Back to Journals » Cancer Management and Research » Volume 12
Evaluation of Contrast-Enhanced Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) in the Detection of Retropharyngeal Lymph Node Metastases in Nasopharyngeal Carcinoma Patients
Authors Chen J, Luo J, He X ![]() , Zhu C
, Zhu C ![]()
Received 29 December 2019
Accepted for publication 21 February 2020
Published 9 March 2020 Volume 2020:12 Pages 1733—1739
DOI https://doi.org/10.2147/CMAR.S244034
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chien-Feng Li
Jie Chen,1 Jingwen Luo,2 Xia He,3 Chenjing Zhu3
1Department of Oncology, Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 2Department of Oncology, West China School of Medicine, West China Hospital, Sichuan University, Chengdu, People’s Republic of China; 3Department of Radiation Oncology, Jiangsu Cancer Hospital & Jiangsu Institute of Cancer Research & The Affiliated Cancer Hospital of Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China
Correspondence: Xia He; Chenjing Zhu
Department of Radiation Oncology, Jiangsu Cancer Hospital & Jiangsu Institute of Cancer Research & The Affiliated Cancer Hospital of Nanjing Medical University, Nanjing, Jiangsu Tel/Fax +86-28-85475576
Email [email protected]; [email protected]
Introduction: We performed this study to explore the diagnostic accuracies and cutoff values of contrast-enhanced computed tomography (CT) and magnetic resonance imaging (MRI) for the detection and diagnosis of metastatic retropharyngeal lymph nodes (RLNs) in patients with nasopharyngeal carcinoma (NPC).
Methods: One hundred and twenty-eight patients with a total of 159 RLNs were included in the study. The sizes of maximal and minimal axial diameters of each node on both contrast-enhanced CT and MRI images were measured. The characteristics of the RLNs (malignant or benign), as well as the survival of patients, were classified based on the results of follow-up MRI.
Results: RLN size cutoffs of 4– 11 mm for minimal axial diameter were used. We found that MRI showed higher sensitivity while CT demonstrated higher specificity. The reasonable criterion for the diagnosis of metastatic RLNs in MRI was a minimal axial diameter of ≥ 6 mm, which yielded a sensitivity, specificity and diagnostic odds ratio (DOR) of 0.71, 0.82 and 10.88.
Conclusion: The radiologic criteria that should be used for the assessment of RLN metastases in NPC patients are nodes with a minimal axial diameter of ≥ 6 mm on MR images.
Keywords: retropharyngeal lymph node, metastasis, nasopharyngeal carcinoma, cutoff, MRI
Introduction
Nasopharyngeal carcinoma (NPC) is a common malignancy in Southeast Asia where the age-standardized rate of NPC incidence was 21 per 100,000 person-years, whereas the incidence in other parts of the world was only less than 1 per 100,000 person-years.1 Retropharyngeal lymph nodes (RLNs), located within the retropharyngeal space and bound anteriorly by the middle layer of the deep cervical fascia, posteriorly by the prevertebral fascia, and laterally by the carotid sheath,2,3 were regarded as sentinel lymph nodes in NPC patients. Metastasis to RLNs was an important prognostic factor in head and neck cancers. However, due to their relatively deep anatomical locations2 and their complicated surgical dissections,4 biopsy and surgical removal were not easy to be operated. In such cases, imaging assessment was important for the diagnosis of RLN pathologies.5
The imaging examinations of RLNs in patients with NPC could be made on the basis of several radiologic modalities, such as computed tomography (CT), positron emission tomography (PET), and magnetic resonance imaging (MRI). In the diagnosis of local and metastatic nasopharyngeal carcinomas, a recent meta-analysis suggested that CT showed good accuracy in the diagnosis of N stage, while MRI had good accuracy in diagnosis of T stage.6 In clinical practice, MRI was the preferred method for evaluating the soft tissues of the head and neck with high soft-tissue discrimination,7 and Kato et al have reported that MRI was superior to CT for detecting metastatic RLNs with high contrast resolution and the metallic artifacts were less severe in MR imaging.5
However, the radiologic criteria for the size of a RLN are contentious, and different RLN size criteria have been suggested. Lam et al took 4 mm as the upper limit of normal RLN.8 A minimal axial diameter of 5 mm was also proposed as abnormal for RLNs in patients with NPC.9,10 Zhang et al11 and Li et al12 reported that nodes with a minimal axial diameter 6 mm or larger should be used for assessment of RLN metastases. Given these uncertainties, it remains important to define the size criteria. Our study aimed to compare CT and MRI for detecting RLN metastasis and to establish the diagnostic criteria in patients with NPC.
Materials and Methods
Patients
From February 1, 2016 to January 1, 2019 we searched the electronic medical chart system of Jiangsu Cancer Hospital, China, for pathologically confirmed and previously untreated NPC patients. One hundred and twenty-eight patients were enrolled in our analyses. All these patients underwent both contrast-enhanced CT and MR imaging before chemoradiotherapy. Initial image modality for reference standard of positive vs negative RLN was MRI. The interval between contrast-enhanced CT and MRI examinations for the same patient was no more than 1 month. Written informed consent was obtained from each individual participant and the experimental protocol was approved by the Clinical Research Ethics Committee of Jiangsu Cancer Hospital. This study was conducted in accordance with the Declaration of Helsinki.
Imaging Protocol
The CT examinations were performed on a multi-detector computed tomography (MDCT) scanner (Somatom Definition, Siemens AG, Medical Solutions, Forchheim, Germany). All patients underwent CT scan with coverage from the skull vertex to 2 cm below the inferior margin of the clavicle. Contrast-enhanced planning CT scans with a 3-mm slide thickness were obtained after an intravenous bolus injection of 100 mL of monomeric nonionic contrast media (250 mg iodine/mL) at an injection rate of 2 mL/sec.
MR examination was performed with a 1.5 Tesla scanner (Achieva, Phillips Medical Systems, Netherlands) on patients for head and neck imaging. The examined area extended from the suprasellar subarachnoid cistern to the inferior margin of the sternal end of the clavicle using a head-and-neck coil. Before the injection of contrast material, unenhanced T1-weighted images in the axial plane, and axial, coronal and sagittal T2-weighted images were obtained. After the intravenous administration of gadolinium-complexed diethylene triamine pentaacetic acid (Gd-DTPA, 0.1 mmol/kg body weight, injection rate: 1.5 mL/s), fat-suppressed T1-weighted spin-echo images were performed sequentially, with the same parameters that were used before Gd-DTPA injection. The section thickness was 5 mm and intersection gap was 1 mm.
Treatment and Follow-Up
After tumor assessments performed by CT or MRI at baseline, all patients received image-based intensity-modulated radiotherapy (IMRT). The technique and dose of radiotherapy was in consistent with the NCCN guidelines. Therapeutic responses were evaluated by follow-up MRI.
Image Assessment
An experienced general radiologist (10 years of post-training experience in head and neck imaging) and an oncological radiologist (8 years of post-training experience) separately reviewed all the MR images with the electronic calipers in the PACS (Centricity Radiology RA600, GE Healthcare). They both were unaware of the information of patients including the names, laboratory results, or clinical diagnoses of patients. Any disagreements were resolved by discussion with a third author.
The minimum axial diameter, as well as the maximum axial diameter which was perpendicular to the course of the internal jugular vein of each visible RLN, were measured. The minimum axial diameter corresponded to the widest diameter of the node in the axial plane that was perpendicular to its maximum axial diameter. Axial diameter measurements were made mainly using T2-weighted axial images.12
Statistical Analysis
Cutoff values from 4 mm to 11 mm were used. True positive (TP), true negative (TN), false positive (FP), and false negative (FN) were calculated according to the different size criteria. A summary of sensitivity, specificity, positive likelihood ratios (PLR), negative likelihood ratios (NLR) and diagnostic odds ratio (DOR) with corresponding 95% confidence intervals (CIs) were yielded by TP, FP, FN and TN for CT and MRI.
In addition, we used the receiver operating characteristic (ROC) curve and the overall area under the curve (AUC) of ROC to determine the diagnostic performance of these two imaging modalities in the detection of metastatic RLNs, and to assess the effectiveness of different size criteria. The closer the area is to 1.0, the better the diagnostic test is.13 The left-upper point of ROC curve is considered the best diagnostic cutoff value. All the above statistical analyses were performed by Meta-Disc Version 1.4 and SPSS 17.0 (SPSS Inc., Chicago, IL, USA).
Results
Assessment of RLNs
Among the 128 patients with NPC, a total of 159 RLNs were assessed. One hundred and fifty-eight lateral RLNs were detected on gadolinium-enhanced T2-weighted images and contrast-enhanced CT images, and only one medial RLN was observed.
Treatment results were assessed by central imaging vendor review using Response Evaluation Criteria in Solid Tumors, version 1.1 (RECIST v1.1). Complete response (CR) was defined as the disappearance of all lesions. Duration of response was the interval from first RECIST v1.1–recorded response to progressive disease in patients who achieved at least a partial response.
A decrease in the sum of target disease of ≥30% represents partial response (PR),14 progressive disease (PD) is an increase in sum of target disease ≥20%, or the development of a new lesion, and stable disease lies between partial response and progressive disease. Accordingly, a positive or malignant RLN was considered if it resolved after the completion of radiotherapy or progressed during the follow-up MRI, whereas a negative or benign RLN was stable in size after radiotherapy and the patient remained disease-free during the subsequent follow-up.15
We identified 13 benign (8.7%) and 146 malignant (91.93%) RLNs. The mean values of the minimal axial, maximal axial, and longitudinal diameters of the malignant RLNs were all greater than those of the benign RLNs. The minimum diameter of RLNs on CT was ≥3 mm whereas on MRI was ≥2.2 mm. Complete resolution occurred in 128 (80.50%) lymph nodes and partial resolution occurred in 17 (10.69%) RLNs. One (0.63%) lymph nodes showed progressive disease. Thirteen lymph nodes remained stable and had no evidence of progressive disease at follow-up MRI.
Comparison of MRI and Contrast-Enhanced CT
Size criteria from ≥4 mm to ≥11 mm for minimal axial diameter was used to identify lymph node metastases. TP referred to the positive lymph nodes that were correctly labeled while FP were the negative lymph nodes that were incorrectly labeled as positive. The sensitivity, specificity, PLR, NLR and DOR of these cutoffs of different size criteria were calculated accordingly (Tables 1 and 2). MRI showed higher sensitivity while CT demonstrated higher specificity (Figure 1). The AUC for the detection of metastatic RLNs is shown in Tables 1 and 2. The mean AUCs for contrast-enhanced CT and MRI were 0.6938 (standard error 0.0666) and 0.8554 (standard error 0.0332), respectively, which suggested that MRI was more accurate for the diagnosis of RLN metastases.
 |
Table 1 The Sensitivity, Specificity, DOR, PLR, NLR and AUC for Several Cutoffs of Different Size Criteria for Contrast-Enhanced CT |
 |
Table 2 The Sensitivity, Specificity, DOR, PLR, NLR and AUC for Several Cutoffs of Different Size Criteria for MRI |
 |
Figure 1 (A) Sensitivity, (B) specificity for contrast-enhanced computed tomography (CT) and (C) sensitivity, (D) specificity for magnetic resonance imaging (MRI) in the diagnosis of metastatic retropharyngeal lymph node. Abbreviation: CI, confidence interval. |
Cutoff Values of RLN Metastases
The ROC curves of the minimal axial diameter showed great effectiveness in the detection of metastatic RLNs (Figure 2). Of all the size criteria, a minimal axial diameter of ≥6 mm was the most accurate criterion to assess RLN involvement. For MRI, the sensitivity, specificity, PLR, NLR and DOR of this criterion were 0.71 (95% CI 0.63–0.78), 0.82 (95% CI 0.48–0.98), 3.89 (95% CI 1.11–13.69), 0.36 (95% CI 0.25–0.52) and 10.88 (95% CI 2.26–52.46), respectively. Compared with the commonly used criteria of a minimal axial diameter of ≥5 mm, the sensitivities of a minimal axial diameter of ≥6 mm versus ≥5 mm were 0.71 (95% CI 0.63–0.78) versus 0.93 (95% CI 0.87–0.96), and the specificities were 0.82 (95% CI 0.48–0.98) versus 0.50 (95% CI 0.16–0.84). Meanwhile, for contrast-enhanced CT, the minimum axial diameter of 6 mm was also the most effective with the sensitivity, specificity, PLR, NLR and DOR of 0.55 (95% CI 0.47–0.63), 0.86 (95% CI 0.42–1.00), 3.87 (95% CI 0.63–23.88), 0.52 (95% CI 0.37–0.74) and 7.41 (95% CI 0.87–63.06), respectively.
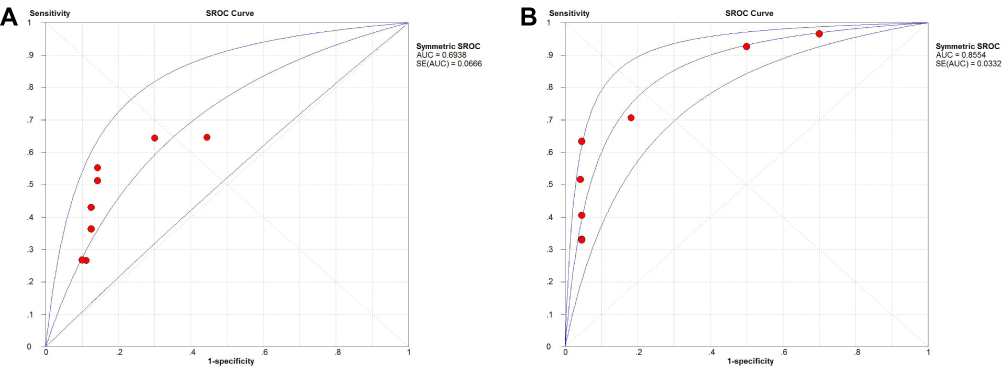 |
Figure 2 Summary receiver operating characteristic (SROC) curve for (A) contrast-enhanced computed tomography (CT) and (B) magnetic resonance imaging (MRI). Abbreviations: AUC, area under the curve; SE, standard deviation. |
Discussion
Size of the lymph node is the most frequently used criteria for differential diagnosis. The minimal axial diameter was superior to the maximal axial diameter in the diagnosis of RLN metastases.16 Since very different diagnostic criteria have been utilized in relevant studies about metastatic RLNs in NPC patients, leading to the occurrence of false positive or false negative results, it is warranted to determine the unified criteria that are most appropriate.
Previous published reports9,10,17,18 have used the criterion of a minimal axial diameter of 4 or 5 mm for a radiologic diagnosis of abnormal RLNs. Our study was in consistent with a previous study11 that proposed a minimum axial diameter of 6 mm as the cutoff between normal and abnormal RLNs, and the best clinical prediction was obtained using this criterion.12 RLNs ≥6 mm were associated with tumor proliferation, resulting in an increased risk of distant metastasis and decreased OS and DMFS.19 Since head and neck radiation represented a therapeutic challenge given their proximity to radiosensitive structures, in particular, the parotid gland, the posterior pharyngeal wall and the pharyngeal constrictor muscles,20,21 it was necessary to determine whether certain lymph node was in need of radiotherapy for reducing potential harm to other organs. Based on the criteria above, even if the tumors were in stage T1 or T2, it was suggested that NPC patients with RLNs ≥6 mm and no distant metastases underwent concurrent chemoradiotherapy or induction chemotherapy.22,23
In the detection of many tumors, MR imaging provided considerably superior soft-tissue images in contrast to that of non-contrast-enhanced CT. However, for contrast-enhanced CT, Bipat et al reported that no significant difference between contrast-enhanced CT and 1.5-T MRI (63.8 and 64.4%, respectively) was observed for colorectal liver metastases.24 A comparison of contrast-enhanced CT and MRI for predicting the malignant potential of intraductal papillary mucinous neoplasm (IPMN) of the pancreas also suggested that the diagnostic performance for predicting malignant IPMNs was comparable with each modality without significant difference.25 PET/CT has also been applied in detecting lymph node; however, it was reported that PET/CT was inferior to enhanced CT for detecting RLN metastases in NPC patients, especially in those with a minimum axial diameter of <1 cm and those near the primary tumor.27,28 In our study, MRI were more accurate for the diagnosis of RLN metastases with an AUC of 0.8554 than contrast-enhanced CT which had an AUC of 0.6938. The great soft-tissue contrast of MRI not only allows for the differentiation of individual RLN from adjacent normal structures,26 but also permits the identification of small RLNs.
There are several limitations in our study. Firstly, the sample size of lymph nodes examined was relatively small. Therefore, the comparison of sensitivity and specificity between contrast-enhanced CT and MRI and the cutoff value of metastatic RLNs in MRI still should be verified in subsequent studies. Secondly, the deep anatomic location prevented pathological confirmation of the nature of the lymph node. Although it was very much likely that RLN ≥ 6 mm be malignant and ≤6 mm be benign, false negative and false positive diagnoses might be induced. Thirdly, enlarged RLNs were sometimes hard to differ from primary tumor because of the adjacent location and even the same signal intensity on radiological images. Furthermore, even MRI was not able to fully depict all of the small RLNs metastases.
In conclusion, MRI was more accurate than CT in the detection of RLN metastases in NPC Patients. The criterion for MRI based on a minimal axial diameter of 6 mm or larger was the most accurate, which might be useful in planning treatment regimens. The diagnostic criteria for CT on the size of metastatic lymph nodes was also suggested as 6 mm. However, further studies are still needed to confirm our results.
Compliance with Ethical Standards
Research involving Human Participants: Written informed consent was obtained from each individual participant and the experimental protocol was approved by the Clinical Research Ethics Committee of Jiangsu Cancer Hospital. This study was conducted in accordance with the Declaration of Helsinki.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chua ML, Wee JT, Hui EP, Chan AT. Nasopharyngeal carcinoma. Lancet. 2016;387(10022):1012–1024. doi:10.1016/S0140-6736(15)00055-0
2. Tang C, Komakula S, Chan C, et al. Radiologic assessment of retropharyngeal node involvement in oropharyngeal carcinomas stratified by HPV status. Radiother Oncol. 2013;109(2):293–296. doi:10.1016/j.radonc.2013.09.001
3. Coskun HH, Ferlito A, Medina JE, et al. Retropharyngeal lymph node metastases in head and neck malignancies. Head Neck. 2011;33(10):1520–1529. doi:10.1002/hed.v33.10
4. Chu HR, Kim JH, Yoon DY, Hwang HS, Rho YS. Additional diagnostic value of (18)F-FDG PET-CT in detecting retropharyngeal nodal metastases. Otolaryngol Head Neck Surg. 2009;141(5):633–638. doi:10.1016/j.otohns.2009.08.008
5. Kato H, Kanematsu M, Watanabe H, Mizuta K, Aoki M. Metastatic retropharyngeal lymph nodes: comparison of CT and MR imaging for diagnostic accuracy. Eur J Radiol. 2014;83(7):1157–1162. doi:10.1016/j.ejrad.2014.02.027
6. Chen WS, Li JJ, Hong L, Xing ZB, Wang F, Li CQ. Comparison of MRI, CT and 18F-FDG PET/CT in the diagnosis of local and metastatic of nasopharyngeal carcinomas: an updated meta analysis of clinical studies. Am J Transl Res. 2016;8(11):4532–4547.
7. Guenzel T, Franzen A, Wiegand S, et al. The value of PET compared to MRI in malignant head and neck tumors. Anticancer Res. 2013;33(3):1141–1146.
8. Lam WW, Chan YL, Leung SF, Metreweli C. Retropharyngeal lymphadenopathy in nasopharyngeal carcinoma. Head Neck. 1997;19(3):176–181.
9. Liu LZ, Zhang GY, Xie CM, Liu XW, Cui CY, Li L. Magnetic resonance imaging of retropharyngeal lymph node metastasis in nasopharyngeal carcinoma: patterns of spread. Int J Radiat Oncol Biol Phys. 2006;66(3):721–730. doi:10.1016/j.ijrobp.2006.05.054
10. Tang L, Li L, Mao Y, et al. Retropharyngeal lymph node metastasis in nasopharyngeal carcinoma detected by magnetic resonance imaging: prognostic value and staging categories. Cancer. 2008;113(2):347–354. doi:10.1002/cncr.v113:2
11. Zhang GY, Liu LZ, Wei WH, Deng YM, Li YZ, Liu XW. Radiologic criteria of retropharyngeal lymph node metastasis in nasopharyngeal carcinoma treated with radiation therapy. Radiology. 2010;255(2):605–612. doi:10.1148/radiol.10090289
12. Li YZ, Xie CM, Wu YP, et al. Nasopharyngeal carcinoma patients with retropharyngeal lymph node metastases: a minimum axial diameter of 6 mm is a more accurate prognostic predictor than 5 mm. AJR Am J Roentgenol. 2015;204(1):20–23. doi:10.2214/AJR.14.12936
13. Habibzadeh F, Habibzadeh P, Yadollahie M. On determining the most appropriate test cut-off value: the case of tests with continuous results. Biochem Med (Zagreb). 2016;26(3):297–307. doi:10.11613/issn.1846-7482
14. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–247. doi:10.1016/j.ejca.2008.10.026
15. Yen TC, Chang YC, Chan SC, et al. Are dual-phase 18F-FDG PET scans necessary in nasopharyngeal carcinoma to assess the primary tumour and loco-regional nodes. Eur J Nucl Med Mol Imaging. 2005;32(5):541–548. doi:10.1007/s00259-004-1719-2
16. van den Brekel MW, Stel HV, Castelijns JA, et al. Cervical lymph node metastasis: assessment of radiologic criteria. Radiology. 1990;177(2):379–384. doi:10.1148/radiology.177.2.2217772
17. Ma J, Liu L, Tang L, et al. Retropharyngeal lymph node metastasis in nasopharyngeal carcinoma: prognostic value and staging categories. Clin Cancer Res. 2007;13(5):1445–1452. doi:10.1158/1078-0432.CCR-06-2059
18. King AD, Ahuja AT, Leung SF, et al. Neck node metastases from nasopharyngeal carcinoma: MR imaging of patterns of disease. Head Neck. 2000;22(3):275–281. doi:10.1002/(SICI)1097-0347(200005)22:3<275::AID-HED10>3.0.CO;2-N
19. Cheng SH, Jian JJ, Tsai SY, et al. Long-term survival of nasopharyngeal carcinoma following concomitant radiotherapy and chemotherapy. Int J Radiat Oncol Biol Phys. 2000;48(5):1323–1330. doi:10.1016/S0360-3016(00)00779-3
20. Grégoire V, Levendag P, Ang KK, et al. CT-based delineation of lymph node levels and related CTVs in the node-negative neck: DAHANCA, EORTC, GORTEC, NCIC,RTOG consensus guidelines. Radiother Oncol. 2003;69(3):227–236. doi:10.1016/j.radonc.2003.09.011
21. Feng FY, Kim HM, Lyden TH, et al. Intensity-modulated chemoradiotherapy aiming to reduce dysphagia in patients with oropharyngeal cancer: clinical and functional results. J Clin Oncol. 2010;28(16):2732–2738. doi:10.1200/JCO.2009.24.6199
22. Blanchard P, Baujat B, Holostenco V, et al. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): a comprehensive analysis by tumour site. Radiother Oncol. 2011;100(1):33–40. doi:10.1016/j.radonc.2011.05.036
23. Pignon JP, Le Maitre A, Maillard E, Bourhis J. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): an update on 93 randomised trials and 17,346 patients. Radiother Oncol. 2009;92(1):4–14. doi:10.1016/j.radonc.2009.04.014
24. Bipat S, van Leeuwen MS, Comans EF, et al. Colorectal liver metastases: CT, MR imaging, and PET for diagnosis–meta-analysis. Radiology. 2005;237(1):123–131. doi:10.1148/radiol.2371042060
25. Choi SY, Kim JH, Yu MH, Eun HW, Lee HK, Han JK. Diagnostic Performance and Imaging Features for Predicting the Malignant Potential of Intraductal Papillary Mucinous Neoplasm of the Pancreas: A Comparison of EUS, Contrast-Enhanced CT and MRI. Abdom Radiol (NY); 2017.
26. Johnson PJ, Elders R, Pey P, Dennis R. Clinical and magnetic resonance imaging features of inflammatory versus neoplastic medial retropharyngeal lymph node mass lesions. Vet Radiol Ultrasound. 2016;57(5):557. doi:10.1111/vru.2016.57.issue-5
27. Tang LL, Ma J, Chen Y, et al. [The values of MRI, CT, and PET-CT in detecting retropharyngeal lymph node metastasis of nasopharyngeal carcinoma]. Ai Zheng. 2007;26(7):737–741. Chinese.
28. Wu IS, Hung GU, Chang BL, et al. Is unenhanced 18F-FDG-PET/CT better than enhanced CT in the detection of retropharyngeal lymph node metastasis in nasopharyngeal carcinoma? Ear Nose Throat J. 2016;95(4–5):178–184.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.