")
Back to Journals » Clinical Ophthalmology » Volume 17
Evaluation of Foveal Avascular Zone After Strabismic and Anisometropic Amblyopia Therapy in Saudi Children Using Optic Coherence Tomography Angiography: A Cohort Study
Authors Sesma G , Al Mairi T , Khashoggi HF, AlDhahi SI, Aljohar F, Khandekar R , Awad A
Received 8 September 2023
Accepted for publication 5 December 2023
Published 8 December 2023 Volume 2023:17 Pages 3775—3784
DOI https://doi.org/10.2147/OPTH.S435252
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Gorka Sesma,1 Tasnim Al Mairi,2 Heba Fareed Khashoggi,1 Shorog Ibrahim AlDhahi,1 Fahad Aljohar,3 Rajiv Khandekar,4 Abdulaziz Awad1
1Pediatric Ophthalmology and Strabismus Division, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia; 2Emergency Department, Almoosa Specialist Hospital, Al Mubarraz, Saudi Arabia; 3Diagnostic and Imaging Department, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia; 4Department of Vision Science, University of British Columbia, Vancouver, Canada
Correspondence: Gorka Sesma, Pediatric Ophthalmology and Strabismus Division, King Khaled Eye Specialist Hospital, Al Urubah Branche Road, West Building 2nd Floor, Riyadh, 11462, Saudi Arabia, Tel +966 11 4849700, Fax +966 11 4821908, Email [email protected]
Purpose: Optical coherence tomography angiography (OCTA) noninvasively images retinal microvasculature. Foveal avascular zone (FAZ) biomarkers can act as indicators of various forms of amblyopia, making them valuable tools for clinicians. The purpose of this study was to assess the effect of amblyopia therapy on the FAZ using OCTA to determine FAZ size in children with untreated amblyopia.
Patients and Methods: This two-arm cohort study enrolled 23 children with untreated strabismic or anisometropic amblyopia who underwent OCTA between 2021– 2022. Each arm had 23 eyes, with one arm having amblyopic eyes and the other having normal eyes. FAZ area, perimeter, and circularity index were measured before and quarterly during 1 year of occlusion therapy. Differences in avascular zone biomarkers between amblyopic and fellow eyes were compared and linked to demographic and ocular factors.
Results: Similar FAZ areas were found in the amblyopic (0.3 mm2) and nonamblyopic eyes (0.28 mm2) (P = 0.83), with no significant change in either group (P = 0.93). Amblyopic eyes showed a larger FAZ perimeter reduction (0.12 mm2) than fellow eyes (0.02 mm2), but the difference was not statistically significant (P = 0.09). The circularity index in amblyopic eyes matched with fellow eyes (0.67 mm2), P = 0.38. Initial visual acuity and strabismus correlated with changes in the follow-up FAZ area.
Conclusion: Amblyopia treatment did not significantly alter FAZ area in this cohort. Perimeter variations between amblyopic and fellow eyes require further study. The conclusions were limited by the sample size and lack of randomization.
Plain Language Summary: Amblyopia is a common vision problem in children in which one eye does not see the fellow eye. This can occur if the eyes are not lined up right or if their prescriptions are different. Amblyopia is treated by placing a patch over the stronger eye to help the weaker eye better see.
Researchers have used a technique called optical coherence tomography angiography (OCTA) to compare the foveal avascular zone (FAZ) before and after treatment in children with amblyopia. The FAZ is a spot on the back of the eye where there are no blood vessels or light-sensitive cells. Changes in the FAZ may indicate the severity of amblyopia.
The study included 23 children with untreated amblyopia. Over the course of more than a year, measurements of FAZ area, perimeter, and roundness were taken before and during occlusion therapy. The size of the FAZ was also compared between the eyes with and without amblyopia.
At the start of the study and after treatment, there were no significant differences between the FAZs of amblyopic eyes and other eyes. There were some differences in the size of the FAZ between eyes. Changes in the FAZ area were linked to the initial state of vision and misalignment.
Overall, this study found that occlusion therapy did not change FAZ area in children with amblyopia. More research is needed to determine why the FAZ perimeter can differ between the eyes. Larger randomized studies would provide more information about how the FAZ changes when treating amblyopia.
Keywords: amblyopia, optical coherence tomography angiography, foveal avascular zone, occlusion therapy, biomarkers
Introduction
Optical coherence tomography angiography (OCTA) is a noninvasive technique used to image the microvasculature of the retina and choroid. It has been widely used since its introduction in 2014,1 and has been used to assess and monitor the effectiveness of interventions for multiple ocular conditions, including diabetic retinopathy, glaucoma, age-related macular degeneration, macular dystrophies, retinitis pigmentosa, central serous chorioretinopathy, uveitis, optic neuropathies, and amblyopia.2 It is also helpful to guide healthcare professionals in the management of patients with systemic diseases, such as diabetes, hypertension, Alzheimer’s disease, and multiple sclerosis.3 Up to 20 different OCTA parameters have been used to study microvascular changes in the retina and choroid in ocular and systemic diseases. The foveal avascular zone (FAZ) is a prominent feature.4 The foveal avascular zone (FAZ) is an area of the fovea where OCTA does not reveal blood vessels in healthy normal eyes. It consists of a superficial FAZ at the superficial level and a deep FAZ at the deep level of the retina.5 For the quantitative analysis of the OCTA metrics and the study of the structural and vascular status of the macula, the area, perimeter and circularity index of FAZ are software-generated biomarkers built into OCTA machines.6 Kim et al reported a mean (± standard deviation) FAZ area of 0.329 ± 0.115 millimeters square (mm2), mean perimeter length of 2.279 ± 0.418 millimeters (mm), and FAZ shape of 0.769 ± 0.064 mm in normal healthy individuals.7
Amblyopia is a leading ailment of visual disabilities that cause morbidity.
The impact of the macular FAZ on amblyopia is poorly understood. Various FAZ-related biomarkers have been used to conduct comparative analyses between amblyopic and nonamblyopic fellow eyes. While some studies have reported inconclusive results regarding the differences in the foveal anterior zone (FAZ) between amblyopic and fellow eyes, other studies have found no such differences.8,9 For example, Nourinia et al reported a larger FAZ in amblyopic eyes compared to unaffected eyes,10 while Yilmaz et al noted a smaller FAZ in amblyopia versus fellow eyes.11 Additionally, a study on Chinese children found that the perfusion parameters of the superficial retinal layer, such as the FAZ area, perimeter, and circularity, were significantly higher in amblyopic eyes compared to fellow eyes with anisometropic amblyopia.11 Given the divergent results of previous studies, our research aimed to fill the existing gap in the literature by examining the changes in the foveal area zone (FAZ) associated with unilateral amblyopia and its treatment, and providing a more definitive understanding of the issue.
Another important factor to consider is correcting magnification errors in both the amblyopic and nonamblyopic eyes before interpreting the results of FAZ.12 Therefore, further investigation is necessary to validate the discrepancies in FAZ-related biomarkers between the amblyopic and nonamblyopic eyes.
Few studies have used OCTA-generated biomarkers to track the efficacy of amblyopia treatment. Gunzenhauser et al studied 12 children with unilateral amblyopia were studied by Gunzenhauser et al,13 and it was found that after a four-month period of amblyopia therapy, the retinal vascular density in the deep capillary plexus of the macula increased. A study of 33 amblyopic children in China revealed that the area and circularity of the FAZ decreased after six months of amblyopia therapy, and the latter was well correlated with an improvement in visual acuity in treated eyes.14
To our knowledge, OCTA-generated FAZ biomarkers, such as FAZ area, perimeter, and circularity, have not been used to monitor the effects of different types and severity levels of amblyopia therapy. Given this gap, we formulated the following research question: How do FAZ biomarkers (area, perimeter, and circularity) generated by OCTA change after amblyopia therapy in children with unilateral strabismic or anisometropic amblyopia? We hypothesized that the OCTA-derived FAZ area, perimeter, and circularity would remain unchanged in amblyopic eyes following amblyopia treatment.
We present the OCTA-generated area, perimeter, and circularity parameters of the FAZ at baseline and after amblyopia treatment as well as the determinants of the changes observed in the amblyopic and fellow eyes of Saudi children with strabismic and/or anisometropic unilateral amblyopia. Leveraging OCTA biomarkers to examine FAZ alterations provides novel information on pediatric amblyopia and response to treatment. This study offers a new perspective on this common pediatric eye condition and its treatment effects.
Materials and Methods
This study was reviewed and approved by the Institutional Research Board of the King Khaled Eye Specialist Hospital (20139-P). The tenants of the Declaration of Helsinki strictly adhered to the study protocol, and followed the principles and applicable guidelines for the protection of human subjects in biomedical research. Parents of the children with unilateral amblyopia provided written informed consent to participate in this study.
We recruited patients with unilateral strabismic or anisometropic amblyopia who had not received prior treatment. Amblyopic patients started unilateral occlusion therapy based on best corrected visual acuity obtained following the amblyopia treatment study group criteria.15
Patients were followed up every three months over a one-year period between January 2021 and January 2022 in the Pediatric Ophthalmology Division. A comprehensive ophthalmologic examination, including OCTA and occlusion assessment, was performed at each of the four quarterly visits. The exclusion criteria were lack of patching compliance, parental refusal of OCTA, bilateral amblyopia, deprivation amblyopia, prematurity, systemic diseases, eccentric fixation, and ophthalmic conditions other than strabismus.
In this prospective two-armed cohort study, the participants’ eyes were divided into two arms: amblyopic eyes (Gr-1) and fellow nonamblyopic eyes (Gr-2). To achieve a 95% confidence interval and 80% power with a 1:1 ratio of Gr-1 to Gr-2, a sample size of 23 amblyopic eyes was required at baseline and after treatment based on calculations using Open Epi software for a mean difference in a cohort study.16
Macular microvascular network images within the superficial capillary plexus (SCP) layer were obtained for amblyopic and fellow eyes using spectral-domain OCTA (REVO nx, Optopol Technology, Poland). A 6×6 mm macular scan was acquired for each eye. The automated process outlined the FAZ profile and calculated its area and circularity by using a built-in analytical algorithm. The device uses a software program that employs a series of automated image-processing steps to identify and quantify the foveal avascular zone (FAZ). The specific algorithm used is not publicly disclosed; however, it has been validated and operates as follows.
High-resolution OCTA images depicting depth-resolved retinal vasculature were acquired using an OCTA instrument. Advanced segmentation techniques then isolate the retinal layers and distinguish blood vessels from the surrounding tissue. The algorithm then detects and delineates the borders of the FAZ, identifying the central avascular area of the macula that lacks perfused capillaries. With the FAZ outlined, the software measures the number of pixels within the defined region and converts this into a physical area in units such as square millimeters. Additionally, the circularity of the FAZ was calculated by analyzing its shape contours. Through this automated sequence, the proprietary algorithm developed by the company enabled reliable and validated quantification of clinically relevant FAZ metrics (Figure 1). Although the specific details of their software are proprietary, the general workflow demonstrates an optimized approach for precise FAZ analysis.
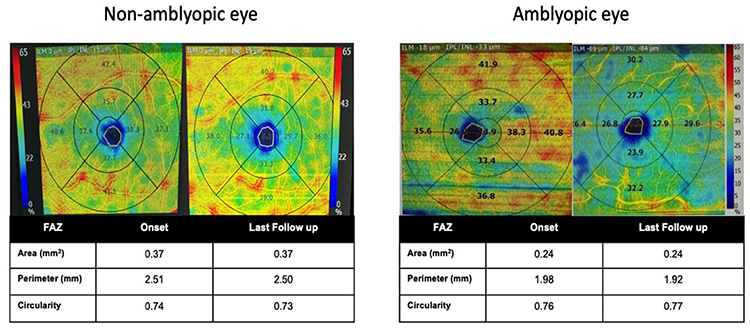 |
Figure 1 Foveal Avascular Zone (FAZ) Parameters in Amblyopic and Nonamblyopic Eyes at Study Onset and Final Follow-Up. The presented graph depicts the FAZ area (in mm2), perimeter (in mm), and circularity in the amblyopic eye in comparison with the nonamblyopic fellow eye at the beginning and conclusion of the study. It is noteworthy that no significant discrepancies were detected between the amblyopic and nonamblyopic eyes in terms of the FAZ parameters at either time point. However, minor reductions in the FAZ perimeter were observed in the amblyopic eye throughout the study. |
The SCP layer is a thin layer of tissue that lies between the internal limiting membrane and outer border of the inner plexiform layer in the eye. The ratio of the perimeter of the FAZ to that of a circle with an equal area, which ranges from 0 to 1, was used to determine the circularity of the FAZ. A value closer to 1 indicated a more regular circular shape. We assumed that the circularity of the FAZ at baseline was 0.7 ± 0.1 in the eye with amblyopia, and four months after amblyopia treatment, it was 0.8 ± 0.12, as reported by Huang et al.14 We ensured high-quality scan with an experienced technician trained by the OCTA company. The built-in software automatically rejected scans if the artifacts affected the interpretation of the scan results. The FAZ area was measured and corrected for the magnification factor due to variations in axial length using the formula:  .17
.17
We collected demographic variables such as age, sex, and eyes with amblyopia. We evaluated the refractive status using cycloplegic refraction and, based on spherical equivalent values, classified them as myopic, emmetropic, or hyperopic. If the spherical equivalent of one eye was ± 1 diopters different from that of the other eye, we termed it anisometropia. Visual acuity was measured using the LogMAR scale. We categorized the amblyopia grades as “mild”, “moderate”, “and” severe based on visual acuity between 0.20 to 0.30, 0.30 to 0.70, and less than 0.70, respectively. We also classified and grouped the causes of amblyopia, including strabismus and anisometropia.
The primary outcome was the discrepancy in the area, perimeter, and circularity of the FAZ at the final follow-up after amblyopia therapy in comparison with the baseline in amblyopic eyes and fellow eyes.
Data were collected using a pre-tested data collection form and then transferred to the Statistical Package for Social Studies (SPSS 25) spreadsheet, which was developed by IBM (NY, USA). Qualitative data are presented as numbers and percentages. Quantitative variables, if normally distributed, are presented as means and standard deviations. Variables that were not normally distributed or of small sample sizes are presented as medians and interquartile ranges. Matched-pair analysis was used to validate the comparison between amblyopic and fellow eyes for normally distributed outcome variables. Nonparametric analysis was used to validate comparisons based on the Wilcoxon signed-rank test p-value, and statistical significance was established at P < 0.05. Differences in FAZ area, perimeter, and circularity in the amblyopic eye at the last follow-up and baseline were correlated with different variables using univariate analysis and validated using the Spearman correlation test.
Results
We examined a total of 46 eyes. 23 amblyopic eyes from Gr-1 and 23 fellow eyes from Gr-2 were observed in 23 children. Table 1 summarizes the results of this study.
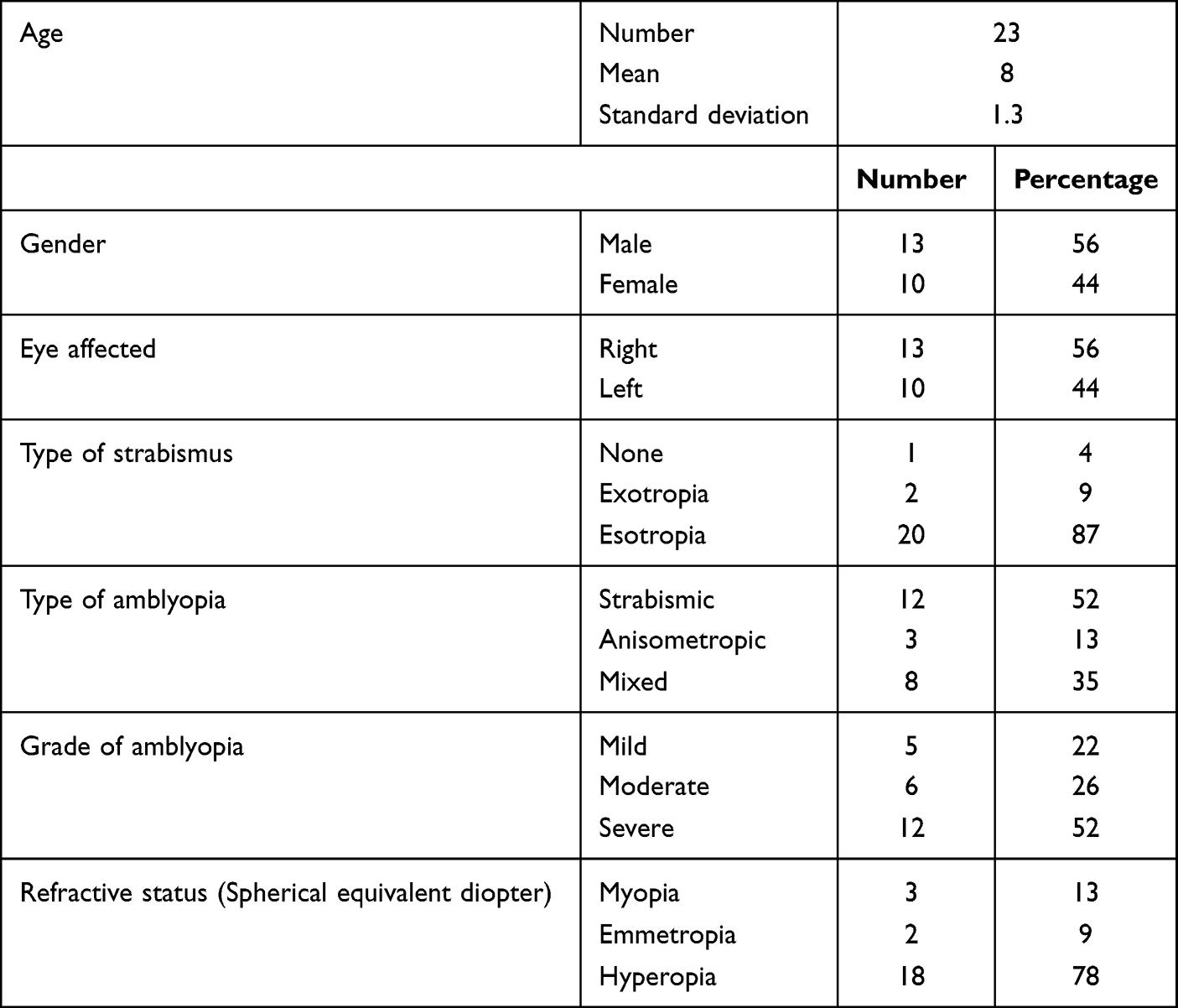 |
Table 1 Demography of Children with Unilateral Amblyopia |
In Gr-1 and Gr-2, vision improved in both eyes. Specifically, in Gr-1, vision improved from a median of 0.9 (interquartile range, 0.6–1.0) to 0.4 (IQR, 0.2–0.6), and this improvement was statistically significant (P = 0.001). In Gr-2, the median logarithmic vision improved from 0.2 (IQR, 0.1–0.2) to 0.0 (IQR, 0.0–0.1). The improvement in logMAR vision was also statistically significant in Gr-2 (P = 0.001). The median duration of the last follow-up was 12 months (IQR, 11–14 months) after amblyopia therapy.
Spearman test results indicated that there were no statistically significant differences in the area, perimeter, and circularity measurements between the amblyopic and fellow eyes, the anisometropic and fellow eyes, and between moderate and severe amblyopic eyes at both onset and the last follow-up.
We discovered a connection between multiple starting variables and three biological markers related to FAZ. A strong correlation was found between changes in the FAZ area (as shown in Table 2) and esotropia (P = 0.046). On the other hand, we found that starting visual acuity was inversely correlated with changes in the FAZ area (P = 0.02).
 |
Table 2 Correlation Between Changes in FAZ-Related Biomarkers in Amblyopic Eyes of Saudi Children and Different Pretreatment Parameters |
Table 3 shows the biomarkers related to FAZ in Gr-1 and Gr-2 at baseline and different follow-up periods. At the third visit after amblyopia therapy, the circularity index of the FAZ in Gr-1 was significantly higher than that in Gr-2 (P = 0.01). The other indices did not differ significantly between the groups.
 |
Table 3 Comparison of Biomarkers Related to the Foveal Avascular Zone by Optical Coherence Tomography Angiography in Gr-1 and Gr-2 of Saudi Children with Unilateral Amblyopia |
We analyzed the changes in biomarkers in patients from Gr-1 and Gr-2 at their fourth visit compared to their first visit. As shown in Figure 2, the median FAZ areas in Gr-1 (0.3 mm2) and Gr-2 (0.28 mm2) were similar (P = 0.83). No significant change in FAZ area was observed in either group (P = 0.93) after 1 year of amblyopia treatment. Gr-1 showed a larger median FAZ perimeter reduction (0.12 mm2) than Gr-2 (0.02 mm2), but this difference was not statistically significant (P = 0.09). The median circularity index in Gr-1 matched with Gr-2 at onset and at the last follow-up (0.67 mm2), without changes during the duration of the study (P = 0.38).
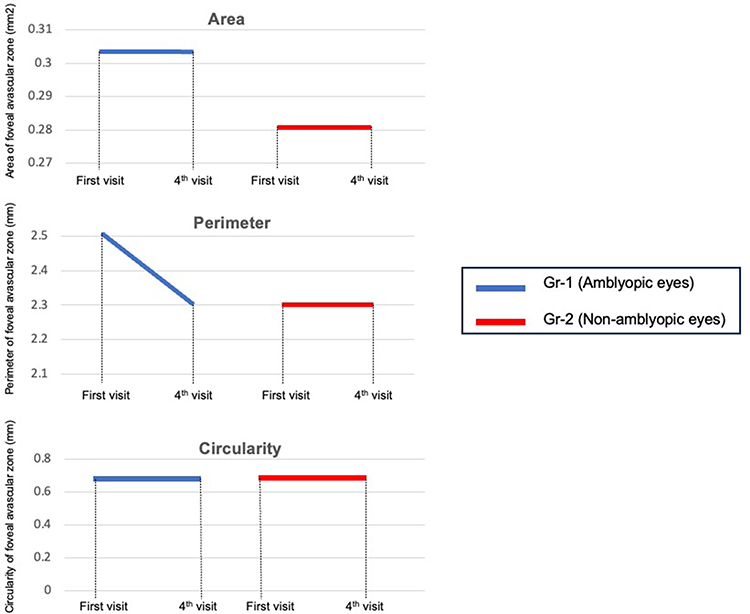 |
Figure 2 Changes in Foveal Avascular Zone (FAZ) Biomarkers in Amblyopic (Gr-1) and Nonamblyopic (Gr-2) Eyes. This line chart illustrates the variations in the median values of avascular, perimetric, and circular areas in the Gr-1 (amblyopic) and Gr-2 (nonamblyopic) eyes between the initial and fourth OCTA assessments. The X-axis represents different assessment visits, categorized as Gr-1 or Gr-2, while the Y-axis represents the area of the foveal avascular zone (in square millimeters), perimeter (in millimeters), and circularity (in millimeters). The red line denotes the median FAZ biomarkers in the amblyopic eyes, whereas the blue line represents the same parameters in nonamblyopic eyes. |
Discussion
Although there was an improvement in visual acuity, biomarkers related to FAZ did not show significant improvement in Saudi children following amblyopia therapy. The difference in FAZ area and circularity at the macula between the two groups (Gr-1 and Gr-2) was not significant, and the perimeter reduction of the FAZ was greater in Gr-1 than in Gr-2, but the difference was not statistically significant (P = 0.09). Strabismus and visual acuity before therapy were significantly correlated with changes in the FAZ area at the last follow-up in amblyopic eyes.
The disparity in functional and vascular changes in the macular area of the amblyopic eye observed in our study after one year of therapy suggests that vision improvement may not occur in the macula but rather in the higher visual centers. The improvement in vision in amblyopic eyes did not appear to have any effect on the vascularity of the fovea. This may be the longest observed impact of amblyopia therapy on the levels of FAZ-related biomarkers, lasting for a median of one year.
Our study discovered both similarities and discrepancies with prior research on foveal avascular zone (FAZ) variations following amblyopia treatment. Our results are consistent with those of Huang et al, who investigated 51 eyes with anisometropic amblyopia and observed no significant change in FAZ area 6 months after therapy (P = 0.29). However, the circularity index of the FAZ did increase significantly following treatment (P < 0.001).15 Similarly, Zhang et al found a 3.36% lower vascular density in the macula of the recovering amblyopia group compared to controls (P = 0.55), but this difference was not statistically significant.12
However, our research conflicts with those of Nourinia et al and Yilmaz et al, who reported enlarged and reduced FAZ areas in amblyopic and fellow eyes, respectively.10,11 These disparities underscore the need for additional controlled studies with adequate sample sizes to clarify the influence of amblyopia and its treatment on FAZ morphology and metrics derived from optical coherence tomographic angiography.
Our investigation revealed that the impact of amblyopia therapy on FAZ area, perimeter, and circularity indices was not significant during the final year of follow-up. Huang et al14 studied 51 eyes with anisometric amblyopia to evaluate the biomarkers of FAZ six months after therapy. The adjustment in the FAZ area following treatment was not significant (P = 0.29). The circularity of FAZ in amblyopic eyes grew significantly after treatment from 0.71 (IQR 0.60–0.80) to 0.80 (IQR 0.76–0.83) after treatment (P < 0.001). The circularity of the foveal avascular zone (FAZ) on OCTA can be utilized as a measure of shape regularity, calculated as 4π × (area/perimeter^2), with a perfect circle having a circularity of 1 and irregular shapes approaching 0.18 OCTA enables noninvasive imaging of the retinal vasculature and FAZ, although the borders may not always be clear. The accuracy and reproducibility of FAZ circularity measurements are contingent upon image quality, resolution, segmentation, and quantification algorithms, and factors such as media opacities, motion artifacts, poor fixation, and segmentation errors can reduce the precision. Most studies have demonstrated good repeatability with intraclass correlation coefficients between 0.8–0.9, but variability exists between different devices and algorithms.19 The minimum change considered clinically significant or detectable above measurement variability has yet to be established, requiring further research. Compared with the FAZ area, circularity may be a more sensitive metric for detecting subtle changes in regularity. FAZ circularity can be used as a metric for shape regularity on OCTA, but the factors affecting measurement accuracy should be considered. Further standardization and validation are necessary to determine the clinically meaningful change thresholds for circularity.
Additionally, vision in the amblyopic eyes in this study also improved significantly. Zhang et al20 also investigated the effects of amblyopia therapy in 39 eyes with anisometropic amblyopia. They found that the axial length-adjusted vascular densities in the macula were 3.36% lower in the recovering amblyopia group than in the control group (P = 0.55), but the difference was not statistically significant. Given that our cohort had strabismic amblyopia in eyes with esotropia and some anisometric amblyopic eyes, it is important to approach comparisons with caution. There appears to be no discernible or consistent alteration in FAZ biomarkers as a result of amblyopia therapy when compared to nonamblyopic eyes. We observed only a significant discrepancy in the circularity index between amblyopic eyes and their matched counterparts at the third visit, which occurred nine months after the initiation of amblyopia therapy. At the final follow-up appointment, there was no significant difference in FAZ biomarkers between amblyopic and nonamblyopic eyes. Wong et al reported no significant difference in the area of the foveal avascular zone (FAZ) between 30 amblyopic eyes and 1045 control eyes. Furthermore, they observed that the circularity of The FAZ was significantly lower in the amblyopic eyes than in the control eyes.21 Nourinia et al in 2022 observed that the area of the FAZ was more extensive in eyes with amblyopia than in unaffected eyes.10 Several studies have reported inconclusive variations in the FAZ area between amblyopic eyes and fellow eyes of children with unilateral amblyopia.5,8,11,14 The FAZ biomarkers do not appear to have any correlation with the development of amblyopia or the health of the fellow eye. We observed no alterations in the perimeter length that were linked to FAZ biomarkers due to amblyopia therapy or when compared to the unaffected eye. Conversely, Choi et al discovered significant changes in the perimeter and circularity biomarkers of the FAZ on OCTA in glaucomatous eyes.22 Altogether amblyopia and its treatment may not alter the perimeter and circularity of the FAZ as in glaucomatous eyes.
In our study, strabismus played a significant role as a confounder/effect modifier in the correlation between FAZ biomarkers and changes after amblyopia therapy. Most of the patients had esotropia and hyperopia. Refractive error correction and fellow eye suppression during treatment could have improved the image focus on the fovea and macular perfusion, leading to changes in the FAZ biomarkers. Amblyopia has been primarily studied as a FAZ biomarker for anisometropic amblyopia.11,23,24 We did not analyze the specific type of strabismus and its impact on the results of our research, as the number of cases with exotropia and emmetropia was small. A study comparing exotropia and intermittent exotropia did not show significant differences in the FAZ biomarkers.25
We did not find that age or sex affected the changes in FAZ biomarkers after amblyopia treatment. Axial length has been demonstrated to grow or increase as young children mature.26 One year of follow-up in a significant number of amblyopic eyes with hyperopia in our study may have contributed to changes in axial length, leading to discrepancies in FAZ biomarkers after therapy. There was a negative but significant correlation between logarithmic vision before therapy and the change in the FAZ area one year after treatment for amblyopia in our study. Wong noted a correlation between baseline log visual acuity and FAZ circularity.21 In hyperopic anisometric eyes, best corrected visual acuity in amblyopic eyes was negatively correlated with vascular density.24 Dense amblyopia is less likely to be a pretherapy BCVA. In amblyopic eyes with anisometropia, vision recovery after therapy can change perfusion and vascular density; however, this has a limited effect on the FAZ. A study by Fujiwara et al in Japan found that age, sex, refractive error, and axial length were not significantly correlated with the FAZ area.27 The age range of our cohort was between 6 and 11 years, and it should be noted that there were limited changes in FAZ observed in this age group. Therefore, the evaluation of FAZ changes in size may be more relevant to the age of the children than the impact of amblyopia treatment. We may consider this as an area for further research to support the hypothesis that the growth of photoreceptors is the reason for the lack of change in FAZ following treatment.
Our study had limitations, including a small subsample of varying ocular parameters, that prevented us from determining their impact on study outcomes. This study may not have had sufficient power to perform a baseline correlation analysis that examined the relationships between certain participant characteristics. We did not measure the axial length of the amblyopic eyes independently, and relied on software-generated adjustments to the FAZ biomarkers. The accuracy of these adjustments could have affected the outcomes for the highly myopic and hyperopic eyes in our study. The current study aimed to explore long-term alterations in OCTA-derived FAZ biomarkers following amblyopia therapy. Our findings contrasted with those of previous research on the short-term outcomes of amblyopia treatment. We conjectured that FAZ biomarkers in eyes treated with refractive correction and occlusion therapy would remain unchanged in the long term despite significant improvements in vision in amblyopic eyes. These findings imply that the outcomes of amblyopia treatment and long-term vision improvement are not affected by structural or vascular changes in the retinal fovea. Visual recovery may occur at a higher level in the visual center than in the macular area due to occlusion.
Conclusion
In this cohort of Saudi children with unilateral amblyopia, one year of occlusion therapy had no significant effect on the area, perimeter, or circularity of the FAZ. While therapy increased visual acuity, FAZ measurements were equivalent between amblyopic and normal eyes. This study provides insights into the potential of FAZ biomarkers for monitoring amblyopia and assessing treatment responses. The findings should be interpreted cautiously given the small sample size.
Abbreviations
OCTA, optical coherence tomography angiography; FAZ, foveal avascular zone; P, p-value; mm2, millimeters squared; mm, millimeters; Gr-1, Group 1 amblyopic eyes; Gr-2, Group 2 nonamblyopic eyes; IQR, interquartile range.
Acknowledgment
Drs. Gorka Sesma and Tasnim Almairi should be considered joint co-first authors because of their equal contribution to the manuscript.
Funding
This study received no funding.
Disclosure
None of the authors have any conflicts of interest to disclose for this work.
References
1. David Cordeiro Sousa. Optical coherence tomographic angiography. American Academy of Ophthalmology. Eyewiki. Available from: https://eyewiki.aao.org/Optical_Coherence_Tomography_Angiography.
2. Coffey AM, Hutton EK, Combe L, Bhindi P, Gertig D, Constable PA. Optical coherence tomography angiography in primary eye care. Clin Exp Optom. 2021;104(1):3–13. doi:10.1111/cxo.13068
3. Sheth J. Commentary: applicability of optical coherence tomography angiography for imaging ocular biomarkers of systemic diseases. Indian J Ophthalmol. 2022;70(5):1677. doi:10.4103/ijo.IJO_247_22
4. Suciu CI, Suciu VI, Nicoara SD, Sokolovska J. Optical coherence tomography (angiography) biomarkers in the assessment and monitoring of diabetic macular edema. Sokolovska J, ed. J Diabetes Res. 2020;2020:1–10. doi:10.1155/2020/6655021
5. Guo M, Zhao M, Cheong AMY, Dai H, Lam AKC, Zhou Y. Automatic quantification of superficial foveal avascular zone in optical coherence tomography angiography implemented with deep learning. Vis Comput Ind Biomed Art. 2019;2(1):21. doi:10.1186/s42492-019-0031-8
6. Shiihara H, Terasaki H, Sonoda S, et al. Objective evaluation of size and shape of superficial foveal avascular zone in normal subjects by optical coherence tomographic angiography. Sci Rep. 2018;8(1):10143. doi:10.1038/s41598-018-28530-7
7. Kim K, Kim ES, Yu SY. Optical coherence tomography angiography analysis of foveal microvascular changes and inner retinal layer thinning in patients with diabetes. Br J Ophthalmol. 2018;102(9):1226–1231. doi:10.1136/bjophthalmol-2017-311149
8. Demirayak B, Vural A, Sonbahar O, et al. Analysis of macular vessel density and foveal avascular zone in adults with amblyopia. Curr Eye Res. 2019;44(12):1381–1385. doi:10.1080/02713683.2019.1639766
9. Sobral I, Rodrigues TM, Soares M, et al. OCT angiography findings in children with amblyopia. J Am Assoc Pediatr Ophthalmol Strabismus. 2018;22(4):286–289.e2. doi:10.1016/j.jaapos.2018.03.009
10. Nourinia R, Rajavi Z, Sabbaghi H, et al. Optical coherence tomography angiography in patients with amblyopia. Strabismus. 2022;30(3):132–138. doi:10.1080/09273972.2022.2097705
11. Liu C, Zhang Y, Gu X, Wei P, Zhu D. Optical coherence tomographic angiography in children with anisometropic amblyopia. BMC Ophthalmol. 2022;22(1):269. doi:10.1186/s12886-022-02486-9
12. Araki S, Miki A, Goto K, et al. Foveal avascular zone and macular vessel density after correction for magnification error in unilateral amblyopia using optical coherence tomographic angiography. BMC Ophthalmol. 2019;19(1):171. doi:10.1186/s12886-019-1177-z
13. Gunzenhauser RC, Tsui I, Velez FG, et al. Comparison of pre-treatment vs. post-treatment retinal vessel density in children with amblyopia. J Binocul Vis Ocul Motil. 2020;70(3):79–85. doi:10.1080/2576117X.2020.1760695
14. Huang X, Liao M, Li S, Liu L. The effect of treatment on retinal microvasculature in children with unilateral amblyopia. J Am Assoc Pediatr Ophthalmol Strabismus. 2021;25(5):287.e1–287.e7. doi:10.1016/j.jaapos.2021.05.011
15. Rebecca S, Braverman MD. PEDIG studies: quality healthcare and amblyopia treatment. American Academy of Ophthalmology, ONE network. Available from: https://www.aao.org/education/disease-review/pedig-studies-quality-healthcare-amblyopia-treatme.
16. Dean AG, Sullivan KM, Soe MM. OpenEpi updated 2013/04/06a. Available from: https://openepi.com/Menu/OE_Menu.htm.
17. Mo S, Krawitz B, Efstathiadis E, et al. Imaging foveal microvasculature: optical coherence tomography angiography versus adaptive optics scanning light ophthalmoscope fluorescein angiography. Invest Ophthalmol Vis Sci. 2016;57(9):OCT130. doi:10.1167/iovs.15-18932
18. Samara WA, Say EAT, Khoo CTL, et al. Correlation of foveal avascular zone size with foveal morphology in normal eyes using optical coherence tomographic angiography. Retina. 2015;35(11):2188–2195. doi:10.1097/IAE.0000000000000847
19. Al-Sheikh M, Tepelus TC, Nazikyan T, Sadda SR. Repeatability of automated vessel density measurements using optical coherence tomographic angiography. Br J Ophthalmol. 2017;101(4):449–452. doi:10.1136/bjophthalmol-2016-308764
20. Zhang T, Xie S, Liu Y, Xue C, Zhang W. Effect of amblyopia treatment on macular microvasculature in children with anisometropic amblyopia using optical coherence tomographic angiography. Sci Rep. 2021;11(1):39. doi:10.1038/s41598-020-79585-4
21. Wong ES, Zhang XJ, Yuan N, et al. Association of optical coherence tomography angiography metrics with detection of impaired macular microvasculature and decreased vision in amblyopic eyes: the Hong Kong Children Eye Study. JAMA Ophthalmol. 2020;138(8):858. doi:10.1001/jamaophthalmol.2020.2220
22. Choi J, Kwon J, Shin JW, Lee J, Lee S, Kook MS. Quantitative optical coherence tomography angiography of macular vascular structure and foveal avascular zone in glaucoma. Bhattacharya S, ed. PLoS One. 2017;12(9):e0184948. doi:10.1371/journal.pone.0184948
23. Hamurcu M, Ekinci C, Koca S, Tugcu B. Evaluation of amblyopic eyes with optical coherence tomography angiography and electrophysiological tests. Indian J Ophthalmol. 2021;69(1):105. doi:10.4103/ijo.IJO_2319_19
24. Doğuizi S, Yılmazoğlu M, Kızıltoprak H, Şekeroğlu MA, Yılmazbaş P. Quantitative analysis of retinal microcirculation in children with hyperopic anisometropic amblyopia: an optical coherence tomography angiography study. J Am Assoc Pediatr Ophthalmol Strabismus. 2019;23(4):201.e1–201.e5. doi:10.1016/j.jaapos.2019.01.017
25. Zhai J, Fang W, Yu X, Ye X, Hou L. Macular perfusion density evaluation in constant and intermittent exotropia by means of optical coherence tomographic angiography. BMC Ophthalmol. 2021;21(1):254. doi:10.1186/s12886-021-02006-1
26. Li S, Yang X, Li M, et al. Developmental changes in retinal microvasculature in children: a quantitative analysis using optical coherence tomographic angiography. Am J Ophthalmol. 2020;219:231–239. doi:10.1016/j.ajo.2020.05.008
27. Fujiwara A, Morizane Y, Hosokawa M, et al. Factors affecting foveal avascular zone in healthy eyes: an examination using swept-source optical coherence tomographic angiography. González-Méijome JM, ed. PLoS One. 2017;12(11):e0188572. doi:10.1371/journal.pone.0188572
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.