Back to Journals » Clinical Epidemiology » Volume 14
Existing Data Sources for Clinical Epidemiology: Database of the National Hospital Organization in Japan
Authors Kanazawa N, Tani T, Imai S ![]() , Horiguchi H, Fushimi K, Inoue N
, Horiguchi H, Fushimi K, Inoue N ![]()
Received 24 January 2022
Accepted for publication 2 May 2022
Published 19 May 2022 Volume 2022:14 Pages 689—698
DOI https://doi.org/10.2147/CLEP.S359072
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lars Pedersen
Natsuko Kanazawa,1,* Takuaki Tani,1,* Shinobu Imai,1– 3 Hiromasa Horiguchi,1 Kiyohide Fushimi,1,2 Norihiko Inoue1,2
1Department of Clinical Data Management and Research, Clinical Research Center, National Hospital Organization Headquarters, Tokyo, Japan; 2Department of Health Policy and Informatics, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, Tokyo, Japan; 3Department of Drug Safety and Risk Management, School of Pharmacy, Tokyo University of Pharmacy and Life Sciences, Tokyo, Japan
*These authors contributed equally to this work
Correspondence: Norihiko Inoue, Department of Clinical Data Management and Research, Clinical Research Center, National Hospital Organization Headquarters, 2-5-21 Higashigaoka, Meguroku, Tokyo, 152-8621, Japan, Tel +81-3-5712-5133, Fax +81-3-5712-5088, Email [email protected]
Abstract: This review introduces the National Hospital Organization (NHO) database in Japan. The NHO has maintained two databases through a system of data collection from 140 hospitals in the NHO. National Hospital Organization Clinical Data Archives (NCDA) is collecting clinical information in real time from the electronic medical records since January 2016, and Medical Information Analysis (MIA) databank is collecting daily insurance claims data since April 2010. The NHO database covers more than 8 million patients in 140 hospitals throughout Japan. The database consists of the information of patient profiles, hospital admission and discharge, diagnosis with ICD-10 codes, text data from medical chart, daily health insurance claims such as medical procedures, medications or surgeries, vital signs and laboratory data, and so on. The NHO database includes a wide variety of diseases and settings, including acute, chronic and intractable diseases, emergency medical services, disaster medicine, response to emerging infectious disease outbreaks, medical care according to health policies such as psychiatry, tuberculosis, or muscular dystrophy, and health systems in sparsely populated non-urban areas. Among several common diseases, the database has representativeness in terms of age distribution compared with the Patient Survey 2017 by the Ministry of Health, Labour and Welfare. Interested researchers can contact ([email protected]) the NHO database division to obtain more information about the NHO database for utilization.
Keywords: National Hospital Organization in Japan, real-world data, big data, diagnosis procedure combination, DPC, validation, database, linkage
Introduction
National Hospital Organization
The National Hospital Organization (NHO) has 140 hospitals throughout Japan with approximately 52,000 hospital beds (Figure 1). The NHO provides ordinary acute care and emergency medical services, as well as disaster medicine, response to emerging infectious disease outbreaks, policy medicine such as psychiatry, tuberculosis, and muscular dystrophy, and health systems in sparsely populated non-urban areas. The NHO functions as a core hospital that provides primary to advanced medical care in each region, regardless of whether it is an urban or suburban area. The NHO also covers treatment of intractable diseases that are difficult for private hospitals to make a profit from, thus functioning as a fortress to protect the health of residents in each region.
 |
Figure 1 Distribution of 140 hospitals in the National Hospital Organization all over Japan. The locations of some representative million cities are also indicated on the map. |
National Hospital Organization Clinical Data Archives (NCDA) and Medical Information Analysis (MIA) Data Bank
The NHO headquarters has established and maintained two databases: the first is the National Hospital Organization Clinical Data Archives (NCDA), which collects real-time clinical information from the electronic medical records of NHO hospitals. The information of the NCDA has been collected since January 2016 including information related to clinical settings obtained from the Standardized Structured Medical Record Information Exchanged (SS-MIX) standardized storage.1 The second is the Medical Information Analysis (MIA) data bank, which collects daily insurance claims information. The MIA data bank started in April 2010 and collects insurance claims information, including the payment system by case-mix and diagnosis-related group (DRG) of diagnosis procedure combination/Per-Diem Payment System (DPC/PDPS).2–7 The DPC data in Japan is a dataset that has been diversely used in hundreds of clinical epidemiological studies over a wide range of subjects, such as internal medicine,8–12 surgery,13 emergency medicine,14–16 psychiatry medicine,17 geriatrics,18 and so on. These two databases can seamlessly link patient information and are used not only for clinical epidemiological research, but also for other purposes and analyses such as clinical quality indicators, analysis of hospital care or financial management, and so on. In the case of a COVID-19 pandemic or influenza pandemic, the databases are utilized to provide timely information to the Ministry of Health, Labour and Welfare (MHLW) and the National Institute of Infectious Diseases.19
Data Coverage
In March 2021, the NHO database collects data from 140 hospitals with more than 8 million patients with 10 years of follow-up (Table 1). Data quality checks and database construction are performed by the Information technology department within the NHO. The multicentre, long-term data brings epidemiological relevance for detailed investigation, which is especially important for the study of rare exposures and diseases. Patients with a history of consistent visits to NHO hospitals for more than 1 year have a median follow-up of 4.17 years, and a maximum follow-up of 10 years, allowing for the study of diseases with long latency periods and long-term outcomes. Japan has adopted a universal health insurance system where all Japanese and foreign nationals residing in Japan are mandated to join. This provides equal access to medical care to all citizens regardless of region or income, and the NHO database includes broad range of patients, regardless of their social background.
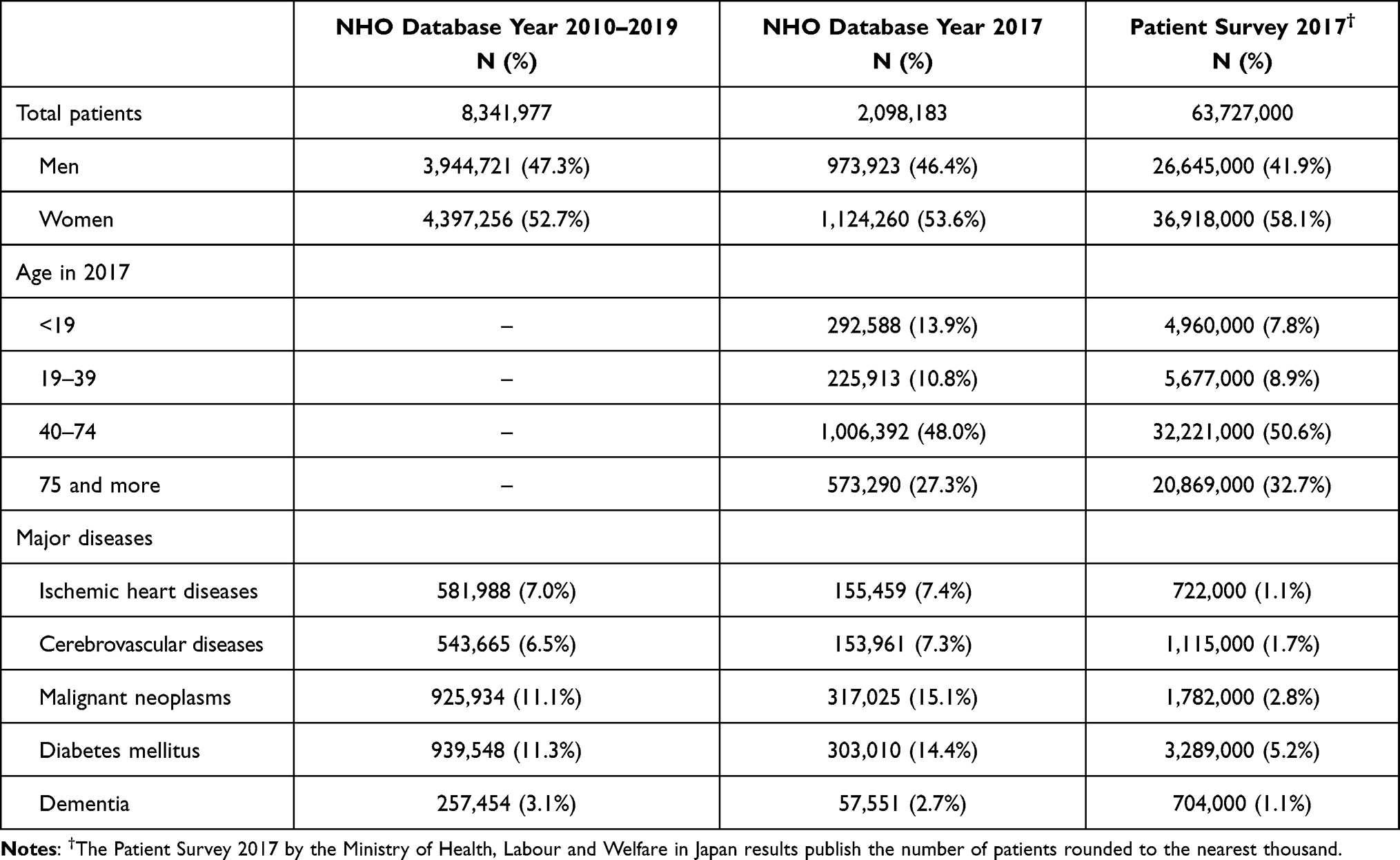 |
Table 1 Patient Demographic in NHO Database |
Data Governance, Practice, and Patient Confidentiality
NHO strives to operate within Japanese laws and guidelines to protect confidentially. To protect patient confidentiality, patient identifiers are securely stored in the security room. Engineers are in charge of extracting the data in the security room, anonymizing the data, and handing it over to the researchers. Researchers cannot access the database directly. These processes ensure the anonymity and security of the information.
Funding Sources of NHO Database
The NHO database is developed and operated by the National Hospital Organization with its own funds.
Ethics for Researches Using NHO Database
For researchers who wish to use and analyze individual patient-level data in the NHO database, research proposals should be submitted to be reviewed by the Institutional Review Board (IRB) in the NHO Headquarters or each hospital. The IRB in the NHO includes external experts and covers a wide range of disciplines, including law, humanities, social sciences, statistics, and medicine, to ensure a multidisciplinary review of ethical validity. Although individual informed consent is not required to conduct the study due to the anonymized data, the research plan will be published on the NHO website and patients will be guaranteed the opportunity to opt out. In addition, the detailed dataset definition regarding the research has to be reviewed by the Review Board for Data Utilization in the NHO Headquarters whether the data content is appropriate according to the study protocol.
Details of NHO Database
Data Types and Contents
The data in the NHO database have insurance claims and clinical information with timestamp, covering many types of facility-level and patient-level characteristics (Table 2): diagnosis, medical procedures, medications, laboratory test, culture test, hospital admission and discharge, severity of diseases, etc. The most significant feature of the NHO database is that information entered on the electronic medical record is collected in real time, allowing for analysis of the latest hospital and patient information.
 |
Table 2 Summary of Data Collected in NHO Database |
The diagnosis and code with the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) and the Japanese claims code are also accompanied by a record of the disease’s start date. The medical procedures defined by the Japanese reimbursement system, such as ICU admission and invasive ventilators, are recorded in the database on a daily basis and the start and end dates, and duration of medical practices can be counted. Especially, laboratory tests and culture tests are also recorded with the timestamp of ordering and performing tests, submitting specimens, running tests, and reports of the results. Patient outcomes include a wealth of information, such as death, length of stay, cost, and discharge destination. The NHO database does not collect the types of data with the intention of specific research purposes, such as self-reported survey data or genotype data.
Data Linkage
The NHO data are available at both the patient and hospital levels, depending on the purpose. Since the patient data are anonymized, data linkage at the patient level with the external database is not possible. However, data linkage at the hospital level is possible, with established linkages to public data such as the Patient Survey and the Survey of Medical Institutions by the Ministry of Health, Labour and Welfare, and demographic statistics. It is also possible to link the location information at the patient or the hospital level, including zip codes and routes, to broad areas on the map that do not identify individual patients.
Frequency of Data Collection
The data is collected from each hospital to the NHO headquarters. Claims information is collected monthly and the electronic medical records in real time via the internal secure network in the NHO. The collected data is built by a specialized information department and made available to researchers.
Data Quality
The NHO has specialized engineers who constantly check the data registration status, and if omissions or delays occur, will contact the hospital personnel and assist the hospital until the data is registered correctly. In addition, since the claims data is submitted to the insurer or the government, the data is checked for errors through an error checking system to ensure there are no input errors.
Data Resource Use
Validation Study
The NHO database is an invaluable source for clinical epidemiology and conducting observational studies. However, as with other hospitals in Japan, the data in the NHO database itself is billing and clinical information obtained from routine practice and is not originally intended for use in clinical research. Classification bias can occur when non-sensitive or unspecific tests, or incorrect variables of diagnostic criteria are used. Therefore, some validation studies for the NHO database have been conducted, and new studies are currently still ongoing. Since the information in the NHO database can link to the medical charts in the NHO hospitals at the patient level, several validation studies were conducted. In the validation study of diagnosis, procedures, and laboratory results in the NHO database with chart reviews, the primary diagnosis had sensitivity of 78.9% and specificity of 93.2%, respectively.20 Imai et al described the validity of detecting previously resolved hepatitis B virus infection in the NHO database with the chart review as the golden standard, with the positive predictive value (PPV) of 85.8%.21 In addition, the validation study of comparison with the procedure-based and the diagnosis-based identifications of severe sepsis and disseminated intravascular coagulation in administrative data was conducted.22 This validation study showed that the procedure-based algorithm is more sensitive than the diagnosis-based algorithm and has the potential to improve the likelihood of disease identification from the NHO database. Most recently, developing regression model-based event detection and validation could identify postsurgical infections from the routinely-collected DPC data in the NHO database on a cut-off score with C-statistic of 0.885, sensitivity of 92% and specificity of 72%, and on another cut-off score with sensitivity of 75% and specificity of 91%.23
Published Works
The NHO database has been used for many other clinical epidemiology studies as well as validation studies: predictors of survival in the elderly after cardiopulmonary resuscitation,24 risk stratification for physical morbidity associated with atypical antipsychotic treatment in Parkinson’s disease,25 activities of daily living after hip fracture surgery in elderly patients with spinal anesthesia,26 and a comparison of walking ability between peripheral nerve block and local infiltration analgesia after knee joint replacement surgery.27
Equalization of Medical Practices
To maintain and improve the quality of daily clinical practices with equality among all 140 hospitals in the NHO, the NHO headquarter is providing the clinical indicators in various processes and outcomes by calculating the clinical indicator’s values from the NHO database based on evidence-based guidelines.28,29 For example, some medical practices such as the proper usage of anticancer drugs or anticoagulation, are based on several evidences and adopted in the guidelines. If the recommendations are not followed in daily clinical practice and the medical treatment is carried out as desired, evidence-based evaluations will not be possible. In that case, even if database records are used in observational studies, it may be difficult to compare them with previously published studies based on the evidence. When the value of the clinical indicator has an outlier, the NHO Headquarters provides supportive information to the hospitals for detecting the reasons.
Strengths and Weaknesses of NHO Database
Strengths
Strengths of the NHO database as a research resource include basic patient attributes and diagnoses, medical practices, detailed laboratory tests and culture tests, and multicentre data collection from 140 hospitals on daily basis.
Breadth of data
As a national hospital, it provides a uniform medical system throughout Japan. The NHO database covers a wide range of diseases, from general diseases to policy medicine, intractable diseases, and rare diseases such as muscular dystrophy, severely multiple handicapped children, intractable neurological diseases, tuberculosis, and AIDS. In addition, electronic medical record information is linked to insurance claim information, which can be used for research on treatment effects and costs. It is one of the few large and continuous databases that can be used for researches at various levels: individual, hospital, regional, and national.
Representativeness and focus of NHO database
In Table 1 and Figure 2, compared with the Patient Survey 2017,30 the NHO database has representativeness in terms of the age proportion, and has focus on the acute care and severe diseases among the five major diseases defined by the Ministry of Health, Labour and Welfare: ischemic heart diseases (ICD-10 code: I20–I25), cerebrovascular diseases (I60–I69), malignant neoplasms (C00–C97), diabetes mellitus (E10–E14), dementia including vascular dementia (F01) and Alzheimer’s disease (F03). The patient number and proportion of the five major diseases stratified by age had very similar patterns of age distribution between the NHO database and the Patient Survey 2017 (Figure 2). However, when comparing the disease distribution, the NHO has a very higher proportion than the Patient Survey in the year 2017 (Table 1): ischemic heart diseases (NHO, 7.4% vs Patient Survey, 1.1%), cerebrovascular diseases (7.3% vs 1.7%), malignant neoplasm (15.1% vs 2.8%), and diabetes mellitus (14.4% vs 5.2%). Since the Patient Survey covered clinics and various types of hospitals throughout Japan, including many minor illnesses that do not require hospitalization, such as the common cold. Comparing proportions of the five major diseases with the Patient Survey shows that the NHO hospitals focus on acute and severe illness. For example, NHO’s percentage of cancer patients is far greater than the patient survey. This is due to the presence of 35 of NHO’s 140 hospitals (including 3 cancer centers) that coordinate cancer care in the region. The NHO also covers medical care for intractable diseases, and covers 68.8% of muscular dystrophy patients (ICD-10 code G710) who visit hospitals and clinics, as estimated from the Patient Survey 2017.30
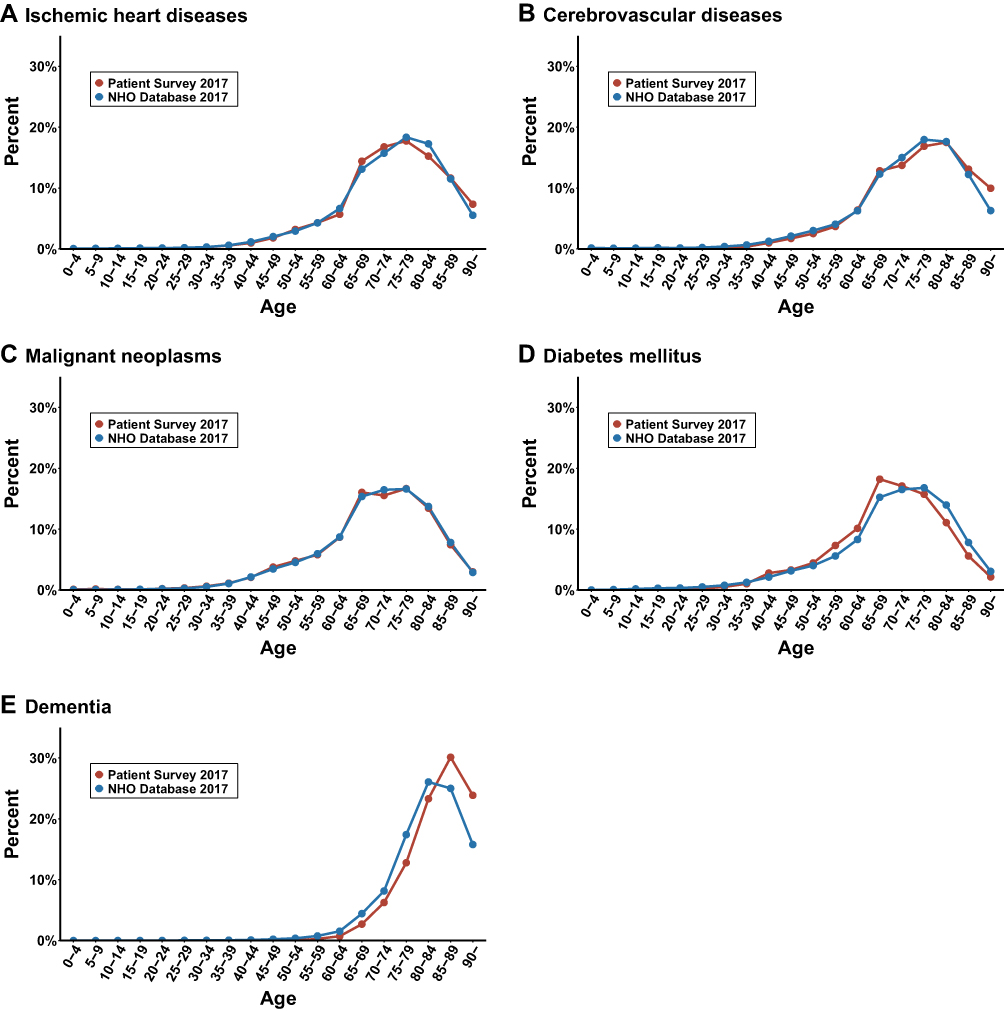 |
Figure 2 Comparison of age distribution of patients between Patient Survey 2017 and NHO database in 2017 among the five major diseases: (A) Ischemic heart diseases, (B) Cerebrovascular diseases, (C) Malignant neoplasms, (D) Diabetes mellitus, (E) Dementia. |
Weaknesses
Missing Data
As for claims data, missing measurements are few because checks are carefully performed for medical fee billings. However, the claims data sometimes contain erroneous entries for clinical information such as patient profiles or patient status. In addition, codes indicating “unknown” are sometimes selected. Our previous validation study showed the validity of diagnoses, procedures, and laboratory data in the NHO database.20 The primary diagnoses in the NHO database had a specificity exceeding 96% and a sensitivity of 78.9%. The 10 common procedures of the NHO database had over 90% in both specificity for nine procedures and sensitivity for six procedures.20 Although the validation study showed 95% of agreement between the NHO database and chart reviews,20 there may be incorrectly entered or omitted vital data. When analyzing data, careful examination of the proportions and patterns of missing values may be necessary to make missing imputation.
Facility-Based Data
The data are created in each hospital. Therefore, the information out of the hospitals are not recorded. Social aspects related to health, such as social support, family structure, use of over-the-counter medications, income, and education level, are not recorded. There are some missing patient groups, such as uninsured patients and those who receive self-pay treatment or uninsured care. However, the proportion of uninsured patients is very small in Japan’s universal health insurance system.
General Issues of EHR and Challenges in NHO
Epidemiological studies using electronic health records (EHRs) data still generally have several weaknesses and overarching challenges, not only in the NHO database: validity of data, representativeness, data availability and interpretation, and missingness.31–33 For example, as noted in the previous section, hospital EHRs do not contain information on medical care provided outside the hospital. As a solution to this problem, based on the “Next Generation Medical Infrastructure Law” (official name “Act on Anonymized Medical Data That Are Meant to Contribute to Research and Development in the Medical Field”) which was legislated in 2018, the project has been initiated to expand the capability of the data resources by the linkage of the EHR data from the NHO database and the clinics across the country held by the Japan Medical Association. This collaboration will enable more consistent analyses of patient data and is expected to contribute to new medical discoveries.
Conclusion
The NHO database accumulates real-world data based on medical care at 140 hospitals across the country, and is used for many clinical studies. In recent years, many diverse medical information data resources exist in Japan that can be used for research.34–37 For example, Biobank Japan, which has collected hundreds of thousands of serum samples and clinical information on diseases, is an example of other large-scale data resources.36,37 Each of these medical information databases has a different focus and layers of granularity, from the societal to the molecular level. In the future, increased collaborations of data resources with different characteristics can be expected to yield new scientific findings, and it is important that their use be accompanied by ethical protections. In Japan, as in many other countries, many issues remain to be resolved in the future, such as laws, social consensus, ethical considerations, procedures, and technology, in order to achieve linkage and utilization of diverse data resources. As these issues will be resolved and data are properly utilized in the future, more diverse scientific outcomes will be achieved, from the individual level, such as tailor-made medicine, to the societal level, such as policy evidence.
Data Resource Access
Access to patient-level data is provided by the NHO for health research purposes and is dependent on the research protocol approved by the NHO’s ethical review committee.
Researchers who desire to use this data must plan their research in accordance with the Ministry of Health, Labour and Welfare’s guidelines for medical research. Careful consideration must be given to the ethics of the research design, protection of patients’ personal information, and access and preservation of data to ensure that patients' rights are protected in conducting research. The NHO can provide collaboration and support for data coding and consultation by the NHO researchers and professional information technicians to ensure that the data is fit for purpose. For more information about applying to use the NHO database, please contact the Database planning division, Information technology department of the NHO by e-mail ([email protected]).
Acknowledgment
We are grateful to Mr. Masaya Nakadera and Mr. Masato Koizumi, the database engineers who prepared the aggregate data. As this paper uses existing aggregate data without directly enrolling subjects, the Ethical Guidelines for Medical and Health Research Involving Human Subjects, established by the Japanese Ministry of Health, Labour and Welfare, Ministry of Education, Culture, Sports, Science and Technology, and Ministry of Economy, Trade and Industry, stipulate that ethical approval and Informed consent are not legally required.
Funding
This review is not funded by a specific project grant.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kimura M, Nakayasu K, Ohshima Y, et al. SS-MIX: a ministry project to promote standardized healthcare information exchange. Methods Inf Med. 2011;50(2):131–139. doi:10.3414/ME10-01-0015
2. Fushimi K, Hashimoto H, Imanaka Y, et al. Functional mapping of hospitals by diagnosis-dominant case-mix analysis. BMC Health Serv Res. 2007;7(1):1–8. doi:10.1186/1472-6963-7-50
3. Hamada H, Sekimoto M, Imanaka Y. Effects of the per diem prospective payment system with DRG-like grouping system (DPC/PDPS) on resource usage and healthcare quality in Japan. Health Policy. 2012;107(2–3):194–201. doi:10.1016/j.healthpol.2012.01.002
4. Hayashida K, Murakami G, Matsuda S, Fushimi K. History and profile of diagnosis procedure combination (DPC): development of a real data collection system for acute inpatient care in Japan. J Epidemiol. 2021;31(1):1–11. doi:10.2188/jea.JE20200288
5. Okamura S, Kobayashi R, Sakamaki T. Case-mix payment in Japanese medical care. Health Policy. 2005;74(3):282–286. doi:10.1016/j.healthpol.2005.01.009
6. Yasunaga H, Matsui H, Horiguchi H, Fushimi K, Matsuda S. Application of the diagnosis procedure combination (DPC) data to clinical studies. J UOEH. 2014;36(3):191–197. doi:10.7888/juoeh.36.191
7. Yasunaga H, Ide H, Imamura T, Ohe K. Impact of the Japanese diagnosis procedure combination-based payment system on cardiovascular medicine-related costs. Int Heart J. 2005;46(5):855–866. doi:10.1536/ihj.46.855
8. Inoue N, Fushimi K. Adjunctive Corticosteroids decreased the risk of mortality of non-HIV pneumocystis pneumonia. Int J Infect Dis. 2019;79:109–115. doi:10.1016/j.ijid.2018.12.001
9. Yamana H, Tsuchiya A, Horiguchi H, et al. Epidemiological study of adult-onset Still’s disease using a Japanese administrative database. Rheumatol Int. 2022;31(4):452–460. doi:10.1007/s00296-016-3546-8
10. Tagami T, Matsui H, Fushimi K, Yasunaga H. Intravenous immunoglobulin and mortality in pneumonia patients with septic shock: an observational nationwide study. Clin Infect Dis. 2015;61(3):385–392. doi:10.1093/cid/civ307
11. Wada T, Yasunaga H, Horiguchi H, et al. Outcomes of Argatroban treatment in patients with atherothrombotic stroke: observational nationwide study in Japan. Stroke. 2016;47(2):471–476. doi:10.1161/STROKEAHA.115.011250
12. Yagi M, Yasunaga H, Matsui H, et al. Impact of rehabilitation on Outcomes in Patients with Ischemic Stroke: a Nationwide Retrospective Cohort Study in Japan. Stroke. 2017;48(3):740–746. doi:10.1161/STROKEAHA.116.015147
13. Shinjo D, Matsumoto K, Terashima K, et al. Volume effect in paediatric brain tumour resection surgery: analysis of data from the Japanese national inpatient database. Eur J Cancer. 2019;109:111–119. doi:10.1016/j.ejca.2018.12.030
14. Imaeda T, Nakada T, Takahashi N, et al. Trends in the incidence and outcome of sepsis using data from a Japanese nationwide medical claims database-The Japan Sepsis Alliance (JaSA) study group-. Crit Care. 2021;25(1):1–9. doi:10.1186/s13054-021-03762-8
15. Sasabuchi Y, Yasunaga H, Matsui H, et al. The volume-outcome relationship in critically ill patients in relation to the ICU-to-hospital bed ratio. Crit Care Med. 2015;43(6):1239–1245. doi:10.1097/CCM.0000000000000943
16. Tagami T, Matsui H, Moroe Y, et al. Antithrombin use and 28-day in-hospital mortality among severe-burn patients: an observational nationwide study. Ann Intensive Care. 2017;7(1):18. doi:10.1186/s13613-017-0244-y
17. Shinjo D, Tachimori H, Maruyama-Sakurai K, Fujimori K, Inoue N, Fushimi K. Consultation-liaison psychiatry in Japan: a nationwide retrospective observational study. BMC Psychiatry. 2021;21(1). doi:10.1186/s12888-021-03241-y
18. Sakata N, Okumura Y, Fushimi K, Nakanishi M, Ogawa A. Dementia and risk of 30-day readmission in older adults after discharge from acute care hospitals. J Am Geriatr Soc. 2018;66(5):871–878. doi:10.1111/jgs.15282
19. Taniguchi K, Mitsushima S, Inoue N, Horiguchi H. Real-time surveillance of COVID-19 using data from the national hospital organization’s electronic medical record network [Japanese]. Available from: https://www.niid.go.jp/niid/ja/diseases/ka/corona-virus/2019-ncov/2488-idsc/iasrnews/10281-495p03.html.
20. Yamana H, Moriwaki M, Horiguchi H, Kodan M, Fushimi K, Yasunaga H. Validity of diagnoses, procedures, and laboratory data in Japanese administrative data. J Epidemiol. 2017;27(10):476–482. doi:10.1016/j.je.2016.09.009
21. Imai S, Yamana H, Inoue N, et al. Validity of administrative database detection of previously resolved hepatitis B virus in Japan. J Med Virol. 2019;91(11):1944–1948. doi:10.1002/jmv.25540
22. Yamana H, Horiguchi H, Fushimi K, Yasunaga H. Comparison of procedure-based and diagnosis-based identifications of severe sepsis and disseminated intravascular coagulation in administrative data. J Epidemiol. 2016;26(10):530–537. doi:10.2188/jea.JE20150286
23. Yamana H, Tsuchiya A, Horiguchi H, et al. Validity of a model using routinely collected data for identifying infections following gastric, colon, and liver cancer surgeries. Pharmacoepidemiol Drug Saf. 2022;31(4):452–460. doi:10.1002/pds.5386
24. Hayashi T, Matsushima M, Bito S, et al. Predictors associated with survival among elderly in-patients who receive cardiopulmonary resuscitation in japan: an observational cohort study. J Gen Intern Med. 2019;34(2):206–210. doi:10.1007/s11606-018-4747-5
25. Iketani R, Imai S, Horiguchi H, Furushima D, Fushimi K, Yamada H. Risk stratification for physical morbidity using factors associated with atypical antipsychotic treatment in Parkinson’s disease: a retrospective observational study using administrative claims data. J Clin Neurosci. 2020;76:189–194. doi:10.1016/j.jocn.2020.04.009
26. Fukuda T, Imai S, Nakadera M, Wagatsuma Y, Horiguchi H. Postoperative daily living activities of geriatric patients administered general or spinal anesthesia for Hip fracture surgery: a retrospective cohort study. J Orthop Surg. 2018;26(1):230949901775410. doi:10.1177/2309499017754106
27. Fukuda T, Imai S, Simoda S, Nakdera M, Horiguchi H. Comparison of peripheral nerve block with local infiltration analgesia regarding walking ability after total knee replacement: a retrospective, propensity-score matched-pair cohort study. J Orthop Surg. 2020;28(2):230949902093165. doi:10.1177/2309499020931656
28. Motohashi T, Kobayashi M, Nakadera M, Kunisawa S, Yuichi I, Fushimi K. Analysis of the calculation definitions for clinical indicators and the calculated values ─Differences between the National Hospital Organization clinical indicators and indicator values at the portal site of healthcare quality indicators. J Japan Soc Healthc Adm. 2015;52(3):139–148. doi:10.11303/JSHA.52.139
29. Kobayashi M, Bito S, Okada C, Fushimi K. Preparation of clinical indicators at the National Hospital Organization and their operation in the future. J Japan Soc Healthc Adm. 2012;49(1):41–50. doi:10.11303/JSHA.49.41
30. Overview of the 2017 patient survey [Japanese]. Available from: https://www.mhlw.go.jp/toukei/saikin/hw/kanja/17/index.html.
31. Gianfrancesco MA, Goldstein ND. A narrative review on the validity of electronic health record-based research in epidemiology. BMC Med Res Methodol. 2021;21(1):234. doi:10.1186/s12874-021-01416-5
32. Schneeweiss S, Avorn J. A review of uses of health care utilization databases for epidemiologic research on therapeutics. J Clin Epidemiol. 2005;58(4):323–337. doi:10.1016/j.jclinepi.2004.10.012
33. Haneuse S, Arterburn D, Daniels MJ. Assessing missing data assumptions in EHR-based studies: a complex and underappreciated task. JAMA Netw Open. 2021;4(2):e210184. doi:10.1001/jamanetworkopen.2021.0184
34. Kuriyama S, Metoki H, Kikuya M, et al. Cohort profile: Tohoku medical Megabank project birth and Three-Generation Cohort Study (TMM BirThree Cohort Study): rationale, progress and perspective. Int J Epidemiol. 2020;49(1):18–19m. doi:10.1093/IJE/DYZ169
35. Takayama J, Tadaka S, Yano K, et al. Construction and integration of three de novo Japanese human genome assemblies toward a population-specific reference. Nat Commun. 2021;12(1):1–14. doi:10.1038/s41467-020-20146-8
36. Hirata M, Nagai A, Kamatani Y, et al. Overview of BioBank Japan follow-up data in 32 diseases. J Epidemiol. 2017;27(3):S22–S28. doi:10.1016/j.je.2016.12.006
37. Sakaue S, Kanai M, Tanigawa Y, et al. A cross-population atlas of genetic associations for 220 human phenotypes. Nat Genet. 2021;53(10):1415–1424. doi:10.1038/s41588-021-00931-x
38. Aujesky D, Auble TE, Yealy DM, et al. Prospective comparison of three validated prediction rules for prognosis in community-acquired pneumonia. Am J Med. 2005;118(4):384–392. doi:10.1016/j.amjmed.2005.01.006
39. Shindo Y, Sato S, Maruyama E, et al. Comparison of severity scoring systems A-DROP and CURB-65 for community-acquired pneumonia. Respirology. 2008;13(5):731–735. doi:10.1111/j.1440-1843.2008.01329.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.