")
Back to Journals » Local and Regional Anesthesia » Volume 12
Evaluation of the attitudes of surgeons about regional anesthesia: a survey study
Authors Yılmaz İnal F , Yılmaz Y , Daşkaya H , Toptaş M , Koçoğlu H , Uysal H, Akkoç İ
Received 8 April 2019
Accepted for publication 29 July 2019
Published 16 September 2019 Volume 2019:12 Pages 89—95
DOI https://doi.org/10.2147/LRA.S211469
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Stefan Wirz
Ferda Yılmaz İnal,1 Yadigar Yılmaz,2 Hayrettin Daşkaya,3 Mehmet Toptaş,4 Hasan Koçoğlu,1 Harun Uysal,4 İbrahim Akkoç4
1Faculty of Medicine, Department of Anesthesiology and Reanimation, Istanbul Medeniyet University, Istanbul, Turkey; 2Department of Anesthesiology and Reanimation, Sultan Abdulhamid Han Education and Research Hospital, Istanbul, Turkey; 3Faculty of Medicine, Department of Anesthesiology and Reanimation, Bezmialem Vakıf University, Istanbul, Turkey; 4Department of Anesthesiology and Reanimation, Haseki Education and Research Hospital, Istanbul, Turkey
Correspondence: Ferda Yılmaz İnal
Faculty of Medicine, Department of Anesthesiology and Reanimation, İstanbul Medeniyet Üniversitesi Göztepe Eğitim ve Araştırma Hastanesi Eğitim Mahallesi Dr. Erkin Caddesi 34722 Kadıköy, Istanbul, Turkey
Tel +90 216 280 3333
Fax +90 505 820 7650
Email [email protected]
Background: The intraoperative attending anaesthesiologist ultimately makes decisions about the anaesthesiology technique to be performed, but the attitudes of surgeons and preferences of patients on this subject may affect their choice. In this questionnaire-based study, we aimed to evaluate the attitudes and behaviors of surgeons about the use of regional anaesthesia (RA) in surgical operations.
Methods: Surgeons from different surgical branches with residencies at 4 different hospitals were asked to complete questionnaires that included reasons for preferring (12 reasons) and not preferring (13 reasons) the use of RA techniques for surgeries, using a 5-point Likert scale.
Results: A total of 156 surgeons from 4 hospitals, out of 167 surgeons who were approached to participate in the study, completed the questionnaire. The most commonly observed reason for a preference towards regional anaesthesia among the surgeons was the risk of general anaesthesia for patients with an American Society of Anesthesiologists (ASA) risk class of III and above. The second most commonly observed reason was for protection from the complications of general anaesthesia, and the third most commonly observed reason was the lower risk of thromboembolisms with regional anaesthesia. The most commonly observed reasons for not choosing regional anaesthesia were found to be incompatibility of the patients and patients’ fears of feeling pain during surgery.
Conclusion: We conclude that programmes for informing surgeons and educating patients about the advantages of RA may increase the preference ratio among surgeons and decrease patients’ refusals to choose this procedure.
Keywords: regional anaesthesia, surgeon’s attitudes, anaesthesiologist
Corrigendum has been published for this article
Introduction
Regional anaesthesia (RA) for surgery is becoming more and more popular all over the world because it has several advantages over general anaesthesia. The use of RA in an institution is generally affected by factors related to the surgeon, anaesthesiologist, or patient that may include a relative shortage of regional anaesthesiology staff, operating room efficiencies, or uncertainty about how best to teach RA techniques.1,2 Although the intraoperative attending anaesthesiologist ultimately makes the decision about the anaesthesiology technique to be performed, the attitudes of surgeons and preferences of patient may affect their choice.3 Furthermore, the feelings of the surgeon about the anaesthetic technique usually influence the preference of the patient.4 It is clear that greater use of RA in an anaesthesiology teaching programme positively affects the learning of residents regarding how to perform RA. In fact, it is necessary to perform a certain percentage of RA procedures in an anaesthesiology residency programme. For example, experience with 40 peripheral nerve blocks is needed for each resident in a residency programme, according to the Accreditation Council of Graduate Medical Education (ACGME).5 There are few studies about the perspectives and attitudes of surgeons towards the application of regional anaesthesia for surgical operations, although many studies have been performed to investigate the preferences and expectations of patients regarding anaesthetic techniques.6–8 For this reason, we aimed to evaluate the attitudes and behaviors of surgeons regarding regional anaesthesia for surgical operations.
Methods
Following the approval of the Ethics Committee of the Medical Faculty of Bezmialem Vakif University (IRB: 71306642-050.01.04), surgeons from different surgical branches with residencies at 4 different hospitals were asked to complete a questionnaire that included their reasons for preferring and not preferring RA techniques for surgeries. The completion of the questionnaire was taken as a surgent’s approval and form of individual consent to participate in the study and deemed to be informed consent.
Twelve reasons for choosing RA (Group A questions) and thirteen reasons for not choosing RA (Group B questions) were determined according to the previous reports. Surgeons were asked to rate their reasons for choosing or not choosing RA using a 5-point Likert scale based on each reason’s degree of importance to them (1: not important, 5: very important). The questionnaire also collected demographic data, including experience as a surgeon and the length of time spent working as a surgeon at the institution. The hospitals where the surgeons had their residencies and became specialists were also noted, along with the surgical departments in which the surgeons worked at the time of the study.
The Statistical Package for the Social Sciences version 22.0 (IBM Corporation, Armonk, NY, USA) program was used for the statistical analysis. The Friedman test was used to compare the reasons for preferring and not preferring RA. Mann-Whitney U tests or Kruskal-Wallis tests were used to determine whether categorical features were effective or not for preferring or not preferring RA. The relationships between the numerical properties and the reasons for preferring or not preferring RA were investigated using Spermin colour correlation analyses. The statistical significance level was set at 5%.
Results
A total of 156 surgeons from 4 hospitals, out of 167 surgeons who were approached to participate in the study, completed the questionnaire. Eleven surgeons could not be reached because they were away from their hospital during the study period. This study reflects the opinions of surgeons regarding regional anaesthesia with a 90% confidence level and an error of 1,36%. The number of surgeons included in the study was found to be sufficient based on a power analysis. The demographic data of the surgeons are presented in Table 1. The most common reason for preferring regional anaesthesia among the surgeons was found to be the risk of general anaesthesia for patients with an American Society of Anesthesiologists (ASA) risk class of III and above (A1), the second most common reason was protection from the complications of general anaesthesia (A2), and the third most common reason was the lower risk of thromboembolisms that regional anaesthesia carries (A11) (Table 2). Among the reasons for choosing regional anaesthesia, the lowest priority one was found to be the ability of the surgeon to communicate with the patient (as the patient is awake) during the operation (A4). The top reasons for not choosing regional anaesthesia were found to be the incompatibility of the patient (B6) and the patient being afraid of feeling pain during the surgery (B8) (Table 3). The lowest priority reason for not choosing regional anaesthesia was found to be the patient being awake (B5).
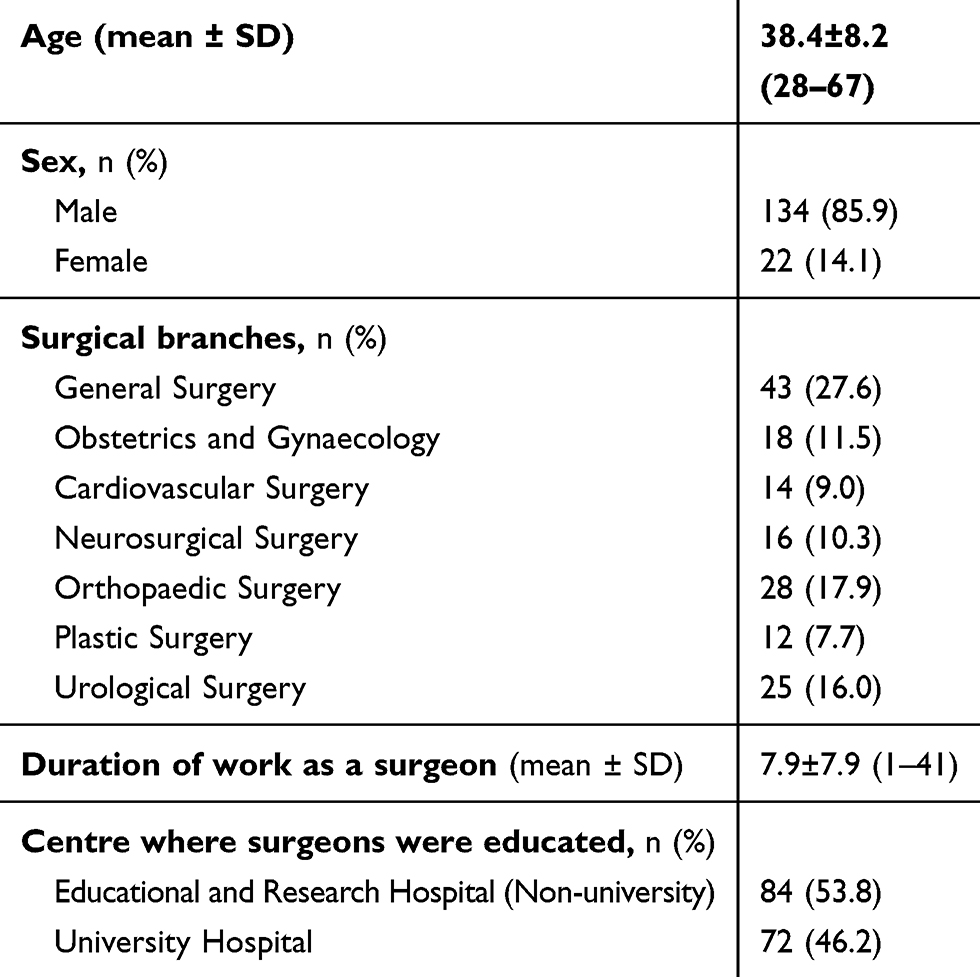 |
Table 1 Demographic data |
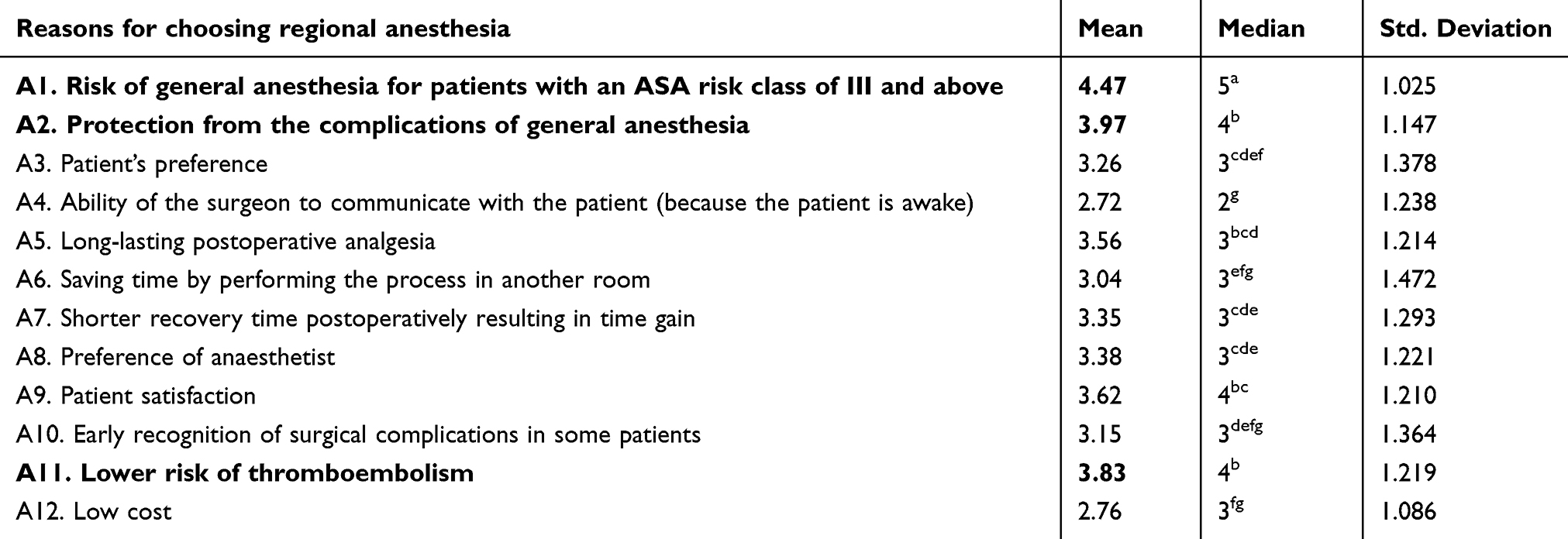 |
Table 2 The reasons for choosing regional anesthesia |
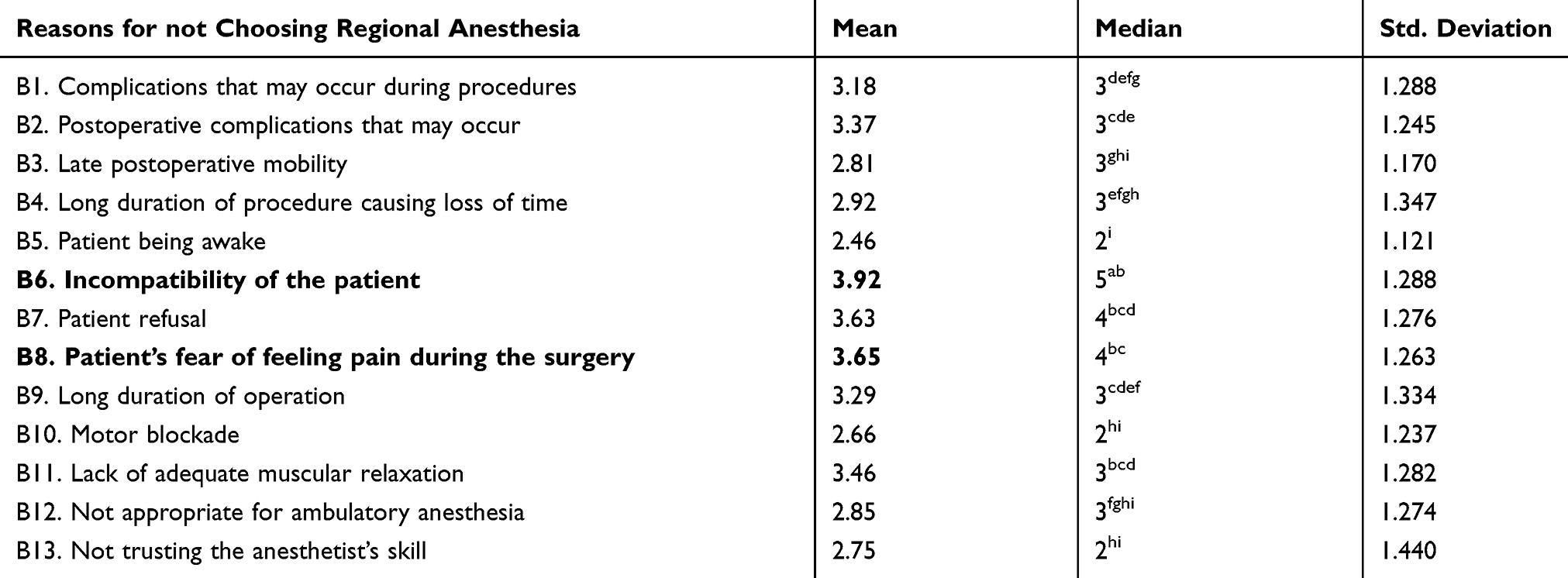 |
Table 3 The reasons for not choosing regional anesthesia |
When surgeons were assessed according to centres where they were educated, saving time by performing the process in another room (A6) and shorter postoperative recovery times, resulting in time gains (A7) were found to be significant parts of the preferences for regional anaesthesia among surgeons educated in university hospitals, while the main reason for choosing regional anaesthesia for surgeons educated in non-university educational and research hospitals was its low cost (A12) (Table 4). When looking at surgical specialties, the top reasons for choosing RA among orthopaedic and general surgeons was its long-lasting postoperative analgesic benefits (A5). Among plastic surgeons, the main reason for choosing RA was the preference of the anaesthetist (A8) (Table 4). A significant negative correlation was observed between the preference of the anaesthetist and the surgeon’s age and duration of work as a surgeon (Table 4).
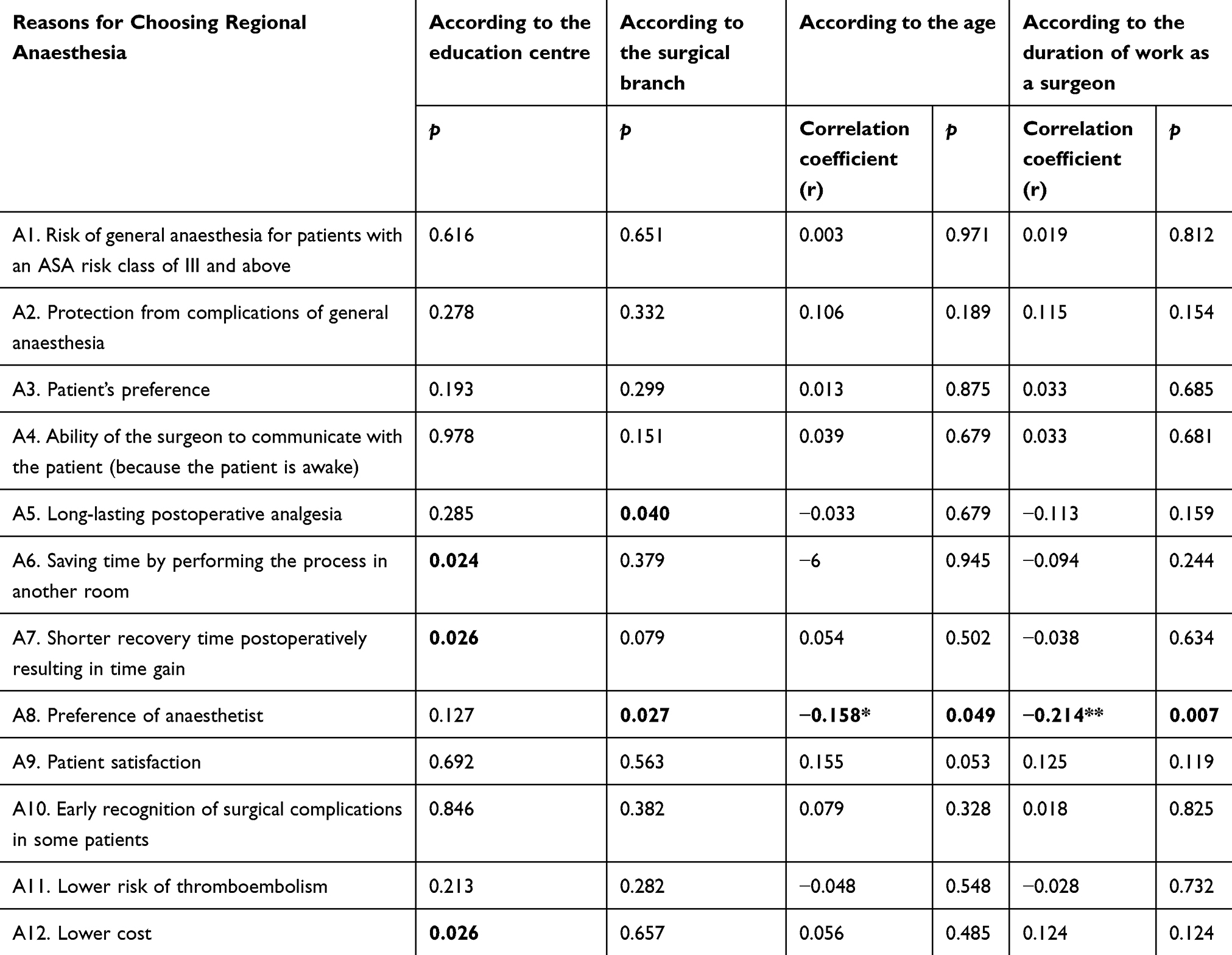 |
Table 4 Reasons for choosing regional anaesthesia according to other parameters |
Long durations of procedures causing loss of time (B4), patients being awake (B5), and not trusting the anaesthetist’s skills (B13) were found to be the top reasons for opposing RA among plastic surgeons, while the top reasons in the obstetrics and gynaecology department were long durations of operations (B9) and the lack of adequate muscular relaxation (B11). A significant negative correlation was found between age and B4, B5 and B11. The surgeon’s age and length of time as a specialist were positively correlated with B13 (Table 5).
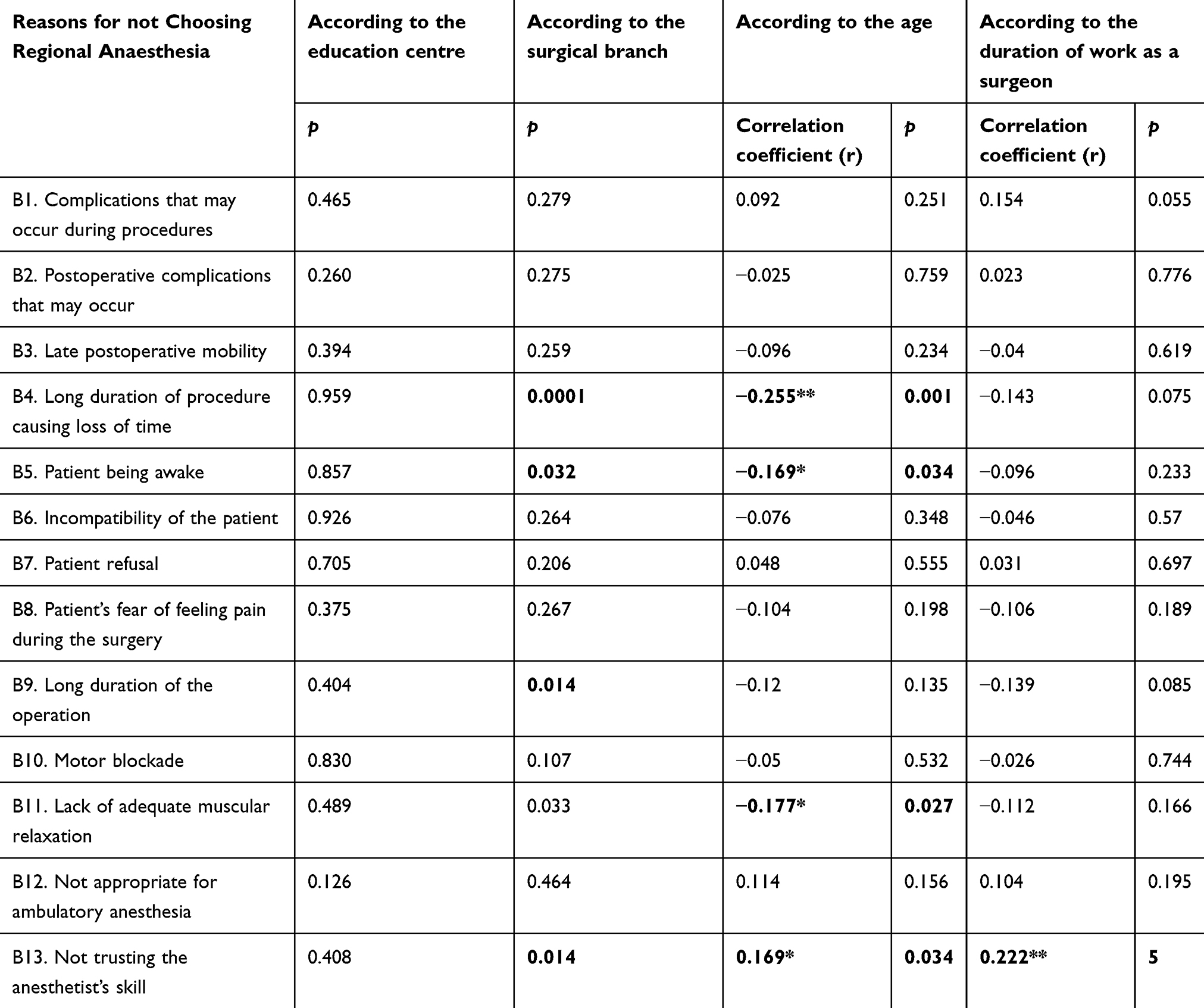 |
Table 5 Reasons for not choosing regional anaesthesia according to the other parameters |
Discussion
The compliance of the patient and the surgical team with the anaesthesiologist’s choice of anaesthetic method, and continued compliance during the entirety of the operation are important for the applicability of anaesthesia. Many patients may be greatly affected by the surgeon when choosing their anaesthetic method, and surgeons have many different beliefs and approaches that are affected by subjective factors such as personal experiences, anxiety and expectations about anaesthetic method preferences. The application of RA is important since the number of complications with RA is reported to be fewer compared to general anaesthesia. However, the benefits of regional anaesthesia have not yet been sufficiently studied, and the rate of regional anaesthesia use is not yet high enough. There are many reasons for this, such as medical contraindications, anaesthesiologist-related factors, surgeon-related factors, patient refusals, delays, unpredictable success, etc. Hanna et al reported that anaesthesiologist-related factors were the primary reason that RA techniques were not used, with a rate of 40%, while surgeon refusals were the second most common reason at 34%.2 Patient refusals accounted for 12% in that study. These results show the importance of the attitudes of surgeons regarding RA. Close communication between surgeons and patients and longer times spent with patients prior to operations are all advantageous for guiding patients’ choices in anaesthesia methods. However, the patient is not able to interact with the anaesthesiologist adequately since the anaesthesiologist usually meets the patient on the day prior to surgery. For this reason, the preference of the surgeon is important so that the anaesthesiologist can avoid problems related to noncompliance in the surgical team. Surgeons were reportedly aware of many of the advantages of regional anaesthesia in previous studies.9–11 Reasons for choosing/not choosing regional anaesthesia for surgical operations have also been reported many times. We used the most commonly encountered reasons from our questionnaire in this study, together with some disadvantages of both RA and general anaesthesia techniques.
One of the important findings in our study is that surgeons participating in the survey chose regional anaesthesia because of the higher risk of general anaesthesia compared to RA in higher-risk patients and for protection from possible complications caused by general anaesthesia. In other words, it can be said that RA is not chosen because of its advantages but rather as an alternative to general anaesthesia in cases where the risk of general anaesthesia is high. Dağlı et al investigated the preferences of obstetricians regarding regional anaesthesia during Caesarean section operations.12 In contrast to our findings, they reported that 80% of obstetricians preferred regional anaesthesia for these operations. The main reasons for this preference were reported to be safety and the lower number of complications compared to general anaesthesia, as obstetricians had noted. From this point of view, it can be thought that surgeons who are lacking information about the advantages of regional anaesthesia need to be more informed and aware of the advantages of regional anaesthesia so that they can consider it as a first option in ASA I-II patients rather than as an alternative to general anaesthesia. On the other hand, this approach of surgeons preferring RA for higher-risk patients is a subjective and unscientific approach, as the most appropriate method of anaesthesia can vary depending on the patient, the type of operation to be performed, the patient’s specific risk factors, and the adequacy of the institution. This approach also indicates that indications and preference for the anaesthetic method should be more informed using more effective information methods.
Incompatibility with patients, patient anxiety about pain, and patient desires were the most common reasons for not choosing regional anaesthesia, among all of the surgeons. Patient-based causes for the preferences of surgeons may be due to believing that the patients will not feel comfortable during surgery. Informing patients about RA, training and increased awareness can improve patient compliance. It may be useful to have longer preoperative anaesthetic visits and to explain the procedures that will be performed in order to relieve anxiety and provide solicitude. A lack of patient-induced negative experiences during operations can change surgeons’ perspectives. The reason rated the least important for a preference against RA was the patient being awake during surgery, which causes some to think that non-anxious, compatible patients being awake does not cause a problem for surgeons.
In this study, we observed that reasons for choosing and not choosing RA changed according to the surgical field. For example, ‘long-term analgesia during the postoperative period was found to be important for choosing RA among orthopaedic and general surgeons, whereas ‘the patient is not sufficiently relaxed’ appeared to be the most common answer in opposition to RA among surgeons in obstetrics and gynaecology. In a survey conducted by Oldman et al to explore the attitudes and knowledge of orthopaedic surgeons regarding regional anaesthesia, forty percent of orthopaedic surgeons directed their patients to choose regional anaesthesia.13 The principal reasons for favouring regional anaesthesia were reported to be less postoperative pain, decreased nausea and vomiting, and safety. Reasons for not favouring regional anaesthesia were reported in that study as delays in the induction of anaesthesia and an unpredictable success rate. In another study, 75% of orthopaedic surgeons reported considering regional anaesthesia to be a safe procedure, and that they therefore prefer this anaesthetic method14 “Saving time by performing the RA procedure in another room” and “short postoperative recovery” were found to be important in our study among surgeons who had been educated at university hospitals, although regional anaesthesia, even performed in the operation room, did not prolong operation room usage times compared to general anaesthesia, as was reported previously.2,11–13,15–18 However, the use of a teaching model in which residents dedicated to an RA rotation and regional blocks perform them in the preoperative area under the supervision of specific regional anaesthesiology faculty has been shown to dramatically increase the number of blocks performed.19 Among surgeons who were educated in education and research hospitals operated by the Ministry of Health, “low cost” was found to be an important factor for choosing RA. All of these factors imply that changes in the preferences of surgical departments were primarily affected by problems that they commonly encounter in their common practices rather than scientific considerations.
When we evaluated the ages of the surgeons, we observed a negative correlation between the ages of the patient and the choice of anaesthetist as a reason for the preference of RA. This may be because the development and use of regional anaesthesia in our country has increased within the last two decades, and the lack of knowledge of older surgeons about regional anaesthesia has reduced their reliability regarding the choice of anaesthesiologist. In our country, the evaluation of RA as a subspecialisation in accordance with the widespread, current scientific developments and expertise training has occurred in the last two decades.20 In addition, RA applications have started to be used more commonly in recent years with the help of imaging tools. These developments have increased the efficiency and quality of RA. We believe that a prejudice against RA could be associated with previous bad experiences of older surgeons who participated in the survey, and positive observations with further experience will change the attitudes of surgeons along with the RA skills of anaesthesiologists. Although it was sufficient according to our power analysis, the number of surgeons surveyed was not very high, which is a shortcoming of our study. If we could have performed this study with a larger number of surgeons, we could have reached a younger population of surgeons, and doing so might have affected the study’s results for the attitudes of surgeons about the reliability of anaesthesiologists for regional anaesthesia.
Our study demonstrated that the main reason for preferring regional anaesthesia among surgeons is to avoid the risks of general anaesthesia, and the main reasons for rejecting RA are the incompatibility of the patient and the patient being afraid of feeling pain during surgery. We conclude that programmes for informing surgeons and educating patients about the advantages of RA may increase the preference ratio of surgeons and decrease patient refusals.
In addition, we want to state that the results of our study are specific to the region and health care system, and although similar, may not be generalizable to other geographics.
Ethics
The completion of the questionnaire was taken as the participants’ approval and form of individual consent to participate in the study and was deemed to be informed consent.
Acknowledgment
The oral presentation for this research was made in May 2017 at the 15th National Regional Anesthesia Congress in Antalya, Turkey.
Author contributions
F Yılmaz İnal, Y Yılmaz and H Daşkaya were responsible for design and conduct of study, data analysis and manuscript preparation. M Toptaş, H Koçoğlu were responsible for design of study, data analysis and manuscript preparation. H Uysal, İ Akkoç were responsible for data analysis and manuscript preparation. All the authors have revised it for important intellectual content and have approved the final version. All authors accept public responsibility fort his study and its conclusions and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Neal JM, Kopacz DJ, Liguori GA, Beckman JD, Hargett MJ. The training and careers of regional anesthesia fellows −1983-2002. Reg Anesth Pain Med. 2005;30:226–232.
2. Hanna MN, Jeffries MA, Hamzehzadeh S, et al. Survey of the utilization of regional and general anesthesia in a tertiary teaching hospital. Reg Anesth Pain Med. 2009;34:224–228. doi:10.1097/AAP.0b013e3181a32c2f
3. Ngan Kee WD, Hung VY, Roach VJ, Lau TK. A survey of factors influencing patients’ choice of anaesthesia for caesarean section. Aust N Z J Obstet Gynaecol. 1997;37(3):300–303.
4. Newsom R, Luff A, Wainwright C, Canning C. UK survey of attitudes to local anaesthesia for vitreoretinal surgery. Eye. 2001;15:708–711. doi:10.1038/eye.2001.234
5. ACMGE Common program requirements. June 10, 20018; effective 7/2007. Chicago, IL, USA: Accreditation Council for Graduate Medical Education. Available from: http://www.acgme.org/acWebsite/RRC_040/040_prIndex.asp.
6. Tong D, Chung F, Wong D. Predictive factors in global and anesthesia satisfaction in ambulatory surgical patients. Anesthesiology. 1997;87(4):856–864. doi:10.1097/00000542-199710000-00020
7. Tait RA, Voepel-Lewis T, Munro HM, Malviya S. Parent’s preferences for participation in decisions made regarding their child’s anesthetic care. Paediatr Anaesth. 2001;11(3):283–290.
8. Matthey PW, Finegan BA, Finucane BT. The public’s fears about and perceptions of regional anesthesia. Reg Anesth Pain Med. 2004;29(2):96–101.
9. Rodgers A, Walker N, Schug S, et al. Reduction of postoperative mortality and morbidity with epidural or spinal anaesthesia: results from overview of randomised trials. BMJ. 2000;321:1493–1497. doi:10.1136/bmj.321.7274.1450
10. Stadler M, Bardiau F, Seidel L, Albert A, Boogaerts JG. Difference in risk factors for postoperative nausea and vomiting. Anesthesiology. 2003;98:46–52. doi:10.1097/00000542-200301000-00011
11. Ganapathy S, McCartney CJ, Beattie WS, Chan VW. Best evidence in anesthetic practice: prevention—epidural anesthesia and analgesia does not reduce 30-day all-cause mortality and major morbidity after abdominal surgery. Can J Anaesth. 2003;50:143–146. doi:10.1007/BF03017846
12. Dağlı R, Dağlı SS. Anaesthetic method preference of obstetricians for caesarean section. Turk J Anaesthesiol Reanim. 2015;43:41–46. doi:10.5152/TJAR.2014.03521
13. Oldman M, CJL M, Leung A, et al. A survey of orthopedic surgeons’ attitudes and knowledge regarding regional anesthesia. Anesth Analg. 2004;98:1486–1490. doi:10.1213/01.ane.0000103265.48380.89
14. Akçaboy EY, Akçaboy ZN, Ekren D, Göğüş N. An assesment of orthopedic surgeons working in a training and research state hospital attitude and knowledge about regional anesthesia. Türkiye Klinikleri J Anest Reanim. 2009;7:143–147.
15. Dexter F. Regional anesthesia does not significantly change surgical time versus general anesthesiaVa meta-analysis of randomized studies. Reg Anesth Pain Med. 1998;23:439–443.
16. Richman JM, Stearns JD, Rowlingson AJ, Wu CL, McFarland EG. The introduction of a regional anesthesia rotation: effect on resident education and operating room efficiency. J Clin Anesth. 2006;18:240–241. doi:10.1016/j.jclinane.2005.08.022
17. Kimberly W, Williams L, Clark L. Does regional anesthesia delay operating time [abstract]. Reg Anesth Pain Med. 2007;32:
18. Sungur MO, Havas F, Karadeniz M, Acar U, Altun D, Seyhan TÖ. The effect of anesthetic technique on operating room usage time in elective cesarean section: spinal or general? Turk J Anaesthesiol Reanim. 2012;40:136–143. doi:10.5222/JTAICS.2012.136
19. Martin G, Lineberger CK, MacLeod DB, et al. A new teaching model for resident training in regional anesthesia. Anesth Analg. 2002;95:1423–1427. doi:10.1097/00000539-200211000-00059
20. Gürkan Y, Kuş A, Aksu C, Ohtaroğlu Ç, Solak M, Toker K. Changing trends and regional anesthesia practices in Turkey. Ağrı. 2014;26(3):131–137. doi:10.5505/agri.2014.26056
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.