Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Ever Smoking is Not Associated with Performed Spirometry while Occupational Exposure and Respiratory Symptoms are
Authors Carlsson L ![]() , Holm M, Edlund M, Ekström M
, Holm M, Edlund M, Ekström M ![]() , Torén K
, Torén K ![]()
Received 26 October 2022
Accepted for publication 6 March 2023
Published 17 March 2023 Volume 2023:18 Pages 341—348
DOI https://doi.org/10.2147/COPD.S394832
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Linnea Carlsson,1,2 Mathias Holm,2 Maria Edlund,2 Magnus Ekström,3 Kjell Torén1,4
1Occupational and Environmental Medicine, Department of Public Health and Community Medicine, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; 2Occupational and Environmental Medicine, Department of Medicine, Sahlgrenska University Hospital, Gothenburg, Sweden; 3Lund University, Faculty of Medicine, Department of Clinical Sciences Lund, Respiratory Medicine, Allergology and Palliative Medicine, Lund, Sweden; 4Discipline of Occupational and Environmental Health, University of KwaZulu-Natal, Durban, South Africa
Correspondence: Linnea Carlsson, Occupational and Environmental Medicine, Department of Medicine, Sahlgrenska University Hospital, PO Box 414, Gothenburg, SE 405 30, Sweden, Email [email protected]
Objective: Despite recommendations, assessment using spirometry or peak expiratory flow is insufficient in the clinical evaluation of suspected obstructive pulmonary disease. The aim was to investigate factors associated with performing spirometry or peak flow expiratory flow assessment.
Methods: Randomly selected subjects from the general population aged 50– 65 completed a respiratory questionnaire with items about the history of previously performed spirometry or peak expiratory flow. The association between ever having had spirometry or peak expiratory flow performed was analyzed for smoking, age, sex, occupational exposures, dyspnea, wheeze, self-reported physician diagnosed asthma and COPD using multivariable logistic regression models. The results are presented as odds ratios (OR) with 95% confidence intervals (95% CIs).
Results: Of the 1105 participants, 43.4% (n=479) had a history of previously performed spirometry or peak expiratory flow. Occupational exposure (OR 1.72, [95% CI] 1.30– 2.27), wheeze (OR 2.29, 1.41– 3.70), and dyspnea (OR 1.70, 1.11– 2.60) were associated with previously performed spirometry. Compared to men, women had spirometry or peak expiratory flow performed less often (OR 0.67, 0.51– 0.86). Neither current smoking (OR 0.83, 0.57– 1.20) or former smoking (OR 1.27, 0.96– 1.67) were associated with performed spirometry or peak expiratory flow.
Conclusion: We found no relation between smoking status and a history of previously performed spirometry or peak expiratory flow in a population-based sample of middle-aged people. This is surprising regarding the strong guidelines which highlight the importance for spirometry surveillance on current smokers due to their increased risk of lung disease. Male sex, respiratory symptoms and occupational exposures to air pollution were associated with previously performed spirometry or peak expiratory flow. The association with occupational exposure may be an effect of pre-employment screening and workplace surveillance, and the findings indicate that females do not receive the same attention regarding spirometry or peak expiratory flow.
Keywords: lung function test, spirometry and PEF, smoking, occupational exposure, respiratory symptoms, SCAPIS pilot
Introduction
The pulmonary function tests dynamic spirometry and peak expiratory flow (PEF) are reliable and valid tests to measure lung function and are corner stones in diagnosing and managing obstructive disease.1 From the spirometry and a forced expiratory maneuver, the forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), and their ratio (FEV1/FVC) as a measure of airflow limitation can be assessed. Spirometry is one of the key instruments in the assessment of chronic obstructive pulmonary diseases (COPDs), where both past and current smokers are at markedly increased risk for developing the disease.1,6 Spirometry is also important in the diagnosis of asthma, ie, for assessing reversibility and bronchial hyperresponsiveness, and in the evaluation of potential restrictive lung disorders.2,3 Spirometry is also an important test in pre-employment screening and in surveillance of workers with exposure to occupational hazards such as silica dust, asbestos and di-isocyanates.4,5
An alternative to spirometry for the diagnosis and management of asthma, including occupational asthma, is assessment of the peak expiratory flow (PEF).2,7 PEF is less reliable than spirometry for diagnosing asthma but can still be valuable for monitoring asthma, especially if there is no access to spirometry.7
Despite the high validity, low cost and a rather simple procedure, spirometry and PEF seem to be underused in clinical practice. A Swedish study found that one-third of patients with asthma were investigated with PEF and only one-third of patients with COPD were investigated with spirometry at their initial visit.8 Similar results with underuse of spirometry in the diagnosis of COPD and asthma have been reported by other studies.9–14
There is scarce knowledge as to why spirometry is underused. A visit to a hospital specialist seems to be associated with the use of spirometry, whereas primary care physicians may underuse spirometry.14,15 Regarding the given guidelines,1,27 tobacco smoking should be associated with performed spirometry. However, in most studies in this area, there are no reports on whether tobacco smoking is associated with performed spirometry. In a few studies, the association with smoking has been assessed but without finding any significant associations.11,14,15 In some studies, spirometry is used less for female patients than males.16,17 Concurrently, there are studies with no gender difference or less used spirometry for men.10,15,19
Previous research has mainly focused on the use of spirometry in cohorts of primary care patients, often with pre-existing asthma or COPD. To the best of our knowledge, there is a lack of research on factors associated with performed spirometry or PEF in the general population. Therefore, the aim of the present study was to, in a general population sample, evaluate factors associated with a history of spirometry or PEF, focusing on sex, smoking, respiratory symptoms and exposure to occupational hazards.
Materials and Methods
Study Population
This was a population-based, cross-sectional study of participants in the Swedish CArdioPulmonary BioImage Study (SCAPIS) pilot. The SCAPIS main study is a multicenter, prospective, observational study including 30,000 randomly selected subjects from the Swedish population register, aged 50–64.20 The SCAPIS pilot study was performed to ensure feasibility, financial and ethical consequences of the main SCAPIS study and included information on previous spirometry and/or PEF. In the SCAPIS pilot, subjects aged 50–64 were selected randomly from the general population in the city of Gothenburg in 2012, where they were sampled equally from areas with high and low socioeconomic status.
Data Collection
The methods and data collection have been described previously.21 The subjects completed a questionnaire with 206 items including information on the history of previous spirometry or PEF, individual characteristics, smoking habits, respiratory symptoms and occupational exposures. The study participants also performed dynamic spirometry (Jaeger MasterScreen PFT, Carefusion, Hoechberg, Germany) according to the Burden of Obstructive Lung Disease (BOLD) study protocol to measure forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC).22 Spirometry was performed before and 15 minutes after inhalation of 400 µg salbutamol. Reference values of FEV1 and FVC were based on a local reference equation.23
Definitions
A history of previously performed spirometry or PEF was defined as an affirmative answer to the question “Have a physician or other medical staff ever let you breathe in a machine/apparatus to measure your lung function (eg, a spirometer or peak flow meter)?” And: “Have you breathed in such a machine/apparatus within the last 12 months?”. Chronic airflow limitation (CAL) was defined as a FEV1/FVC ratio <0.7 after bronchodilation.1 Smoking status was categorized as current smoker, former smoker or never-smoker. Former smokers were defined as those who had smoked for at least 1 year but not during the past year. Occupational exposure to vapor, gas, dust or fumes (VGDF), occupational air pollution, was confirmed by an affirmative answer to the question “Have you ever been exposed at your workplace to vapor, gas, dust, or fumes?” Wheeze was defined by an affirmative answer to: “Do you usually have wheezing or whistling in your chest when breathing?” Physician-diagnosed asthma was defined by an affirmative answer to: “Have you ever had asthma diagnosed by a physician?”.24 Physician-diagnosed COPD/emphysema was defined by an affirmative answer to: “Have you ever had chronic obstructive pulmonary disease or emphysema diagnosed by a physician?”.25 Dyspnea was defined by an affirmative answer to: “Do you experience shortness of breathing when in a hurry walking on flat ground or minor ascents?” Corresponding to a modified Medical Research Council (mMRC) score ≥1.26
Statistical Analyses
Associations with a history of performed spirometry or PEF were analyzed using multivariable logistic regression, expressed as adjusted OR with 95% CI. Separate analysis was made for ever performed spirometry or PEF and within 12 months. Independent variables to include in the models were selected a priori based on subject matter knowledge: smoking status, gender, age, occupational exposure to vapor, gas, dust and fumes (VGDF), wheeze, dyspnea, physician-diagnosed asthma and self-reported COPD/emphysema.
The regression models were performed in a stepwise manner: first a basic model including smoking status, age and gender. Then, analyses with each independent variable added separately to the basic model were performed, in the following order: occupational exposure to VGDF, dyspnea, wheeze, physician-diagnosed asthma and COPD/emphysema. Lastly, a full model was evaluated that included current smoker, former smoker, gender, age, occupational exposure to VGDF, wheeze, and dyspnea. Physician-diagnosed COPD and physician-diagnosed asthma were excluded in the full model due to few subjects. Data management and analysis were performed with SAS version 9.2 (SAS Institute, Cary, North Carolina, USA).
Results
Of the 2243 individuals who were invited to participate in the clinical investigation, 1111 answered the questionnaire. In this study, 1105 cases, where information regarding the history of spirometry or PEF was known, were analyzed, resulting in 552 female and 553 male cases.
Of 1105 investigated persons, 479 (43.4%) had a history of previously performed spirometry or PEF (Table 1). Of those who had a history of previously performed spirometry or PEF, 166 (34.7%) had performed spirometry within the last 12 months.
 |
Table 1 Descriptive Data of Subjects with and without History of Spirometry or PEF |
In the basic models, former smoking (OR 1.42, 95% CI 1.09–1.86), occupational exposure to VGDF (OR 1.83, 95% CI 1.40–2.39), wheeze (OR 2.86, 95% CI 1.81–4.51), and dyspnea (PR 2.12, 95% CI 1.41–3.17) were associated with previously performed spirometry. Current smoking did not show an association with previous history of performed spirometry (OR 1.02, 95% CI 0.73–1.44) (Table 2). The findings were similar for men and women, although the odds ratio for former smoking decreased for women (OR 1.22, 95% CI 0.83–1.79). The odds ratio for a history of previously performed spirometry was lower among women as compared to men (OR 0.63, 95% CI 0.50–0.90).
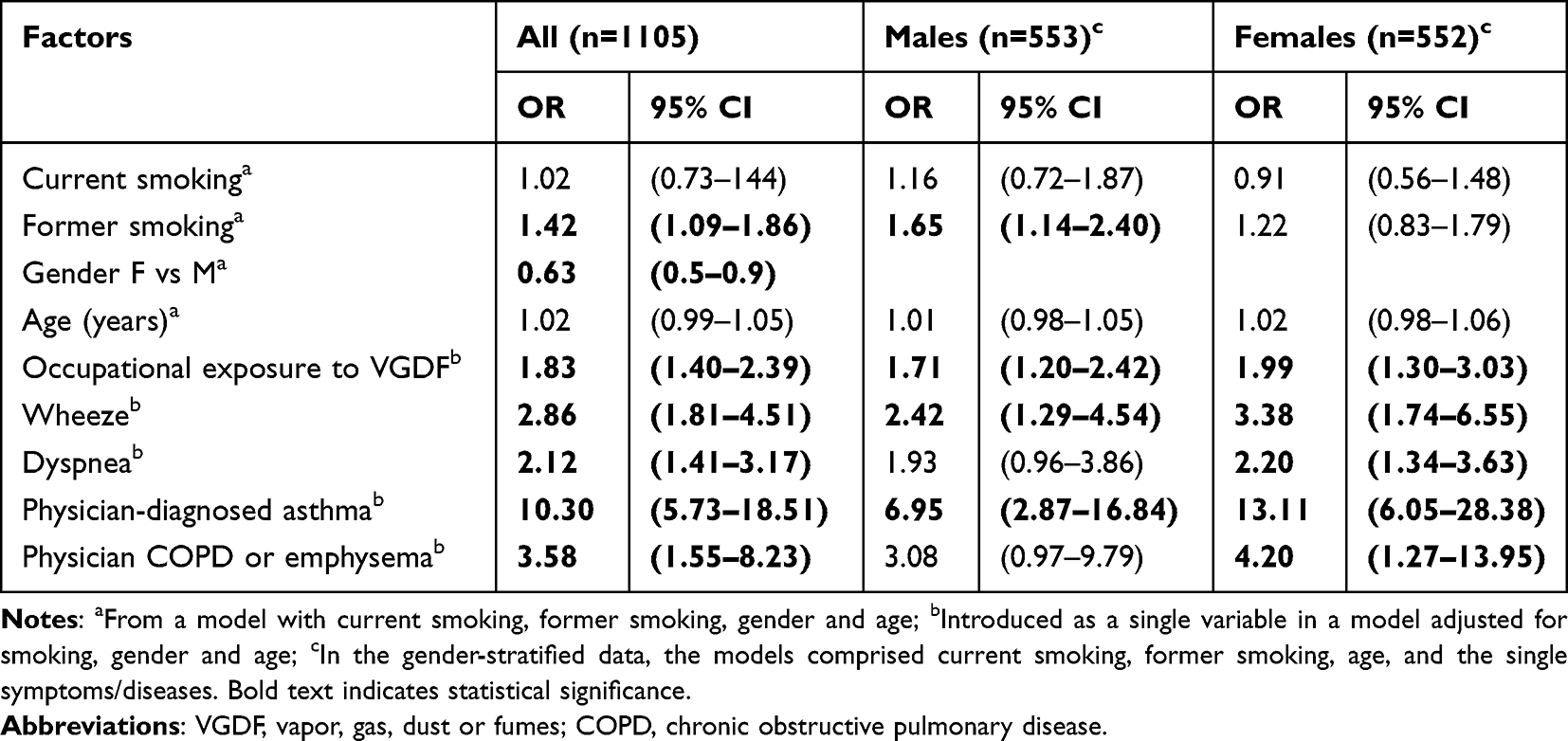 |
Table 2 Factors Associated with a History of Previously Performed Spirometry or PEF (n=479) in Basic Models. Presented as Odds Ratio (OR) with 95% Confidence Intervals (CI) |
In the full model, the increased odds ratios for previously performed spirometry remained for occupational exposure to VGDF, wheeze and dyspnea (Table 3). The associations with former smoking disappeared in the full model which was adjusted for VGDF and respiratory symptoms. This was also seen in the separate models for men and women. The lower odds of previous spirometry among women, compared with men, remained in the full model (OR 0.67, 95% CI 0.51–0.86).
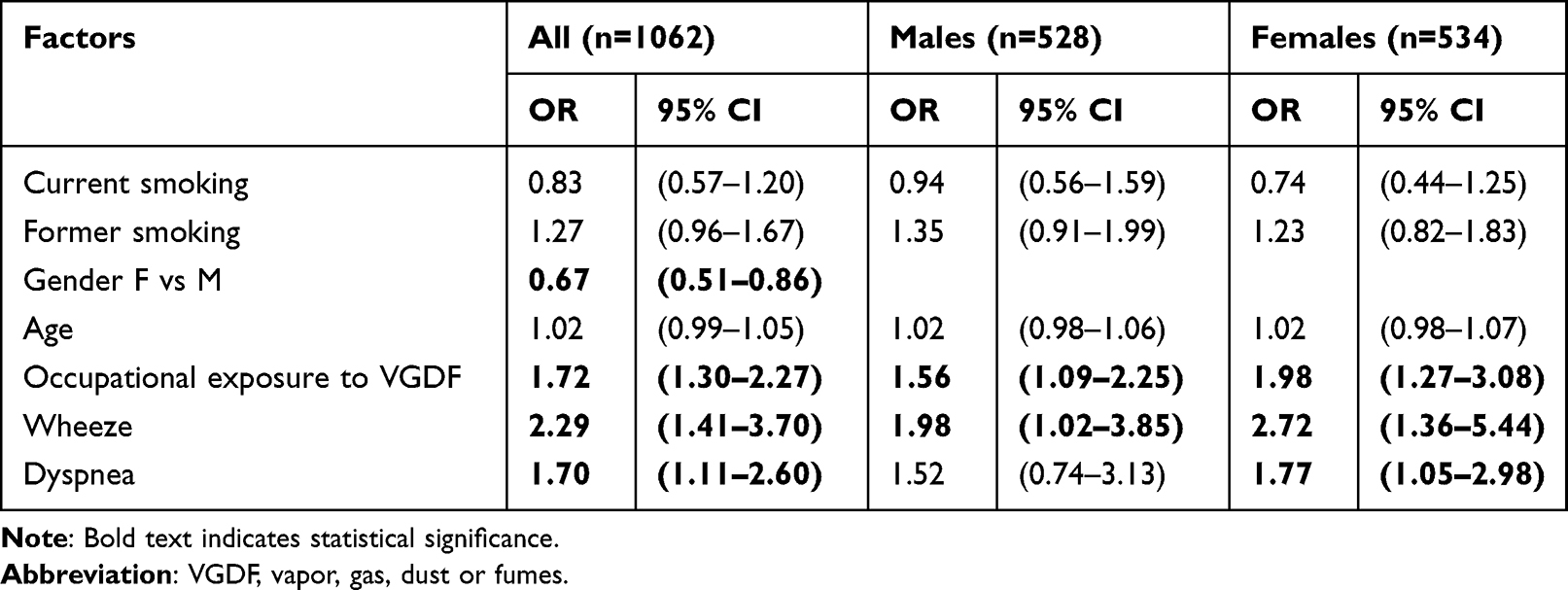 |
Table 3 Factors Associated with a History of Previously Performed Spirometry or PEF (n=479) in a Full Model Comprising All Co-Variates Presented as Odds Ratios (OR) with 95% Confidence Intervals (CI) |
When we analyzed factors associated with spirometry having been performed within the last 12 months, there were associations with occupational exposure to VGDF (OR 2.17, 95% CI 1.47–3.20), wheeze (OR 2.54, 95% CI 1.38–4.69), and dyspnea (OR 2.50, 95% CI 1.47–4.25) (Table 4). There was no relation to either current smoking or former smoking. Regarding gender, the odds ratio indicated underuse of spirometry among women, but with the confidence interval including unity (OR 0.77, 95% CI 0.53–1.13).
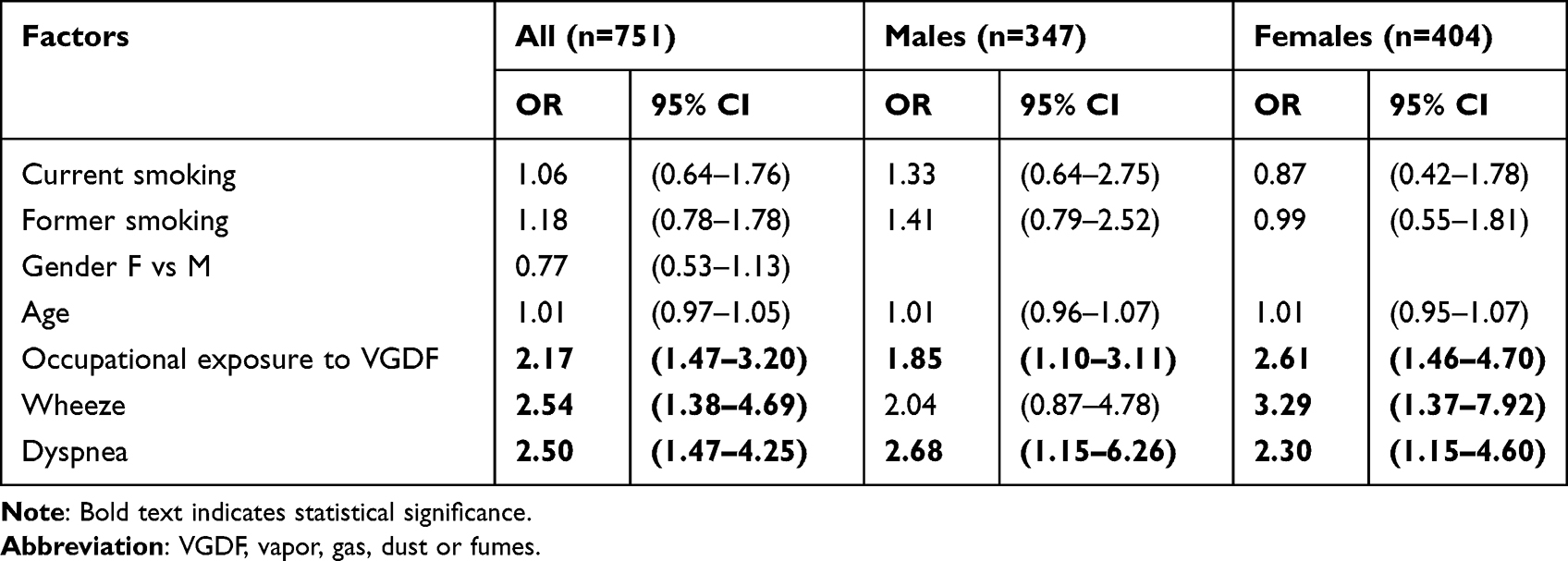 |
Table 4 Factors Associated with Previously Performed Spirometry or PEF Within the Last 12 Months (n=162). Odds Ratios (OR) with 95% Confidence Intervals (CI) from Single Models Comprising All Co-Variates |
Discussion
The main findings in this study were that current smoking or former smoking were not associated with previously performed spirometry or PEF, and that, compared to men, women were less likely to have performed spirometry or PEF. The strongest associated factor with having performed spirometry or PEF was occupational exposure to VGDF.
Current and former smokers are at high-risk of developing COPD and in several guidelines, including a guideline from the Swedish National Board of Health and Welfare, it is recommended that these groups should be assessed with spirometry.6,27 Especially between the ages of 50 and 64 years (the age interval in which our study was performed), people with a history of smoking should have a history of spirometry testing. However, in the basic models, former smoking was associated with previously performed spirometry or PEF. This association disappeared in the fully adjusted models though.
There are several studies reporting that smokers are under-investigated regarding spirometry.6,11,14,15 Previous research has also disclosed how smokers are less likely to seek health care for respiratory symptoms like cough, breathlessness or hoarseness than non-smokers.28,29 Previous studies have demonstrated how the limited use of spirometry contributes to underdiagnosis of asthma and COPD. This is because there are several barriers to performing spirometry, ranging from lack of education to problems interpreting spirometric results.8,30–32 An uncertainty interpreting spirometry values has been highlighted as a reason for not performing the tests. Consequently, spirometry use is higher among physicians who are comfortable interpreting the results.8
There are studies indicating that current smokers who performed spirometry, quit smoking to a larger extent than controls, after the test.6,33,34 If so, this will result in a higher prevalence of former smokers in the group with a previous history of performed spirometry. However, this was not observed in our full model. Irrespectively, this study’s results support actions to understand and to target both current and former smokers regarding their smoking habits and healthcare-seeking behavior. Occupational exposure to VGDF was clearly associated with previously performed spirometry or PEF. It was observed both among men and women and was found both in the basic models and in the full models. There are several guidelines suggesting that workers who are exposed to respiratory hazards should be screened with spirometry, and in case of occupational exposure to specific respiratory hazards, the Swedish work Authority’s regulations require spirometry.4,5,35 Our results could be a consequence of these recommendations and regulations in persons exposed to occupational air pollution.
We found that females, compared to males, were less likely to have performed spirometry or PEF. Similar results have been found in other studies.16,17 However, there are studies showing that males are less investigated with spirometry compared to females.10,15,18 One mechanism for our observation that females less often do spirometry or PEF could be that male workers were more likely to be exposed to occupational hazards, VGDF, than female workers.36 However, in our models, we adjusted for exposure to occupational air pollution, making that explanation less probable even if the Swedish Work Environment Authority reports that male workers have more access to occupational health care service.37 Hence, we conclude that our observation that spirometry is underused among females reflects a real gender inequality regarding spirometry use.
Adults with presented airway symptoms such as dyspnea and current wheeze are recommended by the Swedish National Board of Health and Welfare guidelines to be assessed with a spirometry.27 Our results indicate that persons with dyspnea or wheeze have an increased prevalence of a history of spirometry or PEF. This observation probably has several explanations but may be partly due to existing guidelines.
A major strength of this study was that the participants represent the general population in the age span 50–64 years, thus providing population estimates. Additionally, to our knowledge, this is the first study to examine individual characteristics, occupational exposure and respiratory symptoms as predictors for performing spirometry or PEF. Such information is of great importance in developing and providing healthcare on equal basis. Another strength is that the study is well characterized with a validated questionnaire.
A notable limitation was the impossibility of distinguishing between spirometry and PEF for the outcome variable. There are reasons to believe that even if these tests would have been separated in the self-administrated questionnaire, it may still have been difficult for individuals to differentiate between spirometry or PEF. Spirometry is, however, the primarily recommended test to assess COPD and asthma, and the recommended test in workplace surveillance.5 If recommendations are applied in clinical practice, spirometry may be the predominant test among the study participants.
Another limitation is that we used logistic regression models assessing prevalence odds ratios. When the outcome is rare, this is rather unproblematic. However, when the prevalence is not obviously low, as in our study, where the prevalence of performed spirometry is 43.4%, the odds ratios may have been overestimated.38 It is important to note that the prevalence of the outcome spirometry or PEF in the last 12 months was 21.5% and the assessed odds ratios were quite similar. Therefore, we consider our results valid.
Another weakness is our limited age interval, 50–64 years of age, and a skewed socioeconomic sample.39 For SCAPIS pilot, randomly selected individuals from opposite extremes of socioeconomic status in the City of Gothenburg were selected to gain knowledge about socioeconomic differences in risk factor distributions for diseases, and more specifically, cardiopulmonary diseases. In Bjork et al40 study, they highlight the effects of selection in population-based studies and compared the participants to non-participants for the main SCAPIs study. It displays how residential area (high/low SES), country of birth, civil status, education, occupational status, and disposable income were clearly associated with participation. Still, the relationships we study are not affected by selection bias and our results are only valid for a middle-age interval. Lastly, for some items in the self-reported questionnaire, there is a risk of recall bias. We also stress that the cross-sectional study design means that no conclusions on causality can be drawn.
Conclusions
We found no relation between smoking and previously performed spirometry. This is surprising, considering the strong guidelines which highlight the importance of spirometry surveillance on current smokers due to their increased risk of developing lung disease. These findings call for future research in understanding smokers’ insufficient health care connection and healthcare interventions targeting smokers. Being a man, having respiratory symptoms or occupational exposures to air pollution were associated with previously performed spirometry. The results indicate that women are not receiving the same attention regarding spirometry. The association with occupational exposure may be an effect of pre-employment screening and workplace surveillance.
Ethical Approval
The study was approved by the Regional Committee of Ethics in Umeå (2010/228-31, 2017/14-31) and by the Swedish Ethical Review Authority (2022-04272-02). All included subjects gave their written consent to participate in the study. Our study complies with the Declaration of Helsinki, and all participants were informed about the purpose of the study.
Acknowledgments
The study was supported by the Swedish Heart and Lung Foundation, the Knut and Alice Wallenberg Foundation, the Swedish Research Council (VR), VINNOVA and the Swedish Council for Working Life, Health, and Welfare (FORTE), the Sahlgrenska Academy at the University of Gothenburg, and strategic grants from ALF/LUA in Western Sweden.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Global Initiative for Chronic Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2022 report). GOLD-REPORT-2022-v1.1–22Nov2021_WMV.pdf (goldcopd.org); 2022.
2. Global Initiative for Asthma (GINA). Global strategy for asthma management and preventions, updated 2021. GINA Full Report 2021 Front Cover ONLY (ginasthma.org); 2021.
3. Graham B, Steenbruggen I, Miller M, et al. Standardization of spirometry 2019 update. An official American Thoracic Society and European Respiratory Society technical statement. Am J Respir Crit Care Med. 2019;200:E70–E88. doi:10.1164/rccm.201908-1590ST
4. Townsend C, Lockey M, Velez I, et al. Spirometry in the occupational setting. J Occup Environ Med. 2020;42:228–245. doi:10.1097/00043764-200003000-00003
5. Redlich C, Tarlo S, Hankinson J, et al. Official American Thoracic Society technical standards: spirometry in the occupational setting. Am J Respir Crit Care Med. 2014;189(8):983–993. doi:10.1164/rccm.201402-0337ST
6. Ferguson GT, Enright PL, Buist AS, Higgins MW. Office spirometry for lung health assessment in adults. A consensus statement from the national lung health education program. Chest. 2000;117:1146–1161. doi:10.1378/chest.117.4.1146
7. Wells CD, Joo MJ. COPD and asthma: diagnostic accuracy requires spirometry. J Fam Pract. 2019;68:76–81.
8. Weidinger P, Nilsson J, Lindblad U. Adherence to diagnostic guidelines and quality indicators in asthma and COPD in Swedish primary care. Pharmacoepidemiol Drug Saf. 2009;18:393–400. doi:10.1002/pds.1734
9. Caramori G, Bettoncelli G, Tosatt R, et al. Underuse of spirometry by general practitioners for the diagnosis of COPD in Italy. Monaldi Arch Chest Dis. 2005;63:6–12. doi:10.4081/monaldi.2005.651
10. Joo M, Au J, Fitzgibbon D, McKell H, Lee M. Determinants of spirometry use and accuracy of COPD diagnosis in primary care. J Gen Int Med. 2011;26:1272–1277. doi:10.1007/s11606-011-1770-1
11. Monteaguado M, Rodriguez-Blanco T, Parcet J, et al. Variability in the performing of spirometry and its consequences in the treatment of COPD in primary care. Arch Bronconeumol. 2011;47:226–233. doi:10.1016/S1579-2129(11)70057-X
12. Sokol K, Sharma G, Lin Y, Goldblum R. Choosing Wisely: adherence by physicians to recommended use of spirometry in the diagnosis and management of adult asthma. Am J Med. 2015;128:502–508. doi:10.1016/j.amjmed.2014.12.006
13. Heffler E, Crimi C, Mancuso S, et al. Misdiagnosis of asthma and COPD and underuse of spirometry in primary care unselected patients. Respir Med. 2018;142:48–52. doi:10.1016/j.rmed.2018.07.015
14. Roychowdhury P, Badwal J, Alkhatib F, et al. Spirometry utilization among patients with asthma. J Asthma Allergy. 2020;13:193–203. doi:10.2147/JAA.S254431
15. Arne M, Lisspers K, Ställberg B, et al. How often is diagnosis of COPD confirmed with spirometry? Respir Med. 2010;104:550–556. doi:10.1016/j.rmed.2009.10.023
16. Delgado A, Saletti-Cuesta L, López-Fernández L, Gil-Garrido N, Luna Del Castillo J. Gender inequalities in COPD decision-making in primary care. Respir Med. 2016;114:91–96. doi:10.1016/j.rmed.2016.03.017
17. Watson L, Vestbo J, Postma DS, et al. Gender differences in the management and experience of chronic obstructive pulmonary disease. Respir Med. 2004;98(12):1207–1213. doi:10.1016/j.rmed.2004.05.004
18. Koefoed MM, de Pont Christensen R, Søndergaard J, Ejg Jarbøl D. Lack of spirometry use in Danish patients initiating medication targeting obstructive lung disease. Respir Med. 2012;106(12):1743–1748. doi:10.1016/j.rmed.2012.09.012
19. Akbarshahi H, Ahmadi Z, Currow D, et al. No gender-related bias in COPD diagnosis and treatment in Sweden: a randomised, controlled, case-based trial. ERJ Open Res. 2020;6(4):00342–2020. doi:10.1183/23120541.00342-2020
20. Bergström G, Persson M, Adiels M, et al. Prevalence of subclinical coronary artery atherosclerosis in the general population. Circulation. 2021;144(12):916–929. doi:10.1161/CIRCULATIONAHA.121.055340
21. Toren K, Olin AC, Lindberg A, et al. Vital capacity and COPD: the Swedish CArdioPulmonary bioImage Study (SCAPIS). Int J COPD. 2026;11:927–933.
22. Buist S, McBurnie MA, Vollmer WM, et al; On behalf of the Bold Collaborative Research Group. International variation in the prevalence of COPD (The BOLD study): a population-based prevalence study. Lancet. 2007;370:741–750. doi:10.1016/S0140-6736(07)61377-4
23. Brisman J, Kim JL, Olin AC, Torén K, Bake B. Spirometric reference equations for Swedish adults. Clin Physiol Funct Imaging. 2017;37:640–645. doi:10.1111/cpf.12349
24. Torén K, Brisman J, Järvholm B. Asthma and asthma-like symptoms in adults assessed by questionnaires. Chest. 1993;104:600–608. doi:10.1378/chest.104.2.600
25. Torén K, Murgia N, Olin AC, et al. Validity of physician-diagnosed COPD in relation to spirometric definitions of COPD in a general population study – the SCAPIS pilot study. Int J COPD. 2017;12:2269–2275. doi:10.2147/COPD.S136308
26. Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW, Wedzicha JA. Usefulness of the Medical Research Council (MRC) dyspnoea scale as measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54:581–586. doi:10.1136/thx.54.7.581
27. National Board of Health and Welfare. Nationella riktlinjer för vård vid astma och KOL [National guidelines for care of asthma and COPD]. Stöd för styrning och ledning (Artikelnummer 2018-1-36). Swedish. Swedish https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/nationella-riktlinjer/2020-12-7135.pdf.
28. Friedemann Smith C, Whitaker KL, Winstanley K, Wardle J. Smokers are less likely than non-smokers to seek help for a lung cancer ‘alarm’ symptom. Thorax. 2016;71:659–661. doi:10.1136/thoraxjnl-2015-208063
29. Walabyecki J, Adamosn J, Buckley KHL, et al. Experience of, awareness of - seeking for potential cancer symptoms in smokers and non-smokers: a cross-sectional study. PLosOne. 2017;12:e0183647. doi:10.1371/journal.pone.0183647
30. Jain V, Allison D, Andrews S, Mejia J, Mills P, Peterson M. Misdiagnosis among frequent exacerbators of clinically diagnosed asthma and COPD in absence of confirmation of airflow obstruction. Lung. 2015;193:505–512. doi:10.1007/s00408-015-9734-6
31. Roberts NJ, Smith SF, Partridge MR. Why is spirometry underused in the diagnosis of the breathless patient: a qualitative study. BMC Pulm Med. 2011;11:37. doi:10.1186/1471-2466-11-37
32. Rothnie KJ, Chandan JS, Goss HG, Müllerová H, Quint JK. Validity and interpretation of spirometric recordings to diagnose COPD in UK primary care. Int J COPD. 2017;12:1663–1668. doi:10.2147/COPD.S133891
33. Segnan N, Ponti A, Battista RN, et al. A randomized trial of smoking cessation interventions in general practice in Italy. Cancer Causes Control. 1991;2:239–246. doi:10.1007/BF00052140
34. Humerfelt S, Eide GE, Kvåle G, Aarø LE, Gulsvik A. Effectiveness of postal smoking cessation advice: a randomized controlled trial in young men with reduced FEV1 and asbestos exposure. Eur Respir J. 1998;11:284–290. doi:10.1183/09031936.98.11020284
35. Swedish Work Enviroment Authority. Medical check-ups in working life[Medicinska kontroller i arbetslivet]. Vol. 3. Stockholm, Sweden: AFS; 2019. Swedish.
36. Lytras T, Kogevinas M, Kromhout H, et al. Occupational exposures and 20-year incidence of COPD: the European community respiratory health survey. Thorax. 2018;73:1008–1015. doi:10.1136/thoraxjnl-2017-211158
37. The Swedish Work Environment Authority. The work environment 2019 (2020:2). Arbetsmiljön 2019, rapport 2020:2 (av.se); 2019. Swedish.
38. Axelson O, Fredriksson M, Ekberg K. Use of the prevalence ratio vs. the prevalence odds ratio as a measure of risk in cross sectional studies. Occup Environ Med. 1994;51:574. doi:10.1136/oem.51.8.574
39. Bergström G, Berglund G, Blomberg A, et al. The Swedish CArdioPulmonary BioImage Study: objectives and design. J Intern Med. 2015;278(6):645–659. doi:10.1111/joim.12384
40. Bjork J, Strömberg U, Rosengren A, et al. Predicting participation in the population-based Swedish cardiopulmonary bio-image study (SCAPIS) using register data. Scand J Public Health. 2017;45:45-.49, 45, 45–49.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.