Back to Journals » Patient Preference and Adherence » Volume 16
Evaluation of the Effect of Changing the Normalised Appointment Mode During the Coronavirus Disease 2019 Epidemic on the Development of Day Surgery
Received 19 July 2022
Accepted for publication 4 November 2022
Published 9 December 2022 Volume 2022:16 Pages 3221—3227
DOI https://doi.org/10.2147/PPA.S377139
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Bangju Li, Xizhen Fan, Qun Xia
Day Surgery Ward, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, Anhui, 230001 People’s Republic of China
Correspondence: Xizhen Fan, Day Surgery Ward The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, Anhui, 230001, People’s Republic of China, Tel +86-0551-62283316, Email [email protected]
Objective: To investigate the effect of changing the normal appointment mode on day surgery.
Methods: From December 2020 to December 2021, 302 patients with day surgery admitted to the hospital by using the unified reservation mode of the intelligent bed system were selected as the experimental group, while 302 patients with day surgery admitted to the hospital by using the decentralised bed reservation mode were randomly selected as the control group. The same-day surgery cancellation rate, bed utilisation rate and patient satisfaction were analysed and compared between the two groups.
Results: The treatment experience of the patients in the experimental group was higher than that in the control group. The same-day surgery cancellation rate was lower than that of the control group, with a statistically significant difference (P < 0.05).
Conclusion: The unified computer reservation mode of the intelligent bed reservation system is superior to the decentralised reservation mode across departments. A daytime intelligent bed reservation mode was adopted for unifying bed appointments, which could effectively reduce the same-day cancellation rate of day surgery, improve bed utilisation and improve patient satisfaction.
Keywords: COVID-19, day surgery, surgical cancellation rate, patient satisfaction, evaluation
Introduction
The outbreak of new coronavirus pneumonia in December 2019 has seriously affected the life and health of people. According to a survey, more than 80% of the patients with new coronavirus pneumonia are asymptomatic or presenting only mild pneumonia and have strong infectivity at the early stage of the infection.1
Day surgery is a new surgical mode that is admitted on the same day, operated on the same day and discharged on the same day. It is fast, efficient and safe. This treatment is highly important in the current social extremely tense background of medical and health resources, and it has also received extensive attention from all sectors of society.2 In China, decentralised and unified bed reservation modes are frequently adopted modalities in clinics. The decentralised bed reservation mode refers to the fact that some specialist wards (ophthalmology, paediatric surgery, urology, etc.) in hospitals individually leave a fixed day surgery bed for day surgery patients admitted to the specialist. Day surgery patients are managed by each department and have a separate appointment for surgery.3 However, the high turnover of patients during day surgery and the large staff mobility in the ward make it difficult to implement a stand-alone decentralised surgical appointment during coronavirus pneumonia. Because the epidemic situation has not yet been fully controlled, if a new type of coronary infection enters the day surgery process, it is easy to cause aggregated infection in the ward. Given this, it is critical that cross-infection and epidemic spread are avoided to identify and isolate the new type of patients with coronary pneumonia as soon as possible.4
The unified reservation mode refers to hospitals setting up a day surgery centre consisting of a day appointment management centre, a day ward and a day surgery room. These centres have an independent day surgery information system and a dedicated care team to uniformly manage patients requiring day surgery across departments.3 With the help of the information centre, this study’s department introduced the day intelligent bed reservation system-His system.5 Patients do not need to repeatedly go back and forth from the ward, make appointments or register. Specialists can check the patient’s test results on this system and then telephone the patient to inform them of the operation’s arrangement and rules. Patients only need to go to the ward on time for admission procedures for treatment.
This study aims to compare two kinds of reservation modes: day decentralised reservation mode and day intelligent bed reservation mode. It also aims to investigate the strengths and weaknesses of both during the coronavirus disease 2019 epidemic.
Information and Methodology
Information
Patients were assigned to the control group and the experimental group based on their admission period. In the control group, a traditional appointment mode was used, and 302 day surgery cases from December 2020 to December 2021 were selected, including 117 male and 185 female patients. In the experimental group, a unified intelligent bed system appointment mode was used, and 302 day surgery cases after December 2021 were selected, including 135 male and 167 female patients. At this time, the Information Department made a special bed reservation system for the department. All patients were reserved beds in accordance with the information system instead of using the traditional reservation mode. This study was approved by the Ethics Committee of the First Affiliated Hospital of University of Science and Technology of China.
Method
The Medical Treatment Process of Day-to-Day Surgical Patients Included Eight Links
Outpatient treatment, preoperative routine examination, anaesthesia evaluation, surgical appointment, admission, surgery, discharge and postoperative follow-up guidance.
Specific Process
The admission and surgical procedures of the two groups are shown in Figure 1.
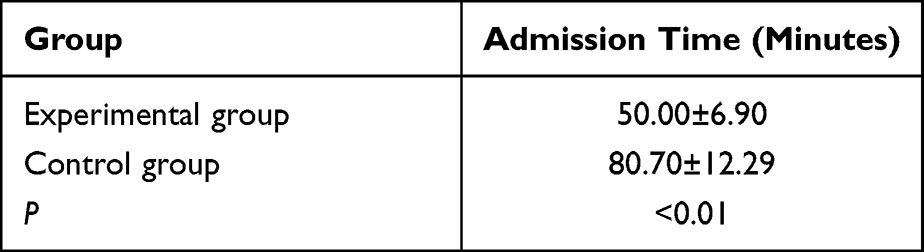 |
Table 1 Comparison Results of Admission Time of Patients with Appointment Mode in the Two Groups |
 |
Figure 1 The flow chart for patient appointment patterns of two groups. |
Evaluation Indicators
- Admission time: Refers to the time required for the doctor to complete the hospitalisation procedure after completing the operation appointment.6
- Cancellation rate of surgery on the same day: After the patient arrived at the hospital on the same day of surgery, the patients who cancelled surgery due to disease factors, their own reasons and imperfect preoperative preparation were statistically analysed. The cancellation rate of surgery = the number of cancelled cases/the total number of appointments in the same period × 100%.
- Patient satisfaction: The patient satisfaction survey mainly included five aspects: the patient’s medical treatment process, surgical treatment effect, doctor–patient communication, health education and medical staff attitude. A total of 25 items were assigned 1–5 points according to “satisfactory”, “more satisfactory”, “general”, “less satisfactory” and “unsatisfactory”, respectively.
The satisfaction questionnaire of each patient has been arranged in the Supplementary Table 1. A total score of the questionnaire < 50 points was satisfactory, and the patients who cancelled the operation were unified and identified as unsatisfactory. The satisfaction rate = satisfactory cases/total cases × 100%.
- Bed utilisation rate: By calculating the bed utilisation rate, the utilisation of bed resources in hospitals before and after the intelligent bed system model was analysed and compared.7
Statistical Processing
The data were analysed by SPSS 22.00 statistical software. Data that did not conform to a normal distribution were presented as percentages (%). The measurement data were expressed as mean ± standard deviation ( ). The t-test was used for the comparison of the mean between the two groups, and the chi-squared (χ2) test or Fisher’s exact probability method were used for the comparison of the mean between the groups of the count data. A P < 0.05 indicated that the difference was statistically significant.
). The t-test was used for the comparison of the mean between the two groups, and the chi-squared (χ2) test or Fisher’s exact probability method were used for the comparison of the mean between the groups of the count data. A P < 0.05 indicated that the difference was statistically significant.
Results
Comparison of Admission Times Between the Two Groups
The admission time of the experimental group was significantly shorter than that of the control group (P < 0.01), indicating that the use of the intelligent bed system model can improve the patient’s medical experience and satisfaction (Table 1).
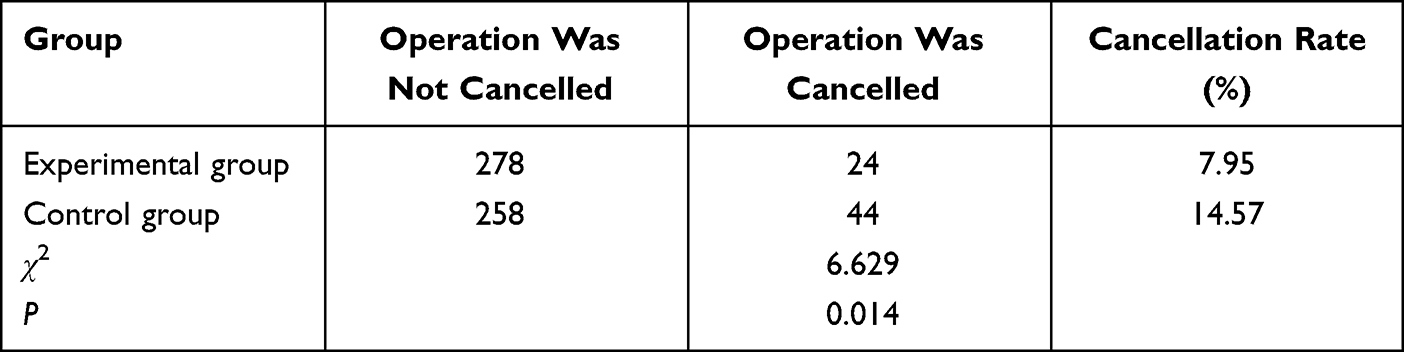 |
Table 2 Comparison of Operation Cancellation Rate of the Two Groups on the Same Day |
Comparison of Surgical Cancellation Rates Between the Two Groups
The surgical cancellation rate in the experimental group was lower than that in the control group (P < 0.05), indicating that the use of the intelligent bed system model can effectively reduce the surgical cancellation rate and provide better treatment services for patients (Table 2).
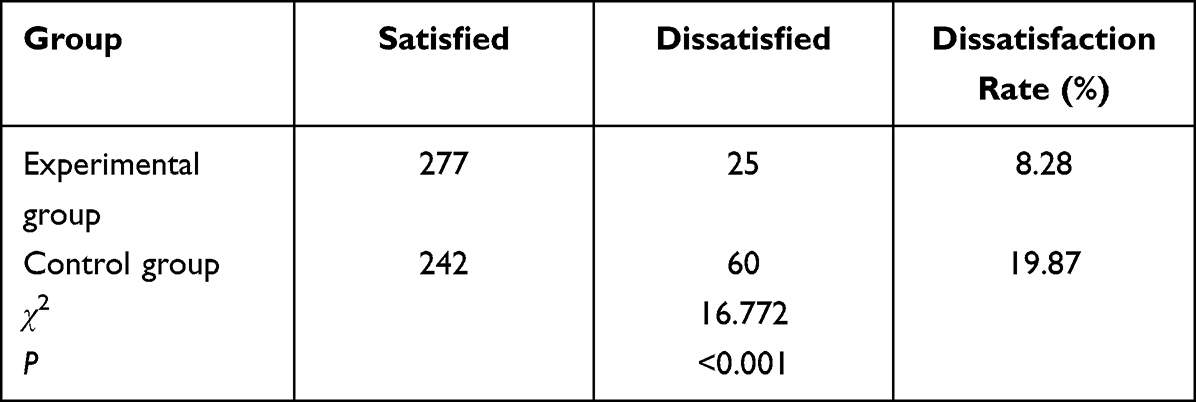 |
Table 3 Comparison Results of Patient Satisfaction of Two Groups by Appointment |
Comparison of Patient Satisfaction Between the Two Groups
The patient satisfaction in the intelligent bed reservation mode of 91.72% was higher than the 80.13% patient satisfaction in the decentralised reservation mode (P < 0.05), indicating that the use of the intelligent bed reservation mode resulted in higher patient satisfaction (Table 3).
 |
Table 4 Comparison of Bed Utilization Rate from 2020 to 2021 |
Comparison of Bed Utilisation Efficiency Between the Two Groups
In the case of a significant reduction in the average length of stay, the utilisation rate of beds has improved, indicating that after the implementation of the intelligent bed system model, the bed resources of the hospital have been fully utilised, and the utilisation efficiency of bed resources has improved significantly (Table 4).
Discussion
Although the domestic epidemic is being gradually and effectively controlled, there are still sporadic cases in some areas, and there is no optimism over the international situation.8 Day surgery is one of the major medical development trends of recent years. Its advantages are a shorter hospital stay, shorter preoperative waiting time and reduced social and economic burden on patients, and it has attracted increased attention in China.9,10 Day surgery patients have shorter turnaround times, more uneventful turnovers, and faster turnarounds than routine inpatient surgery patients. The mobility of the personnel in day wards and operating rooms is large. Once infected, it is highly prone to cluster and cross infection, which places high demands on the prevention and control of new coronavirus pneumonia.11
Due to the gradual expansion of the day-to-day operation volume, the previous SMS, WeChat, telephone and oral appointment methods have been unable to solve the needs of epidemic prevention and have brought great disadvantages to managing the control of the epidemic. The day-to-day operation mode has a short hospitalisation time and a short communication time between patients and medical staff, and patients are unfamiliar with the admission process, resulting in anxiety after their appointments are made.12,13 The previous appointment model is that after the appointment of a specialist is successful, the doctor then telephones the patient to notify them of the hospitalisation time and preoperative precautions. Due to the busy work of doctors, there will be deviations in the evaluation, screening or education in the appointment registration. Poor or missing preoperative health education, biased patient understanding and implementation and inadequate preoperative preparation resulted in high cancellation rates.
With the intelligent bed reservation mode, patients’ basic information is complete. The daytime nurses contact the patients by telephone in advance according to the reservation situation, and the nurses learn the patients’ basic information, history, hypertension, diabetes, etc. The nurses inform the pre-hospital of the method and the importance of continuing to control the basic diseases to improve the compliance of patients and their families.14 In addition, preoperative psychological disorders (such as anxiety and fear) are also important factors that cause preoperative blood pressure and blood glucose abnormalities.15,16 According to the hospitalisation time demand of patients, they can make an appointment for one or two days (the specialist can make an appointment online before three days). For example, when patients who make an appointment cannot be admitted on schedule for various reasons, the specialist would cancel the appointment immediately and re-appointed the next patient, ensuring the bed utilisation rate was maintained to a certain extent. It also met the requirement that the ward did not allow additional beds during the epidemic, thus solving the embarrassment of uncontrolled bed reservations in the ward caused by random appointments.
Insufficient preoperative preparation is an important reason for cancelling surgery after day surgery patients arrive at the hospital.17 Day nurses will also provide patients with psychological comfort and professional guidance according to the reservation system information. These actions can reduce the psychological burden of patients and their families to a certain extent, effectively improve the residence of patients with hypertension and diabetes and reduce the increase in surgery cancellation rate due to disease factors. Especially during an epidemic, these actions can help avoid the risk that patients and their families have not yet detected nucleic acids to seek oral appointments directly from doctors in the ward, which is also in line with epidemic prevention and control.18
The patients’ hospitalisation times were reduced, and the treatments were timely and good, with a better medical experience. The doctors did not need to worry that the operation would be affected because of the wrong appointment information. Day nurses could also know the dynamics of patients in advance, reduce the workload of ward nurses, and improve the working experience of nurses. According to the workload, human resources can be allocated in advance to save on human resources.
Limitations
This study only explores the role of an intelligent appointment model for day surgery. There are still some other surgical diseases that cannot be treated with daytime operations, and the patients requiring these surgeries in the inpatient department did not enrol in this study. Therefore, follow-up studies will further broaden the application of this intelligent appointment model to patients undergoing more surgery types to provide a valuable reference for elective surgery management in the post-epidemic period.
Conclusion
Under the normalisation of the epidemic, the intelligent bed unified reservation mode for day surgery patients is beneficial to homogenisation and standardised management to ensure the accuracy of the reservation. Professional staff should carry out preoperative education to reduce the number of times patients move between different departments, become familiar with preoperative preparation and reduce patients’ preoperative anxieties, fears and worries. High-quality preoperative education can effectively reduce the surgery cancellation rate on the day, improve the utilisation rate of beds and improve the patient’s medical experience. The continuous development of the day-to-day scale makes innovative service processes highly important. Methods and explorations should be continuously summarised to improve nursing work.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of The First Affiliated Hospital of University of Science and Technology of China Anhui Provincial Hospital, and all subjects signed the informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
All of the authors had no any personal, financial, commercial, or academic conflicts of interest separately.
References
1. Wang Y, Chen Y, Qin Q. Unique epidemiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID-19) implicate special control measures. J Med Virol. 2020;92(6):568–576. doi:10.1002/jmv.25748
2. Che G. Current situation and strategy of day surgery in patients with lung cancer by enhanced recovery after surgery. Zhongguo Fei Ai Za Zhi. 2020;23(1):1–4. Chinese. doi:10.3779/j.issn.1009-3419.2020.01.01
3. Wu Q, Xie N, Shao Y. Day surgery appointment scheduling with patient preferences and stochastic operation duration. Technol Health Care. 2021;29(4):697–708. doi:10.3233/THC-192086
4. Yu DL, Liu XN, Ning PT, Xu L, Gao BX. Strategies for the promotion and optimization of ambulatory surgery services under the normalized prevention and control of the new crown pneumonia epidemic. China Med Guide. 2020;22(11):823–827.
5. Xin R. Discussion on the construction of hospital charging internal control based on HIS system environment. Finance Econ. 2022;02:89–91.
6. Jin J, Zhang W, Gao CC, Sheng HQ, Tang LM, Zhu C. Evaluation of application effect of electronic appointment mode in pediatric admission process. Chin Hosp. 2016;20(05):62–63.
7. Lu XC, Liu J, Shen J, Li J. Evaluation of the application effect of the information reservation mode in the admission process of a tertiary general hospital. Jiangsu Health Ser Manage. 2020;31(12):1607–1609+1627.
8. Zhang J, Xia JH, Weng YX, et al. Practice and exploration of resuming daily diagnosis and treatment in public hospitals under normalized epidemic prevention and control. Chin Hosp Manage. 2020;40(9):36–39.
9. Wu LP, Xi KW, Yu H, et al. Research progress on the status quo of participating in ambulatory surgery for medical staff and patients. Chongqing Med. 2020;49(20):3481–3485.
10. Li XY, Wang WL. Application status and development prospect of enhanced recovery after surgery and day surgery in thyroid surgery. J Xi’an Jiaotong Univ. 2019;40(3):494.
11. Ji X, Jing Y, Wu Q, Zhu Z. Thinking of day surgery under the new coronavirus pneumonia epidemic. Chongqing Med. 2020;49(17):2831–2833.
12. Chang J, Shen HL, Sheng Y, Wang H. Exploration on the quality of day surgery nursing based on rapid rehabilitation. Chin Health Qual Manage. 2018;25(04):22–24.
13. Sun XX. Nursing care of 130 cases of breast lumpectomy in day surgery. J Contemp Nurse. 2018;25(08):63–64.
14. Xie R, Khalil I, Badsha S, Atiquzzaman M. An intelligent healthcare system with data priority based on multi vital biosignals. Comput Methods Programs Biomed. 2020;185:105126. doi:10.1016/j.cmpb.2019.105126
15. Fan RP. Research on the Effect of Pestle Point on Preoperative Anxiety and Postoperative Recovery of Patients Undergoing Laparoscopic Cholecystectomy. Chengdu University of Traditional Chinese Medicine; 2018.
16. Yu LX. Current status and prospect of perioperative blood glucose management based on the concept of enhanced recovery after surgery. Qilu Nurs J. 2019;25(08):7–9.
17. Chen W, Zhang SJ, Zhanf YL, Shen L. Analysis of the reasons for cancellation of elective surgery on the day of inpatients. Basic Med Clin. 2022;42(02):296–300.
18. Kueper JK, Terry AL, Zwarenstein M, Lizotte DJ. Artificial intelligence and primary care research: a scoping review. Ann Fam Med. 2020;18(3):250–258. doi:10.1370/afm.2518
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation of the Most Visible Symptoms Associated with COVID-19 Vaccines Among the Residents of Makkah, Saudi Arabia: An Observational, Cross-Sectional Study
Qashqari FS, Alfelali M, Barasheed O, Almaimani R, Alghamdi A, Alharbi SS, Balahmar E, S Alhothali A, Alsharif RH, Jalal NA, Makhdoom H
Infection and Drug Resistance 2023, 16:5107-5119
Published Date: 8 August 2023
Measuring Team Functioning During the COVID-19 Pandemic: Perspectives of Cancer Care Team Members
Attieh S, Kilpatrick K, Chênevert D, Pomey MP, Loiselle CG
Journal of Multidisciplinary Healthcare 2024, 17:2623-2633
Published Date: 27 May 2024