Back to Journals » Risk Management and Healthcare Policy » Volume 15
Evaluation of the Therapeutic Pattern and Pharmaco-Utilization in Hypercholesterolemic Patients Treated with Statins: A Retrospective Study on Italian Real-World Data
Authors Perrone V, Giacomini E, Sangiorgi D ![]() , Andretta M, Bartolini F, Lupi A
, Andretta M, Bartolini F, Lupi A ![]() , Ferrante F, Palcic S, Re D, Degli Esposti L
, Ferrante F, Palcic S, Re D, Degli Esposti L ![]()
Received 19 January 2022
Accepted for publication 8 July 2022
Published 28 July 2022 Volume 2022:15 Pages 1483—1489
DOI https://doi.org/10.2147/RMHP.S358015
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kyriakos Souliotis
Valentina Perrone,1 Elisa Giacomini,1 Diego Sangiorgi,1 Margherita Andretta,2 Fausto Bartolini,3 Alessandro Lupi,4 Fulvio Ferrante,5 Stefano Palcic,6 Davide Re,7 Luca Degli Esposti1
1CliCon S.r.l. Società Benefit – Health, Economics & Outcome Research, Bologna, Italy; 2UOC Assistenza Farmaceutica Territoriale, Azienda ULSS 8 Berica, Vicenza, Italy; 3Dipartimento Farmaceutico-USL Umbria 2, Terni, Italy; 4ASL VCO, Omegna (VB), Italy; 5ASL Frosinone, Frosinone, Italy; 6Azienda Sanitaria Universitaria Integrata Giuliano-Isontina (ASUGI), Trieste, Italy; 7U.O.C. Servizio Assistenza Farmaceutica Territoriale, ASL Teramo, Teramo, Italy
Correspondence: Valentina Perrone, CliCon S.r.l. Società Benefit – Health, Economics & Outcome Research, Via Murri 9, Bologna, 40137, Italy, Tel +39 3450316494, Email [email protected]
Purpose: The study aimed to analyze, in hypercholesterolemic patients under statin medication, patient characteristics and their lipid profile at baseline, the therapeutic pathway, and the pharmaco-utilization, using real-world data in Italy.
Patients and Methods: A retrospective study was conducted using administrative databases of a sample of entities covering 6.5 million health-assisted individuals. Between January 2010 and June 2019, patients with non-familial hypercholesterolemia (nFH) were identified by 1) ≥ 1 low-density lipoprotein cholesterol (LDL-C) measurement (LDL-C assessment date was the index-date) and 2) statin prescription during 6 months before the index-date (pharmaco-utilization period). FH patients were defined by LDL-C evaluation, statin treatment during the pharmaco-utilization period, and a score ≥ 6 according to the Dutch Lipid Clinic Network criteria. nFH patients were divided into four exclusive cohorts based on CV-risk class: 1) with previous CV disease (CVD); 2) with diabetes mellitus; 3) with mixed-dyslipidemia diagnosis; 4) in primary-prevention. Based on LDL-C index values, patient was defined with LDL-C “controlled” if its levels were ≤ 70mg/dl (CVD), ≤ 100mg/dl (diabetes, FH), ≤ 130mg/dl (mixed-dyslipidemia, primary-prevention).
Results: Overall 164,161 nFH patients were included (mean age 72 years, 51% male); of these, 46,782 (28.5%) were CVD (mean age 74 years, 66% male), 34,803 (21.2%) were diabetic (mean age 72 years, 51% male), 1617 (1%) were with mixed-dyslipidemia (mean age 71 years, 48% male) and 80,959 (49.3%) were in primary-prevention (mean age 71 years, 42% male). The proportion of nFH patients with controlled LDL-C was 41.2% for CVD, 73.6% for diabetic, 80.7% for mixed-dyslipidemia, and 79.5% for primary-prevention patients; 49% of nFH patients were adherent to therapy. Overall, 1287 FH patients (mean age 64 years, 42% male) were included; in 39.2% of the patients, LDL-C was controlled, and 44% of the patients were adherent to therapy.
Conclusion: The results of this study highlighted non-optimal therapeutic management of hypercholesterolemic patients in Italian clinical practice, with a notable quote of patients non-adherent to therapy.
Keywords: lipid-lowering agents, pharmacoutilization, real-world evidence, clinical practice
Introduction
The control of lipid levels is one of the most effective strategies for cardiovascular disease (CVD) prevention.1–3 The results of a meta-analysis showed that reductions in low-density lipoprotein cholesterol (LDL-C) by statins safely restrain the incidence of major vascular events.4 As recommended by the European Society of Cardiology (ESC)/European Atherosclerosis Society (EAS) guidelines, plasma LDL-C levels should be lowered as much as possible to prevent CVD, especially in high- and very high-risk patients.2,5,6 A large inter-individual variability in the reduction of LDL-C levels by statins has been found,7,8 also among patients treated with high-dose.8 Several evidences suggested that adherence to statins more than 80% is associated with a significant reduction of CV events, both in primary and secondary prevention.9,10 Other cholesterol-lowering agents have been used in conjunction with statins to achieve the therapeutic goal.11 Due to continued inability to obtain adequate clinical benefit, the availability of novel lipid lowering agents that yield effective and sustained LDL-C reduction would represent an appealing option. In this setting, the evaluation of therapeutic management of hypercholesterolemic patients in real clinical practice would represent a valuable tool to study the appropriateness of therapeutic approaches. The present analysis aimed to evaluate the characteristics of hypercholesterolemic patients being treated with lipid-lowering agents, their treatment patterns, and pharmaco-utilization in terms of adherence to therapy in a real-world Italian setting.
Materials and Methods
Data-Source
The analysis was carried out using data extracted from administrative databases from six Italian Healthcare Entities (geographically distributed across Italy), covering approximately 6.5 million inhabitants. Within the administrative flows, the anonymous univocal numeric code assigned to each patient allowed the electronic linkage of all records for each subject across the databases. Specifically, data-linkage was performed among demographic database (data on patients’ demographic characteristics), pharmaceutical database [data on prescription of drugs reimbursed by the Italian National Health System (INHS), in terms of related Anatomical-Therapeutic Chemical (ATC) code, and prescription date], hospitalization database [information on discharge diagnoses at any level classified according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and date of diagnoses], diagnostic tests and specialist visits database (date of prescription, type, description activity of diagnostic tests and procedure), and laboratory test data of lipid profile (available for 2.4 million of health-assisted individuals). The anonymous univocal numeric code ensured total compliance with the European General Data Protection Regulation (2016/679). No identifiers related to patients were provided to the authors. All the results of the analyses were produced as aggregated summaries, and the data could not be assigned, either directly or indirectly, to a single institution, department, doctor, individual, or individual prescribing behaviors. Based on the Data-Privacy Guarantor Authority (General Authorisation for personal data treatment for scientific research purposes–n.9/2014), informed consent was not required, as its collection would be impossible for organizational reasons. According to the Italian law on conducting observational analysis, the ethics committee of each participating entity was notified and approved the analysis (Supplementary Table 1).
Study Design and Study Population
This is an observational retrospective analysis which included patients affected by familial (FH) and non-familial hypercholesterolemia (nFH) identified by at least one measurement of plasma LDL-C and with at least one prescription of lipid-lowering agents [statins (ATC codes: C10AA, C10BA)] during 6 months before the last available LDL-C assessment (pharmaco-utilization period). The inclusion period was from Jan 2010-June 2019. Patients with FH were identified by a measurement of LDL-C, a statin treatment during the pharmaco-utilization period, and a score ≥6 according to the criteria of the Dutch Lipid Clinic Network (DLCN) [Supplementary Table 2].
Patients treated with proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors (ATC codes: C10AX13, C10AX14) during the pharmaco-utilization period and those who were not present in the databases for the whole study period (ie, relocations) were excluded. The date of last available LDL-C test was defined as index-date. nFH patients were sub grouped in four exclusive cohorts based on CV-risk classes: 1) patients with at least one previous hospitalization for CVD (CVD cohort); 2) patients with diabetes mellitus (with at least two prescriptions of antidiabetic drugs or hospitalization with diagnosis of diabetes mellitus and no previous hospitalization for CV disease, diabetic cohort); 3) patients with at least one hospitalization or with an exemption code for mixed dyslipidemia (mixed-dyslipidemia cohort); iv) patients in primary prevention (primary-prevention cohort), ie, not included in the other cohorts. A detailed description of criteria used for cohorts definition is reported in Supplementary Table 3.
Analysis of Baseline Patients Characteristics
Baseline patients’ characteristics, in terms of age and gender, were evaluated. The comorbidity profile was also assessed by using the Charlson Comorbidity Index (CCI).12 Additionally, patients were stratified accordingly to LDL-C values at index-date (ie, ≤70mg/dl, 71–100mg/dl, 101–130mg/dl, and >130mg/dl).
Treatment Patterns and Pharmaco-Utilization Analyses
In all patients, at the index date the use of statins (atorvastatin, simvastatin, rosuvastatin, lovastatin, pravastatin, fluvastatin) alone or in combination with ezetimibe (atorvastatin/ezetimibe, rosuvastatin/ezetimibe, simvastatin/ezetimibe), or ezetimibe alone, was assessed (Supplementary Table 4).
Adherence to lipid-lowering agents was calculated during the pharmaco-utilization period as the percentage of days (proportion of days covered, PDC) in which a subject had tablets available, from the first prescription until the end of the pharmaco-utilization period. Patients with PDC ≥80% were defined adherent.
Based on LDL-C index values, the patient was defined with “controlled” LDL-C at index date if levels were in accordance with those reported by ESC/EAS guidelines available at the time of the analysis2,5 and by AIFA Note 1313(ie, LDL-C ≤70mg/dl for CVD group, ≤100mg/dl for diabetic and FH cohorts, ≤130mg/dl for mixed-dyslipidemia and primary-prevention cohorts). During all the available periods before the index-date, non-statin-tolerant patients were identified as those presenting ezetimibe monotherapy as the last drug prescription and with prior treatment with three different statins. Additionally, a sensitivity analysis on statins intolerance was carried out; non-tolerant patients were defined as those 1) treated with high-potency (HP) statin (Supplementary Table 4) followed by a low-potency statin and subsequent treatment discontinuation or 2) treated with HP statin combined with ezetimibe, followed by ezetimibe alone.
Statistical Analysis
Continuous variables were reported as mean±standard deviation (SD); categorical variables were expressed as numbers and percentages. For comparative analysis, p value <0.05 was considered statistically significant. All analyses have been performed using STATA SE version 12.0 (StataCorp LLC, College Station, TX, USA).
Results
nFH Patients
Among the sample population, 164,161 patients met the inclusion criteria for nFH (Supplementary Figure 1); they were 72±10.9 years old, 50.8% male, and the plasma levels of LDL-C averaged 94.6±34.5 mg/dl (Table 1). Overall, 46,782 (28.5%) patients fell into the CVD cohort (mean age 74.3±10.6 years, 65.9% male), 34,803 (21.2%) in diabetic cohort (mean age 71.6±10.4 years, 50.6% male), 1617 (1%) into mixed-dyslipidemia cohort (mean age 71.4±11.2 years, 48.4% male), and 80,959 (49.3%) in primary-prevention cohort (mean age 70.8±11.1 years, 42.3% male). As reported in Supplementary Table 5, the stratification of nFH patients by age-ranges has shown that 86.3% of nFH patients were >60 years old, and an average of 40% of CVD patients over 65 years was also affected by diabetes (Supplementary Table 6).
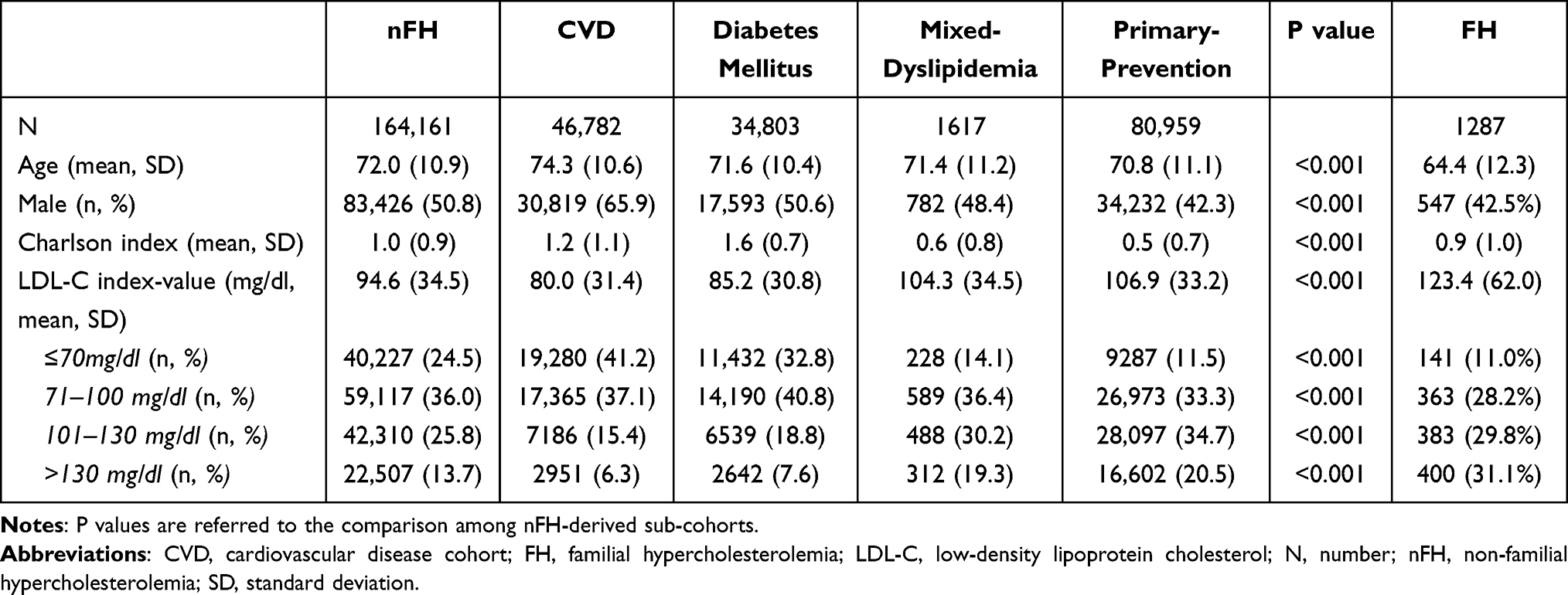 |
Table 1 Baseline Characteristics of FH, nFH Patients and nFH-Derived Cohorts |
The plasma levels of LDL-C averaged 80.0±31.4mg/dl and 85.2±30.8mg/dl in CVD and diabetic patients respectively, and 104.3±34.5mg/dl and 106.9±33.2mg/dl in mixed-dyslipidemia and primary-prevention patients, respectively, (p<0.001) (Table 1). Based on the levels of LDL-C recommended,3,4 in 41.2% of CVD, 73.6%, 80.7%, and 79.5% of diabetic, mixed-dyslipidemia, and primary-prevention patients, respectively, LDL-C levels were controlled at index date (Table 1).
As shown in Figure 1A, at index-date, 47.2% of nFH patients were treated with atorvastatin, 24.9% with simvastatin, followed by 12.2% under rosuvastatin, 6.8% with lovastatin/pravastatin/fluvastatin, and 9% were using the ezetimibe in combination with statins or as monotherapy (Figure 1A). The specular distribution was found stratifying patients among CVD, diabetic, mixed-dyslipidemia and primary-prevention cohorts (Supplementary Figure 2). The percentage of patients adherent to statins during 6-months follow-back period reached 48.7% among overall nFH patients, and specifically 52.7%, 51.2%, 45.3% and 45.3% among CVD, diabetic, mixed-dyslipidemia and primary-prevention patients, respectively (p<0.001) (Figure 1C). Considering the total nFH population, 244 patients (0.1%) (sensitivity analysis: 4395, 2.7%) were found to be intolerant to statins. Specifically, 132 CVD patients (0.3%) (sensitivity analysis: 2486, 5.3%), 38 diabetic patients (0.1%) (sensitivity analysis: 612, 1.8%), and 71 primary-prevention patients (0.1%) (sensitivity analysis: 1259, 1.6%) were deemed intolerant to statins.
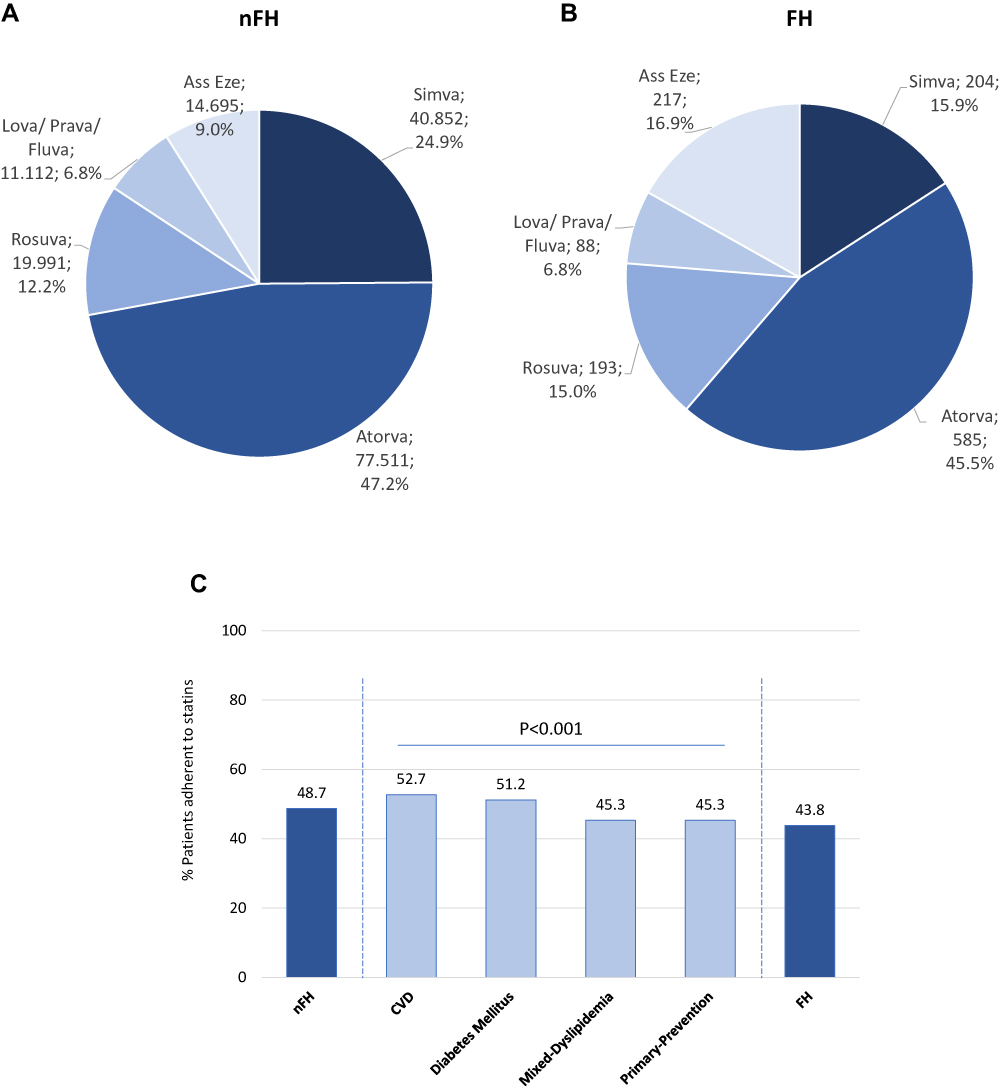 |
Figure 1 Treatment patterns among nFH patients and FH patients, and their adherence to statins. At the index-date, the identification of therapeutic options prescribed among nFH (A) and FH (B) patients was assessed. The percentage of patients adherent to statin medication was evaluated during the pharmaco-utilization period (C). Abbreviations: Atorva, atorvastatin; Simva, simvastatin; Rosuva, rosuvastatin; Lova, lovastatin; Prava, pravastatin; Fluva, fluvastatin; Ass Eze, statin associated with ezetimibe or ezetimibe alone; nFH, non-familial hypercholesterolemia; CVD, cardiovascular disease cohort; FH, familial hypercholesterolemia. |
FH Patients
Overall, 1287 patients with FH were included; they were 64.4±12.3 years old, 42.5% were male, and the plasma levels of LDL-C at the index-date averaged 123.4±62.0 mg/dl (Table 1). The stratification of patients by age-ranges has shown that 24% ranged 50–59 years, 27.6% were across 60–69 years and 28.4% were in the 70–79 years range (Supplementary Table 7). In 39.2% of the patients, LDL-C levels resulted to be controlled at index date, set at values ≤100 mg/dl (Table 1). At baseline, 45.5% of FH patients were treated with atorvastatin, 16.9% were using statins in combination with ezetimibe or ezetimibe monotherapy, 15.9% with simvastatin, 15% under rosuvastatin, followed by 6.8% with lovastatin/pravastatin/fluvastatin (Figure 1B). The 43.8% of the patients resulted in being adherent to statins during the pharmaco-utilization period (Figure 1C). A number of 6 and 69 patients (0.5% or 5.4%) were intolerant to statins, based on classical and sensitivity analysis, respectively.
Discussion
This administrative claims-based observational analysis provided insights into statins pharmaco-utilization among patients affected by nFH and FH, in a real-world Italian setting. Additionally, the availability of laboratory test data of the patients’ lipid profiles allowed to estimate the percentage of patients with controlled LDL-C levels at index date.2,5,13 In both nFH and FH cohorts, atorvastatin was the most prescribed statin, followed by simvastatin and rosuvastatin. As previously reported in a population-based study in southern Italy,14 simvastatin, atorvastatin, rosuvastatin, and pravastatin were the most frequently prescribed as first-line treatment, with atorvastatin more commonly used for secondary prevention. The restraint of LDL-C levels represents one of the most effective strategies for CVD prevention and CV-related mortality.1,15,16 However, data from clinical trials and surveys indicate that a large proportion of statin-treated patients fail to achieve lipid goals, and this phenomenon most frequently occurred among high CV-risk patients.8,17 In the present analysis, in over half of high-risk patients, such as CVD and FH, the LDL-C levels were not controlled at index date. These results confirmed previous reports that current management of dyslipidemia continues to be suboptimal in clinical practice, with a substantial proportion of patients failing to achieve guideline-recommended LDL-C levels.5,6,18–20 Several factors, such as demographic and clinical features of patients, could contribute to lipid target attainment17; thus, the therapeutic management of dyslipidemia should optimized based on patients’ characteristics and their risk factors.21
Non-adherence to treatment was suggested as probably one of the most important factors in the therapeutic failure of hyperlipidemic patients.8 In this study, 56% of FH and 51% of nFH patients were not adherent to statin therapy, with the lower adherence observed among diabetic patients. These results were comparable with those from a previous study performed in Italy showing that the initial statin prescription was not followed by another prescription in 47.5% of the newly-treated patients22 and also a meta-analysis data reported that as many as 60% of the patients may stop their statin therapy within 6 months of treatment initiation.23 In addition, OsMed report-2020 showed a comparable adherence in patients treated with statins in combination with ezetimibe (63.4%).24 Moreover, the low-adherence phenomenon has been previously reported in diabetic patients and can be possibly explained by the complex comorbidity and therapeutic profile of these patients.25
Our cohort of patients reflected real clinical practice, and the results must be interpreted taking into account limitations related to the observational nature of the analysis, which was based on data collected from administrative databases. In particular, since the pharmaco-utilization data derived from medical prescriptions and dispensing, the reasons of non-adherence among the study population were not recapturable in the dataset. In addition, limited clinical data were available for the analysis; thus, it was not possible to include clinical parameters (such as smoking habit and blood pressure control) in the definition of CV-risk classes, as reported by the ESC/EAS guidelines.3–5 Moreover, it should considered the risk of hospital-bias potentially affecting laboratory data . Lastly, the results are representative of the sample population and may not be extended to the overall population.
Conclusion
In conclusion, the present analysis, by integrating administrative datasets with lipid profile data, pictured non-optimal therapeutic management of hypercholesterolemic patients in the real-world scenario of Italian clinical practice, with high-percentage of high-CV risk patients showing uncontrolled LDL-C levels, and not-adherent to lipid-lowering treatment. The monitoring of the lipid profile of hypercholesterolemic patients and the identification of patients with LDL-C levels not adequately controlled could be included in the strategic health planning of INHS to ameliorate prescriptive appropriateness and therapeutic adherence, thus improving clinical outcomes in hypercholesterolemic patients.
Disclosure
Novartis Farma S.p.A. purchased the study report that is the basis for this manuscript. This manuscript was developed by CliCon S.r.l. Società Benefit and sponsored by Novartis Farma S.p.A. All authors report no conflicts of interest in this work. The agreement signed by Clicon S.r.l. Società Benefit and Novartis Farma S.p.A. does not create any entity hip, joint venture or any similar relationship between parties. Clicon S.r.l.Società Benefit is an independent company. Neither CliCon S.r.l. Società Benefit nor any of their representatives are employees of Novartis Farma S.p.A. for any purpose.
References
1. Verschuren WM, Jacobs DR, Bloemberg BP, et al. Serum total cholesterol and long-term coronary heart disease mortality in different cultures. Twenty-five-year follow-up of the seven countries study. JAMA. 1995;274:131–136. doi:10.1001/jama.1995.03530020049031
2. Catapano AL, Graham I, De Backer G, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias. Rev Esp Cardiol. 2017;70:115. doi:10.1016/j.rec.2017.01.002
3. Piepoli MF, Hoes AW, Agewall S, et al.; ESC Scientific Document Group. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016;37:2315–2381. doi:10.1093/eurheartj/ehw106
4. Baigent C, Blackwell L, Emberson J, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376:1670–1681.
5. Reiner Z, Catapano AL, De Backer G, et al. ESC/EAS Guidelines for the management of dyslipidaemias: the Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). Eur Heart J. 2011;32:1769–1818. doi:10.1093/eurheartj/ehr158
6. Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41:111–188. doi:10.1093/eurheartj/ehz455
7. Boekholdt SM, Hovingh GK, Mora S, et al. Very low levels of atherogenic lipoproteins and the risk for cardiovascular events: a meta-analysis of statin trials. J Am Coll Cardiol. 2014;64:485–494. doi:10.1016/j.jacc.2014.02.615
8. Agabiti Rosei E, Salvetti M. Management of Hypercholesterolemia, Appropriateness of Therapeutic Approaches and New Drugs in Patients with High Cardiovascular Risk. High Blood Press Cardiovasc Prev. 2016;23:217–230. doi:10.1007/s40292-016-0155-2
9. Simpson RJ, Mendys P. The effects of adherence and persistence on clinical outcomes in patients treated with statins: a systematic review. J Clin Lipidol. 2010;4:462–471. doi:10.1016/j.jacl.2010.08.026
10. Perreault S, Dragomir A, Blais L, et al. Impact of better adherence to statin agents in the primary prevention of coronary artery disease. Eur J Clin Pharmacol. 2009;65:1013–1024. doi:10.1007/s00228-009-0673-0
11. Pitts RN, Eckel RH. The Emerging Role of PCSK9 Inhibitors in Preventive Cardiology. Eur Cardiol. 2014;9(2):65–70. doi:10.15420/ecr.2014.9.2.65
12. Charlson ME. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–383. doi:10.1016/0021-9681(87)90171-8
13. Gazzetta Ufficiale Serie Generale n.113 del 04 maggio 2020. Modifica della Nota AIFA 13 di cui alla determina AIFA n. 2014. Available from: https://www.gazzettaufficiale.it/eli/gu/2020/05/04/113/sg/pdf.
14. Ferrajolo C, Arcoraci V, Sullo MG, et al. Pattern of statin use in southern Italian primary care: can prescription databases be used for monitoring long-term adherence to the treatment? PLoS One. 2014;9:e102146. doi:10.1371/journal.pone.0102146
15. Baigent C, Blackwell L, et al.; Cholesterol Treatment Trialists’ (CTT) Collaboration. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376:1670–1681.
16. Catapano AL, Tokgözoğlu L. Pharmaceutical strategies for reducing LDL-C and risk of cardiovascular disease. Atheroscler Suppl. 2019;39:100002.
17. Morieri ML, Perrone V, Veronesi C, et al. Improving statin treatment strategies to reduce LDL-cholesterol: factors associated with targets’ attainment in subjects with and without type 2 diabetes. Cardiovasc Diabetol. 2021;20:14. doi:10.1186/s12933-021-01338-y
18. Boekholdt SM, Hovingh GK, Mora S, et al. Very low levels of atherogenic lipoproteins and the risk for cardiovascular events: a meta-analysis of statin trials. J Am Coll Cardiol. 2014;64:485–494.
19. Presta V, Figliuzzi I, Miceli F, et al.; EFFECTUS Steering Committee. Achievement of low density lipoprotein (LDL) cholesterol targets in primary and secondary prevention: analysis of a large real practice database in Italy. Atherosclerosis. 2019;285:40–48. doi:10.1016/j.atherosclerosis.2019.03.017
20. Bruckert E, Parhofer KG, Gonzalez-Juanatey JR, et al. Proportion of high-risk/very high-risk patients in Europe with low-density lipoprotein cholesterol at target according to European guidelines: a systematic review. Adv Ther. 2020;37:1724–1736. doi:10.1007/s12325-020-01285-2
21. Crismaru I, Pantea Stoian A, Bratu OG, et al. Low-density lipoprotein cholesterol lowering treatment: the current approach. Lipids Health Dis. 2020;19(1):85. doi:10.1186/s12944-020-01275-x
22. Corrao G, Conti V, Merlino L, Catapano AL, Mancia G. Results of a retrospective database analysis of adherence to statin therapy and risk of nonfatal ischemic heart disease in daily clinical practice in Italy. Clin Ther. 2010;32:300–310. doi:10.1016/j.clinthera.2010.02.004
23. Liberopoulos EN, Florentin M, Mikhailidis DP, Elisaf MS. Compliance with lipid-lowering therapy and its impact on cardiovascular morbidity and mortality. Expert Opin Drug Saf. 2008;7:717–725. doi:10.1517/14740330802396984
24. OsMed 2020 National Report on medicines use in Italy. Available from: https://www.aifa.gov.it/en/-/rapporto-nazionale-osmed-2020-sull-uso-dei-farmaci-in-italia.
25. Dobrică EC, Găman MA, Cozma MA, et al. Polypharmacy in type 2 diabetes mellitus: insights from an Internal Medicine Department. Medicina. 2019;55:436. doi:10.3390/medicina55080436
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.