster care family).
Adaptation to Changes in Living Environment
Most people in the different groups seemed to experience change as inevitable, and at the same time considered their move as a relief that took them out of “isolation” and domestic hardship.
The prominence of spiritual beliefs in their discourse seemed to facilitate this interpretation of change as the will of spiritual forces; “we accept”, “we must let go”. To mourn one’s home was simpler for people living in nursing homes than for those living in foster care families. Those in foster care families experienced their situation as an eternal transit and complained about proximity with “strangers”; “it’s embarrassing”, “I used to have the whole house for myself, now I have to share with others”. The term “strangers” was often used by people living in foster care families.
“It made me feel funny because it was the first time I came to people’s home, I used to stay alone at home”.
Death was rarely mentioned by participants living at home, who were more preoccupied with their daily lives and organizing their health care. In contrast, participants living in nursing homes had fewer material concerns. Foster family participants did not explicitly name death, but rather referred to it in paraphrases, which were expressed with some degree of fear related to the fact that they felt they were “not in the right place” to die, that they felt alone and too far from their family and ancestors; “I don’t want to die here”, “I don’t want to be buried here”, “my whole family is here”. Conversely, nursing home participants spontaneously spoke of their death or of how they prepared for it; “I’m waiting for someone to call me up there”, “I paid my death insurance”. They thus expressed a greater sense of serenity; “I’m going to leave one day, I’m waiting for that day”, “I’m waiting to go up there to join my loved ones”. Although the older people in both last two groups all mentioned that death was inevitable, it seemed that their perceptions differed somewhat.
As expected, people living at home were those who seemed less affected by the change, as they experienced a growing attachment to the service provider. Nevertheless, older individuals living in a nursing home eventually tended to consider the institution as their “new home” and could somehow “feel at home” whereas in foster care families, they often felt as if they were a “stranger” living in the house of a family but not part of the family “(foster care family) people are at home here”. The nursing home appeared as a “stat of no-return” which seemed in a sense more easily accepted than foster care, which was perceived as a “permanent transit state”; “I wait, I don’t know what to do”. The notion of “home” was central especially for older people who were displaced to either foster care or the nursing home.
Satisfied and Unmet Needs Expressed
The satisfied and unmet needs were spontaneously expressed. For people living at home, the needs expressed concerned a wide variety of demands for services to facilitate and support the continuity of their home life (“tele assistance”, “meal delivery”, “transport”). To a lesser extent, they expressed needs for “safety”, “mobility”, proximity to shops and management of “money”. People in nursing homes first spontaneously mentioned the advantages of being in an institution and their satisfaction concerning mostly small services; “hairdressing”, “manicure-pedicure”, “laundry care” which seemed very important to them. They complained a little about “food”, “lack of staff empathy” or proximity in common areas, but acknowledged that these complaints were rather trivial.
People living in foster care families first expressed the unmet needs, particularly “occupational activities”, “lack of warm relationships”, “lack of outings”, “the authority of the hosts”. The satisfied needs expressed were mostly limited to vital dimensions such as “drinking”, “eating”, “sleeping”, or “signs of attention”.
Discussion
This qualitative study provides deep insights into older people perceptions46 about three different types of lifestyle/living environment changes imposed on them as a result of a decline in their autonomy.
According to the International Classification of Function, aging and chronic diseases may cause impairments, which in turn may limit patients’ activities and independence. Both the environment and the place where the participants were living contributed to their perceptions about their quality of life and health status, and can potentially impact their participation restrictions. Older people can adopt an active or a passive attitude regarding their interactions with the environment, their effective integration and, consequently, their perception of their autonomy. This was particularly obvious for people who decided to go to a nursing home to prevent the degradation of their perceived autonomy (ie, their participation). Their anticipation of a potential loss of autonomy seemed to help them tolerate the change more easily.
In most cases, except for two people who declared they did not participate at all, the older people participated the process of choosing their living environment with relatives and/or professionals. A stronger involvement seemed to simplify their final acceptance of the situation.
For all groups, not only brothers, sisters, children, and grandchildren but also nephews and nieces continued to take part in the person’s referential field. Moreover, friends and neighbors helped support the older people throughout the decision-making process leading up to the change. This underlines the importance of the notion of an “extended family”, also observed in other cultures,47 as an important social network.
Overall, spiritual beliefs seemed to help older people to accept the changes48 and to accept their perceived loss of autonomy in all three groups.
We found that the notion of “home” was central, especially for older people who were displaced to either foster care or a nursing home. Individual housing can be seen as the concretization and fulfilment of a life course,49 and “home” evokes everything to which we are symbolically attached.50 Home is considered to be part of our identity,51 as well as a place of refuge and security. It is also the place of personal expression of freedom and peace. However, this notion becomes a paradox with aging, when autonomy is reduced and domestic accidents become a danger.
Having to leave home for an institution may be viewed as a trauma.52 However, we found that it may be attenuated in some ways, as being surrounded by similar people can also be viewed as comforting and reassuring. There was a “domestication” of the institution that gave residents a sense of “home”. This is consistent with research showing that some people preferred to live in a residence for older people because they were free of the burden of being cared for and supported by their families,53 and reported satisfaction with living in a nursing home.54 This was not the case for people living in foster care families, who experienced their situation as an eternal transit in a family to which they do not belong, and expressed a constant feeling of living with “strangers”. The difficult and sometimes impossible adaptation to the foster care family seemed to accentuate unmet needs and dissatisfaction. Results suggest that, no matter where people live, they need to feel like they are part of the group around them. In order to maintain their autonomy and establish a positive relationship with their new environment, people need both a social climate that could be referred to as a “family” and “a life project” with different occupations. This suggests that the change of living environment could reduce the perceived loss of autonomy by maintaining an acceptable level of participation.
Strengths and Limitations
This study is original in several ways. Firstly, the study investigated and compared three different living environments designed to support older people whose autonomy is decreasing. Secondly, unlike quantitative questionnaires, qualitative methods facilitate the collection of unexpected information that can emerge spontaneously from participants.55,56 However, very few qualitative studies have been undertaken to collect older individuals’ perceptions in this context. Thirdly, Martinique is an interesting place to conduct this research because of the diversity of life paths, multiculturalism, inequalities and particularly rapid demographic changes in proportion of the population who are over 60 years old.57–59 We acknowledge that this study presents some limitations. Even though data saturation was reached, we might obtain additional findings with a different sample. Nevertheless, as in all qualitative studies, this study cannot represent the experiences of all older people losing their autonomy. Instead, this study presents new emerging knowledge about older adults’ perceptions in this situation. In addition, qualitative studies can be subject to analysis and interpretation bias. However, this risk was minimized by the independent coding of the interviews by two researchers, and the frequent exchanges between investigators of different backgrounds.60
Five institutions were contacted by mail, only three agreed to meet with us, and only one agreed to enable us to conduct interviews with the residents. This nursing home is the oldest on the island, and has the largest number of residents. Our experience indicates institutions housing older people are relatively reluctant to open their doors to “outsiders”, even if they are researchers.
Finally, the group of interviewees living in this institution turned out to be diverse in terms of social and professional categories, gender, level of school education, occupation and municipality of origin.
Conclusions
Older peoples’ loss of autonomy is not only caused by physio-pathological factors, but may also be mediated by psycho-social factors and interactions with their living environment. Feeling at home in their new environment was key factor that increased the likelihood that individuals would accept their new accommodations, and feel that the accommodations were meeting their needs, whether they were living in an institution, a foster family, or in their home. These findings provide new and important insights into how older people facing decreasing autonomy experience changes in living environments with implications for the development of services and policy.
Certain dimensions of utmost importance for older people to improve their quality of life and feeling of remaining in control of their life should be used as quality criteria for services and institutions. These dimensions help to recreate the feeling of “home” and maintaining perceived autonomy as much as possible. This means that a personalized needs assessment should be systematically implemented when an older person enters any type of institution. This would enable the institution to better understand their needs, and makes it possible to achieve two major objectives: to feel at home and to maintain the greatest possible perceived autonomy.
Implications for Practice
In practice, these results call for the development of tools designed to carry out personalized assessment at the entrance of older person in institutions or foster care families to better understand the elements that should be considered to help those people feeling at home and maintaining their autonomy. Although Martinique is a French territory, it is an overseas Caribbean region, which retains its own identity, due to its history and its geography. In order to develop these assessment tools, this type of study should be repeated in different countries and different communities as social and cultural factors may be strong determinants of the dimensions mentioned above.
Abbreviations
COREQ, COnsolidated criteria for Reporting Qualitative research; INSERM, French National Institute of Health and Medical Research; MMS, Mini Mental States; SSIAD, Services de Soins Infirmiers à Domicile, ie, home nursing services.
Data Sharing Statement
All the data of the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
We confirm that verbal informed consent was approved by the Ethics Institutional Review Board of INSERM, and that the participants' informed consent included publication of anonymized responses.
Acknowledgments
We thank Alexandra DIMA for her participation and advice. We also thank SEMAVIL, Max TANIC, The Nursing Home of Lamentin city, The SSIAD of Lamentin and AMDOR association for the inclusion of participants.
Thanks to Sarah SKINNER for the proofreading.
Funding
This work was supported by both public (Association National de la Recherche et de la Technologie: national association for research and technology) and private funding from the: Conventions Industrielles de Formation par la REcherche (CIFRE), (Industrial Training Agreements through Research) program.
Disclosure
All authors report no conflicts of interest.
References
1. Dumont G-F. Les Territoires Face Au Vieillissement En France Et En Europe? (The Territories Face of Aging in France and Europe). Géographie - Politique- Prospective. Paris: Éditions Ellipses; 2006:416 p.French.
2. Barbieri M. La mortalité départementale en France ». (Departmental mortality in France). Population. 2013;68(3):433–479. doi:10.3917/popu.1303.0433
3. Dumont G-F. Vieillissement de la population de France: les trois causes de son accentuation. Popul Avenir. 2017;732(2):
4. Millet C. La décroissance démographique martiniquaise s’amplifierait à l’horizon de 2030. (Martinique’s demographic decline is expected to increase by 2030). INSEE Flash. 2017; 66. French.
5. Breton D, Condon S, Marie C-V, Temporal F. Les départements d’Outre-Mer face aux défis du vieillissement démographique et des migrations. (Overseas regions facing the challenges of demographic aging and migration). Population Sociétés. 2009;460:4.
6. Temporal F, Marie C-V, Bernard S. Insertion professionnelle des jeunes ultramarins: DOM ou métropole? (Professional integration of young ultramarines: overseas regions or cities?). Population. 2011;66(3):555–599. doi:10.3917/popu.1103.0555
7. Bessy P, Riche C. Le retour au pays pour la retraite des personnes nées dans les DOM. Une enquête sur les intentions. (The return to the country for the retirement of people born in the overseas regions. An inquiry into intentions). Economie et statistique. 1993;270(1):51–61. doi:10.3406/estat.1993.5825
8. Diderichsen F, Andersen I, Manuel C, et al. Health Inequality - determinants and policies. Scand J Public Health. 2012;40(8_suppl):12–105. doi:10.1177/1403494812457734
9. Wood P-H-N, Badley E. An epidemiological appraisal of disablement. In: Bennett AE, editor. Recent Advances in Community Medicine. Edinburgh: Churchill Livingstone; 1978:149–173.
10. Rockwood K, Fox RA, Stolee P, Robertson D, Beattie BL. Frailty in elderly people: an evolving concept. CMAJ. 1994;150(4):489–495.
11. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56(3):M146–M156. doi:10.1093/gerona/56.3.M146
12. Prince M, Ali GC, Guerchet M, Prina AM, Albanese E, Wu YT. Recent global trends in the prevalence and incidence of dementia, and survival with dementia. Alzheimers Res Ther. 2016;8(1):23. doi:10.1186/s13195-016-0188-8
13. Hogan D, Macknight C, Bergman H. On the behalf of the steering committee, Canadian initiative on frailty and aging, models, definitions and criteria of frailty. Aging Clin Exp Res. 2003;15(3):3–29.
14. Nagi S-Z. jhnkj. Health Society. 1976;54(4):439–467.
15. Muller F, Denis B, Valentin C, Teillet L. Human ageing: demographic trends and medical implications. Nutrition Clinique et Métabolisme. 2004;18(4).
16. Dormont B, Grignon M, Huber H. Health expenditure growth: reassessing the threat of ageing. Health Econ. 2006;15(9):947–963. doi:10.1002/hec.1165
17. Hébler S. Perte D’autonomie Précoce Des Séniors, Tempérée Par L’aide De L’entourage. (Early Loss of Autonomy of Seniors, Tempered by Help from Those Around Them). INSEE;2018:92. French
18. Fanon J-L Analyse de la réponse du dispositif sanitaire et médico-social aux besoins de la population âgée dépendante en Martinique. (Analysis of the response of the health medico-social system to the needs of the dependent elderly population in Martinique). La société Martiniquaise de Gérontologie et Gériatrie. DEPAMAR, Juillet 2012. French
19. Beaugendre C, Breton D, Marie C-V. « Faire famille à distance » chez les natifs des Antilles et de La Réunion. (« Making family at a distance » among natives of the Antilles and Reunion). Recherches familiales. 2016;13(1):35–52. doi:10.3917/rf.013.0035
20. Meron M, Okba M, Viney X. Les femmes et les métiers: vingt ans d’évolutions contrastées. (Women and professions: twenty years of contrasting developments. Social data). In: Données sociales La société Française. INSEE. 2006:225–234.
21. Lavoie J-P Familles et soutien aux parents âgés dépendants. (Families and support for dependent elderly parents). Paris et Montreal, L’Harmattan, 2000, cite dans Lien social et Politique, 2001, 46, 181–183. French
22. Weber A. Des enquêtes nationales pour connaître l’aide apportée par les proches en raison d’un handicap ou d’un problème de santé. (National surveys to find out about help from family members due to a disability or health problem). Inf Sociales. 2015;n° 188(2):42–52. (). doi:10.3917/inso.188.0042
23. Finkelstein ES, Carrington Reid M, Kleppinger A, Pillemer K, Robinson J. Are baby boomers who care for their older parents planning for their own future long-term care needs? J Aging Soc Policy. 2012;24(1):29–45. doi:10.1080/08959420.2012.630905
24. Kojima G, Liljas A EM, IIiffe S. Frailty syndrome: implications and challenges for health care policy. Risk Manag Healthc Policy. 2019;12:23–30.
25. Mantovani J, Rolland C, Andrieu S Étude sociologique sur les conditions d’entrée en institution des personnes âgées et les limites du maintiena domicile (Sociological study on the conditions of entry into an institution for the elderly and the limits of home support). DREES, 2008, 83. French
26. Abdi S, Spann A, Borilovic J, De Witte L, Hawley M. Understanding the care and support needs of older people: a scoping review and categorization using the WHO international classification of functioning, disability and health framework (ICF). BMC Geriatr. 2019;19(1):195. doi:10.1186/s12877-019-1189-9
27. Blasimme A. Physical frailty, sarcopenia, and the enablement of autonomy: philosophical issues in geriatric medicine. Aging Clin Exp Res. 2017;29(1):
28. Lee VS, Simpson J, Froggatt K. A narrative exploration of older people’s transitions into residential care. Aging Ment Health. 2013;17(1):48–56. doi:10.1080/13607863.2012.715139
29. Boggatz T. Quality of life in old age – a concept analysis. Int J Older People Nurs. 2016;11(1):55–69. doi:10.1111/opn.12089
30. Vanleerberghe P, De Witte N, Claes C, Schalock RL, Verté D. The quality of life of older people aging in place: a literature review. Qual Life Res. 2017;26(11):2899–2907. doi:10.1007/s11136-017-1651-0
31. Ingrand I, Paccalin M, Liuu E, Gil R, Ingrand P. Positive perception of aging is a key predictor of quality-of-life in aging people. PLoS One. 2018;13(10):e0204044. doi:10.1371/journal.pone.0204044
32. Van Leeuwen KM, Van Loon M S, Van Nes FA, et al. What does quality of life mean to older adults? A thematic synthesis. PLoS One. 2019;14(3):e0213263. doi:10.1371/journal.pone.0213263
33. Morris JN, Declerq A, Hirdes JP, et al. Hearing the voice of the resident in long-term care facilities – an internationally based approach to assessing quality of life. J Am Med Dir Assoc. 2018;19(3):207–215. doi:10.1016/j.jamda.2017.08.010
34. Hébler S Perte d’autonomie précoce des seniors, tempérée par l’aide de l’entourage. (Early loss of autonomy of older people, tempered by the help of the entourage). INSEE Martinique, 2018, 92. French
35. Répertoire des établissements d’hébergement pour personnes âgées. (Directory of Seniors’Accommodation). Martinique, 2019. French
36. Bardin L L’analyse de contenu. (The content analysis). Paris: Presses universitaires de France; 2007. French
37. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
38. Kivits J, Balard F, Fournier C, Winance M Les recherches qualitatives en santé. (Qualitative health research). Armand Colin; 2016. French
39. McDowell I. Measuring Health. A Guide to Rating Scales and Questionnaires. Oxford: Oxford University Press; 2006.
40. Coloralfi KJ, Evans B. Qualitative descriptive methods in health science research. HERD. 2016;9(4):16–25. doi:10.1177/1937586715614171
41. Fritzen-Pedicini C, Bleasdale S-C, Brosseau L-M, et al. Utilizing the focused conversation method in qualitative public health research: a team-based approach. BMC Health Serv Res. 2019;19(1):306. doi:10.1186/s12913-019-4107-0
42. Bengtsson M. How to plan and perform a qualitative study using content analysis. Nurs Plus Open. 2016;2:8–14. doi:10.1016/j.npls.2016.01.001
43. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
44. Dahlgren L, Emmelin M, Winkvist A. Qualitative Methodology for International Public Health. Umea ̊: Umea ̊ International School of Public Health, Epidemiology and Public Health Sciences, Umea ̊ University; 2004.
45. Lincoln Y, Guba E Naturalistic Inquiry. Newbury Park: Sage; 1985.
46. Bardin L L’analyse de contenu. (The content analysis). Paris: Presses universitaires de France, 2007.French
47. Nguyen A-W, Taylor R-J, Chartters L-M, Taylor H-O, Lincoln K-D, Mitchell U-A. Extended family and friendship support and suicidality among African Americans. Soc Psychiatry Psychiatr Epidemiol. 2017;52(3):299–309. doi:10.1007/s00127-016-1309-1
48. Velasco-Gonzalez L, Rioux L-J. The spiritual well-being of elderly people: a study of a French sample. Relig Health. 2014;53(4):1123–1137. doi:10.1007/s10943-013-9710-5
49. Cho E, Kim H, Kim J, Lee K, Meghani S-H, Chang S-J. Older adult residents’ perceptions of daily lives in nursing homes. J Nurs Scholarsh. 2017;49(5):495–503. doi:10.1111/jnu.12314
50. Rollero C. and De Piccoli N. Does place attachment affect social well-being? Eur Rev Appl Psychol. 2010;60(4):233–238.
51. Vitman Schorr A, Khalaila R. Aging in place and quality of life among the elderly in Europe: a moderated mediation model. Achr Gerontol Geriatr. 2018;77:196–204. doi:10.1016/j.archger.2018.04.009
52. Moore A, Carter B, Hunt A, Sheikh K. ‘I am closer to this place’ – space, place and notions of home in lived experiences of hospice day care. Health Place. 2013;19:151–158. doi:10.1016/j.healthplace.2012.11.002
53. Haney D-B, Fletcher P-C, Robertson-Wilson J-E. A qualitative investigation of the self-perceived health behavior changes in seniors after their transitions into a retirement home. Clin Nurse Spc. 2018;32(3):129–138. doi:10.1097/NUR.0000000000000372
54. McCann M, O’Reilly D, Cardwell C-A. Census-based longitudinal study of variations in survival amongst residents of nursing and residential homes in Northern Ireland. Age Ageing. 2009;38(6):711–717. doi:10.1093/ageing/afp173
55. Rodriguez-Martin B, Martinez-Andrés M, Cerva-Monteagudo B, Notario-Pacheco B, Martinez-Vizcaino V. Perception of quality of care among residents of public nursing-homes in Spain: a grounded theory study. BMC Geriatr. 2013;13(1):65. doi:10.1186/1471-2318-13-65
56. Spangler D, Blomqvist P, Lindberg Y, Winblad U. Small is beautiful? Explaining resident satisfaction in Swedish nursing home care. BMC Health Serv Res. 2019;19(1):886. doi:10.1186/s12913-019-4694-9
57. Drageset J, Haugan G, Tranvag O. Crucial aspects promoting meaning and purpose in life: perceptions of nursing home residents. BMC Geriatr. 2017;17(1):254. doi:10.1186/s12877-017-0650-x
58. Robbert J, Roy R. The effects of sociodemographic factors on quality of life among people aged 50 years or older are not unequivocal: comparing SF-12, WHOQOL-BREF, and WHOQOL-OLD. Clin Interv Aging. 2019;14:231–239. doi:10.2147/CIA.S189560
59. Choi K-S, Stewart R, Dewey M. Participation in productive activities and depression among older Europeans: survey of health, ageing and retirement in Europe (SHARE). Int J Geriatr Psychiatry. 2013;28(11):1157–1165. doi:10.1002/gps.3936
60. Carr L-T. The strengths and weaknesses of quantitative and qualitative research: what method for nursing? J Adv Nurs. 1994;20(4):716–721. doi:10.1046/j.1365-2648.1994.20040716.x
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.