Back to Journals » ClinicoEconomics and Outcomes Research » Volume 16
Expanding Access to Patient Care in Community Pharmacies for Minor Illnesses in Washington State
Authors Akers JM ![]() , Miller JC, Seignemartin B, MacLean LG, Mandal B, Kogan C
, Miller JC, Seignemartin B, MacLean LG, Mandal B, Kogan C
Received 19 December 2023
Accepted for publication 15 April 2024
Published 3 May 2024 Volume 2024:16 Pages 233—246
DOI https://doi.org/10.2147/CEOR.S452743
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Samer Hamidi
Julie Marie Akers,1,* Jennifer C Miller,1,* Brandy Seignemartin,2,* Linda Garrelts MacLean,1,* Bidisha Mandal,3,* Clark Kogan4,*
1College of Pharmacy and Pharmaceutical Sciences, Washington State University, Spokane, WA, USA; 2College of Pharmacy, Idaho State University Anchorage Campus, Anchorage, AK, USA; 3School of Economic Sciences, Washington State University, Pullman, WA, USA; 4Department of Mathematics, Washington State University, Pullman, WA, USA
*These authors contributed equally to this work
Correspondence: Julie Marie Akers, Washington State University, College of Pharmacy and Pharmaceutical Sciences, 412 E Spokane Falls Blvd, Spokane, WA, 99202-2131, USA, Tel +1 425 985 2277, Email [email protected]
Introduction: As the shortage of primary care providers widens nationwide, access to care utilizing non-physician providers is one strategy to ensure equitable access to care. This study aimed to compare community pharmacist-provided care for minor ailments to care provided at three traditional sites of care: primary care, urgent care, and emergency department, to determine if care provided by pharmacists improved access with comparable quality and reduced financial strain on the healthcare system.
Methods: Pharmacy data was provided from 46 pharmacies and 175 pharmacists who participated across five pharmacy corporations over a 3-year period (2016– 2019). Data for non-pharmacy sites of care was provided by a large health plan, matching episodes of care for conditions seen in the community pharmacy. Cost-of-care analysis was conducted using superiority study design and revisit data analysis was conducted using noninferiority study design.
Results: Median cost-of-care across traditional sites of care was $277.78 higher than care provided at the pharmacies, showing superiority. Noninferiority was demonstrated for revisit care when the initial visit was conducted by a pharmacist compared to traditional sites.
Discussion: The authors conclude community pharmacist-provided care for minor ailments improved cost-effective access for patients with comparable quality and reduced financial strains on the healthcare system.
Keywords: patient access, community pharmacy, minor ailments, cost of care
Introduction
As the need for healthcare in the United States grows beyond capacity, it is imperative we find new healthcare delivery models to ensure equitable access to efficient healthcare options. We are currently facing a scarcity of healthcare providers, and in 2012 it was projected that by the year 2025 we will face a shortage of primary care physicians (PCP), reaching up to 52,000.1 Despite the roles of nurse practitioners and physician assistants expanding, it is estimated nearly 1 million office visits per year needed by patients will go unmet due to lack of provider availability.1 Patients living in low-income neighborhoods with less access to retail clinics or urgent care centers, who are facing long wait times for primary care (PC) appointments, or who work during hours when PC office hours exist often end up in the emergency department (ED) for medical treatment.2 For reference, in the United States a PCP visit is an outpatient visit with a provider for services, such as chronic medical conditions, annual wellness visits, and same-day appointments for urgent needs that are manageable by a general provider in an outpatient setting during normal daytime business hours. Urgent Care visits are open extended hours (evenings and weekends) and are the site of care for conditions that cannot wait until a PCP visit can be scheduled or that may need services more advanced than provided by a PCP, such as X-ray or casting broken bones but are not considered life threatening. An ED visit is for emergency care needs that may be life threatening, require emergency surgery, or require advanced imaging for conditions such as stroke or heart attack. According to the National Association of Community Health Centers, Inc., more than one-third of all ED visits are avoidable and could be treated in an ambulatory setting with a savings of more than $18 billion dollars annually.3 ED treatment of urinary tract infections (UTIs) alone accounts for approximately $4 billion per year in healthcare costs.4
It has been suggested that diversification of roles within the healthcare delivery system, along with workforce development efforts, can be capitalized upon to increase population health in a more efficient way.5,6 Activities such as motivational interviewing and helping patients set goals for lifestyle modifications have been shown to greatly increase population health.5 In addition, non-physician healthcare professionals can help fill the demand-capacity gap by utilizing technology and standing orders to provide patient care.6
Throughout the years, pharmacists’ roles have evolved from solely medication dispensing functions to providing medication therapy management and other healthcare services designed to improve patient outcomes. Pharmacists have been integrated into health system care teams to help improve patient outcomes and forge innovative health delivery models through interprofessional collaborations in the community setting.7 Key elements of pharmacy education prepare pharmacists to be medication experts, solve therapeutic problems, provide patient-centered care, advance population health, collaborate interprofessionally, and advocate for patients at the highest level.8 The potential for pharmacists’ clinical expertise to improve patient outcomes has been well studied in a range of scenarios, from examination of pharmacist-recommended clinical interventions implemented by a provider to direct pharmacist-provided care in managing acute and chronic disease states.7
In Rear Admiral Scott Giberson’s Report to the US Surgeon General in 2011 titled “Improving Patient and Health System Outcomes through Advanced Pharmacy Practice”, he outlines 55 peer-reviewed articles showing improved clinical outcomes for patients when pharmacists were involved in patient care delivery.7 One systematic review of 12 randomized controlled trials including 2,060 patients showed pharmacist-directed or pharmacist-collaborative care was correlated with a significant decrease in all-cause hospitalizations (11 studies, 2026 patients) and heart failure hospitalizations (11 studies, 1977 patients).9
In the community pharmacy setting, both in the US and around the world, pharmacists have utilized Collaborative Practice Agreements (CPAs) and other prescriptive authority avenues to provide patients with access to affordable and expeditious screenings, treatment initiation, and medication management for many minor or acute ailments and chronic health conditions. Approximately 90% of all Americans live within 5 miles of a community pharmacy, with those residing in metropolitan areas living less than 2 miles from a pharmacy.10 Proximity, walk-in patient access and extended hours make pharmacists the most accessible healthcare professionals in many geographic areas.
Point of Care (POC) testing and the ability for pharmacies to obtain a Clinical Laboratory Improvement Amendment (CLIA) Certificate of Waiver opened the door for pharmacists to enhance patient care access by providing screenings and prompt treatment initiation within the same pharmacy visit. Various CLIA-waived tests utilized in the outpatient and community pharmacy settings include those for Group A Streptococcus, influenza, Hepatitis C, HIV, hemoglobin A1c, cholesterol, and Helicobacter Pylori.11,12 As of 2020, more than 15,600, or approximately 28% of US pharmacies, held CLIA-waiver certificates.13
Not all conditions appropriate for pharmacist-initiated treatment require testing. There are a number of minor ailments that can be effectively treated in a community pharmacy setting based on patient reported symptoms and examination. Uncomplicated UTIs are among these minor ailments. Since 2010, pharmacists around the world have provided patient care related to uncomplicated UTIs, with positive perceptions reported by patients and pharmacists.14 Infectious disease guidelines do not require urine testing for uncomplicated UTI treatment, though pharmacists might consider criteria for referral prior to treatment initiation, such as patients who report flank pain, fever, chills, pregnancy, and others.15 Treatment guidelines provide a framework for assessment and treatment with antimicrobial therapy or referral for complications when appropriate.12 Many patients have reported seeking care at a pharmacy sooner than they would have with a general practitioner due to increased patient access to a community pharmacy.12 Pharmacists have demonstrated improved antimicrobial stewardship for UTIs in ED and long-term care settings. Additionally, pharmacists are engaged in work to improve outpatient stewardship programs, which is promising for the future of antimicrobial stewardship of pharmacist-initiated interventions in the outpatient setting.16–19
Although some conditions appropriate in a community pharmacy setting do not require the use of CLIA-waived POC tests, like uncomplicated UTIs, others can utilize POC technology to assist in determining if and when medication therapy should be initiated. A literature review found positive evidence demonstrating pharmacist involvement in POC testing and, when appropriate, initiation of therapy to be successful in improving patient access to safe and effective care for influenza, Group A Streptococcus, Helicobacter pylori (H. pylori), Hepatitis C, and human immunodeficiency viruses (HIV).20
As new patient-centered care delivery models are implemented in the community pharmacy setting, we should seek to ensure these care models meet patient needs and are sustainable. Correspondingly, the goals of this study were to conduct a cost-of-care and quality-of-care analysis by comparing pharmacist-provided care for selected conditions to care provided at three traditional sites of care: PCP, urgent care, and ED. The cost-of-care analysis includes median and mean costs from all sites of care for initial care and any revisit care needed for the same episode-of-care. The quality analysis compared patient revisit data as a measure to ascertain if the care provided by community pharmacists reduced the access burden on the traditional healthcare system. In addition, data was collected on the feasibility of offering services in a community pharmacy setting, which included training, supplies needed, space requirements, documentation, workflow, and compliance with prescriptive authority regulations. Data for traditional sites were collected from a large health plan in Washington state and compared to data collected from participating community pharmacies in Washington state over a 3-year period. Community pharmacies utilized in the study include drugstores, groceries, multidepartments, and big boxes. Washington state was selected for the study due to pharmacist delegated prescriptive authority through collaborative drug therapy agreements having been in place since 1979, with no limitation on patient eligibility, disease state, or medication prescribed. Many pharmacists included in the study were experienced in providing patient care services such as for immunizations and POC testing. In addition, pharmacists in Washington state are recognized as medical providers with billing authority, although at the time of this study the authority was new and not implemented in any of the study pharmacy locations.
Materials and Methods
Community Pharmacy Patient Visit Data
Data collected during monthly pharmacy site visits were used for pharmacy sites of care. Individuals under age 18 were excluded from the study. Cost per condition were set within each pharmacy company, of which it became the out-of-pocket cost for a patient to receive the service at that location. Participating study pharmacies did not bill patient insurance. The research team had no influence or decision-making authority as to the price each pharmacy organization set as their price for patient care services. Pharmacy mean and median cost per condition were both calculated; however, mean was utilized in the analysis due to cost data distribution having little variability.
Revisit data from pharmacy claims was collected through 30-day follow-up telephonic calls conducted by researchers. Data were reliant on patient-reported information, which could impact the accuracy of the data. Patient-reported data collected regarding revisits included when the revisit occurred, site of care for the revisit, and if symptoms resolved after the revisit. Utilizing the patient-reported site of care for a revisit, median cost from the traditional site of care data was utilized, in addition to the original pharmacy cost, to complete the total cost of care for those patient encounters. Difference in proportion of revisits between traditional sites of care and pharmacies was compared as a measure of quality with a noninferiority test using an equivalence margin of 20%.21 Confidence intervals on the difference in the proportion of revisits were established with Wilson intervals.22 Noninferiority testing was performed using a 1–2α confidence interval with an α level of 0.05.23
Traditional Sites of Care Patient Visit Data
Health plan episodes claim lines data were used to obtain cost and visit data for traditional sites of care. Primary diagnosis codes were categorized into the conditions considered in this study. Claims for individuals under age 18 were removed from consideration. For cost comparison, only the cost of anchor claims and computed total cost by episode, condition, and provider site of care were considered. An anchor claim was categorized as being the first claim for the condition for that patient in a previous 30-day window of time. Episode costs included that of the anchor claim and any revisit claims within 30-days post-anchor claim organized by the condition and traditional provider site of care. Cost distributions were right-skewed, and thus median costs were used in place of mean costs to reflect cost expectations for a typical episode. Bootstrapping was employed to construct 95% confidence intervals on the median cost. Differences between the median episode cost from each traditional site of care setting and the fixed pharmacy cost along with 95% bootstrap confidence intervals were computed by subtracting a fixed pharmacy cost.
Data for traditional sites of care claims were available only up to monthly resolution, limiting the accuracy to which revisits could be identified. We defined a member revisit as a subsequent episode, as determined through increasing episode number that met the condition of having a claim date either in the same month or 1 month later. We summarized the follow-up visits by constructing a table of episode counts as well as computing the proportion of episodes that were follow-ups by traditional site of care and condition.
The cost-of-care analysis was conducted using superiority study design, comparing community pharmacies to traditional sites of care. The revisit data analysis was conducted using noninferiority study design, comparing the pharmacy setting to traditional sites of care.
There were several steps undertaken in the design of the project, in addition to data analysis methods. These included training programs in partnership with the Washington State Pharmacy Association (WSPA), entering into agreements with community pharmacy organizations to participate in the research project, and to develop a Physician Advisory Committee (PAC) to ensure standards of care are met and to incorporate the PACs feedback into live training sessions.
The WSPA has an online refresher training certificate program titled “Clinical Community Pharmacist”, which was made accessible to pharmacists participating in this study. The certificate program focuses on ailments and conditions often seen in a community pharmacy setting. This includes both continuation of care for previously diagnosed conditions, as well as the assessment and initiation of treatment for certain ailments. Conditions included in the research project can be found in Supplemental Box 1.
The research team approached several community pharmacy leaders to recruit sites for participation in the study. A mix of community pharmacies was desired as well as representation from varied regions in Washington state. Five large pharmacy organizations participated in the study with pharmacies located in southwest Washington, the Seattle/Puget Sound area, and the Spokane/Eastern Washington area. Pharmacies included two grocery chains, one drugstore chain, one multidepartment chain, and one warehouse club company. Overall, a total of 46 pharmacies participated and 175 pharmacists were trained.
Live training was created to facilitate participating pharmacists’ application of the online certificate modules through patient case discussions aimed at increasing confidence in the clinical decision-making process. The operational portion of the training included patient study consent and federally mandated health privacy forms, documentation requirements for data collection, and partner-specific operational components of implementing a new patient-care service. The clinical portion of the training was dedicated to patient case discussions related to each condition. Activities ranged in complexity and each activity emphasized the decision-making process to determine if a patient met criteria for pharmacist intervention or if referral to a different care provider was appropriate.
Pharmacists were required to complete the online training modules prior to attending the live session. Live training sessions conducted by the researchers were held either onsite at the pharmacy partner location in a large meeting room or on campus at the researcher’s university, depending on geographic location and space availability (grant funds supported training module costs, however, each pharmacy organization remained responsible for pharmacist wages). While there is no legal requirement in Washington state for pharmacists to receive additional training to provide these services, researchers required the training to participate in the study to minimize gaps in knowledge based on the length of time since completing pharmacy education and utilization of the knowledge and/or skill set in practice prior to the study.
Researchers shared best practices for documentation, record storage, and patient care workflow; however, implementation of patient care service was customized by each organization. Prescriptive authority Collaborative Drug Therapy Agreements (CDTAs) were the responsibility of each pharmacy organization, and the agreements were signed between each pharmacist and a delegating prescriber, as required in Washington state. Some variability in CDTAs exist, as the delegating prescriber customizes the agreement to meet their standard of care and referral criteria. Each pharmacy organization included policies and procedures to ensure a patient’s primary care provider, if they had one, was notified of the care provided by the pharmacist. Having CDTAs in place was a requirement for each organization to participate in the study as, without CDTAs, the pharmacists would not have the authority to prescribe treatment, when needed, based on their assessment of the patient and would have been required to refer all patients needing prescription treatment to a traditional site of care. Study recruitment began during the initial patient intake process at each pharmacy location. Consent into the study was not required for patients to receive care from the pharmacist, as determined by the IRB review.
Researchers visited pharmacies every 4 weeks over a period of 3 years to collect data, as documentation was in paper format. Data collected included patient demographics, insurance status, health history, and condition-specific information including treatments recommended and/or prescribed (Supplemental Exhibit 1). During each data collection visit, pharmacists were able to ask questions of the researchers to improve patient recruitment or patient care. For patients who consented to participate in the study, a 30-day follow-up phone call was conducted by researchers to assess the clinical outcome of the patient, either positively or negatively, and if additional care was sought (and where) for the condition (Supplemental Exhibit 2). Initial visit and 30-day follow-up data were stored utilizing REDCap electronic data tools hosted at the primary investigator’s university.24,25
This human subject research project was reviewed and approved by the primary investigator’s university Institutional Review Board (IRB) which complies with the Declaration of Helsinki.
Results
Data provided by 4 of the 5 pharmacy companies show 977 patients utilized the service during the 3-year study period ending December 2018, while 506 patients across all 5 pharmacy companies consented to participate in the study (one company chose not to provide aggregate service use data for patients not consented to the study). Of the 506 patients consenting to the study, 10 met referral criteria and were not treated by a pharmacist, resulting in 496 patients being included in comparison data. Patient demographics of pharmacies and traditional sites of care were collected for comparison (Supplemental Exhibit 3).
The total number of patients included from health plan data for comparison for all conditions was 84,555: with hormonal contraception, asthma, UTI, allergies, and headache being the top five (Table 1). For each of the ten conditions listed, cost-of-care was significantly lower when provided by a community pharmacist than in the comparator traditional sites of care. The median overall cost of care for all conditions across all traditional sites of care combined was $277.78 higher than care provided at the community pharmacies (Figure 1). The largest differences in cost of care between traditional sites and community pharmacy, in order of largest to smallest, are EDs, urgent care, and primary care providers at $505.04, $122.74, and $95.97 respectively (Figure 1). Further breakdown of the median cost of care difference by condition shows asthma, UTI, and yeast infection as the three conditions with the highest median difference of cost (Figure 1).
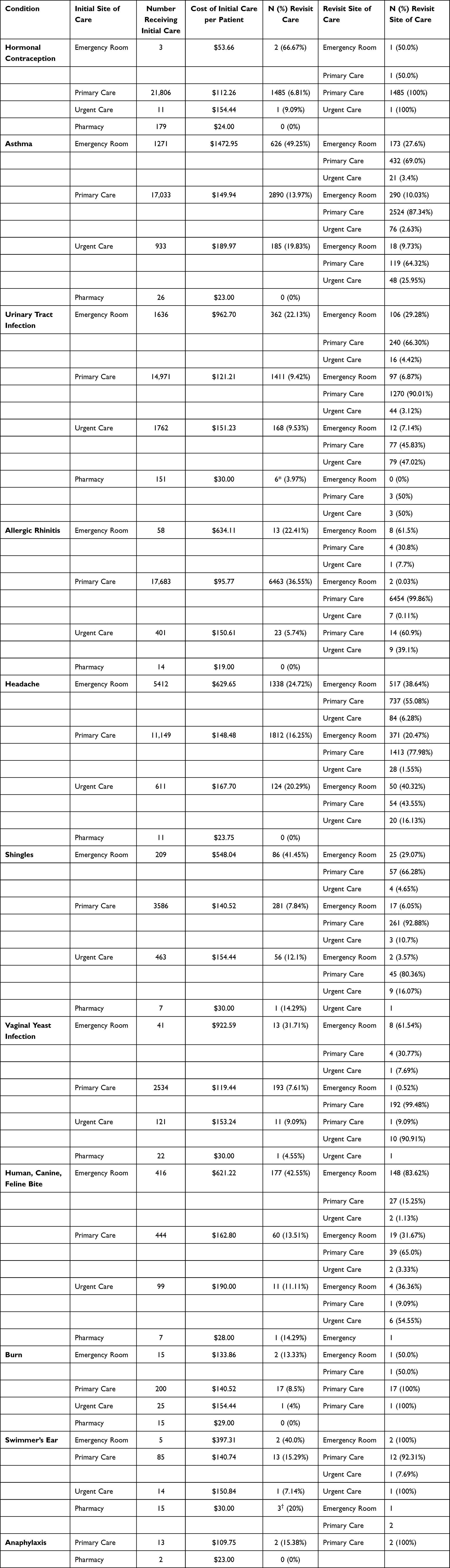 |
Table 1 Initial and Revisit Care by Condition, Initial Site of Care, and Revisit Site of Care |
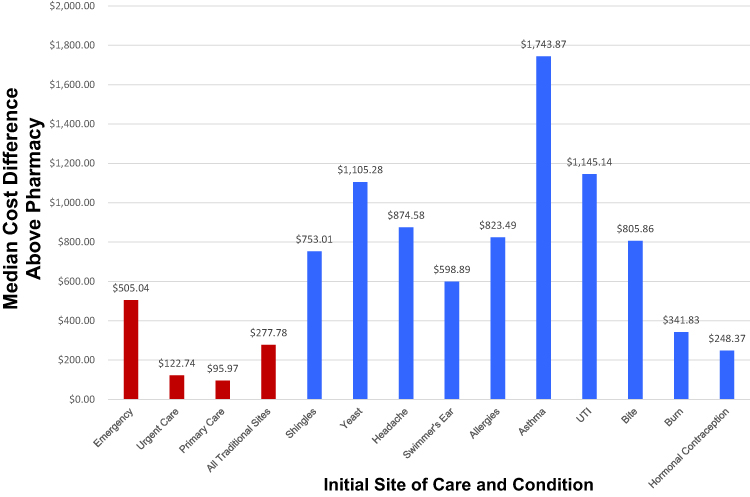 |
Figure 1 Traditional Site of Care Median Cost Difference Above Pharmacy by Initial Site of Care and Condition. |
Patient revisit data was collected to compare the number of patients with an initial visit at a community pharmacy needing to seek additional care to those seen initially at a traditional site of care. The number of patients needing a revisit by condition and the site of care for the revisit can be found in Table 1. The traditional site of care difference in proportion of revisits with 95% CI by condition can be found in Figure 2, which shows noninferiority was found comparing community pharmacy to ED, primary care, and urgent care using a 20% margin (lower CI above −0.2). Further breakdown by conditions within the traditional sites of care show noninferiority in all 11 conditions comparing pharmacy to ED and in 8 of 11 conditions compared to urgent care and primary care (Supplemental Exhibit 4). The total cost of care, including revisits by condition and initial site of care, can be found in Table 2.
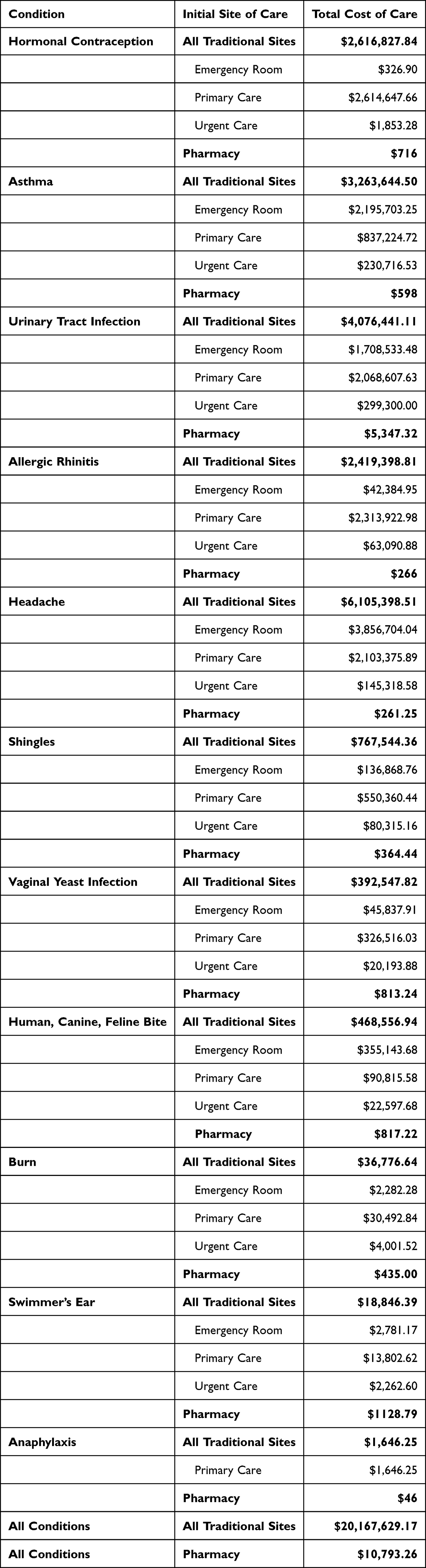 |
Table 2 Total Cost of Care (Initial and Revisit) by Condition and Initial Site of Care |
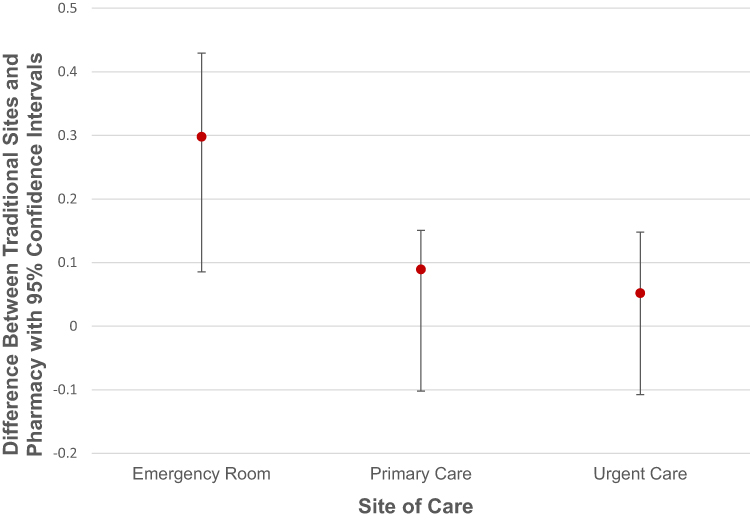 |
Figure 2 Traditional Sites versus Pharmacy Revisit Noninferiority Analysis. |
Discussion
This study quantitatively analyzed the cost-of-care difference between community pharmacies and traditional sites of care for several common conditions and assessed the impact on the healthcare system through revisit data. Data assessing the overall cost-of-care showed a statistically lower mean for patient care interventions provided by a pharmacist in a community pharmacy setting compared to the median cost from EDs, urgent care centers, and primary care. In addition, noninferiority was demonstrated related to the need to revisit care when the initial visit was conducted by a pharmacist compared to traditional sites of care. A sampling of patient comments documented during the 30-day follow up call were positive (Supplemental Exhibit 5). This, in addition to the number of patients who sought care at a community pharmacy, shows feasibility through patient demand as well as the ability to integrate the services into patient care workflows.
Patients in the study paid for services received at the community pharmacy out of pocket. If the 496 patients who received care at the pharmacy had sought care at traditional sites, using the aggregate median cost difference for all three traditional sites of care of $277.78, the additional cost to the healthcare system would have been approximately $138,000. In comparison, using the same aggregate median cost difference of $277.78, if the 84,555 patients who had sought care initially at a traditional site of care had been seen at a community pharmacy, the cost savings would be approximately $23,500,000. The potential cost savings to the healthcare system are staggering. As demonstrated, expanded opportunities for patients to receive clinical care in accessible, community-based settings may enhance sustainability of the healthcare system and, in turn, lower costs for patients and public health programs. As can be seen in the demographic data (Supplemental Exhibit 3), more women utilized community pharmacies than men, with hormonal contraception and UTI being the two most common conditions. While the overall median cost difference for hormonal contraception was the lowest of the services evaluated, the median cost difference for UTIs was the second highest. The majority of patients seen for a UTI at a traditional site of care in the study utilized the primary care setting; however, a 2015 report by the Washington Health Alliance listed UTIs as the fourth top condition both commercially-insured and Medicaid patients had unnecessarily sought care for at an ED in the five-county Puget Sound region.26 This study found costs of ED care for a UTI to be more than $1000 higher than care provided by a community pharmacist. By anticipating these needs alone, UTI-associated interventions initiated by community pharmacists could reduce healthcare spending significantly.
The pharmacists included in the study all completed the WSPA Clinical Community Pharmacist Certificate Program, however the certificate is not a requirement for providing the services in Washington state. The confidence gained through the certificate program, as well as the 8-hr live training session, may have increased willingness to offer services to patients seeking care. The same certificate program and live training have been included in the required curriculum in the college of pharmacy where the primary investigator has been employed since 2015.27 Recommendations made by the PAC (Supplemental Exhibit 6) were implemented in the live training, and recommendations related to the WSPA training were forwarded to them for consideration. As primary care physician shortage looms, and patient access to care is negatively impacted, pharmacy education programs around the country may have an opportunity to help address the gap in care by providing robust education for advanced patient care services and clinical decision making.
Community pharmacies offering patient care services might consider including methods to communicate with the PCP, allowing for a more complete patient health record and to decrease fragmentation of care. Ideally, community pharmacists would have access to electronic health records and input the care directly. For now, most community pharmacists fax or call a patient’s PCP. This information may or may not be included in the patient’s medical record at all, or in a way that is easily retrievable. One unexpected example of pharmacist and PCP collaboration was a patient informing the community pharmacist they were referred to the pharmacy to be seen for a UTI, as the PCP office stated the patient would be seen sooner than if making an appointment with them. While this is not currently commonplace, this level of trust and collaboration between the clinic and pharmacy is something to strive for in advancing collaborative, patient-centered care.
Conclusion
Overall, this research showed both feasibility and significant patient and public health cost savings when care was provided by a community pharmacist as compared to providers at traditional sites of care. Research findings support nationwide replication of this model of pharmacist-provided patient care resulting in increased access to healthcare for patients, particularly in rural and underserved areas. Enhanced patient outcomes along a continuum of care that is professional and longitudinal, not transactional, are efficient and improved access to timely healthcare.
The findings support the benefit to patients and public health programs of removing barriers to clinical care opportunities for patients in effective community-based settings, such as pharmacies. Due to systematic restrictions, patients in some states would not be able to access the care delivered in this research model. One important barrier, outside the scope of this project, is the lack of patient access to coverage for health interventions in emerging, community-based clinical care settings. Out-of-pocket costs may exacerbate barriers to patient access, especially for vulnerable populations, who may stand to benefit the most from enhanced access to care options.
Acknowledgments
We acknowledge the contributions of Chad Murphy, BS, PharmD, SVP/Chief Clinical Officer with Premera Blue Cross; Andrea Lazarus, PhD, Associate Dean for Research with the Washington State University College of Pharmacy and Pharmaceutical Sciences; Physician Advisory Committee members; Douglas Weeks, PhD; the Washington State Pharmacy Association; Bartell Drugs, Costco, Fred Meyer, Rosauers, and Yoke’s Fresh Market pharmacy personnel.
Preliminary findings were presented in a short oral presentation at the 2023 NACDS TSE Conference.
Disclosure
Dr Julie Akers and Dr Jennifer Miller report grants from the National Association of Chain Drug Stores Foundation, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Petterson SM, Liaw WR, Phillips RL, Rabin DL, Meyers DS, Bazemore AW. Projecting US primary care physician workforce needs: 2010–2025. Ann Fam Med. 2012;10(6):503–509. doi:10.1370/afm.1431
2. Weinick RM, Burns RM, Mehrotra A. Many emergency department visits could be managed at urgent care centers and retail clinics. Health Aff. 2010;29(9):1630–1636. doi:10.1377/hlthaff.2009.0748
3. National Association of Community Health Centers. 2006 Data on Community Health Centers Summary of Findings. National Association of Community Health Centers; 2006.
4. ER visits for UTIs add almost $4 billion a year in unnecessary healthcare costs. Infection Control Today; 2013. Available from: https://www.infectioncontroltoday.com/view/er-visits-utis-add-almost-4-billion-year-unnecessary-healthcare-costs.
5. Corso KA, Dorrance KA, LaRochelle J. The physician shortage: a red herring in American health care reform. Mil Med. 2018;183(3):220–224. doi:10.1093/milmed/usy211
6. Bodenheimer TS, Smith MD. Primary care: proposed solutions to the physician shortage without training more physicians. Health Aff. 2013;32(11):1881–1886. doi:10.1377/hlthaff.2013.0234
7. Giberson S, Yoder S, Lee MP. Improving Patient and Health System Outcomes Through Advanced Pharmacy Practice. A Report to the U.S. Surgeon General. Office of the Chief Pharmacist. U.S. Public Health Service; 2011.
8. Accreditation Council for Pharmacy Education. Accreditation standards and key elements for the professional program in pharmacy leading to the doctor of pharmacy degree; 2015. https://www.acpe-accredit.org/pdf/Standards2016FINAL.pdf.
9. Koshman SL, Charrois TL, Simpson SH, McAlister FA, Tsuyuki RT. Pharmacist care of patients with heart failure a systematic review of randomized trials. Arch Intern Med. 2008;168(7):687. doi:10.1001/archinte.168.7.687
10. Open for business: pharmacies respond to emergency. Rx Impact: A Drug Store News Special Report; 2016:7–9. Available from: https://s3.amazonaws.com/dig.drugstorenews.com/2016-02-rximpact/html5/index.html?page=1&noflash.
11. Erwin PB, Pitlick MK, Peters GL. Maintenance of goal blood pressure, cholesterol, and A1C levels in veterans with type 2 diabetes after discharge from a pharmacist-managed ambulatory care clinic. Diabetes Spectr. 2015;28(4):237–244. doi:10.2337/diaspect.28.4.237
12. Gubbins PO, Klepser ME, Dering-Anderson AM, et al. Point-of-care testing for infectious diseases: opportunities, barriers, and considerations in community pharmacy. J Am Pharm Assoc. 2014;54(2):163–171. doi:10.1331/japha.2014.13167
13. Klepser S, Klepser DG, Adams JL, Adams AJ, Klepser ME. Impact of COVID-19 on prevalence of community pharmacies as CLIA-Waived facilities. Res Social Adm Pharm. 2021;17(9):1574–1578. doi:10.1016/j.sapharm.2020.12.003
14. Akers JM, Adams AJ, Klepser ME. Review of pharmacy-based management of uncomplicated urinary tract infections (UTIs) in community pharmacy settings. Int J Pharm. 2018;8:63–69.
15. Gupta K, Hooton TM, Naber KG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the infectious diseases society of America and the European Society for Microbiology and Infectious Diseases. Clin Infect Dis. 2011;52(5):e103–e120. doi:10.1093/cid/ciq257
16. Lingenfelter E, Drapkin Z, Fritz K, et al. ED pharmacist monitoring of provider antibiotic selection aids appropriate treatment for outpatient UTI. Am J Emerg Med. 2016;34(8):1600–1603. doi:10.1016/j.ajem.2016.05.076
17. Zhang X, Rowan N, Mangel Pflugeisen B, Alajbegovic S. Urine culture guided antibiotic interventions: a pharmacist driven antimicrobial stewardship effort. Am J Emerg Med. 2017;35(4):594–598. doi:10.1016/j.ajem.2016.12.036
18. El Mansali S. Canadian Pharmacists Conference 2017 pharmacy practice research highlights. Can Pharm J. 2017;150(5):334–336. doi:10.1177/1715163517725517
19. Dobson EL, Klepser ME, Pogue JM, et al. Outpatient antibiotic stewardship: interventions and opportunities. J Am Pharm Assoc. 2017;57(4):464–473. doi:10.1016/j.japh.2017.03.014
20. Weber NC, Klepser ME, Akers JM, Klepser DG, Alex AJ. Use of CLIA-waived point-of-care tests for infectious diseases in community pharmacies in the United States. Expert Rev Mol Diagn. 2016;16(2):256–264. doi:10.1586/14737159.2015.1116388
21. Kummervold PE, Johnsen JA, Skrøvseth SO, Wynn R. Using noninferiority tests to evaluate telemedicine and e-health services: systematic review. J Med Internet Res. 2012;14(5):e132. doi:10.2196/jmir.2169
22. Altman D, Machin D, Bryant T, Gardner M. Statistics with Confidence: Confidence Intervals and Statistical Guidelines.
23. Walker E, Nowacki AS. Understanding equivalence and noninferiority testing. J Gen Inter Med. 2011;26(2):192–196. doi:10.1007/s11606-010-1513-8
24. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) – a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
25. Harris PA, Taylor R, Minor BL, et al. REDCap Consortium. The REDCap consortium: building an international community of software partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
26. Washington Health Alliance. Right care, right setting: a report on potentially avoidable emergency room visits in Washington state; 2015. Available from: https://wahealthalliance.org/alliance-reports-websites/alliance-reports/right-care-right-setting/.
27. McKeirnan KC, Akers JM, Czapinski JC, Robinson JD. Using collaborative drug therapy agreements to train student pharmacists to provide clinical patient care services. Am J Pharm Educ. 2017;81(2). doi:10.5688/ajpe81231
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.