Back to Journals » Clinical Ophthalmology » Volume 14
Evaluation of Corneal Structure and Endothelial Morphological Characteristics in Type 2 Diabetic and Non-Diabetic Patients
Authors Beato JN ![]() , Esteves-Leandro J, Reis D, Falcão M
, Esteves-Leandro J, Reis D, Falcão M ![]() , Rosas V, Carneiro Â, Falcão Reis F
, Rosas V, Carneiro Â, Falcão Reis F
Received 6 April 2020
Accepted for publication 2 July 2020
Published 14 July 2020 Volume 2020:14 Pages 1993—1999
DOI https://doi.org/10.2147/OPTH.S256244
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
João N Beato, 1, 2 João Esteves-Leandro, 1 David Reis, 3 Manuel Falcão, 1, 2 Vítor Rosas, 1 Ângela Carneiro, 1, 2 Fernando Falcão Reis 1, 2
1Department of Ophthalmology, São João Hospital, Porto, Portugal; 2Department of Surgery and Physiology, Faculty of Medicine, University of Porto, Porto, Portugal; 3Faculty of Medicine, University of Porto, Porto, Portugal
Correspondence: João N Beato
Department of Ophthalmology, São João Hospital, Al Prof Hernâni Monteiro, Porto 4200-319, Portugal
Tel +351 225 51 2168
Fax +351 225 51 3669
Email [email protected]
Purpose: To compare corneal structure and endothelial morphological features between patients with type 2 diabetes mellitus (DM) and non-diabetic patients; and determine if the DM duration, glycated hemoglobin (HbA1c) levels, and diabetic retinopathy (DR) stage affect corneal morphological properties.
Patients and Methods: Sixty diabetic patients and 47 age- and sex-matched controls were enrolled in this cross-sectional study. DM group was analyzed according disease duration, HbA1c levels, and presence of retinopathy. Endothelial cell density (ECD) and morphology (average and coefficient of variation [CV] of cell size, percentage of hexagonal cells) were recorded using non-contact specular microscopy. Central corneal thickness (CCT) and corneal volume were measured by scheimpflug tomography. Univariate and multivariate linear regression analyses were performed to evaluate the relationship between demographical, clinical, and ocular variables with CCT and ECD.
Results: There were no statistically significant differences in the endothelium cell density or morphology between DM and non-DM groups (p> 0.05). Also, there was no statistical difference between groups for CCT or corneal volume (p> 0.05). Multivariate linear regression analysis showed that older age (p=0.028) was significantly associated with lower ECD; CCT was found to be significantly greater in males (p< 0.001) and positively associated with corneal volume (p< 0.001).
Conclusion: The present study did not find any statistically significant differences between the corneal structural and endothelial characteristics of diabetic and non-diabetic subjects; other demographical parameters, such as age and gender, seem to be more determinant for the corneal properties.
Keywords: diabetes mellitus, endothelium, central corneal thickness
A Letter to the Editor has been published for this article.
Introduction
The relationship between corneal ultrastructural changes and elevated plasma glucose concentrations in diabetes mellitus (DM) has been extensively studied in the last decades. Advanced glycosylated end-products (AGEs) accumulation has been shown to cause protein cross-linking and destruction of endothelial cellular structures.1 In addition, the increased aqueous humor glucose levels are believed to directly inhibit endothelial Na+/k+ ATPase activity2 resulting in corneal edema and reduced transparency. Therefore, careful corneal endothelium evaluation of diabetic patients is crucial to accurately plan and perform several ophthalmological procedures, in particular cataract surgery.3,4
Endothelial cell analysis plays an important role in daily clinical practice as it gives valuable information on corneal function and viability. Moreover, assessments of the corneal thickness have been proposed as a surrogate marker of endothelial barrier dysfunction in DM, due to the direct physical effect of hyperglycemia on the corneal hydration.5,6
Despite the larger number of studies addressing corneal endothelial morphology and thickness changes in diabetic patients, this relationship is far from being clarified. For example, several studies reported that diabetic corneas had lower endothelial cell density (ECD) with higher polymegathism and pleomorphism7–10 and greater corneal thickness,8,11 while others reported no differences compared to non-diabetic subjects.3,12,13 Several reasons may have contributed to contradictory conclusions, namely the different designs used (eg, DM diagnosis, endothelial evaluation method, sample size calculation7,11), subject’s characteristics (eg, race, type, and severity of DM) and inadequate statistical methodology (eg, paired eye data without statistically accounting for it14–16).
The purpose of this study was to evaluate the differences in corneal structural and endothelial morphological features between patients with and without type 2 DM. In addition, it aimed to determine if the DM duration, HbA1c levels, and diabetic retinopathy (DR) stage affect corneal thickness and endothelial morphological properties.
Patients and Methods
Subjects and Protocol
This cross-sectional observational study was conducted at the Department of Ophthalmology, Centro Hospitalar São João, Porto, Portugal. The protocol adhered to the tenets of the Declaration of Helsinki and was approved by the Centro Hospitalar São João Institutional review board. Written consent was obtained from each participant.
Caucasian type 2 diabetic patients and controls, aged 50 or older, scheduled for cataract surgery between September 2015 and March 2016 were invited to participate.
Full selection criteria are described elsewhere;17 but in short, DM diagnosis was confirmed by medical history and glycated hemoglobin (HbA1c) levels ≥ 6.5%. The exclusion criteria included the presence of any ocular disease, except cataract and DR (however, patients with eyes with uncontrolled complications of proliferative DR and/or white/brown cataracts were excluded); prior eye surgery (except for intravitreal treatment > 120 days or laser photocoagulation > 90 days before surgery of diabetics); axial length [AL] > 26 mm or refractive error > 6 diopters of spherical equivalent; wearing of contact lenses; pseudoexfoliation syndrome; systemic connective tissue diseases; and current treatment with glucocorticoids.
Participants underwent a complete ophthalmological examination in a standardized fashion by the same ophthalmologist (JNB), including DR classification based in 7 standard ETDRS fundus photographs. Central corneal thickness [CCT] and volume were evaluated with the Pentacam® HR Scheimpflug tomographer (Oculus, Wetzlar, Germany; software version 1.20r87) in the low flash intensity automatic release mode. Corneal endothelial morphological properties (central endothelial cell density [cells ⁄ mm2], average cell size [mm2], coefficient of variation [CV] of cell area, and the percentage of hexagonal cells) were assessed using the non-contact specular microscope Topcon® SP-3000P (Topcon, Tokyo, Japan) in the automatic-mode. For each eye, three photographs were taken and independently analyzed using a semi-automated technique, in which the computer program (ImageNet system, version 3.5.5) automatically outlines endothelial cells that are reviewed and corrected manually if necessary. The average of the three measurements was used for each parameter. All measurements were performed in a darkened room between 1 and 7 pm, without cycloplegia, and the patients were told to blink immediately before each examination.
At the end of the visit, all patients carried out vital signs assessment and venous blood sampling for the evaluation of serum HbA1c.
Sample Size Calculation
We hypothesized that patients with longstanding DM would have lower endothelial cell densities compared to non-diabetic subjects. For a type I error of 0.05 and type II error of 0.20 (80% power), considering a mean difference of ECD ≥ 175 cells to be significant and assuming the SD for non-DM group of 300 cells,7 the minimal required sample size would be 47 subjects in each group. We included additional patients in the DM group in order to perform subgroup analysis.
Data and Statistical Analysis
Diabetic subjects were classified into subgroups according to DM duration (<10 and ≥10 years); HbA1c levels (<7.0% and ≥7.0%) and DR (absence or presence of DR). According to patient self-reports, smoking status was evaluated (never smokers and active/former smokers groups). Body mass index (BMI, in kg/m2) was calculated as weight/height2 using measured weight and height.
Statistical analysis was performed using the SPSS® statistical software (version 21.0 for Mac OS; SPSS Inc., Chicago, IL., USA). In the present study, only the fellow non-scheduled eye of each patient undergoing monocular cataract surgery was used for statistical analyses. The Kolmogorov–Smirnov test and normal probability plots were used to confirm the normal distribution of the data. Parametric or non-parametric tests were used for continuous variables comparison between the DM and non-DM groups, according to the normality of data. Chi2 or Fisher´s exact tests were performed for categorical variables comparison. Univariate and multivariate linear regression analyses, using generalized linear models, were performed to identify the potential demographical/clinical (age, gender, body mass index [BMI], DM duration, HbA1c levels, smoking history, systemic hypertension, dyslipidemia) and ocular variables (AL, intraocular pressure, CCT, corneal volume, ECD, DR stage) associated with CCT and ECD. Statistical significance for all the analyses was set at a P value less than 0.05.
Results
Sixty diabetic patients and 47 non-diabetic controls were enrolled in the study. Demographic and clinical characteristics of the study population did not show any significant differences between groups, except for the levels of HbA1c and prevalence of dyslipidemia (Table 1).
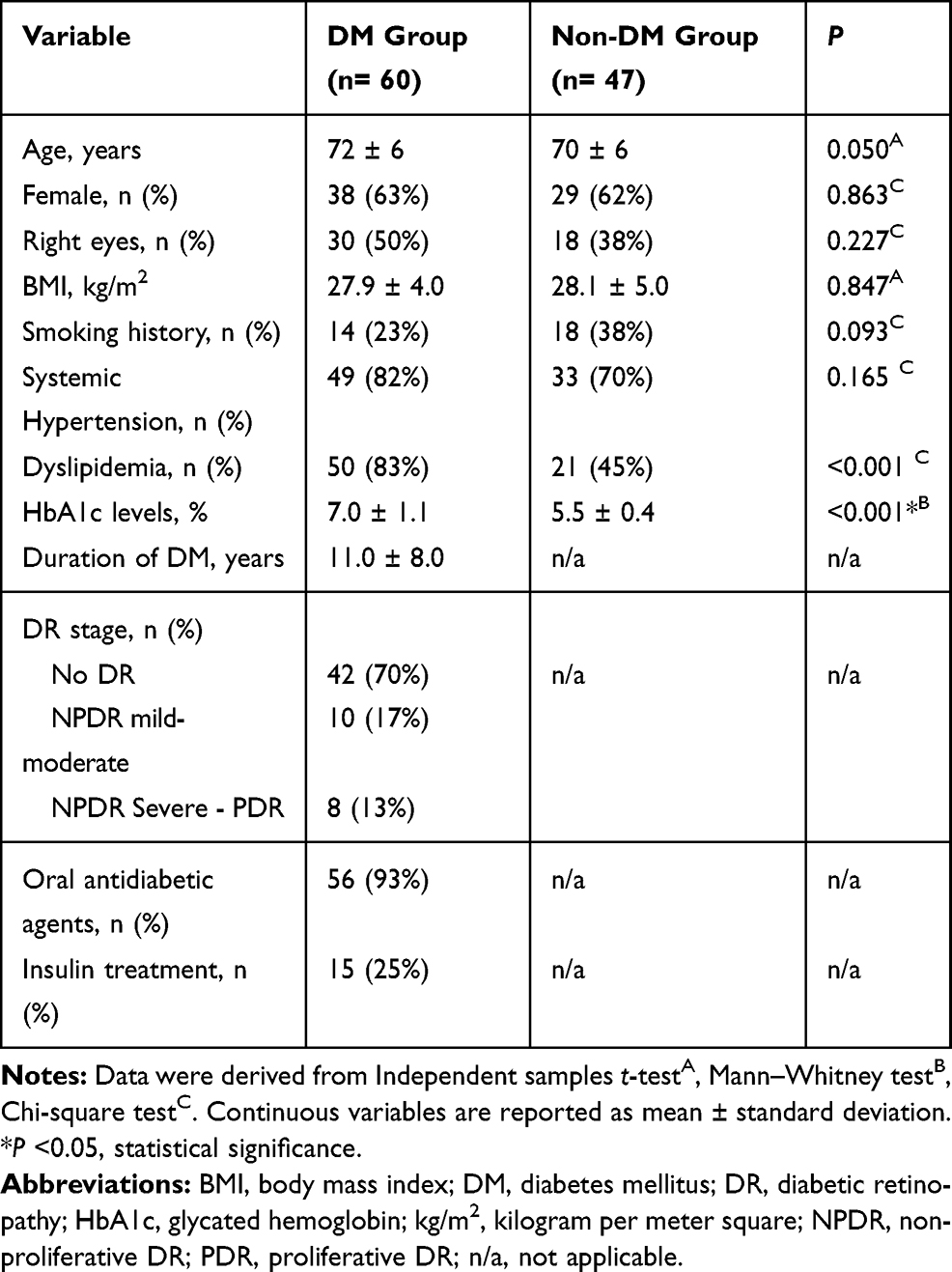 |
Table 1 Demographic and Clinical Characteristics of the Study Population |
In the DM group, duration of DM was significantly associated with HbA1c levels (p=0.004, Chi2 test) and severity of DR (p=0.014, Fisher´s exact test), as well as, severity of DR and HbA1c levels (p=0.028, Fisher´s exact test).
Comparison of Ocular Parameters Between DM and Non-DM Groups
There were no significant differences between groups for any of the studied variables (Table 2), although ECD (mean difference, −73.81 cells; 95% confidence interval [CI], −199.08 to +51.46 cells, p=0.245) was lower in the DM group.
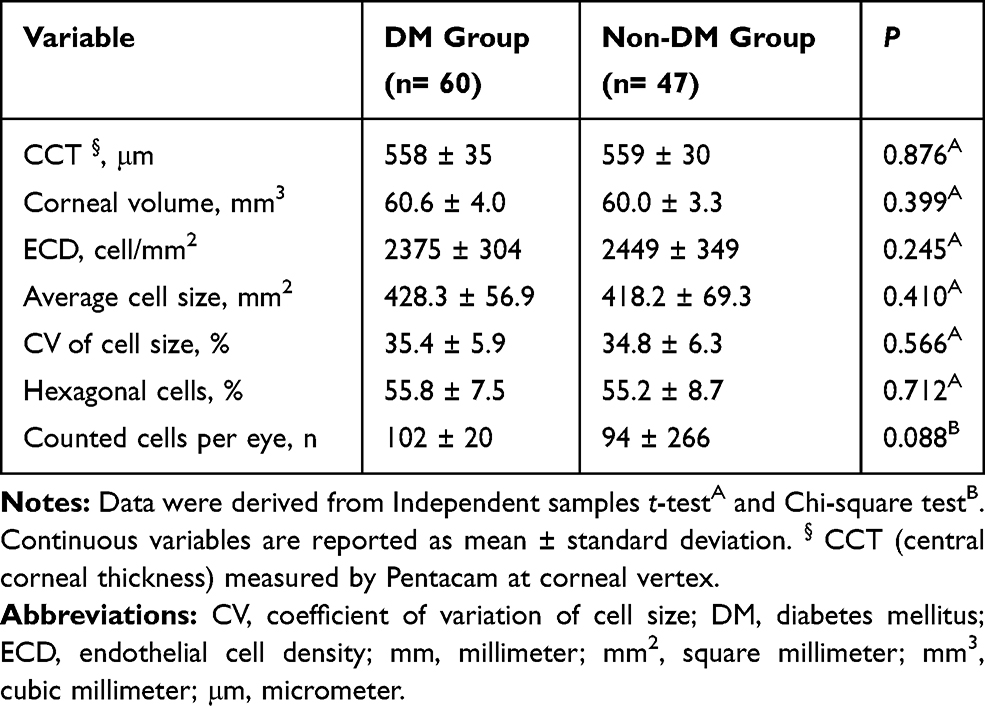 |
Table 2 Ocular Characteristics of the Study Population |
Subgroup Analysis of CCT and ECD in DM Group
Duration of Diabetes
There were no statistically significant differences between groups (DM < or ≥10 years) for any of the corneal variables evaluated (p>0.05, Independent samples t-test; Table 3).
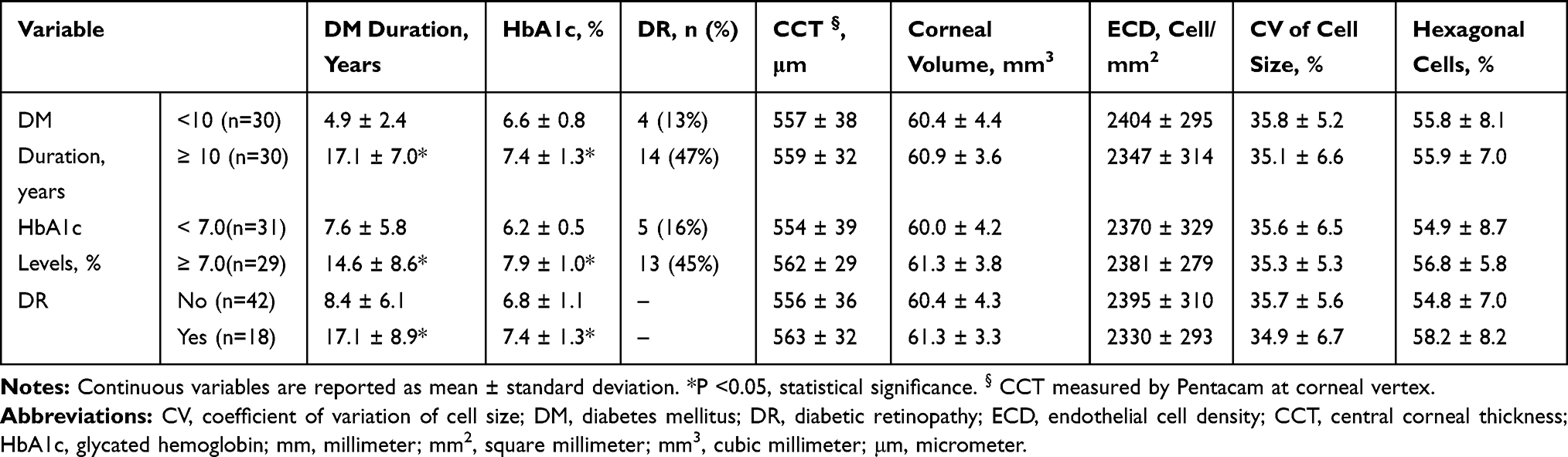 |
Table 3 Subgroup Analysis of Diabetic Patients |
HbA1c Levels
There were no statistically significant differences between groups (HbA1c < or ≥7%) for any of the corneal variables evaluated (p>0.05, Independent samples t-test; Table 3).
DR Stage
There were no statistically significant differences between groups (DM with or without retinopathy) for any of the corneal variables evaluated (p>0.05, Independent samples t-test; Table 3).
Factors Influencing the ECD
Multivariate linear regression analysis showed that older age (p=0.028) was associated with lower ECD (Table 4). In a “fixed model”, patients older than 70 years of age had less 140 endothelial cells compared to patients under 70.
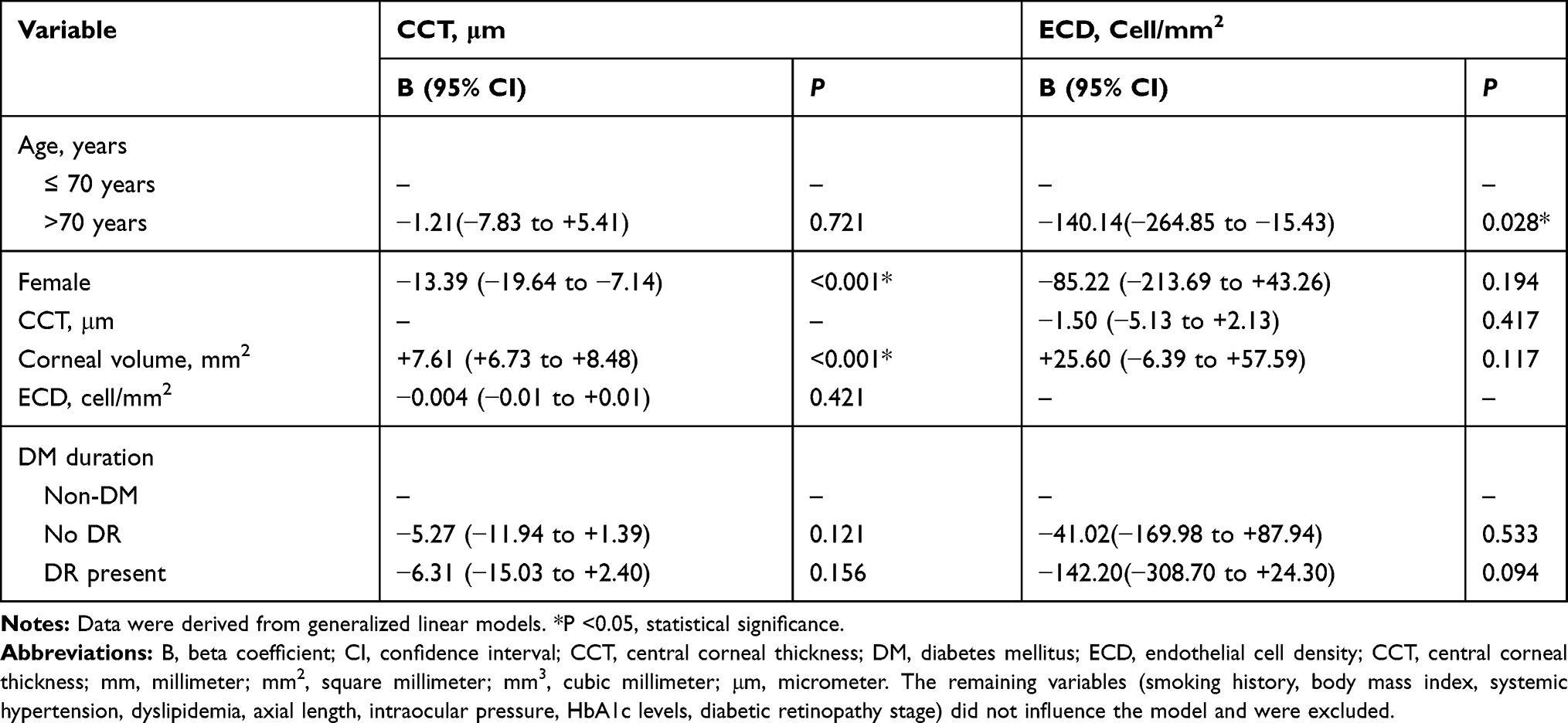 |
Table 4 Multivariate Regression Analysis of the Relative Effects of Clinical and Ocular Characteristics on Endothelial Cell Density (ECD) and Central Corneal Thickness (CCT) |
Factors Influencing the CCT
In multivariate linear regression analysis, CCT was demonstrated to be significantly greater in males (p<0.001) and positively associated with corneal volume (p<0.001). In a “fixed model”, the CCT was found to significantly increase on average 7.6 μm for each increase of 1 mm3 of corneal volume, whereas females are expected to have a significant lower CCT, on average 13.4 μm, in comparison with males (Table 4).
Discussion
This research evaluated the corneal structural and endothelial differences between subjects with and without type 2 DM. The DM group was found to have lower ECD compared to the control group; however, the difference was not statistically significant. In our sample, the ECD was only correlated with age; on the other hand, the CCT was shown to be significantly greater in males and positively associated with corneal volume.
Since the first studies conducted in the early 1980s, extensive literature has been published on the endothelial morphology and corneal thickness changes occurring in diabetic patients (See Supplementary Table 1). However, there have been contradictory results regarding the direct comparisons between them. Since corneal endothelial cells have a limited repair capacity, it is of utmost importance to realize the physical and functional effects of chronic glycemic dysregulation on this structure.
First of all, it is important to note that different definitions of DM were used across studies. Most importantly, the majority of studies relied solely on subjects’ interview for the selection of controls. If this is not a problem in the selection of young individuals for comparison with type 1 DM patients, it might have created an important selection bias of controls for patients with type 2 DM. Additionally, the glycemic status of diabetic patients was not evaluated in several studies.7,14,18,19 In our study, all participants performed HbA1c measurements to avoid patient´ misclassification and allow subgroup analysis of DM patients.
The comparison between studies might be inadequate if different instruments and image analysis techniques are used. This is particularly pertinent in these studies where both contact5,6,19-22 and non-contact8–11,13,16 methods were used for both CCT and ECD measurements. Additionally, automatic,15,19 semi-automatic,9,11,18 and manual8 methods were performed for ECD assessment; with a variable number of acquired images15,22 and counted cells per image.8,11,19,23 In our study, ECD evaluation was performed with a non-contact specular microscope using a semi-automatic technique and a mean of 100 cells were counted in each of the 3 acquired images, thus ensuring an accurate analysis. In turn, CCT measurements were performed with the Pentacam HR, a high reproducible device.
Interpretation difficulties may also arise if subjects´ characteristics, such as type of DM and severity of DR, are not considered. Some of the authors separately analyzed type 1 and 2 DM patients,14,19,21,22 while other studies did not specify6,13,24-26 or mixed type 1 and 2 patients18,20,27 without accounting for the important differences between them, in particular age and DM duration. On the other hand, the mean ages varied widely between studies and this may have been another source of differences. Larsson et al21 and Inoue et al15 did not find statistical differences on endothelial cell density or morphology between type 2 DM subjects and controls and hypothesized that aging could mask the effect of DM on those parameters; however, the studies performed by Sudhir et al7 and Schultz et al14 showed significant lower ECD and greater morphologic abnormalities, respectively, in type 2 DM patients of several age groups.
As in previous studies,10,11,14,21,22,28,29 our results showed a tendency for reduced ECD in type 2 DM patients compared to controls; however, it did not reach statistical significance. The wide individual variation in the possible endothelial structural damage caused by DM23 or a relatively small sample size of the study populations7 could explain the lack of statistical differences between groups. Assuming the same ECD standard deviation of 300 cells, 251 subjects in each group would be required to detect a difference of 75 cells, given a significance level of 5% and a statistical power of 80%.
Selection of appropriate statistical methods is crucial to interpret the effect of related variables on a particular biological outcome, such as ECD and CCT. The use of simple regression analysis may be misleading because it only measures the strength of the relationship between two isolated variables and does not necessarily reflect the real association between them. Using multiple regression analyses, Inoue et al were not able to find any correlation between ECD and the various systemic or ocular factors in a sample of type 2 DM;23 however, Sudhir and colleagues reported a statistically significant reduction of ECD in type 2 DM subjects.7 More recently, Calvo-Maroto et al described that longer duration of type 2 DM was significantly associated lower ECD8 and Storr-Paulsen et al showed an inverse correlation between ECD and HbA1c levels in type 2 DM patients, after controlling for age.11 Unfortunately, this last study did not provide information on disease duration of DM group.
In line with previous studies, older age7,9,15,30 was correlated with greater endothelial loss; however, our analysis failed to demonstrate any significant relationship between ECD and duration of DM,8 HbA1c levels,11 or DR stage;26,27,30 which can be due to the cross-sectional nature of the study, good glycemic control of DM subjects, and the low number of patients included in the more advanced stages of DR. Those patients with longer duration of DM frequently have other ocular and systemic co-morbidities and for that reason many did not meet the selection criteria.
Besides ECD, endothelial morphological parameters might be affected by glycemic dysregulation. Few studies reported lower hexagonality and higher CV of cell size in subjects with type 2 DM compared to controls,14,19,27,31,32 but our study, like others, found them to be comparable.7,11,15,25,26
Regarding corneal structure, there is still no agreement on the effect of DM on CCT measurements. Few authors reported thicker corneas among diabetic patients,8,9,11,16,18,19 while others showed similar values to controls.7,10,21-23,25,26,28,31,32 Some of the reasons for these variations have been pointed out previously, but it should be stressed that only a limited number of studies accounted for the overnight corneal swelling effect or diurnal variation of CCT.8,9,16,22 In the current study, the presence of type 2 DM was irrelevant to CCT measurements. As previously discussed by Storr-Paulsen and colleagues, the small differences found in most studies may not be clinically relevant in well-controlled diabetics with ECD within normal range and no corneal edema.11
Our multivariate analysis confirmed that CCT was greater in males and positively correlated with corneal volumes.33 Though, it was not possible to demonstrate any significant relation with age,11 DM duration,8,18 or HbA1c levels,8 probably for the same reasons discussed above in ECD analysis.
The present study has several strengths but also some limitations. Considering that only corneal anatomic features were evaluated, it is not possible to conclude about the endothelium functional differences between diabetic subjects and controls. Another drawback is that the time from onset to diagnosis of type 2 DM is unknown in most patients. Nevertheless, that interval could have been minimized in our study since all patients regularly attended primary care physicians.
In summary, the present study did not find any statistically significant differences between the corneal structural and endothelial characteristics of diabetic and non-diabetic subjects. Other demographical variables, such as age and gender, seem to be more determinant for the corneal properties. Further prospective studies with sufficient statistical power and well-defined diabetic and control groups might clarify the role of long-term poor glycemic control on the corneal structural and endothelial changes.
Ethics
Project number: CES 285-15, approved by the Research Ethics Committee of Hospital São João.
Acknowledgment
Meeting presentation: Congress of the European Society of Ophthalmology (SEO), Barcelona, Spain, 10–13th June 2017.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sady C, Khosrof S, Nagaraj R. Advanced Maillard reaction and crosslinking of corneal collagen in diabetes. Biochem Biophys Res Commun. 1995;214(3):793–797. doi:10.1006/bbrc.1995.2356
2. Whikehart DR, Montgomery B, Angelos P, Sorna D. Alteration of ATPase activity and duplex DNA in corneal cells grown in high glucose media. Cornea. 1993;12(4):295–298. doi:10.1097/00003226-199307000-00004
3. Hugod M, Storr-Paulsen A, Norregaard JC, Nicolini J, Larsen AB, Thulesen J. Corneal endothelial cell changes associated with cataract surgery in patients with type 2 diabetes mellitus. Cornea. 2011;30(7):749–753. doi:10.1097/ICO.0b013e31820142d9
4. Morikubo S, Takamura Y, Kubo E, Tsuzuki S, Akagi Y. Corneal changes after small-incision cataract surgery in patients with diabetes mellitus. Arch Ophthalmol. 2004;122(7):966–969. doi:10.1001/archopht.122.7.966
5. McNamara NA, Brand RJ, Polse KA, Bourne WM. Corneal function during normal and high serum glucose levels in diabetes. Invest Ophthalmol Vis Sci. 1998;39(1):3–17.
6. Weston BC, Bourne WM, Polse KA, Hodge DO. Corneal hydration control in diabetes mellitus. Invest Ophthalmol Vis Sci. 1995;36(3):586–595.
7. Sudhir RR, Raman R, Sharma T. Changes in the corneal endothelial cell density and morphology in patients with type 2 diabetes mellitus: a population-based study, Sankara Nethralaya Diabetic Retinopathy and Molecular Genetics Study (SN-DREAMS, Report 23). Cornea. 2012;31(10):1119–1122. doi:10.1097/ICO.0b013e31823f8e00
8. Calvo-Maroto AM, Cervino A, Perez-Cambrodi RJ, Garcia-Lazaro S, Sanchis-Gimeno JA. Quantitative corneal anatomy: evaluation of the effect of diabetes duration on the endothelial cell density and corneal thickness. Ophthalmic Physiol Opt. 2015;35(3):293–298. doi:10.1111/opo.12191
9. Briggs S, Osuagwu UL, AlHarthi EM. Manifestations of type 2 diabetes in corneal endothelial cell density, corneal thickness and intraocular pressure. J Biomed Res. 2015;30:46.
10. El-Agamy A, Alsubaie S. Corneal endothelium and central corneal thickness changes in type 2 diabetes mellitus. Clin Ophthalmol. 2017;11:481–486. doi:10.2147/OPTH.S126217
11. Storr-Paulsen A, Singh A, Jeppesen H, Norregaard JC, Thulesen J. Corneal endothelial morphology and central thickness in patients with type II diabetes mellitus. Acta Ophthalmol. 2014;92(2):158–160. doi:10.1111/aos.12064
12. Mathew PT, David S, Thomas N. Endothelial cell loss and central corneal thickness in patients with and without diabetes after manual small incision cataract surgery. Cornea. 2011;30(4):424–428. doi:10.1097/ICO.0b013e3181eadb4b
13. He X, Diakonis VF, Alavi Y, Yesilirmak N, Waren D, Donaldson K. Endothelial cell loss in diabetic and nondiabetic eyes after cataract surgery. Cornea. 2017;36(8):948–951. doi:10.1097/ICO.0000000000001245
14. Schultz RO, Matsuda M, Yee RW, Edelhauser HF, Schultz KJ. Corneal endothelial changes in type I and type II diabetes mellitus. Am J Ophthalmol. 1984;98(4):401–410. doi:10.1016/0002-9394(84)90120-X
15. Inoue K, Tokuda Y, Inoue Y, Amano S, Oshika T, Inoue J. Corneal endothelial cell morphology in patients undergoing cataract surgery. Cornea. 2002;21(4):360–363. doi:10.1097/00003226-200205000-00006
16. Galgauskas S, Laurinaviciute G, Norvydaite D, Stech S, Asoklis R. Changes in choroidal thickness and corneal parameters in diabetic eyes. Eur J Ophthalmol. 2016;26(2):163–167. doi:10.5301/ejo.5000677
17. Beato JN, Esteves-Leandro J, Reis D, et al. Structural and biomechanical corneal differences between type 2 diabetic and nondiabetic patients. J Ophthalmol. 2019;2019:3764878. doi:10.1155/2019/3764878
18. Lee JS, Oum BS, Choi HY, Lee JE, Cho BM. Differences in corneal thickness and corneal endothelium related to duration in diabetes. Eye. 2006;20(3):315–318. doi:10.1038/sj.eye.6701868
19. Roszkowska AM, Tringali CG, Colosi P, Squeri CA, Ferreri G. Corneal endothelium evaluation in type I and type II diabetes mellitus. Ophthalmologica J Int D’ophtalmologie Int J Ophthalmol Z Augenheilkunde. 1999;213(4):258–261. doi:10.1159/000027431
20. Janiec S, Rzendkowski M, Bolek S. The relation between corneal autofluorescence, endothelial cell count and severity of the diabetic retinopathy. Int Ophthalmol. 1994;18(4):205–209. doi:10.1007/BF00951798
21. Larsson LI, Bourne WM, Pach JM, Brubaker RF. Structure and function of the corneal endothelium in diabetes mellitus type I and type II. Arch Ophthalmol. 1996;114(1):9–14. doi:10.1001/archopht.1996.01100130007001
22. Modis L
23. Inoue K, Kato S, Inoue Y, Amano S, Oshika T. The corneal endothelium and thickness in type II diabetes mellitus. Jpn J Ophthalmol. 2002;46(1):65–69. doi:10.1016/S0021-5155(01)00458-0
24. Itoi M, Nakamura T, Mizobe K, Kodama Y, Nakagawa N, Itoi M. Specular microscopic studies of the corneal endothelia of Japanese diabetics. Cornea. 1989;8(1):2–6. doi:10.1097/00003226-198903000-00002
25. Siribunkum JKP, Singalavanija A, Singalavanija A. Corneal abnormalities in diabetes. J Med Assoc Thai. 2001;84(8):1075–1083.
26. Colak S, Kazanci B, Ozcelik Soba D, Ozdamar Erol Y, Yilmazbas P. Effects of diabetes duration and HgA1C level on corneal endothelial morphology. Eur J Ophthalmol. 2020;1120672120914812.
27. Shenoy R, Khandekar R, Bialasiewicz A, Al Muniri A. Corneal endothelium in patients with diabetes mellitus: a historical cohort study. Eur J Ophthalmol. 2009;19(3):369–375. doi:10.1177/112067210901900307
28. Misra SL, Goh YW, Patel DV, Riley AF, McGhee CN. Corneal microstructural changes in nerve fiber, endothelial and epithelial density after cataract surgery in patients with diabetes mellitus. Cornea. 2015;34(2):177–181. doi:10.1097/ICO.0000000000000320
29. Matsuda M, Ohguro N, Ishimoto I, Fukuda M. Relationship of corneal endothelial morphology to diabetic retinopathy, duration of diabetes and glycemic control. Jpn J Ophthalmol. 1990;34(1):53–56.
30. Durukan I. Corneal endothelial changes in type 2 diabetes mellitus relative to diabetic retinopathy. Clin Exp Optom. 2019.
31. Choo M, Prakash K, Samsudin A, Soong T, Ramli N, Kadir A. Corneal changes in type II diabetes mellitus in Malaysia. Int J Ophthalmol. 2010;3(3):234–236. doi:10.3980/j.issn.2222-3959.2010.03.12
32. Dhasmana R, Singh IP, Nagpal RC. Corneal changes in diabetic patients after manual small incision cataract surgery. J Clin Diagn Res. 2014;8(4):VC03–VC06. doi:10.7860/JCDR/2014/7955.4288
33. Elflein HM, Pfeiffer N, Hoffmann EM, et al. Correlations between central corneal thickness and general anthropometric characteristics and cardiovascular parameters in a large European cohort from the Gutenberg Health Study. Cornea. 2014;33(4):359–365. doi:10.1097/ICO.0000000000000068
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.