Back to Journals » Patient Preference and Adherence » Volume 17
Exercise Self-Efficacy and Fatigue as Predictors of Adherence to Home-Based Exercise Among Patients with Multiple Sclerosis
Authors Almarwani M ![]() , Alosaimi B
, Alosaimi B
Received 29 March 2023
Accepted for publication 6 June 2023
Published 15 June 2023 Volume 2023:17 Pages 1441—1449
DOI https://doi.org/10.2147/PPA.S414884
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Maha Almarwani,1 Bashaier Alosaimi1,2
1Rehabilitation Sciences Department, College of Applied Medical Sciences, King Saud University, Riyadh, Kingdom of Saudi Arabia; 2Physical Therapy Department, Ministry of Health, Riyadh, Kingdom of Saudi Arabia
Correspondence: Maha Almarwani, Rehabilitation Sciences Department, College of Applied Medical Sciences, King Saud University, Riyadh, 11433, Kingdom of Saudi Arabia, Tel +966 118058400, Email [email protected]
Background: Adherence to home-based exercise programs can be improved by determining the factors associated with exercise adoption and maintenance in patients with multiple sclerosis. However, the factors that influence adherence to home-based exercise have been poorly studied among patients with multiple sclerosis in Saudi Arabia. This study aimed to examine predictors of adherence to home-based exercise programs among patients with multiple sclerosis in Saudi Arabia.
Methods: This was a cross-sectional observational study. A total of forty individuals (mean age = 38.65 ± 8.16 years) diagnosed with multiple sclerosis participated in the study. Outcome measures were self-reported exercise adherence, the Arabic version of exercise self-efficacy, the Arabic version of patient-determined disease steps, and the Arabic version of the fatigue severity scale. All outcome measures were assessed at baseline, except for self-reported adherence to exercise, which was measured after 2 weeks.
Results: Our results showed that the adherence to home-based exercise programs was significantly positively correlated with exercise self-efficacy and negatively correlated with fatigue and disability. Exercise self-efficacy (β = 0.62, p < 0.01) and fatigue (β = − 0.24, p = 0.04) were significant predictors of adherence to home-based exercise programs.
Conclusion: These findings suggest that exercise self-efficacy and fatigue should be considered by physical therapists when designing a tailored exercise program for patients with multiple sclerosis. This may facilitate greater adherence to the home-based exercise programs and improve functional outcomes.
Keywords: adherence, exercise self-efficacy, fatigue, home-based exercise, multiple sclerosis
Introduction
Multiple sclerosis (MS) is a common neurological condition. MS was estimated to affect 36 per 100,000 of the global population by 2020.1 The prevalence of MS is also increasing in Saudi Arabia, where it affects 40.4 per 100,000 of the population. In Saudi Arabia, MS is more common in females than males, which is similar to its global prevalence.2 Physical disability, depression, fatigue, loss of balance, and falls are common among patients with MS and affect their quality of life.3,4
Physical therapy is frequently used alongside medication for managing patients with MS.5,6 Due to the progressive nature of MS and the decline in activity levels, patients commonly require long-term exercise interventions. Many studies suggest that physical therapy exercise can be beneficial for the physical, cognitive, and psychological functions of patients with MS.7–10 Home-based exercise programs can help patients with MS overcome barriers to long-term exercise in clinics, such as lack of time, distance, transportation, disability, and high costs.6
The effectiveness of home-based exercise programs for patients with MS depends on adherence to exercise.6,11 However, patients with MS have poor adherence to long-term home-based exercise programs.6 Some studies found barriers to poor adherence to exercise among patients with MS, such as disability, fatigue, and low self-efficacy levels.11–13 Studies have shown that nonadherence to home-based exercise programs is associated with negative functional outcomes, increased healthcare costs, and low exercise self-efficacy.6,11,14–16
Self-efficacy is essential for effective self-management and can be used to improve physical and psychological health outcomes in patients with MS.16 Despite the importance of exercise self-efficacy in adherence to home-based exercise programs, few studies have been conducted globally to examine the association between exercise self-efficacy and adherence to home-based exercise programs among patients with MS. Exercise self-efficacy is the belief in one’s ability to exercise. The adoption and maintenance of exercise have been linked to self-efficacy.17 Previous studies found a positive association between exercise self-efficacy and physical activity.13,18–22 Another study found that fatigue and pain self-efficacy play an important role in MS treatment.18 A high self-efficacy level may result in higher goal setting and adherence to that goal, whereas a low self-efficacy level may result in the opposite.12,23,24 Patients with MS who have high levels of exercise self-efficacy adhere more to exercise programs and have a higher quality of life than those with low levels of exercise self-efficacy.12,25,26 The positive association between adherence to exercise and exercise self-efficacy could reciprocally influence each other.
Adherence to home-based exercise programs can be improved by determining the factors associated with exercise adoption and maintenance in patients with multiple sclerosis. However, these factors have been poorly studied among Saudi patients with multiple sclerosis. Therefore, the purpose of this study was to examine predictors of adherence to home-based exercise programs among patients with multiple sclerosis in Saudi Arabia.
Materials and Methods
Study Design and Setting
An observational cross-sectional study was conducted in outpatient physical therapy MS clinics at King Saud Medical City and King Salman Social Center in Riyadh, Saudi Arabia. This study was conducted in accordance with the Declaration of Helsinki and approved by the College of Medicine Institutional Review Board at King Saud University, Riyadh, Saudi Arabia (E-21-6491). All participants provided informed consent prior to participation.
Participants
A sample of forty Saudi patients with MS were recruited to participate in the study. The participants were clinically diagnosed with MS, aged 18 years or older, and participated in home-based exercise programs prescribed by certified physical therapists. The study excluded participants who experienced a recent MS relapse in the last 30 days, had comorbidities that would prevent them from participating in home-based exercise programs, such as other neurological, orthopedic, and cardiopulmonary conditions, or had a cognitive impairment with a score < 24 on the mini-mental state examination. We targeted a sample size of forty patients with MS based on a power analysis using G*Power (v.3.1.9.7) The statistical test conducted on G-Power was the correlation bivariate normal test with a power of 95%, a one-tailed alpha level of 5%, and a moderate correlation between outcome measures (r =0.50) were assumed.27
Home-Based Exercise Programs
All participants received home-based exercise programs prescribed by their physical therapists. The home-based exercise program was designed to improve muscle strength, flexibility, balance, and endurance. The program included strengthening exercises at moderate intensity for the upper extremity, lower extremity, and core muscles, including arm elevation with dumbbells, leg abduction with an elastic exercise band, and abdominal crunches using body weight. Stretching exercises included biceps stretches, hamstring stretches, and ankle rotations. Standing balance exercises included straight-line walking with as little assistance as possible. Aerobic exercise at moderate intensity included walking for ten minutes. The recommended frequency of the exercise sets was three times per week with a set of 8–10 repetitions for 45 minutes. The participant had 2–5 minutes of rest between sets. The intervention was based upon an exercise training guideline for patients with multiple sclerosis.26
Outcome Measures
Self-Reported Exercise Adherence
The adherence rate was defined as a percentage of the total number of exercises completed compared with the number of prescribed exercises.28 To complete the self-reported adherence, all participants obtained an exercise diary, as well as adequate instructions on how to fill it out. The participants were asked to report their adherence to home-based exercise programs for two weeks. To calculate the adherence rate, the total number of completed exercises for each participant in each session (ranging from 0–8 exercises) was divided by the total number of prescribed exercises. For determining the adherence rate, we used data from the exercise diary. In the exercise diary, a high percentage of exercise reported indicated a high adherence rate to home-based exercise programs.
The Arabic Version of Exercise Self-Efficacy (ESE-A)
The level of exercise self-efficacy was evaluated at baseline by the Arabic version of exercise self-efficacy (Cronbach’s α =0.89).29 It is a valid and reliable self-reported outcome measure for determining the level of exercise self-efficacy in patients with MS. The scale consists of 18 items that measure exercise self-efficacy in various situations, with responses ranging from “0” (can’t do exercise) to “100” (certainly can). The total scores for exercise self-efficacy were calculated as the sum of all scale items, then divided by the total number of items. A higher score indicated a higher level of confidence in performing the exercise.30
The Arabic Version of Patient-Determined Disease Steps (PDDS-A)
The disability severity was measured at baseline and assessed by the Arabic version of patient determined disease steps.31 It is a valid and reliable self-reported outcome measure for determining the severity of disability in patients with MS. It consists of nine ordinal levels, ranging from the lowest “0” (normal level of disability severity) to the highest “8” (severe level of disability).32
The Arabic Version of the Fatigue Severity Scale (FSS-Ar)
The severity of fatigue symptoms was measured at baseline and assessed by the Arabic version of the fatigue severity scale (Cronbach’s α =0.84). It is a valid and reliable self-reported outcome measure for determining fatigue severity among Arabic-speaking patients with MS.33 This scale measures the severity of fatigue symptoms based on their impact on motivation, exercise, physical function, and daily activities among patients with MS. This scale consists of nine items, with responses ranging from “1” (strong disagreement) to “7” (strong agreement). The total score ranges from 0 to 63, with a total score of 36 or more indicating that the individual was fatigued.34
Statistical Analysis
Data were analyzed using SPSS version 25 (IBM, Armonk, NY). The appropriate descriptive statistics were used to summarize the characteristics of participants and the outcome measures for the study. The Mann–Whitney U-test was used to compare the outcome measures between the female and male. A Pearson correlation coefficient was used to examine correlations between variables. Multiple linear regression was used to assess the independent association between adherence to home-based exercise programs and the characteristics of participants and study outcome measures. We only included variables that demonstrated bivariate associations with adherence to home-based exercise programs. This model was developed using stepwise model selection methods and variables in model with the highest R-square kept as the most parsimonious model. We did not include additional covariates considering that only 2–3 variables should be included in a model with our small sample size. Multicollinearity was checked by calculating tolerance and variance inflation factors in the regression model. The results indicate no problems of multicollinearity. Statistical significance was set a priori at two-sided p < 0.05.
Results
Characteristics of Study Participants
In total, 40 patients with MS participated in this study, with a mean (SD) age of 38.65 ± 8.16 years. More than half of the participants (57%) were female, and 90% received social support. Most of the participants were clinically diagnosed with relapsing-remitting MS (87.5%), and the average MS duration was 11.19 ± 6.99 years. Referring to their history of falls, 65% reported no falls in the past 30 days (Table 1).
 |
Table 1 Characteristics of Study Participants (N= 40) |
Descriptions of Outcome Measure
The exercise self-efficacy score was 40.13 (SD =24.67). The patient-determined disease steps score was 4.32 (SD =1.83). The fatigue severity scale score was 4.06 (SD = 1.58). The adherence to the home-based exercise program measured after two weeks was 54.81 (SD = 28.12) (Table 2).
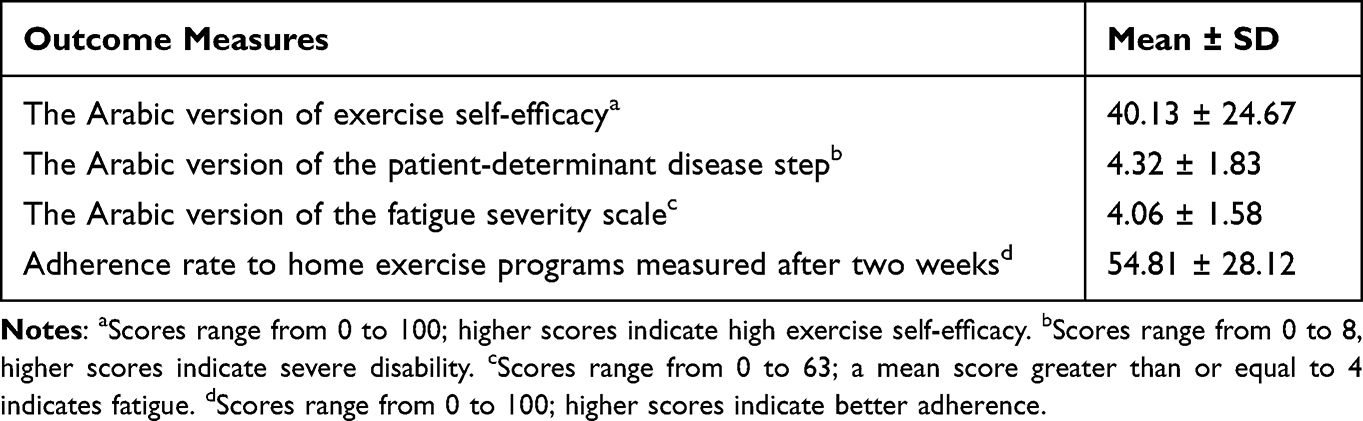 |
Table 2 Description of the Outcome Measures |
There were no significant differences between female and male in the mean scores of the study outcome measures—exercise self-efficacy, fatigue, physical disability, and adherence to home-based exercise programs (Table 3).
 |
Table 3 The Difference Between Females and Males in the Study Outcome Measures |
Correlations Between the Studied Variables
Adherence to home-based exercise programs was significantly positively correlated with exercise self-efficacy (r = 0.71 and p < 0.01), and negatively correlated with the fatigue severity scale (r = −0.47 and p < 0.01), and disability (r = −0.65 and p < 0.01). No statistically significant associations were found between adherence to home-based exercise programs and age, gender, education, job, marital status, social support, body mass index, onset and type of MS, depression, and history of falls (Table 4).
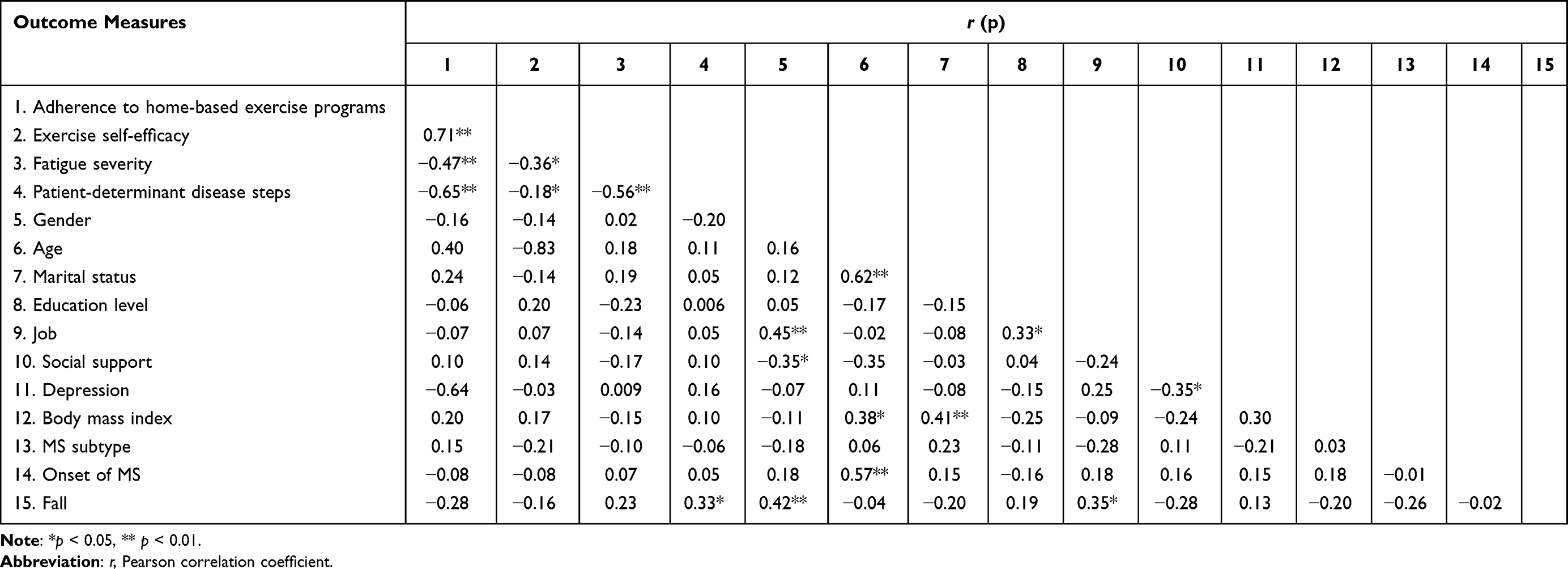 |
Table 4 Correlation of Study Outcome Measures and Characteristics of Participants |
Predictors of Adherence to Home-Based Exercise Programs
The result of the regression model for predictors of adherence to home-based exercise programs was significant (F = 23.5, p < 0.01). The significant predictors of adherence to home-based exercise programs were the exercise self-efficacy scale (β = 0.62, p < 0.01), and fatigue severity scale (β = −0.24, p = 0.04) were all together and independently associated with adherence to home-based exercise programs, with all variables demonstrating about 53% of variability in adherence to home-based exercise programs (Table 5).
 |
Table 5 Stepwise Multiple Linear Regression Model for Predictors of Adherence to Home-Based Exercise Program |
Discussion
To our knowledge, this is the first study to examine predictors of adherence to home-based exercise programs among patients with multiple sclerosis in Saudi Arabia. The results showed a low level of adherence to home-based exercise programs among the participants. Exercise self-efficacy and fatigue were significant predictors of adherence to home-based exercise programs. These results are in line with the social cognitive theory.11,35 This theory proposes that the greater an individual’s perception of their capability, the higher the goals they set for themselves and the more firmly they adhere to accomplishing them.36,37 Self-efficacy is a key component of social cognition.4,37 Exercise self-efficacy in patients with MS is affected by various experiences, including previous participation in similar exercises, observing a similar individual complete an exercise, physical therapist reinforcement, verbal and visual feedback, fatigue and symptom severity.3,38
In addition, adherence to home-based exercise programs was significantly positively correlated with exercise self-efficacy and negatively correlated with fatigue and disability. Previous studies have shown that patients with MS who have low exercise self-efficacy have low motivation to be physically active and improve their health.39–41 These findings were also consistent with social cognitive theory, which suggests that exercise behavior and personal factors, such as cognitive, affective, and physiological events, could reciprocally influence each other.15,19,35
Physical therapy exercises based on the social-cognitive theory that implement positive behavioral change strategies such as goal setting, self-motivation, intention to exercise, positive reinforcement, previous successful exercise adherence, and social support may assist in increasing individuals’ self-efficacy.11,25,30,42 A high level of exercise self-efficacy may help improve adherence to home-based exercise programs, symptoms including fatigue, and health-related quality of life in patients with MS.3,6,42,43 A randomized controlled trial showed that including exercise self-efficacy in the intervention of patients with MS resulted in 90% of the participants feeling confident they would adhere to exercise after completing their supervised exercise programs.44
A previous study that applied a group counseling approach to help individuals interact with peers during the intervention phase revealed that group counseling impacts individuals’ self-efficacy, which helps maintain the behaviors required to sustain outcomes and improve function in patients with MS.45 Patients were most likely to adhere to their home-based exercise programs when they performed the exercises under the supervision of physical therapists.11,14 Moreover, remote online supervision by physical therapists may help patients with MS improve their adherence to home-based exercise programs. A study by Donkers et al that implemented online supervision such as telerehabilitation showed an increase in adherence to home-based exercise programs, especially in patients with severe symptoms.39
Some potential limitations of this study should be acknowledged. First, we measure adherence to exercise for a short period of time with small sample size. Future studies with a larger sample size are recommended to evaluate long-term adherence to home-based exercise programs among patients with MS. Second, our cross-sectional study did not allow casual inferences to be drawn between self-reported adherence to home-based exercise program, exercise self-efficacy and fatigue. Future studies are needed to investigate the effectiveness of an exercise self-efficacy and fatigue intervention, including a control group on adherence to home-based exercise programs. Information on the Expanded Disability Status Scale (EDSS), the MS-specific measure of disability was not available in this study. Response bias to the exercise diary may confound results; however, previous studies with self-reported data from patients with MS have shown a high level of validity.46,47 Finally, no valid Arabic outcome measure to assess adherence to exercise is available in the literature. Consequently, this study used self-reported adherence to the exercise diary, which has been used in previous studies.
Conclusion
Exercise self-efficacy and fatigue were significant predictors of adherence to home-based exercise programs among patients with MS in Saudi Arabia. Our findings suggest exercise self-efficacy and fatigue should be considered by physical therapists when designing a tailored exercise program for MS patients. This may facilitate greater adherence to the home-based exercise program and improve functional outcomes.
Acknowledgments
This work was supported by the Research Center of the Female Scientific and Medical Colleges, Deanship of Scientific Research, King Saud University, Riyadh, Saudi Arabia. The authors would like to acknowledge the SAED MS Organization for helping with the data collection.
Disclosure
The authors report no conflict of interest in this work.
References
1. Walton C, King R, Rechtman L, et al. Rising prevalence of multiple sclerosis worldwide: insights from the Atlas of MS. Multi Scler J. 2020;26:1816–1821. doi:10.1177/1352458520970841
2. AlJumah M, Bunyan R, Al Otaibi H, et al. Rising prevalence of multiple sclerosis in Saudi Arabia, a descriptive study. BMC Neurol. 2020;20:1–7. doi:10.1186/s12883-020-1629-3
3. Guicciardi M, Carta M, Pau M, Cocco E. The relationships between physical activity, self-efficacy, and quality of life in people with multiple sclerosis. Behav Sci. 2019;9:121. doi:10.3390/bs9120121
4. Motl RW, Pekmezi D, Wingo BC. Promotion of physical activity and exercise in multiple sclerosis: importance of behavioral science and theory. Mult Scler J Exp Transl Clin. 2018;4:2055217318786745.
5. Motl RW, Sandroff BM, Kwakkel G, et al. Exercise in patients with multiple sclerosis. Lancet Neurol. 2017;16:848–856. doi:10.1016/S1474-4422(17)30281-8
6. Ghahfarrokhi MM, Banitalebi E, Negaresh R, Motl RW. Home-based exercise training in multiple sclerosis: a systematic review with implications for future research. Mult Scler Relat Disord. 2021;55:103177. doi:10.1016/j.msard.2021.103177
7. Rietberg MB, Brooks D, Uitdehaag BM, Kwakkel G. Exercise therapy for multiple sclerosis. Cochrane Database Syst Rev. 2005;1:1.
8. Halabchi F, Alizadeh Z, Sahraian MA, Abolhasani M. Exercise prescription for patients with multiple sclerosis; potential benefits and practical recommendations. BMC Neurol. 2017;17:1–11. doi:10.1186/s12883-017-0960-9
9. White LJ, Dressendorfer RH. Exercise and multiple sclerosis. Sports Med. 2004;34:1077–1100. doi:10.2165/00007256-200434150-00005
10. Kalron A, Zeilig G. Efficacy of exercise intervention programs on cognition in people suffering from multiple sclerosis, stroke and Parkinson’s disease: a systematic review and meta-analysis of current evidence. NeuroRehabilitation. 2015;37:273–289. doi:10.3233/NRE-151260
11. Essery R, Geraghty AWA, Kirby S, Yardley L. Predictors of adherence to home-based physical therapies: a systematic review. Disabil Rehabil. 2017;39:519–534. doi:10.3109/09638288.2016.1153160
12. McAuley E, Motl RW, Morris KS, et al. Enhancing physical activity adherence and well-being in multiple sclerosis: a randomised controlled trial. Multi Scler J. 2007;13:652–659. doi:10.1177/1352458506072188
13. Motl RW, McAuley E, Wynn D, Sandroff B, Suh Y. Physical activity, self-efficacy, and health-related quality of life in persons with multiple sclerosis: analysis of associations between individual-level changes over one year. Qual Life Res. 2013;22:253–261. doi:10.1007/s11136-012-0149-z
14. Kramer A, Dettmers C, Gruber M. Exergaming with additional postural demands improves balance and gait in patients with multiple sclerosis as much as conventional balance training and leads to high adherence to home-based balance training. Arch Phys Med Rehabil. 2014;95:1803–1809. doi:10.1016/j.apmr.2014.04.020
15. Anens E, Zetterberg L, Urell C, Emtner M, Hellström K. Self-reported physical activity correlates in Swedish adults with multiple sclerosis: a cross-sectional study. BMC Neurol. 2017;17(1):1–7. doi:10.1186/s12883-017-0981-4
16. Casey B, Uszynski M, Hayes S, Motl R, Gallagher S, Coote S. Do multiple sclerosis symptoms moderate the relationship between self-efficacy and physical activity in people with multiple sclerosis? Rehabil Psychol. 2018;63:104. doi:10.1037/rep0000190
17. Fletcher JS, Banasik JL. Exercise self-efficacy. Clin Excell Nurse Pract. 2001;5:134–143. doi:10.1054/xc.2001.24203
18. Theofilou P, Giannouli V, Kolias S, Tsolaki M. Perception of pain self-efficacy and fatigue in Greek patients with multiple sclerosis: a study protocol. Health Psychol Res. 2015;3:1. doi:10.4081/hpr.2015.1556
19. Motl RW, Snook EM, McAuley E, Gliottoni RC. Symptoms, self‐efficacy, and physical activity among individuals with multiple sclerosis. Res Nurs Health. 2006;29:597–606. doi:10.1002/nur.20161
20. Motl RW, McAuley E, Snook EM. Physical activity and quality of life in multiple sclerosis: possible roles of social support, self-efficacy, and functional limitations. Rehabil Psychol. 2007;52:143. doi:10.1037/0090-5550.52.2.143
21. Motl RW, Snook EM. Physical activity, self-efficacy, and quality of life in multiple sclerosis. Ann Behav Med. 2008;35:111–115. doi:10.1007/s12160-007-9006-7
22. Morris KS, McAuley E, Motl RW. Self-efficacy and environmental correlates of physical activity among older women and women with multiple sclerosis. Health Educ Res. 2008;23:744–752. doi:10.1093/her/cym067
23. Picha KJ, Valier AS, Heebner NR, et al. Physical therapists’ assessment of patient self-efficacy for home exercise programs. Int J Sports Phys Ther. 2021;16:184. doi:10.26603/001c.18957
24. Brown SA. Measuring perceived benefits and perceived barriers for physical activity. Am J Health Behav. 2005;29:107–116. doi:10.5993/AJHB.29.2.2
25. Adamson BC, Learmonth YC, Kinnett-Hopkins D, Bohri M, Motl RW. Feasibility study design and methods for project GEMS: guidelines for exercise in multiple sclerosis. Contemp Clin Trials. 2016;47:32–39. doi:10.1016/j.cct.2015.12.002
26. Kim Y, Lai B, Mehta T, et al. Exercise training guidelines for multiple sclerosis, stroke, and Parkinson’s disease: rapid review and synthesis. Am J Phys Med Rehabil. 2019;98:613. doi:10.1097/PHM.0000000000001174
27. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41:1149–1160. doi:10.3758/BRM.41.4.1149
28. Schlagheck ML, Joisten N, Walzik D, et al. Systematic review of exercise studies in persons with multiple sclerosis: exploring the quality of interventions according to the principles of exercise training. Neurol Ther. 2021;10:585–607. doi:10.1007/s40120-021-00274-z
29. Darawad MW, Hamdan-Mansour AM, Khalil AA, Arabiat D, Samarkandi OA, Alhussami M. Exercise Self-efficacy scale: validation of the Arabic version among Jordanians with chronic diseases. Clin Nurs Res. 2018;27:890–906. doi:10.1177/1054773816683504
30. Bandura A. Guide for constructing self-efficacy scales. In: Self-Efficacy Beliefs of Adolescents. Information Age Publishing; 2006:307–337.
31. Aldughmi M, Al-Shorman A, Khalil H, El-Salem K, Alghwiri A. Translation and validation of the Arabic version of the patient determined disease steps in people with multiple sclerosis. Physiother Theory Pract. 2022;38:1281–1288. doi:10.1080/09593985.2020.1839988
32. Hohol MJ, Orav EJ, Weiner HL. Disease steps in multiple sclerosis: a simple approach to evaluate disease progression. J Neurol. 1995;45(2):251–255.
33. Al-Sobayel HI, Al-Hugail HA, AlSaif RM, et al. Validation of an Arabic version of fatigue severity scale. Saudi Med J. 2016;37:73. doi:10.15537/smj.2016.1.13055
34. Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD. The fatigue severity scale: application to patients with multiple sclerosis and systemic lupus erythematosus. Arch Neurol. 1989;46:1121–1123. doi:10.1001/archneur.1989.00520460115022
35. Picha KJ, Howell DM. A model to increase rehabilitation adherence to home exercise programmes in patients with varying levels of self‐efficacy. Musculoskelet Care. 2018;16:233–237. doi:10.1002/msc.1194
36. Plow MA, Resnik L, Allen SM. Exploring physical activity behaviour of persons with multiple sclerosis: a qualitative pilot study. Disabil Rehabil. 2009;31:1652–1665. doi:10.1080/09638280902738375
37. Bandura A Social foundations of thought and action. Englewood Cliffs, NJ; 1986.
38. Riazi A, Thompson AJ, Hobart JC. Self-efficacy predicts self-reported health status in multiple sclerosis. Multi Scler J. 2004;10:61–66. doi:10.1191/1352458504ms986oa
39. Donkers SJ, Nickel D, Paul L, Wiegers SR, Knox KB. Adherence to physiotherapy-guided web-based exercise for persons with moderate-to-severe multiple sclerosis a randomized controlled pilot study. Int J MS Care. 2020;22:208–214. doi:10.7224/1537-2073.2019-048
40. Straudi S, Martinuzzi C, Pavarelli C, et al. A task-oriented circuit training in multiple sclerosis: a feasibility study. BMC Neurol. 2014;14:1–9. doi:10.1186/1471-2377-14-124
41. Motl RW, Sandroff BM. Benefits of exercise training in multiple sclerosis. Curr Neurol Neurosci Rep. 2015;15:1–9. doi:10.1007/s11910-015-0585-6
42. Dobkin BH. Behavioral self-management strategies for practice and exercise should be included in neurologic rehabilitation trials and care. Curr Opin Neurol. 2016;29:693. doi:10.1097/WCO.0000000000000380
43. Williams KL, Low Choy NL, Brauer SG. Center‐based group and home‐based individual exercise programs have similar impacts on gait and balance in people with multiple sclerosis: a randomized trial. PMR. 2021;13:9–18. doi:10.1002/pmrj.12377
44. Carter AM, Daley AJ, Kesterton SW, Woodroofe NM, Saxton JM, Sharrack B. Pragmatic exercise intervention in people with mild to moderate multiple sclerosis: a randomised controlled feasibility study. Contemp Clin Trials. 2013;35:40–47. doi:10.1016/j.cct.2013.04.003
45. Sessford JD, Locke SR, Cary MA, Flora PK, Knox K, Brawley LR. Effect of group counseling plus tailored exercise on mobility function in multiple sclerosis. Int J MS Care. 2021;23:66–72.
46. Wicks P, Massagli M, Kulkarni A, Dastani H. Use of an online community to develop patient-reported outcome instruments: the Multiple Sclerosis Treatment Adherence Questionnaire (MS-TAQ). J Medical Internet Res. 2011;13:e1687. doi:10.2196/jmir.1687
47. Haase R, Schultheiss T, Kempcke R, Thomas K, Ziemssen T. Use and acceptance of electronic communication by patients with multiple sclerosis: a multicenter questionnaire study. J Medical Internet Res. 2012;14:e2133. doi:10.2196/jmir.2133
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.