Back to Journals » Integrated Pharmacy Research and Practice » Volume 13
Expanding HIV Self-Test Kits via Community Pharmacies in Rwanda Has Improved Availability, but Affordability Remains an Issue
Authors Nsengimana A ![]() , Biracyaza E
, Biracyaza E ![]() , Manirakiza A
, Manirakiza A ![]() , Nsekonziza Y, Niyonsenga E
, Nsekonziza Y, Niyonsenga E ![]() , Ntirenganya F
, Ntirenganya F ![]() , Umumararungu T
, Umumararungu T
Received 15 August 2024
Accepted for publication 14 December 2024
Published 20 December 2024 Volume 2024:13 Pages 243—257
DOI https://doi.org/10.2147/IPRP.S489143
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Walid Al-Qerem
Amon Nsengimana,1 Emmanuel Biracyaza,2 Augustin Manirakiza,3 Yvette Nsekonziza,3 Emmanuel Niyonsenga,3 Frederic Ntirenganya,4 Théoneste Umumararungu3
1USAID Global Health Supply Chain Program-Procurement and Supply Management (GHSC-PSM) Project, Kigali, Rwanda; 2School of Rehabilitation Faculty of Medicine, Université de Montréal, Montreal, QC, Canada; 3Department of Pharmacy, University of Rwanda, Kigali, Rwanda; 4Department of HIV/AIDS, Diseases Prevention and Control, Rwanda Biomedical Centre (RBC), Kigali, Rwanda
Correspondence: Amon Nsengimana, Email [email protected]
Background: The World Health Organization (WHO) recommends HIV self-testing (HIVST) to complement the existing HIV testing services. Pursuant to this, Rwanda approved the over-the-counter sale of Oral Quick HIV self-tests in community pharmacies, facilitating home testing and addressing accessibility issues. However, the availability and affordability of HIVSTs in these settings remains unexplored. Hence, this study determined the availability and affordability of HIVST kits in Community Pharmacies across Rwanda.
Methods: This cross-sectional study was conducted among 220 licensed community pharmacists between February and May 2023. Tools standardized by WHO and Health Action International (HAI) were used to evaluate the affordability of HIVST kits. An ANOVA followed by a post-hoc test examined significant price differences across regions. Bivariate and multivariate logistic regression analyses were used to identify the factors associated with the availability of HIVST kits.
Results: The availability was 76%, with 53% being finger-stick tests. Pharmacies owned by pharmacists were almost twice as likely to have HIVST available (AOR=1.858; 95%: 1.280– 2.629, p=0.007) than their counterparts. Pharmacies in Kigali were more likely to stock HIVST (AOR=3.549; 95%: 1.283– 9.814, p=0.015) than in other regions. Pharmacies experiencing frequent requests for HIVST were more likely to have HIVST available (AOR=0.22; 95%: 0.07– 0.66, p< 0.001) than those with fewer requests. Both oral quick and finger-stick HIVST were priced beyond the affordability of low-income earners. Moreover, significant price differences for Oral Quick HIVST (F=11.349; p< 0.001) were observed across regions, with Kigali’s prices significantly differing from those in the southern (p< 0.001) and western Provinces (p=0.004).
Conclusion: HIVSTs are not economically priced for the lowest-paid workers, with variations in availability and prices across the country. Policymakers should apply subsidies or price regulation strategies to make HIVST more affordable, ensuring equitable access to all regions and income levels.
Keywords: community pharmacies, HIV-self tests, availability, affordability
Background
Globally, by 2022, 39 million people were living with human immunodeficiency virus (HIV), while 630 thousand lives were lost due to acquired immunodeficiency syndrome (AIDS) related illnesses.1–3 Two-thirds of the globally reported people living with HIV were from Africa due to a combination of socio-economic, cultural, and structural factors that contribute to the spread of the virus on the continent.1–3 Despite the pressing urgency of public health issues caused by HIV, a significant proportion of individuals worldwide remains unaware of their HIV status. The WHO’s goal is that 95% of people living with HIV (PLHIV) should know their HIV status by 2025.1,4 However, in 2022, globally, only 86% of PLHIV knew their status while 5.5 million people were unaware of their HIV status.1,2 During the same year, in Africa, 90% of PLHIV were aware of their HIV status.1–3
To enhance access to HIV testing services and ensure that 95% of PLHIV will know their HIV status by 2025, the WHO has recommended HIV self-testing (HIVST) as a complement to existing HIV testing services.5,6 The WHO further endorsed this by declaring HIVST a safe and effective testing option, offering convenience to priority populations who might otherwise remain untested.7 Interest in HIVST has increased since then, with many countries adopting HIVST.8 The advantage of HIVST is its ability to allow individuals to collect and interpret their own oral or blood specimens in a private setting, thus allowing for independent testing.9 Due to accessibility issues, HIVST is also helpful in reaching people who are unable to access existing HIV testing sites. In the effort to reduce HIV-associated morbidity, mortality, and transmission, HIVST serves as a critical step towards both prevention and treatment.10
HIV treatment and prevention services are predominantly delivered through public health facilities in most Sub-Saharan Africa (SSA) countries.11,12 However, clients have shown an interest in accessing HIV tests via community pharmacies.13 They prefer these settings because of their convenience, lower costs, faster services, privacy, and responsiveness to pharmacy personnel. These settings offer a vast, largely untapped potential for the delivery of HIV testing to some people because they are less stigmatizing than traditional testing sites.6,14 The accessibility of community pharmacies for HIV testing is also an opportunity for pharmacists to contribute to the identification of undiagnosed HIV in the community.15,16 In areas like SSA, community pharmacy-based HIV service delivery boosts uptake without compromising clinical outcomes and is acceptable among stakeholders.13 In 2012, a combination of health facilities and community-based approaches increased HIV testing in 124 low and middle-income countries (LMICs), testing 118 million people.17 Considering this care-seeking behaviors, community pharmacies offer a unique reach to target populations.12
While the availability of HIVST increases their uptake,18 their cost is also a key factor that clients consider when choosing an HIV test.19 The higher the price, the less affordable they become, particularly for people in Low- and Middle-Income Countries (LMICs), where financial resources are often limited.20,21 Unaffordability and unavailability of medicines have emerged as critical challenges for patients and healthcare systems across LMICs, affecting equitable access to healthcare.22 This leads to significant challenges in accessing necessary treatments, often resulting in catastrophic healthcare expenditures and driving families into financial hardships and impoverishments.23,24 In many African countries, the cost of HIVST varies significantly due to several factors. These factors include the source of the kits, whether they are distributed through public or private channels, and local market dynamics such as chains and distribution costs.11,25 Research conducted in these countries has shown that public facilities often receive subsidies or external financial support for these tests which can reduce the cost to end users.26 In contrast, private providers typically charge higher prices to cover operational costs and profit margins, leading to higher prices for consumers.11,27 The integration of HIVST into existing healthcare services, such as those in Malawi, South Africa, Zambia, and Zimbabwe, shows how different models of distribution, such as community-based or facility-based—affect cost structures.25,28
Although Rwanda has met UN/AIDS 95–95-95 targets,3,29 one of which aims for 95% of PLHIV to know their status, expanding HIV testing is still crucial for meeting the WHO 2030 HIV elimination objectives. Based on recent data, HIV testing is available in 99% of health facilities, with all health facilities recognized by the Rwanda Ministry of Health (MOH) offering free testing.30,31 However, private clinics do not offer free HIV testing; instead; they offer it at a price determined by MOH’s rules and regulations.31 Conversely, the cost of HIVST kits in community pharmacies remains unregulated. When the WHO released a strategic framework in 2018, assisting countries in implementing and expanding the use of HIV self-testing,9,32 Rwanda approved the over-the-counter sale of Oral Quick HIVST kits in community pharmacies, enabling home testing.33 This is viewed as an essential step in increasing HIV status awareness, overcoming barriers such as stigma, and accessibility issues in healthcare such as waiting times for HIV testing at public health facilities. However, there is still a knowledge gap regarding whether HIVSTs are widely available and economically priced for Rwandans who prefer community pharmacies. To address this gap, this study aimed to determine the availability and affordability of HIVST in Community Pharmacies in Rwanda. The issue of affordability is particularly relevant considering that the median income in Rwanda is 621$,34 with the lowest-paid employee earning 1000 Rwf (0.7$) per day.35–37 The study findings will help the Rwandan healthcare system examine the implementation progress of expanding access to HIVST via community pharmacies and design new measures to strengthen it. The findings will also inform HIV prevention and testing policies in Rwanda and develop community pharmacy services regarding HIVST.
Methods
Study Design
This cross-sectional study was conducted between February 1st and May 30, 2023, and aimed to determine the availability and affordability of HIV self-test kits in Community Pharmacies in Rwanda.
Study Settings and Population
Rwanda is a landlocked country in East Africa composed of four administrative provinces (East, West, South, North) and the capital city of Kigali. It shares borders with the Democratic Republic of Congo in the west, Tanzania in the east, Uganda in the north, and Burundi in the south. The World Bank classifies Rwanda as a low-income country.38 In 2022, the fifth Rwandan population and housing census reported a population of 13,246,394 people. The most common economic activity in Rwanda is agriculture (53.4% of the total employment). Nearly 2.3 million Rwandan households engage in this sector.39 The pharmaceutical workforce consists of pharmacists and pharmacy technicians. As of 2022, the National Pharmacy Council (NPC) has reported 1138 registered Pharmacists and 12 pharmacy technicians.40 The pharmacy profession is regulated by the Rwanda Food and Drug Authority (FDA). Most pharmacists work in the private sector, particularly community pharmacies, whereas 39% work in the public health sector.41 Throughout the study period, 720 Rwanda FDA-authorized community pharmacies were established across the country.
Sample Size and Sampling Procedure
By applying the Yamane method, we calculated the sample size (nY) for this study based on the number of community pharmacies listed by the Rwanda FDA,  ,42 where “N” stands for population size, and “e” for alpha level (e = 0.05) at the confidence level of 95%. By substituting values, we computed
,42 where “N” stands for population size, and “e” for alpha level (e = 0.05) at the confidence level of 95%. By substituting values, we computed  257. From the calculated sample size, participants were recruited using simple random sampling based on the geographical distribution of community pharmacies across various regions of the country, reflecting a well-considered selection made via simple random sampling. However, we obtained active participation from 220 community pharmacists for an intended sample size of 257, resulting in an 85% response rate. Lack of time and interest were the primary reasons for declining participation in the study.
257. From the calculated sample size, participants were recruited using simple random sampling based on the geographical distribution of community pharmacies across various regions of the country, reflecting a well-considered selection made via simple random sampling. However, we obtained active participation from 220 community pharmacists for an intended sample size of 257, resulting in an 85% response rate. Lack of time and interest were the primary reasons for declining participation in the study.
Data Collection Procedures
The data collection process was carried out by three interns from the University of Rwanda, each with prior experience in data collection. Prior to data collection, they underwent a thorough two-days training program consisting of sessions lasting three hours each, focusing on ethical considerations, data collection instruments, and study objectives, all conducted under the supervision of the research team. Subsequently, the data collectors reached community pharmacists at their respective workplaces, providing them with a detailed explanation of the underlying objectives of the study. Upon obtaining consent from willing participants, the data collectors distributed a self-administered questionnaire, which was prepared in English to adhere to academic standards in Rwanda. Throughout the data collection process, the data collectors remained readily available to provide detailed explanations to the participants who sought clarification on any aspect of the questionnaire. Participants were assured of their right to withdraw from the study at any point, without the need to provide a reason. Furthermore, data collection was conducted anonymously to uphold confidentiality, ensuring that the participants’ privacy was respected throughout the process.
Data Collection Instruments
The questionnaire was composed of five main parts. The first part focused on pharmacists’ characteristics, including gender, age, marital status, education level, working experience, pharmacy location, and pharmacy ownership. The second part addressed the availability of HIVST kits and unveiled the reasons for the non-availability in certain pharmacies; the third part treated the price of HIVST kits that involved comprehensive evaluation of the pricing of each type available; the fourth part was about clients’ requests for HIVST and the prevalence of clients expressing interest in obtaining HIVST kits and determining weekly occurrence of these requests to evaluate the demand for HIVST kits and the role of pharmacies in meeting this demand; and the last part assessed the views of community pharmacists regarding their role in HIV prevention through an open-ended question, capturing their efforts to curb the spread of HIV.
Data Analysis
The collected quantitative data was imported into Microsoft Excel for cleaning. After cleaning, the dataset was transferred to the Statistical Package for Social Sciences (SPSS) version 25.0 for Windows. The accuracy of the imported data was verified to ensure its reliability. Descriptive statistics, including frequencies, percentages, means, and standard deviations, were used to present quantitative data. Availability was analyzed by checking whether the HIVST kit was present on the day of data collection. When either Finger-stick HIVST or oral-based HIV self-testing options had zero stock, they were categorized as unavailable. A qui-square test was conducted to identify significant variables associated with the availability of HIVST kits. Additionally, bivariate logistic regression analyses were performed to calculate the crude odds ratio (COR) to identify key significant factors of HIVST kit availability. All significant factors from this process were exported to multivariate logistic regression models, which produced adjusted odds ratios (AOR). Confidence interval of 95% was considered for indicating the strength of associations.
To assess both the availability and affordability of HIVST, the WHO and Health Action International (WHO/HAI) methodology was used. WHO/HAI suggests that availability is measured as the percentage of medicine outlets in which the medicine was found on the day of the data collection, while it also suggests that a treatment course requiring more than one day’s wage is unaffordable.43 In Rwanda, the lowest-paid unskilled government worker earns 1000 Rwandan Francs (Rwf) per day, according to the World Minimum Wage.35–37 A similar amount was used in previous studies.36,37 Analysis of Variance (ANOVA) was conducted to assess whether the prices of HIVST kits varied across geographical locations. In all statistical analyses, statistical significance was set at p of less than 0.05, indicating a significant relationship between the variables.
Results
Characteristics of Respondents
Table 1 shows the characteristics of the respondents: 56% of the respondents were aged 24–29 years, 30% were 30–34 years, 9% were 35–39 years, 4% were 40–44 years and only 1% were aged 45 years or above. Regarding educational background, 97% had a bachelor’s degree, while 3% held a master’s degree. The work experience analysis revealed that 76.8% of the respondents had between 1–5 years of professional experience, 17.7% had 6–10 years, 5% had 11–15 years, and 0.5% had more than 15 years of work experience. Most respondents (78%) were pharmacy employees, while 22% were pharmacy owners. During the study period, 60% of the respondents reported working in Kigali City, the capital city of Rwanda.
 |
Table 1 Socio-Demographic Characteristics of the Study Respondents (n=220) |
Availability of HIV Self-Tests in Community Pharmacies
Table 2 shows the availability of HIVST kits in community pharmacies in Rwanda. Among the 220 pharmacies, 24% (n=52) did not have any HIV self-tests available in stock, but 76% (n = 168) did. Of the 220 pharmacies, 53% had Finger-stick HIV self-tests, 23% had Oral Quick HIV self-tests, and 24% had no HIV self-tests. However, among the 168 pharmacies who reported having HIVST kits, 70% had Finger-stick HIV self-tests, while 30% had Oral Quick HIV self-tests. The non-availability of HIVST kits in wholesale pharmacies (46%) and the ambiguity of rules governing HIVST in community pharmacies (27%) were identified as the main contributing factors leading to 24% of pharmacies having no HIVST kits available.
 |
Table 2 Availability of HIV Self-Tests in Community Pharmacies in Rwanda |
One pharmacist said that HIVSTs are not easily available in wholesale pharmacies, and it is not clear whether they are permitted for retail sale. Users are not interested in or trust the quick oral tests. There should be a clear notification regarding their official authorization to be sold in retail pharmacy”. (Female community pharmacist aged 28 years). Another one added, “The blood test-based kits are not available at the wholesale pharmacy level where we used to purchase them, and people do not accept the oral quick tests because they doubt the results it gives”. (Male community pharmacist aged 32 years).
As depicted in Table 3. A chi-square test was conducted to assess the association between the availability of HIVST kits and the geographical locations of community pharmacies. The analysis yielded a Pearson Chi-square statistic of 4.734 with a p-value of 0.316, implying no significant association between the availability of HIVST kits and the geographical location of community pharmacies. These results suggest that the accessibility of HIV self-tests is consistent across different geographic areas, with availability not influenced by the location of community pharmacies.
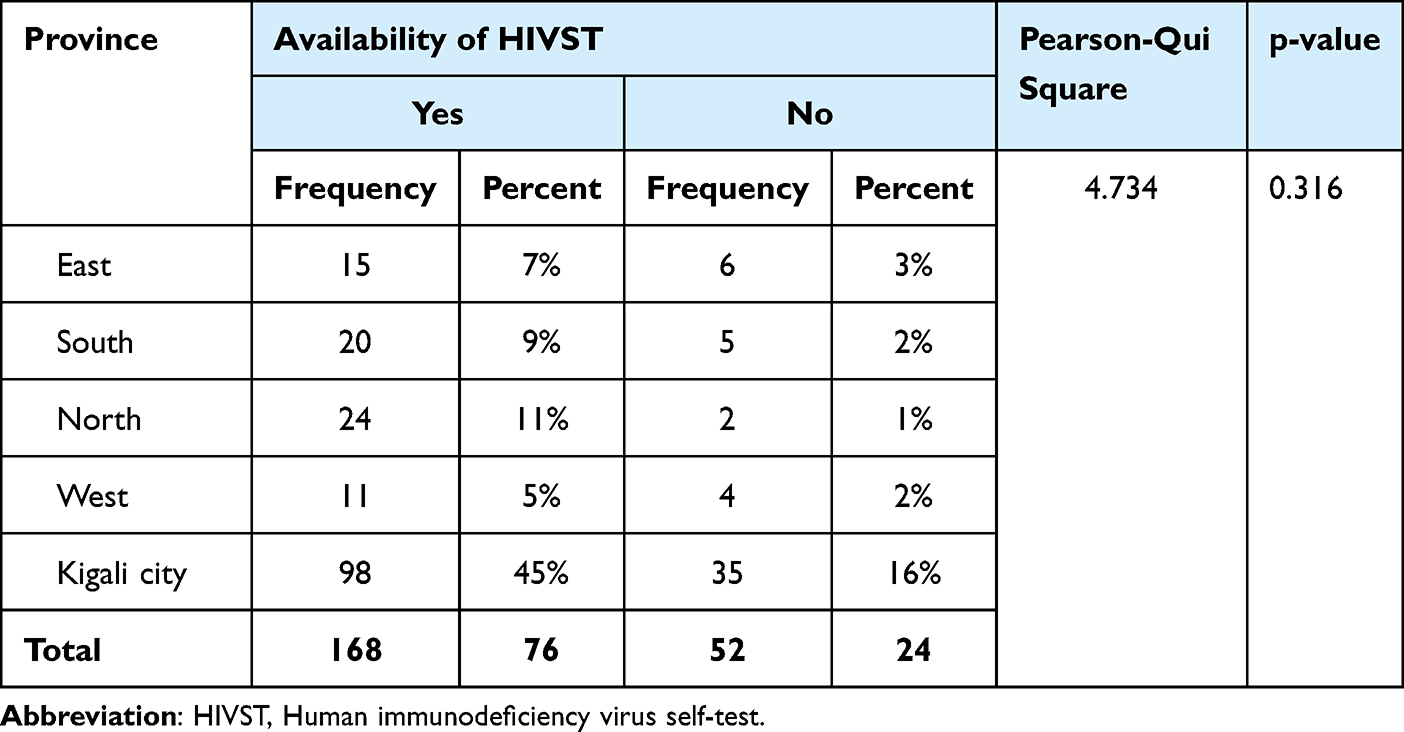 |
Table 3 Availability of HIVST by Geographical Locations of Community Pharmacies |
Clients’ Request of HIV Self-Tests in Community Pharmacies
Table 4 shows that when respondents were asked whether they had been requested by clients to sell HIV self-tests within the previous week, 93% confirmed that they had received such requests, while 7% indicated otherwise. Of the respondents, 63% reported that these requests occurred three or more times per week. Among the various types of HIV self-tests, Finger-stick HIV emerged as the most frequently requested, with 83% of respondents reporting that it was the preferred choice among their clients. A few Pharmacists stated that clients reported the test results at a rate of 2%.
 |
Table 4 Clients’ Request of HIV Self-Tests in Community Pharmacies |
Cost of HIV Self-Tests in Community Pharmacies
Table 5 shows the cost range of Finger-stick HIV self-tests and Oral Quick HIV self-tests, with a Finger-stick HIV self-test costing between 1500Rwf ($1.1) and 3500 Rwf ($2.5) with an average cost of 2500Rwf ($1.8), while Oral Quick tests cost between 2500Rwf ($1.8) and 6000 Rwf ($4.3) with an average of 4438 Rwf ($3.2). The average HIVST was calculated to be $2.50, which is equivalent to a three-day wage for the lowest-paid unskilled employee in Rwanda, and thus, unaffordable. However, most participants reported selling Finger-stick HIVST 1500 Rwf ($1.1), while Oral Quick HIVST was at 2500 Rwf ($1.8). As cost increased, there was a corresponding decrease in the number of users, suggesting a sensitivity to pricing among consumers. Respondents were further asked whether clients had ever claimed HIVST to be expensive. Of the 220 respondents, 62% said that their clients claimed that HIVST were expensive. Half of the respondents (50.5%) confirmed that Oral Quick HIV self-tests were the most frequently reported by clients as expensive HIVST.
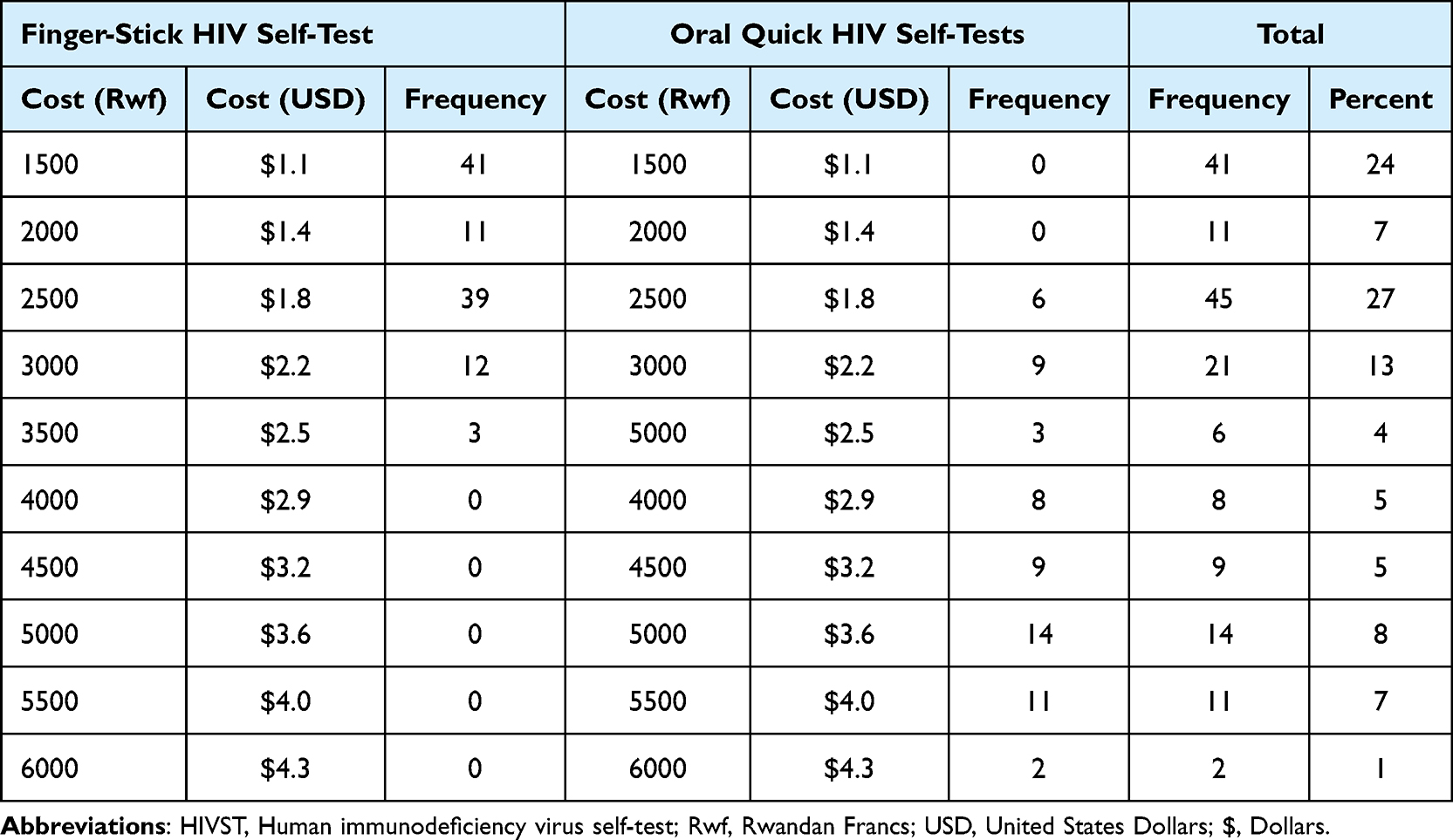 |
Table 5 Costs for HIVST in Community Pharmacies |
Cost of HIV Self-Tests by Region
As shown in (Table 6 and Table 7), the one-way ANOVA showed that the price of Oral Quick HIV self-tests varied significantly across the Rwandan regions, whereas the Finger-stick HIV self-test did not (F=3.845, p=0.06). Following one-way ANOVA, a post hoc test as presented in Table 7, was used to determine which regions had significantly different prices from the others. The results showed that the price of Oral Quick HIV self-tests differed significantly between Kigali City and the two provinces, the Southern (p<0.001), and the Western one (p=0.004).
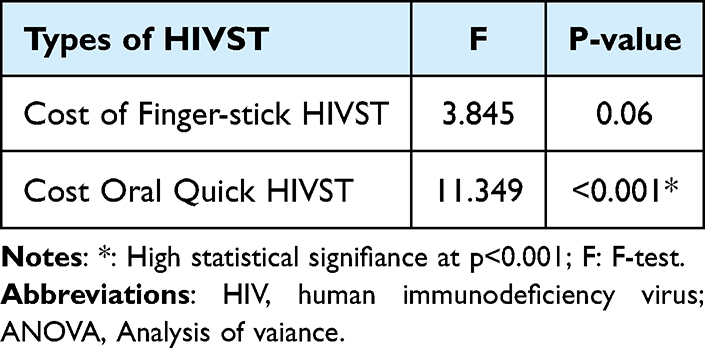 |
Table 6 Results of One-Way ANOVA Test with the Cost of the Types of HIVST |
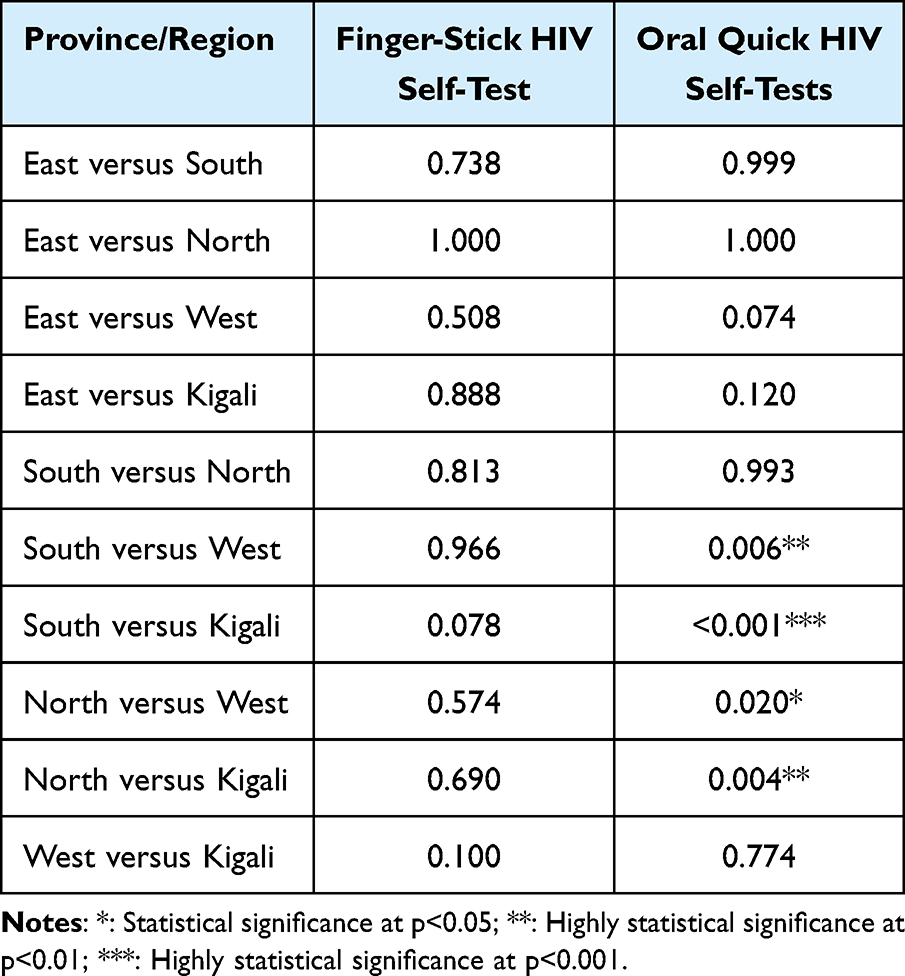 |
Table 7 Results of Post Hoc Test |
Factors Associated with the Availability of HIV Self-Tests
Table 8 shows the results of the bivariate logistic regression and multivariate logistic regression model analyses for the factors associated with the availability of HIVST. In bivariate logistic regression analyses, we found that pharmacy ownership, request for HIVST, training using HIVST, and location for the pharmacies were significantly associated with the availability of HIVST. In multiple logistic regression models, our results indicated that HIVSTs were more likely to be available in pharmacies where pharmacists were also the owners (AOR=1.858, 95% CI: 1.280–2.629, p=0.007) than their counterparts. Pharmacies with frequent requests for HIVSTs from clients were more likely to have HIVST available (AOR=0.22; 95%: 0.07–0.66, p<0.001) than those who did not report any request. Pharmacies located in Kigali City had higher odds of HIVST availability than those outside the city (OR=3.549, 95% CI; 1.289–9.814; p=0.015).
 |
Table 8 Bivariate and Multivariate Logistic Regression Analyses for the Factors Associated with the Availability of HIV Self-Tests |
Discussions
This study assessed the availability and affordability of HIVST in community pharmacies. Our results revealed that the prevalence of stocking HIVSTs was high (76%), with the majority (53%) being Finger-stick HIV self-testing. Although direct comparisons with wealthier nations such as Netherlands and New York City9,44 where similar studies have been conducted, are challenging due to Rwanda’s low-income status, this study underscores Rwanda’s improved availability of HIVST. This is particularly significant, given the lack of comparable studies in similar low-resource settings. Scholars have noted that the lack of availability often deters individuals from getting tested.12 The improved availability in the current study may be attributed to a policy that approved the over-the-counter sale of Oral Quick HIV self-tests in community pharmacies in 2018.33 This strategy increases HIV status awareness, overcoming barriers such as stigma and accessibility issues such as waiting times for HIV testing at public health facilities.45 Given the proximity of community pharmacies to the public, this highlights the significant progress that has been made in Rwanda. Furthermore, this study found a significant correlation between pharmacy location and the availability of HIVSTs, agreeing with findings from other regions, such as the Netherlands where a correlation between pharmacy location, and the availability of HIV self-tests was reported.9 This suggests that HIVST accessibility is not consistent across urban and rural areas. This may be attributed to the nature of healthcare infrastructure and policies. Although the country has made efforts to decentralize healthcare services to ensure that even rural areas have access to essential health commodities, challenges remain. This is unfortunate, especially for people living in rural areas, which comprise 72.1% of Rwandans.46 Thus, expanding HIV testing availability in Rwanda is still crucial for achieving the WHO 2030 hIV elimination objectives.
The factors that contributed to HIVSTs’ non-availability included regulatory ambiguity, concerns regarding reliability, and non-availability at wholesalers. Similarly, reliability concerns in the Netherlands have been a reason for the non-availability of HIVST.9 These findings can be attributed to various reasons. First, the regulatory framework surrounding medical devices, such as HIV self-tests, may be unclear or evolving, leading to delays or hesitations in approvals and market entry. Additionally, concerns about the accuracy and reliability of HIV self-tests may deter regulatory agencies from approving them for sale or discourage healthcare providers from stocking them. Issues related to test performance, false positives or negatives, and user errors can undermine confidence in these products, limiting their availability in the market. In addition, the limited availability of HIVST kits at wholesalers can be influenced by various factors, including supply chain inefficiencies, distribution challenges, and market demands. In regions where wholesalers are not adequately stocked with HIVSTs or face logistical barriers in their distribution to retailers, the overall availability of these tests can be affected. Moreover, as in a previous study, Rwandan community pharmacists showed that regulatory ambiguity hinders their involvement in health promotion.47 This means that community pharmacists need education on pharmacy regulatory policies to ensure compliance with and adherence to regulations governing their profession.
Although Rwanda approved over-the-counter sale of Oral Quick HIV self-tests in community pharmacies,32 its price remains high for the lowest-paid Rwandans. HIVST costs are unaffordable, with an average cost of 2.5$, equivalent to three days’ wage for the lowest-paid unskilled employee, while WHO/HAI suggests that a treatment course requiring more than one day’s wage is unaffordable.43 However, compared to a systematic literature review in SSA that reported the mean cost estimate of HIVST at 12.5$, the current study demonstrates a significantly lower cost of HIVST.48 The study also revealed price variations across the regions, with community pharmacists stating that clients often complain about high prices. Kigali, the capital city, displayed higher prices compared to the Southern and Western Provinces. These findings align with broader economic patterns often observed in capital cities, where higher living costs, increased demand, and greater operational expenses, such as rent and wages, contribute to elevated pricing. To justify this, Kigali, as an urban and economic hub, experiences heightened demand for healthcare products, potentially driving prices upward due to market forces. Additionally, pharmacies in Kigali may cater to a demographic with greater purchasing power, which could allow for higher markups. In contrast, rural and less urbanized areas such as the Southern and Western Provinces often have lower average incomes, which may constrain the pricing strategies of pharmacies. However, despite the lower prices in these provinces, affordability remains a critical concern, particularly for low-income earners, as the cost of finger-stick HIVST kits exceeds the daily wage of many individuals earning 1000 RWF per day. This finding underscores a significant barrier to access, particularly in rural areas where poverty levels are higher and individuals may have limited financial capacity to prioritize health-related expenditures. These finding is like a study in Tanzania which also found price variations between pharmacies.49 The price discrepancies can be attributed to several factors. First, logistical challenges and transportation costs may contribute to higher prices in remote or rural areas, where infrastructure is less developed. Limited competition among suppliers in these regions can also lead to higher prices because of reduced market pressure. Additionally, variations in purchasing power and economic conditions among different regions may influence pricing strategies, with suppliers adjusting prices according to the local demand and affordability levels. Furthermore, factors such as taxes, import duties, and distribution fees can differ across regions, affecting the final retail price of HIV self-tests. Like any other health commodity, the cost of HIVST is an important factor to consider when choosing an HIVST.6,17 To make HIVST more affordable, measures such as reduced profit markups or partners providing HIVST through social marketing at a lower cost to clients can be implemented. Alternatively, in a previous study, community pharmacists stated that for some self-tests, it would be preferable if the government and partners provided these tests to community pharmacies at no cost so that patients would only have to pay for testing.47 Although HIV testing is free in public health facilities, it did not prevent clients from seeking HIVST in community pharmacies, where 93% of community pharmacists reported being asked about HIVST by their clients.
Strengths and Limitations of the Study
This study has several strengths. First, it was the first to investigate the availability and affordability of HIV Self-Test Kits in Community Pharmacies in Rwanda, shedding light on an important aspect of healthcare access. Second, this study had a large sample size and was conducted comprehensively, allowing the authors to generalize their findings. Moreover, the use of validated data-collection instruments ensured the accuracy of the results. Third, the selection of community pharmacies across all provinces made the findings generalizable to all pharmacy users in the country. Fourth, the results of this study offer important insights that can improve adherence to these rapid tests by improving universal access to HIV prevention, care, support services, and treatment. Finally, the study’s findings could significantly contribute to the achievement of the 2030 Sustainable Development Goals (SDGs) by ending the HIV epidemic as a public health threat.
However, there are certain limitations that warrant further discussion. First, there is a lack of literature on community pharmacists in Rwanda, and direct interviews with clients seeking HIVSTs to understand their economic pricing are absent. Additionally, the use of a cross-sectional design limits the ability to establish causality. Furthermore, not all factors were included in the analyses, potentially leading to overestimation or underestimation of results. Incorporating qualitative methods to explore the sociocultural context could have complemented the quantitative analysis. Moreover, a high rate of participant dropouts (16.8%) was observed, which could have influenced the study’s outcomes. We also recognize that the hypothetical nature of the questions regarding HIVSTs may not accurately predict future behavior. In addition, our affordability analysis did not account for benchmarks such as median household income and urban-rural disparities due to the unavailability of such data. Moreover, our study did not investigate the additional drivers of regional price variations, such as purchasing power and competition among pharmacies, beyond logistical challenges. Lastly, the minimum wage used for the lowest-paid unskilled worker in Rwanda may be out-dated and less practical, as it fails to account for current inflation rates and rising living costs, thereby inadequately reflecting present economic realities.
Future Directions
Based on our results, we recommend that future researchers explore the impacts of different pricing models on access to HIVST not only in Rwanda but also across other SSA countries, where affordability continues to be a significant barrier to widespread HIVST and early diagnosis. Scientific evidence on this topic would help inform strategies to improve affordability and access in LMICs. Additionally, it is important to explore the role of stigma in the uptake of HIVST through qualitative methods to understand its impact on individuals’ willingness to access testing. Additionally, studies should examine how stigma intersects with other barriers, such as affordability and availability, to inform more effective public health interventions that address both social and logistical challenges in HIV testing. As our study did not perform benchmarks such as median household income and urban-rural disparities, future research should incorporate these variables to provide a more detailed understanding of affordability challenges. Indeed, future scholars are suggested to consider the drivers of regional prices variations to better understand the dynamics influencing pricing disparities. Lastly, longitudinal studies could track changes in stigma over time and its evolving influence on HIV testing behaviors in different communities.
Conclusion
HIV self-tests are widely available across community pharmacies. This study revealed that HIV self-tests are more available in pharmacies owned by pharmacists, those with frequent client requests, and those located in the capital city. Furthermore, the price varies significantly across the regions, with the capital city showing a difference compared to other regions. Despite improved availability, HIVST kits remain unaffordable to the lowest earners which causes unequal access to these services. To make these tests more affordable, measures such as reduced profit markups or partners providing HIVST through social marketing at a lower cost to the client can be implemented. Implementing strategies like reducing profit markups through social marketing can make HIVST more affordable. Policymakers should consider subsidizing HIVST or providing them for free to low-income populations, as part of a broader strategy to increase testing rates and reduce the spread of HIV. Likewise, partnerships with non-governmental organizations (NGOs) and public health initiatives could help distribute subsidized or free kits in underserved regions to mitigate the financial burden on vulnerable populations. Moreover, constant monitoring of HIVST distribution, pricing, and utilization patterns is necessary to assess the effectiveness of implemented measures. Evaluating these metrics can help in making data-driven adjustments to policies and strategies, ensuring that HIVST becomes a viable option for all Rwandans. In addition, public health campaigns are also essential to empower the population about the availability and importance of HIV self-testing. Such campaigns can also address stigma and encourage more individuals to utilize HIVST, thereby increasing testing rates and early detection. The Rwanda FDA can collaborate with the Ministry of Health to organize gatherings of community pharmacists, who currently employ most of Rwanda’s pharmacists, to share regulatory policy information and provide a platform for pharmacists to reduce the number of people who are still unaware of their HIV status.
Data Sharing Statement
All relevant data are included in this manuscript. Data may be shared upon reasonable request to the corresponding author.
Ethics Approval and Consent to Participate
The Institutional Review Board (IRB) of the College of Medicine and Health Sciences, University of Rwanda approved this study (Ref: CMHS/IRB/144/2023). All participants received a consent form outlining the study details. Those who provided valid written informed consent were then given access to the research survey. The protection of confidentiality was also safeguarded. Furthermore, participation in the study was entirely voluntary, and participants did not receive any compensation for their involvement in this research. Special precautions were taken to protect the identities of the respondents. On the consent form, the participants agreed that their identities would remain anonymous when reports or articles about the study were published. This commitment to anonymity has been instrumental in maintaining privacy and confidentiality between the researchers and participants.
Acknowledgments
The authors gratefully acknowledge community Pharmacists who consented to participate.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Authors of the current study assert that they received no financial support for the research, authorship and/or publication of this study.
Disclosure
The authors declare no conflicts of interests.
References
1. World Health Organization (WHO). HIV and AIDS.; 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/hiv-aids.
2. UNAIDS. Global HIV & AIDS statistics — fact sheet; 2023. Available from: https://www.unaids.org/en/resources/fact-sheet.
3. UNAIDS. THE PATH THAT ENDS AIDS 2023 UNAIDS GLOBAL AIDS UPDATE.; 2022. The joint united nations programme on HIV/AIDS (UNAIDS). Available from: https://www.unaids.org/en/resources/documents/2023/global-aids-update-2023.
4. World Health Organization (WHO). HIV statistics, globally and by WHO region, 2023.; 2022. Available from: https://cdn.who.int/media/docs/default-source/hq-hiv-hepatitis-and-stis-library/j0294-who-hiv-epi-factsheet-v7.pdf.
5. World Health Organization (WHO). WHO recommends HIV self-testing – evidence update and considerations for success; 2019. Available from: https://www.paho.org/en/documents/who-recommends-hiv-self-testing-evidence-update-and-considerations-success.
6. Calderon Y, Cowan E, Rhee JY, Brusalis C, Leider J. Counselor-based rapid HIV testing in community pharmacies. AIDS Patient Care STDS. 2013;27(8):467–473. doi:10.1089/apc.2013.0076
7. World Health Organizaton. Guidelines on HIV self-testing and partner notification: supplement to consolidated guidelines on HIV testing services; 2016. Available from: https://iris.who.int/bitstream/handle/10665/251655/9789241549868-eng.pdf.
8. Figueroa C, Johnson C, Ford N, et al. Reliability of HIV rapid diagnostic tests for self-testing compared with testing by health-care workers: a systematic review and meta-analysis. Lancet HIV. 2018;5(6):e277–e290. doi:10.1016/S2352-3018(18)30044-4
9. Kandil C, Hugtenburg J, Heijman T, et al. Availability and accessibility of HIV self-tests and self-sample kits at community pharmacies in the Netherlands. AIDS Res Ther. 2023;20(1). doi:10.1186/s12981-023-00529-9
10. Myers JE, El-Sadr WM, Zerbe A, Branson BM. Rapid HIV self-testing: long in coming but opportunities beckon. AIDS. 2013;27(11):1687–1695. doi:10.1097/QAD.0b013e32835fd7a0
11. Hamilton A, Thompson N, Choko AT, et al. HIV self-testing uptake and intervention strategies among men in sub-Saharan Africa: a systematic review. Front Public Health. 2021;9. doi:10.3389/fpubh.2021.594298
12. Mugo PM, Micheni M, Shangala J, et al. Uptake and acceptability of oral HIV self-testing among community pharmacy clients in Kenya: a feasibility study. PLoS One. 2017;12(1):e0170868. doi:10.1371/journal.pone.0170868
13. Kuo AP, Roche SD, Mugambi ML, et al. The effectiveness, feasibility and acceptability of HIV service delivery at private pharmacies in sub-Saharan Africa: a scoping review. J Int AIDS Soc. 2022;2022(10):26027. doi:10.1002/jia2.26027/full
14. Weidle CPJ, Lecher CS, Botts LW, et al. HIV testing in community pharmacies and retail clinics: a model to expand access to screening for HIV infection. J Am Pharm Assoc. 2003;54(5):486–492. doi:10.1331/JAPhA.2014.14045
15. HIV testing in retail pharmacies | diagnose | effective interventions | HIV/AIDS | CDC.
16. Lee VJ, Choon Tan S, Earnest A, Suet Seong P, Hee Tan H, Sin Leo Y. User acceptability and feasibility of self-testing with HIV rapid tests. JAIDS Journal of Acquired Immune Deficiency Syndromes. 2007;45(4):449–453. doi:10.1097/QAI.0b013e318095a3f3
17. Wong V, Johnson C, Cowan E, et al. HIV self-testing in resource-limited settings: regulatory and policy considerations. AIDS Behav. 2014;18(SUPPL. 4):415–421. doi:10.1007/s10461-014-0825-9
18. Mavedzenge SN, Baggaley R, Corbett EL. A review of self-testing for HIV: research and policy priorities in a new era of HIV prevention. Clinl Infect Dis. 2013;57(1):126–138. doi:10.1093/cid/cit156
19. Unitaid, World Health Organization. Market and Technology Landscape:HIV Rapid Diagnostic Tests for Self-Testing.
20. Empringham B, Karellis A, Kashkary A, et al. How much does HIV self-testing cost in low and middle income countries? A systematic review of evidence from economic studies. Front Public Health. 2023;11. doi:10.3389/fpubh.2023.1135425
21. Maheswaran H, Petrou S, MacPherson P, et al. Cost and quality of life analysis of HIV self-testing and facility-based HIV testing and counselling in Blantyre, Malawi. BMC Med. 2016;14(1):1–12. doi:10.1186/s12916-016-0577-7
22. Njau B, Covin C, Lisasi E, et al. A systematic review of qualitative evidence on factors enabling and deterring uptake of HIV self-testing in Africa. BMC Public Health. 2019;19(1):1–16. doi:10.1186/s12889-019-7685-1
23. Niëns LM, Brouwer WBF. Measuring the affordability of medicines: importance and challenges. Health Policy. 2013;112(1–2):45–52. doi:10.1016/j.healthpol.2013.05.018
24. Yenet A, Nibret G, Tegegne BA. Challenges to the availability and affordability of essential medicines in African countries: a scoping review. Clinicoecon Outcomes Res. 2023;15:443–458. doi:10.2147/CEOR.S413546
25. Sande L, Matsimela K, Mwenge L, et al. Costs of integrating HIV self-testing in public health facilities in Malawi, South Africa, Zambia and Zimbabwe. BMJ Glob Health. 2021;6(Suppl 4):e005191. doi:10.1136/bmjgh-2021-005191
26. Harichund C, Moshabela M. Acceptability of HIV Self-testing in sub-Saharan Africa: scoping study. AIDS Behav. 2018;22(2):560–568. doi:10.1007/s10461-017-1848-9
27. Cambiano V, Johnson CC, Hatzold K, et al. The impact and cost-effectiveness of community-based HIV self-testing in sub-Saharan Africa: a health economic and modelling analysis. J Int AIDS Soc. 2019;22(S1):82–93. doi:10.1002/jia2.25243
28. Matsimela K, Sande LA, Mostert C, et al. The cost and intermediary cost-effectiveness of oral HIV self-test kit distribution across 11 distribution models in South Africa. BMJ Glob Health. 2021;6(Suppl 4):1–10. doi:10.1136/bmjgh-2021-005019
29. Rwanda Ministry of Health. Rwanda ministry of health HIV annual report 2022 −2023.; 2023. Available from: https://rbc.gov.rw/fileadmin/user_upload/report23/HIVAnnualreport2022-2023.pdf.
30. Rwanda Biomedical Centre (RBC). Rwanda national HIV annual report. 2015.; 2015. Available from: https://rbc.gov.rw/fileadmin/user_upload/report2019/report2019/AnnualReportforHIV2015-2016.pdf.
31. Rwanda Ministry of Health. Republic of Rwanda ministry of health national guidelines for prevention and management of HIV, STIs & other blood borne infections edition 2013. 2013. Available from: https://rbc.gov.rw/fileadmin/user_upload/guide/FINALGUIDELINES_2013.pdf.
32. World Health Organization. HIV self-testing strategic framework: a guide for planning, introducing and scaling up.; 2018. Available from: https://www.who.int/publications/i/item/9789241514859.
33. Rwanda Biomedical Center. National Guidelines for Prevention and Management of HIV and STIs Edition 2016.; 2016. Available from: https://rbc.gov.rw/fileadmin/user_upload/guide/SIGNEDENGLISH2016VERSION.pdf.
34. World Population Review. Median income by country 2024; 2024. Available from: https://worldpopulationreview.com/country-rankings/median-income-by-country.
35. World Minimum Wage Rates. 2023 - Minimum-Wage.org. Available from: https://www.minimum-wage.org/international.
36. Bizimana T, Kayumba PC, Heide L. Prices, availability and affordability of medicines in Rwanda. PLoS One. 2020;15(8):e0236411. doi:10.1371/journal.pone.0236411
37. Rurangwa C, Ndayisenga J, Sezirahiga J, Nyirimigabo E. Availability and affordability of anticancer medicines at cancer treating hospitals in Rwanda. BMC Health Serv Res. 2023;23(1). doi:10.1186/s12913-023-09706-y
38. World Bank, New world bank country classifications by income level: 2022-2023. Available from: https://blogs.worldbank.org/opendata/new-world-bank-country-classifications-income-level-2022-2023.
39. National Institute of Statistics of Rwanda(NISR). 5th population and housing census 2022. Available from: https://statistics.gov.rw/publication/main_indicators_2022.
40. National Pharmacy Council. Guidelines for grading pharmacy professionals in Rwanda. 2022. Available from: https://www.pharmacycouncil.rw/wp-content/uploads/2017/02/Grading-guidelines.pdf.
41. Rwanda Ministry of Health. Ministry of Health. National Pharmacy Policy.; 2016. Available from www.moh.gov.rw/fileadmin/templates/policies/Pharmacy-Policy_Rwanda-2016.pdf.
42. Naing N. Determination of sample size. Malaysian J Med Sci. 2003;10(2):84–86.
43. World Health Organization (WHO). Measuring medicine prices, availability, affordability and price components. 2nd edition. World Health Organization Available from: https://www.who.int/publications/i/item/WHO-PSM-PAR-2008.3.
44. Myers JE, El-Sadr Davis OY, Weinstein ER, et al. Availability, accessibility, and price of rapid HIV self-tests, New York City pharmacies, summer 2013. AIDS Behav. 2017;21(2):515–524. doi:10.1007/S10461-016-1594-4/METRICS
45. Crawford ND, Myers S, Young H, Klepser D, Tung E. The role of pharmacies in the HIV prevention and care continuums: a systematic review. AIDS and Behavior. 2021;25(6):1819–1828. doi:10.1007/s10461-020-03111-w
46. National Institute of Statistic of Rwanda (NISR). RPHC5 thematic report:population size, structure and distribution.; 2022. Available from: https://statistics.gov.rw/publication/1975.
47. Nsengimana A, Isimbi J, Uwizeyimana T, et al. Malaria rapid diagnostic tests in community pharmacies in Rwanda: availability, knowledge of community pharmacists, advantages, and disadvantages of licensing their use. Glob Health Res Policy. 2023;8(1). doi:10.1186/s41256-023-00324-z
48. Ahmed N, Ong JJ, McGee K, et al. Costs of HIV testing services in sub-Saharan Africa: a systematic literature review. BMC Infect Dis. 2022;22(Suppl 1):1–20. doi:10.1186/s12879-024-09770-7
49. Chiu C, Hunter LA, McCoy SI, Mfaume R, Njau P, Liu JX. Sales and pricing decisions for HIV self-test kits among local drug shops in Tanzania: a prospective cohort study. BMC Health Serv Res. 2021;21(1). doi:10.1186/s12913-021-06432-1
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Challenges to the Availability and Affordability of Essential Medicines in African Countries: A Scoping Review
Yenet A, Nibret G, Tegegne BA
ClinicoEconomics and Outcomes Research 2023, 15:443-458
Published Date: 13 June 2023