Back to Journals » Lung Cancer: Targets and Therapy » Volume 16
Evaluation of the Effectiveness and Safety Profile of First-Line Immune Checkpoint Inhibitors Combined with Chemotherapy in Pulmonary Sarcomatoid Carcinoma
Received 12 September 2024
Accepted for publication 13 May 2025
Published 9 June 2025 Volume 2025:16 Pages 73—83
DOI https://doi.org/10.2147/LCTT.S494990
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Sai-Hong Ou
He Du, Xinyu Song, Fengying Wu
Department of Oncology, Shanghai Pulmonary Hospital, Tongji University School of Medicine, Shanghai, 200433, People’s Republic of China
Correspondence: Fengying Wu, Department of Oncology, Shanghai Pulmonary Hospital, Tongji University School of Medicine, Shanghai, 200433, People’s Republic of China, Email [email protected]
Background: Pulmonary sarcomatoid carcinoma (PSC) represents a rare subtype of non-small cell lung cancer (NSCLC), and it has poor pathologic differentiation, aggressive progression, and early metastasis. Conventional antitumor therapies demonstrate limited efficacy against PSC, which is frequently associated with unfavorable clinical outcomes.
Methods: We conducted an open-label, single-arm Phase II trial. This study has been registered with Clinical Trials (ChiCTR2000031478). Patients received immune checkpoint inhibitor (ICI) combination with chemotherapy, the treatment continued until disease progression, unacceptable toxicity, patient withdrawal, or death. The primary endpoint was objective response rate (ORR), with secondary endpoints comprising progression-free survival (PFS), disease control rate (DCR), overall survival (OS), and treatment-emergent adverse events.
Results: From March 2021 through August 2023, a total of 38 patients were enrolled. The study comprised predominantly male participants (91%, n=34) with a median age of 65.4 years. Notably, 86.8% (n=33) had smoking histories. The ORR and DCR were 73.7% and 94.7%, respectively. The median PFS was 13.3 months (95% CI, 10.2– 15.7) and median OS was not reached. The most common immune-related adverse events were pneumonitis, the incidence of which was 13.2%. The majority of observed AEs were grades 1 or 2 and all AEs were manageable. Only two patients discontinued treatment due to grade 3 immune-related pneumonitis during the study.
Conclusion: In our trial, we found that ICI combination with chemotherapy showed robust efficacy alongside acceptable toxicity in advanced-stage PSC. Taken together, ICI combination with chemotherapy could be a better option for PSC.
Keywords: pulmonary sarcomatoid carcinoma, PD-1 inhibitors, immunotherapy
Introduction
Pulmonary sarcomatoid carcinoma (PSC) is a rare, specialized subtype of non-small cell lung cancer (NSCLC), which accounts for around 0.5% of all lung cancer types.1,2 However, diagnosing PSC can be difficult, especially when only limited biopsy samples are available. Histologically, PSCs frequently appear as biphasic neoplasms, because morphologically it can contain a conventional component of NSCLC and a sarcomatoid component or heterologous sarcomatous tissue. Current therapeutic strategies predominantly align with established NSCLC management protocols. However, PSC exhibit distinct biological characteristics compared to other NSCLC subtypes, demonstrating marked aggressiveness and showing limited response to conventional platinum-based chemotherapy as well as targeted therapy, so they have a poorer outcome than NSCLC, with a median overall survival of less than 7 months with chemotherapy.3,4 Given these therapeutic limitations, developing innovative therapeutic strategies for PSC has emerged as a pressing priority at present.
Therefore, there is an urgent need to identify novel treatment modalities for PSC.
The advent of immune checkpoint inhibitors has revolutionized therapeutic outcomes in NSCLC, conferring unprecedented sustained survival benefits in those patients.5,6 Several predictive biomarkers have been uncovered for identifying ICI-responsive patients, such as PD-L1 expression and tumor mutational burden (TMB). A series of studies have shown that higher PD-L1 expression was correlated with enhanced therapeutic response of PD-1/PD-L1 inhibitors in NSCLC. According to research findings, elevated PD-L1 levels are more prevalent in PSC relative to conventional NSCLC, and increased PD-L1 expression could correlate with improved survival outcomes following immunotherapy.7,8 Besides, PSC exhibits a high TMB level compared to other NSCLC subtypes. Patients with a history of smoking are more likely to harbor mutations, and the high mutation rate of PSC may be associated with genetic instability because of tobacco exposure. There was a trend that patients with high PD-L1 expression and high TMB tumors had better clinical outcomes.9 Recent reports proved that anti-PD-1/PD-L1 inhibitors represent good efficacy in PSC as second-line or beyond.9,10 In addition, retrospective analyses have demonstrated preliminary efficacy signals of first-line immunotherapy in PSC, while the reports are limited to retrospective studies with no adequately powered multicenter randomized controlled trials to back it up.11 Therefore, we performed the current prospective single-center study to evaluate the combination of PD-1 inhibition with platinum-based chemotherapy in treatment-naive locally advanced or metastatic PSC.
Methods
Study Design
This open-label, single-arm phase II trial aimed to evaluate the safety and efficacy of ICIs plus chemotherapy as first-line treatment in patients with advanced PSC. Patients received intravenous PD-1 inhibitors at a dose of 200 mg combined with chemotherapy of platinum plus paclitaxel for 4 cycles, and then PD-1 inhibitors as maintenance therapy until 2 years. Treatment was maintained until the occurrence of disease progression, intolerable toxicity, medical conditions preventing continuation, investigator-determined discontinuation, or participant consent withdrawal.
Patients
Inclusion criteria required adult patients with histologically confirmed advanced PSC. Besides, all participants complied with the outlined eligibility criteria: 1) aged 18 years or older, 2) had not undergone any prior systemic treatment for metastatic disease, 3) presented with an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1, 4) demonstrated measurable lesions as defined by Response Evaluation Criteria in Solid Tumors (RECIST; version 1.1) guidelines, 5) have adequate organ function, 6) asymptomatic brain metastases or treated brain metastases clinically stable for at least 2 weeks. The key exclusion criteria included: 1) autoimmune disease, 2) a condition requiring immunosuppressive medications, 3) active pneumonitis or a history of steroid-dependent non-infectious pneumonitis, 4) Ongoing hepatitis B or C virus infection, 5) a history of HIV infection.
Ethical approval for this study was granted by the institutional ethics committee of Shanghai Pulmonary Hospital, Tongji University. Informed consent forms were voluntarily signed by all enrolled patients. This study was registered with Clinical Trials (ChiCTR2000031478). The study complied with the Declaration of Helsinki.
Assessments
The expression of PD-L1 was examined by means of immunohistochemistry (IHC) employing the monoclonal antibody 22C3 (Dako, Carpinteria, CA). The classification of PD-L1 expression (low or high) was determined by the tumor proportion score (TPS). PD-L1 positivity was defined as the presence of tumor cell membranes demonstrating positive staining in more than 1% of tumor cells in a given sample. High PD-L1 expression was classified as a TPS of ≥50% using the 22C3 antibody, while low PD-L1 expression was classified as a TPS of ≥1% and <50% using the 22C3 antibody.
Radiographic tumor assessments were performed at 8-week intervals during the initial 6-month period, followed by 12-week intervals thereafter. Patients received treatment until either progression of the disease or cessation of therapy owing to unacceptable toxicity, or for other reasons, or up to two years. Survival follow-up was conducted at approximately 3-month intervals through clinic visits or telephonic interviews in accordance with the protocol. Tumor assessments were undertaken by two medical oncologists with clinical expertise (CS and DH) independently according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1. Conflicts were settled through consultation with an additional experienced oncology physician.
Any disagreements were resolved by a third senior medical oncologist (FY).
The study’s primary endpoints was investigator-evaluated ORR according to RECIST 1.1 criteria, with secondary endpoints consisting of PFS, DOR, and OS assessments. Adverse events (AEs) were tracked and classified by severity in accordance with the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0. Safety data were collected for all treated patients every 2 weeks during therapy and for ≤3 months after the last dose of immunotherapy.
PFS was calculated as the duration from the initiation of ICI combination with chemotherapy to the first recorded instance of disease progression (per protocol criteria) or all-cause mortality. Patients without events were censored at their most recent follow-up assessment. OS was measured from the start of ICI combination with chemotherapy until death from any cause or the final documented follow-up for surviving individuals. Safety was assessed by evaluating the incidence of adverse events, and the adverse events were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events v4.0 guidelines.
Statistical Analysis
We employed descriptive analyses to characterize baseline demographics and therapeutic variables. The primary efficacy assessments were performed in all the patients who received at least one dose of ICI combination with chemotherapy. The sample size is calculated based on the desired effect size, significance level (0.05), statistical power (≥80%), and potential expected proportion. To allow for several non-evaluable patients, 38 patients were planned to be enrolled in the study. Kaplan–Meier curves were used to estimate OS, PFS of PSC patients. A 95% confidence interval (95% CI) was computed for the corresponding estimates. Statistical significance was defined as p < 0.05 (two-tailed), with analyses conducted in SPSS 22.0.
Results
Baseline Patient Characteristics
Between March 2021 and August 2023, a total of 38 patients with PSC were enrolled, and the clinicopathological characteristics of these participants are summarized in Table 1. Of the 38 patients evaluated, 35 (91.0%) were male and 3 were female. The age range was 50–79 with a median age of 65.4±7.4 years, and the percentage of patients over 70 was 23.7%. Thirty-six out of 38 patients (52.4%) had an ECOG performance status score of 0 or 1. The majority of patients were ever-smokers. Twenty-four (68.7%) patients were diagnosed with percutaneous lung biopsy. All patients were treatment-naive and received ICIs combined with chemotherapy as first-line treatment. Of the enrolled 38 patients, 16 patients were treated with pembrolizumab, 7 with Carelizumab, 11 with tislelizumab, 4 with Sintilimab.
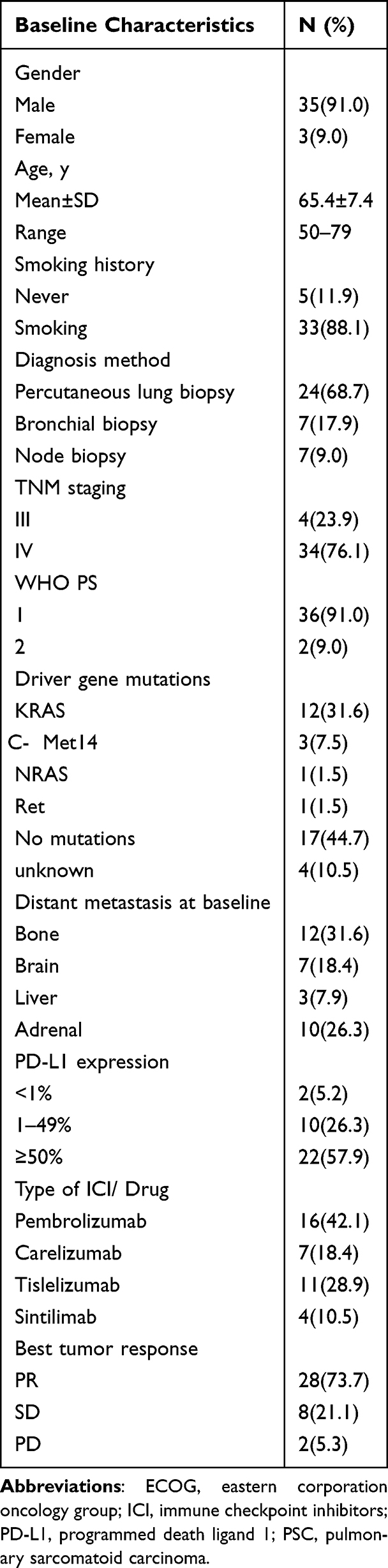 |
Table 1 Baseline Characteristics and Treatment of the 38 PSC Patients Who Received ICIs Combined with Chemotherapy |
Of the enrolled 38 patients, 34 had biopsy samples for PD-L1 evaluation, 22 (19.1%) had ≥50% PD-L1 expression and 10 (55.9%) had ≥1% and <50%, 2 were negative expression. The efficacy of patients with different PD-L1 expression is showed in Table 2. Among the 38 patients, the mutational status for driver genes was unknown in 4 patients, 17 (44.7%) patients had no mutation, 12 (31.6%) patients had KRAS mutations, 3 (7.5%) had METex14 skipping mutations, 1 (1.5%) had Ret fusion, and 1 (1.5%) harbored NRAS mutations. All enrolled patients were diagnosed at advanced stages (III/IV) and 31 patients had distant metastasis. The efficacy of patients with different mutation types is shown in Table 3, and the efficacy of patients with different immune drugs in combination chemotherapy is shown in Table 4. Bone (31.6%) was the most common site of metastases, 10 (26.3%) had adrenal gland metastases, 7 (18.4%) had brain metastases and 3 (7.9%) patients had liver metastases.
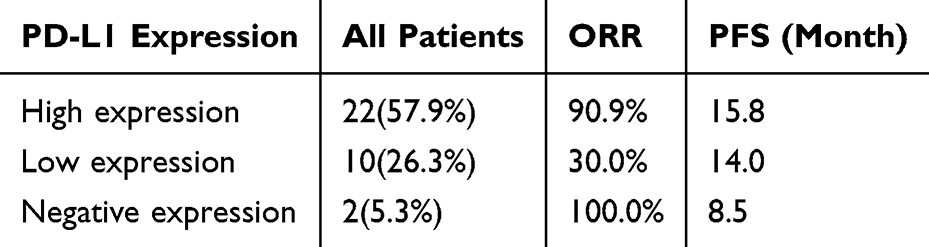 |
Table 2 The Efficacy of Patients with Different PD-L1 Expression |
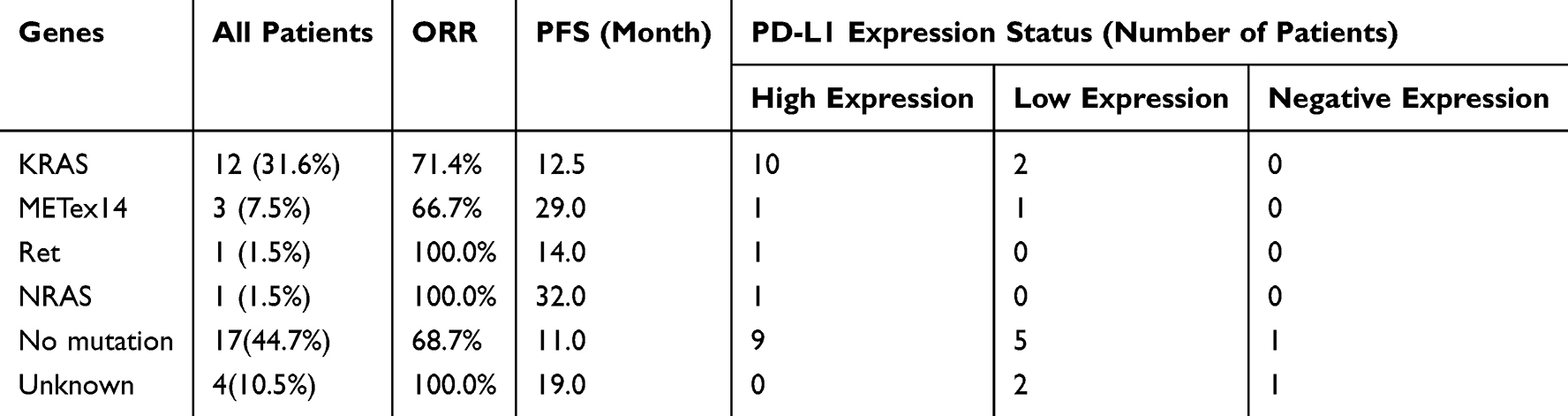 |
Table 3 The Efficacy of Patients with Different Mutation Types |
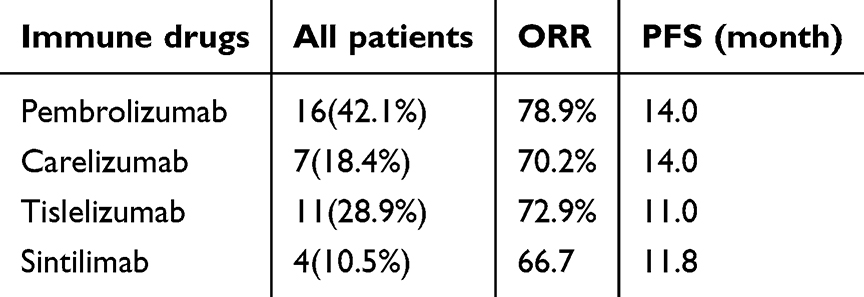 |
Table 4 The Efficacy of Patients with Different Immune Drugs in Combination Chemotherapy |
Treatment and Outcome of Immunotherapy
The median follow-up time for this cohort was 17 (range: 3–35) months. All enrolled patients were administered a minimum of one dose of PD-1 inhibitors and therefore qualified for safety evaluation. Therapeutic outcomes showed absence of complete responses (CR), with 28 partial responses (PR), 8 cases of stable disease (SD), and 2 progressive disease (PD) events among the 38 participants. The ORR was 73.7%. The median PFS was 13.3 months (95% CI, 10.2–15.7 months) and median OS was not reached (Figure 1). Among the 12 patients with KRAS mutations, 8 PR, 3 SD, and 1 PD were achieved. The median PFS was 9.1 months (95% CI, 3.1–22.9 months) (Figure 2). Regarding genomic alteration profiles, the median PFS was 14.5 months versus 13.5 months (95% CI, 6.3–11.7, p=0.231) in patients harboring oncogenic drivers vs those lacking pathogenic variants (Figure 3). In the PD-L1 high expression (⩾50%) cohort, the ORR was 90.9%, median PFS 15.8 months, in the PD-L1 low-expression cohort, the ORR was 30%, median PFS 14.0 months, and in the PD-L1 negative expression cohort, the ORR was 100%, median PFS 8.5 months. Furthermore, we evaluated survival outcomes according to the expression level of PD-L1 and found no significant differences in the PFS and OS (p=0.365 and 0.897) (Figure 4). The comparison of survival outcomes according to PD-L1 expression status demonstrated that the positive PD-L1 expression group was associated with longer PFS (median: 14.1 versus 8.5 months) than the negative PD-L1 expression group,
 |
Figure 1 Median PFS and OS in overall population. |
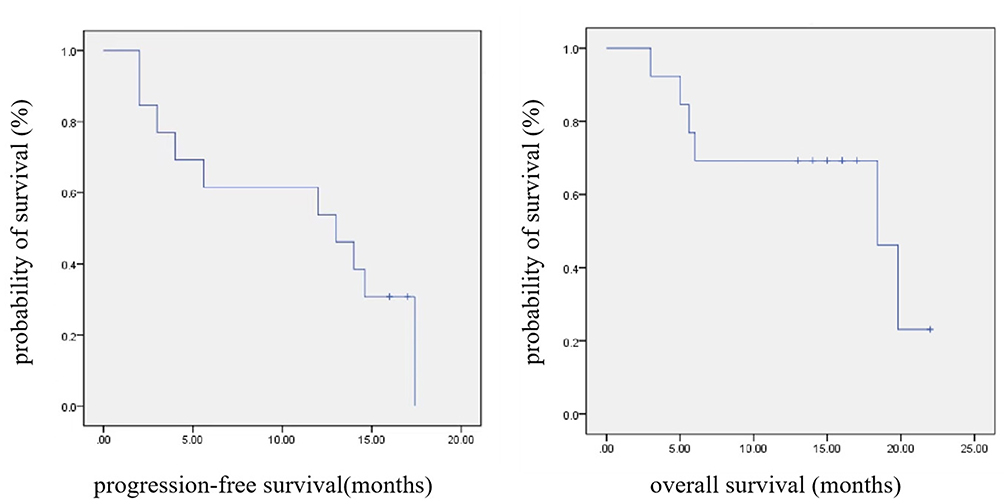 |
Figure 2 Median PFS and OS in overall population according to KRAS mutations. |
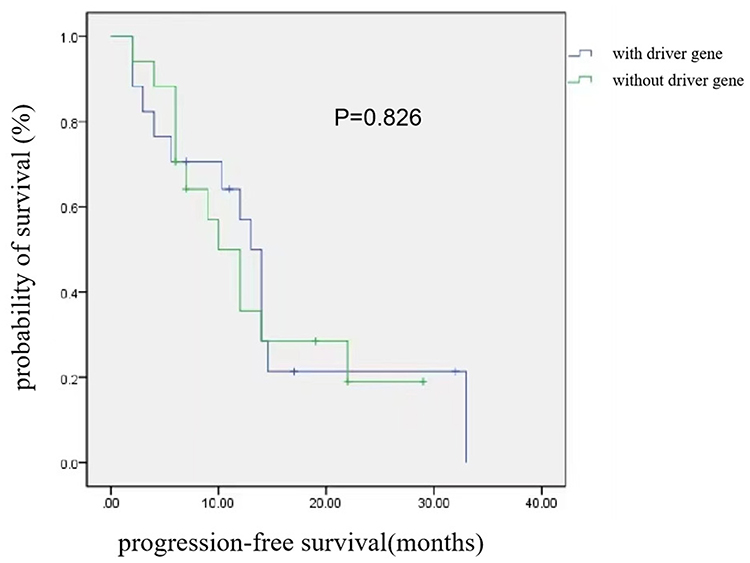 |
Figure 3 The median PFS in patients with and without driver gene. |
 |
Figure 4 Median PFS and OS in overall population according to the expression level of PD-L1. |
Stratified survival analysis based on PD-L1 expression revealed significantly prolonged PFS in the positive PD-L1 expression patients versus the negative PD-L1 expression patients (median: 14.1 versus 8.5 months), but there were no statistically significant differences among subgroups of PD-L1 high, low and negative expression.
Figure 5 demonstrated the depth of response to ICI combination with chemotherapy, and most patients experienced disease control and showed a decrease in tumor size. The overall DCR were 94.7% (95% CI, 46.0–78.2%).
 |
Figure 5 Waterfall plot of best percentage change from baseline in the sum of longest tumour diameters, according to PD-L1 expression in tumour cells. Patient marked with asterisk (※) was considered to show disease progression as best response for non-measurable lesions. PD-L1, programmed death-ligand 1. |
Immune Related Adverse Events
Among the treated patients with PSC, 10 patients (26.4%) had experienced immune-related adverse events of any grade. The most common immune-related adverse event was pneumonitis and the incidence was 13.2%, which occurred in five patients. Other irAEs included two cases of nephritis (grade 1 and grade 2), two cases of hepatitis (grade 1 and grade 2), two cases of thyroiditis (grade 1) and one skin rash (grade 1). Two patients treated with Carelizumab and Tislelizumab, respectively, discontinued treatment due to immune-related pneumonitis (grade 3). They all recovered after two weeks to three months of symptomatic treatment. No fatal adverse events attributable to the therapeutic regimen were observed. There were two patients gone through two different irAEs, one patients treated with treated with Tislelizumab suffer from Grade 1 hepatitis and Grade 2 nephritis, another patients treated with Pembrolizumab gone through Grade 1 pneumonitis and Grade 2 hepatitis. On the whole, the irAEs of different ICB agents used in this study had no statistically significant differences.
Discussion
To the best of our knowledge, this is the first single-center prospective trial to demonstrate the efficacy and long-term safety of ICIs combined with chemotherapy for advanced PSC patients as first-line immune therapy. We revealed the remarkable efficacy of ICIs combined with chemotherapy for advanced PSC, the ORR was 73.7%, median PFS was 13.3 months, which met the primary endpoint. The outcomes based on current data are far better than anticipated, first-line chemotherapy plus immunotherapy has promising therapeutic potential in the treatment of PSC.
Because it is a rare subtype of non-small cell lung cancer, there are few prospective studies that have investigated the effectiveness of ICIs in PSC. Zhou et al performed a multi-center, retrospective and real-world study to evaluate the therapeutic outcomes of PD-1/PD-L1 inhibitor-based combination regimens in PSC patients, the ORR was 73.8%, median mPFS was 10.3 months.11 Zeng et al also performed a multicenter, retrospective analysis, it included 21 PSC patients who received combination therapy or immunotherapy alone as first-line therapy, the median PFS and OS were 9.2 months and 22.8 months, respectively.12 A retrospective study from French included stage III/IV PSC, which treated with ICI monotherapy as a second-line treatment or beyond, it exhibited high response rates and extended OS under PD-1/PD-L1 inhibitor therapy.8 Babacan et al conducted a meta-analysis of published studies to evaluate immune checkpoint inhibitor therapeutic outcomes in PSC populations. Among 90 patients who received ICI monotherapy, the objective response rate was 54.5%, and the median progression-free survival was 7.0 months.9 KCSG-LU16-07 (NCT03084471) was a open-label phase II trial evaluating anti-PD-L1 (durvalumab) plus anti-CTLA-4 (tremelimumab) dual immune checkpoint blockade in patients with recurrent or metastatic PSC, with the ORR of 26.7%, median PFS and OS 5.9 months and 15.4 months, respectively.13 On the whole, all these studies demonstrated good efficacy and manageable toxicity profile of ICI monotherapy or combination therapy in patients with PSC.
Comparative oncogenomics revealed distinct mutational landscapes between PSC and NSCLC, with KRAS and MET (exon 14 skipping) mutations emerging as cardinal oncogenic drivers in PSC pathogenesis.14–16 In our study, KRAS mutations were detected in 31.6% of our study population, demonstrating close concordance with the 33% prevalence rate reported in TCGA lung adenocarcinoma datasets.17 Among the 12 patients with KRAS mutations, the ORR was 66.7%, the median PFS was 9.1 months, which was shorter than that of overall population of 16.2 months. Consistent with our data, Filippo et al demonstrated that patients carrying KRAS mutations exhibited markedly reduced survival rates following surgical resection of PSC, suggesting these genetic alterations negatively impact clinical outcomes.16 However, the discovery of immunotherapy and KRAS G12C inhibitors has dramatically transformed the therapeutic approach for NSCLC patients harboring KRAS mutations. New KRAS G12C inhibitors and several combination therapy strategies, including with immune checkpoint inhibitors or chemotherapy are being investigated in numerous clinical trials. This will hopefully answer questions as regards optimal treatment regimen in these patients.
Retrospective analyses had demonstrated elevated PD-L1 prevalence rates in cohorts with PSC.18 Velcheti et al documented PD-L1 positivity in 9 of 13 patients (69.2%) in their cohort.19 Consistent with these findings, our findings revealed that 84.2% of patients were positive for PD-L1 expression. This was consistent with the range of 53% to 90.2% in PSC as documented in prior research.20,21 In addition, 57.9% of patients showed a high level of PD-L1 expression. Among the 32 patients with PD-L1 positive expression, the ORR was 71.9%, the median PFS was 15.2 months. The PD-L1 expression was used as biomarkers for treatment effect, Lee indicates that 80.0% of PSC with high PD-L1 expression, and these patients were associated with longer PFS and OS.22 The results were consistent with ours. Our data had a tendency that patients with PD-L1 positive expression had longer PFS compared to those with PD-L1 negative expression (14.1 versus 8.5 months). In addition, studies had confirmed that PSC displayed pronounced lymphohistiocytic infiltration with predominant CD4+ T cell clusters and macrophage aggregation,21,23,24 and these cells function as pivotal mediators in immune-mediated tumor suppression, which indicated that PSC may benefit from immunotherapy. The safety data from this study on combined immunotherapy and chemotherapy aligned with the anticipated results derived from existing knowledge on immune-related adverse events, there was no new AEs recognised. Almost one-third of the patients had experienced immune-related adverse events, and all adverse events demonstrated controllability and maintained alignment with established safety profiles. Treatment discontinuations attributable to irAEs remained infrequent, with a minimal incidence of three documented cases throughout the trial period, and the immune checkpoint inhibitors administered in the three patients were camrelizumab and tislelizumab, respectively. Pneumonitis was the most common adverse event observed, with an incidence rate of 13.2%. The incidences of other irAEs, such as nephritis, hepatitis, skin rash and thyroiditis, were much lower, they were 5.3%, 5.3%, 2.6% and 5.3%, respectively, which indicated that ICIs combined with chemotherapy demonstrated favorable tolerability, and the most of observed AEs were grades 1 or 2.
While valuable, the findings of this study have some limitations. First, as this was a single-arm clinical trial, not a randomized controlled trial, and it was not possible to directly compare ICIs plus chemotherapy with conventional chemotherapy. Second, the scarcity of PSC cases resulted in a restricted number of participants, so which was difficult to draw definitive conclusions regarding the efficacy and safety of ICIs plus chemotherapy. However, our findings suggest that ICIs plus chemotherapy was a potential option to treat PSC, this study was the initial prospective trial in patients with PSC about ICIs plus chemotherapy as first-line therapy and met the primary endpoint of PFS, but future large-scale clinical trials are required to confirm our results.
In conclusion, ICIs combined with chemotherapy have demonstrated promising efficacy with well-tolerated adverse events in the treatment of PSC, achieving an ORR of 73.7% with a PFS of 13.3 months (95% CI, 10.2–15.7). These efficacy metrics notably surpass historical controls receiving chemotherapy alone, where conventional paclitaxel-based chemotherapy typically yield median PFS less than 7 months. Regarding safety, the most prevalent irAE was immune-related pneumonitis. The toxicity profile remained manageable, with 80.0% (8/10) of irAEs were categorized as grade 1 or 2 in severity. In consideration of this combined treatment activity in PSC, further prospective randomized control studies of ICIs combined with chemotherapy should be considered for patients with PSC.
Data Sharing Statement
We intend to share our individual identified participant data. The demographic and baseline characteristics can be accessible by contacting the corresponding author at email: [email protected] immediately upon publication for at least 5 years.
Funding
The authors acknowledged the financial support received for the research. This study was supported in part by Clinical Research Foundation of Shanghai Pulmonary Hospital (FKLY20019), and Shanghai “Science and Technology Innovation Action” Medical Innovation Clinical Research Special Project (23Y11908600).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Steuer CE, Behera M, Liu Y, et al. Pulmonary sarcomatoid carcinoma: an analysis of the national cancer data base. Clin Lung Cancer. 2017;18:286–292.
2. Yendamuri S, Caty L, Pine M, et al. Outcomes of sarcomatoid carcinoma of the lung: a surveillance, epidemiology, and end results database analysis. Surgery. 2012;152:397–402. doi:10.1016/j.surg.2012.05.007
3. Zheng Y, Fu Y, Zhong Q, et al. The treatment of advanced pulmonary sarcomatoid carcinoma. Future Oncol. 2022;18:727–738. doi:10.2217/fon-2021-1071
4. Liu X, Wang F, Xu C, et al. Genomic origin and intratumor heterogeneity revealed by sequencing on carcinomatous and sarcomatous components of pulmonary sarcomatoid carcinoma. Oncogene. 2021;40:821–832. doi:10.1038/s41388-020-01573-9
5. Antonia SJ, Villegas A, Daniel D, et al. Durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. N Engl J Med. 2017;377:1919–1929. doi:10.1056/NEJMoa1709937
6. Garon EB, Rizvi NA, Hui R, et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N Engl J Med. 2015;372:2018–2028. doi:10.1056/NEJMoa1501824
7. Zhou F, Huang Y, Cai W, et al. The genomic and immunologic profiles of pure pulmonary sarcomatoid carcinoma in Chinese patients. Lung Cancer. 2021;153:66–72. doi:10.1016/j.lungcan.2021.01.006
8. Mayenga M, Assie JB, Monnet I, et al. Durable responses to immunotherapy of non-small cell lung cancers harboring MET exon-14-skipping mutation: a series of 6 cases. Lung Cancer. 2020;150:21–25. doi:10.1016/j.lungcan.2020.09.008
9. Domblides C, Leroy K, Monnet I, et al. Efficacy of immune checkpoint inhibitors in lung sarcomatoid carcinoma. J Thorac Oncol. 2020;15:860–866. doi:10.1016/j.jtho.2020.01.014
10. Babacan NA, Pina IB, Signorelli D, et al. Relationship between programmed death receptor-ligand 1 expression and response to checkpoint inhibitor immunotherapy in pulmonary sarcomatoid carcinoma: a pooled analysis. Clin Lung Cancer. 2020;21:e456–e463.
11. Zhou F, Guo H, Zhou X, et al. Immune checkpoint inhibitors plus chemotherapy in patients with locally advanced or metastatic pulmonary sarcomatoid carcinoma: a multicentric real-world study. Ther Adv Med Oncol. 2022;14:17588359221136759.
12. Qian X, Wang Y, Liu F, et al. The efficacy and safety analysis of first-line immune checkpoint inhibitors in pulmonary sarcomatoid carcinoma. Front Immunol. 2022;13:956982.
13. Kim M, Keam B, Ock CY, et al. Phase II study of durvalumab and tremelimumab in pulmonary sarcomatoid carcinoma: KCSG-LU16-07. Thorac Cancer. 2020;11:3482–3489.
14. Mehrad M, Roy S, LaFramboise WA, et al. KRAS mutation is predictive of outcome in patients with pulmonary sarcomatoid carcinoma. Histopathology. 2018;73:207–214.
15. Pelosi G, Gasparini P, Conte D, et al. Synergistic activation upon MET and ALK coamplification sustains targeted therapy in sarcomatoid carcinoma, a deadly subtype of lung cancer. J Thorac Oncol. 2016;11:718–728. doi:10.1016/j.jtho.2016.01.009
16. Lococo F, Gandolfi G, Rossi G, et al. Deep sequencing analysis reveals that KRAS mutation is a marker of poor prognosis in patients with pulmonary sarcomatoid carcinoma. J Thorac Oncol. 2016;11:1282–1292. doi:10.1016/j.jtho.2016.04.020
17. Cancer Genome Atlas Research N. Comprehensive genomic characterization of squamous cell lung cancers. Nature. 2012;489:519–525. doi:10.1038/nature11404
18. Maneenil K, Xue Z, Liu M, et al. Sarcomatoid carcinoma of the lung: the Mayo clinic experience in 127 patients. Clin Lung Cancer. 2018;19:e323–e333. doi:10.1016/j.cllc.2017.12.008
19. Velcheti V, Rimm DL, Schalper KA. Sarcomatoid lung carcinomas show high levels of programmed death ligand-1 (PD-L1). J Thorac Oncol. 2013;8:803–805. doi:10.1097/JTO.0b013e318292be18
20. Kim S, Kim MY, Koh J, et al. Programmed death-1 ligand 1 and 2 are highly expressed in pleomorphic carcinomas of the lung: comparison of sarcomatous and carcinomatous areas. Eur J Cancer. 2015;51:2698–2707. doi:10.1016/j.ejca.2015.08.013
21. Vieira T, Antoine M, Hamard C, et al. Sarcomatoid lung carcinomas show high levels of programmed death ligand-1 (PD-L1) and strong immune-cell infiltration by TCD3 cells and macrophages. Lung Cancer. 2016;98:51–58. doi:10.1016/j.lungcan.2016.05.013
22. Lee J, Choi Y, Jung HA, et al. Outstanding clinical efficacy of PD-1/PD-L1 inhibitors for pulmonary pleomorphic carcinoma. Eur J Cancer. 2020;132:150–158. doi:10.1016/j.ejca.2020.03.029
23. Fallet V, Saffroy R, Girard N, et al. High-throughput somatic mutation profiling in pulmonary sarcomatoid carcinomas using the LungCarta panel: exploring therapeutic targets. Ann Oncol. 2015;26:1748–1753. doi:10.1093/annonc/mdv232
24. Chen J, He Q, Liu J, et al. CD8+ tumor-infiltrating lymphocytes as a novel prognostic biomarker in lung sarcomatoid carcinoma, a rare subtype of lung cancer. Cancer Manag Res. 2018;10:3505–3511. doi:10.2147/CMAR.S169074
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.