Back to Journals » Clinical Ophthalmology » Volume 17
Evaluation of Higher Order Aberrations and Anterior Segment Parameters Changes After Implantable Collamer Lens Implantation for High Myopia
Authors Nassar GA ![]() , Abbas EN
, Abbas EN ![]() , Khalil MMAA
, Khalil MMAA ![]() , Tharwat E
, Tharwat E ![]() , Mohammed AR
, Mohammed AR
Received 17 January 2023
Accepted for publication 17 March 2023
Published 10 April 2023 Volume 2023:17 Pages 1097—1107
DOI https://doi.org/10.2147/OPTH.S405182
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ghada A Nassar,1 Ezzat N Abbas,2 Mahmoud Mohammed Ahmed Ali Khalil,2 Ehab Tharwat,2 Ahmed R Mohammed2
1Department of Ophthalmology, Faculty of Medicine, Cairo University, Cairo, Egypt; 2Department of Ophthalmology, Faculty of Medicine, Al-Azhar University, Cairo, Egypt
Correspondence: Ghada A Nassar, 10 Said Street, Heliopolis, Cairo, 11757, Egypt, Tel +2 01222397300, Fax +20223636504, Email [email protected]
Purpose: To evaluate changes in higher order aberrations (HOAs) induced by implantable collamer lens (ICL) implantation in correction of high myopia and to compare the anterior segment parameters before and after surgery. Also, to correlate these parameters with HOAs, the best corrected visual acuity (BCVA) and intraocular pressure (IOP).
Methods: This prospective interventional cohort case series study included 40 eyes with high myopia that underwent ICL V4c implantation. They were evaluated pre-operatively and post-operatively at 1st and 3rd month HOAs using Scheimpflug Sirius Camera. The anterior segment parameters were evaluated by optical biometry. Correlations between HOAs, BCVA and anterior segment parameters were evaluated.
Results: The mean pre-operative BCVA was 0.67 ± 0.17, while post-operative BCVA was 0.74 ± 0.16 (p-value < 0.001). The spherical equivalent was − 13.66 ± 2.23 pre-operatively, while post-operatively it was − 0.77 ± 0.65 (p-value < 0.001). The mean pre-operative root mean square (RMS) of HOAs was 0.62 ± 0.11 μm, while mean post-operative RMS in the 1st month was 0.82 ± 0.29 μm (p-value < 0.001). At 3rd month, it was 0.63 ± 0.17 μm (p-value = 0.685). The mean pre-operative anterior chamber depth (ACD) was 3.66 ± 0.26 mm. It decreased in the post-operative 1st month to 3.46 ± 0.30 mm, while in 3rd month 3.45 ± 0.24 mm (p-value < 0.001, < 0.001) respectively. The mean pre-operative anterior chamber angle (ACA) 45.98 ± 8.39 o while, the mean ACA was 31.65 ± 4.14, 31.03 ± 3.74 post-operatively (p-value < 0.001, < 0.001) respectively. There was significant increase in IOP (p-value < 0.001).
Conclusion: ICL implantation is safe and effective in correction of high myopia, as HOAs increase at first month post-operatively then, return to the pre-operative level by 3rd month. However, anterior segment parameters show significant changes which may need longer follow up.
Keywords: implantable collamer lens, higher order aberrations, anterior segment parameters, Scheimpflug Sirius Camera, optical biometry, ICL, HOA
Introduction
Implantable collamer lens (ICL) has been documented to be safe and successful for correction of high myopia. ICL implantation has many benefits over corneal refractive surgeries such as laser in situ keratomileusis (LASIK) and photorefractive keratectomy (PRK). This is because ICL implantation avoids corneal complications, such as post LASIK ectasia and dry eye syndrome. ICLs also provide a wider range of refractive error correction. Furthermore, there are less possibilities of higher order aberrations (HOAs) in ICL implantation when compared to corneal refractive surgeries, as cornea is prolate in ICL implantation, but it changes to oblate after corneal surgery. Although different techniques in laser surgery and wave front optimized ablation, there are some factors which affect the outcome of laser surgery such as pre-operative HOAs, pupil size and cyclotorsional misaligned position of laser ablation.1,2
A newly designed ICL with a 360 µm central hole in the central optical zone (V4C-ICL) avoids the need for peripheral iridotomy and decrease the incidence of complications such as anterior subcapsular cataract. The central hole is beneficial for the circulation of aqueous humor. However, HOAs may be created due to their optic properties and different corneal incisions of surgery. There are few studies which evaluated the effect of HOAs in V4C ICL implantation to assess their efficacy, safety and predictability after surgery. Their results revealed changes in HOAs with either positive or negative spherical aberrations. Moreover, visual disturbance, such as glare and halos were described early post-operatively. The effect of cylindrical wall of the central hole V4C-ICL may be added. It acts as an another optical surface, which may induces glare and halos.3,4
Despite its safety, ICL implantation may still cause some complications such as endothelial cell loss, cataract and glaucoma. This is mainly secondary to under or oversizing of the lens. Therefore, the anterior segment parameters are valuable to avoid these complications. Central anterior chamber depth (ACD) and white to white (WTW) are essential parameters for the proper choice of ICL surgery and suitable sizing of ICL.5,6
Furthermore, evaluation of anterior chamber angle (ACA) could be beneficial to predict the risk of angle closure. The intraocular pressure (IOP) was reported to be increased after ICL implantation in previous studies. So, evaluation of ACA and IOP is important to evaluate the status of angle after surgery. Hence, accurate measurements of anterior segment parameters such as ACD, ACA and WTW are valuable for successful results after surgery.7–9
In our study, we aimed to evaluate the effect of ICL implantation on HOAs and anterior segment parameters in patients with high myopia by comparing the pre-operative and post-operative parameters and correlating the different parameters with visual acuity, refraction, HOAs and IOP using optical biometry and Scheimpflug imaging for safety and predictability of ICL implantation in high myopic correction.
Materials and Methods
This prospective observational cohort case series study was performed at Global Eye Center (GEC) in collaboration with Ophthalmology department, Cairo University Hospital, for the period between May 2022 to November 2022. It was approved by the Research Ethics Committee of Faculty of Medicine, Cairo University and was conducted in compliance with principles of Helsinki declaration. All patients signed a written informed consent to participate in the study and for publication of data before enrollment in the study. Forty eyes of 27 patients with high myopia more than –8 diopter, underwent ICL V4c implantation in one or both eyes, were included in this study with age ranged from 21–45 years, patients with stable pre-operative refraction for 6 months, ACD greater than 3 mm. All patients included were not fit for LASIK. All included patients underwent full ophthalmological examination and follow up for 3 months. Patients with high degree of myopic astigmatism (cylinder more than –4 diopter), corneal opacities or any media opacity, uveitis, glaucoma, or increased intra-ocular pressure (more than 20 mmHg) were excluded. Patients with systemic diseases especially collagen diseases were also excluded from the study.
Pre-operative Evaluation
A written informed consent was signed by all patients. All included patients underwent full ophthalmological examination including: Uncorrected visual acuity (UCVA), best corrected visual acuity (BCVA), anterior segment examination and IOP by Goldmann applanation tonometry.
Measurement of HOAs and Anterior Segment Parameters
- Assessment of HOAs was evaluated using combined Scheimpflug–Placido disc system, Sirius camera (Costruzione Strumenti Oftalmici; CSO Camera Inc., Florence, Italy).
- Measurement of anterior segment parameters were done, including ACD, corneal curvature (flatter corneal meridian and steeper corneal meridian) and WTW using optical biometry (IOL master 700, Zeiss, Jena, Germany).
- Measurement of ACA and central corneal thickness (CCT) by CSO Sirius camera.
- Calculation of ICL power using optical biometry and CSO data in the STAAR Formula and by following manufacturer’s instructions.
Surgical Steps of ICL Implantation
In this study, the ICL type is (V4C; STAAR Surgical, Monrovia, CA, USA).
- All patients were operated under local peri-bulbar anaethesia via temporal approach.
- Corneal incision by microkeratome 3.2mm and a small side port using 19 g MVR blade, at right angle of the main incision (at 6 O’clock in right eye and at 12 O’clock in left eye) were done.
- The AC was filled with ophthalmic viscoelastic device (OVD) to protect the lens and corneal endothelium from surgically induced trauma.
- The cartridge was inserted bevel down and the ICL was injected slowly using the (STAAR Surgical) injector with proper orientation.
- OVD was injected on top of the ICL.
- The haptics were pushed gently with footplates under the iris by small spatula through the side port.
- The viscoelastic was removed using Simcoe double way cannula.
- Acetylcholine (Miochol) was injected to get rapid miosis.
- Hydration of the corneal incisions was done.
Post-operative Evaluation
All patients were examined on the 1st day and the 3rd day then, after 1 month and 3 months for evaluation of UCVA, BCVA, refraction and IOP in each visit. HOAs and anterior segment parameters (ACD, ACA, CCT, corneal curvatures and WTW distance) were evaluated after 1 month and 3 months post-surgery and compared with the pre-operative parameters. Correlations between the different parameters, UCVA, BCVA, post-operative refraction and IOP were evaluated. The pre-operative and post-operative various parameters were compared with analysis of all clinical and investigative data.
Statistical Analysis
Data were coded and entered using the statistical package for the Social Sciences (SPSS) version 28 (IBM Corp., Armonk, NY, USA). Data was summarized using mean and standard deviation in quantitative data and using frequency (count) and relative frequency (percentage) for categorical data. Comparisons between pre and post were done using paired t test. For comparison of serial measurements (pre, post1 and post 2), repeated measures ANOVA was used. Correlations between quantitative variables were done using Pearson correlation coefficient. P-values less than 0.05 were considered as statistically significant.
Results
Forty eyes of 27 patients that fulfilled the inclusion criteria were identified.
Epidemiology and Clinical Data
The mean age of the patients was 20.90 ± 1.66 years (range: 18–25). The study included 18 females (65%) and 9 males (35%) of the 27 patients. The BCVA in decimal significantly improved post-operatively. Pre-operative BCVA was 0.67 ± 0.17, while post-operative BCVA was 0.74 ± 0.16 (p-value < 0.001). The post-operative UCVA was 0.62 ± 0.16. The spherical equivalent (SE) was −13.66 ± 2.23 pre-operatively, while post-operatively it was −0.77 ± 0.65 (p-value < 0.001). The IOP was significantly increased post-operatively. The mean post-operative IOP was 17.13 ±1.64 mmHg post-operatively versus 16.05 ± 1.62 mmHg pre-operatively (p-value < 0.001).
IOL Master and CSO Data
From the IOL Master data, the post-operative data at 1 and 3 months were compared with the pre-operative data. The mean pre-operative flatter corneal meridian (K1) was 43.43 ± 1.34 D, while the mean post-operative K1 decreased at 1st month to 43.35 ± 1.32 D. The difference was statistically non-significant (p-value = 0.377). The post-operative K1 at 3rd month was 43.38 ± 1.14 D. The difference was non-significant (p-value = 0.608). The mean pre-operative steeper corneal meridian (K2) was 45.05 ± 1.34 D, while the mean post-operative K2 increased at 1st month to 45.57 ± 1.32 D. The difference was statistically significant (p-value < 0.001). The mean post-operative K2 was 45.45 ± 1.26 D at 3rd month. The difference was statistically significant (p-value < 0.001). The mean pre-operative cylinder was −1.68 ± 0.82, which increased in the post-operative 1st −2.19 ± 1.18, while in 3rd −2.05 ± 0.85. The P- value was significant (p-value < 0.001, < 0.001 respectively) (Figure 1). The mean pre-operative ACD was 3.66 ± 0.26 mm, which decreased in the post-operative 1st month to 3.46 ± 0.30 mm, while in 3rd month 3.45 ± 0.24 mm. The P- value was statistically significant (p-value < 0.001, < 0.001 respectively) (Figure 2). All data are listed in Table 1.
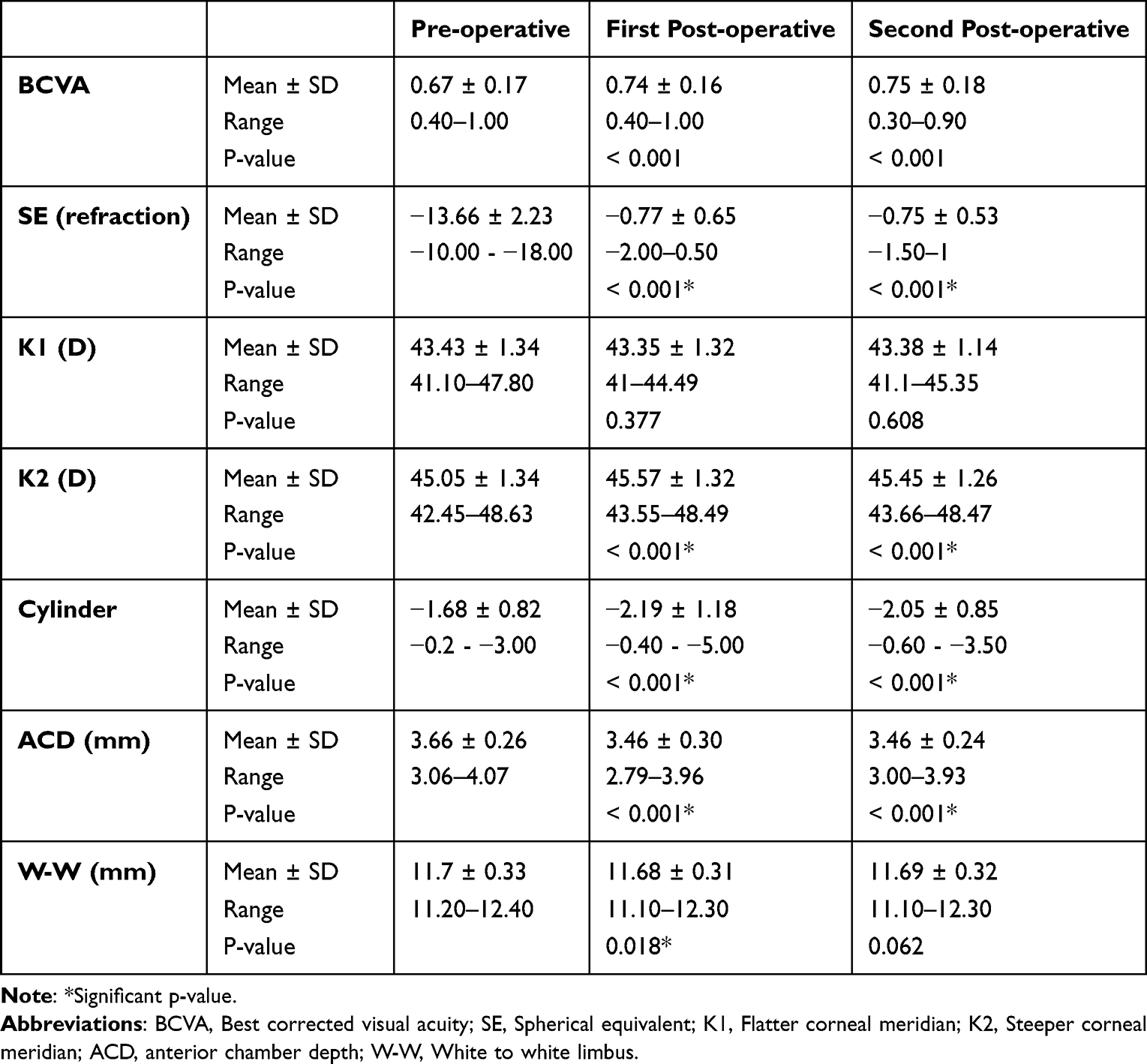 |
Table 1 Comparison of Clinical Data and IOL Master Between the Pre-operative and Post-operative Follow Up |
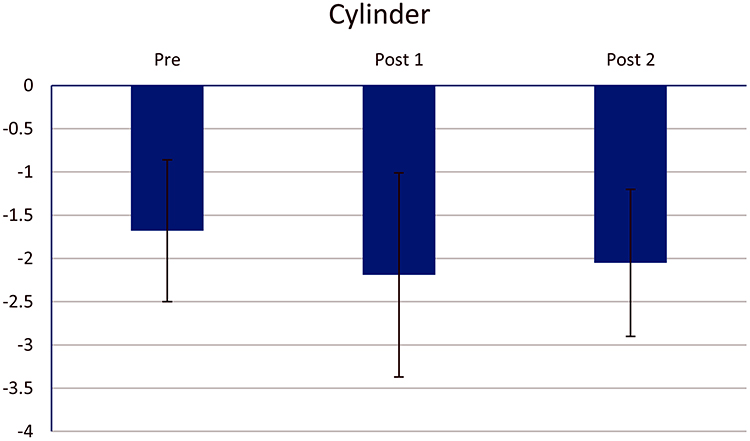 |
Figure 1 The pre-operative and post-operative cylinder at 1st and 2nd follow up. |
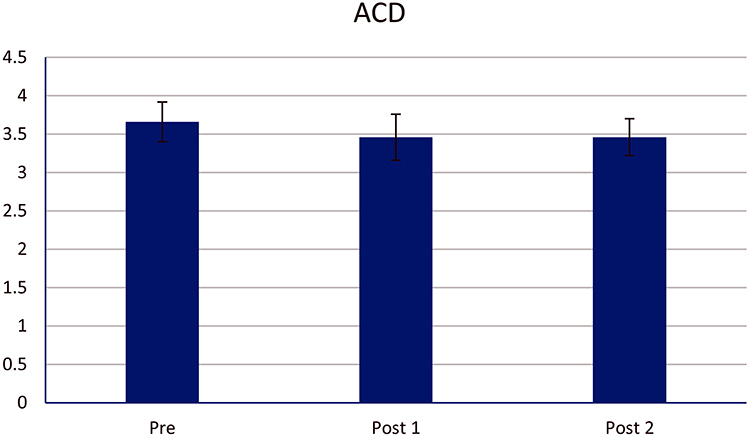 |
Figure 2 The pre-operative and post-operative anterior chamber depth (ACD) at 1st and 2nd follow up. |
There was significant increase in the mean root mean square (RMS) of HOAs in the first post-operative follow up at 1st month (p-value < 0.001). The mean post-operative RMS in the 1st month was 0.82 ± 0.29 µm compared to compared to the mean pre-operative RMS, which was 0.62 ± 0.11 µm. While, mean RMS decreased to nearly the pre-operative value, as the mean post-operative RMS at 3rd month was 0.63 ± 0.17 µm. The difference was non- significant (p-value = 0.685) (Figure 3).
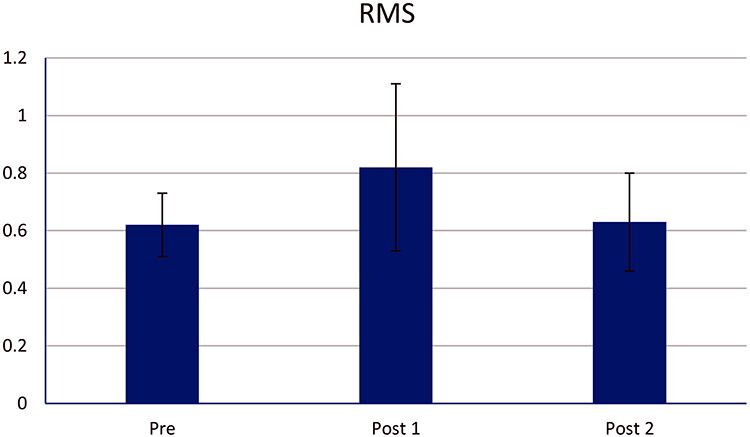 |
Figure 3 The pre-operative and post-operative root mean square (RMS) at 1st and 2nd follow up. |
There was non-significant difference in the CCT in the first at 1st month (p-value = 0.867). The mean post-operative CCT in the 1st month was 522.85 ± 32.65 µm compared to the mean pre-operative CCT, which was 522.38 ± 31.49 µm. It decreased at 3rd, which was 516.68 ± 30.93 µm. The difference was statistically significant (p-value = 0.03). The mean ACA was 31.65 ± 4.14, 31.03 ± 3.74 respectively post-operatively, compared to the mean pre-operative ACA 45.98 ± 8.39. There was statistically significant decrease in ACA (p-value < 0.001, < 0.001 respectively) (Figure 4). These data are shown in (Table 2).
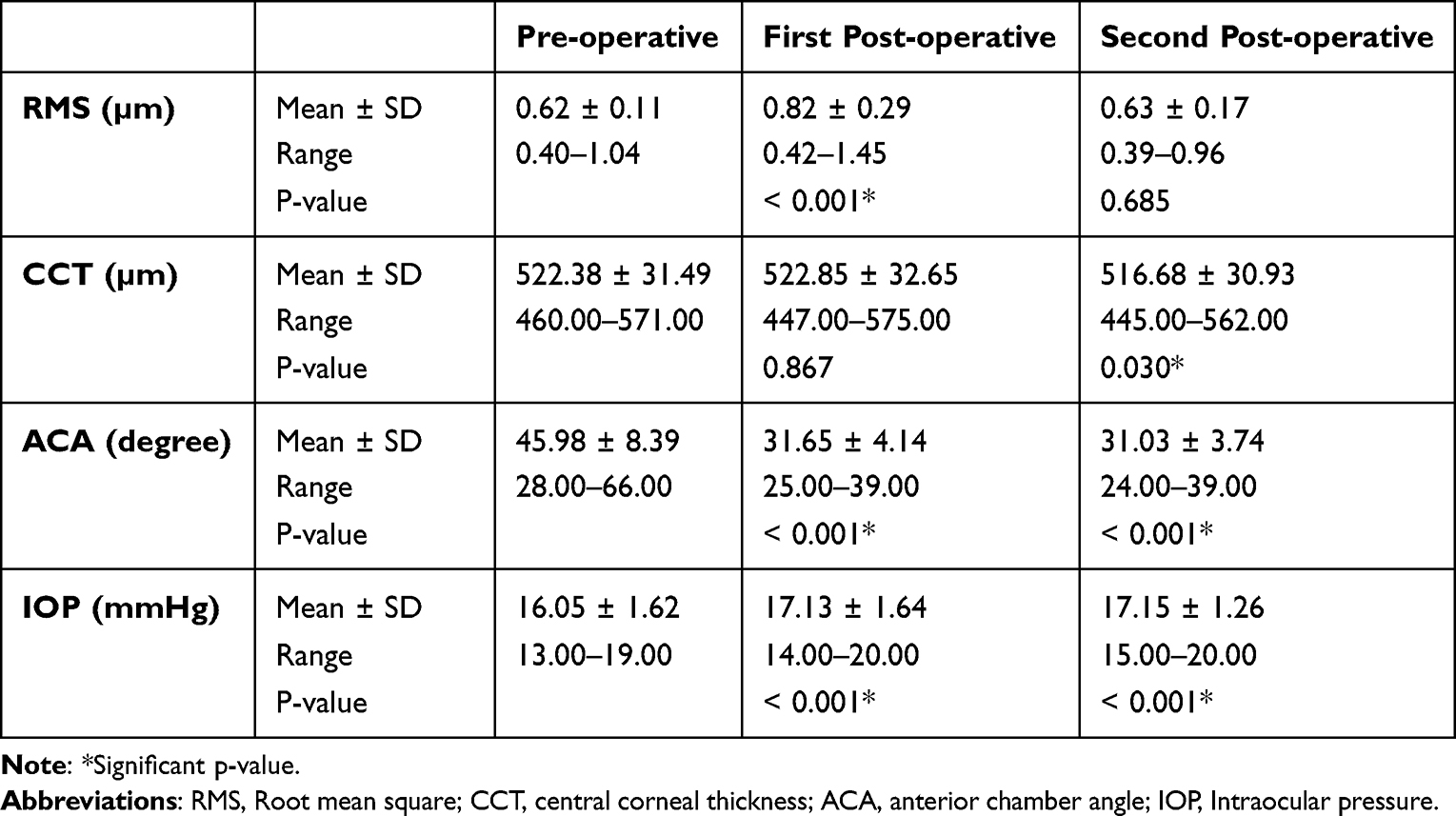 |
Table 2 Comparison of Scheimpflug Imaging Data and Intraocular Pressure Between the Pre-operative and Post-operative Follow Up |
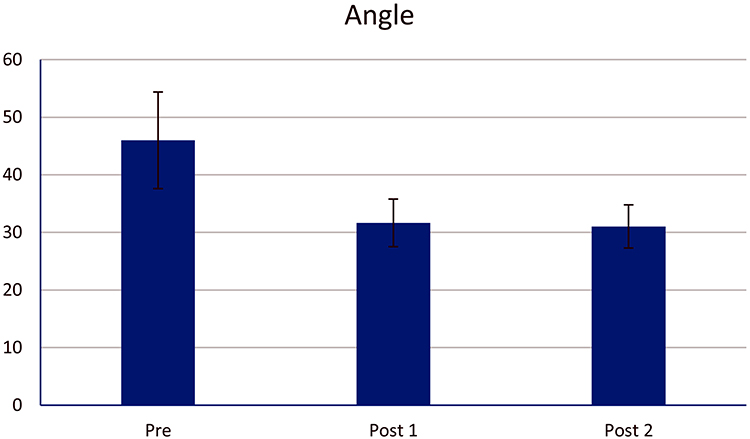 |
Figure 4 The pre-operative and post-operative anterior chamber angle (ACA) at 1st and 2nd follow up. |
When comparing the first and second post-operative follow up, there were statistically significant difference in K2, RMS and CCT (p-value 0.039, < 0.001, < 0.001 respectively) (Table 3).
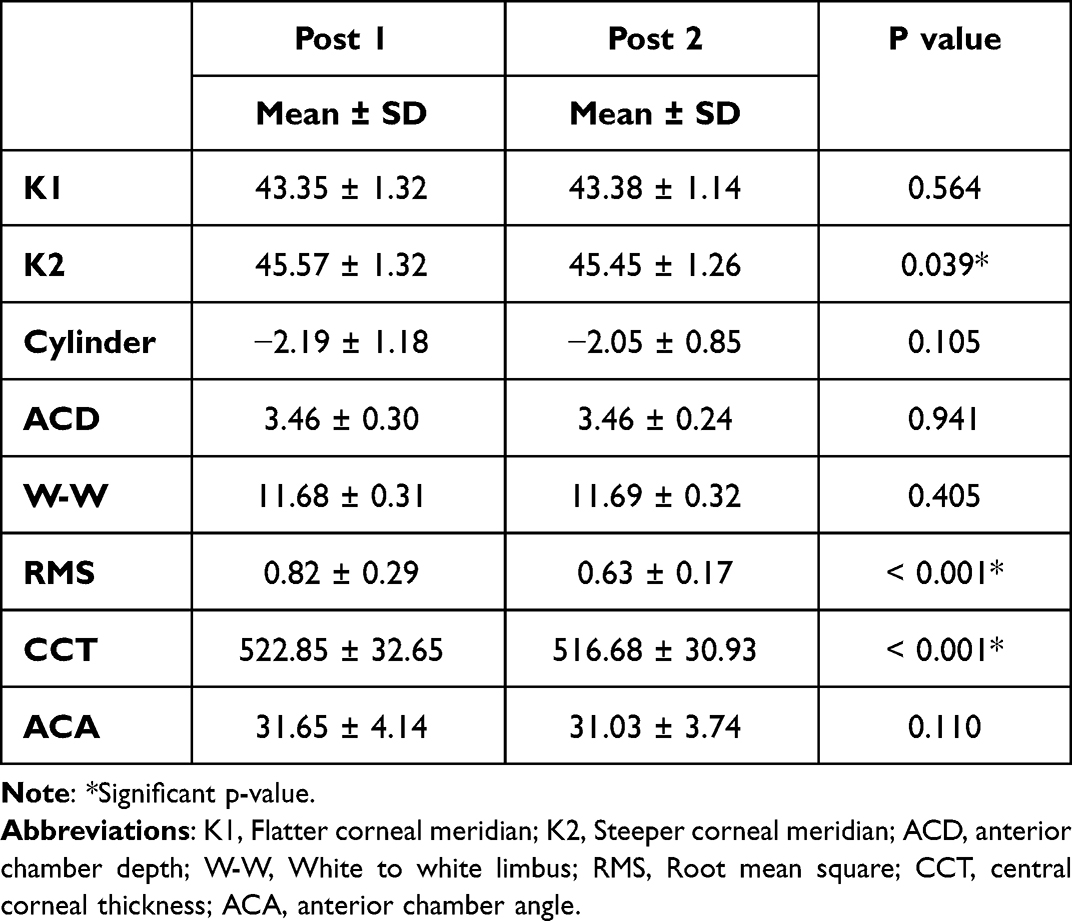 |
Table 3 Comparison of Different Parameters Between the Pre-operative and Post-operative Follow Up |
Correlation of Various Parameters
By Pearson correlation of the pre-operative parameters, there were statistically insignificant correlations between RMS with BCVA, K1, K2 and cylinder. On the other hand, there were statistically significant positive correlation between ACD and angle (r = 0.437, p = 0.005) and statistically significant negative correlation between ACD and IOP (r = −0.437, p = 0.005). There was insignificant positive correlation between ACD and CCT.
In the post-operative follow up, there were statistically insignificant correlations between RMS with BCVA, K1 and K2 at the 1st and 3rd month post-operatively. However, the correlation between RMS and cylinder at the 1st month was significant negative correlation (r = −0.317, p = 0.046). The correlations between RMS and BCVA, K1, K2 and cylinder are shown in (Table 4).
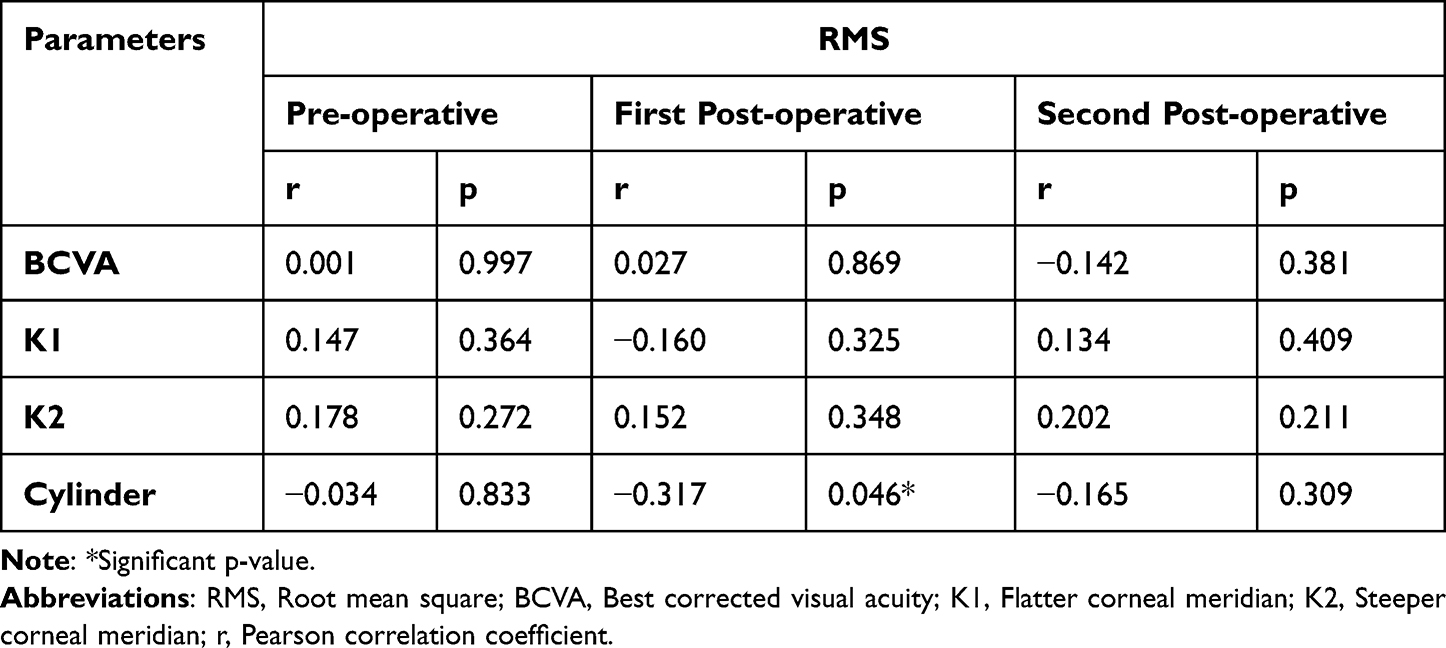 |
Table 4 Correlation Between the Root Mean Square with the Best Corrected Visual Acuity, K1, K2 and Cylinder |
The correlation between ACD with the ACA and CCT at the 1st and 3rd months post-operatively was statistically insignificant positive correlation (Figure 5). However, there was statistically significant negative correlation between ACD and IOP at the 1st month post-operatively(r = −0.426, p = 0.008) (Table 5).
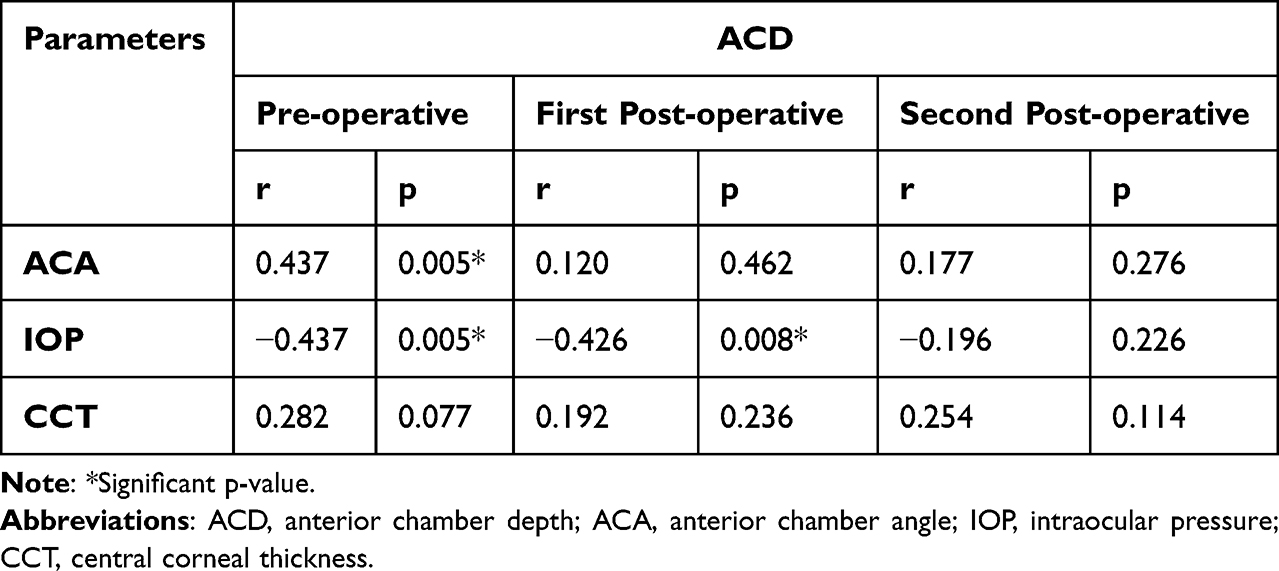 |
Table 5 Correlation Between the Anterior Chamber Depth with the Anterior Chamber Angle, Intraocular Pressure and Central Corneal Thickness |
 |
Figure 5 (A and B) Graphs showing the correlation between ACD and ACA at 1st and 2nd follow up. |
Discussion
ICL implantation is an acceptable option for moderate and high myopic correction. It is superior to corneal refractive surgery, as it preserves the shape and anatomical structure of the cornea. It is also safer than clear lens extraction (CLE), as CLE may cause complications such as loss of accommodation, retinal breaks and retinal detachment. However, evaluation of HOAs plays valuable role in visual quality and refractive outcome. Changes of total HOAs should be taken in consideration for the patient satisfaction.10,11
In our study, we evaluated the effect of V4C; STAAR Surgical ICL implantation on the total HOAs. We found significant increase in HOAs at the 1st month post-operatively. This may be due to the corneal incision before complete healing of the wound. This might affect the corneal morphology, consequently increased corneal aberrations. The post-operative induced total HOAs were presumed to be caused by corneal incision induced irregular cylinder, healing process of the corneal wound, and tear film irregularities at 1st month early post-operatively. This tear film instability might lead to rough corneal surface. Nevertheless, increase of negative spherical aberrations might happen due to ICL special structure.
However, we found significant decrease in HOAs at the 3rd month as compared to the 1st month post-operatively. Several factors may explain this finding. The spherical aberrations resulted from different focusing rays of the peripheral and central parts of the lens could be adjusted by the phakic IOL so, the summation of different rays was zero. Also, correction of the low order aberrations might result in improvement of HOAs. Moreover, ICL implantation did not affect the morphological structure of the cornea which remained intact. On the other hand, all corneal refractive surgeries such as small incision lenticule extraction (SMILE) may cause morphological changes in the cornea, which may lead to changes in HOAs.12
In a study done by Hashemian et al, they did not find significant changes in HOAs in ICL and TICL for correcting myopic astigmatism, although the spherical aberrations increased.13 In contrast to a study done by Kayhan et al, they found significant changes in HOAs, coma and trefoil in entire and internal elements. These might be related to ICL design or its positioning.14 Comparative study was done by Fu et al, to compare HOAs between ICL and SMILE. They did not find any correlation between HOAs and visual complaints in both groups. They reported comparable safety and prognosis of both modalities on the visual outcome.15
In this study, we found significant decrease in the ACD, which was accurately measured from the corneal endothelium to the anterior surface of the ICL. Moreover, the vault was the distance between the back surface of the ICL and the anterior surface of the natural lens.16 This decrease in the ACD was explained by vaulting of the ICL, which was due to increase in convexity of the lens. This vaulting was maximal in the early post-operative period which might relatively improve after longer follow up. In addition, there was significant decrease in the ACA. This was due to pushing of the iris lens diaphragm forward by ICL vaulting. The P- values for ACD and ACA were (P- value < 0.001, < 0.001) respectively at the 1st and 3rd month post-operatively.
Fernandez-Vigo et al, found that the narrowing of the ACA remained stable at 3 months post-operatively. In a study done by Singh et al, they found significant narrowing of ACA with a negative correlation pre-operative ACD and IOP.17,18
Some studies have evaluated the IOP after ICL implantation. In contrast to our results, a study done by Niu et al, reported that ICL V4c implantation in patients with high myopia and shallow ACD had stable visual outcomes without significant increase in IOP.19 Also, Lin et al, found that anterior segment parameters became stable with average IOP early after surgery.20 However, Zhang et al, found that increased IOP and secondary glaucoma could occur after ICL implantation but with lower incidence in central hole ICL.21
On the other hand, the cylinder significantly increased due to coincident corneal incision, which was not done in the steep corneal meridian. This reason also explained the significant increase in K 2 (P- value < 0.001, < 0.001) respectively. A study done by Alonso-Juarez & Villoria found that low diopter toric implantable collamer lens (TICL) was suitable for low degree of astigmatism.22
Moreover, there was significant increase in IOP post-operatively (P- value < 0.001) due to significant decrease in the ACD and ACV. In a study done by Senthil et al, they reported the presence of ocular hypertension and secondary glaucoma after ICL implantation, which might be due to open angle or angle closure glaucoma.23 In contrast to a study done by Arguello et al, they found that IOP fluctuations were not statistically significant after ICL implantation.24
As regards the correlations, there was a significant negative correlation between RMS of the total HOAs and cylinder at the 1st month. This correlation might be explained by the presence of other variants affecting RMS, which were tear film irregularities at the 1st month post-operatively. Also, the healing process of the corneal incision might affect RMS. This coincides with our finding at the 3rd month, with non-significant correlation between RMS and cylinder due to resolving of the two previously mentioned variants.
Also, there was statistically significant negative correlation between ACD and IOP pre-operatively (r= −0.437, p= 0.005) and at the 1st month post-operatively(r = −0.426, p = 0.008). We found that as ACD decreased, the IOP increased. This was due to significant decrease in ACA. Another cause of increase in IOP was vaulting of the ICL in front of the pupil and decreasing the drainage.
In our study, we concluded that HOAs may not be necessarily measured before ICL implantation, in contrast to corneal refractive surgery, as it has no effect on HOAs by the 3rd month post-operatively.
We also recommend that patients after ICL implantation need longer follow up and further evaluation for possibility for increase in IOP post-operatively. In addition, patients with primary open angle glaucoma (POAG), which is relatively common in high myopia, are at high risk of increased IOP. The meticulous follow up of IOP is important in the early post-operative period in these patients and control of IOP if it is high.
The main strength of our study is the association between the functional outcome, visual quality and the anatomical anterior segment parameters, including the correlation between various parameters, BCVA and refraction.
The limitation of this study is the small sample size. We did not evaluate the TICL for correction of myopic astigmatism. In addition, corneal incision in the steep meridian should be taken into consideration to decrease the post-operative astigmatism. Also, one of our limitations was that we did not evaluate the vault measurement. We need future studies of larger sample size, including correction of both myopia and astigmatism.
Conclusion
ICL implantation is safe and predictable in correction of highly myopic patients. The final quality of vision post-operatively is not affected by the early induced HOAs, as the HOAs increase at first month post-operatively then, return to the pre-operative level by 3rd month. However, the significant decrease in the ACD and ACA and significant increase of IOP may need longer follow up of these patients.
Data Sharing Statement
All data of the study are available by the corresponding author on a reasonable request.
Ethical Approval
This study was approved by the Institutional Review Board and Ethics Committee of the Faculty of Medicine, Cairo University by Ethics Committee Code N-90-2022.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kamiya K, Shimizu K, Igarashi A, et al. Posterior chamber phakic intraocular lens implantation: comparative, multicenter study in 351 eyes with low to moderate myopia. Br J Ophthalmol. 2018;102:177–181. doi:10.1136/bjophthalmol-2017-310164
2. Alfonso J, Cueto L, Bartolozzi B, Montes R, Fermandez L. Five year follow up of correction of high myopia: posterior chamber phakic intraocular lens with a central hole design. J Refract Surg. 2019;35(3):169–176. doi:10.3928/1081597X-20190118-01
3. Lee H, Kang D, Choi J, et al. Analysis of preoperative factors affecting range of optimal vaulting after implantation of 12.6-mm V4C implantable collamer lens in myopic eyes. BMC Ophthalmol. 2018;18:163. doi:10.1186/s12886-018-0835-x
4. Wei R, Li M, Zhang H, et al. Comparison of objective and subjective visual quality early after implantable collamer lens V4C and small incision lenticule extraction (SMILE) for high myopia correction. Acta Ophthalmol. 2020;98(8):943–950. doi:10.1111/aos.14459
5. Aruma A, Li M, Choi J, et al. Visual outcomes after small incision lenticule extraction and implantable collamer lens V4C for moderate myopia: 1- year results. Graefes Arch Clin Exp Ophthalmol. 2021;259:2431–2440. doi:10.1007/s00417-020-04982-4
6. Eom Y, Kim D, Ryu D, et al. Ring-shaped dysphotopsia associated with posterior chamber phakic implantable collamer lenses with a central hole. Acta Ophthalmol. 2017;95:170–178. doi:10.1111/aos.13248
7. Nakamura T, Isogai N, Kojima T, Yoshida Y, Sugiyama Y. Implantable collamer lens sizing method based on swept-source anterior segment optical coherence tomography. Am J Ophthalmol. 2018;187:99–107. doi:10.1016/j.ajo.2017.12.015
8. Garcia G, Payne A, Ojeda J, et al. Anterior segment optical coherence tomography angle and vault analysis after toric and non-toric Implantable Collamer Lens V4C implantation in patients with high myopia. Br J Ophthalmol. 2018;102:544–548. doi:10.1136/bjophthalmol-2017-310518
9. Almalki S, Abubaker A, Alsabaani N, Edward D. Causes of elevated intraocular pressure following implantation of phakic intraocular lenses for myopia. Int Ophthalmol. 2016;36:259–265. doi:10.1007/s10792-015-0112-4
10. Kobashi H, Kamiya K, Igarashi A, Matsumura K, Komatsu M, Shimizu K. Long-term quality of life after posterior chamber phakic intraocular lens implantation and after wavefront-guided laser in situ keratomileusis for myopia. J Cataract Refract Surg. 2014;40(12):2019–2024. doi:10.1016/j.jcrs.2014.03.028
11. Domínguez-Vicent A, Ferrer-Blasco T, Pérez-Vives C, Esteve-Taboada J, Montés-Micó R. Optical quality comparison between 2 collagen copolymer posterior chamber phakic intraocular lens designs. J Cataract Refract Surg. 2015;41(6):1268–1278. doi:10.1016/j.jcrs.2014.09.050
12. Chen X, Wang Y, Zhang J, Yang S, Li X, Zhang L. Comparison of ocular higher-order aberrations after SMILE and Wavefront-guided Femtosecond LASIK for myopia. BMC Ophthalmol. 2017;17:42. doi:10.1186/s12886-017-0431-5
13. Hashemian S, Farrokhi H, Foroutan A, et al. Ocular higher-order aberrations changes after implantable collamer lens implantation for high myopic astigmatism. J Curr Ophthalmol. 2017;30(2):136–141. doi:10.1016/j.joco.2017.10.002
14. Kayhan B, Coskunseven E, Sahin O, Pallikaris I. The effects of implantable collamer lens implantation on higher order aberrations. Int J Ophthalmol. 2019;12(12):1848–1852. doi:10.18240/ijo.2019.12.05
15. Fu M, Li M, Xian Y, et al. Two-Year Visual Outcomes of Evolution Implantable Collamer Lens and Small Incision Lenticule Extraction for the Correction of Low Myopia. Front Med. 2022;9:780000. doi:10.3389/fmed.2022.780000
16. Almorín-Fernández-Vigo I, Guillén I, Fernández-Vigo JI, et al. Agreement between optical coherence and Scheimpflug tomography: vault measurements and reproducibility after implantable collamer lens implantation. J Fr Ophtalmol. 2021;44(9):1370–1380. doi:10.1016/j.jfo.2021.03.007
17. Fernández-Vigo J, Macarro-Merino A, Fernández-Vigo C, et al. Effects of Implantable Collamer Lens V4c Placement on Iridocorneal Angle Measurements by Fourier-Domain Optical Coherence Tomography. Am J Ophthalmol. 2016;162:43–52. doi:10.1016/j.ajo.2015.11.010
18. Singh R, Vanathi M, Kishore A, Tandon R, Singh D. An anterior segment optical coherence tomography study of the anterior chamber angle after implantable collamer lens-V4c implantation in Asian Indian Eyes. Indian J Ophthalmol. 2020;68(7):1418–1423. doi:10.4103/ijo.IJO_1540_19
19. Niu L, Miao H, Han T, et al. Visual outcomes of Visian ICL implantation for high myopia in patients with shallow anterior chamber depth. BMC Ophthalmol. 2019;19:121. doi:10.1186/s12886-019-1132-z
20. Lin Q, Yang D, Zhou X. Early outcomes of anterior segment parameters after implantable collamer lens V4c implantation. BMC Ophthalmol. 2022;22:429. doi:10.1186/s12886-022-02656-9
21. Zhang H, Gong R, Zhang X, Deng Y. Analysis of perioperative problems related to intraocular Implantable Collamer Lens (ICL) implantation. Int Ophthalmol. 2022;42(11):3625–3641. doi:10.1007/s10792-022-02355-w
22. Alonso-Juárez E, Velázquez-Villoria D. Low Diopter Phakic Implantable Collamer Lens: refractive and Visual Outcomes in Low Myopia and Myopic Astigmatism. Clin Ophthalmol. 2022;16:2969–2977. doi:10.2147/OPTH.S373378
23. Senthil S, Choudhari NS, Vaddavalli PK, Murthy S, Reddy JC, Garudadri CS. Etiology and Management of Raised Intraocular Pressure following Posterior Chamber Phakic Intraocular Lens Implantation in Myopic Eyes. PLoS One. 2016;17:e0165469. doi:10.1371/journal.pone.0165469
24. Argüello J, Portillo H, Vergara M, et al. Intraocular pressure fluctuations in patients implanted with an implantable collamer lens (ICL V4c). Three-month follow-up. Arch Soc Esp Oftalmol. 2019;94(8):367–376. doi:10.1016/j.oftal.2019.05.010
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.