Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 15
Evaluation of the Small Airways in Patients with Chronic Obstructive Pulmonary Disease and Alpha-1 Antitrypsin Deficiency
Authors Ferrari da Cruz T ![]() , Rufino R
, Rufino R ![]() , Lopes AJ
, Lopes AJ ![]() , Noronha A
, Noronha A ![]() , Medeiros Anselmo F
, Medeiros Anselmo F ![]() , Henrique da Costa C
, Henrique da Costa C ![]()
Received 24 May 2020
Accepted for publication 27 July 2020
Published 24 September 2020 Volume 2020:15 Pages 2267—2274
DOI https://doi.org/10.2147/COPD.S262418
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Thaís Ferrari da Cruz, Rogerio Rufino, Agnaldo José Lopes, Arnaldo Noronha, Fernando Medeiros Anselmo, Cláudia Henrique da Costa
Pneumology Department, Pedro Ernesto Hospital of State University of Rio de Janeiro, Rio de Janeiro, PR, Brazil
Correspondence: Thaís Ferrari da Cruz Av João Gualberto, 253 Ap 241, Cep: 80030-000, Curitiba, PR, Brazil Tel +55 41 99911-4487
Email [email protected]
Introduction: Small airways are not evaluated with traditional pulmonary function tests. The aim of this study was to evaluate the small airways in patients with chronic obstructive pulmonary disease (COPD) with a nitrogen washout test and to verify whether there is a difference between patients with COPD due to smoking and those with COPD due to alpha-1 antitrypsin mutation.
Methods: Sixteen patients with mutation in the SERPINA1 gene and 45 patients with no mutation were included in this cross-sectional study. All pulmonary function tests, including the single breath nitrogen washout test, were performed for all patients and alpha-1 antitrypsin dosage was assessed with immunonephelometry.
Results: A comparison of patients with COPD due to smoking and those with COPD due to smoking and mutation revealed a significant difference in closure volume (%), which was the poorest in the mutation group. In the group with COPD and mutation, there was an inverse correlation between smoking and closure volume (%). We also verified that similar to forced expiratory volume in the first second (FEV1), the phase III slope (%) and ΔN2 750– 1250 mL (%) could be used to differentiate the severity of airflow limitation.
Conclusion: Our results suggest that both variables, phase III slope and the ΔN2 750– 1250 mL (%), could be related to COPD severity. Therefore, alterations at the distribution of the location of the emphysema could alter the results of closer volume and that the nitrogen washout test is more sensitive when compared to traditional pulmonary function test in evaluating COPD patients.
Keywords: serine proteinase inhibitors mutation, chronic obstructive pulmonary disease, alpha-1 antitrypsin deficiency, respiratory function tests, nitrogen washout test
Introduction
Small airways, defined as those with an internal diameter of less than 2 mm, are not evaluated by traditional pulmonary function tests. Therefore, interest has recently increased for tests such as nitrogen washout, which can evaluate small airways.1 Moreover, with the modernization of pulmonary function tests, greater availability of equipment, commercialization, and increasing interest in the evaluation of small airways, this examination has emerged as an important tool to evaluate patients with pulmonary diseases, particularly as it is a noninvasive and rapid test.2–4
Chronic obstructive pulmonary disease (COPD) is a heterogeneous disease caused by both genetic alterations and exposure to noxious gases.1,4 It is associated with high morbidity and mortality, leading to a significant worsening of the quality of life of affected individuals. Therefore, COPD is a major public health concern worldwide. COPD can become a more serious problem when it presents with early onset, particularly in patients with alpha-1 antitrypsin deficiency.5 Regardless of the triggering risk factor, COPD starts in the small airways before the manifestation of symptoms. Hence, this region is called the silent zone of the lung.4,6 Local inflammation begins with epithelial destruction, accumulation of mucus, and remodeling of the airways.4
The small airways do not contain cartilage in their walls, which accounts for most of the obstruction related to COPD.6,7 This region of low resistance contributes only 10% of the resistance of the airways. Therefore, when local obstruction occurs, the resistance slightly increases and has little repercussion on the respiratory mechanisms. However, there is a large change in ventilation distribution, and traditional pulmonary function tests such as spirometry, full body plethysmography, or diffusion cannot evaluate this repercussion.4 The single-breath maneuver in the nitrogen washout test has been the most used technique as it is quicker and easier to complete than the multiple breath maneuver.3 As described by Deus et al,2 an increase in the phase III slope and the ratio of closure volume (CV) to vital capacity (VC) (CV/VC) indicate heterogeneity of ventilation distribution and small airway disease, respectively. Recent studies have shown that the phase III slope provides a highly sensitive evaluation of pathology in the small airways by identifying changes that other pulmonary function tests cannot.4 In addition, alterations of the phase III slope and CV/VC ratio can demonstrate heterogeneity in the distribution of small airway ventilation. A previous study showed an increase in the phase III slope with clinical symptoms such as worsening dyspnea and decreased exercise tolerance.1 The present study aimed to evaluate the small airways in patients with COPD during the stable phase of the disease with a nitrogen washout test and to verify whether there is a difference between patients with COPD due to smoking and those with COPD caused by alpha-1 antitrypsin deficiency.
Materials and Methods
Study Design
This cross-sectional study evaluated the small airways of patients with stable COPD. The data were collected in the city of Rio de Janeiro from October 2016 to October 2017. Patients were initially contacted by telephone, followed by a face-to-face assessment in which the researchers evaluated them according to the selection criteria and performed the study’s procedures.
Participants
Inclusion criteria were as follows: (i) age >18 years; (ii) visiting the pulmonology outpatient clinic of Pedro Ernesto Hospital (State University of Rio de Janeiro); (iii) diagnosed with COPD according to the criteria of the Global Initiative for Chronic Obstructive Lung Disease (GOLD); and (iv) presenting with compatible clinical characteristics and spirometry with FEV1/FVC ratio (forced expiratory volume in the first second/forced vital capacity) post-bronchodilator <0.7.8 Moreover, patients should have a smoking history of >10 cigarette pack years or mutation of the SERPINA1 (serine protease inhibitor 1).
Exclusion criteria were as follows: (i) diagnosis of lung diseases from other causes (eg, pulmonary fibrosis, tuberculosis sequel); (ii) exacerbation of lung disease in the previous three months; (iii) infectious diseases of any nature in the previous three weeks; (iv) history of asthma, rhinitis, or respiratory allergy; (v) patients who have previously undergone thoracic surgery; (vi) pregnant women; and (vii) patients who have previously undergone transplantation or presenting with a history of inability to undergo respiratory function tests.
Study Procedure
The following data were collected: age, sex, body mass index, occupational history, smoking history, and home oxygen use. All pulmonary function tests were performed even if the patient had undergone a recent spirometry to ensure that the tests were performed by the same person and using the same device. Spirometry and volume and diffusion capacity measurements were performed using the HD CPL equipment (nSpire Health Inc., Longmont, CO, USA) and followed the standardization and interpretation of the American Thoracic Society, 2005.9 The equations to adjust the differences in data such as weight, height and age between the participants reported by Knudson et al10 and Neder et al11 were adopted.
The nitrogen washout test was performed using the HD PFR 3000 apparatus (nSpire Health, Inc.). The single-breath maneuver washout was performed according to the recommendations of the American Thoracic Society/European Respiratory Society.12 In the single-breath nitrogen washout technique, the patient begins to exhale all air up to their residual volume and then slowly inhales 100% oxygen to their full lung capacity. The patient continues to perform a full expiration, and at that moment, the device records a vertical curve quantifying the exhaled nitrogen.6 In healthy individuals who undergo a washout test, the phase III represents the expiration of the alveolar air in the small airways; after which phase IV or closing volume begins. The closure is progressive and ascending, and it is represented by the nitrogen expiration curve that progressively rises to reach the closure of the pulmonary apices where nitrogen is more concentrated.6 We evaluated ΔN2 750–1250 mL (%) (Change in the percentage of exhaled nitrogen between the 750 and 1250 mL portion of single-breath nitrogen washout), phase III slope, and the CV/VC (Closing Volume/Vital Capacity) ratio.
Alpha-1 antitrypsin dosage was also assessed with immunonephelometry on a filter paper. Blood obtained from the distal region of one of the fingers of the hand was dropped onto a filter paper. In patients with low alpha-1 antitrypsin levels, ie, less than 2.64 mg/dL, the presence of a mutation was confirmed with the molecular study of the SERPINA1 gene or by genetic sequencing, as required. These processes were conducted at the Laboratory Medicina Afip. This procedure has been performed routinely in the COPD clinic for all patients and was performed specifically for the study when the patients did not have a diagnosis reported in their medical record.
Classification of the severity of airflow limitation in COPD was based on the criteria presented in the GOLD (2018). The value of FEV1 post-bronchodilator during spirometry was used to classify severity as follows: mild, FEV1≥80%; moderate, FEV1<80% and≥50%; severe, FEV1<50% and≥30%; and very severe, FEV1<30%.8
Statistical Analysis
For quantitative variables, we present the mean, median, minimum value, maximum value, first and third quartiles, and standard deviation. Qualitative variables are presented as frequencies and percentages. For comparison of the groups in relation to quantitative variables, we conducted Student’s t-tests for independent variables and nonparametric Mann–Whitney samples. The nonparametric Kruskal–Wallis test was used to compare COPD classifications in relation to the nitrogen washout variables and, when necessary, the covariance analysis model was adjusted with pack years as a covariate. Values of p<0.05 were considered statistically significant. Data were analyzed with IBM SPSS Statistics v.20.0 software (IBM Corp., Armonk, NY).
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki. The project was approved by the research ethics committee of the Pedro Ernesto University Hospital, CAAE: 55174,616.3.0000.5259 and all patients provided informed consent before any study procedures were carried out.
Results
A total of 582 patients were followed up at the COPD clinic through random telephone contact. Of the 299 patients successfully contacted, 147 appeared to be eligible to participate in the study and were invited to attend the institution. Of these 147 patients, 75 attended on the date scheduled for the assessment. Inclusion and exclusion criteria were applied to these 75 patients, and 14 patients were found to be unfit for participation in the study. Of the 299 patients contacted, 46 had some mutations of SERPINA1 (serine protease inhibitor 1) and 16 were included in the study. Table 1 presents the genotypes included in the study. Of the 16 patients with some type of mutation, 5 had severe mutations. Among the 61 included patients, we found that 45 had no SERPINA1 mutation and 16 had a mutation, with 5 patients having severe mutations. The below flowchart shows patient recruitment (Figure 1).
 |
Table 1 Variations of Mutations of the SERPINA1 Gene of Patients Included in the Study |
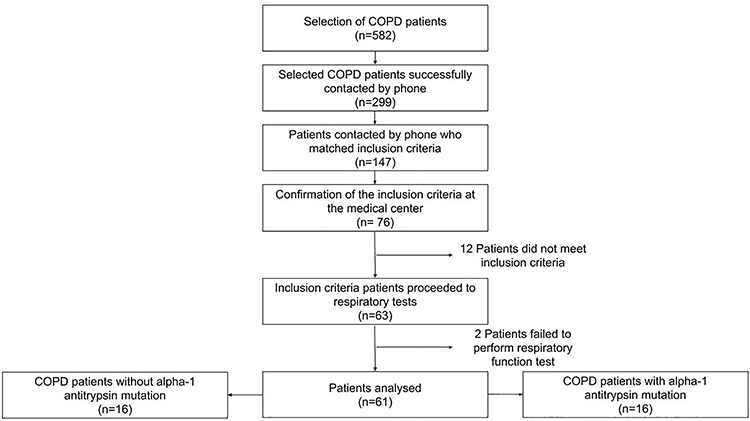 |
Figure 1 Recruitment flowchart. |
Among the 61 participants, 33 were women, and the mean age was 65.5 (SD 7.61) years. The participants were categorized into two groups: with and without mutation of the SERPINA1 gene. We did not observe a significant difference in FEV1/FVC, FEV1% (forced expiratory volume in the first second percentage of predicted), FVC% (forced vital capacity percentage of predicted), TLC% (total lung capacity percentage of predicted), RV% (residual volume percentage of predicted), RV/TLC%, DLCO% (diffusion capacity of the lungs for carbon monoxide percentage of predicted), and KCO% (Krogh’s constant, the value calculated from DLCO/VA: diffusion capacity of the lungs for carbon monoxide/alveolar volume) between both the groups. Moreover, static lung volumes and DLCO were similar in both groups. However, there was a statistically significant difference in the smoking load between the two groups, with a mean value of 28.06 + 25.10 and 75.57 + 56.11 m/a in the gene mutation and no mutation groups, respectively (Table 2).
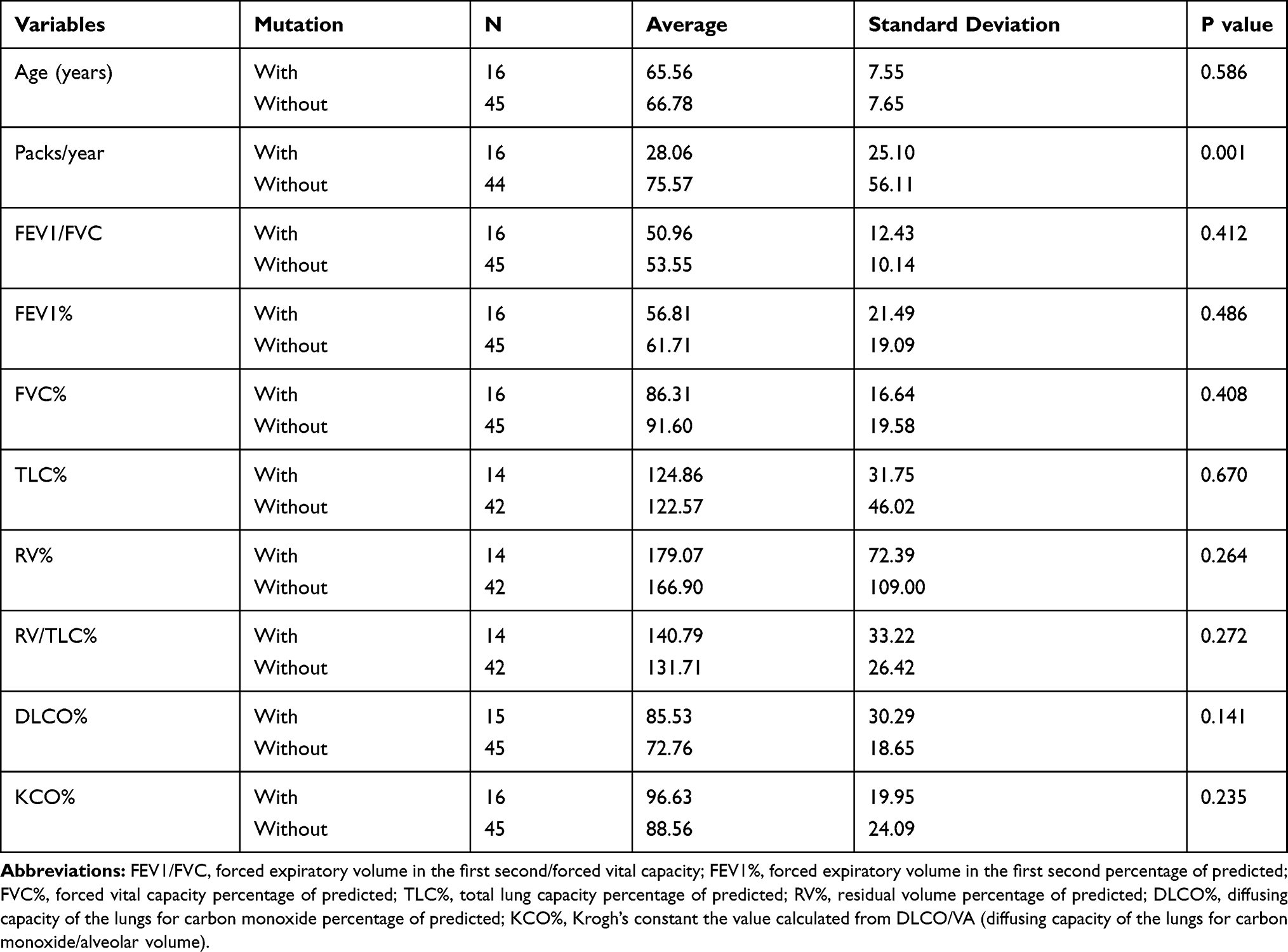 |
Table 2 Evaluation of Clinical and Functional Differences Between Groups of Patients with COPD with and without Mutation of the Alpha-1 Antitrypsin Gene |
We did not observe any statistically significant differences in ΔN2 750–1250 mL (%) or phase III slope (%) between the groups with (n = 16) and without (n = 45) mutation of the SERPINA1 gene, even after controlling for the effects of smoking. The same analyses were performed for comparing patients with COPD (n = 45) and patients with COPD and severe mutations (n = 5). There were no significant differences between the groups in phase III slope (%) or ΔN2 750–1250 mL (%).
However, there was a significant difference in CV (%) between the groups with (n = 16) and without (n = 45) mutation of the SERPINA1 gene (p = 0.019). A significant difference in CV (%) was also noted between patients with severe mutations (n = 5) and those without (n = 45) mutation of the SERPINA1 gene (p = 0.037). The analysis of airflow obstruction (FEV1) showed no difference in the severity of COPD between these groups.
We also assessed whether the main variables of the nitrogen washout test could be used to classify the severity of COPD, as done with spirometry, by categorizing airflow limitation as mild, moderate, severe, and very severe. Because the number of patients in the very severe group was small, we considered the severe and very severe patients in the same group. We verified that like FEV1, both the phase III slope (%) and ΔN2 750–1250 mL (%) could be used to differentiate the severity of airflow limitation. The phase III slope differentiated the group of patients classified as mild COPD from those with moderate COPD and also differentiated the groups of patients with mild COPD from those with severe/very severe COPD (Figure 2). The variable ΔN2 750–1250 mL (%) differentiated the mild COPD group from the severe/very severe COPD group (Figure 3). With regard to the relationship between the smoking load and the CV (%), we observed an inverse relationship in patients with COPD and a mutation of the alpha-1 antitrypsin gene (p = 0.020) (Figure 4). We estimated that for each unit increase in the number of packs/year, there was a decrease of 0.08 units in CV (%) (Table 3).
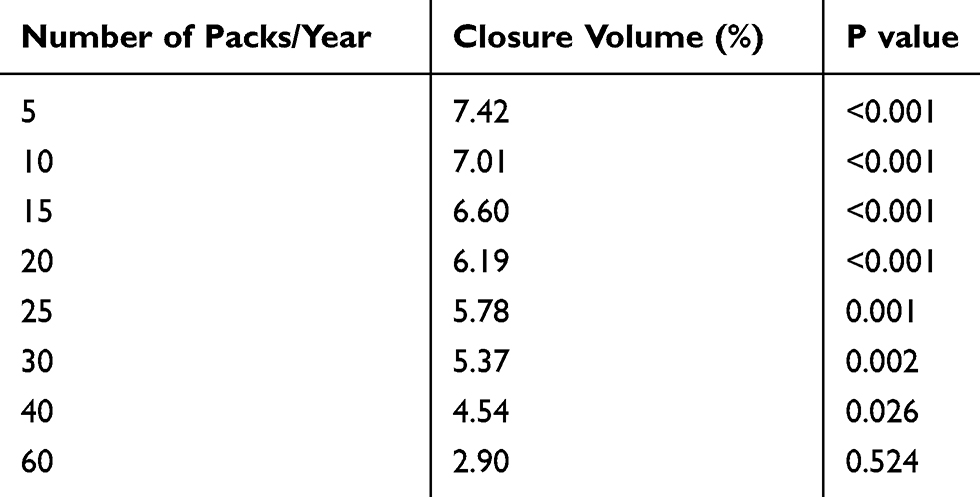 |
Table 3 Relationship Between Closure Volume (%) and Smoking Load in Patients with Alpha-1 Antitrypsin Mutation |
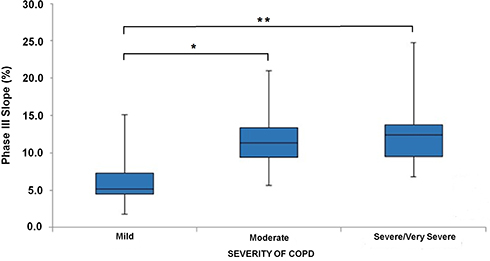 |
Figure 2 Ability of the phase III slope to predict differences in severity between those with mild, moderate, and severe/very severe COPD. *p<0.01 **p<0.001. |
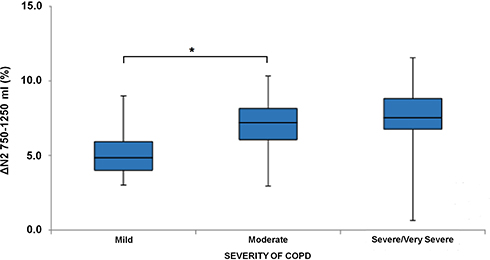 |
Figure 3 Ability of ΔN2 750–1250 mL (%) to predict differences in severity between those with mild and moderate COPD. *p<0.01. |
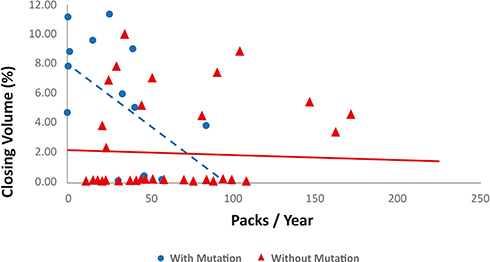 |
Figure 4 Inverse correlations between number of packs/year and closure volume (%) in patients with a mutation of the alpha-1 antitrypsin deficiency gene. Coefficient of determination (R2) = 24.9%. |
Discussion
The present study is the first study to evaluate the small airways and the distribution of ventilation with the nitrogen washout test in patients with COPD with and without mutation in the alpha-1 antitrypsin gene. Although small airways are of major clinical importance, most previous studies have focused predominantly on the early detection of small airway disease due to inhalation of cigarette smoke.13 However, emphysema from any cause increases air space and decreases communication between alveolar spaces and small airways. This impairs microvascular perfusion and leads to poor ventilation distribution. However, this important repercussion in the distribution of ventilation cannot be evaluated with traditional pulmonary function tests.2,4
Studies have reported that the nitrogen washout test can differentiate groups of patients according to the severity of COPD previously evaluated with FEV1.4,6 Although our results confirmed the possibility in differentiating COPD severity using washout test, CV (%) was not a good tool to provide this information as previously reported. In the present study, the phase III slope was related to the severity of COPD and could differentiate between patients with mild and moderate COPD, and between those with mild and severe/very severe COPD. Moreover, ΔN2 750–1250 mL (%) values could also be used to differentiate between patients with differing COPD severity, ie, patients with mild COPD from those with severe/very severe COPD. However, our results suggest that CV (%) is not useful in differentiating patients with COPD according to severity.
Another finding of this study was the inversely proportional correlation between number of packs/year and CV in patients with a mutation in the alpha-1 antitrypsin gene (n = 16). This is contradictory to what was expected because as reported in the literature, CV (phase IV) is increased in patients with COPD due to smoking.6 In practice, CV measures the difference in volume from the closure of the small airways to the residual volume.13 To explain the tracing of the CV obtained under normal conditions, a simple model is proposed, on the basis of the assumption that the intrinsic properties of the lungs are uniform, that there is a single closing pressure of the airways, and that all regions of the lung experience the same change in pleural pressure. Although these criteria are not met, even in lungs considered normal, they enable understanding of the mechanisms involved in the generation of closure volume traces.13
Isolated segments of the lungs expand evenly but, within the chest, this behavior is different, mainly because the pleural pressure in the intact chest has a vertical gradient with more negative values in the upper portions. Accordingly, the transpulmonary pressure is higher in the upper zones, and the upper units expand more than the lower ones.13 A previous study evaluated the effects of gravity on lung perfusion heterogeneity in humans during the Spacelab Life Science mission.14 A significant decrease in phase VI elevation was demonstrated when assessments were performed in the absence of gravity, thus confirming that airway closure occurs first in gravity-dependent lung regions (bases), and that the phase IV slope curve is strongly related to the topography of ventilation heterogeneity.14 In other words, if the difference between apex and base tends to equalize, the elevation of the phase IV curve tends to flatten.
Nitrogen washout depends on differences in nitrogen concentration in each lung region and is determined by differences in mechanical properties in different regions of the airways. In a healthy individual, phases III and IV can be accurately defined. Under these conditions, phase III slope remains constant and the abrupt increase in the curve of nitrogen concentration represents the beginning of phase IV. In patients with lung disease, the phase III slope progressively increases with disease severity, thus reflecting uneven dilution of alveolar gas, and the variation between phases III and IV may become less evident as the disease progresses. In patients with more severe disease, such a significant increase in the phase III slope may make it difficult to identify the beginning of phase IV.15
The data of the present study showed an inversely proportional relationship between smoking and CV values in patients with the SERPINA1 gene mutation. We hypothesized that patients with alpha-1 antitrypsin deficiency with a progressively higher smoking load would have progressively more severe COPD. Moreover, if these patients have a very large elevation in the phase III slope that makes it difficult to identify the starting point of phase IV, it would lead to a phase IV that is proportionally and disguisedly flattened, and with smaller values. This study tested this proportional increase in the phase III slope in relation to the reduction in CV, but the findings did not support our hypothesis. This study also did not demonstrate a proportional reduction in FEV1. Lapperre observed that alterations in the topographic distribution of ventilation would alter the results of the nitrogen washout test.16
This study also demonstrated a significant difference in CV (%) between patients without mutation and those with mutation, and between patients without mutation and those with severe mutation of the alpha-1 antitrypsin gene. Initially, it was thought that this difference could be justified by a difference in severity between the groups, but FEV1 values of all the groups were similar. Moreover, we did not observe a difference in the phase III slope and ΔN2 750–1250 mL (%) between the groups. Thus, our results suggest that CV (%) was a more sensitive indicator of differences between patients with COPD associated with alpha-1 antitrypsin deficiency and those with COPD exclusively due to smoking. We could also consider that the alpha-1 antitrypsin group has a more severe small airways disease.
Our study has some limitations, which should be borne in mind when considering the results. It should be noted that the groups had different numbers of participants; the group with COPD exclusively due to smoking included 45 individuals and the group with COPD with a mutation of the alpha-1 antitrypsin gene (a rare mutation) included only 16 individuals. Clinical and functional characteristics were similar between the groups, except for smoking, which was significantly lower in patients with the mutation. Of the 16 patients with a mutation in the alpha-1 antitrypsin gene, 11 had a history of previous smoking despite having a lower smoking burden. This fact corroborates the recent recommendations of WHO and ATS/ERS, which suggest a dose of alpha-1 antitrypsin at least once in all patients diagnosed with COPD to facilitate the recognition and orientation of these individuals.17
A further limitation is that when patients were classified into subgroups according to the severity of the disease, the resulting subgroups had small numbers of individuals. We encountered difficulties similar to those reported by authors such as Mikano et al3 who emphasized that although evaluation with the single-breath maneuver of the nitrogen washout test is easy to perform in schoolchildren and adults, patients with severe COPD may face difficulties in performing the test. In our experience, patients with very severe COPD, who have greater difficulties in performing the required maneuvers in respiratory function tests, also have more difficulty in reaching the study center, which makes it difficult to include this group of patients in research.
Conclusion
Although the importance of the small airways in the genesis and development of pulmonary diseases in general is clear, many questions remain regarding their precise role and the best way to assess this lung region. The nitrogen washout test could be easily performed in most patients with COPD. Moreover, both the phase III slope and the ΔN2 750–1250 mL (%) were related to COPD severity. The washout test with the variable CV (%) enabled the observation of a higher involvement of the small airways in patients with COPD and mutation of the SERPINA 1 gene. Further studies are needed to determine the role of nitrogen washout variables, particularly CV, in the study of small airways of patients with COPD caused by smoking and by mutation of the SERPINA1 gene. Our results suggest that the nitrogen washout test is more sensitive than traditional pulmonary function test in evaluating COPD patients, mainly in small airways disease.
Abbreviations
COPD, chronic obstructive pulmonary disease; CV, closure volume; DLCO, diffusion capacity of the lungs for carbon monoxide; FEV1, forced expiratory volume in the first second; FVC, forced vital capacity; KCO, Krogh’s constant; RV, residual volume; TLC, total lung capacity; VA, alveolar volume; VC, vital capacity.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Lopes AJ, Marinho CL, Alves UD, et al. Relationship between ventilation heterogeneity and exercise intolerance in adults with sickle cell anemia. Braz J Med Biol Res. 2017;50(8). doi:10.1590/1414-431x20176512
2. Deus CAL, Vigário PS, Guimarães FS, Lopes AJ. Nitrogen single-breath washout test for evaluating exercise tolerance and quality of life in patients with chronic obstructive pulmonary disease. Braz J Med Biol Res. 2018;51(4):. doi:10.1590/1414-431x20177059
3. Mikamo M, Shirai T, Mori K, et al. Predictors of phase III slope of nitrogen single-breath washout in COPD. Respir Physiol Neurobiol. 2013;189(1):42–46. doi:10.1016/j.resp.2013.06.018
4. Boeck L, Gensmer A, Nyilas S, et al. Single-breath washout tests to assess small airway disease in COPD. Chest. 2016;150(5):1091–1100. doi:10.1016/j.chest.2016.05.019
5. Camelier AA, Winter DH, Jardim JR, Barboza CEG, Cukier A, Miravitlles M. Deficiência de alfa-1 antitripsina: diagnóstico e tratamento. J Bras Pneumol. 2008;34(7):514–527. doi:10.1590/S1806-37132008000700012
6. Konstantinos Katsoulis K, Kostikas K, Kontakiotis T. Techniques for assessing small airways function: possible applications in asthma and COPD. Respir Med. 2016;119:e2–e9. doi:10.1016/j.rmed.2013.05.003
7. McDonough JE, Yuan R, Suzuki M, et al. Small- airway obstruction and emphysema in chronic obstructive pulmonary disease. N Engl J Med. 2011;365(17):1567–1575. doi:10.1056/NEJMoa1106955
8. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of COPD: Full Repo 2018. 2017. Available from: http://www.goldcopd.com.
9. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
10. Knudson RJ, Lebowitz MD, Holberg CJ, Burrows B. Changes in the normal maximal expiratory flow-volume curve with growth and aging. Am Rev Respir Dis. 1983;127(6):725–734. doi:10.1164/arrd.1983.127.6.725
11. Neder JA, Andreoni S, Castelo-Filho A, Nery LE. Reference values for lung function tests. I. Static volumes. Braz J Med Biol Res. 1999;32(6):703–717.
12. Robinson PD, Latzin P, Verbanck S, et al. Consensus statement for inert gas washout measurement using multiple- and single- breath tests. Eur Respir J. 2013;41(3):507–522. doi:10.1183/09031936.00069712
13. Milic-Emili J, Torchio R, D’Angelo E. Closing volume: a reappraisal (1967–2007). Eur J Appl Physiol. 2007;99(6):567–583. doi:10.1007/s00421-006-0389-0
14. Prisk GK, Elliott AR, Guy HJ, Kosonen JM, West JB. Pulmonary gas exchange and its determinants during sustained microgravity on Spacelabs SLS-1 and SLS-2. J Appl Physiol. 1995;79(4):1290–1298. doi:10.1152/jappl.1995.79.4.1290
15. Barbini P. A functional mathematical model to simulate the single-breath nitrogen washout. Open Biomed Eng J. 2013;7(1):81–92. doi:10.2174/1874120720130701003
16. Lapperre TS, Willems LNA, Timens W, et al. Small airways dysfunction and neutrophilic inflammation in bronchial biopsies and BAL in COPD. Chest. 2007;131(1):53–59. doi:10.1378/chest.06-0796
17. American Thoracic Society, European Respiratory Society. American Thoracic Society/European Respiratory Society statement: standards for the diagnosis and management of individuals with alpha-1 antitrypsin deficiency. Am J Respir Crit Care Med. 2003;168(7):818–900.18. doi:10.1164/rccm.168.7.818.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.