Back to Journals » Cancer Management and Research » Volume 11
Exercise during adjuvant treatment for colorectal cancer: treatment completion, treatment-related toxicities, body composition, and serum level of adipokines
Authors Shim YJ, Kim HJ ![]() , Oh SC, Lee SI
, Oh SC, Lee SI ![]() , Choi SW
, Choi SW
Received 14 March 2019
Accepted for publication 13 May 2019
Published 11 June 2019 Volume 2019:11 Pages 5403—5412
DOI https://doi.org/10.2147/CMAR.S208754
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chien-Feng Li
Yoo Jin Shim,1* Hong Jun Kim,2* Sang Cheul Oh,3 Sun Il Lee,4 Seung Wook Choi1
1Department of Sports and Leisure, Sungshin Women’s University, Seongbuk-gu, Seoul 02844, Republic of Korea; 2Division of Oncology, Department of Internal Medicine, Kyung Hee University School of Medicine, Dong-dae-mun-gu, Seoul 02447, Republic of Korea; 3Division of Oncology, Department of Internal Medicine, Korea University Guro Hospital, Guro-gu, Seoul 08308, Republic of Korea; 4Department of Surgery, Korea University Guro Hospital, Guro-gu, Seoul 08308, Republic of Korea
*These authors contributed equally to this work
Objectives: The primary aim of this study was to investigate the beneficial effect of exercise on completion rates of adjuvant treatment, which is one of the major prognostic factors among patients with locally advanced colorectal cancer after undergoing curative resection followed by adjuvant treatment.
Design: Prospective pilot study
Methods: We assigned patients who were scheduled to undergo adjuvant treatment (N=39) to the exercise group or the control group in a 2:1 ratio in the order of enrollment. Patients completed questionnaires and underwent assessment of the outcome variables at the start of chemotherapy and upon completion of treatment.
Results: A fivefold lower possibility of dose adjustment in the exercise group compared to the control group was demonstrated (OR, 0.188; p=0.023; 95% CI, 0.044–0.793). A significantly smaller proportion of the exercise group had grade 3 or 4 nausea (p=0.018) and neurotoxicity (P=0.024) symptoms. Muscle to fat ratios were significantly reduced in the control group (p=0.039), but not in the exercise group (p=0.742). Serum levels of leptin were significantly increased in the control group (p=0.038), but not in the exercise group (p=0.073). Serum levels of adiponectin were significantly increased in the exercise group (p=0.026) but tended to be decreased in the control group with no statistical significance (p=0.418).
Conclusions: Exercise training among patients with colorectal cancer was found to have a beneficial impact on adjuvant treatment completion rates and treatment-associated toxicities. This program was also shown to be beneficial to patients’ body compositions and serum levels of adipokines.
Keywords: exercise, chemotherapy, adjuvant, chemoradiotherapy, adjuvant, colorectal neoplasms, body composition, adipokines
Introduction
Colorectal cancer (CRC) accounts for 10% of the prevalence of all types of cancers, with approximately 600,000 deaths worldwide per annum.1 Adjuvant treatment after curative resection of locally advanced CRC has been considered as standard care, since a study investigating a regimen of treatment with 5-fluorouracil plus levamisole for a year was published in the early 1990s.2 After several clinical trials in the 2000s, a 6-month chemotherapeutic regimen of fluoropyrimidine plus oxaliplatin (FOLFOX) has been established as standard adjuvant treatment in stage II with high risk and stage III CRC patients.3
Despite improved survival rates of patients with locally advanced CRC due to established standard adjuvant treatment,3 5-year recurrence rates of patients with stage II or III CRC are still considerable: 20% and 30–50%, respectively.4 Among several factors worsening cancer recurrence, completion rates of adjuvant chemotherapy have been shown to be a major prognostic factor.5 Efforts to confirm the non-inferiority of 3 months of treatment to the current 6 months of treatment have been ongoing6 to address concerns about considerable toxicities and costs even with shortened duration of treatment (from a year to 6 months); however, these attempts seem to have reached an impasse.7 Thus, for now, the best strategy appears to be the completion of the entire 6-month schedule of standard adjuvant treatment.
Completion rates of adjuvant treatment in patients with stage III CRC were reported not to reach 70% (66%).5 Fatigue and physical frailty were reported as major factors related to incomplete adjuvant treatment in patients with stage III CRC.8 Forty-six percent of patients undergoing adjuvant chemotherapy for CRC report substantial general weakness, which worsens during therapy.9 Several studies, conducted among patients with breast cancer, prostate cancer, and CRC, have demonstrated the beneficial effects of exercise programs for physical fitness during adjuvant chemotherapy.10,11 However, no study reported in English has demonstrated the positive effect of exercise programs on the completion rates of adjuvant treatment.
The primary aim of the current study was to investigate the beneficial effect of physical exercise for patients undergoing adjuvant chemotherapy, in terms of completion rates and treatment-related toxicities. Additionally, we evaluated the effect of physical exercise on body composition and serum levels of adipokines in patients undergoing adjuvant chemotherapy.
Patients and methods
The present pilot, single-center, prospective controlled study was approved by the institutional review board of Korea University Guro Hospital (KUGH16034-001). Blinding of patients was impossible, due to the nature of this study comparing an exercise group with a controlled group. From January 2016 to January 2017, we enrolled patients with CRC who underwent curative resection followed by adjuvant treatment. All patients were eligible if they had histologically confirmed CRC; however, only adenocarcinoma cases were enrolled. We excluded patients with serious cardiopulmonary conditions, orthopedic problems, glomerular filtration rates lower than 50 mL/min per 1.73 m2, liver cirrhosis, Eastern Cooperative Oncology Group performance status higher than 2 score, or any history of other cancers.
Patients were recruited from a CRC multidisciplinary care center. After providing informed consent to possibly eligible patients, we completed baseline characteristics assessments. For every two patients assigned to the exercise group, one patient was assigned to the control group in the order of enrollment in the study. Flow chart of participant inclusion in the study is shown in Figure 1.
 | Figure 1 Flow chart of participant inclusion in the study. |
Education and counseling for the exercise program were conducted before admission for adjuvant treatment. The program comprised 50 min of home-based exercise three times a week during adjuvant treatment. In addition to exercise education, written information and logbooks were distributed to be utilized in home-based exercise. Patients recorded the amount and intensity of exercise, and discomfort during exercise in the logbooks; thus, we were able to re-establish the intensity of exercise every two weeks.
To enhance core muscle and cardiopulmonary function, aerobic and anaerobic exercises were alternately performed. Considering that most cancer patients are relatively old and have significant physical differences, exercise strength was not allowed to exceed 11–14 points by the Borg rating of perceived exertion scale.12 For patients with poor performance status due to side effects of surgery, the intensity of exercise was reduced further, and gradually implemented. The 5-min exercise program consisted of 10 min of warm-up core stretching, 30 min of alternating exercise (aerobic and anaerobic), and 10 min of wrap-up core stretching.
For warming up for 10 min, the stretching focused on the core parts (belly, spine, thigh, and buttock). Its moves were sit and press both knees, grab one leg and bend forward, cross legs and turn the upper body, prostrate and raise the upper body, cat pose, and lie down and twist waist.
The main exercise, which was 30 min, proceeded as a circular workout composed of a series of aerobic and anaerobic exercises, designed to enhance the full-body muscles and cardiopulmonary functions which had been downgraded by surgery and anticancer chemotherapy. The aerobic exercises were walking, march step, V-step, step touch, skip step, and kick step, and the anaerobic exercises were stand on one leg, lunge, arm curl, squat, lateral raise, and leg raise. Two sets of total 12 aerobic and anaerobic moves were implemented with each move done for a minute and with breaks of 5 or 6 min in between. The main exercise, which is a circular workout, alternated aerobic and anaerobic exercises.
The wrap-up exercise, which lasted 10 min, adopted the same program as for warm-up, the stretching in the core parts (belly, spine, thigh, and buttock).
Enrolled patients completed questionnaires and underwent assessment of the outcome variables at the start of chemotherapy and completion of treatment. The primary outcomes were completion rates of adjuvant treatment; it was defined as failure to complete treatment when adjuvant treatment was terminated prematurely, or when the dose of chemotherapeutic drugs was reduced beyond the standard dose calculated by body surface area, regardless of the rate of reduction.
The secondary outcomes included treatment-related toxicities, serum levels of adipokines, and body composition. The treatment-related toxicities were classified by grades 0–4 according to the common toxicity criteria guidelines. Serum levels of adipokines including adiponectin and leptin were analyzed using the human Leptin ELISA kit (R&D systems Co., Abingdon, UK) and human Adiponectin ELISA kit (R&D systems Co.). Body composition was measured with cross-sectional images taken by computed tomography at the level of the inferior surface of the third lumbar vertebra (L3), since several data have shown that subcutaneous fat area (SFA) and skeletal muscle area (SMA) measured at the L3 level are most closely correlated with whole body subcutaneous fat volume and skeletal muscle volume, respectively.13 A multi-detector computed tomography scanner (SOMATOM Definition AS+, Siemens Healthcare, Erlangen, Germany) was used to take 2-mm thick axial images. The SFA and SMA of cross-sectional images were measured using Image J (ver. 1.80; National Institutes of Health, Bethesda, MD, USA), and muscle to fat ratio (MFR) was calculated by dividing the SMA by the SFA (Figure 2). Height was measured using a digital stretcher DS-102 (JENIX, Seoul, Korea), and the vertical distance from the sole to the apex was measured after taking the upright posture so that the subject’s eyes and jaw were horizontal.
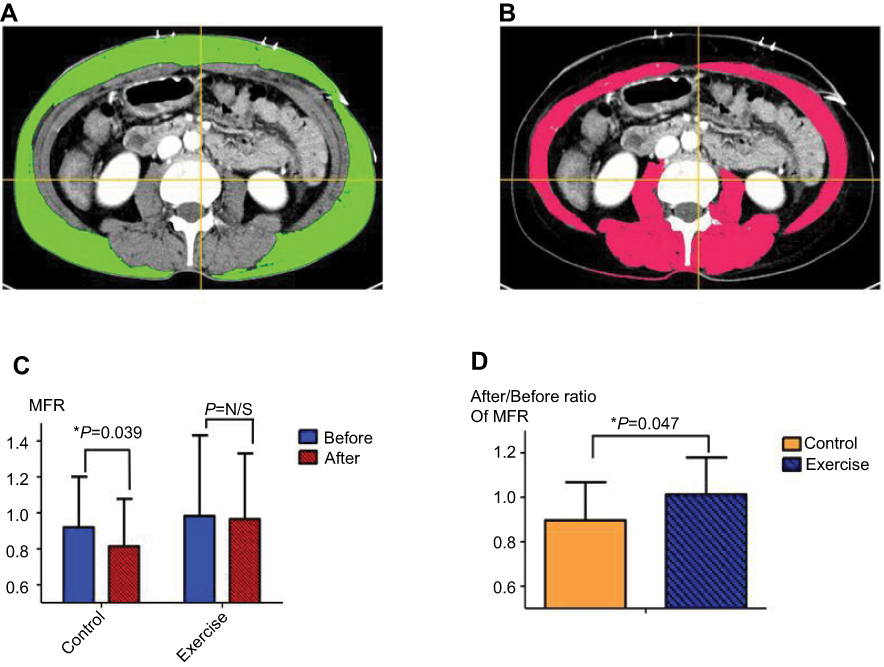 | Figure 2 (A and B) Subcutaneous fat area (SFA) and skeletal muscle area (SMA) of cross-sectional images, marked in green and red, respectively, were measured by using Image J (ver. 1.80, National Institutes of Health). (C) Muscle to fat ratio (MFR) was calculated by dividing the SMA by the SFA. MFRs were significantly reduced during the adjuvant treatment in the control group, but not in the exercise group. (D) MFR changes before and after adjuvant treatment were significantly different between the control and exercise groups. *p<0.05.Abbreviation: N/S, not significant. |
Since this study was a pilot controlled study, the sample size was fixed by the number of patients enrolled during the study period (between January 2016 and January 2017). Different completion rates of chemotherapy between the exercise group and the control group were assessed by binary logistic regression methods. We also assessed the differences in chemotherapy completion rates, toxicities related to chemotherapeutic agents, and other clinical parameters between both groups by using the chi-square test. In order to measure changes in serum levels of adipokines and body compositions before and after chemotherapy, a paired t-test was performed in each group. To compare the changes in adipokines and body compositions between both groups, we performed an independent t-test. We considered a p-value <0.05 as statistically significant. All statistical analyses were performed using SPSS version 20.0 for Windows (IBM, Armonk, NY, USA).
Results
Between January 2016 and January 2017, 65 CRC patients who underwent curative resection and were scheduled to receive adjuvant treatment were considered for enrollment in this study. Forty-two patients were recruited and provided written informed consent. Reasons for non-participation (n=23) were the time burden (n=11), travel distance (n=7), and ineligibility (n=5). Twenty-seven patients were assigned to the exercise group, two of whom were lost to follow-up during treatment. Fifteen patients were assigned to the control group, one of whom was lost to follow-up during treatment. Only 11 and 5 patients in the exercise and control groups, respectively, agreed to undergo the serum analysis. Baseline characteristics of the study patients (N=39) are presented in Table 1. The entire population was Korean or Korean Chinese, and had a median age of 58 (range, 41–77) years. The clinical parameters including age, sex, body surface area, body mass index, performance status, tumor markers, and genetic mutations were not significantly different between the exercise and control groups; age: 59.8±10.2 vs 60.0±8.6, p=0.923, body surface area: 1.63±0.15 vs 1.66±0.20, p=0.543, body mass index: 22.3±2.9 vs 23.4±3.3, p=0.279.
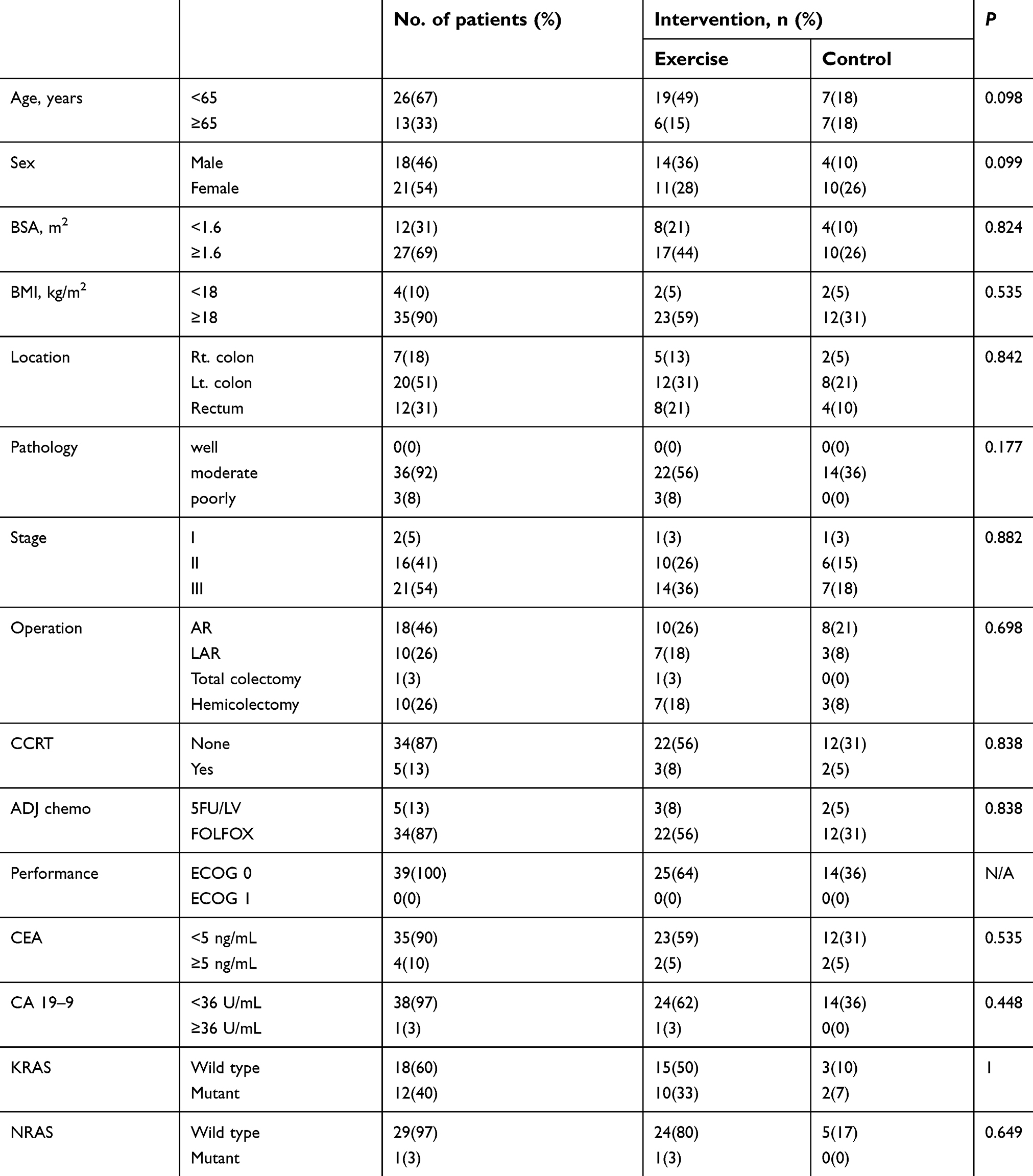 | Table 1 Baseline characteristics of the study patients (N=39) |
The majority of patients had stage II or III disease (95%), and received only adjuvant chemotherapy (87%) rather than concurrent chemo-radiation therapy (CCRT) followed by chemotherapy (13%); and chemotherapy regimen as FOLFOX (87%) rather than 5-fluorouracil/leucovorin (5FU/LV) (13%). Regardless of whether the patients received only chemotherapy or CCRT followed by chemotherapy, the duration of treatment was generally 6 months, and no significant difference in timing of treatment initiation was observed.
Information on adjuvant treatment completion rates is presented in Table 2. In total, 13 patients (33%) failed to complete treatments, and the reasons for dose reduction or premature termination included grade 3 or 4 neurotoxicity, neutropenia, and neutropenic fever. Compared with the control group, a significantly lower proportion of the exercise group failed to complete the prescribed regimen (57% and 20%, respectively, p=0.018). Binary logistic regression analysis demonstrated an approximately fivefold lower possibility of failure to complete in the exercise group compared with the control group (odds ratio, 0.188; 95% confidence interval: 0.044–0.793; p=0.023).
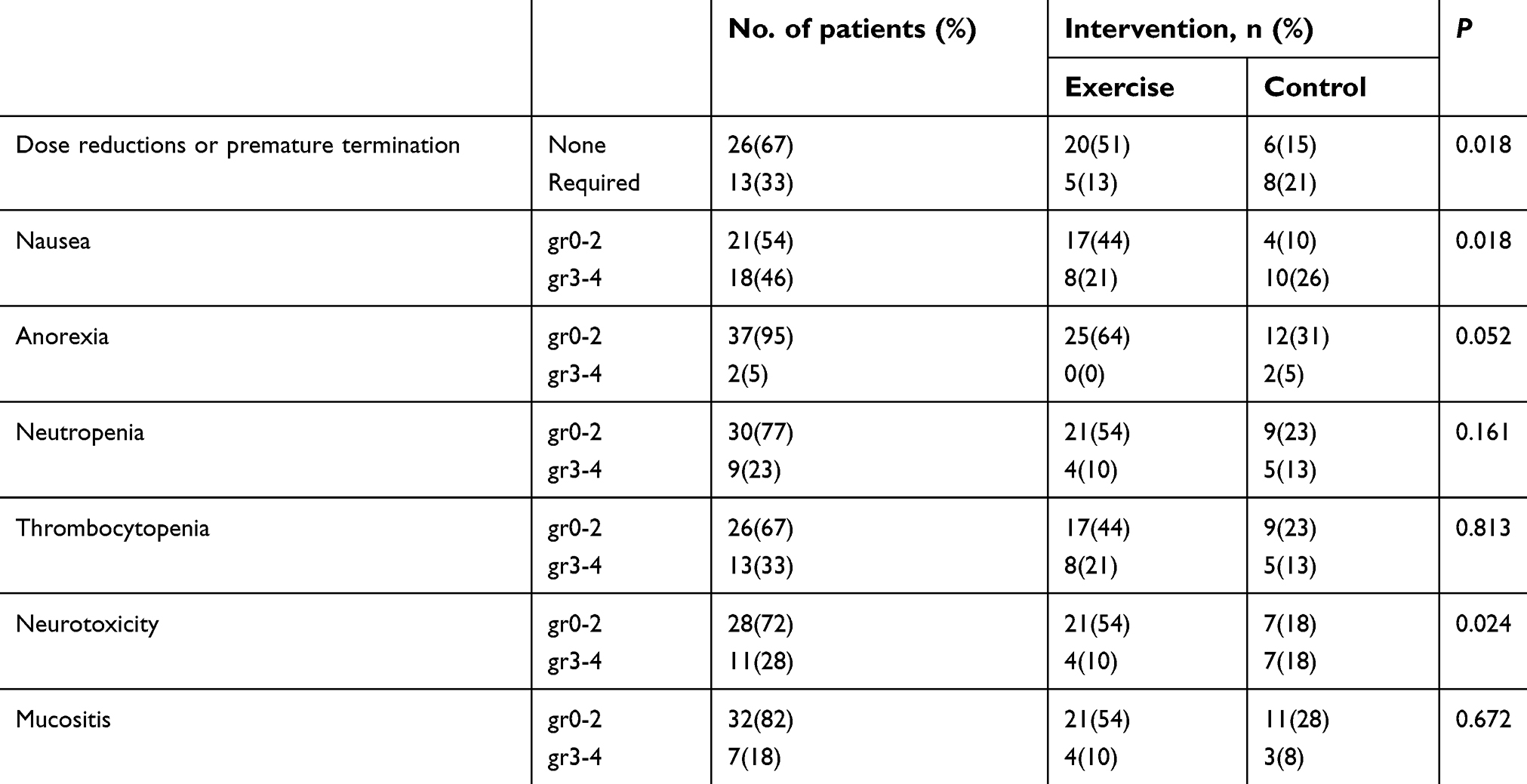 | Table 2 Effect of exercise intervention on chemotherapy completion rates and treatment-related toxicities |
Effects of exercise intervention on treatment-related toxicities are shown in Table 2. Compared with the control group, a significantly smaller proportion of the exercise group had grade 3 or 4 nausea symptoms (71% and 32%, respectively, p=0.018). Compared with the control group, a significantly lower proportion of the exercise group had grade 3 or 4 neurotoxicity symptoms (50% and 16%, respectively, p=0.024). A higher proportion of the control group tended to complain of severe anorexia, but this did not approach statistical significance (p=0.052).
Effects of the exercise intervention on body composition and serum levels of adipokines during adjuvant treatment are shown in Table 3, and Figures 2 and 3. MFRs were significantly reduced during adjuvant treatment in the control group, but not in the exercise group (p=0.039 and 0.742, respectively). The reduction rate of MFRs during adjuvant treatment was significantly greater in the control group than in the exercise group (p=0.047). Serum levels of leptin were significantly increased during adjuvant treatment in the control group, but not in the exercise group (p=0.038 and 0.073, respectively). Serum levels of adiponectin were significantly increased during adjuvant treatment in the exercise group, but tended to be decreased in the control group with no statistical significance (p=0.026 and 0.418, respectively). The rate of increase of serum levels of leptin during treatment was not significantly different between both groups (p=0.535). The changes in serum levels of adiponectin during treatment were not significantly different between both groups (p=0.169). Regardless of whether the patients received the exercise program or not, body surface area, body mass index, and serum levels of CEA and CA 19-9 were not changed significantly from start to completion of treatment.
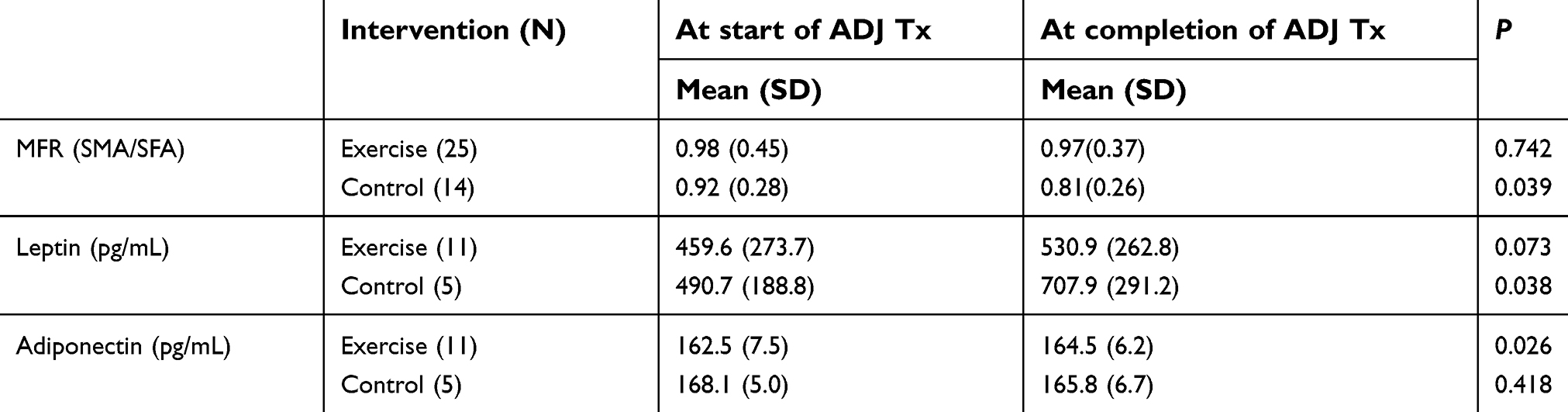 | Table 3 Effect of exercise intervention on body compositions and serum levels of adipokines in patients undergoing adjuvant treatment |
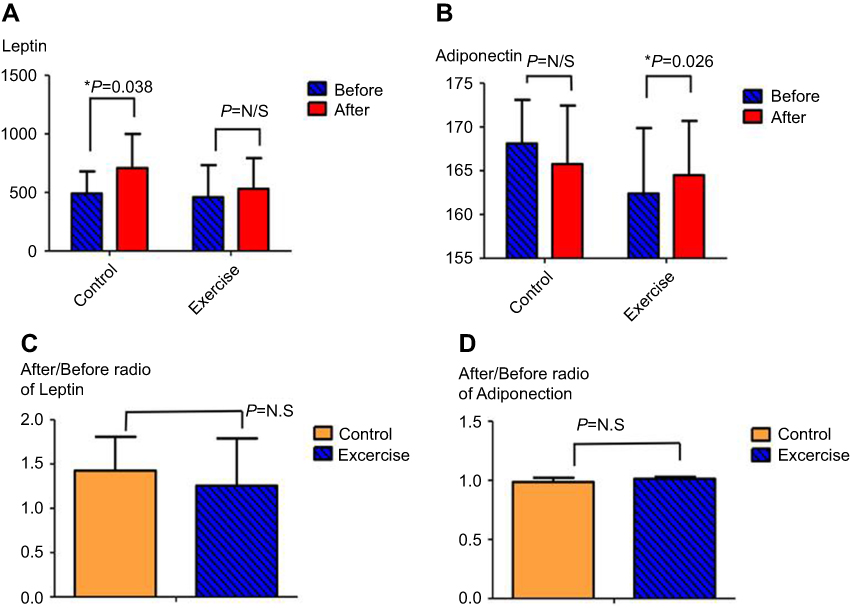 | Figure 3 (A) Serum levels of leptin were significantly increased during adjuvant treatment in the control group, but not in the exercise group. (B) Serum levels of adiponectin were significantly increased during adjuvant treatment in the exercise group, but tended to be decreased in the control group. (C and D) Changes in serum levels of both leptin and adiponectin before and after adjuvant treatment were not significantly different between the control and exercise groups. *p<0.05.Abbreviation: N.S, not significant. |
Discussion
Five-year recurrence rates among patients with locally advanced CRC are still noticeable, despite improved outcomes by standard adjuvant treatment,4 and are closely associated with failure to complete adjuvant treatment as prescribed regimens.5 Given that physical exercise has a beneficial effect on fatigue and general weakness which are the main reasons for failure to complete adjuvant treatment,8 we designed this study to investigate the positive association between exercise program and completion rates of adjuvant treatment and demonstrated it among CRC patients who underwent curative resection. To the best of our knowledge, this is the first pilot, single-center, prospective study in English on the subject. Also, we identified that exercise favorably affects treatment associated toxicities including nausea and neuropathy, and this program was shown to be beneficial to patients’ body compositions and serum adipokine levels.
Physical function and quality of life were improved by an 18-week exercise program in 57 patients with breast cancer, lymphoma, testicular cancer, and CRC.14 In addition, Shariati et al reported that 36 CRC patients undergoing chemotherapy were found to experience reduction in fatigue by conducting 40 min exercise programs implemented thrice weekly for 4 weeks.15 A few previous trials including these two studies demonstrated that exercise could reduce the main causes of delayed treatment or abandonment of chemotherapy schedule,8,14,15 while the current study demonstrated the direct effect of the exercise program on completion rates of adjuvant treatment. There have been a few subgroup analyses16 which suggest that the beneficial effects of exercise result in improved survival outcomes, although cogency of subgroup analysis is somewhat diminished. Further well-designed studies with a sufficient follow-up period are needed to prove it.
Anti-cancer treatment results in decreased muscle mass, accumulation of abdominal fat tissue, and reduction of aerobic capacity and joint operating range, while sarcopenia increases physical dysfunction,17 duration of hospitalization,18 rates of hospital-acquired infection,19 and chemotherapy-related toxicities.20 Muscle mass itself is even proposed as an important indicator for reduced toxic side effects of chemotherapy,21 and muscle mass evaluation is recommended to be quantified by computed tomography images as done in the current study.22 In this study, unlike the control group, there were no significant reductions in MFR in the exercise group, indicating that the muscle mass had been kept constant through exercise while undergoing adjuvant treatment for about 6 months. Compared to a previous study,14 which even showed increased muscle mass by exercise during the treatment period, the results of this study may be disappointing; however given that the study patients were comparatively old, it seemed obvious that the exercise program had been effective.
Adipokines or adipocytokines, which include leptin and adiponectin, are substances secreted mainly from adipose tissue, and have been known to have effects on obesity, insulin resistance, type 2 diabetes, and metabolic syndrome.23 Recently, some adipokines including leptin, adiponectin, tumor necrosis factor-alpha, interleukin (IL)-6, IL-8, and IL-10 were reported to be engaged in cell proliferation, angiogenesis and cancer cell development.24 Leptin affects insulin, tumor necrosis factor-alpha, glucocorticoid, reproductive hormones, and prostaglandin, stimulating the growth of not only normal cells but also cancer cells.25 Leptin was reported to be overexpressed in CRC cells, promote the proliferation of colonic epithelial cells, and reduce CRC cell death.26 On the other hand, adiponectin, in combination with its receptors, is reported to activate downstream target 5ʹ AMP-activated protein kinase to inhibit gluconeogenesis and promote oxidation of fatty acids, increasing insulin sensitivity.27 In addition, adiponectin is known to have preventive effects on arteriosclerosis and inflammation,27 and was shown to inhibit proliferation of colonic cells through the 5ʹ AMP-activated protein kinase pathway and mTOR signaling pathway.28 A few studies reported that the serum levels of adiponectin are inversely correlated with the number of colorectal adenomas.29 In the current study, serum levels of leptin were significantly increased in the control group, but not in the exercise group, and those of adiponectin were significantly increased during adjuvant treatment in the exercise group, but tended to be decreased in the control group with no statistical significance.
The current study has a few limitations. First, this study was performed in a single center. However, this limitation may in fact be advantageous, because the same testing equipment and consistent standard of analysis were used in this single center. Second, this study enrolled a relatively small sample size, which is a common limitation of pilot studies. Unlike the general population of CRC patients, only 33% of the final sample was age 65 or older, which might be due to the small sample size. Some of the non-significant findings in this study also could be due to this limitation. We calculated proper sample size for a future randomized controlled trial by G*Power 3.1.9.4 software,30 assuming a moderate effect of exercise program on treatment completion rates, according to Cohen with 0.378 effect size.31 We used the power of 0.8 and alpha =0.05, applied in two groups (exercise group and control group) analyzing the results by a two-way Fisher’s exact test. Expecting a sample loss of about 20%, we suggest including 32 individuals in each group for the future study.
Conclusion
In this study, exercise training for patients who underwent curative resection of CRC improved adjuvant treatment completion rates and treatment-associated toxicities, including nausea and neuropathy. Additionally, the current study suggests that exercise has beneficial effects on patients’ body compositions and serum levels of adipokines.
Practical implications
- Physical exercise may be a beneficial method to improve adjuvant treatment completion rates in patients with colorectal cancer.
- To prevent treatment-associated toxicities, including nausea and neuropathy, exercise training would be effective intervention.
- Exercise appears to have a beneficial effect on patients’ body compositions and serum levels of adipokines.
Acknowledgments
This research did not receive any specific grant from any funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jemal A, Center MM, DeSantis C, Ward EM. Global patterns of cancer incidence and mortality rates and trends. Cancer Epidemiol Prev Biomarkers. 2010;19(8):1055–9965. EPI–1010–0437.
2. Moertel CG, Fleming TR, Macdonald JS, et al. Levamisole and fluorouracil for adjuvant therapy of resected colon carcinoma. N Engl J Med. 1990;322(6):352–358. doi:10.1056/NEJM199002083220602
3. André T, Boni C, Navarro M, et al. Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colon cancer in the MOSAIC trial. J Clin Oncol. 2009;27(19):3109–3116. doi:10.1200/JCO.2008.20.6771
4. Gunderson LL, Jessup JM, Sargent DJ, Greene FL, Stewart AK. Revised TN categorization for colon cancer based on national survival outcomes data. J Clin Oncol. 2010;28(2):264. doi:10.1200/JCO.2009.24.0952
5. Morris M, Platell C, Fritschi L, Iacopetta B. Failure to complete adjuvant chemotherapy is associated with adverse survival in stage III colon cancer patients. Br J Cancer. 2007;96(5):701. doi:10.1038/sj.bjc.6603627
6. André T, Iveson T, Labianca R, et al. The IDEA (International Duration Evaluation of Adjuvant Chemotherapy) collaboration: prospective combined analysis of phase III trials investigating duration of adjuvant therapy with the FOLFOX (FOLFOX4 or modified FOLFOX6) or XELOX (3 versus 6 months) regimen for patients with stage III colon cancer: trial design and current status. Curr Colorectal Cancer Rep. 2013;9(3):261–269.
7. André T, Vernerey D, Mineur L, et al. Three versus 6 months of oxaliplatin-based adjuvant chemotherapy for patients with stage iii colon cancer: disease-free survival results from a randomized, open-label, International Duration Evaluation of Adjuvant (IDEA) France, Phase III Trial. J Clin Oncol. 2018;36(15):1469–1477. doi:10.1200/JCO.2017.76.0355
8. Dobie SA, Baldwin L-M, Dominitz JA, Matthews B, Billingsley K, Barlow W. Completion of therapy by medicare patients with stage III colon cancer. JNCI. 2006;98(9):610–619. doi:10.1093/jnci/djj159
9. Berger AM, Grem JL, Visovsky C, Marunda HA, Yurkovich JM. Fatigue and other variables during adjuvant chemotherapy for colon and rectal cancer. Oncol Nurs Forum. 2010;37(6):E359–69. doi:10.1188/10.ONF.E359-E369.
10. Puetz TW, Herring M. Differential effects of exercise on cancer-related fatigue during and following treatment: a meta-analysis. Am J Prev Med. 2012;43(2):e1–e24.
11. Van JV, Velthuis MJ, Steins CB, et al. Effects of an exercise program in colon cancer patients undergoing chemotherapy. Med Sci Sports Exerc. 2016;48(5):767–775.
12. Dawes HN, Barker KL, Cockburn J, et al. Borg’s rating of perceived exertion scales: do the verbal anchors mean the same for different clinical groups? Arch Phys Med Rehabil. 2005;86(5):912–916.
13. Irlbeck T, Massaro J, Bamberg F, O’Donnell C, Hoffmann U, Fox C. Association between single-slice measurements of visceral and abdominal subcutaneous adipose tissue with volumetric measurements: the Framingham Heart Study. Int J Obes. 2010;34(4):781–787. doi:10.1038/ijo.2009.279
14. De Backer IC, Van Breda E, Vreugdenhil A, Nijziel MR, Kester AD, Schep GJAO. High-intensity strength training improves quality of life in cancer survivors. Acta Oncol. 2007;46(8):1143–1151.
15. Shariati A, Haghighi S, Fayyazi S, Tabesh H,
16. Jeon J, Sato K, Niedzwiecki D, et al. Impact of physical activity after cancer diagnosis on survival in patients with recurrent colon cancer: findings from CALGB 89803/Alliance. Clin Colorectal Cancer. 2013;12(4):233–238.
17. Janssen I, Heymsfield SB, Ross R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J Am Geriatr Soc. 2002;50(5):889–896.
18. Pichard C, Kyle UG, Morabia A, Perrier A, Vermeulen B, Unger P. Nutritional assessment: lean body mass depletion at hospital admission is associated with an increased length of stay. Am J Clin Nutr 2004;79(4):613–618.
19. Cosquéric G, Sebag A, Ducolombier C, Thomas C, Piette F, Weill-Engerer S. Sarcopenia is predictive of nosocomial infection in care of the elderly. Br J Nutr. 2006;96(5):895–901.
20. Awad S, Tan BH, Cui H, et al. Marked changes in body composition following neoadjuvant chemotherapy for oesophagogastric cancer. Clin Nutr. 2012;31(1):74–77.
21. Palle SS, Møllehave LT, Taheri-Kadkhoda Z, et al. Multi-frequency bioelectrical impedance analysis (BIA) compared to magnetic resonance imaging (MRI) for estimation of fat-free mass in colorectal cancer patients treated with chemotherapy. Clin Nutr ESPEN. 2016;16:8–15.
22. Baracos V, Caserotti P, Earthman CP, et al. Advances in the science and application of body composition measurement. JPEN J Parenter Enteral Nutr 2012;36(1):96–107.
23. Lehr S, Hartwig S, Sell H. Adipokines: a treasure trove for the discovery of biomarkers for metabolic disorders. PROTEOMICS–Clin Appl. 2012;6(1‐2):91–101.
24. Tilg H, Moschen AR. Adipocytokines: mediators linking adipose tissue, inflammation and immunity. Nat Rev Immunol. 2006;6(10):772. doi:10.1038/nri1937
25. Konturek P, Brzozowski T, Sulekova Z, Meixner H, Hahn E, Konturek S. Enhanced expression of leptin following acute gastric injury in rat. J Physiol Pharmacol. 1999;50(4):587–595.
26. Aloulou N, Bastuji-Garin S, Le Gouvello S, et al. Involvement of the leptin receptor in the immune response in intestinal cancer. Cancer Res. 2008;68(22):9413–9422. doi:10.1158/0008-5472.CAN-08-0909
27. Diez JJ, Iglesias P. The role of the novel adipocyte-derived hormone adiponectin in human disease. Eur J Endocrinol. 2003;148(3):293–300. doi:10.1530/eje.0.1480293
28. Sugiyama M, Takahashi H, Hosono K, et al. Adiponectin inhibits colorectal cancer cell growth through the AMPK/mTOR pathway. Int J Oncol. 2009;34(2):339–344.
29. Yamaji T, Iwasaki M, Sasazuki S, Tsugane S. Interaction between adiponectin and leptin influences the risk of colorectal adenoma. Cancer Res. 2010;70(13):0008–5472. CAN–0010–0178.
30. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.3.691
31. Cohen J. Statistical Power Analysis for the Behaviors Science.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.