Back to Journals » Psychology Research and Behavior Management » Volume 16
Existential Loneliness Among Older People from the Perspective of Health Care Professionals: A European Multicenter Study
Authors Edberg AK ![]() , Trogu G, Manattini A, Renn-Żurek A
, Trogu G, Manattini A, Renn-Żurek A ![]() , Modrzejewska DM
, Modrzejewska DM ![]() , Woźnicka EB
, Woźnicka EB ![]() , Popovici S, Pintilie L, Beck I
, Popovici S, Pintilie L, Beck I ![]() , Virbalienė A
, Virbalienė A ![]() , Šiurienė A
, Šiurienė A ![]()
Received 14 February 2023
Accepted for publication 28 May 2023
Published 20 June 2023 Volume 2023:16 Pages 2241—2252
DOI https://doi.org/10.2147/PRBM.S408547
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Anna-Karin Edberg,1 Giusy Trogu,2 Alessandra Manattini,2 Agnieszka Renn-Żurek,3 Daria Maria Modrzejewska,3 Elżbieta Barbara Woźnicka,4 Silvia Popovici,5 Liliana Pintilie,6 Ingela Beck,1 Akvilė Virbalienė,7 Aurelija Šiurienė7
1Kristianstad University, Kristianstad, Sweden; 2Anziani e non solo Societá Cooperativa Sociale, Carpi, Italy; 3University of Humanities and Economics, Lodz, Poland; 4Stefan Batory State University, Skierniewice, Poland; 5Asociatia Demetrius, Iasi, Romania; 6Executive Office of the Order of General Nurses, Midwives and Nurses in Romania, Iasi, Romania; 7Klaipeda State University of Applied Sciences, Klaipeda, Lithuania
Correspondence: Anna-Karin Edberg, Faculty of Health Sciences, Kristianstad University, SE 291 88, Kristianstad, Sweden, Tel +46 44-250 39 75, Email [email protected]
Introduction: Health care professionals (HCPs) encounter different forms of loneliness in their work. It is essential that they have the courage, skills, and tools to deal with loneliness, in particular with existential loneliness (EL) which relates to meaning in life and the fundamentals of living and dying.
Aim: The aim of this study was to investigate HCPs’ views on loneliness among older people and their understanding, perception, and professional experience of EL in older people.
Materials and Methods: In all, 139 HCPs from five European countries participated in audio-recorded focus group and individual interviews. The transcribed materials were locally analyzed using a predefined template. The participating countries’ results were then translated, merged, and inductively analyzed using conventional content analysis.
Results: Participants described different forms of loneliness – a negative form that is unwanted and causes suffering, and a positive form where solitude is desired and sought. The results showed that the HCPs’ knowledge and understanding of EL varied. The HCPs mainly related EL to different types of loss, eg loss of autonomy, independence, hope, and faith, and to concern alienation, guilt, regret and remorse, and concerns about the future.
Discussion and Conclusions: The HCPs expressed a need to improve their sensitivity and self-confidence to engage in existential conversations. They also stated the need to increase their knowledge and understanding of aging, death, and dying. Based on these results, a training program aimed to increase knowledge and understanding of older people’s situation has been developed. The program includes practical training in conversations about emotional and existential aspects, based on recurrent reflections on the topics presented. The program is available at: www.aloneproject.eu.
Keywords: older people, health care professionals, existential loneliness, qualitative, multicenter study
A Letter to the Editor has been published for this article.
A Response to Letter by Mr Priastana has been published for this article.
Introduction
Loneliness is a universal experience, which has been shown to have a detrimental effect on older people’s health.1 Everyone, regardless of age, gender, or cultural or socioeconomic factors, experiences loneliness in their lifetime. Rokach states that it is an experience that cannot be avoided, but also, that we are able to cope with loneliness and possibly reduce its frequency in our lives.2 Peplau and Perlman define loneliness as an unpleasant experience that occurs when a person’s network of social relationships is significantly deficient in either quality or quantity.3 They highlight that loneliness is a subjective experience, not synonymous with objective social isolation.3 A conceptual review based on qualitative studies about loneliness identified three types of distinct, but overlapping, conceptualizations of loneliness: social, emotional, and existential loneliness.4 The conceptualization of social loneliness has been described as an “objective” condition, framed by numbers of social connections being experienced as a sense of disconnection with others. The majority (70%) of the included studies have focused on social loneliness. The common theme in the conceptualization of emotional loneliness is the connection with social isolation and a loss or lack of good quality relationships.4 The third and less commonly described type of loneliness is existential loneliness (EL). In contrast to the other two types, EL has been defined, not only as the absence of meaningful relationships, but as the condition of being fundamentally separated from others and the wider world.
Existential loneliness has been described to relate to aspects of meaning and hope5 and the awareness of being vulnerable and mortal as a human being.6,7 It has historically been described from a philosophical point of view, mainly by existentialists with a focus on questions of human existence and the meaning of life.8–13 However, the concept of EL also has a broad empirical significance, as it is often reinforced when people are left on their own in threatening situations, such as during severe illness.14 Earlier literature reviews and concept analyses on the topic, by Ettema et al,14 Boston et al,15 and Bolmsjö et al,16 describe EL as a feeling of being ultimately alone in our own reflective consciousness, and separated and disconnected from others and the world. They proposed that this condition seems to be linked to aspects of spirituality, which notion is supported by the findings of Mansfield et al.4 Bolmsjö et al define EL as the
Immediate awareness of being fundamentally separated from other people and from the universe, and typically, because of this awareness, experiencing negative feelings, that is, moods and emotions. (p 1321)16
In a recent study conducted in retirement communities in the UK and Australia, the loss of close attachments, lack of physical touch and intimacy, and deterioration of health and body was reported to contribute to the experience of EL.17 Studies from Sweden focusing on frail older people showed that being met with indifference by health care professionals (HCPs) enhanced the negative feeling of EL. On the other hand, being acknowledged by others, being the focus of others’ concern, and having a meaningful exchange of thoughts and feelings eased the negative feeling of EL.18,19 The way HCPs encounter existential needs and EL among older people therefore has a significant impact.
However, HCPs find it challenging to encounter EL in older people in their care.20 Studies on municipal care and services for older people show that communicating about dying and death, as well as encountering older people’s existential needs, is experienced as difficult, and is something that health care staff try to avoid.21 Even HCPs in palliative care, who are trained to take care of patients in different crises, have described how they experienced a loss of protection against their own unwanted thoughts and feelings related to death, meaning that they themselves became vulnerable and therefore felt less prepared to handle their patients’ existential suffering.22
It is, however, important to remember that the prerequisites for handling the challenges that HCPs experience differ between different care contexts.23 For example, Wolf et al describe that pace, light, sound, and the direction of care are important factors affecting the possibilities for staff to adjust to older people’s needs and find space for individual conversations.24 It can also be a challenge for staff in task-oriented care environments to shift focus from being task-oriented to being relation-oriented, ie “having to focus on doing rather than being”.21,25 As existential needs are often expressed in a subtle way26 and older people themselves experience a lack of emotional language through which to express EL,17 there is a risk that the staff do not even detect or recognize EL among the people in their care.
Older people often choose to talk to HCPs instead of burdening someone in their social network when something feels too emotional.27 There is therefore a need to develop supportive interventions for HCPs to learn to detect and recognize EL among older people and to support them in facing loneliness, and particularly EL. There is, further, a need for increased knowledge and awareness among HCPs about different forms of loneliness, with specific focus on EL. As most of the empirical research concerning EL among older people originates from Scandinavia, it seems important to widen and deepen the knowledge about HCPs’ experience of encountering EL to develop cross-cultural support from a European perspective. Health care professionals’ views on loneliness among older people and their understanding, perception, and professional experience of EL among older people are an important basis for tailoring such a support program.
Aim
The aim of this study was to investigate HCPs’ views on loneliness among older people and their understanding, perception, and professional experience of EL in older people.
Research Questions
- What is HCPs’ knowledge and experience of EL among older people?
- How do HCPs identify with, and encounter, EL among older people?
- What are the challenges of encountering EL, and what feelings are evoked in HCPs?
- What support do HCPs receive and what support would they like to receive? What skills would they like to develop?
Materials and Methods
This study is part of the “Innovative Health Professionals Training Program on Existential Loneliness among Older People”, the “ALONE project”. The overall aim of the ALONE project is to develop a cross-cultural support program for HCPs in detecting and recognizing EL among older people and in supporting these people in facing loneliness in general, and EL in particular.
The present study is a multicenter study with a qualitative research design, based on focus group interviews with HCPs in Sweden, Poland, Romania, and Lithuania, and, because of pandemic restrictions, individual interviews in Italy. The interviews focused on HCPs’ views of challenges and limitations in the encounter with EL in their work, underlining their educational and support needs and the skills needed to deal with EL among older people.
Participants
In all, 139 professionals from the five included countries participated in interviews. The sample mainly consisted of registered nurses (n=71), nurse assistants (n=22), and social workers (n=25), but other HCPs (n=21) were also represented. The majority were women (91%) aged between 26 and 70 years (mean 50 years), with work experience in health care and/or social work ranging from 1.7 years to 43 years (mean 19 years). For a detailed description of the sample, see Table 1.
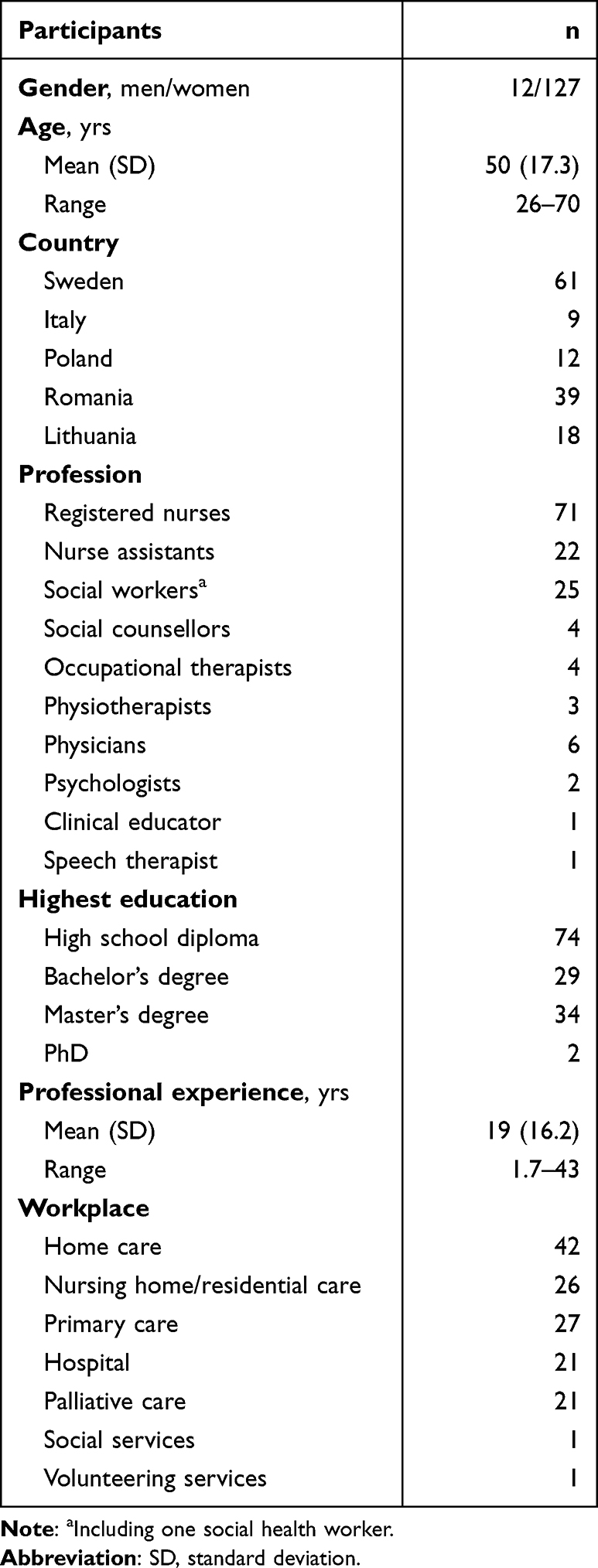 |
Table 1 Demographic Data on Participants (n=139) |
Data Collection and Procedure
Data was collected in 18 focus group interviews, eleven of which were conducted in Sweden, two in Poland, three in Romania, and two in Lithuania. Nine individual interviews were conducted in Italy. Data collection took place during 2020, except in Sweden where data was collected in 2015–2016 and published in the original format in 2018 and 2019.20,23 After permission from the care manager, an information letter describing the aim of the study was provided to HCPs in different contexts (see Table 1), highlighting that (1) participation was voluntary; (2) they could withdraw their participation at any time without giving a reason; (3) their data would be treated with confidentiality; and (4) the results would be published with no possibility to identify individual participants. Health care staff who were interested in participating signed an informed consent, and a time and place for the interviews was set.
Interviews
The main part of the interviews was conducted using focus group discussion. In focus group discussions, the discussion between the participants is the focus of interest, rather than individual participants’ views. Discussions in a focus group therefore rely on group processes and encourage interaction between group members, resulting in deeper exploration of the topic under discussion. Focus groups, through focused discussions, allow the researchers to study the topic of interest in depth, involving a group of people selected based on the study’s aim.28
The focus group discussion was led by a moderator. An observer took notes. A description of the professional background of the moderators and observers in each country is presented in Table 2. To strengthen trustworthiness, all interviews followed the same interview guide (Table 3), which was inspired by Sundström et al,20 with some minor adjustments to accommodate cultural differences. The final version of the guide was agreed by the researchers.
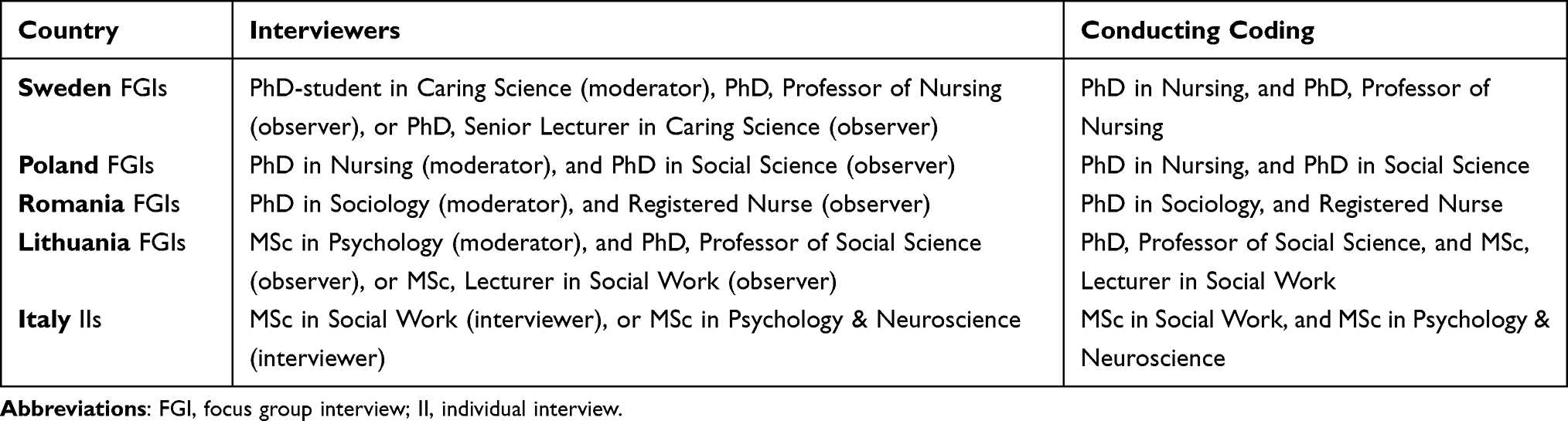 |
Table 2 Professional Background of Interviewers in Individual and Focus Group Interviews, and of Those Conducting the Coding in Each Country |
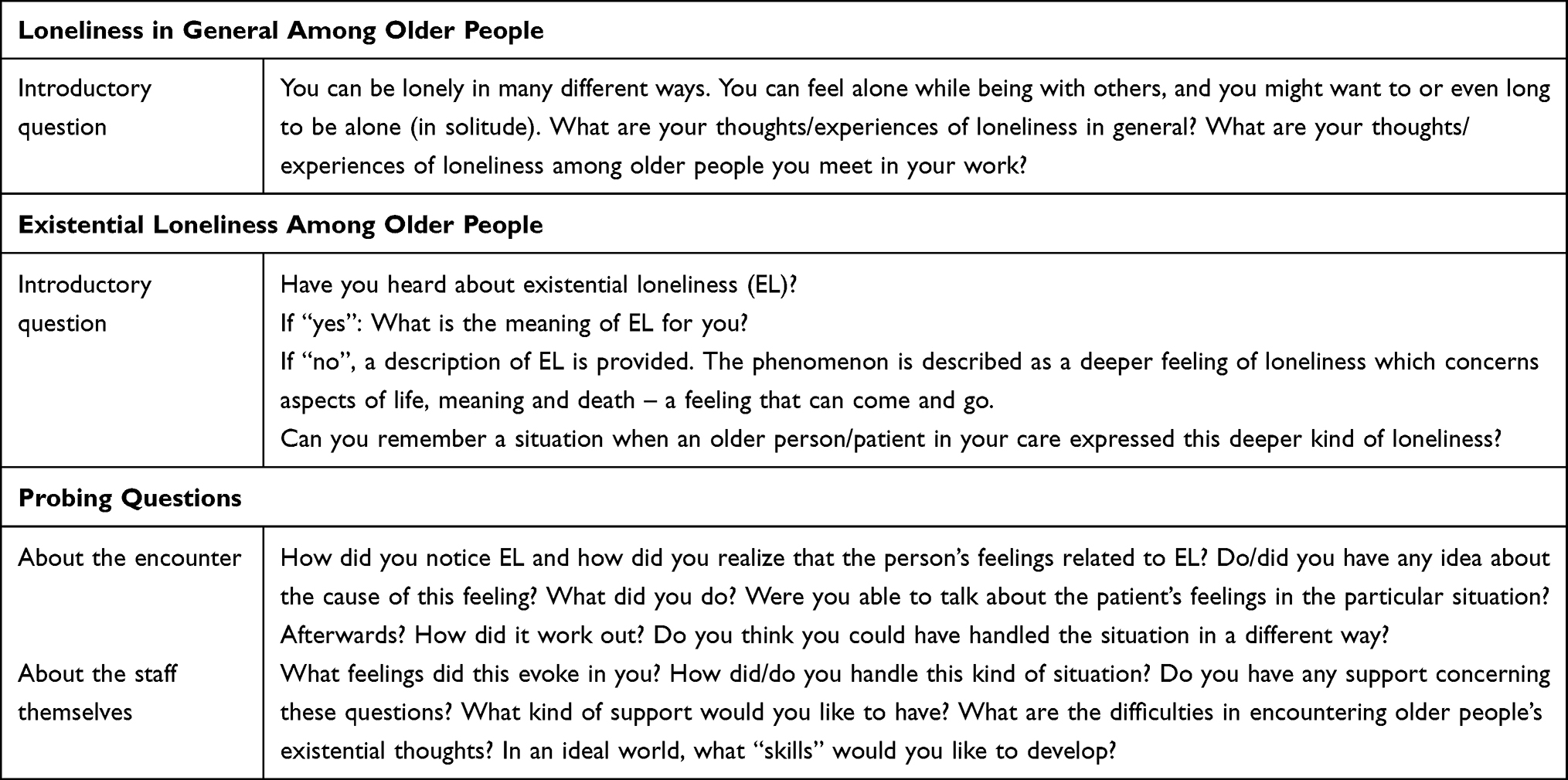 |
Table 3 Interview Guide Used in the Focus Group and Individual Interviews |
After an introduction of the group and the interview format, participants were assured that participation was voluntary and were made aware of their right to withdraw from the interviews at any time. Thereafter, all interviews were initiated with a general question about loneliness. After an initial discussion about loneliness in general, the concept of EL was introduced. To deepen the discussion, predefined follow-up and probing questions were asked (see Table 3). The individual interviews followed the same structure. All interviews were performed in the native language of the participants, lasted between 45 and 97 minutes, and were audio-recorded and transcribed verbatim.
Analysis
At first, all participating countries analyzed their data in line with a jointly developed template for analysis (Table 4). To strengthen confirmability, the coding of the text was done by two persons in each country, following the same structure. The transcripts were read and coded individually, and thereafter, the two persons compared and discussed their coding until they reached agreement. The professional background of the people who made the analysis in each country is presented in Table 2. The results were then translated into English. The results from each country can be found in a report by Trogu et al.29
 |
Table 4 Template for Analysis of the Results |
The five sets of results were then used as a basis for the analysis in this study, meaning that all countries contributed equally to the results. At first, the results concerning loneliness in general among older people were analyzed using conventional inductive content analysis. The text was coded line by line; thereafter, codes with similar content were grouped and labeled.30 The same procedure was then applied to the results concerning EL. The text was grouped and condensed in accordance with the analysis template agreed in advance (see Table 4). All authors critically reviewed the preliminary results and after discussion, some adjustments were made.
Results
Loneliness in General
Health care professionals’ general view of loneliness was that there are different forms of loneliness – a negative form that is unwanted and causes suffering, and a positive form where solitude is desired and sought, as an intimate need. But the HCPs also mentioned the risk of interpreting withdrawal as a wish for solitude when in fact it could be a sign of depression or anxiety. An additional form of loneliness was also described, loneliness when facing death – an experience no one else can share.
The experience of loneliness was described as individual and as differing between people. The HCPs emphasized the importance of listening to individual wishes and needs. In most interviews, loneliness was described as existing irrespective of whether other people are present or not, and the HCPs emphasized that involving more people or initiating activities is therefore not a solution. One HCP said, “If you cannot share your deeper thoughts, you are still alone”, pointing to the importance of having someone who the older people could confide in – not just anyone. Participating HCPs at two of the sites, however, expressed the view that loneliness mainly has to do with how many people are around and also with lack of activities. Nursing home placement was described by these HCPs as the best means to reduce loneliness.
Health care professionals at all sites mentioned loss as a main reason for loneliness. Loss could mean the loss of a partner, children, or friends, resulting in the older person being alone. The HCPs perceived that this contributed to a sense of emptiness, an empty space that could not be filled by someone or something else. As women live longer than men, they were described as lonelier compared with men. The HCPs also mentioned loss of identity, where the older persons lost connection with their history and values or saw themselves as useless as they could no longer do the activities they used to do. Alternatively, they feared illness, helplessness, or death, which made them feel vulnerable. The loss of identity could also have to do with the absence of recovery after tragic events and an inability to maintain relationships. There could also be loss of cognitive functioning, for example in people with dementia who might feel unfamiliar with an environment they did not recognize or who forgot that someone had just visited them. In addition, the HCPs mentioned the loneliness older partners can feel when the person they married is changing into “someone else” because of disease.
Loneliness was perceived by the HCPs to also be related to physical limitations due to loss of abilities such as speech, hearing, and vision, which contributed to the feeling of not being understood and not being able to express one’s thoughts and feelings. But there were also examples of older people suffering from the impact of reduced strength or the inability to walk longer distances, meaning they were cut off from the outside world unless there was public transportation available.
… But this I perceive as loneliness. His wife didn’t understand him, we didn’t understand him, and he didn’t understand himself either. And it is about life and death then ... and he ... he was all into that now and he had regrets. (Focus group, Sweden)
The HCPs’ narrations also mentioned stigma and changing traditions. The HCPs talked about the difficult situation older people faced when their children migrated to larger cities or abroad. Traditionally, children care for their parents until death, and older people’s loneliness was considered a stigma as in some of the participating countries the cultural family norm is multigenerational. The younger generation’s technology skills were also described to deepen the gap between generations, inducing loneliness among the older generation. The HCPs also mentioned the shame of talking about loneliness as society expects people to have a network of family and friends. The HCPs at some interview sites highlighted the importance of religion in reducing loneliness in persons who believe that God looks after and protects people. Other views on the same theme were that older people who work and are active all the time do not experience loneliness: They continue to work, resign themselves to dying, and in this way reach a better afterlife.
Most older persons do not feel lonely. They have old traditions and these practices are very important … the residents of care homes long for religious practices, such as reciting the rosary or singing the litany in local communities. (Focus group, Lithuania)
I observe that older people who pray a lot, [and] spend time in the chapel, don’t complain about loneliness. They say they fill the emptiness with prayer. (Focus group, Poland)
Alcohol abuse was mentioned as another reason for loneliness, mainly in two of the countries. The HCPs described that alcohol was sometimes used by older people in an attempt to reduce loneliness, but also that alcohol consumption led to loneliness as friends and family turned away. Alcohol abuse among children was also mentioned as a reason for older people’s loneliness as it could lead to the children neglecting their parents’ needs. At one site, alcohol abuse was mentioned as a reason for nursing home placement as the family were no longer able to take care of the older person.
Existential Loneliness
Understanding Existential Loneliness
The understanding of EL varied between HCPs from different countries. In Sweden, all participating HCPs had heard of EL, and in Italy, most of the HCPs had. By contrast, in Poland and Lithuania, only some of the HCPs had heard of it, while in Romania none of the HCPs had heard of EL but all were very interested to learn more. However, after the concept of EL was explained, most HCPs recognized it in older people they had met, even if at the time they had not known that it was EL. The HCPs reflected on the meaning of EL and described it as a deep and pervasive sensation that you can experience even when you are surrounded by other people, like living in a world of your own. The HCPs described that it has to do with existence, the meaning of life and a loss of the meaning of life, and the reminder that we are all human and we are all mortal. One participant from Italy said,
… like an unbridgeable void that at some point does not allow you to stay here and now, and that prevents you from feeling life so that you can just fly over it in a detached way.
The HCPs discussed possible causes of EL, such as loss (of loved ones and friends, of autonomy and independence, of physical contact, of personal roles, and of hope and faith), changes in personal life (retirement, health, economy, nursing home placement), drawing conclusions about one’s life (guilt, regrets, remorse), and concerns about the future (fear of own or loved ones’ death and fear of not having the time to complete important life goals), as well as ageism and alienation (exclusion, lack of societal recognition, feeling invisible and forgotten, not being needed, being left behind). The interviews also revealed the view that many older people had grown up in poverty, and had tried to satisfy material needs as adults; now in old age they realized that they had not dealt with their spiritual needs, and that this was related to EL. Overall, the HCPs agreed that there are no common causes of EL as it is possible to experience EL for many different reasons.
Experiences of Existential Loneliness
The HCPs discussed that some older persons expressed their needs clearly, but most of the time the HCPs felt that EL, though present, was not mentioned. Then they recognized EL in an older person’s frequent pleas for attention, or in other vague signs of anxiety and sadness, or in other behaviors such as when the older person became more silent or apathetic and withdrew from human contact.
To support an older person to open up and talk about EL, it is important, according to the HCPs, to show that you are available, and that you have dedicated time for talking; that you are not afraid, and that you are willing to face the person’s emotions. While HCPs in some countries provided a long list of actions that could be taken to reduce EL, others emphasized the importance of listening to the older person talk about their thoughts and needs. Based on this, actions could be taken.
I think it’s more that you don’t … that you don’t have a template and “These are my values” and “My moral ideas and my values about loneliness” and then … no … but I’ll just have to go outside this comfort zone and start to think beyond it. (Focus group, Sweden)
Encountering EL can, however, make an HCP feel insecure. The HCPs described that they felt inadequate, powerless, and sad, and they experienced sorrow and pain, but also compassion and empathy. Some HCPs expressed that EL among people in their care evoked personal experiences of loneliness and made them reflect on their own self and personal story. The HCPs all agreed that it was difficult to meet older people who experienced EL. They felt insecure when they tried to interpret and understand what the older person was communicating. They described feelings of reluctance to meet the older person’s demands and needs, sometimes perceiving the older person as demanding; often they felt insecure about how to break through the older person’s shield. Some experienced fear and difficulties in encountering existential issues. Because of this, it could happen that the HCPs did not encourage older persons to reflect on their feelings and experiences, or, lacking specific knowledge or tools, tried to steer away from existential conversations as they felt uncomfortable with them. Rather than talk, they improvised strategies to “fix” a situation that could not be fixed. Some of the HCPs wished that they were better equipped for such situations, so that it would feel more natural to talk about existential issues. They described their limited ability to support older people in existential matters. But there was also the view that EL was a private experience and, therefore, that such conversations should be avoided.
I don’t feel comfortable talking to seniors about their loneliness. Mostly I just ask if anyone is coming to visit? How do they feel? And if no one visits our clients I only try to cheer them up that the family is probably busy, they don’t have any time, but someone will come soon. (Focus group, Poland)
What I do is try to contact other professionals from other services so that we can assess the situation together and decide how to move forward. I seek extra support because I recognize that I wouldn’t be able to do it alone. (Individual interview, Italy)
Support Needs and Skills Needed to Encounter Existential Loneliness
As with the experience of EL, the HCPs’ experience of training and support varied between the different countries and contexts. Some of the HCPs from Italy and those who worked in palliative care in Sweden had experience of clinical supervision and organized meetings for reflection on practice. Health care professionals in Poland, Lithuania, and Romania had no such experience, and neither did HCPs working in home care, nursing homes, or hospitals in Sweden. The HCPs reflected on the importance of prioritizing conversations about EL and talking about death and dying before it was too late. They expressed that they would probably have handled some situations in the past differently if they had had access to emotional and practical support. Such support could have enabled them to encourage older people to open up about their thoughts and feelings about EL and existential issues, and to prioritize these conversations to the same level as other tasks.
I sometimes feel a little remorse and [these] thoughts remain when I feel I have lost control. I first ask myself whether I was able to achieve what I’m supposed to be doing. (Individual interview, Italy)
It’s not enough just to talk about loneliness, but [we] also [need] to help the older person to overcome it. I can’t do it. I don’t know how to help the person to cope with it. I can only organize time for them, but I can’t conduct in-depth, psychological, or pedagogical conversations with them. (Focus group, Poland)
The HCPs also expressed the need for textbooks and continuous professional development courses to help them understand and communicate better. They mentioned the need to focus more on caring for older people in general, and on loneliness and EL in particular. This need included: theoretical knowledge as well as clinical practice in different areas; a holistic view of human existence; a new (non-medical) approach; theoretical insight into human strengths; and non-verbal communication skills that needed to be improved.
In social work studies, we learned to find problems and work with them, but no one talked about human strengths. Therefore, the spiritual, existential needs of people were not a priority. (Focus group, Lithuania)
I’m not able to talk about loneliness and death with older people. We are not taught [about how to do that] at university. Psychological knowledge isn’t enough. We should have workshops on such skills. (Focus group, Poland)
The skills that were needed to improve the encounter with older people experiencing EL were described to include personal attributes of the HCPs, such as empathy, compassion, understanding, sensitivity, and the courage to engage in existential conversations; knowledge and understanding, such as a deeper understanding of gerontology and geriatrics, death and dying, and the ability to identify EL and give support. Skills such as psychological and religious/spiritual counseling skills, providing consolation to patients who are close to death, managing emotions, being able to listen and create trustful relations, and stimulating conversation by talking about the past, the present, and the future were also highlighted. In addition, it was seen as important to have good self-knowledge, but also to understand the older person’s situation. In the encounter, it was important to show humanity and respect, to have a non-judgmental attitude, and to be curious, thus getting to know the older person and paying attention to their non-verbal communication.
Discussion
The results provided a broad, cross-cultural understanding of HCPs’ experience of different forms of loneliness. Although many HCPs were not familiar with the term “EL”, once the concept was explained to them, they realized that in the course of their work as professionals they often encountered older people experiencing EL. Although the study did not aim to make comparisons between the interview sites, we noted that there were differences in understanding between HCPs from the different countries. Therefore, the social and cultural context seems to be of importance. Chung et al investigated the experience of EL among older people in Sweden and Hong Kong and found that older people in the two locations had similar experiences of EL.31 In both places, EL was related to loss of control, not being understood, isolation, and not being able to find meaning in life. There were, however, some differences between the two locations. Older people in Sweden focused more on their individual needs, while older people in Hong Kong to a greater extent used their family as a reference.31 The study indicates, in line with previous research, that Western culture emphasizes the autonomy of individuals, while Eastern culture emphasizes the importance of family, which also seems to be reflected in the experience of EL. Circumstances related to family were also emphasized in a study from Sri Lanka reporting that the experience of loneliness was enhanced by feeling abandoned by the family and worries about the future.32 The study showed that the suffering of older people could be relieved by keeping in close contact with the family and engaging in common activities, but also by practicing religion. Although all interview sites in our study were European, there were country differences based on culture and religion. For example, changes in traditions, which were diminishing the importance of the family, were emphasized at some sites and less so at others. Moreover, the way in which religion was described, both as a reason for EL and as a way to alleviate EL, differed between countries. The role of religion was not clearly expressed at interview sites in more secular societies. Education and support to increase knowledge and understanding of EL among HCPs must, therefore, be context-specific and allow space for reflections taking the participants’ cultural and individual experiences as a starting point.
The HCPs’ ability to support older people in existential matters was limited. The results showed that the HCPs wished that they were better prepared for such situations. However, the view that talking about EL should be avoided as it was too private was also expressed. This is in line with results from an ethnographic study in a Swedish nursing home context with focus on nurse assistants’ experiences of conversations with the residents about death and dying.33 The results showed that the conversations about death and dying appeared to be emotionally difficult for the HCPs and that they tried to redirect the residents’ attention to something else. Similar results have previously been reported by Beck et al.21 Our results show that the skills needed to encounter EL relate to personal attributes, knowledge, and understanding, as well as spiritual/religious reflection. Knowledge and understanding concerned general knowledge about aging, but also specific knowledge about loneliness and EL, while skills in spiritual/religious matters embraced being able to listen and create trustful relations; finally, personal attributes involved, eg sensitivity and the courage to engage in existential conversations. Bullington et al argue that there is a need for increased awareness as conversations are often automated, ie our listening is shaped by our preconceptions.34 There is therefore a risk that we do not hear what the other person is saying, and therefore are unable to deepen the conversation. This awareness seems essential for being able to stay focused on patients’ and their relatives’ narratives, allowing them to reflect upon, and better understand, their current situation. Therefore, education in combination with practical training in conversation seems to be a key element in tailoring a training program for HCPs caring for older people. This is supported by researchers such as Katajavuori et al stating that, for an educational intervention to be effective, theoretical knowledge should be combined with practical training and reflection.35
The development of a training program seems of utmost urgency as HCPs worldwide encounter loneliness in its different forms among older people, a situation that became evident during the COVID-19 pandemic. In an extraordinary situation of forced isolation, the importance of recognizing, and dealing with, EL among older people has highlighted the need for HCPs to have the power to act.
Methodological Considerations
In qualitative research, aspects of trustworthiness should be considered.36 Trustworthiness includes aspects of credibility, dependability, confirmability, and transferability, rather than internal validity, reliability, objectivity, and external validity/generalizability, which are focused in quantitative research.37 The main methodological concern in this study is the trustworthiness of the data collected. The aim of this study was to investigate HCPs’ views on loneliness among older people, and their understanding, perception, and professional experience of EL among older people as a basis for tailoring a support program that could function in a European context. To strengthen credibility, groups from five countries took part in this study. As the original data material was in the countries’ national language, several steps had to be taken to reduce the risk of inconsistent data and to strengthen confirmability.37 Firstly, the same, detailed, and translated interview guide was used at all sites. The guide had previously been tested and it had been used in the Swedish part of the study, with only minor contextual adjustments having to be made. Secondly, the same template for analysis was used at all interview sites. Thereafter, the results were translated into English. Thirdly, the results from each site were discussed at regular meetings. They were thereafter processed by the Italian partners, but keeping the results from each site intact. Fourthly, the analysis of this study was based on the processed results from each site, where the co-authors representing the five country partners had regular input in the cross-cultural results, which ensured that the results from no site had a disproportionate influence on the overall results. For dependability, the interview guide and the template for analysis are presented in the manuscript.37
The transferability of the results, ie the possibility to transfer the results to a different European context, is one of the main strengths of this study, as the sites represent a variety of different societies with different health care systems, and with different prioritization of family, religion, and socio-economic values, as well as political orientation. Also, the focus groups included different professionals, which has also strengthened transferability of the findings across HCPs.
Relevant parts of the Consolidated Criteria for Reporting Qualitative Research (COREQ) have been applied when presenting this study.38
Conclusion
This study shows that HCPs have a need to improve their sensitivity and self-confidence to engage in existential conversations. They also need to increase their knowledge and understanding of aging, death, and dying. The results of this study have provided a solid basis for developing the content and format of a training program supporting HCPs to encounter EL. We have found evidence that the training program should include elements to increase knowledge and understanding of older people’s situation based on a person-centered approach. Such an approach needs to take older persons’ perspectives into account, and address preconceptions about older people (eg ageism) as well as develop an understanding of spirituality and what it can mean for different people.
We also found evidence that knowledge about different forms of loneliness, and EL in particular, is important. To increase their self-confidence when encountering older people’s EL, HCPs need more knowledge and practical training in the art of listening and conversations about emotional and existential aspects. The training program should be built on the cornerstones of education, practical training, and critical reflection. Based on the findings in this study, a training program has been developed. It is free to use and available in six languages at: www.aloneproject.eu.
Abbreviations
EL, existential loneliness; HCP, health care professional.
Data Sharing Statement
Original data will not be shared for reasons of confidentiality.
Ethics Approval and Informed Consent
The study was conducted in line with the Helsinki Declaration. The voluntariness of participation was emphasized, as were confidentiality and the risks, burden, and benefits of the research. All participants provided written informed consent prior to participation. Study approval by the national ethics boards in the respective countries was applied for and obtained where required in terms of national legislation. As the interviews neither targeted vulnerable groups nor collected personal details, ethical permission was not required in Italy, Romania, Poland, or Lithuania. The interviews in Sweden were part of a larger study; therefore, ethical approval was applied for and granted by the Lund Ethical Review Board (ref 2014/652).
Consent for Publication
No images or videos are included in the paper.
Acknowledgments
We are most grateful to the health care professionals who participated in this study, for taking the time and generously sharing their experiences. We are also grateful to Malin Sundström, Kerstin Blomqvist, and Margareta Rämgård for collecting data in Sweden, and to Ina Valeckienė for collecting data in Lithuania. We also wish to thank Proper English for revising the language.
Author Contributions
The study was designed in collaboration between the five participating sites. The first author had the main responsibility for the cross-cultural analysis of the results and the drafting of the paper. All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, or analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work has been funded by the European Union under the Erasmus+ Programme as part of the project “Innovative Health Professionals Training Program on Existential Loneliness among Older People”, ALONE (project No. 2019-1-PL01-KA202-064933). The European Commission support for the production of this publication does not constitute an endorsement of the contents, which reflect the views only of the authors, and the Commission cannot be held responsible for any use which may be made of the information contained herein.
Disclosure
The authors have no competing interests to declare for this work.
References
1. Courtin E, Knapp M. Social isolation, loneliness and health in old age: a scoping review. Health Soc Care Commun. 2017;25(3):799–812. doi:10.1111/hsc.12311
2. Rokach A. Effective coping with loneliness: a review. Open J Depress. 2018;7(4):61–72. doi:10.4236/ojd.2018.74005
3. Peplau A, Perlman D. Loneliness: A Sourcebook of Current Theory, Research and Therapy. New York: Wiley; 1982.
4. Mansfield L, Victor C, Meads C, et al. A conceptual review of loneliness in adults: qualitative evidence synthesis. Int J Environ Res Public Health. 2021;18(21):11522. doi:10.3390/ijerph182111522
5. Yalom ID. Existential Psychotherapy. New York: Basic Books; 1980.
6. Mijuskovic B. (1980) Loneliness and suicide. J Soc Phil. 1980;11(1):11–17. doi:10.1111/j.1467-9833.1980.tb00610.x
7. Carter MA. Abiding loneliness: an existential perspective on loneliness. Second Opinion. 2000;3:37–54.
8. Frankl VE. Man’s Search for Meaning. London: Hodder & Stoughton; 1946.
9. Heidegger M. Being and Time. London: The Camelot Press; 1962.
10. Buber M. I and Thou. Edinburgh: T & T Clark; 1958.
11. Sartre JP. Being and Nothingness: An Essay on Phenomenological Ontology. London: Routhledge; 1956.
12. Kierkegaard S. The Concept of Anxiety. Princeton NJ: Princeton University Press; 1946.
13. Merleau Ponty M. The Visible and Invisible. Followed by Working Notes. Evanston: Northwestern University Press; 1968.
14. Ettema EJ, Derksen LD, van Leeuwen E. Existential loneliness and end of life care: a systematic review. Theor Med Bioethics. 2010;31(2):141–169. doi:10.1007/s11017-010-9141-1
15. Boston P, Bruce A, Schreiber R. Existential suffering in the palliative care setting: an integrated literature review. J Pain Symptom Manage. 2011;41(3):604–618. doi:10.1016/j.jpainsymman.2010.05.010
16. Bolmsjö I, Tengland B-O, Rämgård M. Existential loneliness: an attempt at an analysis of the concept and the phenomenon. Nurs Ethics. 2019;26(5):1310–1325. doi:10.1177/0969733017748480
17. Carr S, Fang C. A gradual separation from the world: a qualitative exploration of existential loneliness in old age. Age Soc. 2023;43(6):1436–1456. doi:10.1017/S0144686X21001252
18. Sjöberg M, Beck I, Rasmussen BH, Edberg A-K. Being disconnected from life: meanings of existential loneliness as narrated by frail older people. Aging Ment Health. 2018;22(10):1357–1364. doi:10.1080/13607863.2017.1348481
19. Sjöberg M, Edberg A-K, Rasmussen BH, Beck I. Being acknowledged by others and bracketing negative thoughts and feelings: frail older people’s narrations of how existential loneliness is eased. Int J Older People Nurs. 2019;14(1):e12213. doi:10.1111/opn.12213
20. Sundström M, Edberg AK, Rämgård M, Blomqvist K. Encountering existential loneliness among older people: perspectives of health care professionals. Int J Qual Stud Health Well-Being. 2018;13(1):1474673. doi:10.1080/17482631.2018.1474673
21. Beck I, Törnquist A, Broström L, Edberg A-K. Having to focus on doing rather than being—Nurse assistants’ experience of palliative care in municipal residential care settings. Int J Nurs Stud. 2012;49(4):455–464. doi:10.1016/j.ijnurstu.2011.10.016
22. Rämgård M, Neiminen Kristoffersson T. Låt Inte Spindelväven Växa I Ditt Hjärta. En Forskningscirkel Om Poesins Verkan För Sjuksköterskor I Palliativ Vård [Don’t Let the Spider Web Grow in Your Heart. A Research Circle About the Effect of Poetry on Registered Nurses in Palliative Care]. Malmö: Kommunförbundet; 2010. Swedish.
23. Sundström M, Blomqvist K, Edberg AK, Rämgård M. The context of care matters: older people’s existential loneliness from the perspective of healthcare professionals - A multiple case study. Int J Older People Nurs. 2019;14(3):e12234. doi:10.1111/opn.12234
24. Wolf A, Ekman I, Dellenborg L. Everyday practices at the medical ward: a 16-month ethnographic field study. BMC Health Serv Res. 2012;12:184. doi:10.1186/1472-6963-12-184
25. Udo C, Danielsson E, Melin-Johansson C. Existential issues among nurses in surgical care – a hermeneutical study of critical incidents. J Adv Nurs. 2013;69(3):569–577. doi:10.1111/j.1365-2648.2012.06032.x
26. Sundler AJ, Eide H, van Dulmen S, Holmström IK. Communicative challenges in the home care of older persons - A qualitative exploration. J Adv Nurs. 2016;72(10):2435–2444. doi:10.1111/jan.12996
27. Norell Pejner M, Ziegert K, Kihlgren A. Older patients in Sweden and their experience of the emotional support received from the registered nurse – a grounded theory study. Aging Ment Health. 2015;19(1):79–85. doi:10.1080/13607863.2014.917605
28. Bowling A. Research Methods in Health: Investigating Health and Health Services.
29. Trogu G, Manattini A, Renn-Żurek A, et al. Limitations in Caring for Older Persons Related to Existential Loneliness Encountered by Healthcare Professionals. The European Commission; 2020.
30. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
31. Chung BP, Olofsson J, Wong FK, Rämgård M. Overcoming existential loneliness: a cross-cultural study. BMC Geriatr. 2020;20(1):347. doi:10.1186/s12877-020-01753-y
32. Wijesiri M, Samarasinghe K, Edberg A-K. Loneliness among older people living in care homes in Sri Lanka. Int J Older People Nurs. 2019;14(4):e12253. doi:10.1111/opn.12253
33. Alftberg Å, Ahlström G, Nilsen P, et al. Conversations about death and dying with older people: an ethnographic study in nursing homes. Healthcare. 2018;6(2):63. doi:10.3390/healthcare6020063
34. Bullington J, Söderlund M, Sparén EB, Kneck Å, Omérov P, Cronqvist Å. Communication skills in nursing: a phenomenologically-based communication training approach. Nurs Edu Pract. 2019;39:136–141. doi:10.1016/j.nepr.2019.08.011
35. Katajavuori N, Lindblom-Ylänne S, Hirvonen J. The significance of practical training in linking theoretical studies with practice. Higher Educ. 2006;51(3):439–464. doi:10.1007/s10734-004-6391-8
36. Lincoln YS, Guba EG. Naturalistic Inquiry. Newbury Park, CA: SAGE; 1985.
37. Shenton AK. Strategies for ensuring trustworthiness in qualitative research projects. Educ Inform. 2004;22:63–75. doi:10.3233/EFI-2004-22201
38. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.