Back to Journals » Infection and Drug Resistance » Volume 19
Evaluation of Ceftriaxone Utilization in Three Regional Referral Hospitals in Uganda: A Prospective Multicentre Study
Authors Munanura EI ![]() , Ndagire M, Kaggwa B
, Ndagire M, Kaggwa B ![]() , Ndagije HB, Kesi DN, Serwanga A
, Ndagije HB, Kesi DN, Serwanga A ![]() , Rajab K, Kutyabami P, Kazinga C
, Rajab K, Kutyabami P, Kazinga C ![]()
Received 10 February 2026
Accepted for publication 23 May 2026
Published 8 June 2026 Volume 2026:19 602726
DOI https://doi.org/10.2147/IDR.S602726
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemant Joshi
Edson Ireeta Munanura,1,* Margaret Ndagire,2,* Bruhan Kaggwa,1,* Helen Byomire Ndagije,3 Diana Nakitto Kesi,3 Allan Serwanga,3 Kalidi Rajab,1 Paul Kutyabami,1 Caroline Kazinga4
1Department of Pharmacy, Makerere University, Kampala, Uganda; 2Mbale Regional Referral Hospital, Mbale, Uganda; 3National Pharmacovigilance Centre, National Drug Authority, Kampala, Uganda; 4Global Health Uganda, Kampala, Uganda
*These authors contributed equally to this work
Correspondence: Margaret Ndagire, Mbale Regional Referral Hospital, Mbale, Uganda, Tel +256757966211, Email [email protected]
Purpose: This study evaluated Ceftriaxone use in Regional Referral Hospitals (RRHs) in Uganda against treatment guidelines, identified drivers of irrational use, and provided evidence-based recommendations to inform a future framework for improving Ceftriaxone utilization.
Methods: We conducted a prospective mixed-methods study in three RRHs. Quantitative data on Ceftriaxone use were collected using structured questionnaires from 753 inpatients, while key informant interviews explored factors influencing inappropriate use and mitigation strategies in place. Quantitative data were summarized using proportions, means, and standard deviations. Logistic regression analyses (univariate and multivariate) were conducted to determine factors associated with appropriate dosing, frequency, combination therapy, and prescribing. Qualitative data were analysed using content analysis to identify emerging themes.
Results: Overall, appropriate Ceftriaxone use was 68.5% (516/753). Ceftriaxone was mostly prescribed for surgical prophylaxis (41%), as 2 g doses (65.7%), once daily (97.7%), for 5 days (53%). Complete blood count was the most performed test (70.4%); culture and sensitivity testing was only 1%. Appropriate use was associated with the admission ward (surgical; AOR=4.55, p< 0.0001), and the hospital; Lacor RRH (AOR=2.4, p=0.016), and Hoima RRH (AOR=2.6, p=0.002). Staying in hospital > 7 days reduced odds of appropriate use (AOR=0.5, p=0.047). Drivers of inappropriate use included lack of prescription restrictions, non-adherence to guidelines, inadequate supervision, poor drug administration, stockouts, heavy workloads, and limited prescriber knowledge.
Conclusion: Ceftriaxone was appropriately used in 68.5% of cases across three RRHs, indicating suboptimal adherence to national guidelines. A national framework should include prescription restrictions, strengthened culture and sensitivity capacity, and antimicrobial stewardship training for all prescribers.
Keywords: antimicrobials, appropriate use, ceftriaxone utilization
Introduction
Ceftriaxone is a beta-lactam antibiotic administered intravenously or intramuscularly for a broad range of susceptible infections. It is a third-generation cephalosporin and is highly efficacious and largely safe, which underlies its popularity in clinical use in many parts of the world.1–3 In Uganda, Ceftriaxone is the most commonly prescribed antibiotic for patients in hospitals, with 80% exposure among all patients admitted in Mulago National Referral Hospital.4 Findings from different drug utilization studies done in hospitals in Spain, Ethiopia, and South Korea have provided similar outlooks on Ceftriaxone utilization. 1,2
Media reports in Uganda have highlighted concerns about antibiotic inefficacy, including Ceftriaxone, reflecting scientific data on rising resistance.5 Infections caused by non-susceptible organisms cause higher rates of morbidity and mortality and significantly cost more to treat than those due to susceptible organisms.2
The current crisis of declining antibiotic efficacy stems from the rapid emergence of non-susceptible microorganisms to nearly every antibiotic in clinical use. Resistance to Ceftriaxone has been reported to increase over time from 8.3% in 2018 to 78.6% in 2021 amongst gram-negative bacteria, with national surveillance showing persistently high resistance levels through 2024.5 This rate of decline in Ceftriaxone efficacy has been associated with several factors, including irrational use of antibiotics (overuse, misuse), supposed low-quality antibiotics,2,6 and the acquisition and spread of specific resistance genes, particularly extended-spectrum β-lactamases and mosaic penA alleles.7
In low- and middle-income countries (LMICs), factors associated with inappropriate Ceftriaxone use include lack of formularies, weak regulatory enforcement, high patient loads, limited diagnostic capacity, and prescriber habits favouring broad-spectrum antibiotics despite available guidelines.8,9 Previous related studies have reported a high prevalence of inappropriate use of Ceftriaxone in Uganda. For instance, over 81% of cases of inappropriate administration of Ceftriaxone have been reported, with culture and sensitivity testing as low as 7%.10 In 2021, we carried out a retrospective Ceftriaxone utilization evaluation study in nine health facilities in Uganda to obtain a wider perspective. Inappropriate Ceftriaxone use was determined to be 30%, with over 42% of prescribed doses not administered to completion. This study, however, faced a great limitation of poor documentation and filing of patient records, especially at public health facilities.9
Irrational Ceftriaxone use contributes to increased therapy costs (up to 3-fold higher in some LMIC settings), prolonged hospitalization (average 4–7 extra days), delayed patient recovery, and accelerated antimicrobial resistance, with resistance rates exceeding 75% in some Ugandan hospitals.5,8 In this study, therefore, we conducted a prospective Ceftriaxone utilization evaluation in three high-volume public Regional Referral Hospitals in Uganda to obtain a deeper perspective. Rational use of Ceftriaxone was determined by comparing the use of Ceftriaxone with the Uganda Clinical Guidelines 2023.
Materials and Methods
Study Area
The study was conducted in three Regional Referral Hospitals (RRHs) in Uganda. Two of the hospitals are government-owned (Hoima RRH and Mbale RRH), while one is a Private Not for Profit (PNFP — St. Mary’s Hospital Lacor). These hospitals are referral centres for many districts: Lacor (8 districts and 1 city), Mbale RRH (16 districts and 1 city), and Hoima RRH (8 districts and 1 city), each serving a population of 2–4.5 million per annum. Mbale RRH and Hoima RRH have bed capacities of 455 and 308, and estimated inpatient admissions per annum of 54,845 and 26,069 patients, respectively.11 Lacor RRH has a bed capacity of 482 and an estimated inpatient admissions per annum of 58,294.12. The study was conducted at the medical, surgical, paediatric, and maternity wards of the three hospitals since these are the high-volume wards where antibiotics are used most. These four wards account for over 85% of inpatient antibiotic use in Ugandan RRHs based on previous point prevalence surveys,4 making them representative of high-volume Ceftriaxone prescribing. The three RRHs were purposefully selected to represent geographic diversity (western, eastern, northern Uganda) and different ownership models (two government, one PNFP) to allow comparison of Ceftriaxone use across different healthcare system governance structures.
Study Design
This prospective observational study employed a mixed-methods triangulation design, combining quantitative patient record review with qualitative key informant interviews, from June 2021 to February 2023. For the quantitative study, the medical records of inpatients who received Ceftriaxone were reviewed prospectively until the patient was discharged, the patient’s treatment was switched, the patient was referred, the patient died, or up to seven days, whichever came first, over the study period. The most common Ceftriaxone dose durations prescribed are 3–5 days, and the patients’ admission period is 2–7 days.10,13,14
Sample Size and Sampling Procedure
The single proportion formula was used to determine the sample size, assuming a 95% confidence level, an estimated prevalence (p) of 50% for appropriate Ceftriaxone use, a precision of 5%, and a 10% contingency level, yielding a sample size of 1255. The sample size was adjusted based on the total number of patients estimated to receive Ceftriaxone over the study period, based on the fact that over 66% of patients admitted receive Ceftriaxone,4 giving a sample size of 828.
Proportionate sampling was used to determine the number of patients to include in the study from the four wards in each hospital based on bed capacity per ward. The patients who met the inclusion criteria were selected by simple random sampling.
Eighteen key informants were interviewed (six from each study site), and they included heads (or their deputies) of medical, surgical, paediatrics, obstetrics and gynaecology, and laboratory departments, and Medicines Therapeutics Committees.
Inclusion and Exclusion Criteria
We included all inpatients who were prescribed Ceftriaxone during the study period at each of the selected wards. Patients were excluded if their medical records contained insufficient or illegible information, if they declined to provide additional clinical details upon request, or if their clinicians could not provide the necessary information to enable assessment of appropriate Ceftriaxone use.
Data Collection Procedure
Data were collected using both qualitative and quantitative techniques.
Quantitative Data Collection
Data were collected prospectively daily from inpatient medication charts and medical records using a data capture tool. Data were collected by three trained research assistants at each facility under direct supervision by a research team member to ensure accuracy and consistency. The data collection tool comprised two main sections. Section one: patient and clinical characteristics, including demographic data (age, sex), admission and discharge date, co-morbidities, diagnosis, laboratory, and diagnostic results. Section two: Ceftriaxone-specific data, including brand name, indication, dose, dosing frequency, duration of therapy, dispensing details, co-prescribed medications, any subsequent antibiotic switches (and the reasons), category of prescriber, and treatment outcome. The appropriateness of Ceftriaxone use was evaluated against a standard treatment protocol adapted from the WHO Drug Use Evaluation guidelines and the American Society of Health-System Pharmacists Criteria for Drug Use Evaluation.15,16 These criteria were aligned with the Uganda National Treatment Guidelines 2023 to ensure local clinical relevance. Missing clinical information was obtained by direct consultation with the relevant medical team.
Qualitative Data Collection
Qualitative data were collected through semi-structured key informant interviews. The interview guide was organized around five core thematic areas: (1) the clinical and contextual determinants influencing the initiation or discontinuation of ceftriaxone therapy; (2) perceived drivers of inappropriate or non-guideline-concordant use; (3) existing institutional mechanisms — such as protocols, guidelines, and stewardship activities — designed to promote appropriate prescribing; (4) clinician observations regarding ceftriaxone’s lack of efficacy or treatment failure; and (5) patterns of laboratory utilization and the capacity of diagnostic services to guide antimicrobial decisions.
Data Quality Control
The data collection tools were pretested in Mulago National Referral Hospital for clarity and relevance. Additionally, all data collectors were trained on how to use the data collection tools, ethical patient interaction, and appropriate engagement with the health care staff. Throughout the seven-day patient follow-up period, a dedicated research supervisor stationed at each study site conducted ongoing monitoring to verify data completeness and accuracy.
Data Analysis
Data were entered in Epidata software version 3.1 and exported to Stata 16 for analysis. Categorical variables were summarized as frequencies and percentages, while continuous variables like age and weight of patients were summarized using means, standard deviations, and ranges.
Appropriateness of ceftriaxone use was assessed using a composite score based on four criteria: (1) appropriate prescription (indication), (2) appropriate dose, (3) appropriate dosing frequency, and (4) appropriate combination therapy. A total score of 4 was classified as appropriate use; a score below 4 was classified as inappropriate use.
Bivariate associations between each independent variable and appropriate ceftriaxone use were first assessed using univariable logistic regression. This provided unadjusted odds ratios (ORs) with 95% confidence intervals (CIs) and p-values. Variables with a p-value <0.25 in the univariable analysis were selected for inclusion in the initial multivariable logistic regression model. The multivariable model was constructed using backward elimination to identify independent determinants of appropriate use, while controlling for potential confounders. Results are presented as adjusted odds ratios (aORs) with 95% CIs; a p-value <0.05 was considered statistically significant. Model fit was assessed using the Hosmer-Lemeshow test. The responses of the key informants were analysed using thematic content analysis.
A STROBE flow chart was used to present participant enrolment and exclusions (Figure 1).
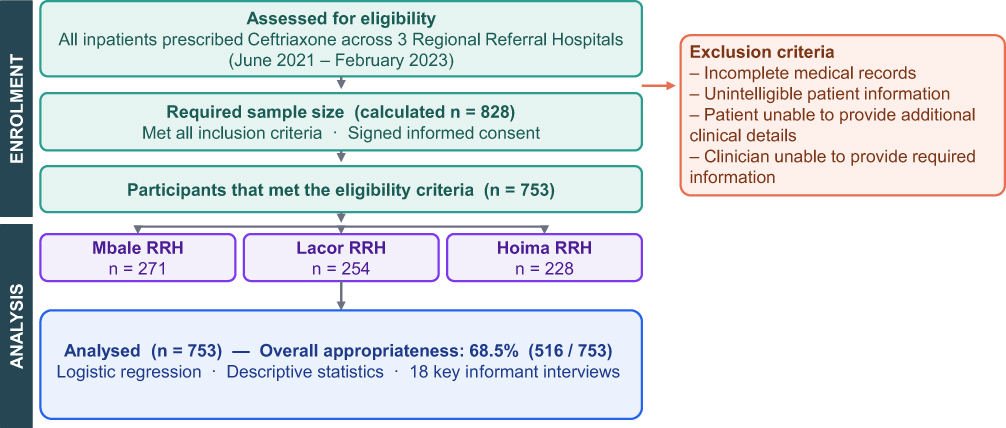 |
Figure 1 STROBE flow chart of participant enrolment and analysis. Of 828 targeted patients, 753 met the inclusion criteria and provided informed consent across three RRHs (Mbale: 271, Lacor: 254, Hoima: 228). All 753 were analysed, with overall appropriate Ceftriaxone use of 68.5% (516/753). |
Results
Participant Flow
A total of 753 eligible patients were enrolled (91.0% of the target 828). Although the initial target was not fully met due to fewer eligible patients during the study period, the achieved sample provided sufficient statistical power. Of the 753 patients, 516 (68.5%) had appropriate Ceftriaxone use, and 237 (31.5%) had inappropriate use. With 15 predictor variables in the multivariate model, the events per variable (EPV) were 34.4 for appropriate use and 15.8 for inappropriate use. Both values exceed the minimum recommended EPV of 10,17 confirming that the study was adequately powered for all planned analyses with low risk of model overfitting.
Demographic Characteristics
Of the 753 participants, the majority were female (387, 51%), of whom 148 (38%) were pregnant. First-time admissions were the highest, at 513 (68%), and referrals were the lowest, at 106 (14%). Age was recorded in 737 (98%) of the patients, ranging from 0 to 99 years, with a median age of 22 years and a mean of 26.7 ± 21.7 years (range 0–99). Weight was recorded for only 337 (44.7%) patients, with a mean of 33.4 ± 22.9 kg (range 1.8–91 kg) and a median of 25 kg. Most patients were from the paediatric ward (188, 25%) and the surgical ward (188, 25%). Most prescribers were interns (371, 49.3%), and Medical Officers (281, 37.3%) (Supplementary Tables 1–6).
Temperature Monitoring
Temperature at admission was recorded for only 483 of 753 patients (64.1%). The average temperature on admission was 37.6°C ± 1.1 (range 31.2–40.1), while the mean temperature on discharge was 36.8°C ± 0.8 (range 35–39.1). Patient temperatures on day 2 or 3 during treatment were not being recorded.
Signs and Symptoms Reported
The majority of patients presented with fever and abdominal pain (367, 49%). Other symptoms reported included productive cough (15%), vomiting (14%), wounds (14%), headache (8%), swelling (8%), difficulty in breathing (5%), chest pain (5%), joint pain (3%), dizziness (2%), bloody urine (2%), back pain (2%), convulsions (2%), restlessness, and bloody diarrhoea.
Conditions for Which Ceftriaxone Was Prescribed
Ceftriaxone was mostly prescribed for pre-operative prophylaxis (309, 41%), septicaemia (93, 12.4%), and pneumonia (78, 10.4%). Caesarean section cases accounted for 91 (29.4%) of the 309 surgical prophylaxis cases (Table 1). Ceftriaxone was also prescribed for non-recommended indications such as stroke (n=6), peptic ulcer disease (n=7), acute gastroenteritis (n=18), hypertension (n=12), and asthma (n=8). This was backed by a key informant who said,
Ceftriaxone is the basic drug for any disease. When the person has come with an accident, maybe an injury, or a cut wound, the starting antibiotic is Ceftriaxone. And from that, you can go to any other drug, depending on the microorganisms that have invaded the wound. (KI-M04)
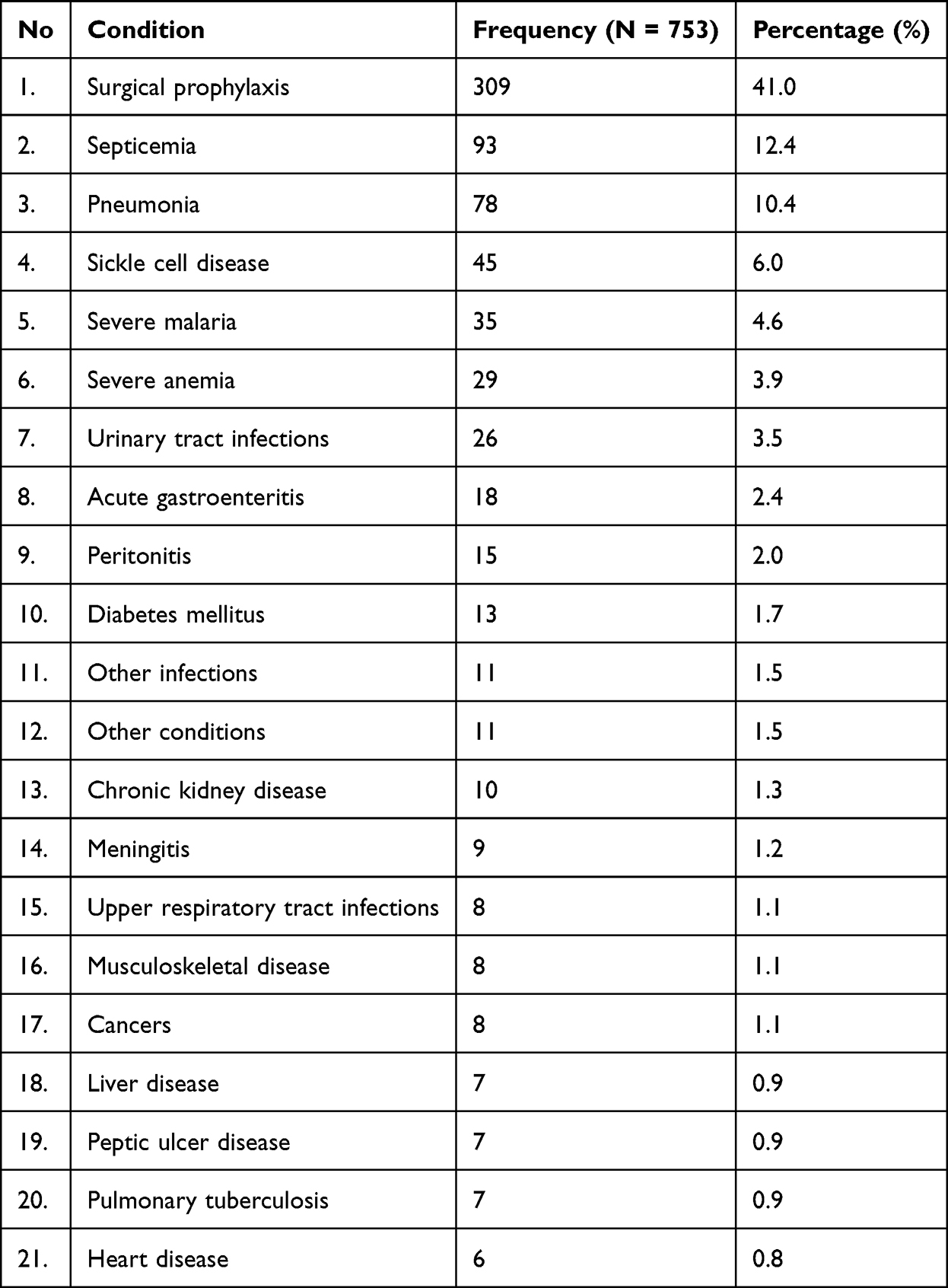 |
Table 1 Common Conditions for Which Ceftriaxone Was Prescribed Among Inpatients (N=753) at Three Regional Referral Hospitals in Uganda, June 2021–February 2023 |
Only 530 (70.4%) patients had a final diagnosis indicated. Of these, 197 (37.2%) were confirmed as bacterial infections by complete blood count and/or culture and sensitivity test, while 209 (39.4%) were surgical prophylaxis cases.
History of Antibiotic Use Before Admission
On admission, 108 (14.3%) patients had previously used antibiotics (Supplementary Table 5). The antibiotics used included Ceftriaxone (159, 21.1% of reported uses), Metronidazole (140, 18.6%), Ampicillin (115, 15.2%), Ampicillin and Cloxacillin combination (102, 13.6%), Gentamycin (77, 10.2%), Ciprofloxacin (57, 7.6%), Amoxicillin (57, 7.6%), Cloxacillin (19, 2.5%), Levofloxacin (19, 2.5%), and Erythromycin (6, 0.8%).
Laboratory Assessment
A total of 530 of 753 (70%) patients had at least one laboratory test conducted before medication. Of the 530 tests conducted, complete blood count was the most common (450, 85%), followed by malaria rapid diagnostic test (365, 68%), liver and renal functionality tests (81, 15%), grouping and cross-matching (44, 8%), urinalysis and serum electrolyte (34, 6%), tuberculosis test (19, 4%), scan (12, 2%), haemoglobin test (12, 2%), and culture and sensitivity (7, 1%).
Other Antibiotics Prescribed Alongside Ceftriaxone
For the 753 patients for whom Ceftriaxone was prescribed, other antibiotics co-prescribed included Metronidazole (365, 48%), Gentamycin (95, 13%), Azithromycin (52, 7%), Ciprofloxacin (29, 4%), Cloxacillin (23, 3%), Ampicillin (18, 2%), Ampiclox® (Ampicillin/Cloxacillin) (11, 1%), Levofloxacin (7, 1%), Amoxicillin (3, 0.4%), and Doxycycline (2, 0.3%).
Prescription of the Appropriate Dose of Ceftriaxone
The doses given ranged from 100 mg to 2 g. The majority were given 2 g (495, 65.7%), followed by 1 g (120, 15.9%), 1.5 g (37, 4.9%), 500 mg (28, 3.7%), 100–250 mg (9, 1.2%), and 750 mg (4, 0.5%). In 60 (8%) patients, the dose of Ceftriaxone was not specified (Table 2 and Supplementary Table 7). Overall, the Ceftriaxone dose prescribed was correct in 681 (90.4%) of cases (Supplementary Table 10). When multivariate analysis was conducted, the ward to which one belonged was the only factor associated with giving an appropriate dose. The odds of giving an appropriate dose in the maternity ward were 14 times those in the paediatrics ward (aOR=14.5, 95% CI 1.03–204.5, p=0.048), and 3 times in the medical ward (aOR=3.0, 95% CI 1.2–7.7, p=0.023) (Table 3).
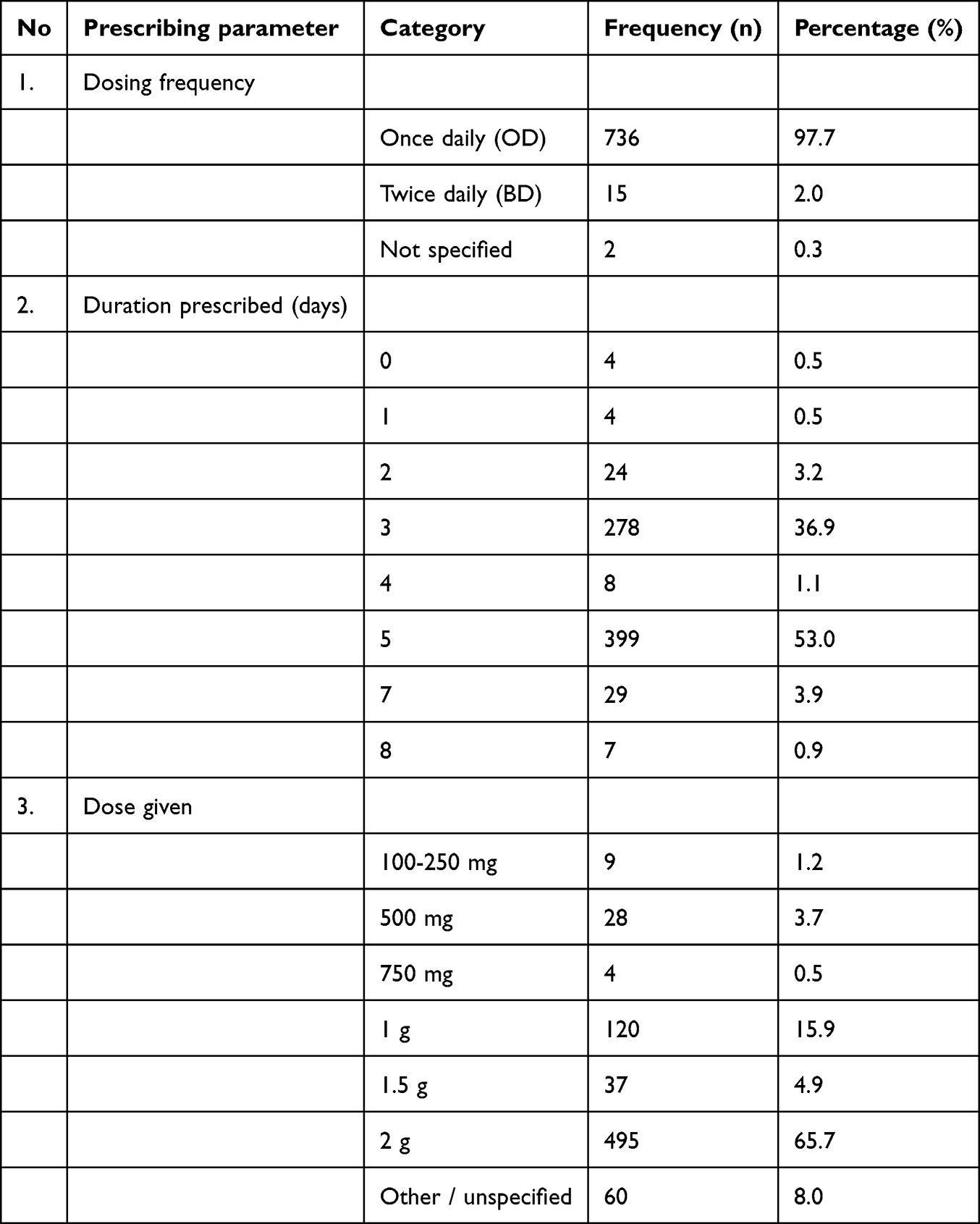 |
Table 2 Ceftriaxone Prescribing Patterns Among Inpatients (N=753) at Three Regional Referral Hospitals in Uganda, June 2021–February 2023 |
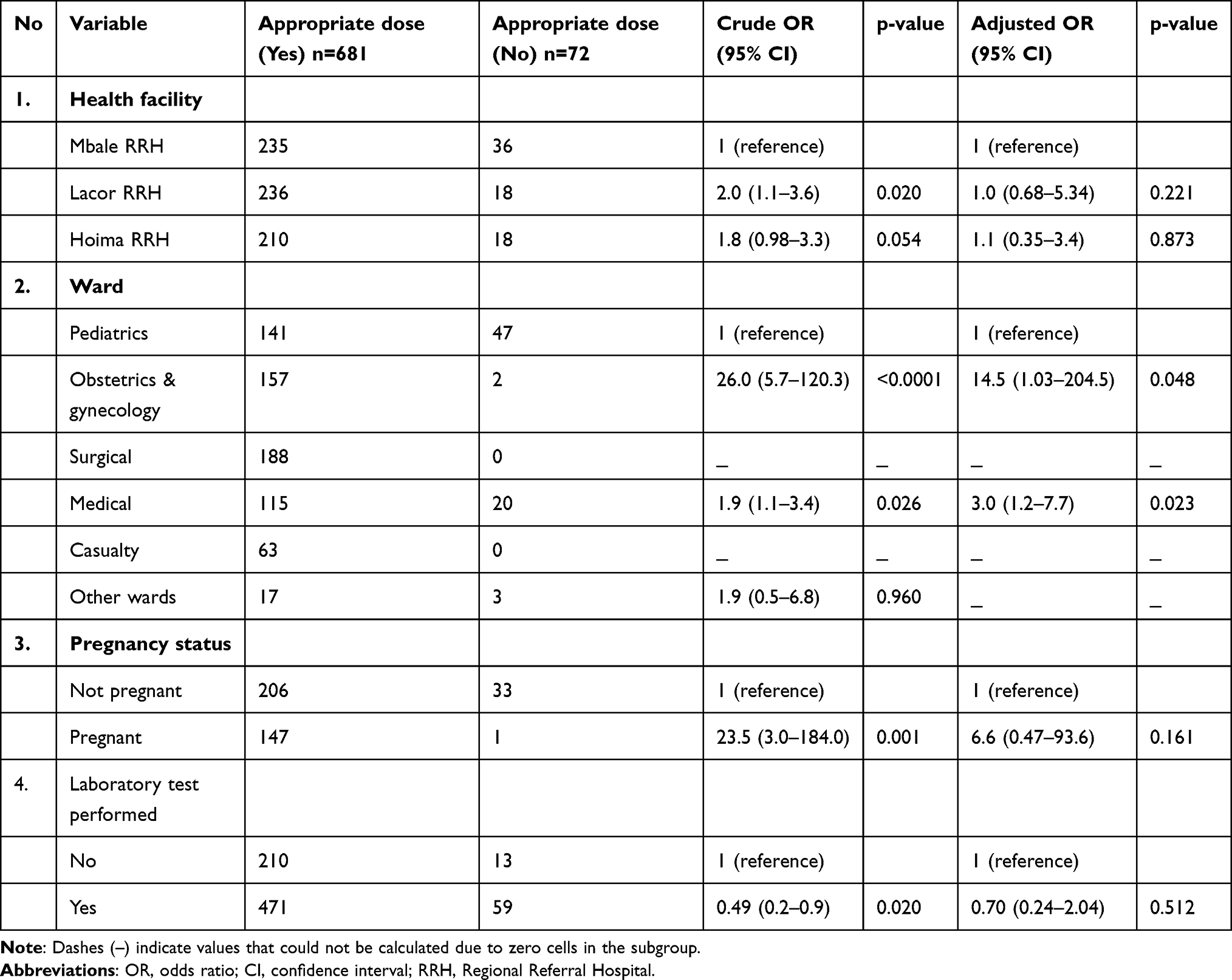 |
Table 3 Factors Associated with Giving an Appropriate Dose of Ceftriaxone Among Inpatients at Three Regional Referral Hospitals in Uganda (N=753) |
Although the prescriber was not statistically significant in giving the right prescription, key informant interviews indicated a lack of restrictions on prescribers as a potential cause of inappropriate use of ceftriaxone:
Patients are seen by various cadres, some by specialists, others by medical officers, others by interns, others by nurses, others by students. Because of a lack of restrictions, you find Ceftriaxone is even used for infections like mild UTIs. (KI-H05)
Prescription of Appropriate Dosing Duration and Frequency
Ceftriaxone was prescribed for 0 to 8 days. The drug was prescribed for 1 day (4, 0.5%), 2 days (24, 3.2%), 3 days (278, 36.9%), 4 days (8, 1.1%), 5 days (399, 53%), 7 days (29, 3.9%), and 8 days (7, 0.9%). Ceftriaxone was prescribed with a dosing frequency of once daily (736, 97.7%), twice daily (15, 2.0%), and unspecified in 2 (0.3%) cases (Table 2 and Supplementary Tables 8 and 9).
The correct frequency of Ceftriaxone was given in 681 (90.4%) patients, while the correct duration was given in 668 (88.7%) (Supplementary Tables 11–12). The only factor associated with the prescription of appropriate dosing frequency at multivariable analysis was the ward to which one belonged. The odds of giving an appropriate dosing frequency in the medical ward were 2.5 times those of the paediatrics ward while controlling for hospital, laboratory test, pregnancy status, and the prescriber (aOR=2.58, 95% CI 1.04–6.37, p=0.04) (Table 4).
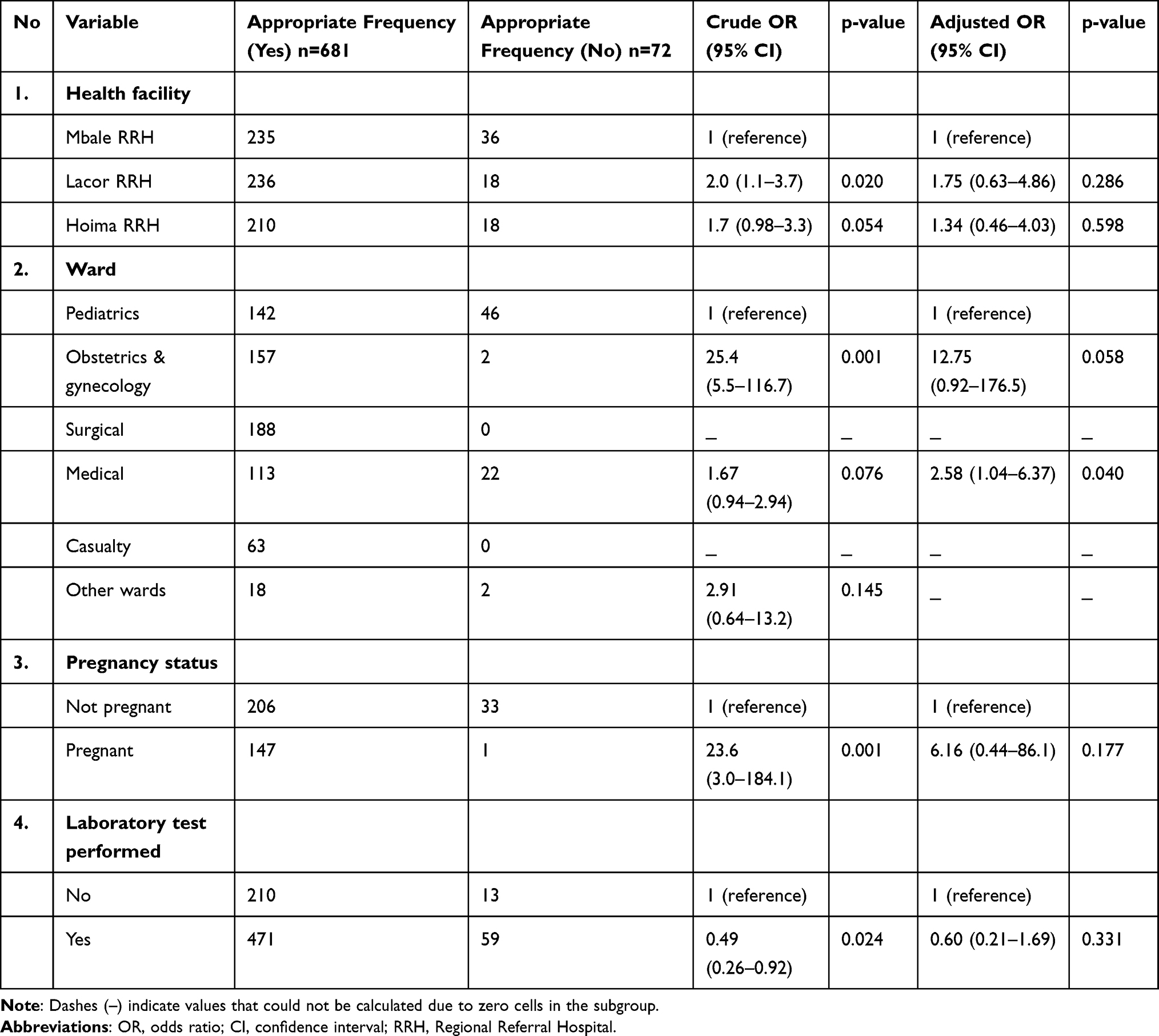 |
Table 4 Factors Associated with Prescribing Ceftriaxone at Appropriate Frequency Among Inpatients at Three Regional Referral Hospitals in Uganda (N=753) |
Prescription of an Appropriate Medicine in Combination with Ceftriaxone
An appropriate combination was given in 531 (70.5%) patients (Supplementary Table 13). Factors associated with giving an appropriate combination of Ceftriaxone with other drugs included the hospital and the ward in which the patient was admitted. Compared to Mbale RRH, the odds of giving an appropriate drug combination with Ceftriaxone were 3 times in Lacor hospital and 2.9 times in Hoima RRH (aOR=3.1, 95% CI 1.56–6.19, p=0.001; and aOR=2.95, 95% CI 1.63–5.34, p=0.0001, respectively), while controlling for ward, nature of admission, sex of patient, laboratory test, and prescriber (Table 5).
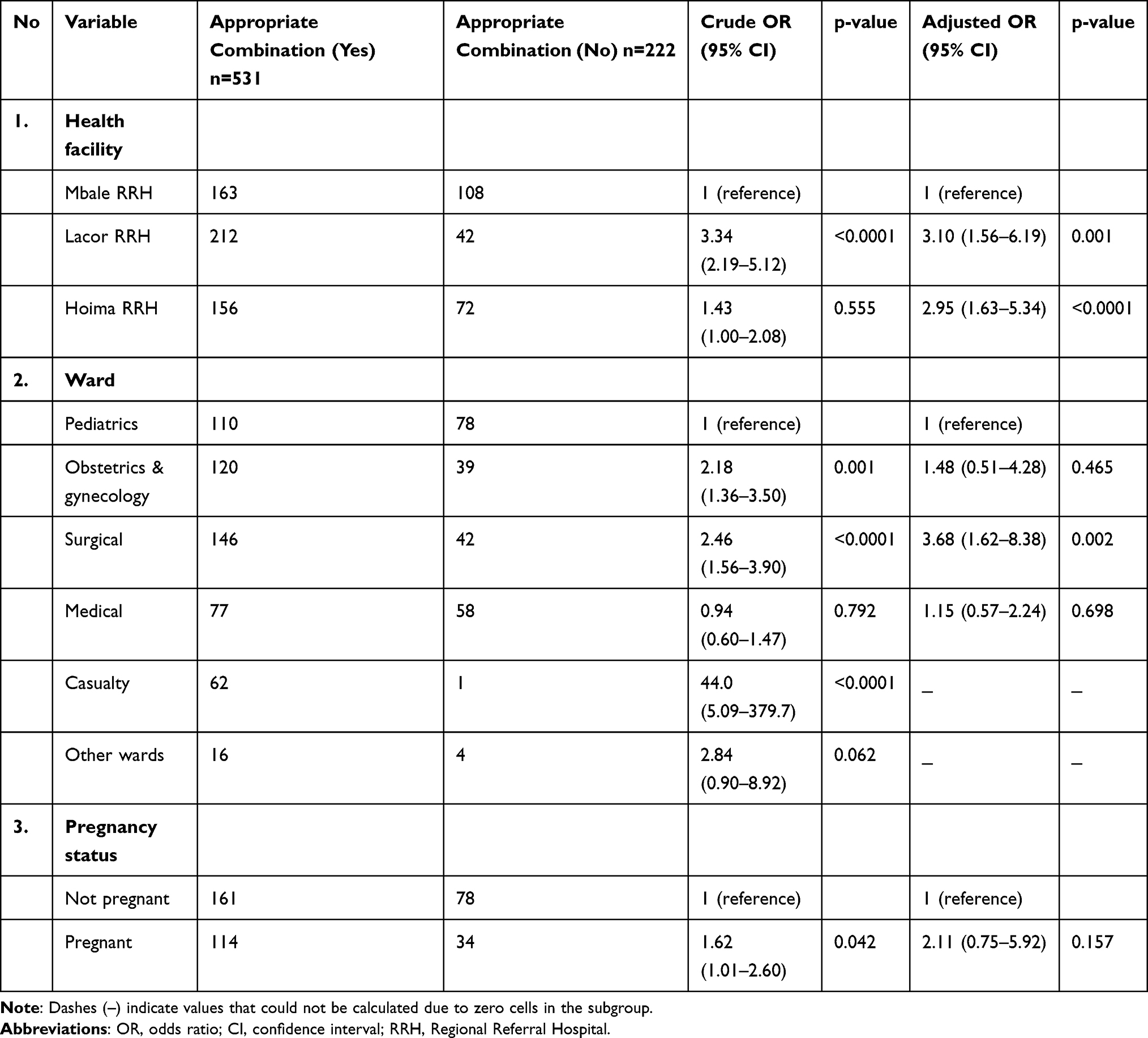 |
Table 5 Factors Associated with an Appropriate Combination While Prescribing Ceftriaxone Among Inpatients at Three Regional Referral Hospitals in Uganda (N=753) |
Treatment Outcomes
The majority of patients (613, 81%) recovered, 94 (12%) were still on the ward after 7 days of follow-up, 29 (4%) died, 13 (2%) were referred, and 4 (1%) self-discharged (Figure 2).
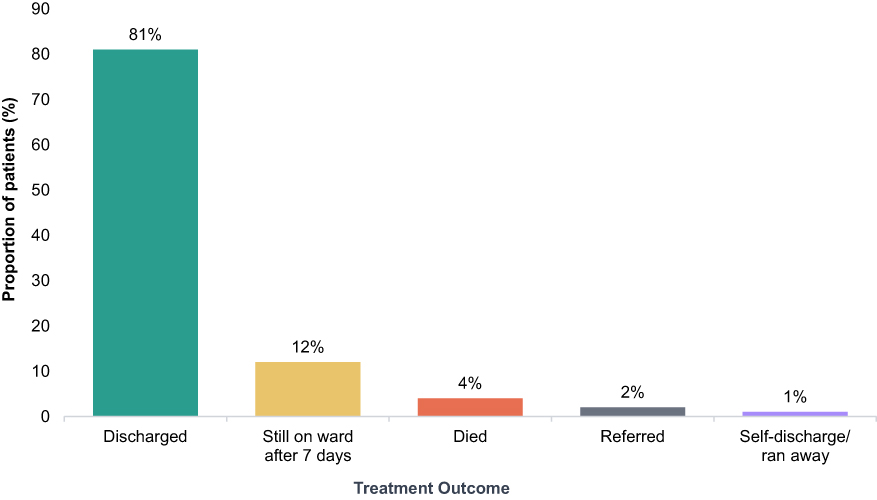 |
Figure 2 Treatment outcomes of patients prescribed Ceftriaxone (N=753). Discharged: 613 (81%); still on ward after 7 days: 94 (12%); died: 29 (4%); referred: 13 (2%); self-discharged: 4 (1%). |
Overall Appropriate Use of Ceftriaxone
The proportion of prescriptions that were overall appropriate was 516 (68.5%) (Supplementary Table 14). Factors associated with the appropriate use of Ceftriaxone were the health facility of admission, the ward of admission, and the cadre of the prescriber. The odds of using Ceftriaxone appropriately were 51 times higher in the casualty ward (OR=51.2, 95% CI 5.8–453.2, p=0.0001), 2.5 times higher in the obstetric and gynaecological ward (OR=2.5, 95% CI 1.6–4.1, p=0.0001), and 2.7 times higher in the surgical ward (OR=2.7, 95% CI 1.7–4.3, p<0.0001) compared to the paediatrics ward. Lacor hospital had 2.9 times the odds of using Ceftriaxone appropriately (OR=2.9, 95% CI 2.0–4.4, p<0.0001) compared to the other two facilities (Table 6). Specialists were 3 times as likely as intern doctors to use Ceftriaxone appropriately (OR=3.3, 95% CI 1.5–6.9, p=0.0009) (Table 7).
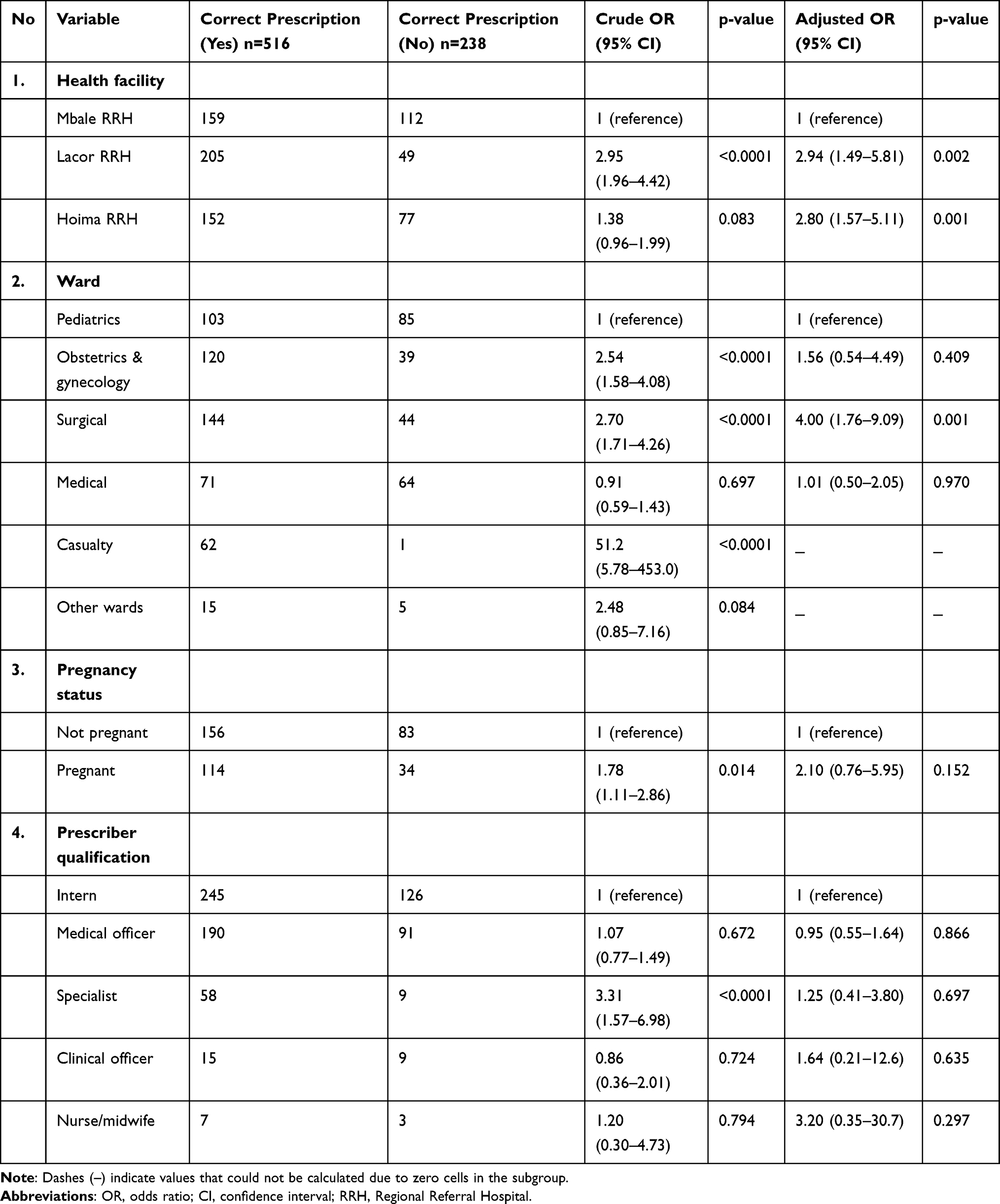 |
Table 6 Factors Associated with Correct Prescription of Ceftriaxone Among Inpatients at Three Regional Referral Hospitals in Uganda (N=753) |
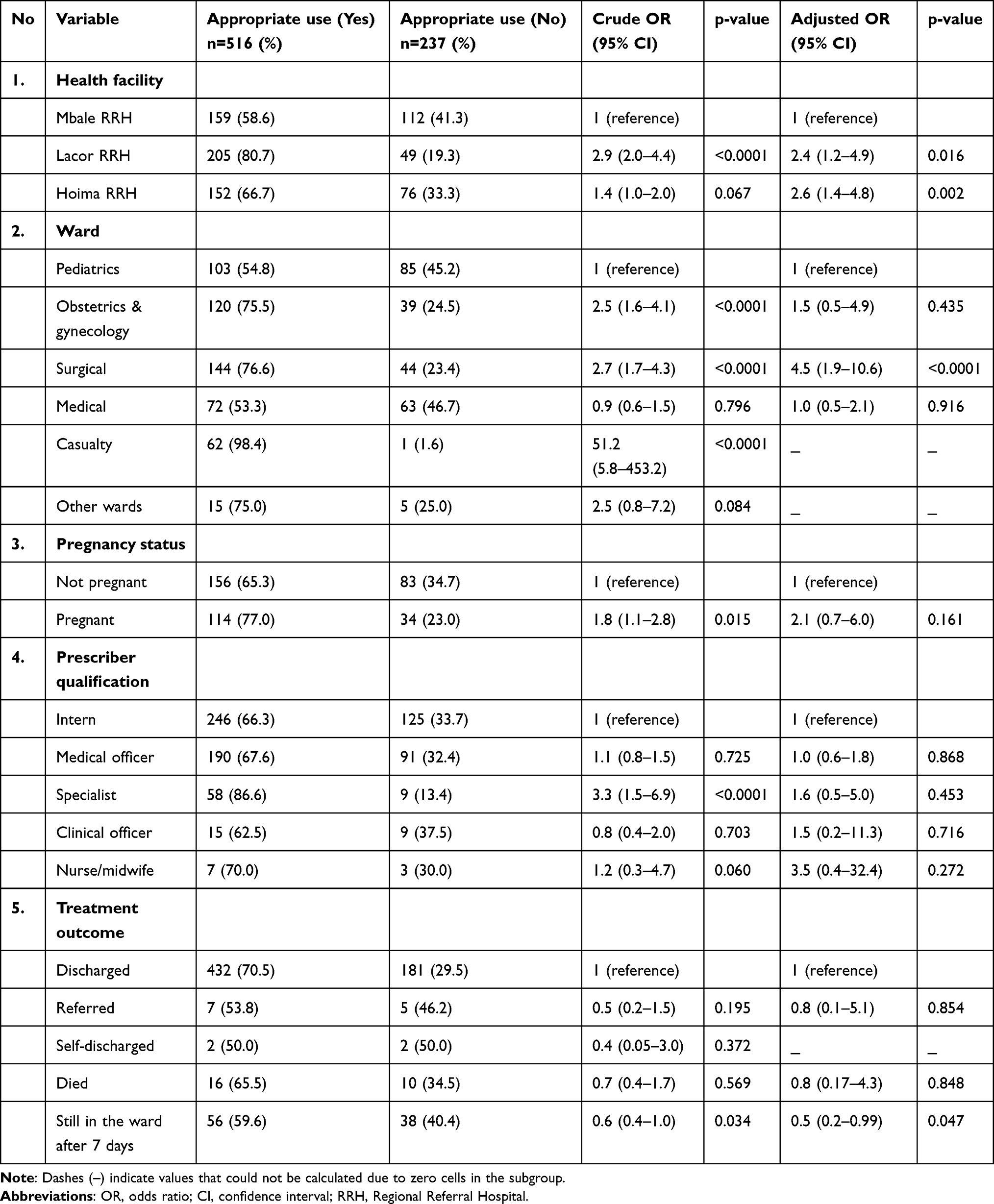 |
Table 7 Factors Associated with Overall Appropriate Use of Ceftriaxone Among Inpatients at Three Regional Referral Hospitals in Uganda (N=753) |
Drivers of Irrational Use and Mitigation Strategies
Key informant interviews were conducted to obtain a deeper understanding of the conditions for which Ceftriaxone is recommended, the reasons for stopping Ceftriaxone treatment before the prescribed dose is completed, the drivers of irrational use of Ceftriaxone, and strategies that can ensure appropriate use of Ceftriaxone.
Ceftriaxone was reported by all respondents as the medicine of choice for severe bacterial infections and for surgical prophylaxis. Major examples of infections for which Ceftriaxone is prescribed include pneumonia, sepsis, complicated urinary tract infections, gastroenteritis, meningitis, and acute chest syndrome, among others. However, respondents also highlighted high levels of misuse regarding indications for which it is prescribed.
In Uganda as a whole, and in this facility, there is some misuse of Ceftriaxone for those infections where you don’t need it. If someone is having just lower abdominal pain, she’s pregnant, it could be early labour, it could be false labour, or it could be Braxton-Hicks contractions. They also give them Ceftriaxone. So, we are misusing it. We are not using it in a proper way. Even for prophylaxis, the recommendation before was to use Ampicillin IV, and it was working well. But people prefer prescribing Ceftriaxone. (KI-H05)
Most respondents considered the quality of Ceftriaxone utilization at their facility as poor. Reasons included prescribing Ceftriaxone without supporting laboratory results, patient attendants with medical backgrounds administering Ceftriaxone to their patients without notifying ward staff, poor adherence to Ceftriaxone administration times, and a lack of restrictions on who should prescribe.
The staff who administer the medication do not strictly follow the administration schedule. When you look at treatment charts, you find that Ceftriaxone has not been given at the required time or the dose has been missed completely. The mismanaged schedule is mainly because of heavy workloads that staff on duty have. (KI-M03)
Various factors were mentioned as major drivers of irrational Ceftriaxone use, including lack of restrictions on who can prescribe Ceftriaxone, failure to adhere to prescribing guidelines, inadequate supervision by hospital administration and external agencies, initiating treatment without laboratory investigations, poor drug administration practices (missed doses, prior reconstitution), self-medication, stockouts, heavy patient loads, and lack of adequate knowledge among prescribers.
Because of the big patient numbers, sometimes ward staff do early reconstitution of Ceftriaxone to administer the required doses swiftly. But this means that reconstituted Ceftriaxone will be standing for longer periods before it’s administered. (KI-L03)
We have had a lot of stockouts in our hospital. Not once, not twice, but it happens almost every other week or so… they send the patients to buy, and some can’t afford, others just buy alternatives. (KI-M03)
At the study sites, various strategies have been put in place to promote rational use of Ceftriaxone and other antibiotics. These include standard operating procedures/guidelines for prescribing, routine point prescription surveys, routine continuing medical education sessions, routine supportive supervision, and alternative antibiotic recommendations based on culture and sensitivity results.
Currently, we are trying to promote the use of laboratory data. In the Obs/Gynae, for example, we are promoting the use of Ampicillin/Cloxacillin and have phased out the use of Ceftriaxone based on data from culture and sensitivity, which shows that resistance against Ceftriaxone is high. (KI-M01)
Our reports indicate that close to 96% of the organisms within this hospital are resistant to Ceftriaxone, and there is a need for action on that to see how that resistance can be brought down. (KI-M02)
There were mixed opinions among respondents regarding Ceftriaxone brands on the market, with differing efficacy. Some thought that some Ceftriaxone brands supplied were of questionable quality, while others blamed the increase in inefficacy solely on irrational use.
Currently, we are having several patients not responding to the Ceftriaxone brand that is mainly supplied by the government. Though we see more improvement with those on other brands, such as Epicephin®. (KI-H01)
Various long-lasting strategies were suggested to ensure appropriate use of Ceftriaxone and other antibiotics, including instituting prescription controls for antibiotics, routine supervision at the health facility level to ensure rational medicine use, establishing and ensuring routine review of standard operating procedures for clinicians, routine continuing medical education for health workers (especially on alternative antibiotics and resistance patterns), improving financing for health facility laboratories, publishing culture and sensitivity test results widely and using them to update medicine lists and procurement plans, and increasing medicine financing to avert rampant stockouts.
Discussion
Irrational antibiotic use results in the emergence of resistant pathogens that, in turn, compromise antibiotics’ effectiveness, leading to treatment failure, compromised patient safety, and increased cost of therapy.8,9
This study evaluated the use and drivers of irrational use of Ceftriaxone in three Regional Referral Hospitals. Overall appropriateness of Ceftriaxone prescription was 68.5%, hence an inappropriateness value of 31.5%, which is within the range of 34% to over 70% as reported in various studies.8,10,18,19 This lower prevalence of inappropriate prescribing could be attributed to the fact that our study included only health facilities at the level of regional referral, and these usually have higher-cadre prescribers and also have better systems of supervision and control, including having active Medicines Therapeutic Committees.20 The factors associated with the appropriate use of Ceftriaxone were the ward to which one was admitted, the hospital to which one was admitted, and the prescriber. Appropriate use of Ceftriaxone was more likely in the casualty ward, which can be explained by the fact that admission periods are shorter and start doses of Ceftriaxone are given as the patient is being managed before transfer to other wards. The PNFP referral hospital had better utilization of Ceftriaxone compared with the public RRHs, since private health facilities usually have better control systems in place.9 Furthermore, specialists have been reported to better prescribe antimicrobials compared to lower-cadre prescribers.21
Our qualitative findings align with studies from Ethiopia and Tanzania,22 where lack of prescription restrictions and heavy workloads drive irrational use. One key informant noted, “Patients are seen by various cadres… even students” (KI-H05), reflecting the absence of restrictive prescribing systems common in many LMICs.9 Another highlighted stockouts and patient affordability as barriers.
The use of Ceftriaxone is always higher in surgical than in medical wards because the medical ward is used for admissions of referral cases and non-infectious diseases, while the surgical ward usually admits pre- and post-operative patients that require surgical prophylaxis. Use of Ceftriaxone for surgical prophylaxis was the most common indication (41%), as also reported in related studies.10,18,23 Ceftriaxone was also prescribed in multiple cases without any documented diagnosis. The preference for prescribing Ceftriaxone in most circumstances is due to its broad-spectrum activity and cost-effectiveness as an antibiotic, as highlighted in previous studies.10,18 This was indeed also confirmed by the key informants in our study.
Some key informants said the efficacy of Ceftriaxone varied according to the brand, with the brands from Germany being reported as being more efficacious than those from elsewhere. This finding is in agreement with a study conducted in Mbarara municipality, Uganda, where some brands were reported to have an extremely low potency.6 However, studies from other countries, like Tanzania and Afghanistan, reported no difference based on brands.3,24
The majority of the population in this study was female, with 38% being pregnant. Antimicrobial agents are among the most commonly prescribed drugs during pregnancy due to increased susceptibility to infections.25 Over 68% of participants were first-time admissions. Various antibiotics, including Ceftriaxone, are widely available in the private sector and can even be accessed without a prescription at private pharmacies in many LMICs, including Uganda.26 This could explain why over 15% of patients enrolled had received prior antibiotic treatment at admission, with over 21% of these having received Ceftriaxone. Ceftriaxone was still prescribed for such patients without doing culture and sensitivity testing (only 1% testing rate), despite the reported increase in bacterial resistance against Ceftriaxone and other antibiotics.5,27
In this study, Ceftriaxone was found to be prescribed mainly once daily, with 2 g being the most common dose given.28 There was a high rate of laboratory investigations (70%) to justify the decision to prescribe Ceftriaxone, with the major test being complete blood count (85%). In most clinical settings, a complete blood count test is done to monitor conditions that affect blood cell counts. Antibiotics like Ceftriaxone are usually given empirically until culture and sensitivity results are available.21 Culture and sensitivity testing requires 2–3 days to produce results,29,30 and such delays could compromise the health status of patients in the paediatric and surgical wards, where patients need to be managed urgently. All three hospitals reported undertaking routine antibiograms for the region to inform resistance patterns and antibiotics of choice. However, as also indicated by key informants, most prescribers are adamant about prescribing Ceftriaxone instead of, for instance, ampicillin/cloxacillin, which has shown better efficacy in drug resistance studies.
A key strength of our mixed-methods approach is that qualitative data revealed why inappropriate use occurs — not just how often. For example, quantitative data showed low culture testing (1%), but interviews explained this is due to 48–72-hour turnaround times (KI-M02). Similarly, while quantitative data identified dose appropriateness, interviews revealed that nurses miss doses due to heavy workloads (KI-M03), and information is unavailable from chart review alone.
Ceftriaxone is a “Watch drug,” supposed to be used as a lifesaving drug against confirmed infections and not prescribed routinely, and only used after confirmed resistance to first-line antibiotics. Despite this, Ceftriaxone was found to be prescribed for mild bacterial infections and other non-recommended conditions such as asthma, acute gastroenteritis, stroke, and hypertension, just as in related studies.9,31 This inappropriate use has been attributed to a lack of and non-adherence to standard operating procedures, lack of prescription controls, lack of routine supervision, limited knowledge among prescribers, and heavy workload.22 Heavy workload was reported by some key informants as a key driver of inappropriate dispensing of prescribed Ceftriaxone doses since health workers get overwhelmed and end up missing some doses.
Despite the above challenges, over 81% of patients followed up in this study were discharged. This is probably because Ceftriaxone is a broad-spectrum antibiotic with activity against a wide range of pathogens and because it was mostly used for prophylaxis. Otherwise, the over 96% resistance to Ceftriaxone reported by one key informant from the hospital laboratory and the national average of 76%5 are reasons to worry when it comes to the use of Ceftriaxone for therapeutic purposes.
Limitations
Several limitations should be acknowledged. First, the 7-day follow-up period may not capture late treatment failures or delayed adverse events. Second, findings may not generalize to lower-level health centres (health centres II–IV) where prescribing practices and resources differ substantially. Third, social desirability bias may have affected key informant responses, despite assurances of confidentiality. Fourth, the study was conducted in only three of Uganda’s 15 RRHs, and while selected for geographic and ownership diversity, results may not represent all RRHs. Fifth, missing data (e.g., weight in 55% of patients, temperature in 36%) limited some analyses.
Conclusion
Overall, Ceftriaxone was appropriately used in 68.5% of cases across the three RRHs, indicating suboptimal adherence to national treatment guidelines. Factors associated with appropriate use included hospital type and ward. Qualitatively, the major drivers of irrational Ceftriaxone use were lack of and non-adherence to standard operating procedures, lack of prescription controls, lack of routine supervision, inadequate laboratory services (especially culture and sensitivity), and limited knowledge among prescribers.
These findings directly inform the development of a national framework that should include: mandatory prescription audits for “Watch” antibiotics, antibiotic stewardship training for all prescribers, rapid diagnostic capacity expansion (especially for culture and sensitivity), restricted prescribing privileges for Ceftriaxone, routine supportive supervision, and ensuring continuous availability of alternative first-line antibiotics such as Ampicillin/Cloxacillin. Specific recommendations include: (1) implement prior approval for Ceftriaxone use, (2) expand on-site culture testing with reduced turnaround time, (3) conduct quarterly antimicrobial stewardship training, (4) mandate routine prescription audits, and (5) ensure continuous availability of alternative first-line antibiotics.
Abbreviations
aOR, adjusted odds ratio; ASHP, American Society of Health-System Pharmacists; CBC, complete blood count; CI, confidence interval; IRB, Institutional Review Board; LMIC, low- and middle-income country; MTC, Medicines Therapeutics Committee; OR, odds ratio; PNFP, Private Not for Profit; RRH, Regional Referral Hospital; SD, standard deviation; SOP, standard operating procedure; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; WHO, World Health Organization.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request. Anonymized summary raw data is provided as Supplementary File 1.
Ethics Approval and Informed Consent
This study was approved by Makerere University-School of Health Sciences-Institutional Review Board (Ref. No. MAKSHSREC-2021-86) and was conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from all study participants before data collection. The informed consent included permission for the publication of anonymized responses and direct quotes from key informant interviews.
Consent for Publication
All participants whose data, quotes, or other material appear in this manuscript provided informed consent for publication. No identifying patient information is included in this article.
Acknowledgments
We are very grateful to the funders of this research, the Makerere University Innovation and Research Fund (MakRIF2) and the National Drug Authority, and to the management and staff of the three hospitals for providing administrative approval and all the necessary support that facilitated data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Makerere University Innovation and Research Fund (MakRIF2) and the National Drug Authority of Uganda. The funders had no direct role in study design, data collection, analysis, interpretation, or manuscript writing.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sileshi A, Tenna A, Feyissa M, et al. Evaluation of ceftriaxone utilization in medical and emergency wards of Tikur Anbessa specialized hospital: a prospective cross-sectional study. BMC Pharmacol Toxicol. 2016;17:7. doi:10.1186/s40360-016-0057-x
2. Kizito M, Lalitha R, Kajumbula H, et al. Antibiotic prevalence study and factors influencing prescription of who watch category antibiotic ceftriaxone in a tertiary care private not-for-profit hospital in Uganda. Antibiotics. 2021;10(10). doi:10.3390/antibiotics10101167
3. Naimi H, Rasekh H, Haem Rahimi M, et al. Assessment of the price-efficacy relationship for multiple brands of ceftriaxone sodium in Kabul: a cross-sectional study. BMC Res Notes. 2016;9(1):86. doi:10.1186/s13104-016-1904-y
4. Kiguba R, Karamagi C, Bird SM. Extensive antibiotic prescription rate among hospitalized patients in Uganda: but with frequent missed-dose days. J Antimicrob Chemother. 2016;71(6):1697–18. doi:10.1093/jac/dkw025
5. Namubiru S, Migisha R, Okello PE, et al. Increasing trends of antibiotic resistance in Uganda: analysis of the national antimicrobial resistance surveillance data, 2018-2021. BMC Infect Dis. 2024;24(1):930. doi:10.1186/s12879-024-09806-y
6. Ssebagereka A. Low antibacterial potency of ceftriaxone brands in Mbarara municipality, Uganda. Acta Sci Med Sci. 7(1):29–35.
7. Tewabe A, Marew T, Birhanu G. The contribution of nano-based strategies in overcoming ceftriaxone resistance: a literature review. Pharmacol Res Perspect. 2021;9(4):e00849. doi:10.1002/prp2.849
8. Meresa Bishaw B, Tegegne GT, Berha AB. Appropriate use of ceftriaxone in sub-Saharan Africa: a systematic review. Infect Drug Resist. 2021;14:3477–3484. doi:10.2147/idr.S329996
9. Kutyabami P, Munanura EI, Kalidi R, et al. Evaluation of the clinical use of ceftriaxone among in-patients in selected health facilities in Uganda. Antibiotics. 2021;10(7). doi:10.3390/antibiotics10070779
10. Manirakiza L, Nambasa V, Nanyonga S, et al. Drug use evaluation (DUE) of ceftriaxone in Mubende Regional Referral Hospital, Uganda: a cross-sectional survey. J Pharm Pharmacol Res. 2019;3(10.26502). doi:10.26502/jppr.0024.
11. Ministry of Health, Uganda. Annual Health Sector Performance Report Financial Year 2018/19. 2019. Available from: https://www.health.go.ug.
12. St. Mary’s Hospital, Lacor. St. Mary’s Hospital Lacor Annual Report Financial Year July 2020 - June 2021. 2021. Available from: https://www.lacorhospital.org.
13. Sewagegn N, Ayichew G, Miskir A, et al. Evaluation of ceftriaxone use for hospitalized patients in Ethiopia: the case of a referral hospital. Int J Pharm Sci Sci Res. 2017;3:26–31.
14. Berhe YH, Amaha ND, Ghebrenegus AS. Evaluation of ceftriaxone use in the medical ward of Halibet National Referral and teaching hospital in 2017 in Asmara, Eritrea: a cross-sectional retrospective study. BMC Infect Dis. 2019;19(1):465. doi:10.1186/s12879-019-4087-z
15. Phillips M, Gayman J, Todd M. ASHP guidelines on medication-use evaluation. American Society of Health-System Pharmacists. Am. J. Health-Syst. Pharm. 1996;53(16):1953–1955.
16. Holloway K, Green T. Drug and therapeutics committees. a practical guide on behalf of the WHO in collaboration with MSH. 2003.
17. Peduzzi P, Concato J, Kemper E, et al. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–1379. doi:10.1016/S0895-4356(96)00236-3
18. Ayele AA, Gebresillassie BM, Erku DA, et al. Prospective evaluation of ceftriaxone use in medical and emergency wards of Gondar University Referral Hospital, Ethiopia. Pharmacol Res Perspect. 2018;6(1):e00383. doi:10.1002/prp2.383
19. Tafere C, Endeshaw D, Demsie DG, et al. Inappropriate ceftriaxone utilization and predictor factors in Ethiopia: a systematic review and meta-analysis. Sci Rep. 2024;14(1):25035. doi:10.1038/s41598-024-75728-z
20. Kimbowa IM, Ocan M, Mukonzo J, et al. The role of medicines and the therapeutics committees’ structure in supporting optimal antibacterial use in hospitals in Uganda: a mixed-method study. PLoS One. 2024;19(1):e0289851. doi:10.1371/journal.pone.0289851
21. Sonda TB, Horumpende PG, Kumburu HH, et al. Ceftriaxone use in a tertiary care hospital in Kilimanjaro, Tanzania: a need for a hospital antibiotic stewardship programme. PLoS One. 2019;14(8):e0220261. doi:10.1371/journal.pone.0220261
22. Belachew SA, Hall L, Selvey LA. “Handing out non-prescribed antibiotics is storing up trouble for the next generation!” Unpacking multistakeholder views of drivers and potential solutions in Ethiopia. BMC Health Serv Res. 2023;23(1):830. doi:10.1186/s12913-023-09819-4
23. Vippadapu P, Gillani SW, Thomas D, et al. Choice of antimicrobials in surgical prophylaxis: overuse and surgical site infection outcomes from a tertiary-level care hospital. Front Pharmacol. 2022;13:849044. doi:10.3389/fphar.2022.849044
24. Nsojo A, Mbotwa C, Rweyemamu L, et al. In vitro performance of cost-differentiated ceftriaxone brands against Escherichia coli: insights from a tertiary referral hospital in Mbeya, Tanzania. JAC-Antimicrob Resist. 2024;6(5):dlae162. doi:10.1093/jacamr/dlae162
25. Baraka MA, AlLehaibi LH, AlSuwaidan HN, et al. Patterns of infections and antimicrobial drugs’ prescribing among pregnant women in Saudi Arabia: a cross-sectional study. J. Pharm. Policy Pract. 2021;14(1):9. doi:10.1186/s40545-020-00292-6
26. Adoko DD, Nakaziba R. Antibiotic self-medication in Otuke district, northern Uganda: prevalence and associated factors. PLoS One. 2025;20(8):e0329290. doi:10.1371/journal.pone.0329290
27. Bazira J, Pauline Petra N, Nakato CN, et al. Trends in antibiotic resistance in uropathogens at Mbarara regional referral hospital (2019–2024): a retrospective study. Infect Drug Resist. 2025;Volume 18:3875–3890. doi:10.2147/IDR.S523848
28. Welch S, Shivam A, Duffy M. Factors influencing ceftriaxone prescribing in an emergency department. J Pharm Pract Res. 2018;48(4):394–395. doi:10.1002/jppr.1433
29. Smith KP, Kirby JE. Rapid susceptibility testing methods. Clinics Lab Med. 2019;39(3):333–344. doi:10.1016/j.cll.2019.04.001
30. Siddiqui F, Gupta A, Purwar S, et al. A prospective study to reduce turnaround time of microbiologically positive blood cultures in patients with sepsis in the intensive care unit. Indian J Med Microbiol. 2022;40(4):541–546. doi:10.1016/j.ijmmb.2022.07.014
31. Gorgulho A, Cunha F, Alves Branco E, et al. Appropriateness of empirical prescriptions of ceftriaxone and identification of opportunities for stewardship interventions: a single-centre cross-sectional study. Antibiotics. 2023;12(2):288. doi:10.3390/antibiotics12020288
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.