Back to Journals » Medical Devices: Evidence and Research » Volume 17
Evaluation of the Functionality in an Emergency Department Setting of an Intravenous Protection Device to Prevent Self-Injection
Authors Bragg K, Albus M, Bragg B, Beste RM ![]() , Simon LV
, Simon LV ![]()
Received 23 November 2023
Accepted for publication 12 March 2024
Published 19 March 2024 Volume 2024:17 Pages 135—142
DOI https://doi.org/10.2147/MDER.S451439
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kara Bragg, Michael Albus, Bradley Bragg, Rachelle M Beste, Leslie V Simon
Emergency Department, Mayo Clinic, Jacksonville, FL, USA
Correspondence: Kara Bragg, Email [email protected]
Background: The United States has an opioid abuse crisis that has been increasing exponentially since 2013. In 2021, there were 220 deaths each day from opioid overdoses in the United States alone. Patients suffering from addiction often present to the emergency department (ED) anticipating that an intravenous (IV) catheter will be placed. This catheter is then accessible for patients to self-inject illicit drugs while under medical care or elope from the facility with the IV in place to self-inject. The misuse of medical IV access is a potential source of prolonged hospitalizations and fatal overdoses nationwide. On two separate occasions, patients were found dead in our ED bathroom after overdosing by accessing their IV site for self-injection. These events prompted the development of the IV SafeLock prototype. The IV SafeLock is designed to prevent intravenous access by the patient while allowing access by specified providers to administer medications. This study aims to investigate prototype usability and functionality by nursing staff in the ED.
Methods: A prospective study was performed with twenty ED nurses in a clinical trial to use the IV SafeLock in the clinical setting. Each nurse was given two months to complete an evaluation of 20 patients requiring IV access. They used the IV SafeLock on infusion ports and Intermittent Needle Therapy (INT) access sites. A Likert scale was used to measure the ease of function and use of the IV SafeLock.
Results and conclusion: The nurses felt that the IV SafeLock was easy to use and achieved its function of protecting the intravenous access site from self-injection. The IV SafeLock prototypes used in the trial were easy to use and functioned as intended most of the time. The IV SafeLock can be used by nursing staff in a clinical setting to help prevent self-injection.
Clinical Trial Registration: NCT05695183 enrolled 01/12/2023.
Keywords: overdose, accidental death, self-injection, opioid crisis, IV safelock, patient safety, intravenous line infection
Introduction
Background
On two separate occasions in 2019, patients were found dead in our suburban ED bathroom from fatal, self-inflicted overdoses. Both patients injected street drugs through the IV access which was placed as part of their emergency medical care. Both incidents were reported internally through risk management. Although national statistics are not reported for incidences like these, they are common throughout healthcare facilities and inflict harsh emotional trauma on patient’s families as well as hospital staff.1,2
Opioid deaths are the leading cause of death from injury in the United States.3 In 2017, the CDC reported 70,237 overdose deaths, of which 67.8% involved opioids.4 Unfortunately, the opioid epidemic continues to rise year after year with a rise in synthetic opioids, most particularly fentanyl.5 The number of drug-related overdose deaths increased more than 16% between 2020 and 2021.5 In 2025, the annual number of opioid overdose deaths was projected to reach nearly 82,000.6 Estimated hospital costs of heroin and prescription overdose are greater than $700 million annually.7 These costs do not include legal costs from a seminal event where a patient self-injected while receiving hospital care.7
The death of a patient is a stark reminder of this common but often marginalized patient safety problem. In addition to overdoses, patients who self-inject may experience intravenous line infections and prolonged hospital stays. These adverse events are costly to the institution and, more importantly, to the wellbeing of our patients and staff. The stress of current world events is only intensifying the mental health and addiction crisis facing this country.8 We need a tool to protect our patients and the staff who care for them from the devastating consequences of addiction.
There is no available means of securing access to IVs placed in the hospital setting. Currently, if there is a significant concern that a patient may abuse their IV, a one-on-one sitter may be required. This costly and cumbersome intervention can only be justified in extreme cases and is not a viable solution. Alternately, many institutions limit the number of IVs placed.9 This restricts the quality of care available to the patient. Patients may require prolonged hospitalizations to receive IV medications if they are deemed to be unsafe to discharge with a PICC (peripherally inserted central catheter) due to a history of substance abuse.
We must protect our patients from the devastating effects of this disease. Addiction is a crisis in our country and our hospitals. The IV Safe Lock is a small, inexpensive, and easy-to-use device that secures access points to intravenous systems preventing patient access, misuse, and potential dire consequences (patent pending 17/480,726).
Hypothesis
IV SafeLock will function as designed.
Aim
To establish the usability and functionality of the IV SafeLock in the clinical setting among ED nurses.
Objective
The IV SafeLock was designed to prevent intentional IV access by patients while allowing provider access to administer medications as indicated. This study measured IV SafeLock functionality and usability by surveying nursing staff after device utilization in the ED setting.
Materials and Methods
Materials
The device is a clamshell that locks closed and is set prior to placement by an institution-specific key. Each unit is delivered in a universal configuration with the ability to be set to any key configuration. The lock is set to the institution’s key at the point of use. Once set, the device is locked over IV access ports and can only be removed with the institution-specific key (Figure 1). It is easy for nurses to place and remove but cannot be accessed without the corresponding key. The device works on unused port sites (Figure 2) as well as all tubing connection points (Figure 3) and offers protection during infusion (Figure 4). The locking mechanism allows for a single mass-produced unit which is set to an institution-specific key at the time of placement. In this way, the same locking unit may be distributed to many facilities. A key taken from one area hospital will not work on a device placed in a different healthcare facility. The availability of institution-specific keys offers a layer of patient safety should the lock need to be removed in an emergent situation. Anyone within a facility entrusted with a key can unlock any IV Safe Lock within that institution. The key can be signed out to a specific nurse when needed and returned in a secure fashion. The IV Safe Lock is designed to be mass-produced from injection molding. It is entirely plastic and MRI-compatible.
 |
Figure 1 Key as it would be inserted into the device. |
 |
Figure 2 Device as it would fit around an INT hub. |
 |
Figure 3 Device secured around infusion tubing. |
 |
Figure 4 Device secured at a y-port. |
The IV Safe Lock can be utilized with a variety of intravenous catheters (peripheral IVs, central lines, or PICC lines), anywhere IV access is required, and there is a potential for patient misuse. This prototype offers needed protection from overdose, unexplained infections, altered mental status, and subsequent need for prolonged inpatient care. Initially created for use in the ED, it offers clear benefits throughout the healthcare environment. The IV Safe Lock will be an invaluable addition to inpatient wards and outpatient surgical areas. Outside the hospital, this device can protect patients in skilled nursing facilities, rehabilitation facilities, and patients receiving home infusions.
Methods
A prospective study was developed using a clinical trial. Twenty ED nurses were recruited through department Email and department postings. Signed consent was obtained from the participating nurses. The selected ED nurses received training on the use of the IV SafeLock device through in-person tutorials and instructional handouts. Additionally, all ED nursing team leaders underwent training and have access to a key for redundancy. All ED nurses (including those not enrolled in the study) received a brief overview of the device in the event they encountered the device while providing patient care.
Study nurses were directed to select patient encounters that met study criteria for use of the device. Patient encounters were eligible for inclusion if the patient presented through triage and required IV access. The patient must be aged 18 or over, medically stable, require IV access as part of their visit, and be able to give verbal consent. The verbal consent process was approved by the Mayo Clinic IRB. The study was compliant with the Declaration of Helsinki. Excluded encounters included patients under 18 years old, pregnant, incarcerated, confused, or any member of a protected class as specified by the Mayo Clinic IRB. Patients were excluded if there were signs of acute stroke, acute myocardial infarction, severe sepsis, or shock. Study nurses were also given the discretion to exclude patient encounters if their workload would not permit the use of the device.
Patients under the care of a study nurse who met inclusion criteria were eligible to have the IV SafeLock placed. Each of the 20 enrolled study nurses was given the opportunity to use the device on 20 patient encounters. As such, up to 400 patients could be included in the study. The participating nurse selected eligible patients who presented through triage. Patients were given a description of the study and verbally consented if they wished to participate. Patients had the opportunity to decline participation for any reason and could elect to have the prototype device removed at any time. Selected patients had an additional IV extension added to the primary intermittent needle access site allowing emergency access for intravenous medication administration should the nurse encounter difficulty unlocking the device. The nurses used the device on any intravenous access ports distal to the initial pigtail connection. As such, there would be no interruption of drug administration should the device fail during this study.
The study nurse was assigned a key to unlock and lock the device. The nurse was required to set each device prior to securing it on the IV access port. He or she would lock the device on the IV access ports with the assigned key, unlock and remove the device when medications were to be delivered, and immediately replace and lock the device once the medications had been administered or the intravenous infusion was initiated using the assigned key. If the device failed at any time, the nurse could remove the pigtail attachment and re-establish access to the primary IV access site.
The device was removed at the conclusion of care by the participating nurse or if the patient left the department. At the conclusion of the nurse’s interaction with the patient, the nurse completed an anonymous paper survey of the functionality of the IV SafeLock device. No patient identifiers were present on the survey completed. The surveys were collected weekly by the study directors. The information was translated into electronic format spread sheets for data analysis. Survey responses represent the outcome data for out study. This data is presented below as overall percent response as well as mean response per nurse using standard Likert scale interpretation methods10,11.
Results
Original data was collected and recorded after study completion on 10/7/23. Data was extracted from a Likert scale with 13 questions. The first two questions discussed consent and ensuring the patient met inclusion criteria. This information is depicted in percent as well as visual form (Table 1 and Figure 5). The next five questions addressed how the nurse felt about using the IV SafeLock and the final six questions discussed the function of the lock while in use. This information is depicted in percent as well as visual form (Table 2 and Figure 6).
 |
Table 1 Device Usability Results |
 |
Table 2 Device Functionality Results |
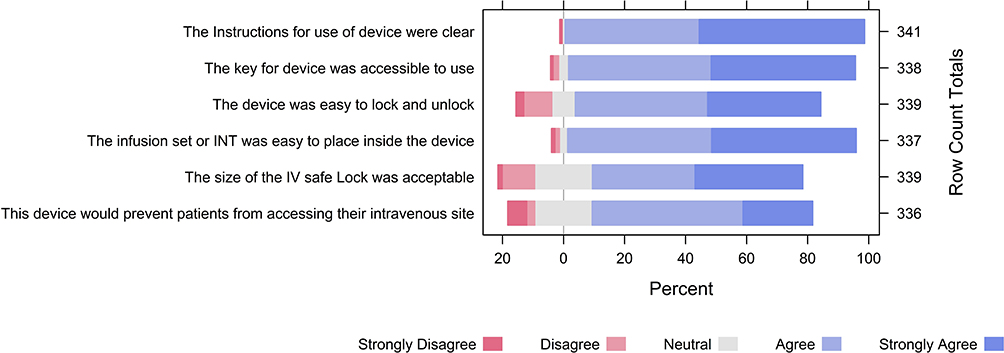 |
Figure 5 Device usability visualization. |
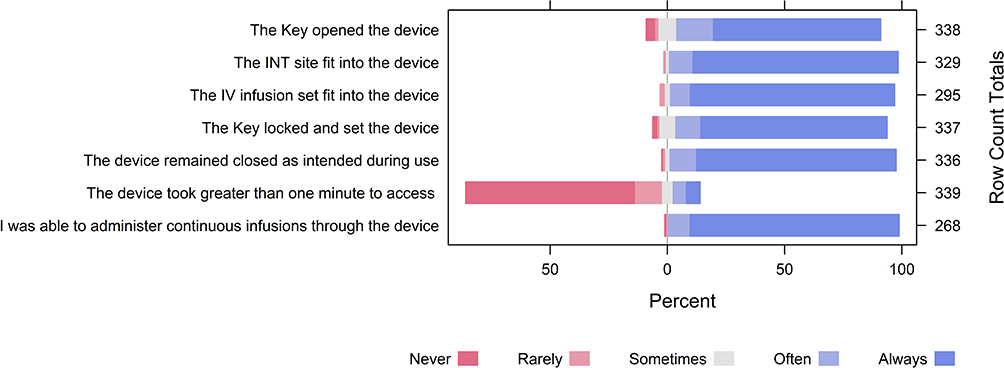 |
Figure 6 Device functionality visualization. |
Of the original twenty study nurses, two left the department prior to the initiation of the study leaving 40 incomplete/unreturned surveys. There were 10 additional surveys from active participants that were not returned. This resulted in 350 of the original 400 surveys returned for analysis. Nine of these surveys had a blank Likert scale and written comments. Our survey included a “N/A” choice. For the sake of statistical analysis, “N/A” will be counted as blank as it is an intentional placeholder if a question is felt not to be relevant to the operational use of the device. Three questions on individual surveys had multiple answers selected. Those three individual instances were reverted to blank for analysis.
Figures 5 and 6 represent the survey data taken in its entirety. The survey data can also be compared across the individual study nurse participants. Of the eighteen nurses who participated in the study, 11 nurses returned all 20 surveys, 4 nurses returned 19 surveys, 1 nurse returned 17 surveys, 1 nurse returned 16 surveys, and 1 nurse returned 112 surveys. To evaluate nurse study participants and correct for variation in surveys returned, the responses for each nurse were assessed to gauge their overall survey response. This data is represented in Figures 7 and 8.
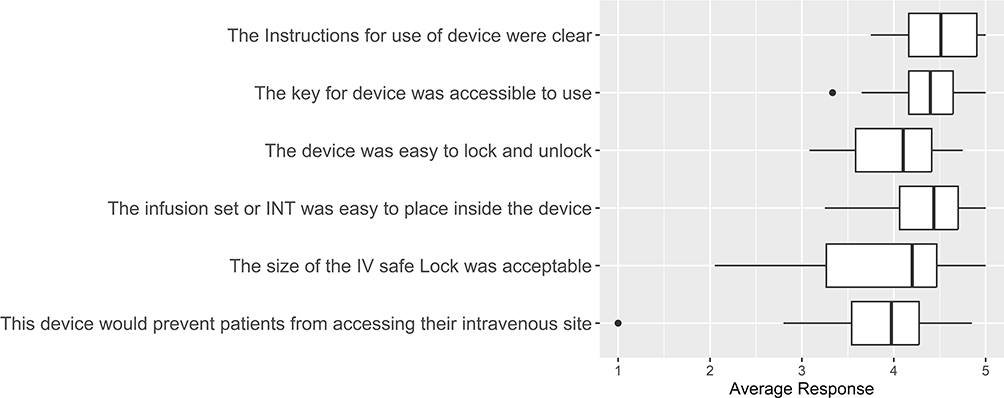 |
Figure 7 Boxplot of individually averaged nurse responses to device usability. |
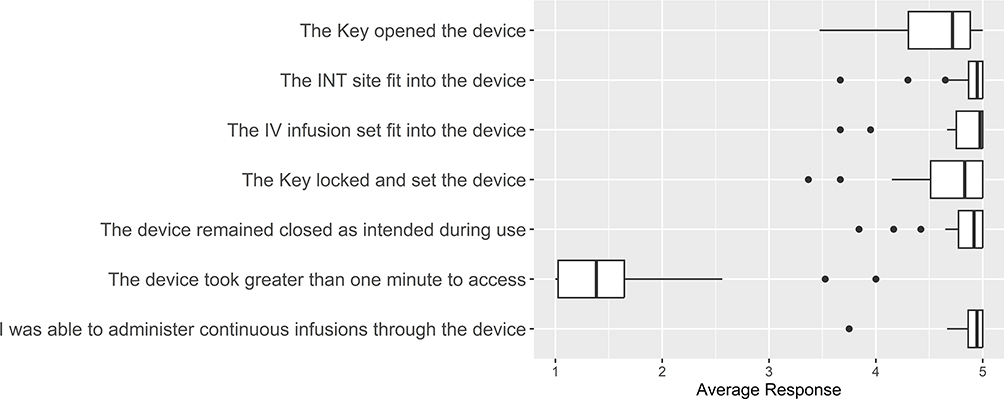 |
Figure 8 Boxplot of individually averaged nurse responses to device functionality. |
Discussion
The survey results (Table 1) demonstrate that the studied ED nurses thought the device was overall easy to use and the basic instructions served as intended. There was noted disagreement among the participants regarding the size of the device; however, most felt it was acceptable.
The most noted difficulty with the device was the keys. Our initial trial in the simulation lab used handmade metal keys which showed consistent performance for 500 uses per lock. The design tolerances of metal keys necessitated the use of 3D-printed keys for this study. Some of these keys did not adequately withstand the forces of setting and locking the device. We would expect the results for locking and unlocking ease to improve if the study were repeated with machined keys.
The device functioning analysis (Table 2) reaffirmed that the device performed as expected in the clinical setting. The key easily opens the device 87% of the time, and the INT or infusion tubing fits into the device 87% of the time. Additionally, it took less than one minute to access the device 68% of the time. It was noted that certain nurses had more difficulty in general and their scores consistently showed poorer performance and ease of use. Many nurses also commented that the lock became more familiar with repeated use. There was no date stamp on the surveys returned; therefore, we could not track potential improvement in use, functionality, and time to access.
The consideration of individual nurses in Figures 7 and 8 shows an overall positive response and the presence of few outliers. Two to three outliers were found in fitting the device or infusion into the device, inserting the key, and keeping the device locked. It was noticed that one nurse returned 12 surveys and was an outlier in 7 of the responses. This may have skewed that data if he/she had returned all 20 surveys with similar responses.
The Mayo Clinic IRB approved the clinical trial with a fail-safe mechanism, and an additional catheter connection was added to the INT site. This would allow for the device to be immediately removed without risk to the patient if the lock were to fail at any time. Over the course of the study, there were no reported use instances of this fail-safe. However, the presence of this catheter connection altered some of the nurse’s perceptions regarding patient ease for intentional access and was written in the survey comments. This also likely negatively impacted responses for device prevention of patient self-injecting (9% disagreeing or strongly disagreeing).
Overall, the response from the nursing staff was positive. The device functioned as intended and was easy to use. It performed well in a live hospital setting, with patients getting various intravenous infusions and medications.
Limitations of the Study
This study investigated device usability and functionality from a nursing perspective. It did not assess the prevention of intentional patient access and patient safety, which are areas of future research.
Conclusion
The prospective study of the functionality of IV SafeLock in the clinical setting showed that the lock functioned as intended. This is an encouraging development to help providers and nurses treat patients who inject drugs into their vascular access devices while receiving intravenous therapy.
Data Sharing Statement
The authors will make all deidentified data available on request for a period of 2 years following publication by contacting the corresponding author.
Ethics Statement
This study was approved by the Mayo Clinic IRB and was funded by an internal institutional grant. The study was performed in compliance with the Declaration of Helsinki.
Disclosure
The clinical trial was done to evaluate the prototype in a live hospital environment. The trial was executed with the intention of securing a medical device company to license the product. A patent was pending at the time of the clinical trial.
Dr Kara Bragg reports grants, non-financial support from Mayo Clinic, outside the submitted work; in addition, Dr Kara Bragg has a patent 17/480,726, not licensed yet. Dr Michael Albus reports grants from Mayo Clinic, outside the submitted work; in addition, Dr Michael Albus has a patent 17/480,726, not licensed. The authors report no other conflicts of interest in this work.
References
1. Eaton EF, Westfall AO, McClesky B, et al. In-hospital illicit drug use and patient-directed discharge: barriers to care for patients with injection-related infections. Open Forum Infect Diseases. 2020;7(3). doi:10.1093/ofid/ofaa074
2. Chapple HS. Placing a central vascular access device in a patient with substance use disorder: the ethical position of the infusion nurse. J Infus Nurs. 2021;44(1):21–25. doi:10.1097/nan.0000000000000407
3. Powell D, Pacula RL, Taylor E. How increasing medical access to opioids contributes to the opioid epidemic: evidence from medicare part D. J Health Econ. 2020;71:102286. doi:10.1016/j.jhealeco.2019.102286
4. Scholl L, Seth P, Kariisa M, Wilson N, Baldwin G. Drug and opioid-involved overdose deaths - United States, 2013–2017. MMWR Morb Mortal Wkly Rep. 2019;67:51–52.
5. Control CfD. Understanding the opioid overdose epidemic. web page. Center for disease control and prevention; 2023. Available from: https://www.cdc.gov/opioids/basics/epidemic.html.
6. Chen Q, Larochelle MR, Weaver DT, et al. Prevention of prescription opioid misuse and projected overdose deaths in the United States. JAMA Netw Open. 2019;2(2):e187621. doi:10.1001/jamanetworkopen.2018.7621
7. Hsu DJ, McCarthy EP, Stevens JP, Mukamal KJ. Hospitalizations, costs and outcomes associated with heroin and prescription opioid overdoses in the United States 2001-12. Addiction. 2017;112(9):1558–1564. doi:10.1111/add.13795
8. Zolopa C, Hoj S, Bruneau J, et al. A rapid review of the impacts of “Big Events” on risks, harms, and service delivery among people who use drugs: implications for responding to COVID-19. Int J Drug Policy. 2021;92:103127. doi:10.1016/j.drugpo.2021.103127
9. Brooks HL, Salvalaggio G, Pauly B, et al. ”I have such a hard time hitting myself, I thought it’d be easier”: perspectives of hospitalized patients on injecting drugs into vascular access devices. Harm Reduct J. 2022;19(1):54. doi:10.1186/s12954-022-00637-1
10. Sullivan GM, Artino AR Jr. Analyzing and interpreting data from likert-type scales. J Grad Med Educ. 2013;5(4):541–542. doi:10.4300/jgme-5-4-18
11. University CM. Tips for presenting survey data effectively. Available from: https://www.cmu.edu/student-success/other-resources/handouts/comm-supp-pdfs/presenting-likert-data.pdf.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.