")
Back to Journals » Clinical Ophthalmology » Volume 17
Evaluation of the Efficiency and Safety of a 27-Gauge 20,000 Cuts per Minute Vitreous Cutter
Authors Doi Y, Muraoka Y , Tsujikawa A
Received 10 May 2023
Accepted for publication 23 June 2023
Published 18 July 2023 Volume 2023:17 Pages 2037—2043
DOI https://doi.org/10.2147/OPTH.S418371
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Yuta Doi, Yuki Muraoka, Akitaka Tsujikawa
Department of Ophthalmology and Visual Sciences, Kyoto University Graduate School of Medicine, Kyoto, Japan
Correspondence: Yuki Muraoka, Department of Ophthalmology, Kyoto University Graduate School of Medicine, Sakyo-ku, Kyoto, 606-8507, Japan, Tel +81 075-751-3250, Fax +81 075-752-0933, Email [email protected]
Purpose: The aim of this study was to evaluate the efficiency and safety of a 27-gauge (G) 20,000 cuts per minute (cpm) vitreous cutter in clinical settings.
Patients and Methods: This was a retrospective and observational study of 40 eyes of 40 patients with idiopathic epiretinal membrane (ERM). Twenty patients (20 eyes) were treated using a 27G 10,000-cpm vitreous cutter (Advanced ULTRAVIT® Probe, Alcon), whereas the remaining 20 patients (20 eyes) were treated using a 27G 20,000-cpm cutter (Hypervit® dual-blade probe, Alcon). All the surgeries were performed by the same surgeon (YM). The time from the start of vitrectomy to the start of ERM peeling was independently measured by two separate examiners using digital videos of each surgery. The average duration of vitrectomy was calculated for each patient. Additionally, the data of the patients in the two groups were extracted from their medical and surgical records and compared.
Results: The time from the initiation of vitrectomy until the start of ERM peeling was 184 ± 56.9 and 152 ± 39.5 s for the 10,000-cpm and 20,000-cpm groups, respectively. The duration of vitrectomy was significantly shorter in the 20,000-cpm group than in the 10,000-cpm group (p = 0.041). Postoperative vitreous hemorrhage was observed in one patient in the 10,000-cpm group, whereas no complications were observed in the 20,000-cpm group.
Conclusion: In a clinical setting, the 27G 20,000-cpm vitreous cutter may have a higher safety profile and higher efficacy for vitreous removal than that of the 27G 10,000-cpm vitreous cutter.
Keywords: pars plana vitrectomy, 20, 000-cpm cutter, 10, 000-cpm cutter, epiretinal membrane
Introduction
Since the introduction of minimally invasive vitreoretinal surgery in 1970 by Machemer,1 considerable technological progress has been made in the development of vitrectomy systems.2–4 It has been demonstrated that increasing the gauge number of the vitreous cutter during vitrectomy results in a shorter duration of postoperative intraocular inflammation, faster restoration of visual acuity, and reduction of intra- and postoperative complications.5–8
In 2010, Oshima et al introduced 27-gauge (G) vitreous surgery.9 A cutting rate of 7500 cuts per minute (cpm) was introduced in 2013, 10,000 cpm in 2017, and 20,000 cpm in 2020. Several reports have shown that a 27G cutter is superior to a 25G cutter in terms of patient satisfaction and recovery of visual acuity, and thus a somewhat longer surgery time, than that of the 25G cutter.10
A 20,000-cpm dual-blade vitreous cutter, which is designed to prevent a decrease in vitreous flow, has been recently developed. Previous reports indicate that a higher cutter speed can enhance the efficiency of vitreous aspiration. Indeed, non-clinical studies have found that the vitreous aspiration flow achieved with a 20,000-cpm cutter is 25% higher than that achieved with a 10,000-cpm cutter. Despite these promising findings, no studies have yet evaluated the efficiency and safety of a 27G, 20,000-cpm cutter in clinical practice. This gap in the literature led us to investigate the performance of this new cutter. Specifically, the aim of this study was to compare the efficiency and safety of a 27G, 20,000-cpm cutter with those of a 27G, 10,000-cpm cutter in clinical practice.
Materials and Methods
Study Design
This retrospective, observational study was performed using the medical and surgical records of 40 eyes of 40 patients with idiopathic epiretinal membranes (ERM) who underwent vitreous surgery conducted using a 27G, 10,000-cpm vitreous cutter (Advanced ULTRAVIT® Probe; Alcon) or a 27G, 20,000-cpm vitreous cutter (Hypervit® dual-blade probe; Alcon) at Kyoto University from April 2020 to December 2021.
This study was conducted according to the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of Kyoto University Graduate School of Medicine (Kyoto, Japan). As this was a retrospective study, written informed consent was not obtained from the patients; instead, a homepage with information on the purpose of this study was created for the patients to read. The information on the homepage indicated that any patient could opt out of the study at any time via telephone, fax, or email.
The inclusion criteria for the patients were as follows: (1) aged at least 40 years old; (2) underwent vitreous surgery for ERM with posterior vitreous detachment; and (3) was followed up for at least 1 week after surgery. The exclusion criteria were as follows: (1) history of intravitreal injection and/or vitreous surgery; (2) presence of asteroid hyalosis, uveitis, retinal detachment, and/or retinal circulatory disease; and (3) vitreous surgery performed because of a complication that arose during cataract surgery. This last exclusion criterion was applied because in some cataract surgeries, damage to the posterior capsule may necessitate an anterior vitrectomy. In such cases, the core vitrectomy duration can be shorter as the anterior vitreous has already been removed. To maintain consistency in our study, we chose to exclude these cases as they could potentially skew the measurement of vitrectomy time.
All vitreous surgeries were performed by a single ophthalmologist (YM) using a four-port trocar cannula system (Alcon Constellation Vision System; Alcon Laboratories, Fort Worth, Texas, USA). We specifically chose the four-port system to enhance illumination and visibility during surgery, crucial aspects for the effective treatment of epiretinal membranes. One of the ports was dedicated to a chandelier illumination system, which was utilized in all cases. Our rationale for this choice was the belief that to fully leverage the benefits of the wide viewing system, it would be advantageous to increase the area that can be simultaneously illuminated.
The settings for 27G, 20,000-cpm vitreous surgery were as follows: cutting rate, 20,000-cpm and straight aspiration, 0–650 mmHg. The settings for 27G, 10,000-cpm vitreous surgery were as follows: cutting rate, 10,000 cpm and straight aspiration, 0–650 mmHg. Intraocular pressure (IOP) was maintained at 25 mmHg irrespective of the mode of vitreous surgery performed. The surgical microscope used during the surgeries was a Zeiss Hi-R 900 (Lumera) model. The internal limiting membrane (ILM) was stained using brilliant blue G to differentiate ERM from ILM peeling. The ERM was carefully peeled off with the intraocular forceps. The cut part was sutured if any leakage was observed after removal of the trocar.
The duration of vitrectomy was recorded and subsequently included as a parameter for evaluating the efficiency of the 10,000- and 20,000-cpm cutters. In this study, we determined the duration of vitrectomy for each patient using digital video recordings of the surgeries. Specifically, the duration was calculated from the start of the vitrectomy until the initiation of ERM peeling. This measurement was performed independently by two researchers (YD and YM) for each surgery. We recorded each surgery and the duration of vitrectomy was measured once from each video by both researchers. Consequently, two measurements were derived from each surgery. To obtain the mean duration of vitrectomy for each patient, we averaged these two measurements. This methodology allowed us to derive a single mean duration value for each patient, which we subsequently used in our analysis to compare the efficiency of the 10,000-cpm and 20,000-cpm vitreous cutters.
All patients underwent ophthalmological examinations at Kyoto University Hospital. The authors retrieved the medical records of each patient and evaluated the following information: age, sex, preoperative logarithm of the minimum angle of resolution (logMAR) visual acuity, preoperative IOP, axial length, intraoperative complications, presence or absence of complications 1 day after surgery, the proportion of ports that required suture, logMAR visual acuity 1 week after surgery, and presence of complications 1 week after surgery.
Statistical Analysis
Data are presented as means ± standard deviations. Visual acuity was measured using the Landolt chart and converted to logMAR units. Paired t-tests were used to analyze the results of the 25G and 27G groups. Statistical significance was set at 0.05.
Results
Forty patients met the inclusion criteria for this study. The characteristics of the patients included in this study are shown in Table 1. There were no significant differences in age, sex, preoperative IOP, or axial length between the 10,000- and 20,000-cpm groups. Table 2 shows the comparisons of the clinical parameters of the 10,000-cpm and 20,000-cpm groups.
 |
Table 1 Characteristics of the Included Patients |
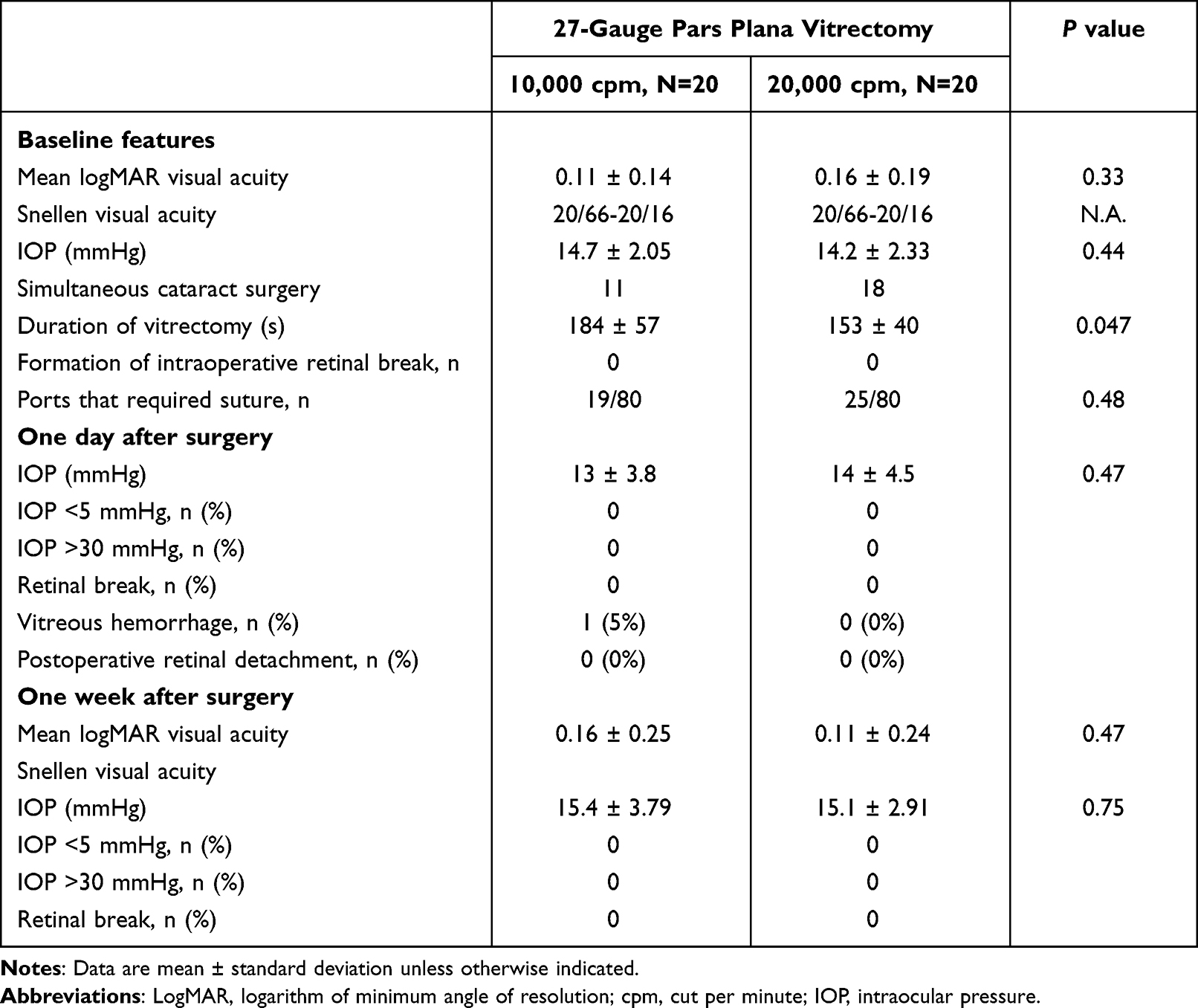 |
Table 2 Comparisons of the Clinical Features of Patients in the 10,000- and 20,000-Cuts per Minute Groups |
Duration of Surgery
The duration of vitrectomy was 184 ± 57s for the 10,000-cpm group and 153 ± 40s for the 20,000-cpm group. The duration of vitrectomy in the 20,000-cpm group was significantly lesser than that in the 10,000-cpm group (p = 0.047).
Visual Acuity
There was no significant difference in preoperative logMAR visual acuity between the 20,000-cpm (0.16 ± 0.19) and 10,000-cpm (0.10 ± 0.14) groups (p = 0.48). In addition, there was no significant difference in postoperative logMAR visual acuity 1 week after surgery between the 20,000-cpm (0.11 ± 0.24) and 10,000-cpm (0.16 ± 0.25) groups (p = 0.47).
Scleral Wound Closure
There was no significant difference between the 20,000- and 10,000-cpm groups in terms of the proportion of ports that required suture (10,000 cpm: 19/80; 20,000 cpm: 25/80) (p = 0.48).
Changes in Intraocular Pressure
There was no significant difference in preoperative IOP between the 20,000-cpm (14.2 ± 2.33) and 10,000-cpm (14.7 ± 2.05) groups (p = 0.44). Postoperative high IOP (>31 mmHg) or low IOP (<5 mmHg) was not observed in both groups.
Complications
One patient in the 10,000-cpm group had vitreous hemorrhage, whereas no patient in the 20,000-cpm group had any postoperative complication (eg, retinal detachment).
Discussion
In this study, we evaluated and compared the efficiency and safety of the 27G, 20,000-cpm and 27G, 10,000-cpm vitreous cutters through the retrospective analysis of the records of 40 eyes of 40 patients with ERM who underwent vitrectomy. The results suggested that the 27G, 20,000-cpm cutter has the same safety profile as that of the 27G, 10,000-cpm cutter but is slightly more efficient.
A previous non-clinical study using swine vitreous reported that the 27G, 20,000-cpm cutter could aspirate more vitreous per unit time compared to the 27G, 10,000-cpm cutter.11 However, the effectiveness of the 27G, 20,000-cpm cutter has not yet been evaluated in actual clinical practice. Though complications associated with 27G vitrectomy have been reported,12 no comparisons of complications associated with the use of the 27G 20,000-cpm cutter or the 27G 10,000-cpm cutter have been documented.
In our study, the mean duration of surgery in the 20,000-cpm group was significantly shorter than that in the 10,000-cpm group (Table 2). The 10,000-cpm cutter utilizes a single-blade structure, whereas the 20,000-cpm cutter features a dual-blade structure, achieving 20,000 cpm as its inner cylinder drives the dual-blade structure 10,000 times.
Non-clinical studies have reported that the 27G dual-blade cutter achieves a higher aspiration flow rate in swine vitreous compared to the 27G single-blade cutter.11,13 The duty cycle of the single-blade cutter decreases as the cut rate increases, leading to a decrease in vitreous aspiration flow. Conversely, the duty cycle of the dual-blade cutter remains consistent as the cut rate increases, resulting in an increased vitreous aspiration flow. In our study, the significantly shorter duration of vitrectomy in the 20,000-cpm group, compared to the 10,000 cpm group, may be attributed to the structural differences between these vitreous cutters.
In this study, one patient in the 10,000-cpm group experienced vitreous hemorrhage 1 day after surgery. However, the 20,000-cpm group exhibited no postoperative complications. No patients in either group presented with intraoperative retinal tear or postoperative retinal detachment. Given the limited sample size and the nature of our retrospective study, it may not be statistically powered to detect rare complications. The beveled-tip cutters, used in both groups, are reported to have a more proximal mean aspiration flow angle compared to flat-tip cutters,14 which could help mitigate retinal movement during aspiration. This may have contributed to the absence of intraoperative retinal tears or postoperative retinal detachments in both groups.
The duty cycle of the dual-blade cutter does not decrease even when the cut rate is increased, resulting in a more stable suction flow rate compared to the single-blade cutter.11 Therefore, the 20,000-cpm cutter is expected to be associated with a lower rate of complications, such as iatrogenic retinal tear or rhegmatogenous retinal detachment, than the 10,000-cpm cutter. However, there were no significant differences in the occurrence of complications between the two groups in this study. Suprachoroidal hemorrhage, a dreaded complication of vitrectomy,15 was not present in this study. The short postoperative follow-up period and the rarity of both intraoperative retinal tear and retinal detachment may explain this outcome.
The 27G cutter is reportedly useful for a variety of vitreoretinal surgery indications such as proliferative vitreoretinopathy requiring silicone oil and diametric tractional retinal detachment,16 while the 27G dual-blade cutter is also suggested to be useful for treating dropped nucleus due to its ability to maintain a high aspiration flow rate.17 As such, it is expected to be useful in all scenarios. As expected, there was no significant difference in wound suturing between the two groups. The wound size was the same for patients treated with the 20,000-cpm cutter as for those treated with the 10,000-cpm cutter. In 27G vitrectomy, wound leakage is reportedly not observed and suturing is not necessary.18 The 27G cutter is shorter and weaker than the 25G cutter, necessitating more dynamic movements when shaving the peripheral vitreous, which may result in larger, leakier wounds.19 As such, less experienced surgeons must use the 27G cutter with caution.
Limitations
Our study does bear several limitations. Firstly, as a retrospective analysis, we could not rigorously control for patients’ conditions across groups. Secondly, the evaluation of vitrectomy duration, conducted through video recordings, might lack precision. Thirdly, while our findings demonstrate significant differences in the performance of the two cutters, the small sample size may limit their generalizability. Lastly, our short follow-up period restricts a comprehensive understanding of the long-term safety and effectiveness of these cutters.
Conclusion
This study indicates that the 27G, 20,000-cpm cutter may be more efficient than the 27G, 10,000-cpm cutter, while presenting a similar safety profile. However, these findings should be interpreted cautiously and validated through larger, prospective studies. A more comprehensive understanding of the long-term safety and effectiveness of these cutters warrants the need for future studies with longer follow-up periods. In conclusion, our findings highlight the potential of the 27G, 20,000-cpm cutter in vitrectomy and underscore the need for further research in this field.
Acknowledgments
The abstract of this paper was presented at the EURETINA 2022 Hamburg as a e-poster presentation with interim findings.
Author Contributions
All authors have significantly contributed to the work reported in various ways, whether in the conception, study design, execution, acquisition of data, analysis, interpretation, or across these areas. YD and YM had full access to all the study data and take responsibility for the integrity of the data and the accuracy of the data analysis.
Each author participated in drafting, revising, or critically reviewing the article. All authors have given their final approval of the version to be published. They have agreed collectively on the journal to which the article has been submitted. Furthermore, every author has reviewed and consented to all versions of the article - before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage. Lastly, all authors agree to take responsibility and be accountable for the entirety of the work presented in the article.
Funding
This work was partially supported with an investigator-initiated study grant from Alcon Japan, Ltd. (Tokyo, Japan), a grant-in-aid for scientific research (Grant number 20K09771) from the Japan Society for the Promotion of Science (Tokyo, Japan), and by Canon INC. (Tokyo, Japan). The funders had no role in the study design, data collection, analysis, decision to publish, or manuscript preparation.
Disclosure
Yuki Muraoka has received grant and financial support from Bayer Yakuhin, Novartis Pharma, Canon, Santen Pharmaceutical, Senju Pharmaceutical, and AMO Japan. Akitaka Tsujikawa has received grant and financial support from Canon, Findex, Santen Pharmaceutical, Kowa Pharmaceutical, Pfizer, AMO Japan, Senju Pharmaceutical, Wakamoto Pharmaceutical, Alcon Japan, Alcon Pharma, Otsuka Pharmaceutical, Tomey Corporation, Taiho Pharma, HOYA, Bayer Yakuhin, Novartis Pharma, Chugai Pharmaceutical, Astellas, Eisai, Daiich-Sankyo, Janssen Pharmaceutical, Kyoto Drug Discovery & Development, Allergan Japan, MSD, Ellex, Sanwa Kagaku Kenkyusho, Nitten Pharmaceutical, Kyowa kirin, and AbbVie GK. None of the abovementioned funding sources were involved in the design, conduct, and preparation of this study or the writing of the article. The authors report no other conflicts of interest in this work.
References
1. Machemer R, Buettner H, Norton EW., et al. Vitrectomy: a pars plana approach. Trans Am Acad Ophthalmol Otolaryngol. 1971;75:813–820.
2. Eckardt C. Transconjunctival sutureless 23-gauge vitrectomy. Retina. 2005;25:208–211. doi:10.1097/00006982-200502000-00015
3. Fujii GY, De Juan E, Humayun MS, et al. Initial experience using the transconjunctival sutureless vitrectomy system for vitreoretinal surgery. Ophthalmology. 2002;109:1814–1820. doi:10.1016/S0161-6420(02)01119-3
4. Fujii GY, De Juan E, Humayun MS, et al. A new 25-gauge instrument system for transconjunctival sutureless vitrectomy surgery. Ophthalmology. 2002;109:1807–1812. doi:10.1016/S0161-6420(02)01179-X
5. Rizzo S, Genovesi-Ebert F, Murri S, et al. 25-gauge, sutureless vitrectomy and standard 20-gauge pars plana vitrectomy in idiopathic epiretinal membrane surgery: a comparative pilot study. Graefes Arch Clin Exp Ophthalmol. 2006;244:472–479. doi:10.1007/s00417-005-0173-6
6. Inoue Y, Kadonosono K, Yamakawa T, et al. Surgically- induced inflammation with 20-, 23-, and 25-gauge vitrectomy systems. Retina. 2009;29:477–480. doi:10.1097/IAE.0b013e31819a6004
7. Kadonosono K, Yamakawa T, Uchio E, et al. Comparison of visual function after epiretinal membrane removal by 20-gauge and 25-gauge vitrectomy. Am J Ophthalmol. 2006;142:513–515. doi:10.1016/j.ajo.2006.03.060
8. Sandali O, El Sanharawi M, Lecuen N, et al. 25-, 23-, and 20-gauge vitrectomy in epiretinal membrane surgery: a comparative study of 553 cases. Graefes Arch Clin Exp Ophthalmol. 2011;249:1811–1819. doi:10.1007/s00417-011-1752-3
9. Oshima Y, Wakabayashi T, Sato T, et al. A 27-gauge instrument system for transconjunctival sutureless microincision vitrectomy surgery. Ophthalmology. 2010;117:93–102. doi:10.1016/j.ophtha.2009.06.043
10. Ma J, Wang Q, Niu H. Comparison of 27-gauge and 25-gauge microincision vitrectomy surgery for the treatment of vitreoretinal disease: a systematic review and meta-analysis. J Ophthalmol. 2020;2020:6149692. doi:10.1155/2020/6149692
11. Inoue M, Koto T, Hirakata A. Comparisons of flow dynamics of dual-blade to single-blade beveled-tip vitreous cutters. Ophthalmic Res. 2022;65:216–228. doi:10.1159/000521468
12. Lubiński W, Gosławski W, Podborączyńska–Jodko K, et al. Comparison of 27-gauge versus 25-gauge vitrectomy results in patients with epiretinal membrane: 6-month follow-up. Int Ophthalmol. 2020;40:867–875. doi:10.1007/s10792-019-01250-1
13. Nepita I, Repetto R, Dodero A, et al. Experimental assessment of the performance of vitreous cutters with fluids with different rheological properties. Graefes Arch Clin Exp Ophthalmol. 2021;259(5):1113–1121. doi:10.1007/s00417-020-05061-4
14. Inoue M, Koto T, Hirakata A. Flow dynamics of beveled-tip and flat-tip vitreous cutters. Retina. 2021;41:445–453. doi:10.1097/IAE.0000000000002811
15. Tabandeh H, Sullivan PM, Smahliuk P, Flynn HW, Schiffman J. Suprachoroidal hemorrhage during pars plana vitrectomy. Risk factors and outcomes. Ophthalmology. 1999;106(2):236–242. doi:10.1016/S0161-6420(99)90062-3
16. Khan MA, Shahlaee A, Toussaint B, et al. Outcomes of 27 augemicroincision vitrectomy surgery for posterior segment disease. Am J Ophthalmol. 2016;161:36–43. doi:10.1016/j.ajo.2015.09.024
17. Watanabe A, Tsuzuki A, Arai K, Gekka T, Tsuneoka H. Treatment of dropped nucleus with a 27-gauge twin duty cycle vitreous cutter. Case Rep Ophthalmol. 2016;7(1):44–48. doi:10.1159/000443721
18. Rizzo S, Barca F, Caporossi T, Mariotti C. Twenty-seven–gauge vitrectomy for various vitreoretinal diseases. Retina. 2015;35(6):1273–1278. doi:10.1097/IAE.0000000000000545
19. Mitsui K, Kogo J, Takeda H, et al. Comparative study of 27-gauge vs 25- gauge vitrectomy for epiretinal membrane. Eye. 2016;30(4):538–544. doi:10.1038/eye.2015.275
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.