Back to Journals » Clinical Epidemiology » Volume 13
Existing Data Sources for Clinical Epidemiology: The Danish Study Group of Infections of the Brain Database (DASGIB)
Authors Bodilsen J ![]() , Larsen L
, Larsen L ![]() , Brandt CT, Wiese L, Hansen BR, Andersen CØ, Lüttichau HR
, Brandt CT, Wiese L, Hansen BR, Andersen CØ, Lüttichau HR ![]() , Helweg-Larsen J, Storgaard M, Nielsen H
, Helweg-Larsen J, Storgaard M, Nielsen H ![]()
Received 25 June 2021
Accepted for publication 27 August 2021
Published 4 October 2021 Volume 2021:13 Pages 921—933
DOI https://doi.org/10.2147/CLEP.S326461
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Eyal Cohen
Jacob Bodilsen,1 Lykke Larsen,2 Christian Thomas Brandt,3,4 Lothar Wiese,4 Birgitte Rønde Hansen,5 Christian Østergaard Andersen,6 Hans Rudolf Lüttichau,7 Jannik Helweg-Larsen,8 Merete Storgaard,9 Henrik Nielsen1,10
1Department of Infectious Diseases, Aalborg University Hospital, Aalborg, 9000, Denmark; 2Department of Infectious Diseases, Odense University Hospital, Odense, 5000, Denmark; 3Department of Infectious Diseases, Nordsjællands Hospital, Hillerød, 3400, Denmark; 4Department of Infectious Diseases, Sjælland University Hospital, Roskilde, 4000, Denmark; 5Department of Infectious Diseases, Hvidovre University Hospital, Copenhagen, 2650, Denmark; 6Department of Clinical Microbiology, Hvidovre University Hospital, Copenhagen, 2650, Denmark; 7Department of Infectious Diseases, Herlev Gentofte Hospital, Copenhagen, 2730, Denmark; 8Department of Infectious Diseases, Rigshospitalet, Copenhagen, 2100, Denmark; 9Department of Infectious Diseases, Aarhus University Hospital, Aarhus, 8200, Denmark; 10Department of Clinical Medicine, Aalborg University, Aalborg, 9000, Denmark
Correspondence: Jacob Bodilsen
Department of Infectious Diseases, Aalborg University Hospital, Mølleparkvej 4, Aalborg, DK9000, Denmark
Tel +45 97660566
Email [email protected]
Abstract: Central nervous system (CNS) infections are rare diseases that are associated with considerable morbidity and mortality. Increased knowledge based on contemporary data is a prerequisite for improved management and prevention of these serious conditions. Yet, population-based databases of patients hospitalized with CNS infections remain scarce. The Danish Study Group of Infections of the Brain (DASGIB) has prospectively registered information on all adults ≥ 18 years of age admitted with CNS infections at departments of infectious diseases in Denmark since 2015. The main variables collected are baseline demographics, blood and cerebrospinal fluid tests, imaging results, and outcome using the Glasgow Outcome Scale score. To investigate important aspects for each type of CNS infections, additional variables are included specifically for bacterial meningitis, viral meningitis, encephalitis, brain abscess, neurosyphilis, and Lyme neuroborreliosis. From 2015 to 2020, a total of 3579 cases of CNS infections have been recorded in the DASGIB database. Using the unique civil registration number assigned to all Danish residents, the database can be unambiguously linked with nationwide healthcare registries at the individual level. This enables researchers to conduct detailed population-based and longitudinal observational studies of risk and prognosis of CNS infections and to compare them with matched population cohorts. The database is well-suited for epidemiological research and the DASGIB network forms a solid infrastructure for future national and international collaborations.
Keywords: CNS infections, epidemiology, database, cohort studies, bacterial meningitis, viral meningitis, encephalitis, brain abscess, cerebral abscess, neurosyphilis, syphilis, Lyme neuroborreliosis, borreliosis
Introduction
Infections of the central nervous system (CNS) may be caused by an abundance of different pathogens including bacteria, virus, fungi, and parasites.1,2 Accordingly, the clinical spectrum of disease is wide and ranges from self-limiting viral meningitis to medical emergencies such as bacterial meningitis requiring immediate treatment. The microorganisms may enter the CNS by direct invasion or by hematogenous spread. Key factors for evasion of host defense mechanisms involve defects in neuroanatomical barriers, pathogen virulence factors, and presence of immuno-compromising conditions.
The clinical presentation and prognosis of CNS infections has been examined in several high-quality cohort studies and databases, which have provided us with valuable knowledge.3–15 However, the majority of studies in CNS infections are still limited by retrospective design and small sample sizes, or they may have relied on administrative registries and microbiological databases without access to detailed clinical data.14–18 Hence, the Danish Study Group of Infections of the Brain (DASGIB) was established in 2014 and a prospective recording of all adults admitted with CNS infections at departments of infectious diseases in Denmark was initiated as of January 1, 2015.
A Historical Perspective of Research on CNS Infections
Studies of CNS infections has a longstanding tradition (Table 1). Bacterial meningitis has been studied extensively including effects of antiserum and antibiotic treatments as well as changes in epidemiological characteristics, especially after the introduction of vaccines against major pathogens such as Haemophilus influenzae type b, Neisseria meningitidis, and Streptococcus pneumoniae in childhood vaccination programs.19–23 However, viral CNS infections, neurosyphilis, and Lyme neuroborreliosis have also received considerable attention through the last century,24–37 whereas brain abscess has been studied somewhat less frequently.38–40
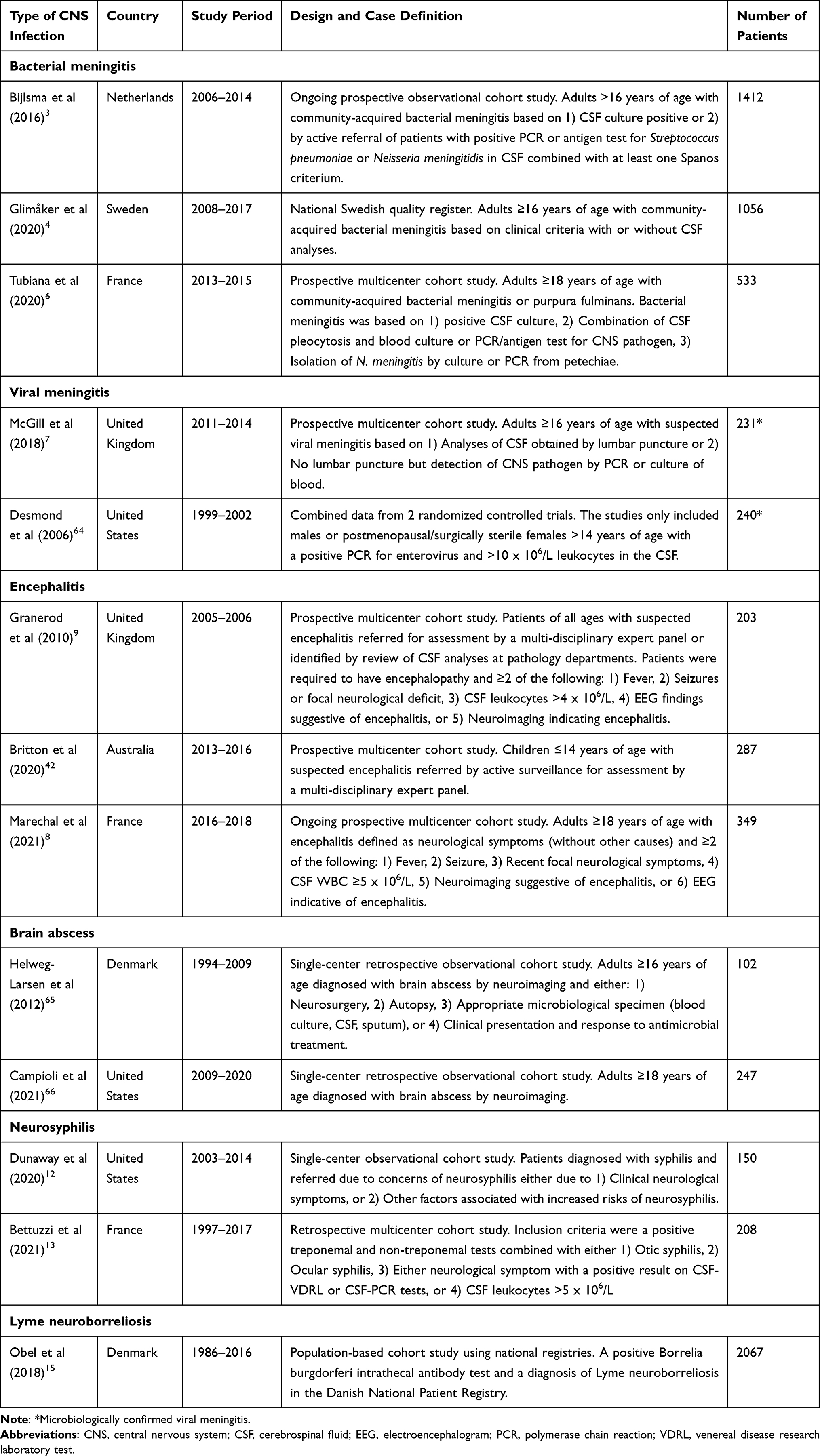 |
Table 1 Overview of Selected Databases and Observational Cohort Studies of Central Nervous System Infections |
Strategies for Studies on CNS Infections
Patients with CNS infections may be identified by retrieval of positive test results for certain pathogens in cerebrospinal fluid (CSF) or other CNS samples using electronic information systems at departments of clinical microbiology. Although this strategy allows the researcher to examine specific microorganisms and leads to a well-defined group of patients, it usually does not encompass the entire clinical spectrum of many CNS infections and determination of whether or not a pathogen is a contaminant may be difficult. Sometimes the diagnostic yield is hampered by preceding antimicrobial treatment or the pathogen may be identified in other clinically relevant samples, eg blood cultures, combined with clinical markers of CNS infection such as CSF pleocytosis or cranial imaging. Occasionally, the pathogen may be difficult to identify, eg due to decreased sensitivity of microbiological analyses at different stages of disease in patients with encephalitis or because of inaccessibility of a brain abscess.
The identification of patients with CNS infections may also be conducted by searches in healthcare registries using the World Health Organisation’s International Classification of Diseases (ICD) codes. Important limitations of this approach are that diagnosis codes may vary between different versions of ICD and that the positive predictive value, sensitivity, and specificity may be low. In addition, lack of clinical details precludes analyses based on the clinical characteristics.
In contrast, large multi-center clinical databases have the potential to include the entire range of clinical presentations of the examined CNS infections combined with detailed clinical observations. Several prospective observational studies have been conducted in bacterial meningitis in adults using different definitions ranging from CSF culture positive cases only to allowance of inclusion of patients based solely on clinical criteria.3,4,6 Other CNS infections have rarely been examined in prospective clinical registries. A few studies have investigated hospitalized adults suspected of CNS infections,7,41 whereas other databases have focused on children or adults with encephalitis.8,9,42
DASGIB – Aim and Organization
To improve research as well as quality of treatment and care of CNS infections, physicians at Danish departments of infectious diseases founded the DASGIB study group in 2014. This resulted in the establishment of the nationwide, prospective, and population-based DASGIB database of all patients admitted with community-acquired CNS infections at departments of infectious diseases in Denmark as of January 1, 2015 (Figure 1). Initially, the study group consisted of representatives from the departments of infectious diseases at hospitals in Aalborg, Aarhus, Odense, Hvidovre, Roskilde, Hillerød, and Copenhagen (Rigshospitalet). In 2018, the group was expanded to also include a member from Herlev Hospital. The DASGIB study group is managed by the secretariat located in Aalborg.
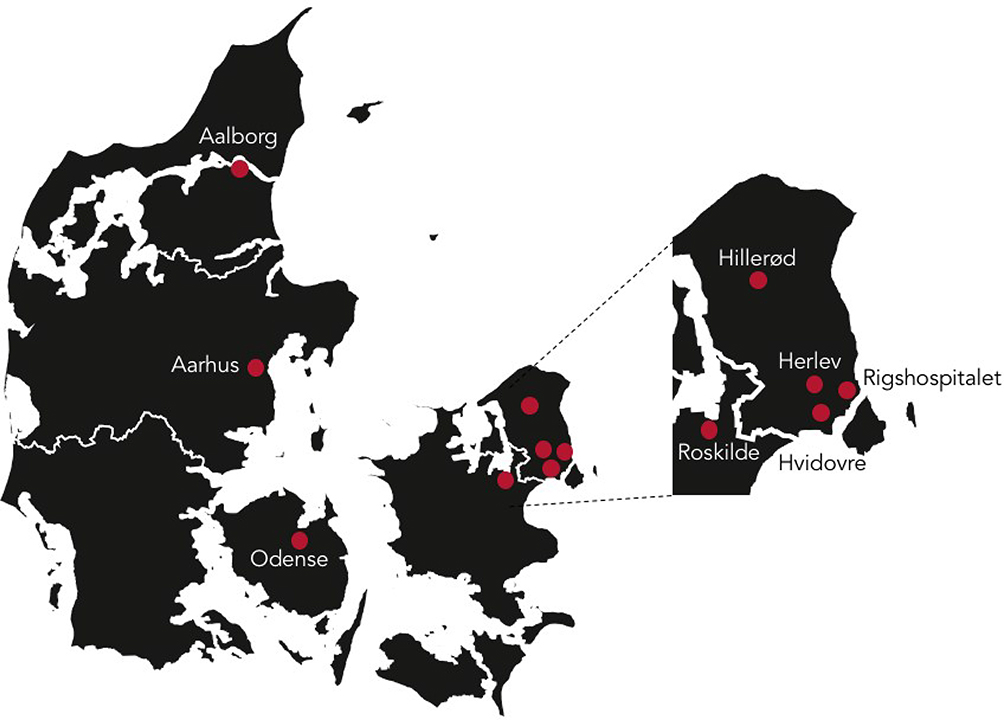 |
Figure 1 The geographical distribution of the Danish Study Group of Infections of the Brain (DASGIB) study sites. |
Setting and Study Population
Denmark is a welfare state and has a mixed rural and urban population totaling 4,666,625 adults ≥18 years of age (5,822,763 including children and adolescents) as of January 1, 2020 (Table 2).43 The Danish healthcare system is tax-financed and all residents are thus provided with access, free of charge at the point of delivery, to general practitioners for primary care and public hospitals for secondary and tertiary care.44 A unique civil registration number is assigned to all Danish residents at birth or immigration. This allows for unambiguous linkage across numerous nationwide registries at the individual level and for complete tracking of migration and vital status with <0.3% loss to follow-up.45 The Danish childhood vaccination program includes vaccines for potential CNS pathogens such as measles, mumps, rubella, H. influenzae type b, and Streptococcus pneumoniae (Table 3).
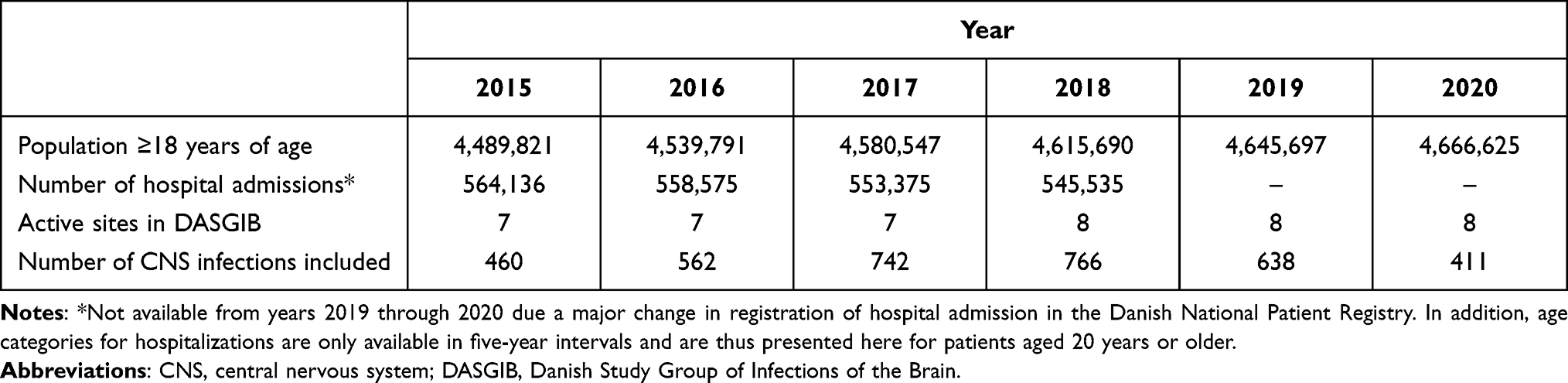 |
Table 2 Demographics of the Adult Danish Population, Number of Hospitalizations Among Adults, and Number of Active Sites in the DASGIB Database Since Initiation on January 1, 2015 |
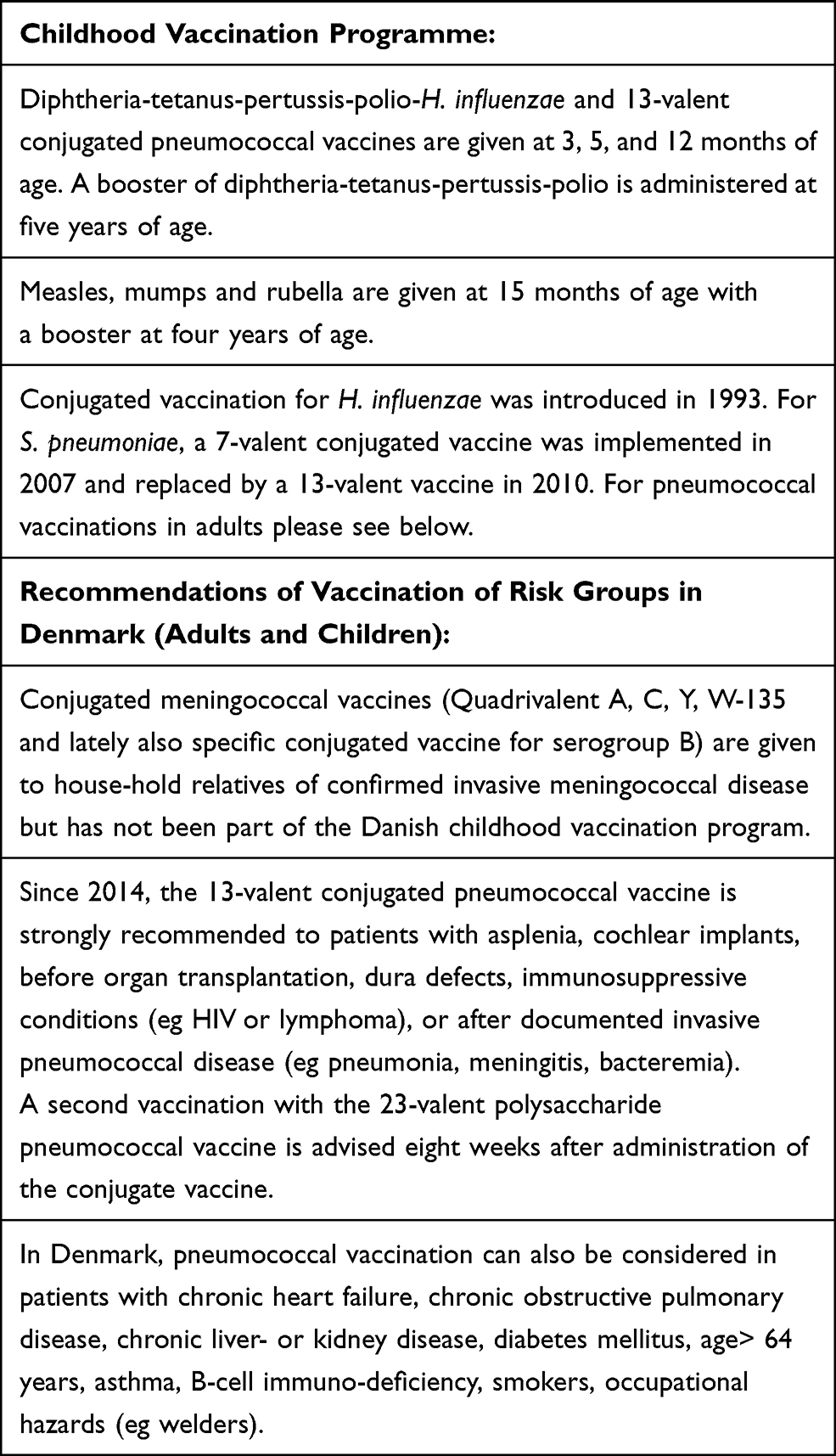 |
Table 3 The Danish Vaccination Program for Known Central Nervous System Pathogens |
According to the Danish Board of Health, all CNS infections are to be managed at hospitals with onsite departments of infectious diseases and availability of round the clock consultation by an infectious disease specialist.46 These are located at the four tertiary care centers in Denmark (Aalborg, Aarhus, Odense, and Rigshospitalet) and at regional centers for infectious diseases at the hospitals at Roskilde, Hvidovre, Hillerød and Herlev-Gentofte.
Currently, departments of neurosurgery and neurocritical care are limited to the four tertiary care centers in Denmark. Nucleic acid amplification tests (NAAT) have been available at all departments of clinical microbiology since the start of the DASGIB database, either as in-house tests (pathogen specific and/or as syndromic panel testing using FilmArray or comparable techniques) or by centralized services provided by Statens Serum Institute (eg 16s DNA amplification or next-generation sequencing). National guidelines for treatment of bacterial and viral meningitis, encephalitis, and Lyme neuroborreliosis are provided by the Danish Infectious Diseases Society.47
Definitions of CNS Infections
Inclusion criteria of CNS infections often vary between studies. The definitions used in the DASGIB database are based on results of lumbar puncture in all patients (except for brain abscess patients) combined with a relevant clinical presentation, microbiological investigations, and cranial imaging (Table 4). Furthermore, CNS infection has to be considered the most probable diagnosis after taking into account all available information from the index and any other relevant hospitalizations at time of medical record review and as assessed by a specialist in infectious diseases. For patients with suspected encephalitis, adherence to the criteria of the International Encephalitis Consortium (year 2013) is generally encouraged but not mandatory since this definition may not capture all conceivable presentations of encephalitis.48,49 Patients with proven or suspected autoimmune encephalitis are excluded. Likewise, patients with nosocomial CNS infections are excluded defined as those occurring during hospitalization for other causes, previous neurosurgery within 30 days of admission, or indwelling hardware in the CNS (eg ventriculo-peritoneal shunts or deep-brain stimulators). In all cases of doubt, patients are discussed with the DASGIB secretary (JB) or at bi-annual DASGIB meetings.
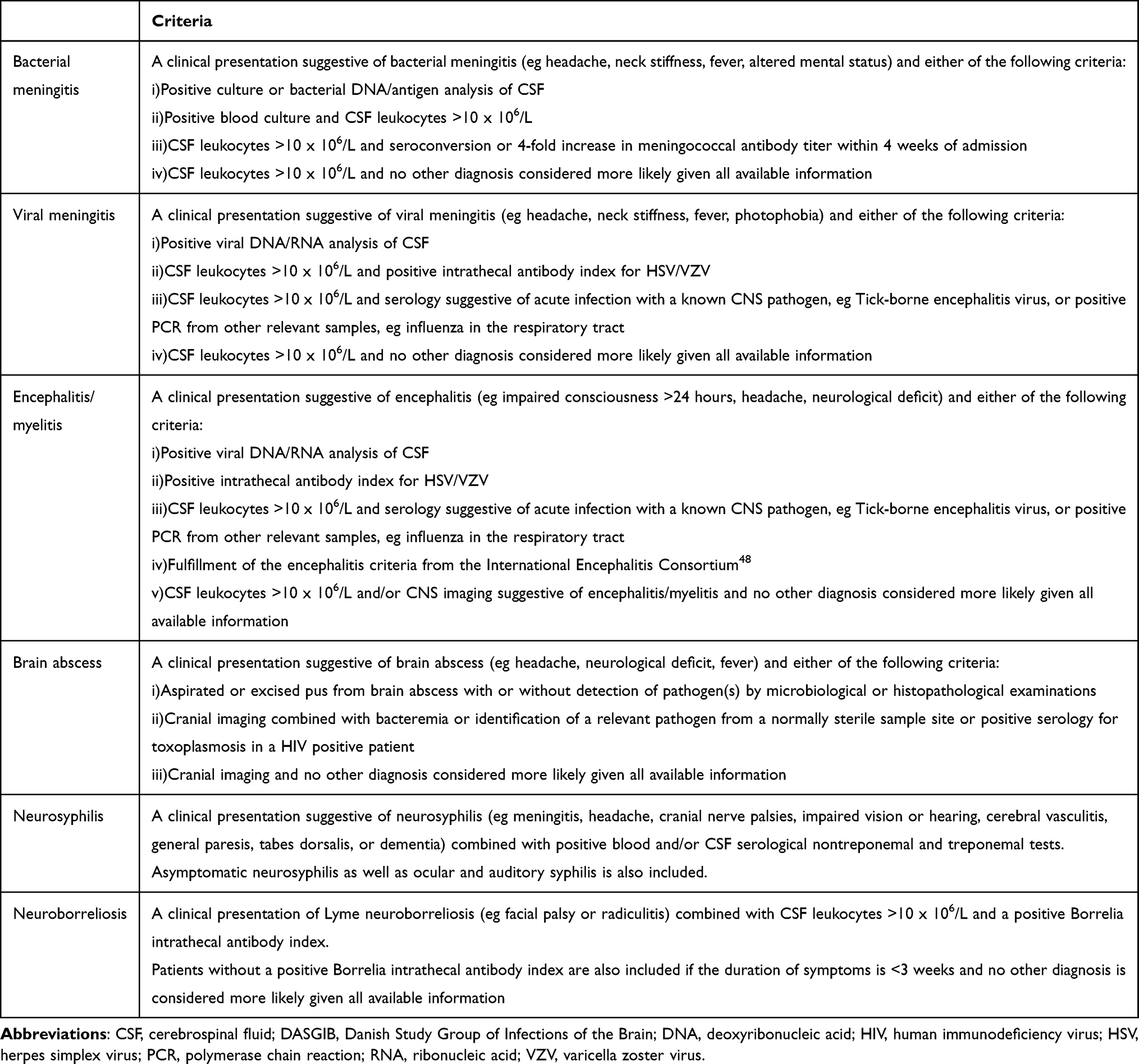 |
Table 4 Definitions for Central Nervous System Infections Used in the DASGIB Database |
Whenever possible, the pathogen is determined, but inclusion of patients with unknown microbiological etiology is allowed to ensure that the entire clinical spectrum of disease is covered. This is important as the pathogen remains unknown for a substantial part of patients with CNS infections which may infer considerable uncertainty among patients and physicians. Hence, increased knowledge on the prognosis of these patients is crucial.
Data Collection and Variables
Data Sources
The primary data sources used for data collection consist of the electronic medical records including ambulance records, doctor’s records, nurse’s charts, laboratory results of blood and CSF analyses, radiological examinations, microbiological analyses, electronic medication records, intensive care unit observation charts, outpatient visits, and any subsequent hospital admissions. However, if patients are treated directly by the local investigator, further information may be obtained by ad hoc personal interviews.
Informatics
An online case report form developed by the IT services at North Denmark Region was used until July 1, 2016 when it was replaced by a more user-friendly and detailed database using REDcap.50 Data are extracted from the medical records by each local DASGIB representative who is a specialist in infectious diseases or by specially trained research assistants. A standard operating procedure for retrieval and entering of data is provided (Supplementary Material) and consultation with the DASGIB secretary is encouraged on a case-to-case basis if in doubt. The database is continuously updated and queries for missing values and outliers are sent to local DASGIB representatives by the DASGIB secretary. Completeness of inclusion of cases with CNS infection is ensured by annual searches at each department of infectious diseases using ICD-10 diagnosis codes or medical record review of all patients with CSF leukocytosis (Supplementary Table 1).
Variables
General information on baseline demographics, blood and CSF tests, imaging results, and outcome for all included cases are recorded in the database (Please see the Supplementary Material for the full case report form). Additional sets of disease-specific variables have been tailored to capture important traits and aspects for each type of CNS infection, ie bacterial meningitis, viral meningitis, encephalitis, brain abscess, neurosyphilis, and Lyme neuroborreliosis.
Main variables registered include date, time, and place of admission; referral and admission diagnoses; duration of symptoms; travel history; pre-existing comorbidities and functional level; exposures; symptoms and signs of relevance for each CNS infection; date and time of antimicrobial treatment, lumbar puncture, and cranial imaging when performed; complications during admission including admission to the intensive care unit and neurocritical care; and Glasgow Outcome Scale51 score at discharge and at 1-, 3-, and 6-months after discharge (Table 5). Concomitant foci of infection are determined according to clinical practice and may rely on microbiological investigations of samples outside the CNS, imaging results, consultations by ear-nose-throat specialists, and echocardiography.
 |
Table 5 Study Variables and Data Sources Used in the DASGIB Database |
Time of hospital admission is used as reference for computations of time to antimicrobial therapy, lumbar puncture, cranial imaging, hospital discharge, and death. Time of empirical antimicrobial treatment is defined as first administration of a drug in dosages recommended for treatment of the specific CNS infection in question,47,52–54 whereas targeted treatment denotes adjustments according to pathogen identification and antimicrobial susceptibility. Occasionally, patients may switch antimicrobial regimens during prolonged treatment in which case the drug used for the majority of treatment is registered. Vital status is obtained from the electronic medical records which are synchronized with the Danish Civil Registration System on a daily basis.44,45
Biobank
Thus far, blood and CSF samples have been collected from 361/3579 (10%) patients with CNS infections at some DASGIB sites (Aalborg, Hvidovre, Skejby, and Rigshospitalet). These samples are stored according to local protocols in freezers at −80° Celsius and can be used for research purposes after obtainment of government approval according to Danish law.
Time Period
All adults hospitalized with a CNS infection at department of infectious diseases in Denmark have been included in the DASGIB database yielding a total of 3579 cases from January 1, 2015 through December 31, 2020 (Figure 2). This included patients ≥16 years of age until June 30, 2016 when changes in hospital visitation practices of all adolescents to pediatric departments were implemented and since then only adults ≥18 years of age have been registered. An outbreak of enterovirus meningitis in years 2017 and 2018 caused a temporary increase in the annual number of included cases of CNS infections.55
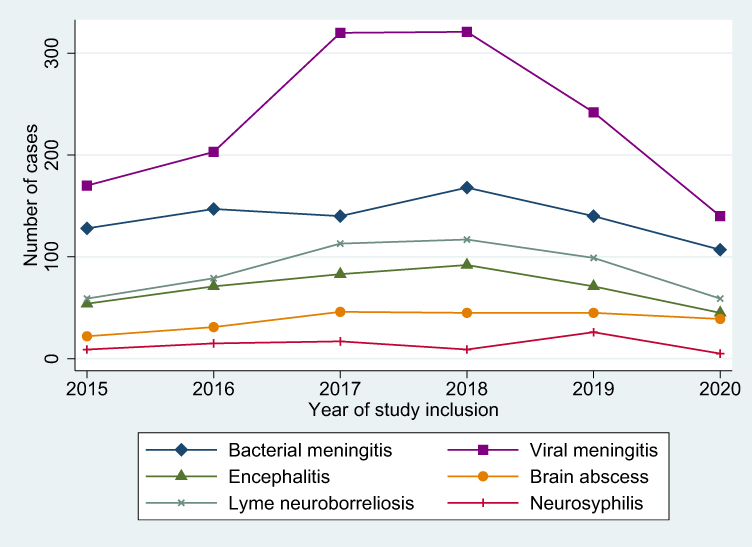 |
Figure 2 Annual number of central nervous system infections included in the Danish Study Group of Infections of the Brain (DASGIB) database. |
Methodological Aspects
Strengths and Weaknesses
A major strength of the DASGIB database is the ongoing inclusion of longitudinal and prospectively collected detailed clinical data on all adults treated for CNS infections at Danish departments of infectious diseases for six years by now. Although CNS infections are relatively rare, this has resulted in an exceptionally large sample size that is unique on a global scale. Moreover, the nationwide and population-based design with virtually complete follow-up for subsequent hospital contacts and mortality adds to the importance of the DASGIB database. The database was developed and is maintained by infectious diseases clinicians, which may help to keep focus on clinically relevant dilemmas and challenges in the management of patients with CNS infections. Another advantage of the database is that the quality and completeness of the recorded information is continuously monitored, and great efforts are made to constantly improve data collection.
The individual civil registration number assigned to all Danish residents also allows for unambiguous linkage of DASGIB data with other nationwide healthcare and socioeconomic registries. This may include the Danish National Patient Registry which holds information on all hospital admissions since 1977 and outpatient visits since 1995;56 the Danish Civil Registration System that contains data on vital and migration status of all Danish residents;45 the Danish Laboratory Database which includes results of most major biochemical laboratories in Denmark corresponding to approximately 80% of the Danish population;57 and the Danish National Prescription Registry that comprises key information on reimbursable drugs dispensed from Danish pharmacies since 1994.58 Combining the DASGIB database with these resources makes it possible to examine large cohorts of CNS infection patients with complete hospitalization history and comorbidities as well as long-term follow-up. The Danish Civil Registration System also allows for the formation of matched cohort and case-control studies by selection of controls from the underlying source population using density sampling.
Importantly, the DASGIB study group comprises representatives from all departments of infectious diseases in Denmark and may thereby coordinate and facilitate a concerted effort of research in CNS infections. This will hopefully continue to foster a synergistic effect that may improve the quality and clinical impact of the planned research projects.
The main limitation is that some patients with relatively non-severe forms of CNS infections such as viral meningitis or Lyme neuroborreliosis may occasionally be treated at regional hospitals or at departments of neurology. In addition, some patients with severe hematological diseases or solid-organ transplants may be managed at other departments without assistance of infectious diseases specialists and thereby missed inclusion into the DASGIB database. This may lead to selection bias if such patients differ substantially from the included patients and an underestimation of incidence using the DASGIB database. However, we expect this bias to be limited given the directive from the Danish Board of Health that all CNS infections should be managed by infectious diseases specialists.46 Another limitation is the lack of uniform procedures for post-discharge patient contact for addressing missing values from the index admission. Finally, local protocols for obtainment and pre-analytic processing of blood and CSF samples are not yet standardized.
Research from the Database
Research from the DASGIB study group has thus far primarily focused on descriptive studies of the clinical presentation and outcome of community-acquired CNS infections. The first study highlighted the usefulness of CSF lactate for the diagnosis of bacterial meningitis in patients with suspected CNS infection.59 CSF lactate is an inexpensive test that can easily be analyzed within minutes after lumbar puncture and is readily available at almost all hospitals. The study showed that CSF lactate had the best diagnostic value for bacterial versus viral meningitis with an area under the curve of 0.976 (95% CI 0.966–0.997) using a cut-off of 3.5 mmol/L. The second study reported the epidemiological trends in meningitis (bacterial and viral) and encephalitis during the first 1.5 years of the DASGIB database. The predominant pathogen in bacterial meningitis was S. pneumoniae, whereas N. meningitidis and Listeria monocytogenes were infrequent compared with other settings.3,4,6 Of note, S. aureus and ß-hemolytic streptococci were the second and third most common causes of bacterial meningitis in the DASGIB cohort during this study period. Viral meningitis was mainly due to Varicella zoster virus and enterovirus, and Herpes simplex virus 1 was the primary pathogen among cases of encephalitis.
Next, two studies have examined the management of Lyme neuroborreliosis in Denmark. One study found that cranial imaging was often performed in elderly comorbid patients to rule out other diagnoses, whereas the second study observed that a substantial diagnostic delay and prolonged antibiotic treatment beyond 14 days was frequent in these patients.60,61
Another study analyzed risk factors and prognosis of seizures in bacterial meningitis using a retrospective derivation cohort and subsequently validating the findings in the DASGIB cohort.62 Risk factors for seizures consisted of pneumococcal etiology, immuno-compromise, and abnormal cranial imaging (mainly stroke), and seizures at any time during illness predicted both in-hospital mortality and unfavorable outcome at discharge. Using the DASGIB cohort, a case series provided a valuable and detailed clinical description of 12 patients with normocellular bacterial meningitis.63 The diagnosis was confirmed by culture (S. pneumoniae, n=10; S. aureus, n=1) or polymerase chain reaction (N. meningitidis, n=1) of the CSF. Importantly, none of the patients had serious immuno-compromising conditions and the overall case-fatality rate was 25%.
A large study on Varicella zoster virus encephalitis highlighted the complexity of the diagnosis and treatment challenges of this life-threatening disease. Predisposing immunocompromising conditions were frequent (39%) and the main symptoms were confusion (76%), headache (56%), nausea (45%), gait disturbance (42%), and personality changes (41%). A diagnosis of cerebral vasculitis was not uncommon (16%) and encephalitic abnormalities (13%) had a predilection for the brainstem and other deep brain structures. Unfavorable outcome at discharge was observed in 69% and was associated with increasing age, vasculitis, and Glasgow Coma Scale score <15.
Finally, the largest study to date on enteroviral meningitis in adults (n=419 cases) showcased a 2017–2018 national epidemic attributable to Echovirus 30.55 Admission diagnoses included CNS infection in 62%, other neurological conditions in 22%, and cerebrovascular diseases accounted in 8%. A polymorphonuclear predominance in the CSF was frequent if lumbar puncture was performed within 3 days of onset of symptoms. Cranial imaging preceded lumbar puncture in 30% of patients and was associated with a delay in time to lumbar puncture from median 1.5 hours (IQR 0.8–2.8) to 4.8 hours (IQR 3.4–7.9; p<0.001 for comparison). A GOS score of 4 was observed in 24% at discharge and was associated with female sex and less frequent in Echovirus 30.
Permissions and Access for Other Researchers
The DASGIB database is approved by the legal department at the North Denmark Region (record numbers 2008-58-0028 with local ID 2017-241 for the database and 2013-41-2502 for the biobank) and the Danish Board of Health (record numbers 3-3013-2579/1 and 3-3013-3168/1). Patient consent or permission from an ethical committee is not required for this type of study in Denmark. All data is managed in compliance with relevant data protection and privacy regulations and in accordance with the Helsinki declaration. The DASGIB study group encourages multidisciplinary collaborations and is very interested in working together with other Danish and international researchers after obtainment of proper approvals. Potential collaborators are invited to contact the corresponding author.
Perspectives
Knowledge on the epidemiology, clinical presentation, and outcome of CNS infections is paramount for identifying and determining research priorities and for allocation of healthcare resources. Unfortunately, high-quality and contemporary data on fundamental characteristics of most CNS infections are scarce and much remains to be explored. Nationwide and population-based studies improve the confidence in incidence estimates, risk factors, and prognosis due to the well-defined catchment area and completeness of follow-up. The large study population of approximately 4.6 million adult Danish residents also provides researchers with the opportunity to examine rare CNS infections and may contribute to detection of emerging pathogens. The DASGIB study group is dedicated to future multidisciplinary research projects that may involve clinical microbiologists, neurologists, neurosurgeons, radiologists, engineers, molecular biologists, and clinical epidemiologists with the hope of gaining new insights into changes in the etiology, risk- and prognostic factors, and treatment of CNS infections.
Already, the DASGIB study group is active in several international research projects including sponsoring an investigator-initiated large randomised non-inferiority trial on early transition to oral treatment of brain abscess that is conducted in Denmark, Sweden, France, the Netherlands, and Australia (ORAL study; EudraCT 2019-002845-39). This international study has triggered a number of other research collaborations with the hope of advancing management of CNS infections further. Finally, the DASGIB infrastructure provides an essential framework for future international clinical trials on CNS infections in Denmark.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
No funding was obtained for this study and all authors report no conflicts of interests.
References
1. Bennett JE, Dolin R, Blaser MJ. Mandell, Douglas and Bennett’s Principles and Practice of Infectious Diseases.
2. Michael SW, Whitley RJ, Marra CM. Infections of the Central Nervous System.
3. Bijlsma MW, Brouwer MC, Kasanmoentalib ES, et al. Community-acquired bacterial meningitis in adults in the Netherlands, 2006-14: a prospective cohort study. Lancet Infect Dis. 2016;16(3):339–347. doi:10.1016/S1473-3099(15)00430-2
4. Glimåker M, Naucler P, Sjölin J. Etiology, clinical presentation, outcome and the effect of initial management in immunocompromised patients with community acquired bacterial meningitis. J Infect. 2020;80:291–297. doi:10.1016/j.jinf.2019.12.019
5. Bodilsen J, Storgaard M, Larsen L, et al. Infectious meningitis and encephalitis in adults in Denmark: a prospective nationwide observational cohort study (DASGIB). Clin Microbiol Infec. 2018;24(10):
6. Tubiana S, Varon E, Biron C, et al. Community-acquired bacterial meningitis in adults: in-hospital prognosis, long-term disability and determinants of outcome in a multicentre prospective cohort. Clin Microbiol Infec. 2020;26(9):1192–1200. doi:10.1016/j.cmi.2019.12.020
7. McGill F, Griffiths MJ, Bonnett LJ, et al. Incidence, aetiology, and sequelae of viral meningitis in UK adults: a multicentre prospective observational cohort study. Lancet Infect Dis. 2018;18(9):992–1003. doi:10.1016/S1473-3099(18)30245-7
8. Maréchal ML, Mailles A, Seigneurin A, Tattevin P, Stahl J-P, Épaulard O. A prospective cohort study to identify clinical, biological, and imaging features that predict the etiology of acute encephalitis. Clin Infect Dis. 2020;73(2):264–270.
9. Granerod J, Ambrose HE, Davies NW, et al. Causes of encephalitis and differences in their clinical presentations in England: a multicentre, population-based prospective study. Lancet Infect Dis. 2010;10(12):835–844. doi:10.1016/S1473-3099(10)70222-X
10. Herlin LK, Hansen KS, Bodilsen J, et al. Varicella Zoster Virus encephalitis in Denmark from 2015 to 2019- a nationwide prospective cohort study. Clin Infect Dis. 2020;72(7):1192–1199. doi:10.1093/cid/ciaa185
11. Glaser CA, Gilliam S, Schnurr D, et al. In search of encephalitis etiologies: diagnostic challenges in the California Encephalitis Project, 1998–2000. Clin Infect Dis. 2003;36(6):731–742. doi:10.1086/367841
12. Dunaway SB, Maxwell CL, Tantalo LC, Sahi SK, Marra CM. Neurosyphilis treatment outcomes after intravenous penicillin G versus intramuscular procaine penicillin plus oral probenecid. Clin Infect Dis. 2019;71(2):267–273. doi:10.1093/cid/ciz795
13. Bettuzzi T, Jourdes A, Robineau O, et al. Ceftriaxone compared with benzylpenicillin in the treatment of neurosyphilis in France: a retrospective multicentre study. Lancet Infect Dis. 2021. doi:10.1016/S1473-3099(20)30857-4
14. Bodilsen J, Dalager-Pedersen M, van de Beek D, Brouwer MC, Nielsen H. Long-term mortality and epilepsy in patients after brain abscess: a nationwide population-based matched cohort study. Clin Infect Dis. 2019;71(11):2825–2832. doi:10.1093/cid/ciz1153
15. Obel N, Dessau RB, Krogfelt KA, et al. Long term survival, health, social functioning, and education in patients with European Lyme neuroborreliosis: nationwide population based cohort study. BMJ. 2018;361:k1998. doi:10.1136/bmj.k1998
16. Bubba L, Broberg EK, Jasir A, et al.; collaborators E study. Circulation of non-polio enteroviruses in 24 EU and EEA countries between 2015 and 2017: a retrospective surveillance study. Lancet Infect Dis. 20;2019:350–361. doi:10.1016/S1473-3099(19)30566-3
17. Omland LH, Vestergaard HT, Dessau RB, et al. Characteristics and long-term prognosis of Danish patients with varicella zoster virus detected in cerebrospinal fluid compared with the background population. J Infect Dis. 2021;224:850–859. doi:10.1093/infdis/jiab013
18. Roed C, Omland LH, Skinhoj P, Rothman KJ, Sorensen HT, Obel N. Educational achievement and economic self-sufficiency in adults after childhood bacterial meningitis. JAMA. 2013;309(16):1714. doi:10.1001/jama.2013.3792
19. Flexner S. The results of the serum treatment in thirteen hundred cases of epidemic meningitis. J Exp Med. 1913;17(5):553–576. doi:10.1084/jem.17.5.553
20. Swartz MN. Bacterial meningitis–a view of the past 90 years. N Engl J Med. 2004;351(18):1826–1828. doi:10.1056/NEJMp048246
21. Swartz MN, Dodge PR. Bacterial meningitis — a review of selected aspects — general clinical features, special problems and unusual meningeal reactions mimicking bacterial meningitis. N Engl J Med. 1965;272(17):898–902. doi:10.1056/NEJM196504292721707
22. Meads M, Harris HW, Samper BA, Finland M, Wilcox C. Treatment of meningococcal meningitis with penicillin. N Engl J Med. 1944;231(15):509–517. doi:10.1056/NEJM194410122311501
23. de Gans J, van de Beek D; Investigators ED in ABMS. Dexamethasone in adults with bacterial meningitis. N Engl J Med. 2002;347(20):1549–1556. doi:10.1056/NEJMoa021334
24. Meyer HM, Johnson RT, Crawford IP, Dascomb HE, Rogers NG. Central nervous system syndromes of “viral” etiology A study of 713 cases. Am J Med. 1960;29(2):334–347. doi:10.1016/0002-9343(60)90029-2
25. Whitley RJ, Soong SJ, Dolin R, Galasso GJ, Ch’ien LT, Alford CA. Adenine arabinoside therapy of biopsy-proved herpes simplex encephalitis. National Institute of Allergy and Infectious Diseases collaborative antiviral study. N Engl J Med. 1977;297(6):289–294. doi:10.1056/NEJM197708112970601
26. Whitley RJ, Alford CA, Hirsch MS, et al. Vidarabine versus Acyclovir therapy in herpes simplex encephalitis. N Engl J Med. 1986;314(3):144–149. doi:10.1056/NEJM198601163140303
27. Sköldenberg B, Alestig K, Burman L, et al. Acyclovir versus vidarabine in Herpes simplex encephalitis. Lancet. 1984;324(8405):707–711. doi:10.1016/S0140-6736(84)92623-0
28. Ghanem KG. REVIEW: neurosyphilis: a historical perspective and review. Cns Neurosci Ther. 2010;16(5):e157–e168. doi:10.1111/j.1755-5949.2010.00183.x
29. Moore JE, Hopkins HH. Asymptomatic neurosyphilis: VI. The prognosis of early and late asymptomatic neurosyphilis. J Amer Med Assoc. 1930;95(22):1637–1641. doi:10.1001/jama.1930.02720220007003
30. Clark EG, Danbolt N. The Oslo study of the natural history of untreated syphilis An epidemiologic investigation based on a restudy of the Boeck-Bruusgaard material a review and appraisal. J Chron Dis. 1955;2(3):311–344. doi:10.1016/0021-9681(55)90139-9
31. White RM. Unraveling the Tuskegee study of untreated syphilis. Arch Intern Med. 2000;160(5):585–598. doi:10.1001/archinte.160.5.585
32. Hopkins HH. Treatment of neurosyphilis: review of results in six hundred and eighty patients. Arch Intern Med. 1933;52(1):66–75. doi:10.1001/archinte.1933.00160010073007
33. Ryberg B. Bannwarth’s syndrome (lymphocytic meningoradiculitis) in Sweden. Yale J Biol Med. 1984;57(4):499–503.
34. Ryberg B, Nilsson B, Burgdorfer W, Barbour AG. Antibodies to Lyme-disease spirochaete in European lymphocytic meningoradiculitis (Bannwarth’s syndrome). Lancet. 1983;322(8348):519. doi:10.1016/S0140-6736(83)90552-4
35. Sköldenberg B, Gårde A, Carlström A, Stiernstedt G, Kolmodin G, Nord CE. Chronic meningitis caused by a penicillin-sensitive microorganism? Lancet. 1983;322(8341):75–78. doi:10.1016/S0140-6736(83)90061-2
36. Steere AC, Grodzicki RL, Kornblatt AN, et al. The spirochetal etiology of Lyme disease. N Engl J Med. 1983;308(13):733–740. doi:10.1056/NEJM198303313081301
37. Steere AC, Malawista SE, Snydman DR, et al. An epidemic of oligoarticular arthritis in children and adults in three Connecticut communities. Arthrit Rheumat. 1977;20(1):7–17. doi:10.1002/art.1780200102
38. Canale DJ. William Macewen and the treatment of brain abscesses: revisited after one hundred years. J Neurosurg. 1996;84(1):133–142. doi:10.3171/jns.1996.84.1.0133
39. Weeds J. Case of cerebral abscess. Nashville J Med Surg. 1872;9:156–171.
40. Brouwer MC, Coutinho JM, van de Beek D. Clinical characteristics and outcome of brain abscess: systematic review and meta-analysis. Neurology. 2014;82(9):806–813. doi:10.1212/WNL.0000000000000172
41. Khatib U, van de Beek D, Lees JA, Brouwer MC. Adults with suspected central nervous system infection: a prospective study of diagnostic accuracy. J Infect. 2017;74(1):1–9. doi:10.1016/j.jinf.2016.09.007
42. Britton PN, Dale RC, Blyth CC, et al. Causes and clinical features of childhood encephalitis: a multicenter, prospective cohort study. Clin Infect Dis. 2019;70(12):2517–2526. doi:10.1093/cid/ciz685
43. Statistics Denmark website. Available from: https://statbank.dk/statbank5a/default.asp?w=2560.
44. Schmidt M, Schmidt SAJ, Adelborg K, et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol. 2019;11:563–591. doi:10.2147/CLEP.S179083
45. Schmidt M, Pedersen L, Sørensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi:10.1007/s10654-014-9930-3
46. The Danish Board of Health website. Gældende specialeplan - Sundhedsstyrelsen (Danish)[Overall organisation of medical specialties in Denmark]. Available from: https://www.sst.dk/da/viden/specialeplanlaegning/gaeldende-specialeplan.
47. Danish Society of Infections Diseases website. Guidelines og retningslinier (Danish) [Guidelines and recommendations]. Available from: http://www.infmed.dk/guidelines.
48. Venkatesan A, Tunkel AR, Bloch KC, et al. Case definitions, diagnostic algorithms, and priorities in encephalitis: consensus statement of the international encephalitis consortium. Clin Infect Dis. 2013;57(8):1114–1128. doi:10.1093/cid/cit458
49. Jackson AC. Problems With Case Definitions and a Need for Revisions by the International Encephalitis Consortium. Clin Infect Dis. 2015;61(2):293. doi:10.1093/cid/civ313
50. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
51. McMillan T, Wilson L, Ponsford J, Levin H, Teasdale G, Bond M. The Glasgow Outcome Scale — 40 years of application and refinement. Nat Rev Neurol. 2016;12(8):477–485. doi:10.1038/nrneurol.2016.89
52. van de Beek D, Cabellos C, Dzupova O, et al. ESCMID guideline: diagnosis and treatment of acute bacterial meningitis. Clin Microbiol Infec. 2016;22:1–26. doi:10.1016/j.cmi.2016.01.007
53. Bodilsen J, Brouwer MC, Nielsen H, Beek DVD. Anti-infective treatment of brain abscess. Expert Rev Anti Infe. 2018;16(7):565–578. doi:10.1080/14787210.2018.1489722
54. Nau R, Sorgel F, Eiffert H. Penetration of drugs through the blood-cerebrospinal fluid/blood-brain barrier for treatment of central nervous system infections. Clin Microbiol Rev. 2010;23(4):858–883. doi:10.1128/CMR.00007-10
55. Bodilsen J, Mens H, Midgley S, et al. Enterovirus meningitis in adults: a prospective nationwide population-based cohort study. Neurology. 2021;97:e454–e463. doi:10.1212/WNL.0000000000012294
56. Schmidt M, Schmidt SAJ, Sandegaard JL, Ehrenstein V, Pedersen L, Sørensen HT. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. doi:10.2147/CLEP.S91125
57. Trier-Poulsen D. Dokumentation af Labdatabasens Forskertabel [Documentation of the Danish Laboratory Database]. Available from: https://sundhedsdatastyrelsen.dk/da/registre-og-services/om-de-nationale-sundhedsregistre/doedsaarsager-og-biologisk-materiale/laboratoriedatabasen.
58. Kildemoes HW, Sørensen HT, Hallas J. The Danish national prescription registry. Scand J Public Health. 2011;39(7 Suppl):38–41. doi:10.1177/1403494810394717
59. Buch K, Bodilsen J, Knudsen A, et al. Cerebrospinal fluid lactate as a marker to differentiate between community-acquired acute bacterial meningitis and aseptic meningitis/encephalitis in adults: a Danish prospective observational cohort study. Infect Dis Nor. 2018;50(7):1–8.
60. Ørbæk M, Bodilsen J, Gynthersen RMM, et al. CT and MR neuroimaging findings in patients with lyme neuroborreliosis: a national prospective cohort study. J Neurol Sci. 2020;419:117176. doi:10.1016/j.jns.2020.117176
61. Nordberg CL, Bodilsen J, Knudtzen FC, et al. Lyme neuroborreliosis in adults: a nationwide prospective cohort study. Ticks Tick Borne Dis. 2020;11(4):101411. doi:10.1016/j.ttbdis.2020.101411
62. Larsen FTBD, Brandt CT, Klastrup L, et al. Risk factors and prognosis of seizures in adults with community-acquired bacterial meningitis in Denmark: observational cohort studies. BMJ Open. 2019;9(7):e030263. doi:10.1136/bmjopen-2019-030263
63. Vestergaard HH, Larsen L, Brandt C, et al. Normocellular community-acquired bacterial meningitis in adults: a nationwide population-based case series. Ann Emerg Med. 2021;77(1):11–18. doi:10.1016/j.annemergmed.2020.05.041
64. Desmond RA, Accortt NA, Talley L, Villano SA, Soong S-J, Whitley RJ. Enteroviral meningitis: natural history and outcome of pleconaril therapy. Antimicrob Agents Ch. 2006;50(7):2409–2414. doi:10.1128/AAC.00227-06
65. Helweg-Larsen J, Astradsson A, Richhall H, Erdal J, Laursen A, Brennum J. Pyogenic brain abscess, a 15 year survey. Bmc Infect Dis. 2012;12(1):332. doi:10.1186/1471-2334-12-332
66. Campioli CC, Almeida NEC, O’Horo JC, et al. Bacterial brain abscess: an outline for diagnosis and management. Am J Med. 2021. doi:10.1016/j.amjmed.2021.05.027
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.