Back to Journals » Clinical Ophthalmology » Volume 16
Evaluation of Urgent Retinal Practice and Safety Measures for Physicians and Patients During COVID-19 Pandemic
Authors Alagorie AR ![]() , Sorour OA, Eltoukhy H, Nassar E
, Sorour OA, Eltoukhy H, Nassar E
Received 24 December 2021
Accepted for publication 6 April 2022
Published 21 April 2022 Volume 2022:16 Pages 1197—1205
DOI https://doi.org/10.2147/OPTH.S355628
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ahmed Roshdy Alagorie, Osama A Sorour, Hesham Eltoukhy, Elsayed Nassar
Department of Ophthalmology, Faculty of Medicine, Tanta University, Tanta, Egypt
Correspondence: Ahmed Roshdy Alagorie, Department of Ophthalmology, Faculty of Medicine, Tanta University, Tanta, Egypt, Email [email protected]
Purpose: To assess the impact of the COVID-19 pandemic on urgent retina practice and factors influencing adherence of physicians and patients to safety measures.
Methods: In this clinical audit, urgent or emergent vitreoretinal surgical disorders that presented to our hospital during the period of 15th March– 15th May 2020 were compared with the period just before the pandemic declaration (15th December 2019– 15th February 2020). Additionally, two questionnaires assessing the adherence to safety measures were circulated to the medical personnel and a sample of patients. The collected data were analyzed, and accordingly, recommendations were proposed to the hospital administration and specific corrective measures were applied. The outcome of applying these corrective measures was assessed in the re-audit cycle during the period of 15th June– 15th August 2020.
Results: There was a significant decrease in the number of urgent or emergent vitreoretinal surgical disorders that presented to our hospital during the pandemic (161 versus 302 cases in a similar period before the pandemic; p = 0.022). Just with the pandemic recession, there was a significant increase in the number of urgent cases (391 versus 161 cases during the pandemic; p = 0.006), also there was an increased number of complex cases. Residents and fellows were less compliant than attending physicians in adherence to safety measures.
Conclusion: Delayed presentation of urgent retinal cases during the pandemic highlights the importance of public awareness of urgent conditions that need immediate medical or surgical care. Attention to young physicians during the pandemic is crucial as they are less adherent to safety measures due to work overload.
Keywords: COVID-19, retina practice, audit
Introduction
The newly discovered coronavirus disease (COVID-19) was claimed, for the first time at the end of 2019, in Wuhan – China, and rapidly became a global pandemic.1 On March 11, 2020, the World Health Organization (WHO) confirmed the COVID-19 as a pandemic outbreak.2
The Egyptian government promptly responded to this pandemic in order to fight the virus and limit its spread. Cities and governorates were partially locked down, non-essential businesses were closed, all teaching and academic activities of schools and universities became online, scientific meetings have been canceled and became online through webinars. Outpatient clinics have been limited to the essential service and elective procedures have been postponed. Public health authorities urged the public to stay at home and seek medical care only for urgent conditions. Physicians were using telemedicine tools to communicate with their patients as much as possible.3
Until now, there are no proven measures to treat the novel COVID-19 disease. Infected persons can develop severe respiratory distress and multi-organ failure resulting in death. The clinical course might become stormy in case of depressed immune status and advanced age.4,5 In addition, multiple ocular manifestations have been reported with COVID-19.6–8
Most ophthalmological examinations require close contact with the patient’s eye, thus increasing the risk of infection to the physicians and patients, especially with the shortage of personal protective equipment such as masks, gloves, and gowns.9,10 During the pandemic, retina practice constituted a challenging situation as it included a wide variety of medical and surgical disorders that might lead to visual loss if not promptly and adequately treated such as retinal detachment, retinal vascular occlusion, and choroidal neovascularization.11,12
Previous studies have reported a reduction of the retinal photoreceptor layer by about 10% of normal width and significant ganglion cell layer changes within a week after retinal detachment.13,14 Moreover, the postoperative final corrected visual acuity significantly correlates with the duration of macular detachment.15
The primary objective of our study was to identify the impact of the COVID-19 pandemic on the number of urgent or emergent vitreoretinal surgical disorders presented to a tertiary ophthalmic center, and the secondary objective was to evaluate adherence of the medical staff and patients to safety measures and factors affecting it.
Patients and Methods
This was a clinical audit performed at Tanta University Hospitals during the period of 15th March–15th May, 2020. Re-audit was conducted during the period of 15th June–15th August, 2020. The audit and re-audit were approved by the Institutional Review Board and adhered to the tenets of Helsinki's declaration. Written informed consent was obtained from all the subjects before enrollment in the study.
Audit Rationale
Implementation of COVID-19 pandemic on urgent retina practice was assessed by evaluating the number and types of urgent or emergent vitreoretinal surgical disorders, as determined by the American Academy of Ophthalmology,16 that presented to the retina service in our hospital during the period of 15th March–15th May, 2020 and compared to the period of 15th December, 2019–15th February, 2020, just before declaration of the pandemic and before any restrictions were applied nationally. Cases that were evaluated included retinal detachment with proliferative vitreoretinopathy (PVR) less than grade B, retinal detachment with PVR more than grade B, tractional retinal detachment threatening or involving the fovea, intraocular foreign body, endophthalmitis, and retinal detachment following globe injuries.
Secondly, a questionnaire assessing the adherence to safety measures during the COVID-19 pandemic and its consequences on the retina practice was circulated to the professors, attending physicians, fellows, residents, and the assisting paramedical staff in the hospital. The questionnaire evaluated adherence to wearing masks and gloves and frequency of changing the mask, hand hygiene after the examination and duration of hand washing, asking patients about Covid-19 symptoms before the examination, implementing social distancing to patients and colleagues, what the physician will do if he feels that the patient is infected with Covid-19 and how much he describes his fear to be infected, and lastly, duration of the examination.
A second questionnaire was distributed to a sample of patients in our hospital that evaluated adherence to wearing masks and gloves, hand hygiene and duration of hand washing, implementing social distancing to doctors and colleagues, what the patient will do if he feels that the doctor is infected with Covid-19 and how much he describes his fear to be infected, and lastly, duration of examination. Additionally, we calculated the average duration of the examination during and before the pandemic by dividing the total number of cases by the duration spent by the physician in the clinic.
The collected data were analyzed, and accordingly, recommendations were proposed to the hospital administration and the following corrective measures were applied:
- In collaboration with the media department of our university, public awareness-raising was achieved by instructions distributed through social media platforms. Patients were encouraged to contact our emergency department if they cannot determine whether their complaint necessitates seeking urgent medical care or not.
- Instruction panels of safety measures were placed in every examination room to remind and encourage residents and fellows to adhere to safety measures.
- An online meeting was scheduled with residents, fellows, nurses, and technicians to inform them about all safety measures, especially when dealing with COVID-19 positive patients in the operating room.
- Front desk employees and nurses were encouraged to spend more time with each patient to instruct them about the safety measures.
The outcomes of applying the corrective measures were assessed in the re-audit during the period of 15th June–15th August, 2020. Also, the number and types of urgent or emergent vitreoretinal surgical disorders conditions that presented to our hospital were assessed in the re-audit.
Statistics
Statistical analyses were performed using SPSS Statistics version 20 (IBM, Armonk, NY). The Chi-square test was used to compare the percentages and the t-test to compare the means. A P value <0.05 was considered to be statistically significant.
Results of the Primary Audit
During the period between 15th March–15th May, 2020, the number of patients presented to the hospital with urgent or emergent vitreoretinal surgical disorders significantly declined compared to a similar period just before the pandemic (15th December, 2019–15th February, 2020). The number of retinal detachment cases with PVR < grade B and PVR > grade B that presented during the pandemic was 71 versus 122 and 15 versus 29 before the pandemic; P < 0.001 and 0.035, respectively. The number of tractional retinal detachment cases during the pandemic was 45 versus 84 before the pandemic; P = 0.001. The number of intraocular foreign body cases was 11 during the pandemic compared to 23 before the pandemic; P = 0.04. The number of endophthalmitis cases was 7 during the pandemic, compared to 17 before the pandemic; P = 0.04. The number of retinal detachment cases following globe injuries was 12 during the pandemic compared to 27 before the pandemic; P = 0.016 (Table 1).
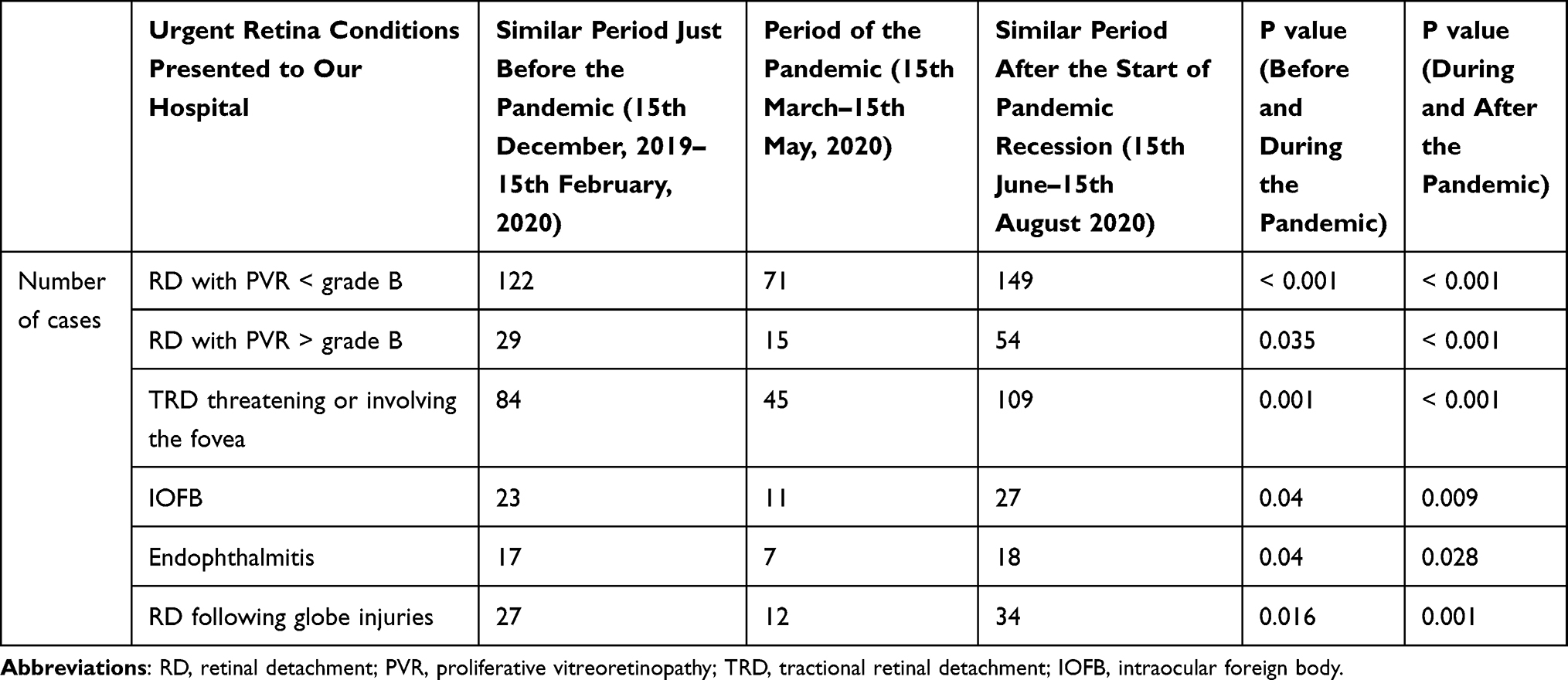 |
Table 1 Number of Urgent Retina Cases Presented During Pandemic and Similar Periods Just Before and After the Pandemic |
The Questionnaire for physicians was answered by 6 professors (15.38%), 12 residents (30.77%), 9 fellows (23.08%), and 12 attending physicians (30.77%).
The results of the Questionnaire showed good adherence to safety measures by all doctors. However, residents and fellows were less compliant with safety measures than professors and attending physicians (Table 2).
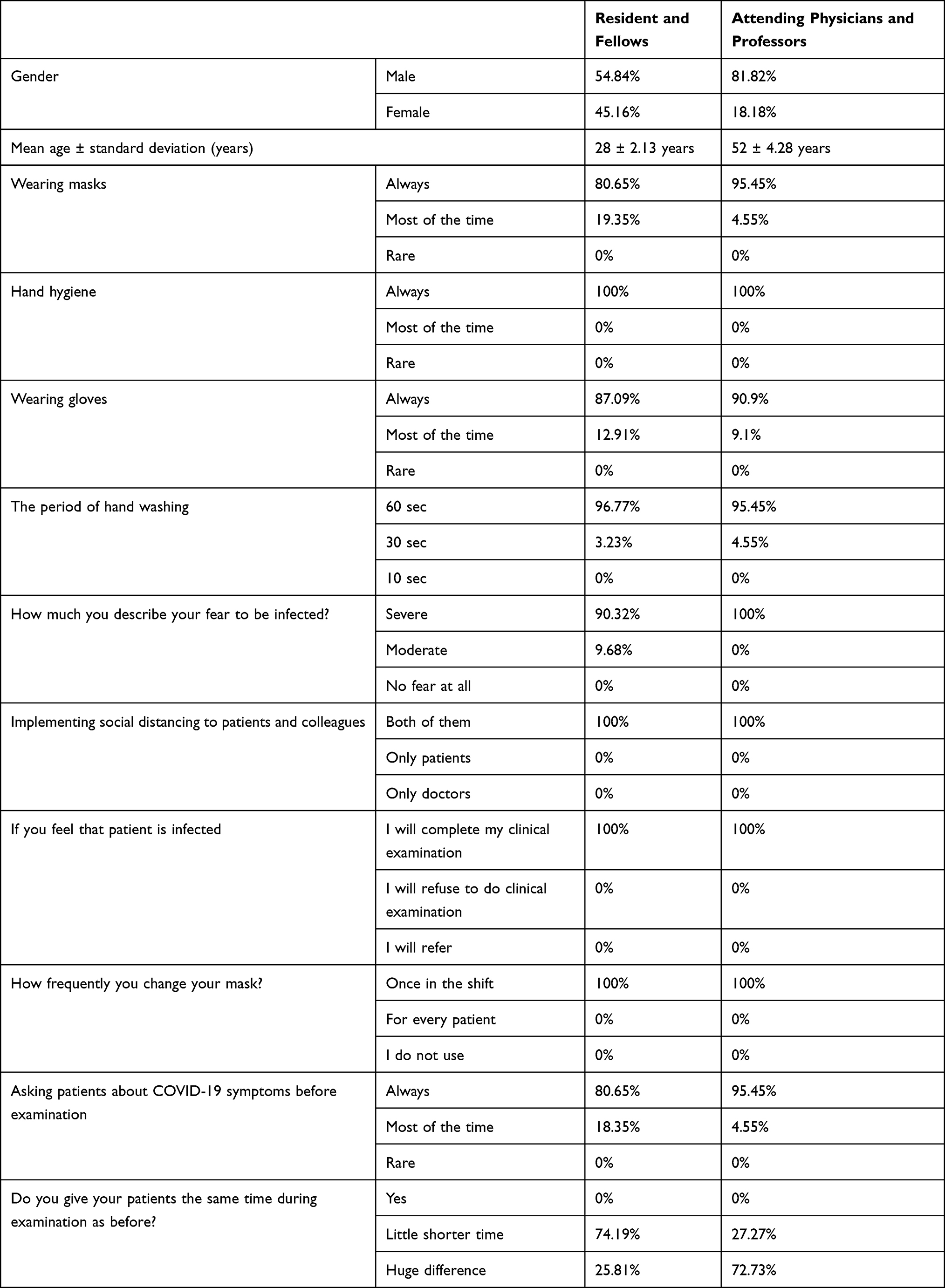 |
Table 2 Questionnaire of Effect of Covid-19 Pandemic on the Retina Practice That Was Circulated to the Physicians |
The Questionnaire for patients was answered by 200 patients. Patients were less adherent to the safety measures than doctors (Table 3).
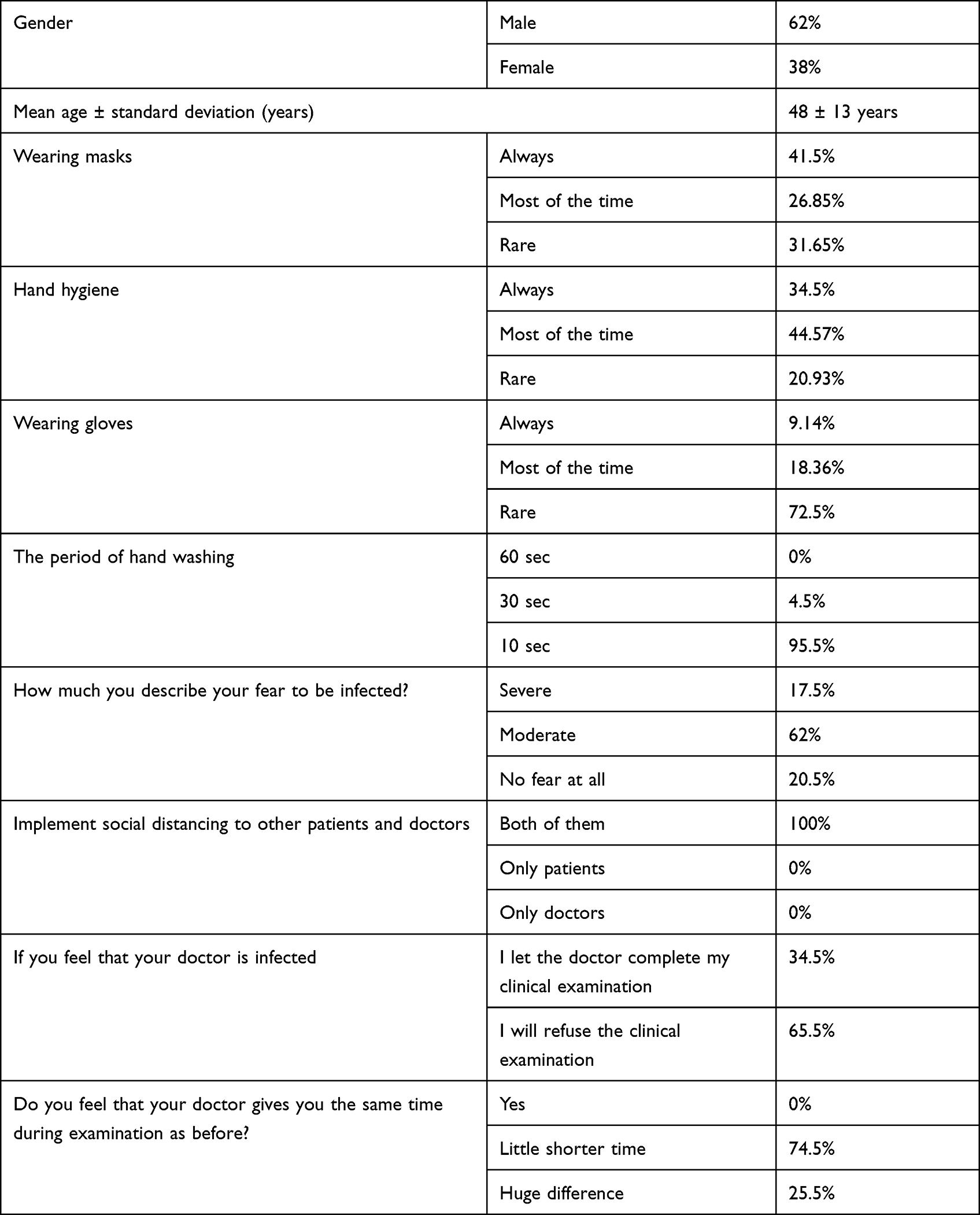 |
Table 3 Questionnaire of Effect of Covid-19 Pandemic on the Retina Practice That Was Circulated to a Sample of Patients |
One of the notable findings in our audit is the direct impact of safety measures on the patient–doctor relationship, both were anxious about getting infected, so instead of previous warm relations, the situation dropped to a tense formal meeting. Moreover, there was a significant decrease in the time of meeting with the patient, pre-pandemic appointment average time was 12 minutes, in comparison with 8 minutes during the pandemic; P = 0.02.
Re-Audit
As the pandemic started to decline, between 15th June and 15th August, 2020, there was a significant increase in the number of urgent cases compared to the pandemic period. Conditions that demonstrated significant increase included retinal detachment (RD) with proliferative vitreoretinopathy (PVR) less than grade B, RD with PVR more than grade B, tractional retinal detachment threatening or involving the fovea, intraocular foreign body, RD following globe injuries, and endophthalmitis.
A simple questionnaire was given to the sub-group of patients with PVR greater than grade B to investigate the cause of delay in seeking medical care. In 37 (68.52%) patients, the cause of delay was the fear of getting infected with COVID-19 from the hospital environment. Five (9.26%) patients were critically ill so, they recognized their decreased vision only after improvement of their general condition. Fifteen (27.78%) patients did not seek medical advice because of reluctance or negligence about the seriousness of their vision problem.
Another Questionnaire was circulated to doctors and patients including a new question “If your compliance to safety measures increased, what was the main reason?”. All residents and fellows showed better compliance with all measures. Twelve (70.59%) residents and fellows stated that shorter shifts allowed them to better adhere to safety measures. However, 5 (29.41%) residents and fellows were encouraged to apply strict safety measures as the increasing number of infections, both globally and locally, eliminated their reluctant attitude.
Patients also showed better adherence to safety measures. One hundred and forty-six (73%) patients confirmed that instructions given by front disc employees and nurses encouraged them to follow safety measures during their presence in the hospital. Twenty-nine (14.5%) patients stated that this was due to awareness by instructions on social media platforms, while in 25 (12.5%) patients, the cause was instruction panels in the waiting area.
Discussion
In this audit, there was a significant decrease in the number of urgent or emergent vitreoretinal surgical disorders presented to our tertiary center, which receives patients from 4 governorates with a population of more than 5 million, during the COVID-19 pandemic. The main reason for that decline was the reluctance of patients to seek medical help due to the fear of contracting COVID-19. In the United States, the Center for Disease Control (CDC) reported a 42% reduction in the emergency department (ED) visits during the period of March 29th–April 25th, 2020.17 Similarly, the Canadian Institute for Health Information (CIHI) reported a decline in the ED visits by 25% in March 2020 compared to March 2019.18
Our findings are in line with previous studies from North America and the UK that reported a significant reduction in retinal detachment cases presented over a 3- to 5-month duration from the start of the pandemic.19–22 In addition, Toro et al reported a significant contraction of the main ophthalmic surgeries during the first month of local lockdown in 10 European countries, and vitrectomy surgeries declined by an average 76% compared to the same period in 2019.23 There was a similar report of reduction of eye surgical procedures in Italy and Poland because of the pandemic.24–26 Poor functional and anatomical outcomes after retinal detachment surgery are common with delayed surgical intervention as a result of persistent vision loss for more than 6 days, increased incidence of macular detachment, and increased extent of retinal detachment.23,27,28
Consequently, the period after the start of pandemic recession witnessed a significant increase in the number of urgent cases and increased number of complex cases, such as RD with significant PVR, advanced tractional retinal detachment, intraocular foreign body, and RD following globe injuries.
On the other hand, Arjmand et al reported a significant increase in the number of retinal detachments presented to a Canadian retina center during the pandemic. The authors attributed this increase to the closure of other ophthalmic clinics in the city. However, the Egyptian health care system has a large sector of private practice that continued to receive urgent cases during the pandemic.29
Our findings elaborate on the importance of preparing tertiary medical centers to be able to handle work overload after periods of pandemics. As this sudden overload occurred, while the pandemic was still recessing, we ensured that surgical care was offered to the patients without delay but without jeopardizing the strict safety measures. This was achieved by increasing the working hours per day in the outpatient clinic and the operating room and working on the weekends, as necessary, to avoid over-crowdedness.
Although all doctors demonstrated good adherence to safety measures, residents were less compliant than fellows and attending physicians. We tried to improve their compliance by decreasing the workload by shortening the duration of the shifts. The majority of residents contributed their improved compliance to the reduced workload. Consequently, we recommend reducing tasks and working hours of residents to improve their adherence to safety measures as they are at higher risk of infection due to long working hours and greater contact with patients. Additionally, studies have reported a negative impact of COVID-19 pandemic on the mental health of physicians with subsequent impact on the residency training program. Therefore, virtual training and surgical simulators should be included in the training programs in addition to traditional training methods.30
The majority of patients affirmed the vital role of front disc employees and nurses in raising their awareness of necessary safety measures. This demonstrates the substantial role of paramedical personnel during the pandemic.
Ferrara et al demonstrated the impact of the pandemic on the medical and surgical training of residents and fellows. Reduction of more than 75% of surgical practice was reported by 74.6% of trainees, and half of them stopped surgeries completely. Alternative methods of training such as simulator training and web-based teaching could play an important role in optimizing the ophthalmology training during the pandemic. This is especially important for retinal fellows due to the long learning curve of vitreoretinal surgery.31
The COVID-19 pandemic raised the ethical issue of prioritizing patients to receive treatment depending on the urgency of the condition and potential adverse outcomes due to delayed treatment.23,32,33 Diseases associated with a high risk of morbidity and mortality due to treatment delay should be prioritized over those with lower risk.34,35
Our study has several limitations, which should be considered when assessing our results. First, the study was conducted at a single tertiary center and needs to be repeated at a national scale in order to be representative of the wide Egyptian health care system. Second, the study might have biases related to health-seeking behavior, economic status of patients, and local epidemiological situation of COVID-19 transmission.
In conclusion, there was a significant decline in the number of urgent retina cases during the pandemic due to patients’ fear of leaving home, which resulted in a significant increase of urgent and complex cases after the pandemic started to decline. Public awareness raised about urgent conditions requiring immediate intervention is crucial, and the medical system should be ready to manage a higher number of urgent and complicated cases after the pandemic. During the pandemic, resident physicians were less compliant with safety measures due to work overload. It is important to give extra attention to young doctors during pandemics as they are more vulnerable to infection due to greater contact with patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This study did not receive specific funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Parrish RK, Stewart MW, Duncan Powers SL. Ophthalmologists Are More Than Eye Doctors-In Memoriam Li Wenliang. Am J Ophthalmol. 2020;213:A1–A2. doi:10.1016/j.ajo.2020.02.014
2. Situation Report −51 WHOC disease 2019 (COVID19). S. No. Available from: https://www.who.int/docs/defaultsource/coronaviruse/situation-reports.
3. Bedford J, Enria D, Giesecke J, et al. COVID-19: towards controlling of a pandemic. Lancet. 2020;395(10229):1015–1018. doi:10.1016/S0140-6736(20)30673-5
4. Liu K, Chen Y, Lin R, Han K. Clinical features of COVID-19 in elderly patients: a comparison with young and middle-aged patients. J Infect. 2020;80(6):e14–e18. doi:10.1016/j.jinf.2020.03.005
5. Mourey L, Falandry C, de Decker L, et al. Taking care of older patients with cancer in the context of COVID-19 pandemic. Lancet Oncol. 2020;21(5):e236. doi:10.1016/S1470-2045(20
6. Meduri A, Oliverio GW, Mancuso G, et al. Ocular surface manifestation of COVID-19 and tear film analysis. Sci Rep. 2020;10(1):20178. doi:10.1038/s41598-020-77194-9
7. De Salvo G, Meduri A, Vaz-Pereira S, Spencer D. An uncommon cold of the retina. Surv Ophthalmol. 2021. doi:10.1016/j.survophthal.2021.08.006
8. Nasiri N, Sharifi H, Bazrafshan A, Noori A, Karamouzian M, Sharifi A. Ocular Manifestations of COVID-19: a Systematic Review and Meta-analysis. J Ophthalmic Vis Res. 2021;16(1):103–112. doi:10.18502/jovr.v16i1.8256
9. Romano MR, Montericcio A, Montalbano C, et al. Facing COVID-19 in Ophthalmology Department. Curr Eye Res. 2020;45(6):653–658. doi:10.1080/02713683.2020.1752737
10. Xia J, Tong J, Liu M, Shen Y, Guo D. Evaluation of coronavirus in tears and conjunctival secretions of patients with SARS-CoV-2 infection. J Med Virol. 2020;92(6):589–594. doi:10.1002/jmv.25725
11. Arjmand P, Murtaza F, Eshtiaghi A, Popovic MM, Kertes PJ, Eng KT. Impact of the COVID-19 pandemic on characteristics of retinal detachments: the Canadian experience. Can J Ophthalmol. 2021;56(2):88–95. doi:10.1016/j.jcjo.2020.12.008
12. Moussa M, Elshorbagy MS, Emarah A, et al. Intravitreal injections of anti-VEGF agents during COVID-19 pandemic: clinical audit from Tanta University Hospital. Int Ophthalmol. 2021;41(4):1437–1443. doi:10.1007/s10792-021-01719-y
13. Murakami T, Okamoto F, Sugiura Y, Okamoto Y, Hiraoka T, Oshika T. Changes in aniseikonia and influencing-factors following successful macula-off retinal detachment surgery. Sci Rep. 2019;9(1):11588. doi:10.1038/s41598-019-48112-5
14. Menke MN, Kowal JH, Dufour P, et al. Retinal layer measurements after successful macula-off retinal detachment repair using optical coherence tomography. Invest Ophthalmol Vis Sci. 2014;55(10):6575–6579. doi:10.1167/iovs.14-14412
15. Greven MA, Leng T, Silva RA, et al. Reductions in final visual acuity occur even within the first 3 days after a macula-off retinal detachment. Br J Ophthalmol. 2019;103(10):1503–1506. doi:10.1136/bjophthalmol-2018-313191
16. American Academy of Ophthalmology. List of urgent and emergent ophthalmic procedures; 2020. Available from: https://www.aao.org/headline/list-of-urgent-emergentophthalmic-procedures.
17. Hartnett KP, Kite-Powell A, DeVies J, et al. Impact of the COVID-19 Pandemic on Emergency Department Visits - United States, January 1, 2019-May 30, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(23):699–704. doi:10.15585/mmwr.mm6923e1
18. Canadian emergency department vi 1 sits drop 25% in early weeks of COVID-19 pandemic 2 | CIHI [Internet]. [cited 2020 October 18]. Available from: https://www.cihi.ca/en/canadian3.emergency-department-visits-drop-25-in-early-weeks-of-covid-19-pandemic.
19. Shams F, El-Abiary M, Goudie C, Yorston D. Effects of lockdown on retinal detachment incidence in Scotland. Eye. 2021;35(4):1279–1280. doi:10.1038/s41433-020-1029-3
20. Rohl A, Kalhorn A, Singh J, Mandava N. Decreased retinal detachments during a COVID-19 lockdown period in Colorado. Acta Ophthalmol. 2020. doi:10.1111/aos.14570
21. Poyser A, Deol SS, Osman L, et al. Impact of COVID-19 pandemic and lockdown on retinal detachments. Eye. 2020:1–2. doi:10.1038/s41433-020-01137-x.
22. Awad M, Poostchi A, Orr G, Kumudhan D, Zaman A, Wilde C. Delayed presentation and increased prevalence of proliferative vitreoretinopathy for primary rhegmatogenous retinal detachments presenting during the COVID-19 pandemic lockdown. Eye. 2021;35(4):1282–1283. doi:10.1038/s41433-020-1056-0
23. Toro MD, Brézin AP, Burdon M, et al. Early impact of COVID-19 outbreak on eye care: insights from EUROCOVCAT group. Eur J Ophthalmol. 2021;31(1):5–9. doi:10.1177/1120672120960339
24. dell’Omo R, Filippelli M, Virgili G, et al. Effect of COVID-19-related lockdown on ophthalmic practice in Italy: a report from 39 institutional centers. Eur J Ophthalmol. 2022;32(1):695–703. doi:10.1177/11206721211002442
25. Dmuchowska D, Cwalina I, Krasnicki P, et al. The Impact of Three Waves of the COVID-19 Pandemic on the Characteristics of Primary Rhegmatogenous Retinal Detachments at a Tertiary Referral Centre. Clin Ophthalmol. 2021;15:3481–3491. doi:10.2147/OPTH.S323998
26. Dmuchowska DA, Pieklarz B, Konopinska J, Mariak Z, Obuchowska I. Impact of Three Waves of the COVID-19 Pandemic on the Rate of Elective Cataract Surgeries at a Tertiary Referral Center: a Polish Perspective. Int J Environ Res Public Health. 2021;18:16. doi:10.3390/ijerph18168608
27. Kim JD, Pham HH, Lai MM, Josephson JW, Minarcik JR, Von Fricken M. Effect of symptom duration on outcomes following vitrectomy repair of primary macula-off retinal detachments. Retina. 2013;33(9):1931–1937. doi:10.1097/IAE.0b013e3182877a27
28. Hassan TS, Sarrafizadeh R, Ruby AJ, Garretson BR, Kuczynski B, Williams GA. The effect of duration of macular detachment on results after the scleral buckle repair of primary, macula-off retinal detachments. Ophthalmology. 2002;109(1):146–152. doi:10.1016/s0161-6420(01
29. Gericke CA, Britain K, Elmahdawy M, Elsisi G. Health System in Egypt. van Ginneken E, Busse R, editors. Health Care Systems and Policies. Health Services Research: Springer, New York, NY; 2018. doi:10.1007/978-1-4614-6419-8_7-1
30. Dub N, Konopińska J, Obuchowska I, Lisowski Ł, Dmuchowska DA, Rękas M. The Impact of the COVID-19 Pandemic on Ophthalmology Residents: a Narrative Review. Int J Environ Res Public Health. 2021;18:21. doi:10.3390/ijerph182111567
31. Ferrara M, Romano V, Steel DH, et al. Reshaping ophthalmology training after COVID-19 pandemic. Eye. 2020;34(11):2089–2097. doi:10.1038/s41433-020-1061-3
32. Ghanbari V, Ardalan A, Zareiyan A, Nejati A, Hanfling D, Bagheri A. Ethical prioritization of patients during disaster triage: a systematic review of current evidence. Int Emerg Nurs. 2019;43:126–132. doi:10.1016/j.ienj.2018.10.004
33. Toro M, Choragiewicz T, Posarelli C, Figus M, Rejdak R. Early Impact of COVID-19 Outbreak on the Availability of Cornea Donors: warnings and Recommendations. Clin Ophthalmol. 2020;14:2879–2882. doi:10.2147/OPTH.S260960
34. Elfalah M, AlRyalat SA, Toro MD, et al. Delayed Intravitreal Anti-VEGF Therapy for Patients During the COVID-19 Lockdown: an Ethical Endeavor. Clin Ophthalmol. 2021;15:661–669. doi:10.2147/OPTH.S289068
35. Hanna TP, Evans GA, Booth CM. Cancer, COVID-19 and the precautionary principle: prioritizing treatment during a global pandemic. Nat Rev Clin Oncol. 2020;17(5):268–270. doi:10.1038/s41571-020-0362-6
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.