Back to Archived Journals » Innovation and Entrepreneurship in Health » Volume 3
Evolving to a new service-dominant logic for health care
Received 31 July 2015
Accepted for publication 24 November 2015
Published 29 January 2016 Volume 2016:3 Pages 25—33
DOI https://doi.org/10.2147/IEH.S93473
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Rubin Pillay
Keith A Joiner,1,2 Robert F Lusch3,4
1Department of Internal Medicine, College of Medicine, The University of Arizona, Tucson, AZ, USA; 2Department of Economics, Eller College of Management, The University of Arizona, Tucson, AZ, USA; 3Department of Marketing, Eller College of Management, The University of Arizona, Tucson, AZ, USA; 4McGuire Center for Entrepreneurship, Eller College of Management, The University of Arizona, Tucson, AZ, USA
Abstract: Consumers value health and a sense of well-being. The health care system cannot supply these values, but only “products” such as hospitalization, ambulatory care, medications, procedures, and preventative care. These components of health care represent neither the value within the system nor the desired final output. Nonetheless, the health care system has focused inordinately on the products, to the point of suggesting that they have intrinsic value. We link this situation to the concept of goods-dominant logic, which has dominated business and managerial thinking since the Industrial Revolution. We then explain why and how moving to service-dominant logic is essential for consumers and providers to better cocreate value from products which are not intrinsically valuable. The challenge of cocreating value is confounded by information asymmetry, and by the myriad factors in the health care ecosystem that contribute to or detract from health and well-being. A new lexicon, emanating from service-dominant logic, is suggested to facilitate the move away from a goods-dominant mindset.
Keywords: service, health, ecosystem, health care
Introduction
The dramatic rise in health care expenditures in the USA over decades has not been aligned with proportionate improvements in health care outcomes, particularly when compared with other developed countries.1 This has led to calls for more value for the health care dollar. Recognizing that value is a broad term, one definition of value is health outcome/cost.2 While logical in its formulation and in estimation of costs, less obvious is the meaning of outcomes. Most commonly, metrics such as infant mortality, life expectancy, and mortality due to treatable conditions are used to define outcomes.3 In this article, we propose a new paradigm for envisioning outcomes and, more specifically, value in health care, based on the concept of service-dominant (S-D) logic. In so doing, we suggest a new lexicon to accompany this paradigm.
For too long, value in health care had a different meaning – it was based on a dominant perspective of value in health care and its management rooted in an outdated managerial logic. The dominant logic, often referred to as an old manufacturing, industrial, or goods-dominant (G-D) logic, informs us that the pathway to continual human well-being is to invent more tangible goods and interventions that are then diffused throughout society for massive application and problem solution.
G-D logic emerged during the Industrial Revolution and the high division of labor in society that resulted. It is the logic of separation where goods can be standardized and produced separately and away from the customer. Goods produced in this way are created at high efficiency and embedded with value and then stored and distributed through additional value-adding activities – selling and branding. The customer is then someone who can be targeted and promoted to in order to create sales and maximize firm profits.
The G-D logic has pervaded not only the manufacturing of goods but also the overall mindset for how humans exchange.4 One party is known as the creator of a product and the other party is the passive recipient of the value this product provides. In health care, G-D logic is manifested in the profusion of more specialized and sophisticated providers, delivery systems, pharmaceuticals, medical devices, facilities, procedures, sources of information (genomics, proteomics, metabolomics), information technologies, and more.
The problem is that none of these products represent what people inherently need, let alone want. What they need and want are solutions to their health care problems, the experience of healthy living, and ideally, a sense of wellness. Nonetheless, G-D logic is so ingrained in our managerial mindset that it even controls how the next health care revolution is being designed and implemented. This is despite using terms to describe the revolution that suggest otherwise – patient-centered care, wellness care, personalized/precision medicine,5,6 consumer-driven/directed care,7 patient activation and engagement, and more. In reality, these are too often being conceptualized and implemented as the customization of goods and treatments as they are delivered and provided to individual patients. It is a G-D logic approach to health care and will not work, at least in isolation.
A G-D logic framing of the relationship between the provider and the patient views the provider as experienced, knowledgeable, innovative, creative, and the source or creator of value.8 The patient is viewed as inexperienced, unknowledgeable, passive or dull, and someone who consumes and uses up or destroys value. This represents the logic of separation between producer and consumer or in health care between health care providers and patients.
S-D logic is one of togetherness. Both the health provider and the consumer (or client or customer – rather than patient) are sensing and experiencing, creating, integrating resources, and learning.9 In the process, they cocreate value using a definition of value, which far transcends that reflected by concepts, including patient engagement and patient activation, and measurements such as life expectancy, mortality in infancy or from treatable conditions, vaccination rates, and more. We elaborate on this distinction in the remainder of the manuscript by explaining the concept of S-D logic, its applications (and misapplications) to health and health care, and a new lexicon to guide a process of transition.
The broad concept of S-D logic
S-D logic is the logic of togetherness where actors use their applied knowledge and skills (competences) to provide benefit to another and to benefit themselves. S-D logic is based on relationships, mutual trust, and win–win exchange. When goods are involved they are service distribution mechanisms or service appliances (ie, people hire products to get a job done). Because of its interactional nature and the constant adjustment of actors and how they appraise value, each actor is always learning how to better serve and function in a dynamic environment.
The genesis of the service revolution goes back more than 100 years, Bastiat10 made an observation in 1848 that was largely ignored. Very succinctly he observed:
[…] the great economic law is this: Services are exchanged for services […] It is trivial, very commonplace; it is, nonetheless, the beginning, the middle, and the end of economic science.10
But even then in the mid-19th century with factories in Europe and North America and beyond, turning out with increasing efficiency and low-price tangible goods, Bastiat was at best ignored and generally ridiculed for his thinking.
In 2004, a pair of North American scholars11 persuasively argued that Bastiat was correct in his observation. If a service is simply “what a good is not”, then we really do not know the essence of a service. Vargo and Lusch11,12 define a service as the application of the knowledge and skills (competences) of one actor for the benefit of another. Sometimes the knowledge and skills are embedded into a tangible good (tool) but other times the knowledge and skills are provided directly to another actor. Consequently, service is the dominant form of exchange and goods are merely an indirect way of providing a service. In this sense, people hire products (goods) for the service they provide and to get a job done. Jumping ahead, pharmaceuticals, medical devices, electronic health records, new delivery models, payment reform, and on and on are hired to get a job done.
Today S-D logic is rising in ascendance primarily because of the information revolution. As humans have moved from a one-to-one communication through most of their civilization to a one-to-many communication over the last few hundred years and to a many-to-many communication over the last 2 decades, the power of the individual has risen. No longer is the consumer viewed as the passive recipient of value-laden goods that producers provide them so they can consume and hence destroy value. Today the individual (or household) is more and more itself a business of sort that combines a lot of resources (including tangible goods) to cocreate value.
Furthermore, due to the information revolution, individuals are now active actors in a network of other actors. What increasingly gives them power and influence are their individual knowledge and skills that they use for their benefit and that they exchange and share with others. While today this is still too often through traditional bureaucratic organizations, this is rapidly in decline. Emerging in its place is network intensive and highly adaptable organizational structures for service exchange; what some call value constellations. As these networks unfold and value constellations emerge, we witness the organization and the individual not as a fixed form but a dynamic organism in a service ecosystem. Enterprises, industries, and countries that recognize the power of service ecosystems and how to capitalize on them will be better able to create economic wealth and viable systems.
S-D logic for health care is not synonymous with patient activation and engagement
An inevitable reaction to the above from those in the health care delivery sector is that the concepts are already embraced and are being implemented. The emphasis on patient-centered care, wellness care, personalized medicine, patient engagement, patient activation, and more are the processes that are alleged to capture patient value, all facilitated by the information revolution, social media, health care delivery reform, and more. While we acknowledge that there is overlap between S-D logic and these areas of emphasis, we argue herein that a strong, albeit nuanced GD bias continues to dominate, because the primary focus is on delivery of goods.
Much of this bias emanates from the dominant terminology within the health care field. G-D logic as applied to health care is about nouns. Hospital rooms, outpatient clinics, medications, medical devices, medical images, laboratory tests, doctors, nurses, electronic health records, accountable care organizations, genomics, and on and on. S-D logic is about verbs: healing, caring, monitoring, resting, walking, talking, eating, sleeping, visiting, learning, feeling, curing, thinking, sharing, recovering, and dying. Framed with an S-D logic mindset, terms such as adapting, facilitating, stewarding, cocreating, revealing, improving, supporting, promoting, elucidating, learning, and more capture what the patient–provider dynamic should reflect. We elaborate on the nomenclature issue throughout the remainder of the paper.
Extensive literature deals with the concepts of patient activation and patient engagement. “Patient activation” reflects a patient’s knowledge, skills, ability, and willingness to manage his or her own health and care. “Patient engagement” is a broader concept that combines patient activation with interventions designed to increase activation and promote positive patient behavior such as obtaining preventive care or exercising regularly. Patient engagement is one strategy to achieve the “triple aim” of improved health outcomes, better patient care, and lower costs.13 The two terms are often used synonymously, since patient activation is considered a necessary component of patient engagement.
The patient activation approach14 centers on a series of prescribed behaviors which the patient is expected to embrace, and in doing so, will lead to improvement of outcomes in their interactions with providers and the health care system.15,16 Value for the patient is largely defined by the health care system – the state of patient activation is assessed by determining the patient’s level of agreement or disagreement with 13 measures of “patient’s willingness and ability to take independent actions to manage their health and care”.17 There is a presupposition that independence is necessary, and that answering the questions in the affirmative will create value for patient. Patient activation only peripherally involves domains that are not explicitly related to health care (social situation, cultural and religious beliefs, economic considerations, work, play, and more). Similarly, interactions with other individuals (such as family, friends, and peers), let alone cocreation with providers, are not directly included in assessing the level of patient activation.
Taking diabetes as an example, patients with higher activation scores are more likely to engage in healthy behaviors such as regular exercise, a healthy diet, medication adherence, and preventative measures. There is a strong link between education and higher patient activation measure scores. They may or may not fare better on quantitative measures of their diabetes and overall health, such as blood pressure, cholesterol, HbA1c, and lipids, although self-reported health is associated with higher activation scores.18 It is unclear whether patients with higher activation scores are those with more adherent personalities, and may likely ascribe adherence to better health. Regardless, activation metrics are not a direct assessment of value.
Both successes and failures are described with implementation of programs designed to increase engagement and activation. While successes are described (http://healthaffairs.org/blog/2013/02/04/february-health-affairs-issue-new-era-of-patient-engagement/), there are numerous impediments to successful implementation.19–26 These include the following.
From the perspective of physicians
- They do not believe they have the time. (Of interest, there is no robust evidence that shared decision making takes more time).
- Physicians are concerned that patient education and decision aids subvert their role.
- Providers often fail to recognize that a decision is possible. This problem can be exacerbated by clinical practice guidelines, derived from evidence-based medicine.
- Physicians do not have the full range of information in preference-sensitive conditions. Patients and providers can have vastly different notions of what is important. There is often a silent misdiagnosis of patient preferences.
- Providers are not adequately trained.
From the perspective of consumers
- Often the most vulnerable consumers are the least involved. Allowing them to opt out, which often occurs, exacerbates inequalities of care.
- Cultural and language issues exacerbate the concerns listed in the previous paragraph.
- Shared decision-making conflicts with well-known cognitive limitations that are part of human nature. Alternative approaches are needed, such as choice architecture, opt out, and precommitment.
- Consumers need to be explicitly invited to participate. There should be no assumption that decisions are conscious and prospective.
Approaches to dealing with these impediments are typically addressed singly, rather than through a holistic approach. We suggest that a parsimonious solution to most if not all of the above issues emanate from S-D logic, which posits that value is defined by the customer. Addressing S-D logic explicitly acknowledges that consumers cocreate value by integrating many resources in a variety of ways. These resources can be “private resources” such as family, friends, and colleagues. Other resources may be “public resources” such as nature (the atmosphere, forests, lakes, mountains, etc), governing laws and regulations, and transfer payments. Finally, there are “market resources” or those obtained in the market through economic exchanges such as payment for medical or health products. Hence, value is not to be equated to a health care provider delivering medical treatments since this is a highly firm or provider-centric perspective. Rather a customer- or patient-centric perspective translates into the recognition that value for many if not most consumers comes from in part or mostly from engaging in activities outside the process of behavioral change, or even healthy behavior. The starting point for shared decision making is therefore to ascertain and elicit from the consumer their personal sense of value, and to ensure that decision alternatives are framed as value propositions, more so than medical decisions.
Value from the customer’s perspective of health enhancement may include such intertwined positive experiences that are now more “enabled” such as having lunch with a grandchild, attending a sporting event, a high school graduation, going to church, book club, and the like. They may also include intertwined negative experiences that one is “relieved” of as a result of health care treatment. Such as no longer having to drive congested streets to twice weekly visit a health care professional, no longer needing to remember to take medications, or no longer having to worry where to obtain the financial resources to pay for health care. So in essence it is the relieving of these generally negative experiences that result in something of positive value to the customer.
In summary, “enabling and relieving” are more likely to represent value than eating healthy, or necessarily advocating independence on the part of the consumer. To say that being healthier makes all of these activities more feasible misses the point. First, that may or may not be true, and depends entirely on the individual. Second, it is not a zero sum game. Providers can help consumers cocreate the pathway to value in ways that go well beyond patient activation measures and/or typical medical interventions or advice.
Assessment and empirical implementation of S-D logic in health care
Customer value practice styles
The concept of S-D logic as applied to health care is new. Scant literature exists under that nomenclature. McColl-Kennedy et al27 evaluated styles used by customers in cocreating value with the health care system. In-depth interviews revealed five practice styles, two of which – “team management” and “partnering” – were consistent both with the concept of S-D logic and with a higher quality of life. These styles were considered particularly important for individuals with chronic disease, where incorporating a wide range of activities and experiences across private, public, and market resources facilitates health.
Motivational interviewing
Perhaps, the clearest evidence for the effectiveness of this approach comes from studies conducted under the rubric of motivational interviewing (MI).28 The main focus of MI is facilitating behavior change. Individuals are encouraged and directed toward exploring and resolving ambivalence about the change. While the individual does the majority of the talking, the interviewer is more directive than in the current framework of patient-centered care. Value is cocreated as a consequence, since that is the explicit purpose.
In MI, “readiness to change” is not seen as a trait that is imposed but rather is evoked. The consumer is charged with the responsibility for exploring and resolving ambivalence, while the provider’s role is to be directive in assisting the consumer through that process. Providers can be, and often are, nonphysicians, including nurses, nurse practitioners, physician assistants, behavioral therapists, and other physician extenders. Hence, MI fits more naturally under a team-based care approach than does patient-centered care, which has a physician-centric flavor.
MI has been particularly effective in dealing with smoking cessation and drug abuse. While applied less in the setting of organic illness, its relevance to diabetes and obesity is one of the most obvious. As an example, rather than a provider advising their diabetic patient to lose weight to help with control of blood sugar, hypertension, and to prevent end-organ complications, or even to engage with the patient about ways to achieve this, questions such as the following are used: What problems do you have because of your weight? What are some concerns that you have about your weight? What would be the costs to you of changing? What would be the benefits to you of changing? How do your family, friends, coworkers, and others feel about your weight?
Individuals are also prompted to fit their ambivalent feelings into their overall lives by exploring activities of daily living and the impact of their obesity and diabetes on those activities. As with the customer value creation styles, this embeds a broader array of actors and resources (private, public, and market) than is often the case with patient-centered care.
Home-based primary care
As pioneered in the Veterans Administration Health Care System,29 this is a model in which individuals who are functionally or practically home-bound receive primary care in the home, delivered through teams of providers. Such individuals characteristically have multiple chronic conditions, and a large fraction (more than one-third) have some mental and/or behavioral illness that confounds their ability to understand and comply with management guidelines developed in a G-D fashion. This can include individuals with various levels of dementia. While there are clearly situations where application of the principles of S-D logic is problematic at best (eg, coma), these represent a miniscule subset of the overall health and health care landscape.
Individuals in this circumstance have neither the financial nor social resources to make optimal choices regarding their health, yet are massive utilizers of health care resources, due to hospitalizations, emergency department visits, and general ill health. A primary care team, consisting of a core group of a physician, nurse practitioner, and care coordinator, sometimes expanded to include behavioral health specialists, dieticians, social workers, and others visit and review the home situation in conjunction with the consumer. An individualized plan is cocreated which is realistic for both provider and consumer, and is highly cost-effective.
Holistic cancer care
For many, if not most patients with solid organ or liquid cancers, confronting the initial diagnosis, and dealing with all of the subsequent care, involves the entire family at a minimum. More commonly, it includes an even more extended reach of actors such as friends and professional colleagues. The experience also calls upon a range of health care providers (surgical, radiation, gynecologic, medical oncologists, and nurses) and other professionals such as dieticians, social workers, care coordinators, and mental health professionals. This complex interplay of actors, more often than not, occurs in a fragmented fashion, without necessarily or even usually identifying the primary value system for the patient.
Approaches that represent the application of S-D logic to cancer care have been described in a talk given by Leonard Berry,30 a widely published author on service in the health care industry.31 The talk is available at http://www3.mdanderson.org/streams/FullVideoPlayer.cfm?mediaID=3DA190CB-C64F-4660-B00C-9CB5AD142B81. In this presentation, an oncologist is quoted as saying “Oncology practice provides treatment, but that is a fraction of the patients’ needs”. Berry30 describes some of the processes involved in holistic cancer care. Intermountain Healthcare in Salt Lake City, Utah and Integris Health in Oklahoma City, Oklahoma use the following process with newly diagnosed cancer patients: The patient and their family stay in one room on a single day, and are visited sequentially by various professionals who will be involved in their care – physicians, nurses, dieticians, social workers, care coordinators, and others. The patient leaves with a written plan. This approach circumvents the logistical problem of scheduling multiple different meetings on different days, and the anxiety inherent in such, and also allows the providers to coordinate with one another.
The Internet and e-health
Online health information facilitates cocreation of value between consumers and the health ecosystem. Such ready access to information is fundamentally altering the information asymmetry that has previously characterized (and in many respects dominated) the consumer–provider interaction.
Among the most popular sites are those in which the consumer can elicit individualized responses to their inquiries from providers. Most consistent with S-D logic are sites that focus on support and community more so than for diagnosis or treatment. Actors (consumers) are organizing on their own to help each other. They are cocreating value by integrating their resources and experiences. A few examples include HealingWell.com, Dailystrength.org, and PatientsLikeMe.com. Healthfinder.gov (live well, learn how) is a Department of Health and Human Services site with a comprehensive listing of sources for general and specific support. Of interest, this suggests that the health care ecosystem cannot be master planned in the age of the Internet. Both highly credible and less credible sources are equally available.
A rapidly expanding segment allows consumers, for a relatively small fee, to get either primary or secondary opinions online. These latter interactions, while potentially viewed as personalized medicine with S-D logic characteristics, are much more in line with a G-D logic view of the patient–provider interaction. They likely lessen, rather than improve the chances, for cocreation of value.
Mobile technology
Arguably, the most direct application of S-D logic to health and health care is through mobile technologies.32 Devices that permit consumers to seamlessly acquire and (if desired) transmit information regarding their physiological functions and potential health-promoting activities, as part of activities of daily living, are the very essence of S-D logic. Home telehealth is a more comprehensive application of this concept. No attempt will be made to summarize the full range of current and future capabilities of such devices, given the astonishing and rapidly evolving status of the field. Instead, we will focus on critical attributes that require attention. These include:
- Determining the quantity, quality, and form of the information that is desirable and acceptable, both for the consumer and provider
- Optimizing the consumer and provider experience
- Understanding the relationship between the information provided and subsequent consumer behavioral modification.
For example, a device that wirelessly transmits blood glucose levels, blood pressure, or weight to providers is considered an example of individualized, patient-centered care. It is important to understand that the information generated and/or transmitted is not intrinsically value producing, either for the consumer or the provider. It is more akin to G-D logic.
A role of smart devices more in line with S-D logic is one in which the consumer determines the value of the information coming from the device and embeds that value in their decision-making activities and activities of daily living. The device enhances consumer self-efficacy. One formulation is that the conventional provider–consumer interaction is thereby being “creatively destroyed”.
Medical devices and pharmaceuticals
As is the case with mobile devices, and recognizing substantial overlap with that category, medical devices and pharmaceuticals represent other direct applications of S-D logic to health and health care.
One category illustrates the concept clearly. Adherence to medications is one of the most difficult issues for many consumers in managing their health. The reasons for poor adherence are many, and belie any single answer or simplified approach. Tools for improving adherence range from smart phone apps to pill bottles that record or signal when medications are to be taken, refilled, to medication-implanted microchips that send a wireless signal when the chip dissolves in the stomach.
Discussion
S-D logic, as it seeps into the managerial mindset, alters managerial attitudes, decisions, and actions in a profound manner. This is reflected most succinctly in a change in terminology. In Table 1, eleven of these shifts are identified for G-D and S-D logic generally. In Table 2, analogous shifts are suggested for the language describing value cocreation between provider and patient. In Table 3, the narrative goals of some more recent trends in health care are framed in G-D logic and corresponding S-D logic. The intent in all cases is to examine and reexamine the underlying meaning of current terms.
 | Table 1 Contrasting managerial logics |
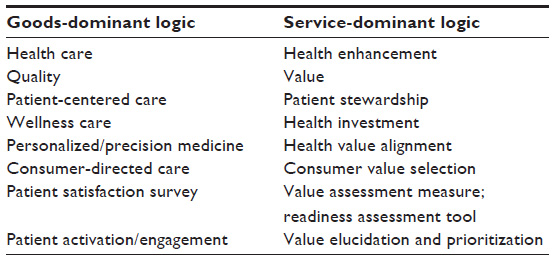 | Table 2 Contrasting terminologies in health and health care |
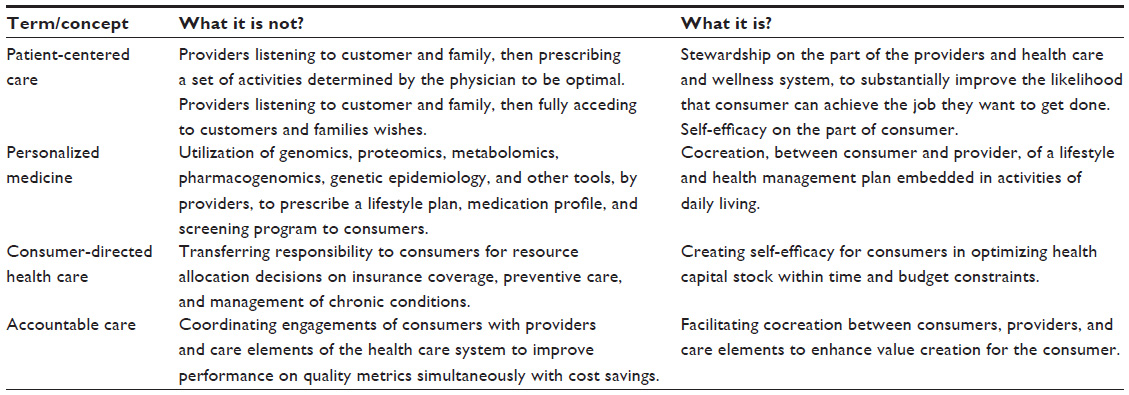 | Table 3 Applications of service-dominant logic to a new language for health and health care |
Consider first, that rather than a firm offering goods and services or tangible and intangible units of output it is viewed as offering a service and experience. Service (singular not plural) focuses on the application of competencies for the benefit of others (beneficiaries). Experience focuses on the beneficiaries’ use of the offering. Consider, for instance, asking patients exiting the hospital if they have a better understanding and/or knowledge of how to prevent future health problems or if they believe they will be able to integrate their learning from a hospital stay into their daily lives to enhance their wellness. These questions are in stark contrast to those commonly asked in patient satisfaction surveys, dealing with perceptions of room cleanliness, courteous staff, tasty food, and even whether nurses, physicians, and other providers listened and were attentive to patients’ needs. An approach that begins to capture this distinction is the Coleman care transitions program.33,34 Patients being discharged from an inpatient facility cocreate a plan for their postdischarge care. A readiness assessment tool is used to assess value alignment between provider and patient.
The logic also shifts from standardized mass production, known in services marketing and management as service factories (servitization) to customized and personalized service. Even though pharmaceuticals and medical devices may be standardized, what is needed is the customized and personal application of these products. Pharmacogenomics constitutes a powerful approach to maximize benefit and minimize harm from pharmaceuticals, by matching patient genotype with the correct drug. Similarly, selecting oncologic agents based on tumor molecular profiling and susceptibility testing is considered state of the art. However, the specter of a G-D logic approach to pharmaceuticals is all too real, given the complexity. In this latter scenario, drugs are customized in a manner that views the patient, and even the provider, as a passive operand resource to be treated without sufficient knowledge to make the nuanced distinctions in matching genotype and drug.
Framed differently, an all too common view of personalized medicine is limited to pharmaceuticals prescribed for preventing, delaying, or treating diseases, with limited or even no attention to all the other factors contributing to health.35 S-D logic replaces the linear tightly linked system of suppliers of products with a value constellation of other cocreating actors, forming a health ecosystem. This includes family, friends, and alternative health care providers as well as a host of wellness services. Many of the actors are not formally part of the established health industry. These conversations today are occurring and being facilitated through the growth of social media.
Health care providers and executives that view health care as a part of an ecosystem will be able to better design and thus, create their health system’s value proposition for the consumer.27,36 There is hope that patient-centered medical homes, accountable care organizations, and other new organizational models, along with interoperable electronic health records, can serve this role, and in doing so at least partially overcome the highly fragmented structure of the current system. Only if these initiatives can and do simultaneously recognize that the value proposition for their consumers is health, rather than health care, will they achieve the potential that is so desirable.
Disclosure
The authors report no conflicts of interest in this work.
References
Woolf SH, Aron L, Panel on Understanding Cross-National Health Differences Among High-Income Countries, Committee on Population, Division of Behavioral and Social Sciences and Education, National Research Council, Board on Population Health and Public Health Practice, Institute of Medicine. US Health in International Perspective: Shorter Lives, Poorer Health. Woolf SH, Aron L, editors. Washington, DC: The National Academies Press; 2013. | |
Porter ME. What is value in health care? N Engl J Med. 2010;363(26):2477–2481. | |
Porter M, Lee TH. The strategy that will fix health care. Harvard Business Review. October, 2013. | |
Kotler P. Marketing Management. 2nd ed. Englewood Cliffs, NJ: Prentice Hall; 1972. | |
Hamburg MA, Collins FS. The path to personalized medicine. N Engl J Med. 2010;363:301–304. | |
Collins FS, Varmus H. A new initiative on precision medicine. N Engl J Med. 2015;372:793–795. | |
Berenson RA, Cassel CK. Consumer-driven health care may not be what patients need – Caveat emptor. JAMA. 2009;301(3):321. | |
Frosch DL, May SG, Rendle KA, Tietbohl C, Elwyn G. Authoritarian physicians and patients fear of being labeled ‘difficult’ among key obstacles to shared decision making. Health Aff (Millwood). 2012;31(5):1030–1038. | |
Lusch RF. Exploring the health service ecosystem: a tribute to Leonard Barry. Paper presented at: PD Converse Symposium, 2008, Champaign, IL. | |
Bastiat F. Selected Essays on Political Economy, 1848. Reprint. Princeton, NJ: D Van Nostrand; 1964. | |
Vargo SL, Lusch RF. Evolving to a new dominant logic for marketing. J Mark. 2004;68(1):1–17. | |
Lusch RF, Vargo SL. Service Dominant Logic. Premises, Perspectives, Possibilities. Cambridge, UK: Cambridge University Press; 2014. | |
James J. Health policy brief: patient engagement. Health Aff (Millwood). 2013;32:1–6. | |
Hibbard JH, Stockard J, Mahoney ER, Tusler M. Development of the Patient Activation Measure (PAM): conceptualizing and measuring activation in patients and consumers. Health Serv Res. 2004;39(4 Pt 1):1005–1026. | |
Hibbard JH, Greene J. What the evidence shows about patient activation: better health outcomes and care experiences; fewer data on costs. Health Aff (Millwood). 2013;32(2):207–214. | |
Hibbard JH, Greene J, Overton V. Patients with lower activation associated with higher costs; delivery systems should know their patients’ ‘scores’. Health Aff (Millwood). 2013;32(2):216–222. | |
Hibbard JH, Mahoney ER, Stockard J, Tusler M. Development and testing of a short form of the patient activation measure. Health Serv Res. 2005;40(6 Pt 1):1918–1930. | |
Mosen DM, Schmittdiel J, Hibbard J, Sobel D, Remmers C, Bellows J. Is patient activation associated with outcomes of care for adults with chronic conditions? J Ambul Care Manage. 2007;30(1):21–29. | |
Legare F, Witteman HO. Shared decision making: examining key elements and barriers to adoption into routine clinical practice. Health Aff (Millwood). 2013;32(2):276–284. | |
Lin GA, Halley M, Rendle KA, et al. An effort to spread decision aids in five California primary care practices yielded low distribution, highlighting hurdles. Health Aff (Millwood). 2013;32(2):311–320. | |
Friedberg MW, Van Busum K, Wexler R, Bowen M, Schneider EC. A demonstration of shared decision making in primary care highlights barriers to adoption and potential remedies. Health Aff (Millwood). 2013;32(2):268–275. | |
Nease RF, Glave Frazee S, Zarin L, Miller SB. Choice architecture is a better strategy than engaging patients to spur behavior change. Health Aff (Millwood). 2013;32(2):242–249. | |
King J, Moulton B. Group Health’s participation in a shared decision-making demonstration yielded lessons, such as role of culture change. Health Aff (Millwood). 2013;32(2):294–302. | |
Bernabeo E, Holmboe ES. Patients, providers, and systems need to acquire a specific set of competencies to achieve truly patient-centered care. Health Aff (Millwood). 2013;32(2):250–258. | |
Hoffmann TC, Montori VM, Del Mar C. The connection between evidence-based medicine and shared decision making. JAMA. 2014; 312(13):1295–1296. | |
Djulbegovic B, Guyatt GH. Evidence-based practice is not synonymous with delivery of uniform health care. JAMA. 2014;312(13):1293–1294. | |
McColl-Kennedy JR, Vargo SL, Dagger TS, Sweeney JC, Van Kasterin Y. Health care customer value cocreation practice styles. J Service Res. 2012;15(4):370–389. | |
Butler C, Rollnick S. Motivational Interviewing in Health Care: Helping Patients Change Behavior. New York, NY: The Guilford Press; 2008. | |
DeJonge KE, Taler G, Boling P. Independence at home: community-based care for older adults with severe chronic illness. Clin Geriatr Med. 2009;25(1):155–169. | |
Berry L. Profiles in improvement. Paper presented at: Institute for Healthcare improvement, December 2014. | |
Berry L, Seltman K. Management Lessons from Mayo Clinic: Inside One of the World’s Most Admired Service Organizations. New York, NY: McGraw Hill; 2008. | |
Topal E. The creative destruction of medicine. New York, NY, USA: Basic Books; 2012. | |
Parry C, Coleman E, Smith J, Frank J, Kramer A. The care transitions intervention: a patient-centered approach to facilitating effective transfers between sites of geriatric care. Home Health Services Quarterly. 2003;22(3):1–18. | |
EA C, Parry C, Chalmers S, Min SJ. The care transitons intervention. Results of a ramdomized controlled trial. JAMA. 2006;166(17):1822–1828. | |
Schork NJ. Personalized medicine: time for one-person trials. Nature. 2015;520:7549. | |
Nambisan P, Nambisan S. Models of consumer value cocreation in health care. Health Care Manage Rev. 2009;34(4):344–354. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.