Back to Archived Journals » Open Access Journal of Sports Medicine » Volume 16
Exercise-Associated Hyponatremia: Serum Sodium, Symptomatology, Severity, and Sport Specificity
Authors Armstrong LE ![]() , McDermott BP, Young SL, Casa DJ
, McDermott BP, Young SL, Casa DJ
Received 29 July 2025
Accepted for publication 18 October 2025
Published 15 November 2025 Volume 2025:16 Pages 159—177
DOI https://doi.org/10.2147/OAJSM.S556848
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Andreas Imhoff
Lawrence E Armstrong,1 Brendon P McDermott,2,* Suzanne L Young,3,* Douglas J Casa1,*
1Department of Kinesiology, Korey Stringer Institute, University of Connecticut, Storrs, CT, 06269-1110, USA; 2Department of Health, Human Performance and Recreation, Heat & Hydration Optimization (H2O) Laboratory, University of Arkansas, Fayetteville, AR, 72701, USA; 3Department of Agriculture and Nutrition Science, Southern Utah University, Cedar City, UT, 84720, USA
*These authors contributed equally to this work
Correspondence: Lawrence E Armstrong, Email [email protected]
Abstract: Exercise-associated hyponatremia (EAH) is an important cause of preventable morbidity and mortality. EAH refers to a low blood sodium concentration [Na+] of < 135 mmol·L− 1, during or within 24 h of sustained endurance exercise. The current EAH literature contains ambiguities among field studies and unresolved clinical issues. Seeking clarity and resolution, we conducted manual searches of two large electronic databases using pre-defined inclusion criteria and discovered 1516 article titles and abstracts. Subsequent reviews of 345 full-length articles identified 56 eligible field research studies that reported 220 EAH cases during seven outdoor endurance activities (5– 29.5 h duration). Our evaluations of these EAH cases generated the following seven findings. First, a greater percentage, not the absolute number, of women experienced EAH than men. Second, event specificity may account for much of the wide range of EAH symptoms and signs (SAS) reported among different outdoor activities. Third, out of 220 reported cases of EAH, none were asymptomatic when [Na+] was < 130 mmol·L− 1. Fourth, the absolute value of [Na+] is not a reliable predictive index of EAH clinical severity or presentation. Fifth, running or hiking resulted in far more EAH cases and published epidemiological studies than cycling, swimming, and triathlon events. Sixth, the most common mild EAH complaints were nausea, weakness or lethargy, dizziness, headache, and extremity swelling. Seventh, the most common SAS of moderate-to-severe EAH (ie, suggesting hyponatremic encephalopathy) included altered mental status, vomiting, seizure, agitation/restlessness, collapse, and loss of consciousness. In conclusion, these findings should inform pre-event medical planning, on-site medical staff briefings, as well as the diagnosis of EAH severity in field settings. We also propose that our inventory of position statements and consensus documents will meet the needs of athletes and coaches who seek dependable information regarding risk factors and prevention.
Keywords: encephalopathy, cyclist, runner, swimmer, triathlete, hiker
Introduction
Musculoskeletal and dermatologic injuries are relatively common at outdoor endurance events. Critical, life-threatening medical complications, including exercise-associated hyponatremia (EAH), exertional heatstroke, and cardiac arrest occur less frequently1 but require rapid recognition and appropriate treatment to increase the likelihood of a positive outcome.2–4 To avoid inappropriate treatment and adverse outcomes, care providers in race medical tents and in hospital settings must differentiate EAH from other causes that present with similar signs and symptoms (SAS) such as dehydration, heat exhaustion and exertional heatstroke.4–9 This is essential because advanced cases of EAH may involve non-cardiogenic pulmonary edema, cerebral edema, or death.7,10–13
With few exceptions,14 the decisive diagnostic criterion for EAH in most clinical laboratories is a blood sodium concentration ([Na+]; serum or plasma) below 135 mmol·L−1 which occurs during or up to 24 h after prolonged exercise, regardless of the presence or absence of SAS.3,7,12,15,16 Thus, EAH may appear in either asymptomatic or symptomatic forms; the former can rapidly progress to the latter within a single athletic or recreational activity.11,17 Asymptomatic athletes with [Na+] <135 mmol·L−1 usually are identified while participating in research studies or are detected in blood samples obtained for reasons other than suspicion of EAH. These individuals typically present with nonspecific and transient complaints which are commonly experienced by other participants who do not seek medical care following exercise, and whose [Na+] is rarely analyzed.18–21 In contrast, athletes with symptomatic EAH typically report to race medical facilities or to hospital emergency departments after finishing an event, seeking treatment for a variety of symptoms. Observations of neurologic impairment, seizures, or vomiting should raise the index of suspicion for moderate-to-severe EAH3,6,7,17,19,21 and prompt the measurement of serum [Na+] to confirm or exclude EAH diagnosis.6,7,19,22 However, symptomatology may not reveal the severity of EAH in all athletes. For example, runners who required on-site medical treatment for various complaints (eg, dizziness, headache, vomiting, seizure), were observed by Hsieh et al.14 They reported that no unique sign or symptom distinguished marathon runners with a serum [Na+] <130 mmol·L−1 from those who were normonatremic (>135 mmol·L−1). A similar conclusion was published in a field study of ultramarathoners by Hoffman et.al.23 No SAS distinguished runners who developed EAH along a 161-km course from those not developing EAH. Additional supportive evidence has been reported in the sport of road cycling. The total symptoms score of ultraendurance cyclists, evaluated with a validated symptoms questionnaire, was not statistically correlated to the change of serum [Na+] (range, +6 to −11 mmol·L−1) during a 164-km summer mass participation event.15 These ambiguities indicate that additional focused studies are warranted to clarify EAH SAS and their potential relationships to serum [Na+].
Other important issues regarding EAH remain unresolved. In response, the present narrative review focuses on five clinically relevant but unanswered questions. First, are women at greater risk of experiencing asymptomatic and symptomatic EAH than men? Although field studies have observed that women are at greater risk of experiencing EAH,6,10,24–27 it is important to note that other publications confirm no effect of sex on EAH development.28–34 Second, are EAH signs, symptoms, and serum [Na+] similar during outdoor running, cycling, swimming, and hiking activities? A few previous publications have considered aspects of this question but the scope of those articles was limited.35–38 A corollary of this question is: at which outdoor athletic and recreational activities have no cases of EAH been observed? Third, what is the relationship between serum [Na+] and the SAS of EAH? Fourth, do specific SAS distinguish mild EAH from moderate-to-severe EAH? Fifth, which organizational position statements and expert consensus reports provide readily available information about EAH? Considering the aforementioned discordant findings, ambiguities, and topics that require further investigation, we propose that these five clinically relevant questions will reveal previously unrecognized relationships among symptomatology, EAH severity, [Na+], male-female differences, and the types of outdoor sport activities. These associations can be integrated into a medical support strategy that optimizes decision-making and the treatment of athletes during competitive sports, and recreational enthusiasts at mass participation events.
Terminology
Clarifications of terminology utilized in the present review are necessary. To illustrate, the term “exercise-associated hyponatremia” is preferred; the terms “exercise-induced hyponatremia” and “exertional hyponatremia” do not appear herein. This procedure follows the convention of Wolfson,39 who observed in 1995 that evidence per se does not support the concept that exercise induces this disorder. Also, the lexicon associated with EAH is not universally established. To standardize key terms, we have adopted the following definitions developed in 2014 and 2019 by the Wilderness Medical Society,7,40 and in 2015 by the Third International Exercise-Associated Hyponatremia Consensus Development Conference.19 Thus, we define “exercise-associated hyponatremia” by a serum, plasma, or [Na+] below the normal reference range of 135 mmol·L−1 that occurs during or up to 24 h after prolonged physical activity. “Asymptomatic EAH” relies only on a biochemical determination ([Na+] <135 mmol·L−1), whereas “symptomatic EAH” refers to a biochemical diagnosis combined with clinical SAS.7,40 Further, our manual search of two large electronic databases revealed minor differences among the classification of EAH severity. Hew et al31 delineated three EAH categories in 2003: “mild” (130–135 mmol·L−1), “moderate” (121–129 mmol·L−1), and “critical” (≤120 mmol·L−1). In contrast, three EAH categories included “mild” (130–135 mmol·L−1), “moderate” (125–129 mmol·L−1), and “severe” (<125 mmol·L−1), as compiled from five sources.24,41–44 In the present review, rather than classifying EAH severity on the basis of a concentration range or specific [Na+] values, we aggregate SAS from four sources3,7,19,45 to classify “mild EAH” and “moderate-to-severe EAH” in tables and figures.
Search Methods
Utilizing the vast range of information stored on internet digital media, manual searches for relevant articles were performed in the PubMed and Google Scholar electronic databases. Combinations of the following key words during literature searches emphasized the clinical diagnosis of exercise-associated hyponatremia (EAH) during large group, recreational, or competitive sport disciplines: “exercise-associated hyponatremia”, “exertional hyponatremia”, “exercise-induced hyponatremia”, “cyclist”, “cycling”, “biker”, “biking”, “runner”, “running”, “triathlon”, “triathlete”, “swimmer”, “swimming”, “open water swimming”, “hiker”, “hiking”, “trekker”, “trekking”, “sport” “athlete”, “athletic”. All manual searches included “exercise-associated hyponatremia”, “exertional hyponatremia”, and “exercise-induced hyponatremia” as key words. After removing duplicate records generated by PubMed and Google Scholar, the abstracts and titles of all records were evaluated to determine which studies should be further assessed for eligibility. We then evaluated all articles in portable document format (.pdf) to ascertain if they met the following inclusion criteria: full-text, peer-reviewed, English language, without publication year limits and available through April 24, 2025. Finally, the remaining articles were included in the present review only if (a) data originated at outdoor sport competitions, mass participation events, or recreational activities; (b) each diagnosis of EAH included a measurement of serum or plasma Na+ concentration <135 mmol·L−1;3,7,12,15,16 and (c) clinical SAS (or absence thereof) and the athlete’s sex were described for each case of EAH.
Results
Using the keywords and inclusion criteria described above, the manual screenings of 1516 article titles and abstracts, plus the subsequent reviews of 345 full-length articles, identified the 56 field research studies that were accepted for inclusion in tables and figures. Figure 1 illustrates the steps in this selection process.
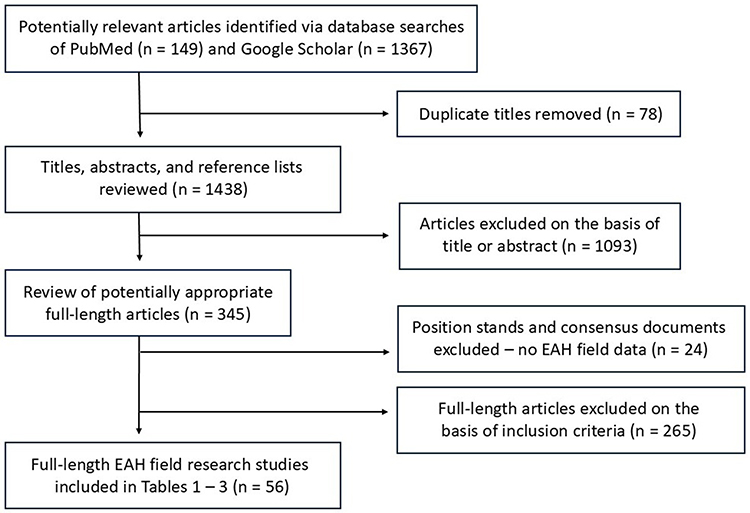 |
Figure 1 The selection process for the field research studies which appear in tables and figures. |
The 220 EAH patients described in Table 1 were diagnosed at 66 different outdoor sport competitions, mass participation events, or recreational activities; column 1 specifies the duration of exercise (h), distance completed (km), and year of these events. Each entry in columns 2–5 describes the serum [Na+] (4 categories), symptomatic or asymptomatic clinical presentation, and the number of female and male patients. Tables 1 and 2 describe the same cyclists, runners, swimmers, triathletes, and hikers.
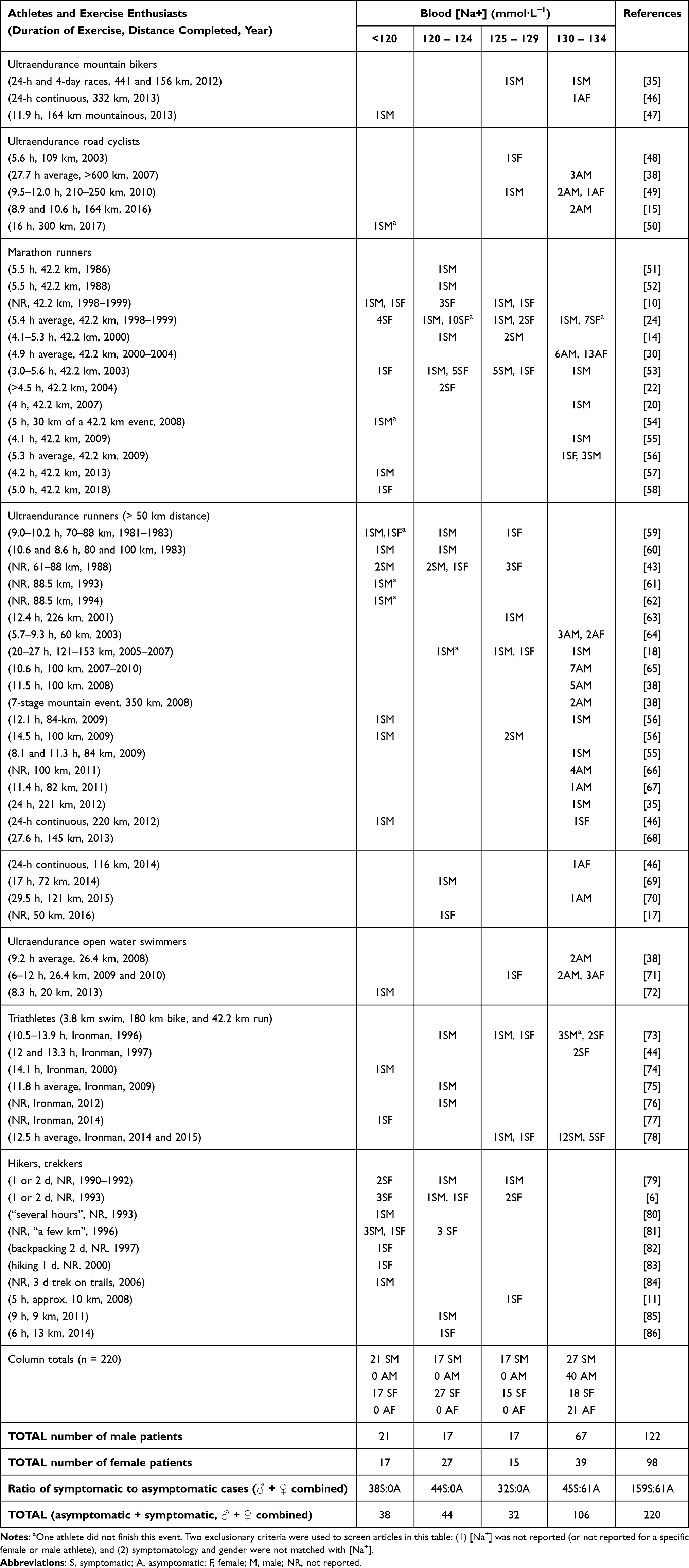 |
Table 1 EAH Cases Associated with Outdoor Sport Competitions, Mass Participation Events, or Recreational Activities. Each Data Point (Columns 2–5) Describes the Blood Sodium Concentration, Number of EAH Patients, Symptomatic or Asymptomatic Clinical Presentation, and Sex of Patients |
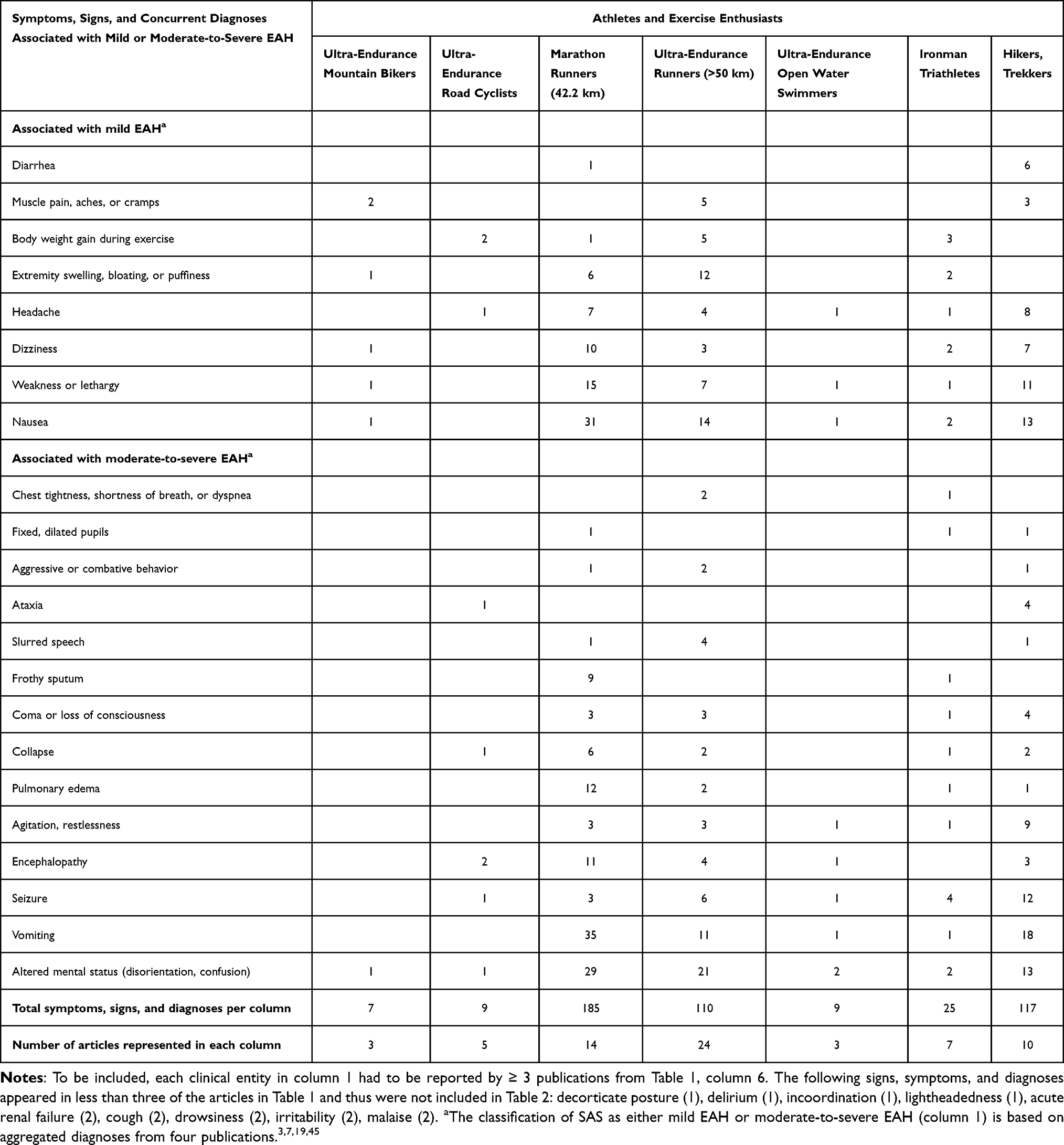 |
Table 2 Number of Symptoms, Signs and Diagnoses Reported Among Cyclists, Runners, Swimmers, Triathletes, and Hikers Who Were Diagnosed with EAH |
Table 2 presents (a) two categories of symptoms, signs, and diagnoses: mild EAH and moderate-to-severe EAH; and (b) the number of times each clinical characteristic was reported. The dual classification of SAS as either mild EAH or moderate-to-severe EAH (Table 2, column 1) was created after articles were screened for inclusion and was based on four publications.3,7,19,45
The associations between [Na+] and specific symptoms, signs, and concurrent diagnoses are shown in Table 3. In a few articles, the [Na+], EAH SAS, or the sex of each athlete could not be matched with each other (ie, not reported); this resulted in some column totals or row totals to be different in Tables 1–3.
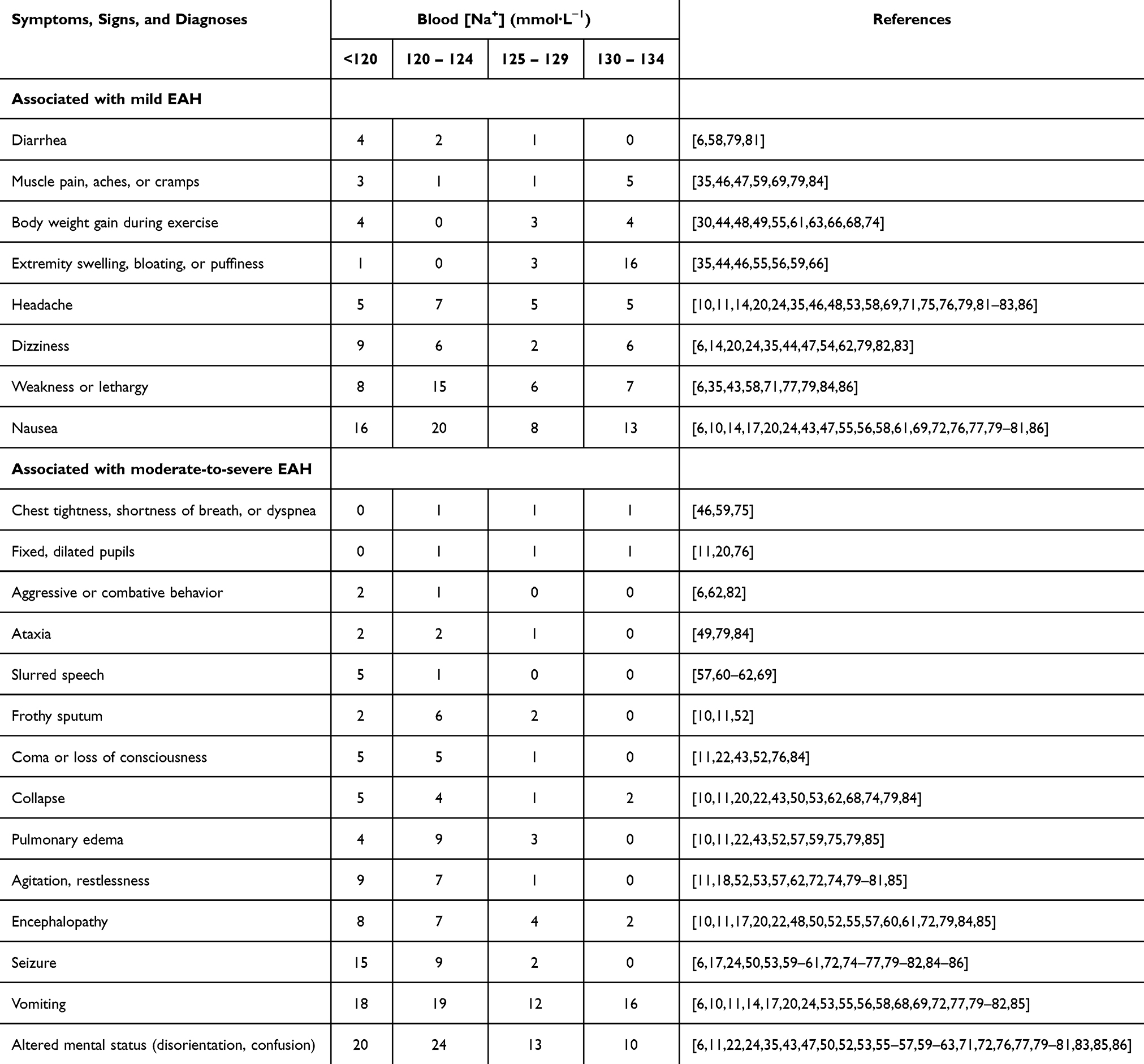 |
Table 3 The Associations of Blood Sodium Concentration with the Symptoms, Signs, and Concurrent Diagnoses of EAH Patients (Seven Sport Disciplines Combined) |
Among the field studies delineated in Tables 1–3, the average number of EAH cases was 3.9. Seventy-nine percent of these studies reported 1–4 EAH cases, and descriptive statistics (ie, height, body mass, exercise time to completion) predominated. Ninety-five percent of these field studies (Tables 1–3) performed no significance testing (eg, t-test or analysis of variance) of EAH patients versus athletes without EAH. Two figures allow an assessment of EAH symptomatology. First, Figure 2 offers a visual comparison of the most common SAS of EAH (≥10 reports minimum, females and males combined) observed in seven outdoor events. This figure visually summarizes the data in Table 2. SAS are depicted in two categories: mild and moderate-to-severe. Second, Figure 3 depicts the number of asymptomatic and symptomatic EAH cases reported (females and males combined, seven outdoor events combined). This figure visually summarizes the data in Table 1. The numeric values above each bar indicate the ratio of asymptomatic-to-symptomatic cases. Females comprised the following percentages of EAH cases (asymptomatic and symptomatic combined) in Figure 3: <120 mmol·L−1, 44.7%; 120–124 mmol·L−1, 61.4%; 125–129 mmol·L−1, 46.9%; 130–134 mmol·L−1, 36.8%; and total EAH cases (all [Na+] categories, n = 220), 44.5%.
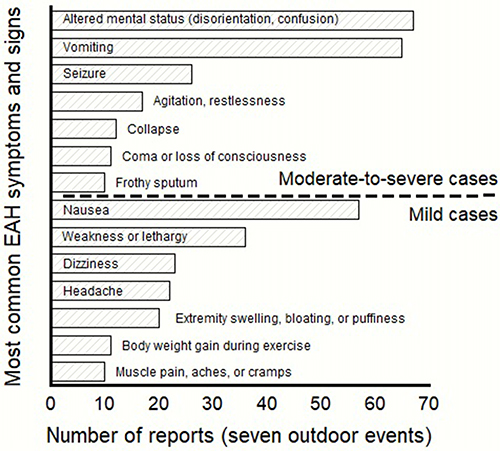 |
Figure 2 Most common SAS associated with EAH. |
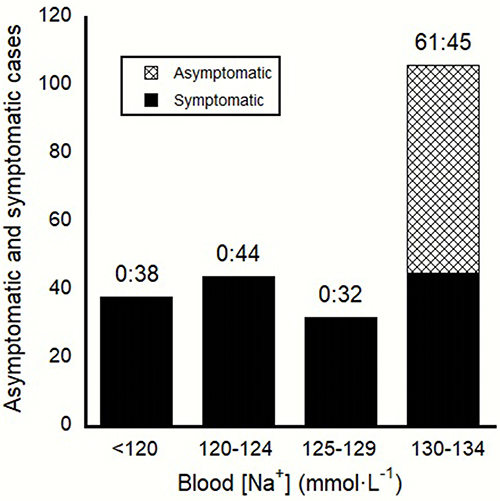 |
Figure 3 Number of asymptomatic and symptomatic EAH cases at different blood [Na+]. |
Table 4 provides a compilation of 24 outdoor events at which no case of asymptomatic or symptomatic EAH was observed between the years 1970 and 2025. Although Table 1 demonstrates that EAH was diagnosed in 220 patients at 66 different outdoor events, Table 4 demonstrates that EAH is not diagnosed at all athletic competitions and mass participation events.
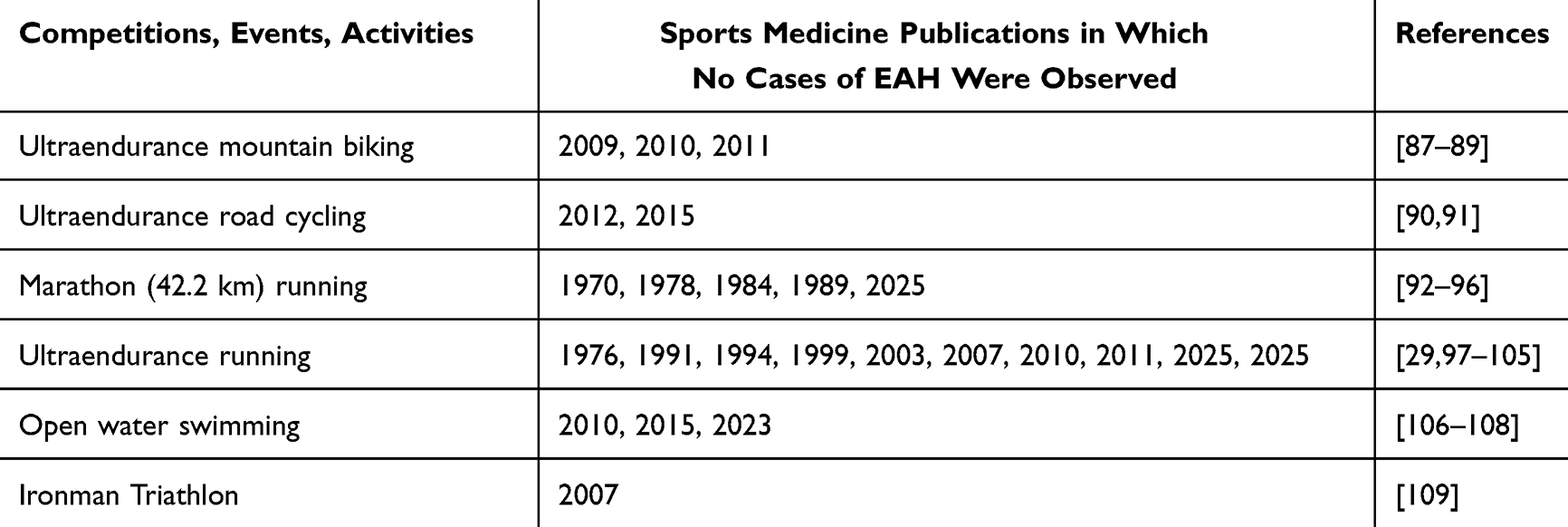 |
Table 4 Twenty Four Outdoor Sport Competitions and Mass Participation Events Where No Case of Asymptomatic or Symptomatic EAH Was Observed (1970–2025) |
Table 5 presents a guide to six aspects of EAH (columns 3–8). These topics were published by professional sports medicine organizations and consensus writing groups (2006–2021). The information in these 11 articles provides readily available online information for clinicians and physiologists, as well as athletes and coaches.
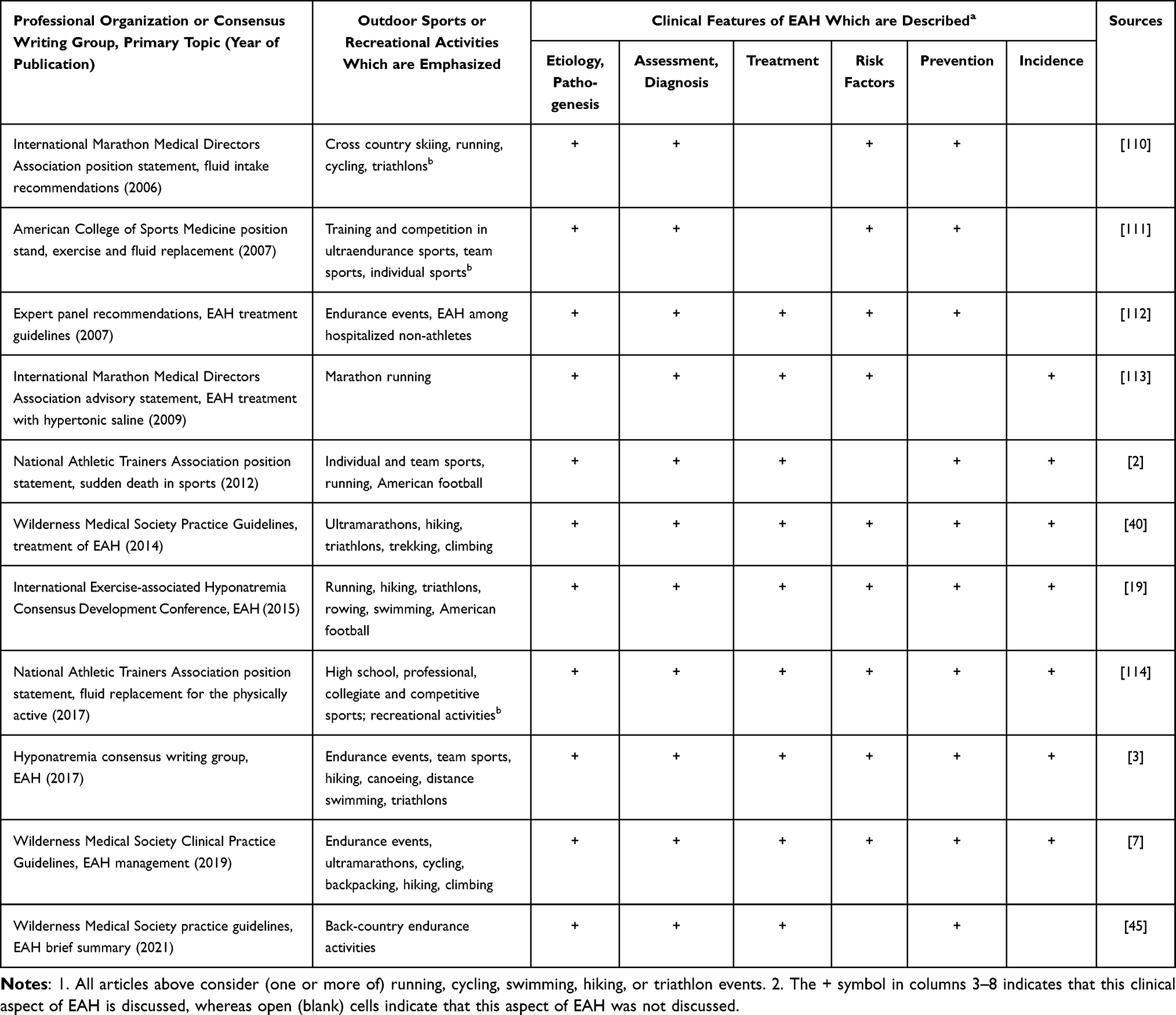 |
Table 5 Position Statements of Professional Sports Medicine Organizations and Consensus Documents of Expert Writing Groups That Describe Relevant Clinical Aspects of EAH |
Discussion
The mechanisms by which EAH develops, progresses, and either persists or is resolved are complex, and involve whole-body water and sodium imbalances.3,115 Although multiple overlapping EAH etiologies have been identified,3,15,115,116 their differences have impeded universal agreement regarding the mechanisms and symptoms involved.3,7,15,117–119 Nevertheless, our extensive manual search of electronic databases (Figure 1) indicates that the following two concepts are widely accepted by clinicians and physiologists. First, an increased ratio of total body water volume relative to the amount of solute in the extracellular compartment (ie, total body exchangeable sodium) is the primary pathogenic cause of asymptomatic and symptomatic EAH.6,28,31,41,81,112,116,120 This complex, dynamic clinical condition may result from excessive fluid intake (ie, exceeding the volume of sweat secreted), a large sodium loss in sweat, inappropriate mobilization of internal sodium stores, and/or inappropriately elevated blood arginine vasopressin concentration (ie, renal water retention which lowers [Na+]).7,19,112,116,121 Second, asymptomatic or mild cases of EAH can progress rapidly to severe and life-threatening encephalopathy. Thus, symptomatic EAH requires prompt recognition, initial resuscitation, and rapid treatment to minimize morbidity.2,7,19,22,112 This necessitates that the on-site medical team be aware of common EAH SAS and recognize those which characterize both mild and severe cases. Unlike these two widely accepted concepts, our online search of electronic databases revealed important clinical issues regarding EAH that have not been adequately resolved or investigated.115 In response, the following paragraphs examine five questions which are relevant to EAH diagnosis and the care of athletes and recreational enthusiasts in field settings.
Are Women at Greater Risk of Experiencing Asymptomatic and Symptomatic EAH Than Men?
Although numerous risk factors for EAH have been proposed,7,26,30,115,122 it is important to acknowledge that the identification of risk factors implies a correlation with higher rates of EAH, but not necessarily causation or an independent association with EAH.122 Regarding the influence of biological sex, behavioral characteristics, and physiological differences, multiple field research teams have reported that women are at greater risk of experiencing EAH than men,6,10,24–27 whereas other investigators observed no effect of sex on EAH development in athletes.28–34 The fact that the existing EAH literature consists primarily of studies with limited sample sizes (ie, case reports) impedes the clarification of differences between the sexes.26 This current state of the existing literature is addressed in Table 1. The 220 EAH cases in this table were diagnosed at 66 different outdoor sport competitions, mass participation events, or recreational activities. These cases included 98 females and 122 males, initially suggesting that men have a greater risk of experiencing EAH than women. In terms of clinical assessment, women comprised 48.4% of all symptomatic cases and 34.4% of asymptomatic cases in Table 1. However, in the majority of endurance and ultraendurance events, the number of female competitors is less than male competitors. In 2013, for example, Chlibková et al29 noted that the proportion of females among ultrarunners was 10–20%.123 Subsequently, the worldwide participation trends of ultraendurance competitors were reviewed by Scheer.124 He reported the following proportion of females among the total number of finishers, at various running distances: 50 km, 29.2%; 100 km, 15.3%; 100 mi, 19.1%; and 24-h races, 23.1%. Scheer also reported that women accounted for approximately 32% of all finishers in ultradistance open water swimming—a high percentage when compared to other endurance events. In addition, a field study of Ironman triathlon competitors published in 2023 by Johnson et al prospectively examined three decades of medical records (1989–2019; 53,355 total entrants).26 They discovered that 9,482 athletes sought medical attention for a variety of medical complaints. The athletes who were diagnosed with EAH (n = 740) represented 29.7% of all women and 21.2% of all men who had serum [Na+] analyzed (n = 3,138). These data suggested that a greater percentage, not the absolute number, of women experienced EAH than men.26,28 Unfortunately, because few of the articles in Table 1 reported the total number of male and female race participants, we recommend that future field studies examine this matter.
The column totals shown in the bottom rows of Table 1 demonstrate that, when all levels of [Na+] are considered, symptomatic EAH was diagnosed in 77 women and 82 men, whereas asymptomatic EAH was experienced by 21 women and 40 men. Clearly, the majority of cases in Table 1 involve symptomatic EAH, for both men and women. This finding (a) agrees with the previously published guidelines of the Wilderness Medical Society,40 and (b) likely occurs because athletes with asymptomatic EAH typically present with nonspecific and transient complaints which are commonly experienced by others who do not seek medical care.18–21 However, this finding opposes an observation published by an expert consensus development team.19 That group concluded that symptomatic EAH is rare and occurs with considerably less frequency than asymptomatic EAH. We interpret this disparity to be the result of an analysis that involved a smaller sample of EAH cases (ie, often from a single sport discipline) than the 220 EAH cases described in Table 1.
To clarify the aforementioned uncertainties, a more comprehensive understanding of the influence of biological sex can be derived from a longitudinal study design versus a cross-sectional design (ie, which is utilized in most EAH studies). The former would involve making several observations of the same athletes across several years. The latter would involve comparing different groups of athletes at a single point in time such as an outdoor endurance event. Specifically, we recommend prospective cohort studies as an alternative to retrospective case reports, as a means of overcoming biases in subsequent research. These prospective cohort studies would involve collecting data over time to compare the occurrence of EAH in women and men. However, we acknowledge that prospective cohort studies (a) require access to a large pool of research subjects who agree to be followed longitudinally (ie, across many endurance events), (b) can be very costly/time consuming, and (c) may result in bias due to test subject attrition.
Are EAH Signs, Symptoms, and [Na+] Similar During Outdoor Running, Cycling, Swimming, Triathlon, and Hiking Activities?
Our manual search of electronic databases (Figure 1) determined that three epidemiological studies and one narrative review previously considered some aspects of this question, but the scope of those articles was limited. In total, these three field studies35,36,38 described 28 EAH cases that occurred during competitive ultra running, road cycling, ultra mountain biking, and ultra swimming. The single narrative review article focused on EAH prevalence during swimming, cycling, running, triathlons, and multi-day stage events but did not compare similarities and differences of signs, symptoms, or [Na+] among these sports. In contrast, Tables 1 and 2 offer a comprehensive view of symptomatic EAH, asymptomatic EAH, [Na+], SAS, and concurrent diagnoses that were observed during seven different outdoor events. This comprehensive approach has value because 91% of the previously published articles in Table 1 involved medical encounters during a single sport or recreational activity.
Due to the distinctive fluid-electrolyte perturbations (ie, deficits or excesses) and stressors (ie, venue, terrain, ambient temperature) which athletes experience in various sports, it is possible that EAH SAS and the [Na+] in blood are unique to some or all athletic disciplines. If true, event specificity could account for much of the wide range of EAH SAS or prevalences reported among sport and recreational activities.3,7,28,37 Indeed, Tables 1 and 2 provide evidence for event specificity in four ways. First, all 33 cases of EAH in triathletes, and all 25 cases of EAH in hikers/trekkers, were symptomatic (Table 1). Of the remaining five sports, none exhibited a similar symptomatic-to-asymptomatic ratio. Second, the number of EAH cases (columns 2–5) and publications (column 6) in Table 1 was greatest in marathons and ultramarathons. This likely was influenced by the large number of participants and running events worldwide. Third, few cases of EAH in Table 1 occurred among mountain bikers and road cyclists. This observation supports a previous review of cyclists37 in which a low prevalence of EAH was reported in 10 field studies. Those authors and others121,125 have observed that cycling is unique in that, unlike runners, cyclists carry nutrition on their bicycle frame and in their jersey pockets, thereby modulating their individual fluid needs. Supporting the concept of event specificity in a parallel clinical domain, the incidence of hyperthermia and exertional heatstroke are considerably lower in cyclists and open water swimmers than among endurance runners and triathletes,126 due to differences of heat dissipation from skin to air or water. Fourth, no case of mild EAH (ie, [Na+] of 130–134 mmol·L−1) in Table 1 occurred among hikers and trekkers. We interpret this to be an example of individuals who experienced nonspecific and transient complaints which are commonly experienced by others who do not seek medical care after endurance exercise. As a result, their [Na+] was not analyzed and their asymptomatic EAH went unrecognized.
The following corollary question provides additional relevant information: at which outdoor athletic and recreational activities have no cases of EAH been observed? Table 1 summarizes 220 EAH patient diagnoses at 66 different outdoor events, between the years 1981–2018. However, Table 4 establishes that EAH was not reported at 24 outdoor events which spanned more than a half century (1970–2025). These competitive and mass participation events included mountain biking, road cycling, open water swimming, Ironman triathlons, marathon and ultraendurance running.
What is the Relationship Between Serum [Na+] and the SAS of EAH?
The reduced extracellular [Na+] and total osmolality that is characteristic of EAH may result in an abnormally large shift of water into the confined space of the skull. In advanced cases, this can develop into hyponatremic encephalopathy, herniation, depression of the respiratory center, or death.7,19,20 However, previously published clinical studies have not clarified the SAS of EAH at different levels of [Na+], likely because multiple EAH mechanisms have been identified116 and because idiosyncratic etiologies have been reported among endurance athletes with similar post-exercise [Na+].15 Further complicating this complexity, the number of EAH cases at any single event typically is small (Table 1), making it difficult to statistically evaluate the relationship between serum [Na+] and EAH SAS. As evidence of this, Table 1 shows that (a) an average of 3.3 EAH cases were diagnosed at each of the 66 outdoor sport competitions, mass participation events, or recreational activities; and (b) more than half (53.0%) of the studies in column 6 reported only 1 case of EAH.
Figure 3 depicts 220 asymptomatic and symptomatic EAH cases (representing the seven endurance activities in Table 1), at different levels of [Na+]. This figure demonstrates that 61 asymptomatic patients had a [Na+] of 130–134 mmol·L−1, and that 45 symptomatic patients also were within this range. The fact that no asymptomatic EAH case, in seven different activities, involved a verified [Na+] of <130 mmol·L−1 suggests that this concentration represents the lower boundary of asymptomatic cases. This observation supports the 2014 Wilderness Medical Society practice guidelines for the treatment of EAH40 and two narrative review articles,27,127 which indicated that patients with a [Na+] ≥130 mmol·L−1 generally are either minimally symptomatic or asymptomatic. In fact, the information in Figure 3 closely resembles a figure published by Speedy et al in 1999,127 depicting 40 hyponatremic ultradistance triathletes.
Two additional considerations are relevant. First, the aforementioned Wilderness Medical Society guidelines40 state that symptomatic EAH (ie, a biochemical analysis of [Na+] combined with clinical SAS) has a much lower incidence than asymptomatic EAH.40 Combining seven different outdoor activities, our Figure 3 refutes this conclusion in that the number of symptomatic EAH cases is 2.6 times greater than the number of asymptomatic cases (159:61 ratio). Second, the number of symptomatic cases in Figure 3 did not differ greatly across the four [Na+] categories depicted. This finding supports multiple authorities19,45,55,128,129 who concluded that the absolute value of [Na+] is not a reliable predictive index of EAH clinical severity.
Table 3 suggests that only a portion of EAH SAS is observed more frequently as [Na+] progressively decreases. Our visual inspection of the right-to-left trends in columns 2–5 of Table 3 (ie, representing decreasing [Na+]) suggests that the following EAH SAS (ie, total number of reports in parentheses) trend toward supporting this paradigm: diarrhea (7), aggressive or combative behavior (3), ataxia (5), slurred speech (6), coma or loss of consciousness (11), collapse (12), agitation or restlessness (17), seizure (26), and altered mental status (67). Regarding mild EAH, 87.5% (7/8) of the SAS (upper eight rows of Table 3) were not observed more frequently as [Na+] progressively decreased. Regarding moderate-to-severe EAH (lower 14 rows of Table 3), 57.1% (8/14) of the SAS increased when [Na+] progressively decreased; all of these were associated with cognitive function and central nervous system control of bodily functions. Therefore, we recommend that medical teams covering outdoor endurance activities employ selected SAS from Table 3 to create an a priori medical staff plan that optimizes field diagnosis and treatment of EAH. This plan should consider (a) the sport discipline involved (Table 2) and event specificity (described above), plus (b) a review of athlete medical records (ie, common SAS associated with EAH) from previous years.
Do Specific SAS Distinguish Mild EAH from Moderate-to-Severe EAH?
The SAS associated with EAH depend on both the magnitude of the serum sodium decrease as well as the rate at which this decrease occurs,19,40,128,129 because both phenomena alter intracellular-extracellular homeostasis.130–133 The complex interactions of these two deviations (ie, magnitude and rate of change), plus inter-individual differences among athletes and sport-specific stressors, make it difficult to predict the clinical severity of EAH solely on the basis of [Na+].19,45,55,127,128 As a result, clinicians often evaluate neurological SAS when considering a diagnosis of encephalopathy or severe EAH.10,22,24,40,60,134 Therefore, in the present review, we have aggregated SAS from four harmonized sources3,7,19,45 to distinguish “moderate-to-severe EAH” from “mild EAH” cases. Figure 2, Tables 2, and 3 follow this convention and provide novel information to assist the interpretation of EAH severity. Regarding these data, we present three clarifications. First, the classification of SAS as “mild” and “moderate-to-severe” represents a clinical paradigm. These two classes of SAS are not mutually exclusive; they may exist concurrently. Second, it is likely that the order/timing of SAS appearance will vary from one patient to another. This means that some moderate-to-severe SAS may appear before mild SAS. Third, the observations of SAS in Figure 2, Tables 2, and 3 were not guided by the same clinical survey or SAS checklist. This suggests that (a) considerable diagnostic variability existed among event medical teams, and (b) recognition of SAS relied on the various past encounters of medical team members with EAH patients. Thus, we recommend that EAH be considered as a differential diagnosis when common EAH SAS are recognized.
Figure 2 allows evaluation of the most common EAH SAS (women and men combined) from Table 2 that were observed at seven different outdoor events. The mild EAH cases (lower half of Figure 2) often involved nonspecific and transient complaints which are commonly experienced by others who do not seek medical care following strenuous endurance exercise (eg, fatigue, presyncope, or dizziness).18–21 The most common “mild EAH” complaints in Figure 2 were nausea, weakness or lethargy, dizziness, and headache. The most common SAS of “moderate-to-severe EAH” included altered mental status, vomiting, seizure, agitation/restlessness, collapse, and loss of consciousness. Because these neurological SAS suggest possible hyponatremic encephalopathy,7,19,20 we recommend that future field studies focus on the interactive associations among observed SAS (Figure 2) and long-term outcomes, especially for athletes who exhibit severe SAS (Tables 2 and 3). In future longitudinal studies (ie, involving months and years of observations) it will be important to recognize that neurologic impairment, seizures, or vomiting raise the index of suspicion for moderate-to-severe EAH.3,6,7,17,19,21
Table 2 is structured so that the SAS associated with both mild and moderate-to-severe EAH can be compared across each of the seven outdoor events. The column totals (bottom two rows) in Table 2 indicate that upright exercise resulted in far more EAH cases and published epidemiological studies than cycling, swimming, and triathlon events. Specifically, marathons, ultramarathons, and hiking (ie, all weight-bearing activities) accounted for 89.2% (412/462) of all EAH cases in Table 2. To our knowledge, no previous publication has recognized or provided a hypothetical explanation for this phenomenon. Thus, we propose that the association between EAH prevalence and upright exercise warrants future epidemiological research to determine the underlying mechanisms and influential factors. Considering non-weight-bearing exercise, the fewest diagnoses (ie, and the fewest publications) of EAH occurred among mountain bikers, road cyclists, and open water swimmers. This observation supports a previous review involving cyclists,37 in which a low prevalence of EAH was reported in 10 field studies. Our manual search of online databases discovered no comparable review of ultraendurance open water swimming.
Which Organizational Position Statements and Expert Consensus Reports Provide Readily Available Information About EAH?
Table 5 presents a guide to various aspects of EAH (columns 3–8) that are available in four position statements prepared by professional sports medicine organizations, and in seven expert reports produced by consensus writing groups (2006–2021). This table serves as a resource for physicians, physician assistants, and nurses who require detailed information regarding the etiology, diagnosis, and treatment of EAH, as indicated in columns 3–5. Athletes and coaches may seek information regarding EAH risk factors and the prevention of EAH, as summarized in columns 6 and 7. By consulting the articles in Table 5, readers will discover that clinicians at outdoor endurance events must differentiate EAH from other causes that present with similar SAS (ie, dehydration, heat exhaustion, exertional heatstroke).4–9 This is vital because appropriate treatment varies among these disorders and because asymptomatic or mild cases of EAH can progress rapidly to severe and life-threatening encephalopathy.7,10–13 Also, athletes and coaches can benefit from the documents in Table 5 by reviewing (a) the expert recommendations regarding fluid intake during endurance exercise, and (b) preventive strategies (eg, pre-race education, body weight scales at check points, nutrition and fluid types at aid stations). These guidelines often are tailored to meet the unique characteristics of specific sports.
Limitations
The findings of the present review may be subject to the methodological limitations of the 56 field research studies that were selected for inclusion (Figure 1). We acknowledge the following potential limitations. First, no case of mild EAH (ie, serum [Na+] of 130–134 mmol·L−1) in Table 1 occurred among hikers and trekkers. This may have resulted from their nonspecific and transient complaints, which are commonly experienced by others who do not seek medical care after endurance exercise. As a result, their serum [Na+] may not have been measured, and their asymptomatic EAH may have gone unrecognized. The influence of this factor on the other six sport disciplines in Table 1 is unknown. Second, due to the vast distances between the course starting line and finish line in numerous point-to-point ultraendurance events, those field studies did not report the data of individuals who dropped out along the course or bypassed patient care at event medical facilities. Third, few of the field studies in Table 1 reported the EAH cases of athletes who became ill up to 24 h after leaving the event venue. As a result, the number of EAH cases may be greater than reported, at numerous outdoor endurance events. Fourth, the number of EAH cases in Figure 3 and Tables 2–4 may have been biased by either unpublished EAH cases, or the recognition of a high prevalence of EAH cases, in specific sport disciplines. For example, the medical teams covering mountain biking, road cycling, and open water swimming events may have been less inclined to publish EAH field studies, when compared to the medical teams covering marathon and ultramarathon events. Fifth, preventive strategies (eg, pre-race education, body weight scales at check points, nutrition and fluid types at aid stations) often vary and may have contributed to the varying incidence among outdoor events. Sixth, we did not examine actual case outcomes or predicted outcomes (eg, based on SAS or presentation severity) because the requisite information was not described. Therefore, we recommend that future epidemiological studies act to counteract these potential limitations by (a) discriminating nonspecific and transient complaints from neurological SAS that suggest a diagnosis of EAH, (b) utilizing a standardized SAS survey or checklist that is specific to the sport discipline involved, (c) providing on-site instrumentation that measures serum [Na+] when EAH is suspected, (d) identifying competitors who drop out or bypass patient care, and (e) publishing the relevant medical information of all EAH diagnoses. Seventh, although a considerable number of risk factors for EAH have been proposed,7,26,30,115,122 the identification of additional risk factors could benefit athletes, medical teams, and race directors at outdoor events. These factors could include hydration practices (eg, individualized planned drinking), environmental conditions, and athlete characteristics (eg, age, fitness level, body mass index). We recommend that future field studies evaluate these and other potential risk factors.
Conclusion
EAH symptom recognition is challenging due to the interactions of multiple complex factors, especially the dynamic relationship between serum [Na+] and symptomatology. Ambiguities and unresolved clinical issues also exist regarding athlete sex as a risk factor, undefined inter-individual differences among athletes, and event-specific stressors. Our review of previously published EAH epidemiological studies prompted us to focus on five clinically relevant questions. Our responses to these questions are unique because they represent 220 EAH patients at 66 different outdoor events, whereas most previous EAH reports involved a small number of athletes who participated in a single outdoor event. Because these patients participated in seven different endurance activities, the present review provides a unique, wide-ranging overview of EAH. It is therefore relevant that severe EAH, verified by a [Na+] <120 mmol·L−1, occurred in all of the seven sport and recreational activities. We propose that the information provided in this review will inform future pre-event medical planning, on-site medical staff briefings, as well as the diagnosis and treatment of EAH in field settings. We also propose that our compilation of readily available position statements and consensus documents will inform athletes and coaches who seek detailed information regarding EAH risk factors and the prevention of EAH.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this review.
Disclosure
DJC declares receiving honoraria from Gatorade for speaking engagements and consulting activities. Gatorade is a corporate partner of the Korey Stringer Institute, University of Connecticut, where DJC serves as the Chief Executive Officer. He also reports research grant funding from Liquid IV and personal fees from Clif Bar as a consultant. All authors declare no other conflicts of interest in this work.
References
1. Breslow RG, Giberson-Chen CC, Roberts WO. Burden of injury and illness in the road race medical tent: a narrative review. Clin J Sport Med. 2021;31(6):e499–e505. doi:10.1097/JSM.0000000000000829
2. Casa DJ, Guskiewicz KM, Anderson SA, et al. National athletic trainers’ association position statement: preventing sudden death in sports. J. Athl. Train. 2012;47(1):96–118. doi:10.4085/1062-6050-47.1.96
3. Hew-Butler T, Loi V, Pani A, Rosner MH. Exercise-associated hyponatremia: 2017 update. Front Med. 2017;421. doi:10.3389/fmed.2017.00021
4. Lipman GS, Gaudio FG, Eifling KP, Ellis MA, Otten EM, Grissom CK. Wilderness medical society clinical practice guidelines for the prevention and treatment of heat illness: 2019 update. Wilderness Environ Med. 2019;30(4):S33–S46. doi:10.1016/j.wem.2018.10.004
5. Armstrong LE. Heat Exhaustion. Adams WM, Jardine J, eds.:Exertional Heat Illness: A Clinical and Evidence-Based Guide. Springer Nature: 2020. 81–115:chap5.
6. Backer HD, Shopes E, Collins SL, Barkan H. Exertional heat illness and hyponatremia in hikers. Am J Emergency Med. 1999;17(6):532–539. doi:10.1016/s0735-6757(99)90191-2
7. Bennett BL, Hew-Butler T, Rosner MH, Myers T, Lipman GS. wilderness medical society clinical practice guidelines for the management of exercise-associated hyponatremia: 2019 update. Wilderness Environ Med. 2020;31(1):50–62. doi:10.1016/j.wem.2019.11.003
8. Binkley HM, Beckett J, Casa DJ, Kleiner DM, Plummer PE. National athletic trainers’ association position statement: exertional heat illnesses. J. Athl. Train. 2002;37(3):329–343.
9. Jerome D, Divito B. Just the facts: exercise-associated hyponatremia. Can. J. Emergency Med. 2025;27(1):11–13. doi:10.1007/s43678-024-00765-6
10. Ayus JC, Varon J, Arieff AI. Hyponatremia, cerebral edema, and noncardiogenic pulmonary edema in marathon runners. Ann Internal Med. 2000;132(9):711–714. doi:10.7326/0003-4819-132-9-200005020-00005
11. Myers TM, Hoffman MD. Hiker fatality from severe hyponatremia in grand canyon national park. Wilderness Environ Med. 2015;26(3):371–374. doi:10.1016/j.wem.2015.03.001
12. Owen BE, Rogers IR, Hoffman MD, et al. Efficacy of oral versus intravenous hypertonic saline in runners with hyponatremia. J Sci Med Sport. 2014;17(5):457–462. doi:10.1016/j.jsams.2013.09.001
13. Veniamakis E, Kaplanis G, Voulgaris P, Nikolaidis PT. Effects of sodium intake on health and performance in endurance and ultra-endurance sports. Int J Environ Res Public Health. 2022;19(6):3651. doi:10.3390/ijerph19063651
14. Hsieh M, Roth R, Davis DL, Larrabee H, Callaway CW. Hyponatremia in runners requiring on-site medical treatment at a single marathon. Med Sci Sports Exercise. 2002;34(2):185–189. doi:10.1097/00005768-200202000-00001
15. Armstrong LE, Lee EC, Casa DJ, et al. Exertional hyponatremia and serum sodium change during ultraendurance cycling. Int J Sport Nutr Exerc Metab. 2017;27(2):139–147. doi:10.1123/ijsnem.2016-0135
16. Montain SJ. Strategies to prevent hyponatremia during prolonged exercise. Curr. Sports Med. Rep. 2008;7(4):S28–S35. doi:10.1249/JSR.0b013e31817f3a64
17. Pomeranz D, Irwin C, Lipman GS. Large-volume hypertonic saline for empiric treatment of severe exercise-associated hyponatremia in an ultramarathon runner. Curr. Sports Med. Rep. 2019;18(5):163–165. doi:10.1249/JSR.0000000000000593
18. Cuthill JA, Ellis C, Inglis A. Hazards of ultra-marathon running in the Scottish Highlands: exercise-associated hyponatraemia. Emer Med J. 2009;26(12):906–907. doi:10.1136/emj.2008.065524
19. Hew-Butler T, Rosner MH, Fowkes-Godek S, et al. Statement of the third international exercise-associated hyponatremia consensus development conference,
20. Petzold A, Keir G, Appleby I. Marathon related death due to brainstem herniation in rehydration-related hyponatraemia: a case report. J. Med. Case Rep. 2007;1:1–7. doi:10.1186/1752-1947-1-186
21. Stuempfle KJ, Lehmann DR, Case HS, et al. Hyponatremia in a cold weather ultraendurance race. Alaska Med. 2002;44(3):51–55.
22. Siegel AJ, Verbalis JG, Clement S, et al. Hyponatremia in marathon runners due to inappropriate arginine vasopressin secretion. Am J Med. 2007;120(5):461.e11–461.e17. doi:10.1016/j.amjmed.2006.10.027
23. Hoffman MD, Fogard K, Winger J, Hew-Butler T, Stuempfle KJ. Characteristics of 161-km ultramarathon finishers developing exercise-associated hyponatremia. Res Sports Med. 2013;21(2):164–175. doi:10.1080/15438627.2012.757230
24. Davis DP, Videen JS, Marino A, et al. Exercise-associated hyponatremia in marathon runners: a two-year experience. J Emergency Med. 2001;21(1):47–57. doi:10.1016/s0736-4679(01)00320-1
25. Hew TD. Women hydrate more than men during a marathon race. Clin J Sports Med. 2005;15(4):148–153. doi:10.1097/01.jsm.0000157652.47572.56
26. Johnson KB, Connolly CP, Cho SP, Miller TK, Sallis RE, Hiller WDB. Clinical presentation of exercise-associated hyponatremia in male and female Ironman triathletes over three decades. Scand J Med Sci Sports. 2023;33(9):1841–1849. doi:10.1111/sms.14401
27. Speedy DB, Noakes TD, Schneider C. Exercise-associated hyponatremia: a review. Emergency Med. 2001;13(1):17–27. doi:10.1046/j.1442-2026.2001.00173.x
28. Almond CS, Shin AY, Fortescue EB, et al. Hyponatremia among runners in the Boston Marathon. N Engl J Med. 2005;352(15):1550–1556. doi:10.1056/NEJMoa043901
29. Chlibkova D, Filipenska M, Knechtle B, et al. No hyponatremia despite continuous plasma sodium decline in female runners during a seven stage ultramarathon. Sci Rep. 2025;15(1):11400. doi:10.1038/s41598-025-90987-0
30. Chorley J, Cianca J, Divine J. Risk factors for exercise-associated hyponatremia in non-elite marathon runners. Clin. J. Sport Med. 2007;17(6):471–477. doi:10.1097/JSM.0b013e3181588790
31. Hew TD, Chorley JN, Cianca JC, Divine JG. The incidence, risk factors, and clinical manifestations of hyponatremia in marathon runners. Clin. J. Sport Med. 2003;13(1):41–47. doi:10.1097/00042752-200301000-00008
32. Hoffman MD, Stuempfle KJ, Rogers IR, Weschler LB, Hew-Butler T. Hyponatremia in the 2009 161-km Western States Endurance Run. Int. J. Sports Physiol. Perform. 2012;7(1):6–10. doi:10.1123/ijspp.7.1.6
33. Kipps C, Sharma S, Tunstall Pedoe D. The incidence of exercise-associated hyponatraemia in the London marathon. Br. J. Sports Med. 2011;45(1):14–19. doi:10.1136/bjsm.2009.059535
34. Rüst CA, Knechtle B, Joleska I, et al. Is the prevalence of exercise-associated hyponatremia higher in female than in male 100-KM ultra-marathoners? Human Movement. 2012;13(2):94–101. doi:10.2478/v10038-012-0009-2
35. Chlibkova D, Knechtle B, Rosemann T, Zakovska A, Tomaskova I. The prevalence of exercise-associated hyponatremia in 24-hour ultra-mountain bikers, 24-hour ultra-runners and multi-stage ultra-mountain bikers in the Czech Republic. J Int Soc Sports Nutr. 11(1):1–17. doi:10.1186/1550-2783-11-3
36. Chlíbková D, Rosemann T, Posch L, Matoušek R, Knechtle B. Pre-and post-race hydration status in hyponatremic and non-hyponatremic ultra-endurance athletes. Chin J Physiol. 2016;59(3):173–183. doi:10.4077/CJP.2016.BAE391
37. Knechtle B, Chlibkova D, Papadopoulou S, Mantzorou M, Rosemann T, Nikolaidis PT. Exercise-associated hyponatremia in endurance and ultra-endurance performance-aspects of sex, race location, ambient temperature, sports discipline, and length of performance: a narrative review. Medicina. 2019;55(9):537. doi:10.3390/medicina55090537
38. Knechtle B, Gnadinger M, Knechtle P, et al. Prevalence of exercise-associated hyponatremia in male ultraendurance athletes. Clin. J. Sport Med. 2011;21(3):226–232. doi:10.1097/JSM.0b013e31820cb021
39. Wolfson AB. Acute hyponatremia in ultra-endurance athletes. Am J Emergency Med. 1995;13(1):116–117. doi:10.1016/0735-6757(95)90280-5
40. Bennett BL, Hew-Butler T, Hoffman MD, Rogers IR, Rosner MH, Wilderness Medical S. Wilderness medical society practice guidelines for treatment of exercise-associated hyponatremia: 2014 update. Wilderness Environ Med. 2014;25(4 Suppl):S30–42. doi:10.1016/j.wem.2014.08.009
41. Armstrong LE, Curtis WC, Hubbard RW, Francesconi RP, Moore R, Askew EW. Symptomatic hyponatremia during prolonged exercise in heat. Med Sci Sports Exercise. 1993;25(5):543–549. doi:10.1249/00005768-199305000-00003
42. Cheng JC, Zikos D, Peterson DR, Fesher KA. Symptomatic hyponatremia: pathophysiology and management. Acute Care. 1989;15:270–292.
43. Irving RA, Noakes TD, Buck R, et al. Evaluation of renal function and fluid homeostasis during recovery from exercise-induced hyponatremia. J Appl Physiol. 1991;70(1):342–348. doi:10.1152/jappl.1991.70.1.342
44. Speedy DB, Noakes TD, Rogers IR, et al. A prospective study of exercise-associated hyponatremia in two ultradistance triathletes. Clin. J. Sport Med. 2000;10(2):136–141. doi:10.1097/00042752-200004000-00009
45. Jonas CE, Arnold MJ. Exercise-associated hyponatremia: updated guidelines from the wilderness medical society. Am Family Phys. 2021;103(4):252–253.
46. Chlíbková D, Rosemann T, Knechtle B, Nikolaidis PT, Žákovská A, Sudi K. Description of three female 24-h ultra-endurance race winners in various weather conditions and disciplines. Chin J Physiol. 2017;60(4):231–241. doi:10.4077/CJP.2017.BAF443
47. Khodaee M, Luyten D, Hew-Butler T. Exercise-associated hyponatremia in an ultra-endurance mountain biker: a case report. Sports Health. 2013;5(4):334–336. doi:10.1177/1941738113480928
48. Dugas JP, Noakes TD. Hyponatraemic encephalopathy despite a modest rate of fluid intake during a 109 km cycle race. Br. J. Sports Med. 2005;39(10):e38. doi:10.1136/bjsm.2005.018820
49. Harris G, Reid S, Sikaris K, McCrory P. Hyponatremia is associated with higher NT-proBNP than normonatremia after prolonged exercise. Clin. J. Sport Med. 2012;22(6):488–494. doi:10.1097/JSM.0b013e3182580ce8
50. Hew-Butler T, Hamilton R, Hamilton B, Colesa Z. Special communication of a case of hypovolemic-associated EAH: lessons learned during recovery. Curr. Sports Med. Rep. 2017;16(4):289–293. doi:10.1249/JSR.0000000000000380
51. Young M, Sciurba F, Rinaldo J. Delirium and pulmonary edema after completing a marathon. Am Rev Respir Dis. 1987;136(3):737–739. doi:10.1164/ajrccm/136.3.737
52. Nelson PB, Robinson AG, Kapoor W, Rinaldo J. Hyponatremia in a Marathoner. Phys Sportsmed. 1988;16(10):78–87. doi:10.1080/00913847.1988.11709624
53. Goudie AM, Tunstall-Pedoe DS, Kerins M, Terris J. Exercise-associated hyponatraemia after a marathon: case series. J R Soc Med. 2006;99(7):363–367. doi:10.1177/014107680609900720
54. Lau MY, Choi YF. Exercise‐associated hyponatremia: a local case report. Hong Kong J. Emerg. Med. 2009;16(2):88–92. doi:10.1177/102490790901600205
55. Lee JKW, Nio AQ, Ang WH, et al. First reported cases of exercise-associated hyponatremia in Asia. Int J Sports Sci Med. 2011;32(4):297–302. doi:10.1055/s-0030-1269929
56. Tan DW, Yap SH, Wang M, et al. Body mass changes across a variety of running race distances in the tropics. Sports Medicine - Open. 2016;2(1). doi:10.1186/s40798-016-0050-3
57. Elsaesser TF, Pang PS, Malik S, Chiampas GT. Large-volume hypertonic saline therapy in endurance athlete with exercise-associated hyponatremic encephalopathy. J Emergency Med. 2013;44(6):1132–1135. doi:10.1016/j.jemermed.2012.11.048
58. Heled Y, Yarom Y, Epstein Y. Hyponatremia following a marathon, a multifactorial case with over infusion of fluids. Curr Sports Med Rep. 2019;18(4):115–117. doi:10.1249/JSR.0000000000000580
59. Noakes TD, Goodwin N, Rayner BL, Branken T, Taylor RK. Water intoxication: a possible complication during endurance exercise. Med Sci Sports Exercise. 1985;17(3):370–375. doi:10.1249/00005768-198506000-00012
60. Frizzell RT, Lang GH, Lowance DC, Lathan SR. Hyponatremia and ultramarathon running. Am J Sports Med Association. 1986;255(6):772–774. doi:10.1001/jama.1986.03370060086025
61. Clark JM, Gennari FJ. Encephalopathy due to severe hyponatremia in an ultramarathon runner. West J Emergency Med. 1993;159(2):188–189.
62. Surgenor S, Uphold RE. Acute hyponatremia in ultra-endurance athletes. Am J Emergency Med. 1994;12(4):441–444. doi:10.1016/0735-6757(94)90057-4
63. Noakes TD, Sharwood K, Collins M, Perkins DR. The dipsomania of great distance: water intoxication in an Ironman triathlete. Br. J. Sports Med. 2004;38(4):e16. doi:10.1136/bjsm.2002.004614
64. Page AJ, Reid SA, Speedy DB, Mulligan GP, Thompson J. Exercise-associated hyponatremia, renal function, and nonsteroidal antiinflammatory drug use in an ultraendurance mountain run. Clin J Sport Med. 2007;17(1):43–48. doi:10.1097/JSM.0b013e31802b5be9
65. Knechtle B, Knechtle P, Rosemann T. Low prevalence of exercise-associated hyponatremia in male 100 km ultra-marathon runners in Switzerland. Eur. J. Appl. Physiol. 2011;111(6):1007–1016. doi:10.1007/s00421-010-1729-7
66. Cejka C, Knechtle B, Knechtle P, Rust CA, Rosemann T. An increased fluid intake leads to feet swelling in 100-km ultra-marathoners - an observational field study. J Int Soc Sports Nutr. 2012;9(1):11. doi:10.1186/1550-2783-9-11
67. Scotney B, Weight RSB. Serum sodium levels, and renal function in an ultra-distance mountain run. Clin. J. Sport Med. 2015;25(4):341–346. doi:10.1097/JSM.0000000000000131
68. Hoffman MD, Stuempfle KJ, Sullivan K, Weiss RH. Exercise-associated hyponatremia with exertional rhabdomyolysis: importance of proper treatment. Clin nephrol. 2015;83(4):235–242. doi:10.5414/CN108233
69. Hoffman MD, Myers TM. Case study: symptomatic exercise-associated hyponatremia in an endurance runner despite sodium supplementation. Int J Sport Nutr Exerc Metab. 2015;25(6):603–606. doi:10.1123/ijsnem.2014-0241
70. Schenk K, Rauch S, Procter E, Grasegger K, Mrakic-Sposta S, Gatterer H. Changes in factors regulating serum sodium homeostasis during two ultra-endurance mountain races of different distances: 69km vs. 121km. Front Physiol. 2021;12:764694. doi:10.3389/fphys.2021.764694
71. Wagner S, Knechtle B, Knechtle P, Rust CA, Rosemann T. Higher prevalence of exercise-associated hyponatremia in female than in male open-water ultra-endurance swimmers: the ‘Marathon-Swim’ in Lake Zurich. Eur. J. Appl. Physiol. 2012;112(3):1095–1096. doi:10.1007/s00421-011-2070-5
72. Rogers IR, Grainger S, Nagree Y. Exercise-associated hyponatremic encephalopathy in an endurance open water swimmer. Wilderness Environ Med. 2015;26(1):59–61. doi:10.1016/j.wem.2014.07.010
73. Speedy DB, Faris JG, Hamlin M, Gallagher PG, Campbell RGD. Hyponatremia and weight changes in an ultradistance triathlon. Clin J Sport Med. 1997;7(3):180–184. doi:10.1097/00042752-199707000-00005
74. Speedy DB, Rogers I, Safih S, Foley B. Hyponatremia and seizures in an ultradistance triathlete. J Emerg Med. 2000;18(1):41–44. doi:10.1016/s0736-4679(99)00160-2
75. Stefanko G, Lancashire B, Coombes JS, Fassett RG. Pulmonary oedema and hyponatraemia after an ironman triathlon. BMJ Case Rep. 2009;2009:bcr0420091764. doi:10.1136/bcr.04.2009.1764
76. Severac M, Orban JC, Leplatois T, Ichai C. A near-fatal case of exercise-associated hyponatremia. Am J Emergency Med. 2014;32(7):813e1–813e2. doi:10.1016/j.ajem.2013.12.041
77. Lewis D, Blow A, Tye J, Hew-Butler T. Considering exercise-associated hyponatraemia as a continuum. BMJ Case Rep. 2018;2018:bcr–2017–222916. doi:10.1136/bcr-2017-222916
78. Bridges E, Altherwi T, Correa JA, Hew-Butler T. Oral hypertonic saline is effective in reversing acute mild-to-moderate symptomatic exercise-associated hyponatremia. Clin J Sports Med. 2020;30(1):8–13. doi:10.1097/JSM.0000000000000573
79. Backer HD, Shopes E, Collins SL. Hyponatremia in recreational hikers in grand canyon national park. J. Wilderness Med. 1993;4(4):391–406. doi:10.1580/0953-9859-4.4.391
80. Putterman C, Levy L, Rubinger D. Transient exercise-induced water intoxication and rhabdomyolysis. Am J Kidney Dis. 1993;21(2):206–209. doi:10.1016/s0272-6386(12)81095-x
81. Zelingher J, Putterman C, Ilan Y, et al. Case series: hyponatremia associated with moderate exercise. Am. J. Med. Sci. 1996;311(2):86–91. doi:10.1097/00000441-199602000-00007
82. Shopes EM. Drowning in the desert: exercise-induced hyponatremia at the Grand Canyon. J Emerg Nurs. 1997;23(6):586–590. doi:10.1016/s0099-1767(97)90274-9
83. Basnyat B, Sleggs J, Spinger M. Seizures and delirium in a trekker: the consequences of excessive water drinking? Wilderness Environ Med. 2000;11(1):69–70. doi:10.1580/1080-6032
84. Rothwell SP, Rosengren DJ. Severe exercise-associated hyponatremia on the Kokoda Trail, Papua New Guinea. Wilderness Environ Med. 2008;19(1):42–44. doi:10.1580/07-WEME-CR-116.1
85. Coler C, Hoffman MD, Towle G, Hew-Butler T. Hyponatremia in an 85-year-old hiker: when depletion plus dilution produces delirium. Wilderness Environ Med. 2012;23(2):153–157. doi:10.1016/j.wem.2012.02.013
86. Hoffman MD, Myers TM. Near-fatal outcome from absence of information about exercise-associated hyponatremia in a wilderness medicine field guidebook. Wilderness Environ Med. 2015;26(2):284–285. doi:10.1016/j.wem.2014.12.024
87. Knechtle B, Knechtle P, Rosemann T, Senn O. No dehydration in mountain bike ultra-marathoners. Clin. J. Sport Med. 2009;19(5):415–420. doi:10.1097/JSM.0b013e3181b47c93
88. Schenk K, Gatterer H, Ferrari M, Ferrari P, Cascio VL, Burtscher M. Bike Transalp 2008: liquid intake and its effect on the body’s fluid homeostasis in the course of a multistage, cross-country, MTB marathon race in the central Alps. Clin J Sport Med. 2010;20(1):47–52. doi:10.1097/JSM.0b013e3181c9673f
89. Knechtle B, Knechtle P, Rosemann T. No case of exercise-associated hyponatremia in male ultra-endurance mountain bikers in the ‘Swiss Bike Masters’. Chin. J. Physiol. 2011;54(6):379–384. doi:10.4077/CJP.2011.AMM050
90. Armstrong LE, Johnson EC, Ganio MS, et al. Effective body water and body mass changes during summer ultra-endurance road cycling. J. Sports Sci. 2015;33(2):125–135. doi:10.1080/02640414.2014.932918
91. Rust CA, Knechtle B, Knechtle P, Rosemann T. No case of exercise-associated hyponatraemia in top male ultra-endurance cyclists: the ‘Swiss Cycling Marathon’. Eur. J. Appl. Physiol. 2012;112(2):689–697. doi:10.1007/s00421-011-2024-y
92. Rose LI, Carroll DR, Lowe SL, Peterson EW, Cooper KH. Serum electrolyte changes after marathon running. J Appl Physiol. 1970;29(4):449–451. doi:10.1152/jappl.1970.29.4.449
93. Cohen L, Zimmerman AL. Changes in serum electrolyte levels during marathon running. South Afr Med J. 1978;53(12):449–453.
94. Whiting PH, Maughan RJ, Miller JD. Dehydration and serum biochemical changes in marathon runners. Eur. J. Appl. Physiol. 1984;52(2):183–187. doi:10.1007/BF00433390
95. Nelson PB, Ellis D, Fu F, Bloom MD, O’Malley J. Fluid and electrolyte balance during a cool weather marathon. Am. J. Sports Med. 1989;17(6):770–772. doi:10.1177/036354658901700608
96. Brock R, Krammel M, Kornfehl A, et al. Emergency point-of-care blood gas analysis during mass gathering events: experiences of the vienna city marathon. J Clin Med. 14(7). doi:10.3390/jcm14072504
97. Noakes TD, Carter JW. Biochemical parameters in athletes before and after having run 160 kilometres. South Afr Med J. 1976;50(40):1562–1566.
98. Kaminsky LA, Paul GL. Fluid intake during an ultramarathon running race: relationship to plasma volume and serum sodium and potassium. J Sports Med Phys Fitness. 1991;31(3):417–419.
99. Rama R, Ibanez J, Riera M, Prats MT, Pages T, Palacios L. Hematological, electrolyte, and biochemical alterations after a 100-km run. Can. J. Appl. Physiol. 1994;19(4):411–420. doi:10.1139/h94-033
100. Fallon KE, Sivyer G, Sivyer K, Dare A. The biochemistry of runners in a 1600 km ultramarathon. Br. J. Sports Med. 1999;33(4):264–269. doi:10.1136/bjsm.33.4.264
101. Stuempfle KJ, Lehmann DR, Case HS, Hughes SL, Evans D. Change in serum sodium concentration during a cold weather ultradistance race. Clin. J. Sport Med. 2003;13(3):171–175. doi:10.1097/00042752-200305000-00008
102. Reid SA, King MJ. Serum biochemistry and morbidity among runners presenting for medical care after an Australian mountain ultramarathon. Clin. J. Sport Med. 2007;17(4):307–310. doi:10.1097/JSM.0b013e31804c77da
103. Knechtle B, Senn O, Imoberdorf R, et al. Maintained total body water content and serum sodium concentrations despite body mass loss in female ultra-runners drinking ad libitum during a 100 km race. Asia Pac. J. Clin. Nutr. 2010;19(1):83–90.
104. Burge J, Knechtle B, Knechtle P, Gnadinger M, Rust CA, Rosemann T. Maintained serum sodium in male ultra-marathoners--the role of fluid intake, vasopressin, and aldosterone in fluid and electrolyte regulation. Hormone Metab Res. 2011;43(9):646–652. doi:10.1055/s-0031-1284352
105. Ribas MR, Ribas DIR, Fernandes P, et al. Acid-base and electrolyte balance responses in the performance of female ultramarathon runners in a 45 km mountain race. Nutrients. 2025;17(5). doi:10.3390/nu17050751
106. Mountjoy M, Junge A, Alonso JM, et al. Sports injuries and illnesses in the 2009 FINA world championships (Aquatics). Br. J. Sports Med. 2010;44(7):522–527. doi:10.1136/bjsm.2010.071720
107. Mountjoy M, Junge A, Benjamen S, et al. Competing with injuries: injuries prior to and during the 15th FINA World Championships 2013 (aquatics). Br. J. Sports Med. 2015;49(1):37–43. doi:10.1136/bjsports-2014-093991
108. Bom H-SH, Jeong YH, Cho S. Injuries and illness during the 2019 gwangju FINA and masters world championships in elite and amateur athletes. Chonnam Med J. 2023;59(1):83. doi:10.4068/cmj.2023.59.1.83
109. Hew-Butler T, Collins M, Bosch A, et al. Maintenance of plasma volume and serum sodium concentration despite body weight loss in ironman triathletes. Clin J Sports Med. 2007;17(2):116–122. doi:10.1097/JSM.0b013e3180326836
110. Hew-Butler T, Verbalis JG, Noakes TD. Updated fluid recommendation: position statement from the International Marathon Medical Directors Association (IMMDA). Clin. J. Sport Med. 2006;16(4):283–292. doi:10.1097/00042752-200607000-00001
111. Sawka MN, Burke LM, Eichner ER, Maughan RJ, Montain SJ, Stachenfeld NS. American college of sports medicine position stand. exercise and fluid replacement. Med Sci Sports Exercise. 2007;39(2):377–390. doi:10.1249/mss.0b013e31802ca597
112. Verbalis JG, Goldsmith SR, Greenberg A, Schrier RW, Sterns RH. Hyponatremia treatment guidelines 2007: expert panel recommendations. Am J Med. 2007;120(11 Supplement A):S1–S21. doi:10.1016/j.amjmed.2007.09.001
113. Siegel AJ, Pujol P, Adams WB, Noakes TD. International marathon medical directors association advisory statement. Clin J Sports Med. Available from: https://immda.org/wp-content/uploads/2015/08/Spring-2009-Hypertonic-Saline.
114. McDermott BP, Anderson SA, Armstrong LE, et al. National athletic trainers’ association position statement: fluid replacement for the physically active. J. Athl. Train. 2017;52(9):877–895. doi:10.4085/1062-6050-52.9.02
115. Rosner MH, Kirven J. Exercise-associated hyponatremia. Clin J Am Soc Nephrol. 2007;2(1):151–161. doi:10.2215/CJN.02730806
116. Noakes TD, Sharwood K, Speedy D, et al. Three independent biological mechanisms cause exercise-associated hyponatremia: evidence from 2,135 weighed competitive athletic performances.
117. Armstrong LE, Stearns RL, Huggins RA, Sekiguchi Y, Mershon AJ, Casa DJ. Reference values for hydration biomarkers: optimizing athletic performance and recovery. Open Access J Sports Med. 2025;16:31–50. doi:10.2147/OAJSM.S508656
118. O’Toole ML, Douglas PS, Laird RH, Hiller DB. Fluid and electrolyte status in athletes receiving medical care at an ultradistance triathlon. Clin. J. Sport Med. 1995;5(2):116–122. doi:10.1097/00042752-199504000-00008
119. Speedy DB, Noakes TD, Kimber NE, et al. Fluid balance during and after an ironman triathlon. Clin. J. Sport Med. 2001;11(1):44–50. doi:10.1097/00042752-200101000-00008
120. Siegel AJ, d’Hemecourt P, Adner MM, Shirey T, Brown JL, Lewandrowski KB. Exertional dysnatremia in collapsed marathon runners: a critical role for point-of-care testing to guide appropriate therapy. Am. J. Clin. Pathol. 2009;132(3):336–340. doi:10.1309/AJCP30OGLSLWLEIY
121. Armstrong LE. Rehydration during endurance exercise: challenges, research, options, methods. Nutrients. 2021;13(3):887. doi:10.3390/nu13030887
122. Hew-Butler T, Almond C, Ayus JC, et al. Consensus statement of the 1st International exercise-associated hyponatremia consensus development conference, Cape Town, South Africa 2005. Clin. J. Sport Med. 2005;15(4):208–213. doi:10.1097/01.jsm.0000174702.23983.41
123. da Fonseca-Engelhardt K, Knechtle B, Rust CA, Knechtle P, Lepers R, Rosemann T. Participation and performance trends in ultra-endurance running races under extreme conditions - ‘Spartathlon’ versus ‘Badwater’. Extrem Physiol Med. 2013;215. doi:10.1186/2046-7648-2-15
124. Scheer V. Participation trends of ultra endurance events. Sports Med Arthrosc Rev. 2019;27(1):3–7. doi:10.1097/JSA.0000000000000198
125. Armstrong LE, Johnson EC, McKenzie AL, Ellis LA, Williamson KH. Endurance cyclist fluid intake, hydration status, thirst, and thermal sensations: gender differences. Int J Sport Nutr Exerc Metab. 2016;26(2):161–167. doi:10.1123/ijsnem.2015-0188
126. Armstrong LE, Johnson EC, Adams WM, Jardine JF. Hyperthermia and exertional heatstroke during running, cycling, open water swimming, and triathlon events. Open Access J Sports Med. 2024;15:111–127. doi:10.2147/OAJSM.S482959
127. Speedy DB, Noakes TD, Rogers IR, et al. Hyponatremia in ultradistance triathletes. Med Sci Sports Exercise. 1999;31(6):809–815. doi:10.1097/00005768-199906000-00008
128. Hew-Butler T, Anley C, Schwartz P, Noakes T. The treatment of symptomatic hyponatremia with hypertonic saline in an Ironman triathlete. Clin J Sports Med. 2007;17(1):68–69. doi:10.1097/JSM.0b013e31802e9c18
129. Verbalis JG. Disorders of body water homeostasis. Best Pract Res Clin Endocrinol Metab. 2003;17(4):471–503. doi:10.1016/s1521-690x(03)00049-6
130. Armstrong LE, Kavouras SA. Thirst and drinking paradigms: evolution from single factor effects to brainwide dynamic networks. Nutrients. 11(12). doi:10.3390/nu11122864
131. Armstrong LE, Munoz CX, Armstrong EM. Distinguishing Low and High Water Consumers-A Paradigm of Disease Risk. Nutrients. 2020;12(3):858. doi:10.3390/nu12030858
132. McCormick SD, Bradshaw D. Hormonal control of salt and water balance in vertebrates. Gen Comp Endocrinol. 2006;147(1):3–8. doi:10.1016/j.ygcen.2005.12.009
133. Thornton SN. Thirst and hydration: physiology and consequences of dysfunction. Physiol Behav. 2010;100(1):15–21. doi:10.1016/j.physbeh.2010.02.026
134. Hew-Butler T, Ayus JC, Kipps C, et al. Statement of the second international exercise-associated hyponatremia consensus development conference, New Zealand, 2007.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Reference Values for Hydration Biomarkers: Optimizing Athletic Performance and Recovery
Armstrong LE, Stearns RL, Huggins RA, Sekiguchi Y, Mershon AJ, Casa DJ
Open Access Journal of Sports Medicine 2025, 16:31-50
Published Date: 7 April 2025