Back to Archived Journals » Research and Reports in Neonatology » Volume 12
Examining Practice Variation Used for Packed Red Blood Cell Transfusions for Preterm Infants in Neonatal Intensive Care Units Across the United States
Authors Everhart KC ![]() , Donevant SB, Iskersky VN, Wirth MD, Dail RB
, Donevant SB, Iskersky VN, Wirth MD, Dail RB
Received 30 June 2022
Accepted for publication 22 September 2022
Published 7 October 2022 Volume 2022:12 Pages 43—48
DOI https://doi.org/10.2147/RRN.S379367
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Robert Schelonka
Kayla C Everhart,1 Sara B Donevant,1 Victor N Iskersky,2 Michael D Wirth,1 Robin B Dail1
1College of Nursing, University of South Carolina, Columbia, SC, USA; 2Department of Neonatology, Prisma Health Richland/Pediatrix, Columbia, SC, USA
Correspondence: Kayla C Everhart, College of Nursing, University of South Carolina, 1601 Greene Street, Columbia, SC, 29208, USA, Email [email protected]
Purpose: Researchers report associations between packed red blood cell (PRBC) transfusions and morbid outcomes in preterm infants. Published standards are lacking for giving PRBC transfusions to preterm infants in the neonatal intensive care unit (NICU). This study examined standard practices reported by nurses across the United States (US) for administering PRBC transfusions to preterms to identify variation in practice which may contribute to the relationship of PRBC transfusions and morbidity.
Design and Methods: A 23-item questionnaire developed using REDCap based on literature and nursing experience of experts on the procedure of administering PRBC transfusions to preterm infants was distributed via social media and email to NICU nurses across the US.
Results: A total of 757 responses received and 518 completed responses were analyzed from level IV (48%) and level III (49%) NICU nurses in 47/50 US states. Most (94%) report PRBCs are ordered for anemia. Most (74%) report NICU policies do not specify warming PRBC transfusions prior to infusing; 10% (n = 53) specifically indicate they warm PRBC transfusions. Only 2% report using a blood warmer device. NICU nurses in the US (66%) reported feedings are altered during the PRBC transfusion. A 97% of nurses reported their NICU employs a specific physiologic assessment policy during PRBC transfusions. The two most common infusion sites used are (99%) peripheral IV as preferred and an umbilical venous catheter (74.5%) as next best option.
Conclusion: This study reveals inconsistencies in PRBC transfusion practices in US NICUs. Vast inconsistencies were shown in warming transfusions and in feeding practices surrounding PRBC transfusions. Future research should examine these variations in PRBC transfusion practices for any contributions to the relationship of PRBC transfusions and morbidity in preterm infants. A standard guideline should be developed based on the research evidence to guide nurses in administering preterm PRBC transfusions.
Keywords: neonate, hypothermia, blood transfusions, survey
Introduction
Due to an immature circulatory system, liver function, and to frequent, yet necessary laboratory testing, preterm infants often experience anemia while hospitalized in the neonatal intensive care unit (NICU).1 As a result, preterm infants may receive repeated blood transfusions with packed red blood cells (PRBCs) over their hospitalization.2 Recent evidence suggests PRBC transfusions may be associated with neonatal morbidity and mortality, mainly the devastating gastrointestinal (GI) complication, Necrotizing Enterocolitis (NEC). After decades of research, an exact causal pathway has yet to be determined.3,4 Some potential variables contributing to the association between NEC and a blood transfusion are the degree of anemia present in the preterm infant prior to the transfusion,5 the overall stress of the PRBC transfusion6 on the preterm infant, and/or the involvement of feeding practices around the time of a PRBC transfusion.7,8
Central hypothermia in preterm infants has been noted during and after PRBC transfusions in studies9 Thermal instability in preterm infants may intensify the stress experience of the blood transfusion. Due to this stress, ischemia of the GI tract may result from transfusing a preterm with PRBCs that have not been pre-warmed, leading to cold stress and slow gut motility, which may interfere with feedings given before, during and/or after the PRBC transfusion. This cascade of events may contribute to the association between PRBC transfusions and increased morbidity such as NEC. Common practice around these variables is not known and we can find no published standards for administering PRBC transfusions to preterm infants related to warming blood, feeding practices, assessment of the infant and best site for infusion. Therefore, our aim is to examine common practices used in neonatal intensive care units (NICUs) across the United States (US) by nurses to administer a PRBC transfusion to a preterm infant when ordered/needed. We know that lack of standards can result in inconsistent practices, and may potentially contribute to infant morbidity and mortality10.
Design and Methods
To identify practice variation around PRBC transfusions from NICU nurses, the profession that carries out the actual procedure, our team developed a 23-item survey in Research Electronic Data Capture11 (REDCap) to use with a descriptive survey study design. This survey research study was approved by the University of South Carolina (UofSC) Institutional Review Board (IRB) and all survey respondents completed an informed consent for participation.
Survey Questions
The team developed the survey questions based on our team’s neonatal clinical experience and a literature review on this subject.12 Content validity for the questions was assessed by a nurse scientist with clinical background as both a neonatal nurse and practitioner with over 10 years as a neonatal researcher, a board-certified neonatal nurse practitioner, and another academic researcher with specific expertise in internet surveys. The questions included yes/no, select all that apply, and short open narrative responses to provide specific detail for analysis. Questions were asked related to warming of blood, feeding practices, site of infusion, and physiological assessment. The questions/answers related to physiological assessment were stratified based on gestational age (GA) of the intended preterm infant, using 23–27 weeks GA and 28–32 weeks GA. Participants could access and complete the survey in 10–15 minutes using an internet connection.
Sample
The population for the national survey included any nurse or nurse practitioner currently working in a NICU in the US. Because nurses perform the PRBC transfusion, they are the best respondents to provide firsthand insight on the processes and protocols. No personal identifying information was collected during the survey. However, the survey included demographic information such as age, years of nursing and NICU experience, education level, and location of the NICU where the nursing respondents worked to provide a rich description of the sample.
Survey Distribution
We employed a variety of recruitment methods including social media and an email blast from Academy of Neonatal Nursing (ANN), a professional neonatal nurses’ organization. Studies have shown that social media has great potential to enhance research recruitment methods.13 The research team members promoted the survey through social media accounts (Facebook and Twitter). Interference from bot infiltration on survey responses via social media was prevented using reCAPTCHA, duplicate text questions to match the responses, and text fields.14 Three weeks after the survey was first promoted on social media and upon approval from the ANN leadership, an email and survey link was sent by ANN to each ANN member once using the ANN member list which was obtained with grant funding.
To increase the response rate, we offered a $50 US dollar gift card, as an incentive, with one random drawing each week for four weeks for participants that provided their personal email. Winners were selected using a random number generator with completed survey identification (ID) numbers. The survey was active for 4 weeks duration during November 2020. We exported the results from REDCap into Microsoft Excel for analysis using descriptive statistics (average, standard deviation [SD], range) for continuous variables and frequencies and percentages for categorical data. Two members of the team independently analyzed the narrative and short answer responses for themes, then discussed and agreed upon consistencies and inconsistencies in the standard practice of transfusing PRBCs to preterm infants in NICUs across the US.
Results
Over the 3 weeks of promotion on social media, we received 687 survey responses. An additional 70 responses were received from the ANN email for a total of 757 survey responses. Of the surveys submitted, 518 had complete responses and were analyzed. One limitation to the low email return through ANN’s email distribution is the possibility that many of the respondents had already completed the survey through the social media. The overall response rate for this survey was 518/757, or 68%. There were no duplicates of the survey as the study team had employed technology blocks to ensure the survey was only allowed to be taken once. There was a total of 236 incomplete survey responses which were not analyzed.
Demographic Data
Of the 518 complete and analyzed responses, all responses included the NICU level of care where the respondent practiced: 48% (n = 249) level IV NICUs, 49% (n = 257) level III NICUs, and 2% (n = 12) level II NICUs. There were no responses from nurses working in a level I NICU. The mean age of nursing respondents was 32 years old (range = 21–66 years; standard deviation (SD)= 9.5) with 7 years of NICU nursing experience on average (range = 1–43 years, SD = 9). Table 1 depicts the nursing respondent demographics. The nursing respondents worked across the US with 47 of the 50 states represented. The educational degrees obtained by the nursing respondents ranged from Associate 7% (n = 35), Bachelors 81% (n = 424), Masters 10% (n = 53), and Doctoral Degrees 1% (n = 5). There were some respondents, 1% (n = 4), that chose “prefer not to answer” for their educational degree. See Table 1 for respondent demographic table.
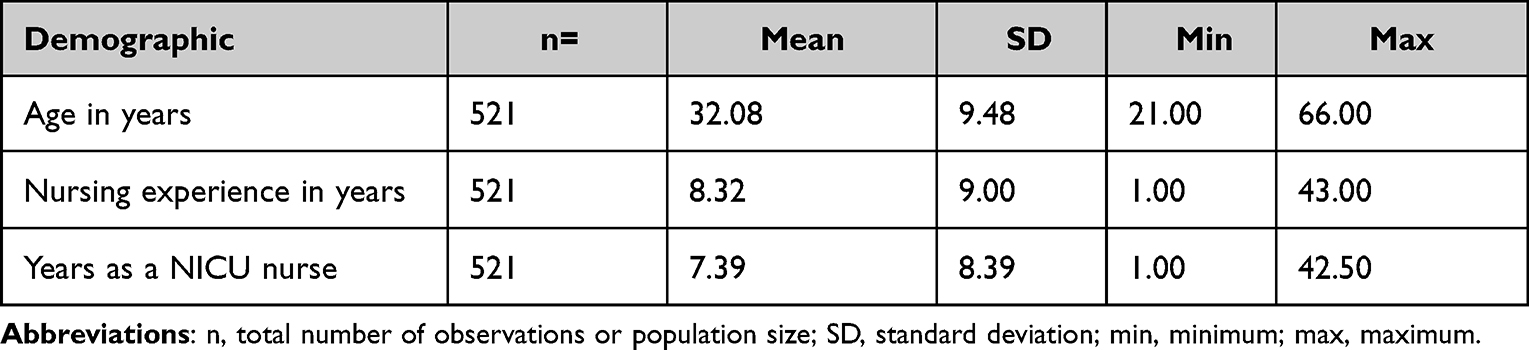 |
Table 1 Demographics of Nursing Respondents |
Clinical Indicators
We asked about the clinical indicators used to determine if a preterm infant should be treated with a PRBC transfusion. The participants selected all answers that applied from the following options: 1) apnea/bradycardia, 2) low hematocrit (HCT), 3) abnormal vital signs, 4) hypotension, 5) hypovolemia, and 6) other. Of the clinical indicators for a PRBC transfusion in preterm infants, participants reported low HCT most frequently 96% (n = 501) followed equally by hypovolemia and apnea/bradycardia at 63% (n = 330). There were no “other” indicators provided in the survey that were inseparable from the options provided by the research team.
Warming of PRBCs
The majority 74% (n = 386) of participants reported they do not warm PRBC transfusions and only 10% (n = 53) of participants specifically indicated they warm PRBC transfusions. However, only 2% (n = 11) reported using a blood warmer device to warm PRBCs. Other warming processes reported included 1) allowed the PRBCs to “sit out”, 2) “warm by ambient air”, or 3) “using my own body heat.”
Feeding Protocols
Most nursing respondents, 66% (n = 343) reported they alter feedings, in some way, during a PRBC transfusion. When asked how the feedings were altered, 41% (n = 212) of nurses indicated that feedings were discontinued for preterm infants before the PRBC transfusion. Because our team did not ask how much time prior to the transfusion, we assume timing of stopping feeds may vary prior to the PRBC transfusion. Most nursing respondents, 57% (n = 300), indicated the infants are made nothing by mouth, or NPO during the transfusion. One important finding in the open-ended questions was related to how practice may vary within the same NICU in relationship to feeding orders and PRBC transfusions. Multiple nursing respondents stated, “Feed orders depend on which doctor or practitioner is giving the orders.” The nursing respondents explained PRBC transfusion practices within their NICU can also vary based on GA of the preterm infant, varying thresholds of vital signs and laboratory values, and clinical presentation.
Physiological Assessment of Preterm Infants
Nursing responses indicated most NICUs have protocols which specify consistency in the physiologic assessment of preterm infants during PRBC transfusions, regardless of GA. Nurses report that preterm infants are routinely assessed every 2–4 hours when not receiving PRBC transfusions. However, 97% (n = 505) of participants indicate their NICU employs a specific assessment policy during a PRBC transfusion, as in the frequency of the variable assessments (heart rate, respiratory rate, temperature, blood pressure) and an hourly (at a minimum) visualization of the infusion site.
Transfusion Access
Because the site where the transfusion is infused may affect an infant’s body temperature, there was a question about site of transfusion. Sites included: 1) peripheral intravenously (PIV), 2) peripherally inserted central catheter (PICC), 3) umbilical arterial catheter (UAC), 4) umbilical venous catheter (UVC), 5) broviac/central venous line, and 5) do not know. Almost all (99%, n = 515) of nursing respondents indicated that a PIV was the preferred administration site for PRBC transfusions. If this was not possible, the next most preferred site was UVC (74.5%, n = 388). Some nursing respondents (25%, n = 130) indicated that UACs are used for PRBC transfusions.
Discussion
These survey results indicate that PRBC transfusion practices vary in NICUs across the US, especially related to the warming or not of PRBC transfusions and if preterm infants are fed around the time of a transfusion. It is interesting to note survey answers specifying that when nurses do want to warm blood, they may warm the blood with alternative means, as opposed to using a commercial blood warmer. Nurses sometimes use “workarounds” to accomplish tasks to achieve the desired outcome, even when knowing this is not evidence-based or best practice.15,16 Using non evidence-based interventions such as using “your own body heat” to warm a syringe of blood to infuse into a preterm infant may be practical, but not necessarily the most appropriate in a unit that strives to prevent infection. Workarounds may potentially place the preterm at greater risk and affirms the need for clinical trials to evaluate interventions used in nursing care. Hulse et al report an in vitro study to evaluate infusing warmed blood products using an inline warmer on preterm infants, delivering blood at near physiologic temperatures compared to cold stored blood with an patient temperature of 21.5 ± 0.1℃.17 Our team currently has a randomized clinical trial (NCT05170633) ongoing to evaluate warming PRBC transfusion versus standard care on the incidence of hypothermia during the blood transfusion in 140 preterm infants, funded by The Gerber Foundation.18
Our survey data reveal variation in feeding practices around administering PRBC transfusions. However, from these data, it is not clear if NICU protocols specify that preterm infants are completely NPO or if clinicians may reduce feeding volumes around the time of PRBC transfusion. Respondents indicated their NICU protocols often do not alter feedings before, during, or after PRBC transfusions; however, some indicated they “do not know” how feedings were altered. It is not clear whether feedings are given at reduced volume or stopped altogether and if the timing of feedings is altered. Feeding practices and PRBC transfusions are variables targeted in ongoing research studies for preterm infants and the incidence of feeding intolerance, NEC, and prolonged hospitalization. Currently, there is a large trial underway in the United Kingdom, “Withholding Enteral Feeds Around Packed Red Cell Transfusions (WHEAT) trial”.19 This multi-center randomized pilot study is using previously collected data to determine whether withholding enteral feedings before, during, and after PRBC transfusions decreases the incidence of NEC.19 In addition to this important study, prospective trials should be conducted to evaluate timing and volume of feedings in relationship to blood transfusions with NEC and other acute morbidity investigated as outcomes in preterm infants.
There was variation in access sites used for PRBC transfusions. Standards dictate that PRBC transfusions may be infused through UACs; however, a UAC is not the preferred route as there is an increased risk of thrombosis.20 Nurses also reported using PICCs as a means for PRBC transfusions, but this transfusion method has an associated risk of hemolysis due to the small-bore catheter.21 If thermal stability of a lower GA preterm infant is a priority and cold stored PRBCs are to be infused to the infant, a site that is not central to the infant’s circulation would optimize thermal stability, which eliminates UVCs and UACs.
We found no published studies exploring associations of body temperature, PRBC transfusions, feedings, and NEC in the preterm infant in a recent literature review.12 Independent of direct breast feeding, general practice for oral and enteral feedings includes warming prior to administration to a preterm infant.22,23 If feedings stored in a refrigerator are warmed prior to being given to a preterm infant, it is unclear as to why cold stored PRBC infusions are not warmed prior to infusing to the same GA infant. Studies are needed to ensure that PRBC transfusions are given to preterm infants using the best evidence-based procedures. In this way, we can optimize health for our most vulnerable patients and reduce preterm morbidity and mortality.
Conclusion
The purpose of this survey was to examine standard practices used for PRBC transfusions for preterm infants in NICUs across the US. The research team aimed to understand current practices from the nursing perspective. By examining current PRBC transfusion practices, we can inform future research and expose variations in practice that may affect preterm health outcomes. The results of this survey research study demonstrate variation in practice which demands more research is conducted to evaluate thermal stability, feeding practices and site of access when transfusing a preterm infant with PRBCs.
Acknowledgments
This National Survey was funded by The Office of the Vice President of Research at the University of South Carolina through a Support to Promote Advancement of Research and Creativity, or SPARC, Graduate Research Grant.
Funding
This original research was funded by the Office of the Vice President of Research at the University of South Carolina.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Counsilman CE, Heeger LE, Tan R, et al. Iatrogenic blood loss in extreme preterm infants due to frequent laboratory tests and procedures. J Matern Fetal Neonatal Med. 2021;34(16):2660–2665. doi:10.1080/14767058.2019.1670800
2. Howarth C, Banerjee J, Aladangady N. Red blood cell transfusion in preterm infants: current evidence and controversies. Neonatology. 2018;114(1):7–16. doi:10.1159/000486584
3. Bazacliu C, Neu J. Necrotizing enterocolitis: long term complications. Curr Pediatr Rev. 2019;15(2):115–124. doi:10.2174/1573396315666190312093119
4. Cho SX, Rudloff I, Lao JC, et al. Characterization of the pathoimmunology of necrotizing enterocolitis reveals novel therapeutic opportunities. Nat Commun. 2020;11(1):1–19. doi:10.1038/s41467-020-19400-w
5. Maheshwari A, Patel RM, Christensen RD. Anemia, red blood cell transfusions, and necrotizing enterocolitis. Semin Pediatr Surg. 2018;27(1):47–51. doi:10.1053/j.sempedsurg.2017.11.009
6. Knobel-Dail RB, Sloane R, Holditch-Davis D, Tanaka DT. Negative temperature differential in preterm infants less than 29 weeks gestational age: associations with infection and maternal smoking. Nurs Res. 2017;66(6):442–453. doi:10.1097/NNR.0000000000000250
7. Rose AT, Patel RM. A critical analysis of risk factors for necrotizing enterocolitis. Semin Fetal Neonatal Med. 2018;23(6):374–379. doi:10.1016/j.siny.2018.07.005
8. Christian VJ, Polzin E, Welak S. Nutrition management of necrotizing enterocolitis. Nutr Clin Pract. 2018;33(4):476–482. doi:10.1002/ncp.10115
9. Knobel R, Holditch-Davis D. Thermoregulation and heat loss prevention after birth and during neonatal intensive-care unit stabilization of extremely low-birthweight infants. Adv Neonatal Care. 2010;10(5 Suppl):S7–S14. doi:10.1097/ANC.0b013e3181ef7de2
10. Atsma F, Elwyn G, Westert G. Understanding unwarranted variation in clinical practice: a focus on network effects, reflective medicine and learning health systems. Int J Qual Health Care. 2020;32(4):271–274. doi:10.1093/intqhc/mzaa023
11. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
12. Everhart KC, Donevant SB, Wirth MD, Dail RB. Examining etiological pathways to necrotizing enterocolitis in very preterm infants. J Neonatal Nurs. 2021;27(2):77–81. doi:10.1016/j.jnn.2020.07.003
13. Topolovec-Vranic J, Natarajan K. The use of social media in recruitment for medical research studies: a scoping review. J Med Internet Res. 2016;18(11):e5698. doi:10.2196/jmir.5698
14. Von Ahn L, Maurer B, McMillen C, Abraham D, Blum M. ReCAPTCHA: human-based character recognition via web security measures. Science. 2008;321(5895):1465–1468. doi:10.1126/science.1160379
15. Debono DS, Greenfield D, Travaglia JF, et al. Nurses’ workarounds in acute healthcare settings: a scoping review. BMC Health Serv Res. 2013;13(1):1–16. doi:10.1186/1472-6963-13-175
16. Beerepoot I, Lu X, Van De Weerd I, Alexander Reijers H. Seeing the signs of workarounds: a mixed-methods approach to the detection of nurses’ process deviations; 2021.
17. Hulse W, Bahr TM, Fredrickson L, et al. Warming blood products for transfusion to neonates: in vitro assessments. Transfusion. 2020;60(9):1924–1928. doi:10.1111/trf.16007
18. The gerber foundation; 2022. Available from: https://www.gerberfoundation.org/pediatric-health/.
19. Gale C, Modi N, Jawad S, et al. The WHEAT pilot trial-WithHolding Enteral feeds Around packed red cell Transfusion to prevent necrotising enterocolitis in preterm neonates: a multicentre, electronic patient record (EPR), randomised controlled point-of-care pilot trial. BMJ open. 2019;9(9):e033543. doi:10.1136/bmjopen-2019-033543
20. Hogan MJ. Neonatal vascular catheters and their complications. Radiol Clin North Am. 1999;37(6):1109–1125. doi:10.1016/S0033-8389(05)70252-9
21. Pettit J. Fostering a new era of vascular access device selection in neonates. Newborn Infant Nurs Rev. 2006;6(4):186–192. doi:10.1053/j.nainr.2006.09.004
22. Gonzales I, Duryea E, Vasquez E, Geraghty N. Effect of enteral feeding temperature on feeding tolerance in preterm infants. Neonatal Netw. 1995;14(3):39–43.
23. Uygur O, Yalaz M, Can N, Koroglu OA, Kultursay N. Preterm infants may better tolerate feeds at temperatures closer to freshly expressed breast milk: a randomized controlled trial. Breastfeed Med. 2019;14(3):154–158. doi:10.1089/bfm.2018.0142
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Neonatal Hypothermia Prediction Model for In-Hospital Transport Using Machine Learning Algorithms: A Single-Center Retrospective Study
Zhang W, Gu X, Gu C, Yao L, Zhang Y, Wang K
Journal of Multidisciplinary Healthcare 2025, 18:3205-3217
Published Date: 4 June 2025