Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Evaluation of Dermatoglyphic Features of Type 2 Diabetic Patients as Compared to Non-Diabetics Attending Hospitals in Southern Ethiopia
Authors Tadesse A, Gebremickael A ![]() , Merid M
, Merid M ![]() , Wondmagegn H
, Wondmagegn H ![]() , Melaku T, Ayele T
, Melaku T, Ayele T ![]() , Meskele S
, Meskele S ![]() , Esubalew H
, Esubalew H ![]() , Birhanu A
, Birhanu A
Received 1 January 2022
Accepted for publication 20 April 2022
Published 24 April 2022 Volume 2022:15 Pages 1269—1280
DOI https://doi.org/10.2147/DMSO.S356728
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ming-Hui Zou
Amanuel Tadesse,1 Abinet Gebremickael,2 Melkamu Merid,3 Habtamu Wondmagegn,2 Tesfaye Melaku,1 Tsegazeab Ayele,2 Simeon Meskele,1 Habtamu Esubalew,3 Asaminew Birhanu2
1Department of Human Anatomy, College of Medicine and Health Sciences, Dilla University, Dilla, Ethiopia; 2Department of Human Anatomy, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia; 3Department of Public Health, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia
Correspondence: Habtamu Wondmagegn, Department of Human Anatomy, College of Medicine and Health Sciences, Arba Minch University, Post Box No: 21, Arba Minch, Ethiopia, Tel +251 913028959, Fax +251 0468810279, Email [email protected]; [email protected]
Background: Diabetes mellitus (DM) is a complex metabolic disorder characterized by persistent hyperglycemia resulting from defects in insulin secretion, insulin action, or both. Type 2 DM has a strong hereditary background. A study of the dermatoglyphic features can help in the early identification of people with a genetic predisposition to develop type 2 DM.
Purpose of the Study: The study was aimed to compare the finger and palmar dermatoglyphics features in type 2 diabetic and non-diabetic patients and to evaluate the association with other variables.
Patients and Materials: Institution-based cross-sectional study was conducted in one referral hospital and three primary hospitals located in Gedeo Zone. Three hundred ninety study participants (130 type 2 diabetics and 260 non-diabetics) from adult OPD and diabetic clinics were included in the study. The association among different dermatoglyphics variables was analyzed using the chi-square test. An independent t-test was conducted to analyze the mean difference and to test the significance of numerical variables. A statistically significant association was declared at P-value < 0.05.
Results: In the present study, a total of 3900 digits (1300 from type 2 diabetic and 2600 non-diabetic) were analyzed for distribution of digital dermatoglyphic patterns. Loop pattern is found to be the commonest in both study groups with a prevalence of 65.8% and 60.7% among type 2 diabetics and non-diabetics, respectively. Both the right-left axial tri-radius angle was significantly higher in type 2 diabetes mellitus patients compared to non-diabetic study participants. Total finger ridge counts and absolute finger ridge counts showed no significant difference in both groups.
Conclusion: The study revealed Loop pattern was more frequent in type 2 DM compared to non-diabetic study participants. Whorl type was more common than arch type in non-diabetic patients compared to type 2 DM groups. The result also showed tri-radius angle is significantly wider in diabetic groups in both hands.
Keywords: dermatoglyphics, type 2 DM, dermatoglyphic patterns, Gedeo Zone
Introduction
Diabetes mellitus (DM) is a complex metabolic disorder characterized by persistent hyperglycemia resulting from defects in insulin secretion, insulin action, or both.1 Including diabetes mellitus (DM) there are many diseases known to be caused genetically. In recent years, Dermatoglyphics is claimed as a screening aid in patients with type 2 diabetes mellitus (T2DM).2
Skin is the outermost part and the largest organ of our body. It is mostly smooth except for the friction ridges which are found on the digits of palms and soles. The term Dermatoglyphics was first coined by Cummins and Midlo in 1926. It is derived from the Greek words “derma” means skin and ‘glyphics’ means carvings. It deals with the study of epidermal ridges and their configurations on the palmar region of hands and fingers and the plantar region of feet and toes. Palm is the most accessible part of the body and easy for dermatoglyphics.3
Evidence from family studies, and, in particular, from identical twins, shows that dermatoglyphic traits are to a large extent determined by heredity. Complex genetical processes are involved and, as yet, the inheritance of the patterns is little understood. Quantitative methods, based on counting ridges between specified points and measurements of angles, have provided further information on the inheritance of dermatoglyphic traits. The number of ridges cutting or touching a straight line between the triradius and the core of a finger pattern gives a measure of the size and complexity. In a loop there is one triradius and so one ridgecount; in a whorl with two triradii there are two counts and the higher is used. For an arch the score is O. The counts on all ten fingers of an individual can be added to give a single value, the total finger ridge-count.3
Ridges begin to appear in embryos at 10 weeks and are permanently established by 17 weeks. The type of pattern that develops is determined genetically and constitutes the basis for examining fingerprints in criminal investigation and medical genetics. Interestingly dermatoglyphic science is based on two major facts; first, the ridges are slightly different for different fingers and no two persons, not even monozygotic twins, show the same fingerprint patterns, and second, unlike other body markers the epidermal ridges are constant throughout life.3 The ridge patterns on the palm and fingers are divided into three groups: Arches, loops and whorls. Arches are formed by a succession of more or, less parallel ridges, which traverse the pattern area. Loop pattern is composed of a series of ridges that enter the pattern area on one side of digit recurve and leave the pattern area on the same side. If the ridges open-up on the ulnar side, the resulting loop is termed as ulnar loop when they open-up towards the radial margin, it is termed as a radial loop. The ridges in a simple whorl are commonly arranged as a succession of concentric rings. Such patterns are described as concentric whorls.4
In addition, dermatoglyphics is related to individual genetics; as the diabetes mellitus has also a genetic background; one can assume that there might be certain dermatoglyphics findings specific to diabetic patients. In clinical medicine, the importance of dermatoglyphics is that it can help in predicting the phenotype of a possible future illness.3,4 Taking into consideration of genetic predisposition of dermatoglyphics and DM, the present study was undertaken to find out the association between them, so that the dermatoglyphics may be helpful in the screening of predisposition towards type 2 diabetes at an earlier age.
Materials and Methods
The present study was conducted in four Governmental Hospitals in Gedeo Zone, namely, Dilla University Referral Hospital, Bule primary Hospital, Yirgachefe primary, and Gedeb primary Hospital. The institution-based cross-sectional study design was employed among randomly selected 130 type 2 diabetic patients and 260 non-diabetics. An interviewer-administered structured questionnaire was designed to collect data on socio-demographic and other related variables. Blood pressure and history were taken to exclude patients with other genetic-related diseases. And blood sugar test was done accordingly. Categorical variables are dermatoglyphic pattern types and the numeric (continuous) variables are epidermal ridge counts and palmar ATD angles.
Inclusion Criteria for Type 2 Diabetic Group (Diabetic Clinic)
- Diagnosed with type 2 DM: Blood sugar level – Fasting −120mg/dl or higher or Postprandial 180 mg/dl or higher,
- Absence of any other genetic disorders like hypertension, Neurological disorders, and Consecutive follow-up for at least three months.
Inclusion Criteria for the Non-Diabetic Group (Adult OPD)
- Normal blood sugar levels– Fasting –lower than 120mg/dl or Postprandial lower than 180 mg/dl and
- Absence of any other overt genetic disorders like hypertension, Neurological disorders, and no known family history of diabetes mellitus.
Study participants with deformity of the hand, which impaired fingerprint visibility, congenital anomalies of the hand, any skin disorders over the hand which will impair the visibility of palmar and fingerprint, and amputation of any phalanx of a single digit were excluded from the study.
Data Collection Procedure
The participant was first briefed about the study, the procedure, and the need for the handprint. After obtaining an informed consent form signed, study participants were requested to wash their hands and dried them with a clean cloth. A small amount of ink was placed on the fingers and palms of the subject with cotton. The hand was rolled starting from the wrist and moving to the fingers with gentle pressure applied from the dorsal side by the subject. The individual fingertips were rolled from ulnar to radial side to obtain rolled fingerprints. The procedure was repeated on the other hand. Soon after the print is taken, it was examined for clarity in the different fingers and the palmar areas. To ensure data quality, training was given to the data collectors. Properly designed data collection materials were prepared. Supervision was carried out by the principal investigator during data collection times to check completeness and consistency.
Operational Definitions
In the present study, fingertip Pattern Configuration was classified as follows based on a classification prepared by Galton, which divided the ridge patterns on the distal phalanges of the fingertips into three groups arches, loops, and whorls.5
Arch (A)
It is the simplest pattern found on fingertips. It consists of more or less parallel ridges, which traverse the pattern area and form a curve that is concave proximally.
Loops (L)
It is the most common pattern on the fingertip. In this, the ridges start from one side, run in parallel lines and then, curve backward to terminate on the same side of their origin.
Whorls (W)
In a whorl, there are multiple circular or oval ridges, one around the other, or a single ridge runs spirally in multiple rounds. In this, there are 2 or more triradii. One triradius is on the radial side and the other on the ulnar side of the pattern.
Triradius
A triradius is formed by the confluence of three ridged systems and the triradial point is the geometric center of the triradius. Ideally, it is the meeting point of three ridges that form angles of approximately 120° with one another.
Core
It is in the approximate center of the pattern.
Radiants (Type Lines)
These are the ridges that emanate from the triradius and enclose the pattern area.
Ridge Counting
The counting is done along the straight lines connecting the triradial point to the point of the core.
Finger Ridge Count (FRC)
Finger Ridge Count (FRC) is defined as the number of ridges intersected by a line between the triradial points to the point of the core.
Total Finger Ridge Count (TFRC)
Represents the sum of the ridge count of all ten digits.
Absolute Finger Ridge Count (AFRC)
AFRC is the sum of ridge counts from all the separate triradii on the fingers (Figure 1).
 |
Figure 1 Showing the finger ridge count for different patterns. Red line indicating finger ridge count of loop pattern, Maroon lines indicating finger ridge count of whorl pattern with two triradii there are two counts and the higher is used. |
ATD angle is formed by lines drawn from digital triradius “a” to the axial triradius “t” and from axial triradius “t” to the digital triradius “d”. It is formed by lines drawn from digital triradius “a” to the axial triradius “t” and from axial triradius “t” to the digital triradius “d”. The more distal the position of “t”, the larger the atd angle6 (Figure 2).
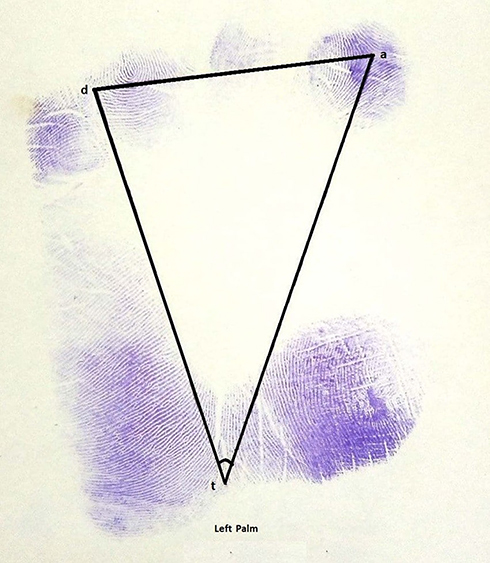 |
Figure 2 Showing the atd angles of the left palm Gedeo Zone governmental hospitals, Southern Ethiopia. |
Axial triradius-The triradius close to the palmar axis is termed axial triradius (t).
Good glycemic control: average fasting blood glucose of 80–130 mg/dL.
Poor glycemic control: average fasting blood glucose of > 130 mg/dL.
Symmetry- the occurrence of specific creases or patterns types on both palms and digits.
Asymmetry –the presence of a specific type of crease or pattern type on one palm or digits.
Statistical Analysis.
Result
In the present study, a total of 406 subjects were planned to participate in the study, and 390 subjects were enrolled which is a 96.05% response rate. Out of these 260 were non-diabetics and 130 were type 2 diabetics. Among the diabetic group, 87 (66.9%) were male and 43 (33.1%) were female. Among non-diabetics 139 (53.5%) were male and 121 (46.5%) were female (Table 1).
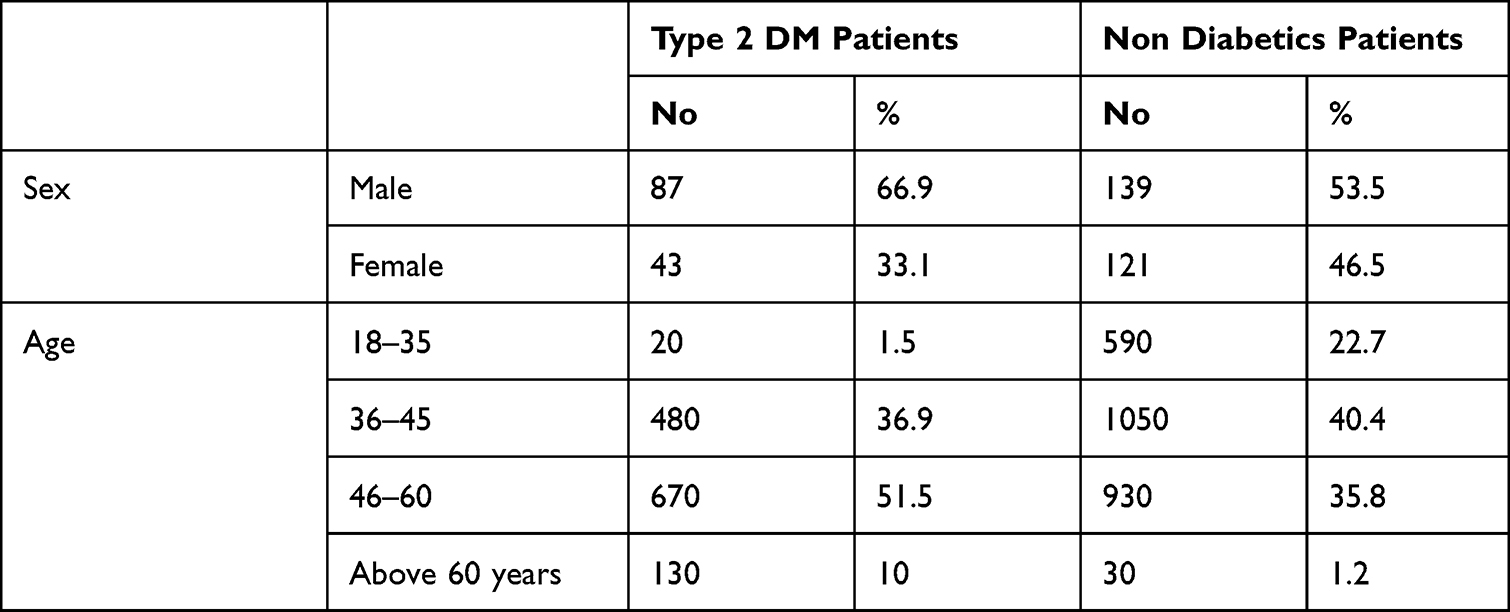 |
Table 1 Frequency Distribution of Socio-Demographic Characteristics of Type 2 DM Patients and Non-Diabetic Patients in Gedeo Zone Public Hospitals, Southern Ethiopia |
A total of 3900 digits were analyzed for distribution of digital dermatoglyphic pattern 1300 and 2600 for each of diabetics and non-diabetic study participants, respectively. Loop type was most frequent 65.8% [95% CI: 63.2, 68.4] in type 2 DM and 60.7% [95% CI: 58.7, 62.5] in non-diabetics, followed by whorl 27.5% [95% CI: 25.2, 29.9] in type 2 DM and 33.8% [95% CI: 32.1, 35.7] in non-diabetics and arches were 6.57% [95% CI: 5.4, 8.0] in type 2 DM and 5.5% [95% CI: 4.6, 6.4] in non-diabetic study participants (Figure 3).
 |
Figure 3 Frequency distribution of finger print pattern among type 2 diabetic and non-diabetic patients Gedeo Zone governmental hospitals, Southern Ethiopia. |
Among those who are type 2 diabetic patients, 43.1% of them had good glycemic control in the last 3 months and 56.7 had poor glycemic control. Comparing the dermatoglyphics pattern of the two group loop pattern was 62.4% in those with poor glycemic control which was lower compared to 70.4% in those with good glycemic control and arch 5% patterns were similarly lower with lower in those with poor glycemic control frequency in those with poor glycemic control compared to 8.9% in those with good glycemic control. But whorl 32.6% type was significantly higher in those with poor glycemic control compared to 20.7% in those who had good glycemic control (Figure 4).
 |
Figure 4 Different finger print patterns of study participants Gedeo Zone governmental hospitals, Southern Ethiopia. |
Factors Associated with Digital Dermatoglyphics Patterns
All independent variables of the study such as sex, body side, symmetries, and type 2 DM status fulfill the assumption of the chi-square test were analyzed and only sex and symmetries were significantly associated with dermatoglyphic patterns in both type 2 DM patients and Non-diabetic patients.
In male fingerprint patterns in type 2 DM and non-diabetics were, 27.1% and 22.7% whorl, 65.1% and 71.9% loop, and 7.8% and 5.3% arch, respectively. On the other hand, in females, the finding for type 2 DM and non-diabetics were, 35.6% and 29.3% whorl, 60.0% and 65.0% loops, 4.4%, and 5.6% arch, respectively. The distribution of arch pattern was significantly higher in type 2 DM group in males but lower in females compared to the non-diabetic group (p<0.05). The loop pattern was found significantly lower in type 2 DM compared to non-diabetic study participants (p<0.05). The distribution of the whorl pattern was significantly higher in the male type 2 DM group as compared to non-diabetic subjects. But it was higher in the female type 2 DM group as compared to non-diabetic study participants (Table 2).
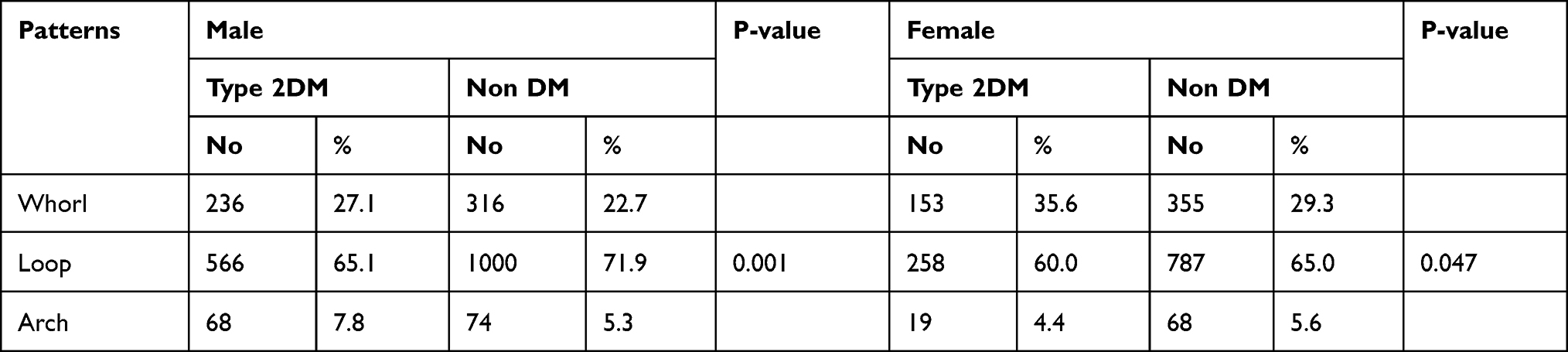 |
Table 2 Prevalence and Chi-Square Test of the Dermatoglyphics Pattern of Both Male and Female in Diabetic and Controls |
A total of 3900 fingerprint patterns on the right and left hands of the study group were assessed. Right hand fingerprint patterns in type 2 DM and non-diabetics were; whorl 29.7% and 26.5%, loop 63.2% and 69.2% and arch 7.1 and 4.4%, respectively. On the left hand the results were; 30.2% and 25.2% whorl, 63.5% and 68.3% loop, 6.3% and 6.5% arch patterns, respectively in type 2 DM and non-diabetics groups. The findings revealed that the distribution of arch pattern was insignificantly lower in right and left hand of the type 2 DM compared to the non-diabetic group. The loop pattern was also insignificantly lower in both hands of the diabetics compared to the non-diabetic group. There was a higher and insignificant difference in the distribution of whorl pattern in both hands of the type 2 DM group as compared to non-diabetic study participants (Table 3).
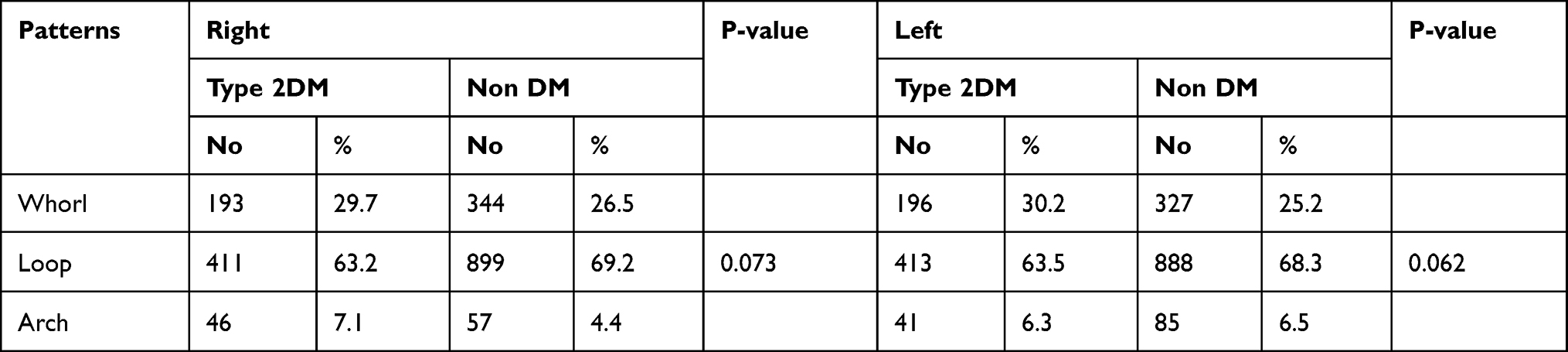 |
Table 3 Prevalence and Chi-Square Test of the Dermatoglyphics Pattern of Both Hands in Diabetic and Controls |
Fingerprint patterns were assessed for symmetries between right and left digits for type 2 DM and non-diabetic study participants. Of 3900 fingerprint patterns studied from type 2 DM study participants who had symmetrical pattern distribution, 27.1% was whorl pattern, 66.9% was loop pattern and 6.0% was arch patterns. On the other hand, of study participants who had asymmetrical pattern distribution, 41.2% were whorl, 49.2% were loops and 9.6% were arch-type patterns. For the non-diabetic study group who had symmetrical pattern distribution, 20.6% were whorl, 76.4% were loops, and 3.1% were arch, whereas, from those who had asymmetrical pattern distribution 39.6% were whorl, 48.7% were loops, and 11.7% were an arch-type of patterns. The finding showed that symmetrical distribution of whorl and arch patterns was higher in type 2 DM study participants when compared to non-diabetic study participants. However, the symmetrical pattern distribution of the loop was lower in diabetics than non-diabetics study participants. Whereas study participants who had an asymmetrical distribution of loop and whorl were higher in type 2 DM than non-diabetics study participants but the asymmetrical distribution of arch was lower in type 2 DM individuals as compared to non-diabetics study participants (Table 4).
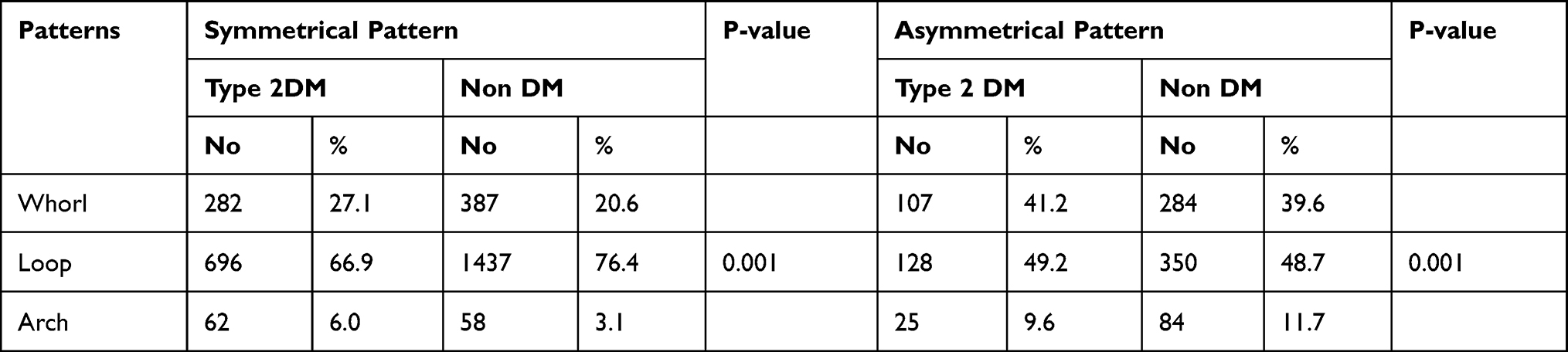 |
Table 4 Prevalence and Chi-Square Test of Symmetryness with Dermatoglyphics Pattern Among Type 2 DM Patients and Non-Diabetic Patient |
Comparison of “atd” Angle, TFRC, and AFRC Between Type 2 Diabetic Patients and Non-Diabetic
Both the right atd and left atd angles were significantly higher in Type 2 diabetic patients compared to non-diabetic study participants (Figure 5).
 |
Figure 5 Palm print of the right hand showing atd angle in Gedeo Zone governmental hospitals, Southern Ethiopia. |
Absolute finger ridge count in type 2 diabetics shows that the mean value was 160.37 compared to total finger ridge count in non-diabetic subjects with a mean value of 150.4 with an insignificant p-value (p > 0.05). The Total Finger Ridge count in type 2 diabetics shows that the mean value was 123.4 compared to the total finger ridge count in normal study participants which was 116.0 without significance (Table 5).
 |
Table 5 Comparison of Atd Angle, TFRC and AFRC Among Type 2 Diabetes and Non-Diabetes Mellitus Patient |
Bivariable and Multivariable Multinomial Logistic Regression Analysis of Digital Dermatoglyphics Patterns
Variables including sex, body side symmetries, and status of type 2 diabetes mellitus fulfilled the assumption of the chi-square test and were analyzed using Bivariable multinomial logistic regression. Three of these values sex and status of type 2 diabetes mellitus showed that p-value less than or equal to 0.05 in Bivariable analysis and then taken to multivariable analysis. On multivariable analysis, sex, symmetries, and diabetes mellitus had a statistically significant association with one or more types of digital dermatoglyphics patterns. Being male was 0.6 times more likely to have whorl type (AOR= 0.666, 95% CI 0.497, 0.892) than an arch-type of dermatoglyphics patterns. The odds of having symmetrical patterns between digits of hands were nearly 1.6 times more likely to have whorl (AOR=1.591, % CI [1.190, 2.128]) and 4 times to have a loop (AOR =4.264, 95% CI [3.221, 5.645]) than arch pattern types (Table 6).
 |
Table 6 Bivariable and Multivariable Analysis of Multinomial Logistic Regression of Associated Factors with Digital Dermatoglyphics Pattern of Public Hospitals in Gedeo Zone |
Discussion
Dermatoglyphics deals with the scientific study of epidermal ridge patterns on the palmar and plantar aspects of fingertips, palms, soles, and toes. Diabetes mellitus and Dermatoglyphics, both are genetically influenced. So some changes in the Dermatoglyphic pattern of type 2DM patients are expected. The procedure of recording epidermal ridge configurations is simple, non-invasive, and inexpensive. Widespread medical interest in epidermal ridges developed only in the last few decades when it became apparent that many patients with chromosomal aberrations had unusual ridge patterns. Inspection of skin ridges, therefore, promised to provide a simple, inexpensive means of information to determine whether a given patient could have a particular chromosomal defect.7,8 Once characteristic dermatoglyphics findings of particular diseases are noted, they can be used as markers to predict the disease in the general population and can be used as a screening tool.
In the present study, the distribution of the fingerprint patterns is dominated by loop followed by whorl pattern, and fewer numbers arch patterns were observed in both diabetic and non-diabetic study participants. The pattern type was analyzed between type 2 DM and non-diabetic study participants and the whorl pattern in type 2 DM (27.5%) was significantly lower than in non-diabetic groups (33.8%). And this was strongly supported by a study in different regions of India which reported that type 2 DM group had a lower whorl type pattern than the non-diabetic group.9–11 In contrast to the findings of the current study, a study done in India, Udaipur region, Vikhei Pathil Hospital and in Sholapur medical College revealed significantly higher whorl pattern among type 2 DM compared to non-diabetic groups.8,12,13
The result from the current study revealed that the frequency of loop pattern was significantly higher in the type 2 DM (65.8%) as compared to the non-diabetic group (60.7%). This Finding of a higher loop pattern was in line with some studies done in India.10,11 On the other hand, several studies done in other regions of India had reported that the non-diabetic group had a higher loop pattern than type 2 diabetic groups.8,13–15 The present study showed that the prevalence of arch type pattern in type 2 DM group 6.57% was significantly higher than non-diabetic group 5.5%. And our study was strongly supported by studies done in Uganda16 and India.9,11 However, studies from the Udaipur and Maharashtra regions of India have reported that the type 2 DM group had a lower arch type pattern than non-diabetic groups.8,11,15 These discrepancies can be explained by racial dermatoglyphic differences from one region to another and ethnohistoric and geographic variations between different human populations.17
Regarding the sex distribution of fingerprint patterns, the occurrence of whorl type, respectively in type 2 diabetic and non-diabetics were 236 (27.1%) and 316 (22.7%) in the males, and 153 (35.6%) and 355 (29.3%) in the females. These findings are strongly supported by studies done in India in both sex.8,13,15 But fewer studies from other regions of India reported that the type 2 diabetic group had a lower whorl pattern than non-diabetic study participants.9 And another study had reported that only male diabetic group had significantly lower whorl patterns.18
In the current study the prevalence of loop-type among type 2 diabetics and non-diabetic groups occurred as 566 (65.1%) and 1000 (71.9%) in males, and 258 (60.0%) and 787 (65.0%) in females, respectively. Such findings are consistent with most studies were done in India.13–15 On the other hand few of the studies done in India in both sexes, have reported that non-diabetic groups had lower loop patterns than type 2 diabetic groups.10,11
In the current study, the prevalence of arch type respectively in diabetic and non-diabetics were 7.8% and 5.3% in males which was strongly supported by studies done in India.11,14 The current finding was 4.4% and 5.6% in female diabetic and non-diabetic groups respectively, And this is in-line with studies done in Uganda and India.15,16 In contrast to the current finding, studies done in Uganda reported a lower frequency of arch patterns in female non-diabetic groups,15,16 and studies from India showed a higher arch frequency of arch patterns in non-diabetic male study participants.11,14
A total of 3900 fingerprint patterns on the right and left hands of study groups were analyzed. On the right hand the following result was found: Whorl 29.7% in type 2 diabetic and 26.5% in non-diabetic groups, which is in line with most of the studies done in India.8,13,14 In contrast to this fewer studies reported lower whorl pattern in diabetic study participants.9
Loop pattern was found in 63.2% of type 2 diabetics and 69.2% of the non-diabetic group. This result was consistent with; studies were done in different regions of India.13–15 However, some studies done in India reported that the loop pattern was lower in non-diabetics than diabetics.11
In addition, the arch was 7.1% in type 2 diabetics and 4.4% non-diabetic group. This is comparable with a study done in India.9,11 However, a study done in Uganda reported that arch was higher in non-diabetic than diabetic study participants in the right hand.16
On the left hand in the present study, the occurrence of whorl type was 30.2% and 25.2% in diabetics and non-diabetic groups respectively. The result revealed that whorl type was higher in type 2 diabetic than non-diabetics group. These findings go along with the studies done in India which revealed a higher whorl pattern in type 2 diabetic group.8,12 The occurrence of loop-type was 63.5% in diabetic and 68.3% in non-diabetic groups. This finding was strongly supported by studies done in different regions of India,13,14 although fewer studies observed that non-diabetic study participants had a higher distribution of loop patterns on the left hand.11 Arch type pattern (6.3% and 6.5%), was lower in diabetic than the non-diabetic group. This finding was similar to a study done in Uganda.16 On the other hand, a study was done in India had reported that diabetic study participants had a higher arch as compared to non-diabetic study subjects.11
Shreds of evidence attest that pattern determination occurs much earlier than the ridge proliferation, possibly influenced by the volar pad’s shape, the embryonic epidermal axon development, or a combination of both. This asserts that patterns develop as early as week’s 6–11, thus indicating that the results of fingerprint discrepancies in this study evidence mid-to-late 1st-trimester insults on the developing fetus.17
In the current study, the mean atd angle of the right palm among type 2 diabetic and non-diabetic subjects were respectively, 42.4±5.27 and 39.6±6.04. This finding revealed an increased atd angle among type 2 diabetic study participants compared to non-diabetics and the mean atd angle of the left hand among type 2 DM and non-diabetics study participants were respectively 41.4±4.9 and 40.0±7.1 in both the right and left hands the finding was strongly supported by most of the studies done in India.19–21 Our study revealed that TFRC and AFRC were higher among diabetic subjects without reaching significance level. The mean value of AFRC was 160.37±79.2 and 150.4±62.4 among diabetics and non-diabetics respectively; the mean TFRC was 123.4±44.2 and 116.0±37.7 among diabetics and non-diabetics study participants, respectively. This finding was consistent with the studies conducted in India.8,14
Conclusion
The study revealed Loop pattern was more frequent in type 2 DM compared to non-diabetic study participants. Whorl type was more common than arch type in non-diabetic patients compared to Type 2 DM groups. The result also showed tri-radius angle is significantly wider in diabetic groups in both hands. The Total Finger Ridge count and absolute finger ridge count in type 2 diabetics is higher than the controls without reaching the level of significance.
Limitation of the Study
The current study had some limitations as the study depends on hospital patients who live in the same geographical area and same ethnicity. Consequently, the population from different ethnicity and the relatively healthier individual were not included.
Abbreviations
AFRC, absolute finger ridge count; DM, diabetes mellitus; FRC, finger ridge count; FBS, fasting blood sugar; FPG, fasting plasma glucose; RBS, random blood sugar; TFRC, total finger ridge count; SD, standard deviation.
Data Sharing Statement
The datasets used and analysed in the current study are available from the corresponding author on reasonable request.
Ethical Approval and Informed Consent
This study was carried out after obtaining ethical approval from Arba Minch University, College of Medicine, and Health Sciences, Institutional Research Ethics Review Board (IRB/023/02/20.; Issue date: 26/11/2020). To ensure confidentiality, it was the anonymous type whereby names of the study subjects were not written on the questionnaire. Written consent from the study participants was obtained after they were briefed about the research intent and asked for their willingness to participate in the study. Their right of denial to participate in the study was also assured. This study was conducted per the declaration of Helsinki.
Acknowledgments
We acknowledge Arba Minch University, study participants, data collectors, supervisors, Dilla University Referral Hospital, Bule primary Hospital, Yirgachefe primary, and Gedeb primary Hospital for their cooperation.
Author Contributions
All authors made substantial contributions to conception and design; execution and acquisition of data; analysis and interpretation of data; took part in drafting the manuscript and revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest for this work.
References
1. American Diabetic Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(Supplement 1):S81–S90. doi:10.2337/dc14-S081
2. Srivatsava S, Burli S. A study of palmar dermatoglyphics in type 2 diabetes mellitus in a Bangalore based population. Indian J Clin Anat Physiol. 2019;6(1):118–125. doi:10.18231/2394-2126.2019.0028
3. Cummins H, Midlo C. Palmar and plantar epidermal ridge configurations (dermatoglyphics) in European‐Americans. Am J Phys Anthropol. 1926;9(4):471–502. doi:10.1002/ajpa.1330090422
4. Bardale R. Principles of Forensic Medicine & Toxicology.
5. Galton F. Finger prints Macmillan. London; 1892.
6. Cummins H, Midlo C. Finger Prints, Palms and Soles: An Introduction to Dermatoglyphics. New York: Dover Publications; 1961.
7. Sudagar M, Radha K, Duraipandian K, Sundaravadhanam K. Study of palmar patterns in diabetic patients. Int J Adv Med. 2014;1(2):117–122.
8. Rakate N, Zambare B. Comparative study of the dermatoglyphic patterns in type II diabetes mellitus patients with non diabetics. Int J Med Res Health Sci. 2013;2(4):955–959. doi:10.5958/j.2319-5886.2.4.153
9. Burute P, Kazi S, Swamy V, Arole V. Role of dermatoglyphic fingertip patterns in the prediction of maturity onset diabetes mellitus (Type II). IOSR J Dent Med Sci. 2013;8(1):1–5. doi:10.9790/0853-0810105
10. Perumal A. Doctor of Philosophy in Anatomy. Vinayaka Missions University; 2016.
11. Sachdev B. Biometric screening method for predicting type 2 diabetes mellitus among selected tribal population of Rajasthan. Int J Cur Bio Med Sci. 2012;2(1):191–194.
12. Ojha P, Gupta G. Dermatoglyphic study: a comparison in hands of type II diabetes mellitus patients and normal persons of Udaipur Region. J Evol Med Dent Sci. 2014;3(47):11358–11369. doi:10.14260/jemds/2014/3486
13. Pathan F, Hashmi R. Variations of dermatoglyphic features in non insulin dependent diabetes mellitus. Int J Recent Trends Sci Technol. 2013;8:16–19.
14. Sharma MK, Sharma H. Dermatoglyphics: a diagnostic tool to predict diabetes. J Clin Diagn Res. 2012;6(3):327–332.
15. Ferozkhan P, Anjali G. Dermatoglyphics in type 2 diabetes mellitus. J Med Educ Res. 2011;1(1):6–8.
16. Marera D, Oyieko W, Agumba G. Variation in dermatoglyphic patterns among diabetics in Western Uganda population. Afr J Sci Res. 2015;7(3):20–25.
17. Yohannes S, Alebie G, Assefa L. Dermatoglyphics in type 2 diabetes with implications on gene linkage or early developmental noise: past perspectives. Curr Trends Future Prospects. 2015;3(1D):297–305.
18. Umana UE. Dermatoglyphic and cheiloscopic patterns among diabetic patients: a study in Ahmadu Bello University Teaching Hospital Zaria, Nigeria. J Biol Life Sci. 2013;4(2):206–214.
19. Nayak V, Shrivastava U, Kumar S, Balkund K. Dermatoglyphic study of diabetes mellitus type 2 in Maharashtrian population. Int J Med Sci Res Pract. 2015;2(2):66–69.
20. Trivedi PN, Singel TC, Kukadiya UC, et al. Correlation of ATD angle with non-insulin dependent diabetes mellitus in Gujarati population. J Res Med Dent Sci. 2014;2:2. doi:10.5455/jrmds.20142211
21. Mittal M, Lala B. Dermatoglyphics: an economical tool for prediction of diabetes mellitus. Int J Med Health Sci. 2013;2(3):292–297.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.