Back to Journals » Patient Preference and Adherence » Volume 17
Exercise Intention and its Associated Factors Among Persons Post-Stroke: A Cross-Sectional Study
Authors Zhou Y ![]() , Hua B, Shi X, Du S, Yuan J, Wang Y
, Hua B, Shi X, Du S, Yuan J, Wang Y
Received 6 June 2023
Accepted for publication 19 September 2023
Published 12 October 2023 Volume 2023:17 Pages 2535—2544
DOI https://doi.org/10.2147/PPA.S424595
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Yi Zhou,1 Biao Hua,2 Xiaoyang Shi,1 Shaoying Du,1 Jing Yuan,1 Yan Wang1
1School of Nursing, Hebei University, Baoding, Hebei, People’s Republic of China; 2Department of Neurology, Affiliated Hospital of Hebei University, Baoding, Hebei, People’s Republic of China
Correspondence: Yan Wang, School of Nursing, Hebei University, No. 342 Yuhuadong Road, Lianchi District, Baoding, Hebei, 071000, People’s Republic of China, Tel/Fax +86 3125075605, Email [email protected] Biao Hua, Department of Neurology, Affiliated Hospital of Hebei University, No. 212 Yuhuadong Road, Lianchi District, Baoding, Hebei, 071000, People’s Republic of China, Email [email protected]
Purpose: To investigate the level of exercise intention and its associated factors among persons post-stroke using the Theory of Planned Behavior.
Patients and Methods: In this cross-sectional study, a total of 333 participants admitted to the neurology units of a tertiary care hospital in China with a confirmed diagnosis of stroke were recruited. A self-administered instrument based on the Theory of Planned Behavior was used to determine the exercise intention and its associated factors among persons post-stroke.
Results: The results revealed that only 128 participants had exercise intention after discharge with a prevalence of 38.4%. Multivariable linear regression analysis revealed that monthly income, living situation, subjective norms, attitude, and perceived behavioral control were significant predictors of exercise intention of persons post-stroke. Perceived behavioral control and living situation were the most relevant factors of exercise intention.
Conclusion: The level of exercise intention among persons post-stroke was found to be low. Perceived behavioral control and living situation were particularly important and contributed to exercise intention. Healthcare professionals’ adequate guidance on exercise should be provided, with a focus on educating both patients and their family members, especially spouses, to promote exercise intention in persons post-stroke.
Keywords: exercise intention, stroke, exercise adherence, Theory of Planned Behavior
Introduction
Stroke is one of the leading causes of death and disability worldwide.1 In China, stroke is also the primary cause of death in urban and rural areas, accounting for 20.5% and 24.2% of all deaths, respectively.2 The American Heart Association (AHA) strongly recommends persons post-stroke should regularly participate in aerobic exercise, resistance (strength) training, flexibility training, and neuromuscular training3 to promote functional independence and range of movement and to prevent the recurrence risk of stroke and other cardiovascular diseases (CVDs).4 However, a large body of evidence demonstrated that sedentary behavior and lack of physical activity and exercise are common issues among persons post-stroke5–7 and exercise adherence was poor in persons post-stroke.8–10 A recent systematic review found that most community-dwelling stroke survivors did not fulfill the recommended 30 minutes of daily moderate to vigorous physical activity (MVPA).11 And a longitudinal study of objectively measured physical activity after stroke reported that less than one-third of the sample accumulated 30 min of daily MVPA in bouts of ≥ 10 min.12 Inadequate physical activity and exercise after a stroke is correlated with reduced muscle strength and cardiopulmonary fitness, decreased ability to perform activities of daily living, and an increased risk of recurrent stroke and other CVDs events.3,13–15 Lack of physical activity and exercise is known to be harmful to persons post-stroke. Considering the negative influences, it is critical to address low exercise adherence among persons post-stroke.
One potential target to address poor exercise adherence is exercise intention, assumed as a motivational factor that influences behavior, which indicates how hard people are willing to try and how much effort they are planning to exert to perform physical activity and exercise.16 The Theory of Planned behavior (TPB), widely applied in various populations and healthcare contexts, believes that a person’s behavior can be predicted by the strength of a person’ s intention.16 As a key factor in predicting exercise behavior, exercise intention is valuable to be understood and serves as an effective target for developing interventions to promote exercise participation.16–19 Previous studies have explored exercise intention based on the TPB, such as persons with CVDs, kidney transplant recipients, individuals with schizophrenia, pregnant women, and other populations.20–23 The TPB is intriguing due to its applicability in investigating motivational factors involved in health promotion and its practicable framework for understanding the determinants of exercise.
The TPB also suggests that intention is determined by some components, including subjective norms, attitudes, and perceived behavior control.16 Subjective norms refer to a person’s perceived social pressure from significant others (e.g., family members, relatives, friends, and healthcare professionals (HCPs)) to perform a behavior. Attitudes reflect the degree to which a person has a positive or negative evaluation of behaviors. Perceived behavioral control indicates a person’s perception of the relative ease or difficulty in performing a behavior based on past behavioral experience, including perceived skills/ability, resources, and facilitators/barriers.16 According to the TPB, if a person perceives more social pressure from family ties or social networks, a more positive attitude, and greater beliefs in controlling facilitators or barriers in performing a given behavior, the stronger should be the individual’s intention to engage in the behavior.24
Despite the impact of exercise intention on exercise participation, there is insufficient evidence regarding exercise intention and its related factors among persons post-stroke. One published study has investigated the will of exercise rehabilitation in young and middle-aged persons post-stroke in 2011,25 and another study has found exercise intention was a predictor of rehabilitation exercise management behavior.26 Both of these papers focused on young or middle-aged persons post-stroke, with one study conducted a long time ago and the other failing to explore the influencing factors. Understanding exercise intention in persons post-stroke and its associated factors is an essential prerequisite for effective intervention to enhance exercise participation in persons post-stroke, further promoting exercise and obtaining better health outcomes.
Thus, the purpose of this study was to investigate the level of exercise intention and its determinants among persons post-stroke based on the TPB.
Materials and Methods
Design
This study was a cross-sectional survey with a convenience sampling method with persons post-stroke in mainland China. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) statement was used to make sure items that should be reported in this study.27
Setting and Participants
The participants were recruited from neurology units of a large tertiary care hospital (with over 2000 inpatient beds) in Baoding, a city located in northern China. The potential participants met the following criteria: (a) with a confirmed diagnosis of stroke, following the diagnostic criteria compiled by the Chinese Medical Association Neuropathy Branch; (b) passed the acute period and had the ability to read and understand; (c) assessed with muscle strength at level 5- or 5 and able to engage in self-care. Patients were excluded if they: (a) had been diagnosed with severe organ dysfunction or malignant tumor; (b) had been diagnosed with mental health problems; (c) had severe conscious or cognitive impairment, or (d) had contraindications related to exercise rehabilitation, such as unstable angina, severe arrhythmias, uncontrolled hypertension, and abnormalities of the locomotor system that affected exercise.
The sample size was calculated by using the G*power software. The minimum sample size of patients was 194 based on a medium effect size of 0.15, α of 0.05, and a power of 0.95 (using the G*power 3.1 version).28 A sample size of 233 was required, considering a 20% inefficiency rate.
Measures
Social-Demographic and Disease-Related Questionnaire
Participants’ social-demographic and disease-related characteristics (age, gender, marital status, education, occupation, personal monthly income, living situation, medical payment methods, first onset of stroke, time after stroke, and comorbidity) were obtained using a self-administered questionnaire.
Exercise Intention Instrument for Stroke Patients
The exercise intention instrument for persons post-stroke was developed by researchers based on a comprehensive literature review, expert consultation, and the TPB.12 The initial questionnaire had 29 items, and after two rounds of expert consultation, the 27-item questionnaire was obtained, which was subsequently tested for reliability and validity in the first 160 persons post-stroke of sample in this study. The overall Cronbach’s α was 0.96, indicating high internal consistency. Cronbach’s alpha specific to measures of subject norms, attitude, perceived behavioral control, and exercise intention, ranged from 0.87 to 0.92. Item content validity index (ICVI) was 0.8–1, and scale content validity index (SCVI) was 0.96, suggesting that the instrument had good content validity. An exploratory factor analysis (EFA) was carried out for the construct validity. Four principal factors were identified in the EFA, which explained 68.0% of the total variance. The final questionnaire consists of 27 items, all of which mapped to the TPB constructs, including subjective norms (5 items), attitude (7 items), perceived behavioral control (9 items), and exercise intention (6 items). Examples of questions are presented in Table 1. A 5-point Likert questionnaire was established (with 1=strongly disagree, 2=disagree, 3=neutral, 4=agree, 5=strongly agree). Items on each dimension were summed such that higher scores represent higher levels of subjective norms, attitude, perceived behavioral control, and exercise intention, respectively. In addition, the average scores of exercise intention dimension ≥4 were regarded as having exercise intention.
 |
Table 1 Examples of Questions by the TPB Constructs |
Data Collection
The data were collected from July 2022 to September 2022. Before the survey, all the investigators were trained on the purpose, inclusion and exclusion criteria, communication skills, and data-collecting methods of this study. Once the patients met the inclusion criteria, the investigators asked eligible patients if they were willing to participate in this survey. Upon expression of interest, the investigators conducted the face-to-face survey with participants before discharge. Personal questionnaire data were reviewed from hospital medical records by researchers. For participants who had difficulty in reading and writing the questionnaires, investigators read the inquiries item-by-item and recorded their answers objectively. The survey took about 10–15 minutes to complete.
Ethics Consideration
This study conformed with the principles outlined in the Declaration of Helsinki and was approved by the Ethics Committee of the Affiliated Hospital of Hebei University. The details of the study were given to the potential participants, and it was made clear that they were voluntary to decide whether to participate or not, and this would not have any impact on them. All participants provided written informed consent before the investigation. The participants were guaranteed that all data would be held securely and confidentially and that it would only be accessed by the research team.
Data Analysis
All analyses were carried out using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). Bar charts and P-P plots were used to explore whether the continuous variables (subjective norms, attitude, perceived behavioral control, and exercise intention) followed a normal distribution. Socio-demographic and disease-related characteristics were described with frequency, percentage, standard deviation, mean, median, range, and percentiles. Bivariate relationships between socio-demographic and disease-related characteristics and exercise intention were analyzed using Student’s t-test, one-way analysis of variance (ANOVA). Pearson correlation analysis was used to examine the relationships among subjective norms, attitude, perceived behavioral control, and exercise intention. Variables identified from t-tests, ANOVA, and correlation analysis that were statistically significantly correlated with exercise intention were included in the multiple linear regression analysis. Dummy variables were set for living situation and occupation, and the dummy variables needed to be entered into the regression model at the same time. For all statistical analyses, the significance level was p<0.05.
Results
Characteristics of the Participants
A total of 333 persons post-stroke were included in this study (Table 2). Their average age was 62.43 (SD 10.45). Most were male (66.7%), married (94.3%), farmers (80.5%), living with spouses or/and children (98.8%), and with co-morbid chronic diseases (69.4%). About half of the participants (44.2%) had attained middle school, and 46.9% of patients’ monthly income were lower than 2000 CNY.
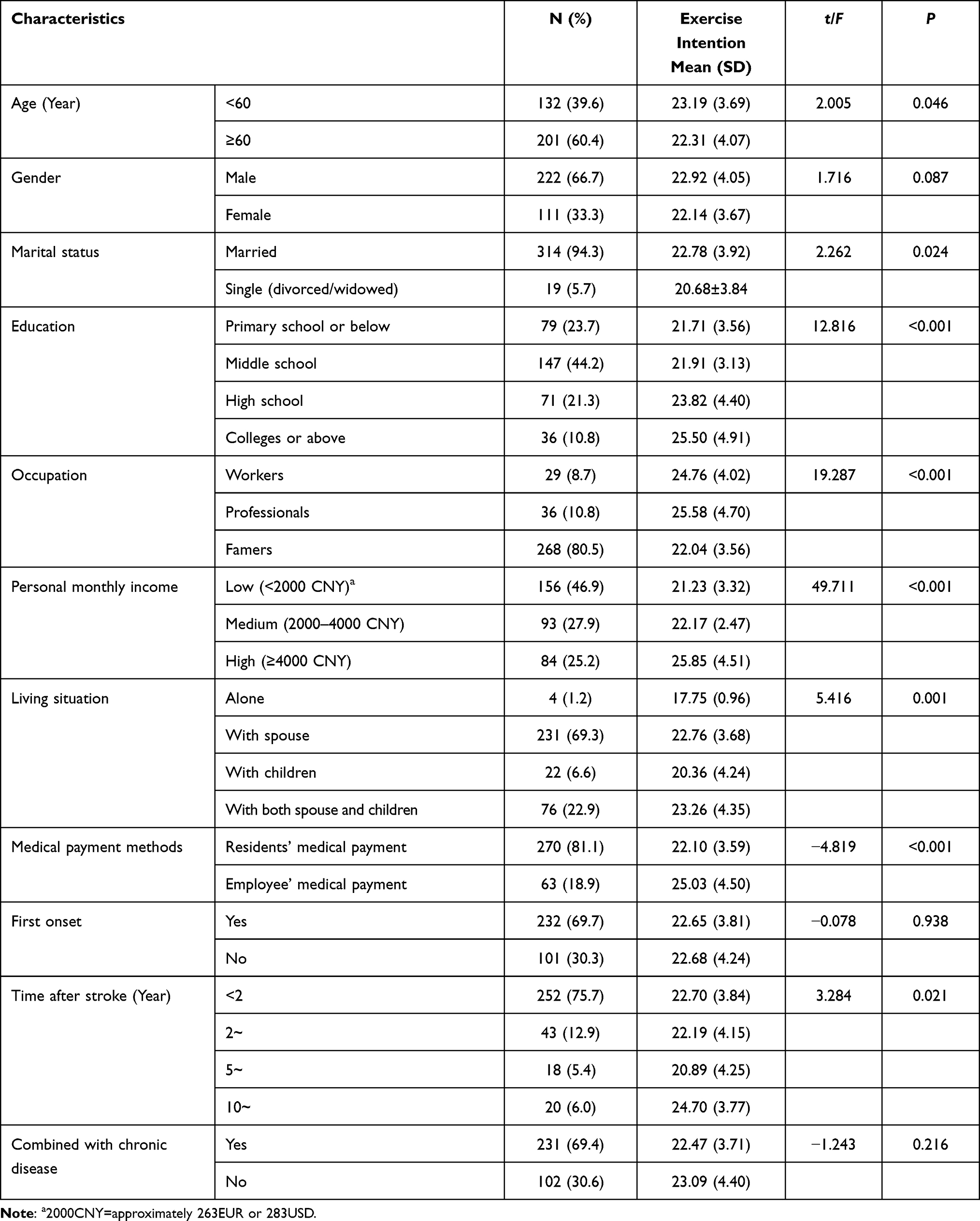 |
Table 2 Characteristics of Participants and Comparison of Exercise Intention Scores Among Persons Post-Stroke with Different Characteristics (n=333) |
Mean Score of Subjective Norms, Attitude, Perceived Behavioral Control and Exercise Intention
Exercise intention was 3.78 (SD 0.66) (consistent with a level of agreement corresponding with “neutral” to “agree”). Only 128 (38.4%) participants had exercise intention, whose score of exercise intention was higher than 4. The score specific to subjective norms was 3.34 (SD 0.62), attitude was 3.56 (SD 0.67), and perceived behavioral control was 3.46 (SD 0.52). The five items with the lowest scores are listed in Table 3.
 |
Table 3 The Five Items with Lowest Scores (n=333) |
Association Between Socio-Demographic and Disease-Related Characteristics and Exercise Intention
The association between participants’ socio-demographics and disease-related characteristics and exercise intention is shown in Table 2. On univariate analysis, the following were all significantly associated with exercise intention: age (t=2.005, p=0.046), marital status (t=2.262, p=0.024), education level (F=12.816, p<0.001), occupation (F=19.287, p<0.001), personal monthly income level (F=49.711, p<0.001), living situation (F=5.416, p=0.001), medical payment methods (t=−4.819, p<0.001), and time after stroke (F=3.284, p=0.021).
Correlation Among Subjective Norms, Attitude, Perceived Behavioral Control and Exercise Intention
The bivariate correlations between the TPB constructs and exercise intention among persons post-stroke revealed significantly moderately positive correlations (Table 4). Perceived behavioral control had the highest correlation to exercise intention (r=0.765, p<0.001), followed by attitude (r=0.739, p<0.001); subjective norms had the lowest correlation to exercise intention (r=0.613, p<0.001).
 |
Table 4 Means and Correlation Matrix for the TPB Constructs (n=333) |
The Multiple Linear Regression Analysis of Exercise Intention
Monthly income (β=0.149, p=0.006), living with spouse (β=0.385, p=0.006), living with both spouse and children (β=0.338, p=0.009), subjective norms (β=0.183, p<0.001), attitude (β=0.241, p<0.001) and perceived behavioral control (β=0.436, p<0.001) were significant predictors of exercise intention of persons post-stroke (Table 5). The model was significant and explained 66.5% of exercise intention (R2=0.665, F=48.092, p<0.001). Perceived behavioral control and living situation were the strongest correlates of exercise intention.
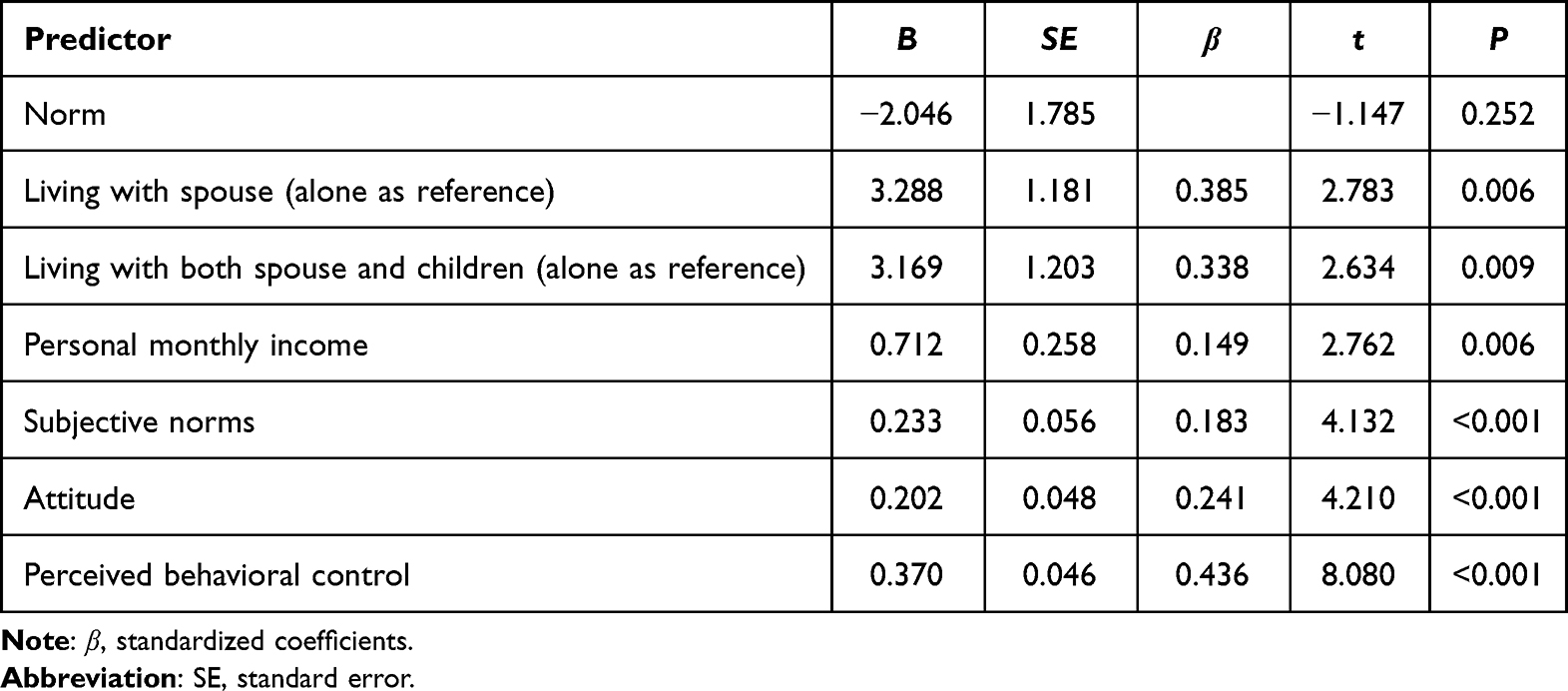 |
Table 5 Multivariable Linear Regression Model for Predicting Exercise Intention of Stroke Patients (n=333) |
Discussion
This study investigated the level and associated factors of exercise intention among persons post-stroke. The mean score of exercise intention was 3.78 (SD 0.66), which was in accordance with a level of agreement corresponding with “neutral” to “agree”. Our results revealed that only 38.4% of persons post-stroke intended to exercise after discharge, which supports previous findings reporting low levels of exercise among persons post-stroke.8,9 Notably, this result was lower than those reported in previous studies,25,26 both of which investigated young and middle-aged persons post-stroke (age <60y). The inconsistency may be attributed to younger patients who undertake more family responsibilities, are willing to return to work, have higher rehabilitation motivation,29 and display better adherence to rehabilitation programs.30 Our univariate analysis results also indicated that older persons post-stroke had lower exercise intention.
Identifying what factors predict the exercise intention of persons post-stroke will provide a reference for HCPs to evaluate high-risk patients with low intention and deliver effective care. Our study found that perceived behavioral control was the primary determinant of exercise intention among persons post-stroke, which agrees with the findings of previous studies.20,23,31 If patients perceive more barriers, their intention to exercise is likely to decrease. Our results showed that inadequate guidance on exercise from HCPs was perceived as the strongest barrier to exercise among persons post-stroke (“I receive guidance from professionals on how to exercise properly” item had the lowest score (2.12)). These results conform to Mahmood et al study, which found that lack of education by the HCPs would result in poor knowledge about stroke exercise and further lead to non-adherence.32 In addition, the period of inpatient rehabilitation may be an opportune time to influence long-term physical activity.33 Therefore, from the view of exercise intention promotion, HCPs’ guidance on exercise should be emphasized and incorporated into inpatients care.
Except for perceived behavioral control, living situation is another strongest predictor of exercise intention. Our study found that persons post-stroke living with a spouse or both a spouse and children were more likely to intend to exercise, which is congruent with the evidence from earlier studies.34 A supportive family is recognized as the most crucial factor in enhancing exercise participation. Family members assist persons post-stroke to carry out a task, encourage them to continue exercises and provide psychological support,32 all of which contribute to promoting the intention to exercise. One important finding is that our results emphasized the vital role of the spouse in facilitating exercise intention, which is supported by the previous evidence that family caregivers, mainly spouses, played an especially critical role in providing support.34 Recent studies have demonstrated that caregiver-mediated intervention with exercise could improve persons post-stroke basic activity of daily life.35 Doing exercises together appears to make patients and caregivers actively involved in rehabilitation.36 Caregiver-mediated exercise interventions, a promising approach to augment stroke rehabilitation, are suggested for broader application and practice. Moreover, the results imply that persons post-stroke living alone and without a spouse should be supported from multiple sources. Nurses, especially community nurses, are in a key position to facilitate these supports by reaching out to individuals, families, and communities.37 The prerequisite is that nurses should have high levels of awareness on providing professional support and further promoting exercise intention of persons post-stroke.
Our study found a positive correlation between attitude and exercise intention among persons post-stroke, which aligns with the constructs of TPB.16 This finding is consistent with previous research indicating significant correlations between attitude and exercise intention among other populations as well.18,38 Attitude is more closely related to a person’s own self-perception and beliefs23 and persons post-stroke with positive attitude and strong beliefs on exercise, were more actively to participate in exercise as previously reported.39 Hence, according to the TPB, this finding suggests that, for persons post-stroke, intervention strategies should be focused on formulating patients’ positive attitudes about exercise (eg, providing exercise education and instruction, highlighting the benefits of exercise, and emphasizing the necessity and feasibility of exercise) to increase exercise intention, which, in turn, improves their exercise behaviors.
The findings that subjective norms were significantly associated with exercise intention, conform to earlier studies in other populations.20,31 Subjective norms reflect the effect of important persons or groups on individual behavioral decisions.16 Persons post-stroke with supportive significant others would have stronger exercise intention than those with less supportive networks.33 HCPs, family members, and friends were identified as significant persons who provide the subjective norms and influence exercise intention.23,40,41 However, this study found that persons post-stroke perceived a low level of support from HCPs regarding their exercise. Our results revealed that support from physicians and nurses had the lowest score in the subjective norm dimension (Table 3). Hence, more guidance and education on exercise for persons post-stroke should be given during the period of inpatient rehabilitation, and also their family members and friends should be encouraged to provide positive support for exercise after discharge.
Besides, a higher level of income was associated with stronger exercise intention in persons post-stroke, which is in accordance with previous study.20 One possible explanation is that persons post-stroke face increased financial burden due to long-term or even lifelong medication and disability resulting from the stroke.2 A systematic review revealed that the highest post-stroke care costs were observed in the USA, with rehabilitation services being the main cost driver.42 Currently, post-stroke outpatients need to be admitted to hospitals for professional rehabilitation exercise in China, but there is a limited budget for rehabilitation exercise and exercise-related information for persons post-stroke with low-income levels. In contrast, higher-income patients could have better access to professional rehabilitation exercise training and obtaining more exercise-related information.26 Given this, nurses, as the key role in educating patients,43 can provide more available exercise-related information for stroke patients with low-income levels. For instance, community nurses could organize community walking programs44,45 or promote the adoption of effective and low-cost Chinese traditional exercise, such as Tai Chi, Baduanjin, and Qigong.46–48
Limitations
Our study has several limitations. First, participants were recruited from neurology departments in a single hospital using a convenient sampling method, thereby limiting the representativeness of the sample. Second, the sample with better limb strength and self-care ability were included, which may restrict the transferability of our findings to stroke patients with poor limb strength. Third, the cross-sectional study design was applied in this study, which does not lend itself to causal inference and can provide information only on correlation and prediction of these factors. Thus, future longitudinal and intervention studies are needed to provide a more comprehensive understanding of the relationship between the factors we identified and exercise intention in persons post-stroke.
Conclusion
This study sheds light on the low level of exercise intention among persons post-stroke and found it was affected by many factors, with perceived behavioral control and living situation being the strongest associations. It underscores the need to increase the guidance provided by HCPs on exercise after stroke. Additionally, caregiver-mediated exercise program should be developed and suggested to broadly applied in persons post-stroke and their caregivers. Also, particular attention should be given to persons post-stroke with low income and those who live without a spouse, as they are more likely to have low exercise intention.
Data Sharing Statement
The data underlying this article will be shared on reasonable request to the corresponding author.
Acknowledgments
We would like to acknowledge the contributions of the persons who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by S&T Program of Hebei (No. 18277735D).
Disclosure
No conflicts of interest has been declared by the authors.
References
1. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1736–1788. doi:10.1016/S0140-6736(18)32203-7.
2. Wang LD, Peng B, Zhang HQ, et al. Brief report on stroke prevention and treatment in China. Chin J Cerebrovasc Dis. 2022;19(02):136–144 doi:10.3969/j.issn.1672-5921.2022.02.011.
3. Billinger SA, Arena R, Bernhardt J, et al. Physical activity and exercise recommendations for stroke survivors: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45(8):2532–2553. doi:10.1161/STR.0000000000000022
4. Gallanagh S, Quinn TJ, Alexander J, Walters MR. Physical activity in the prevention and treatment of stroke. ISRN Neurol. 2011;2011:953818. doi:10.5402/2011/953818
5. Ezeugwu VE, Manns PJ. Sleep duration, sedentary behavior, physical activity, and quality of life after inpatient stroke rehabilitation. J Stroke Cerebrovasc Dis. 2017;26(9):2004–2012. doi:10.1016/j.jstrokecerebrovasdis.2017.06.009
6. Barrett M, Snow JC, Kirkland MC, et al. Excessive sedentary time during in-patient stroke rehabilitation. Top Stroke Rehabil. 2018;25(5):366–374. doi:10.1080/10749357.2018.1458461
7. Choi Y-A, Lee JS, Park JH, Kim YH. Patterns of physical activity and sedentary behavior and their associated factors among nondisabled stroke survivors. Maturitas. 2022;158:10–15. doi:10.1016/j.maturitas.2021.11.009
8. Fu YQ. Analysis of the Current Situation of Out-of-Hospital functional Exercise Compliance and Its Influencing Factors Among Rural Stroke Patients in Changjiang Li Autonomous County of Hainan Province. Hainan Medical University; 2022.
9. Yang YL. Study on the Current Exercise Training Situation in Patients with Stroke at Sequelae Stage. Soochow University; 2018.
10. Miller KK, Porter RE, DeBaun-Sprague E, Van Puymbroeck M, Schmid AA. Exercise after stroke: patient adherence and beliefs after discharge from rehabilitation. Top Stroke Rehabil. 2017;24(2):142–148. doi:10.1080/10749357.2016.1200292
11. Fini NA, Holland AE, Keating J, Simek J, Bernhardt J. How physically active are people following stroke? Systematic review and quantitative synthesis. Phys Ther. 2017;97(7):707–717. doi:10.1093/ptj/pzx038
12. Fini NA, Bernhardt J, Churilov L, Clark R, Holland AE. Adherence to physical activity and cardiovascular recommendations during the 2 years after stroke rehabilitation discharge. Ann Phys Rehabil Med. 2021;64(2):101455. doi:10.1016/j.rehab.2020.03.018
13. Hackam DG, Spence JD. Combining multiple approaches for the secondary prevention of vascular events after stroke: a quantitative modeling study. Stroke. 2007;38(6):1881–1885. doi:10.1161/STROKEAHA.106.475525
14. Ivey FM, Macko R, Ryan A, Hafer-Macko C. Cardiovascular health and fitness after stroke. Top Stroke Rehabil. 2005;12(1):1–16. doi:10.1310/GEEU-YRUY-VJ72-LEAR
15. Han P, Zhang W, Kang L, et al. Clinical evidence of exercise benefits for stroke. In: Xiao J, editor. Advances in Experimental Medicine and Biology. Singapore: Springer; 2017:131–151.
16. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
17. Bandura A. Failures in self-regulation: energy depletion or selective disengagement? Psychol Inq. 1996;7(1):20–24. doi:10.1207/s15327965pli0701_3
18. De Vivo M, Hulbert S, Mills H, Uphill M. Examining exercise intention and behaviour during pregnancy using the theory of planned behaviour: a meta-analysis. J Reprod Infant Psychol. 2016;34(2):122–138. doi:10.1080/02646838.2015.1118022
19. Gao M, Chen X, Sun X, Wang F, Fan L, Sun X. Predicting stage of exercise among patients with type 2 diabetes: a test of the extended theory of planned behavior. Patient Prefer Adherence. 2020;14:277–285. doi:10.2147/PPA.S236813
20. Gao YY. Analysis of Influencing Factors of Exercise Rehabilitation Participation Intention of Patients After PCI Based on the Theory of Planned Behaviour. Henan University; 2021.
21. Twyford J, Lusher J. Determinants of exercise intention and behaviour among individuals diagnosed with schizophrenia. J Ment Health. 2016;25(4):303–309. doi:10.3109/09638237.2015.1124399
22. Shadi KM. Predicting Intentions to Physical Activity in Jordanian Patients with Coronary Artery Disease: Impact of Attitudes, Subjective Norms, and Perceived Behavioral Control. Kent State University; 2020.
23. Lee C-F, Chiang I-C, Hwang F-M, Chi L-K, Lin H-M. Using the theory of planned behavior to predict pregnant women’s intention to engage in regular exercise. Midwifery. 2016;42:80–86. doi:10.1016/j.midw.2016.09.014
24. Ajzen I. Perceived behavioral control, self‐efficacy, locus of control, and the theory of planned behavior 1. J Appl Soc Psychol. 2002;32(4):665–683. doi:10.1111/j.1559-1816.2002.tb00236.x
25. Liu YF, Jiang H, Wang QH. Will of middle-young-aged stroke patients for exercise rehabilitation and the influencing factors. Chin Gen Pract. 2011;14(04):449–452 doi:10.3969/j.issn.1007-9572.2011.04.032.
26. Li Y, Jing X, Tuo M, et al. Correlation study of rehabilitation intention, self-efficacy and rehabilitation exercise management behavior in middle-aged stroke patients. Int J Clin Exp Med. 2019;3(4):119–126 doi:10.26855/ijcemr.2019.10.002.
27. Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/S0140-6736(07)61602-X
28. Faul F, Erdfelder E, Buchner A, Lang A-G. Statistical power analyses using G* Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.4.1149
29. Rapolienė J, Endzelytė E, Jasevičienė I, Savickas R. Stroke patients motivation influence on the effectiveness of occupational therapy. Rehabil Res Pract. 2018;2018:9367942. doi:10.1155/2018/9367942
30. Pishkhani MK, Dalvandi A, Ebadi A, Hosseini M. Factors affecting adherence to rehabilitation in Iranian stroke patients: a qualitative study. J Vasc Nurs. 2019;37(4):264–271. doi:10.1016/j.jvn.2019.07.001
31. Zhu G, Qian X, Qi L, et al. The intention to undertake physical activity in pregnant women using the theory of planned behaviour. J Adv Nurs. 2020;76(7):1647–1657. doi:10.1111/jan.14347
32. Mahmood A, Nayak P, Kok G, English C, Manikandan N, Solomon JM. Factors influencing adherence to home-based exercises among community-dwelling stroke survivors in India: a qualitative study. Eur J Physiother. 2021;23(1):48–54. doi:10.1080/21679169.2019.1635641
33. Simpson DB, Jose K, English C, Gall SL, Breslin M, Callisaya ML. Factors influencing sedentary time and physical activity early after stroke: a qualitative study. Disabil Rehabil. 2022;44(14):3501–3509. doi:10.1080/09638288.2020.1867656
34. Zhao J, Zang Y, Chau JPC, He R, Thompson DR. Chinese stroke survivors’ perceptions of participation in exercise or sitting Tai Chi. Eur J Cardiovasc Nurs. 2021;21(2):143–151. doi:10.1093/eurjcn/zvab036
35. Choo WT, Jiang Y, Chan KGF, et al. Effectiveness of caregiver‐mediated exercise interventions on activities of daily living, anxiety and depression post‐stroke rehabilitation: a systematic review and meta‐analysis. J Adv Nurs. 2022;78(7):1870–1882. doi:10.1111/jan.15239
36. Vloothuis J, Depla M, Hertogh C, Kwakkel G, van Wegen E. Experiences of patients with stroke and their caregivers with caregiver-mediated exercises during the CARE4STROKE trial. Disabil Rehabil. 2020;42(5):698–704. doi:10.1080/09638288.2018.1507048
37. Li Y, Zhang W, Ye M, Zhou L. Perceived participation and autonomy post‐stroke and associated factors: an explorative cross‐sectional study. J Adv Nurs. 2021;77(3):1293–1303. doi:10.1111/jan.14670
38. Dong ML, Fu R, Yin GL. Exploring the factors influencing regular exercise in haemodialysis patients based on the theory of planned behaviour. J Nurs Train. 2019;34(13):1231–1233. doi:10.16821/j.cnki.hsjx.2019.13.022
39. Moorley C, Cahill S, Corcoran N. Stroke among African‐Caribbean women: lay beliefs of risks and causes. J Clin Nurs. 2016;25(3–4):403–411. doi:10.1111/jocn.13061
40. Chou H-F, Weng L-C, Wang Y. Exploring physical activity behavior in middle-aged Taiwanese women based on the theory of planned behavior. Women Health. 2022;62(7):603–611. doi:10.1080/03630242.2022.2098893
41. Trotman IC. Physical Activity and Diabetes: An Application of the Theory of Planned Behavior in the Nation-State of Barbados. Capella University; 2018.
42. Rajsic S, Gothe H, Borba HH, et al. Economic burden of stroke: a systematic review on post-stroke care. Eur J Health Econ. 2019;20(1):107–134. doi:10.1007/s10198-018-0984-0
43. Magwood GS, Nichols M, Jenkins C, et al. Community-based interventions for stroke provided by nurses and community health workers: a review of the literature. J Neurosci Nurs. 2020;52(4):E7–E8. doi:10.1097/JNN.0000000000000512
44. Kim M, Cho K, Lee W. Community walking training program improves walking function and social participation in chronic stroke patients. Tohoku J Exp Med. 2014;234(4):281–286. doi:10.1620/tjem.234.281
45. Lee J-M, Moon -H-H, Lee S-K, Lee H-L, Park Y-J. The effects of a community-based walking program on walking ability and fall-related self-efficacy of chronic stroke patients. J Exerc Rehabil. 2019;15(1):20–25. doi:10.12965/jer.1836502.251
46. Xie G, Rao T, Lin L, et al. Effects of Tai Chi Yunshou exercise on community-based stroke patients: a cluster randomized controlled trial. Eur Rev Aging Phys Act. 2018;15:17. doi:10.1186/s11556-018-0206-x
47. Park M, Song R, Ju K, et al. Effects of Tai Chi and Qigong on the mobility of stroke survivors: a systematic review and meta-analysis of randomized trials. PLoS One. 2022;17(11):e0277541. doi:10.1371/journal.pone.0277541
48. Zou L, Wang C, Chen X, Wang H. Baduanjin exercise for stroke rehabilitation: a systematic review with meta-analysis of randomized controlled trials. Int J Environ Res Public Health. 2018;15(4):600. doi:10.3390/ijerph15040600
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.