Back to Journals » Drug Design, Development and Therapy » Volume 15
Evaluation of Ceftazidime/Avibactam Administration in Enterobacteriaceae and Pseudomonas aeruginosa Bloodstream Infections by Monte Carlo Simulation
Authors Dai Y, Chang W, Zhou X, Yu W, Huang C ![]() , Chen Y
, Chen Y ![]() , Ma X, Lu H, Ji R
, Ma X, Lu H, Ji R ![]() , Ying C
, Ying C ![]() , Wang P
, Wang P ![]() , Liu Z
, Liu Z ![]() , Yuan Q, Xiao Y
, Yuan Q, Xiao Y
Received 10 March 2021
Accepted for publication 20 May 2021
Published 6 July 2021 Volume 2021:15 Pages 2899—2905
DOI https://doi.org/10.2147/DDDT.S309825
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Anastasios Lymperopoulos
Yuanyuan Dai,1 Wenjiao Chang,1 Xin Zhou,1 Wei Yu,2 Chen Huang,2 Yunbo Chen,2 Xiaoling Ma,1 Huaiwei Lu,1 Rujin Ji,2 Chaoqun Ying,2 Peipei Wang,2 Zhiying Liu,2 Qingfeng Yuan,1 Yonghong Xiao2
1Department of Laboratory, First Affiliated Hospital of University of Science and Technology of China, Hefei, People’s Republic of China; 2State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, National Clinical Research Center for Infectious Diseases, Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, Zhejiang Provincial Key Laboratory for Drug Clinical Research and Evaluation, The First Affiliated Hospital, Zhejiang University, Hangzhou, People’s Republic of China
Correspondence: Yonghong Xiao Tel/Fax +865 718 723 6421
Email [email protected]
Purpose: To evaluate the administration regimen of ceftazidime/avibactam (CZA) for bloodstream infections caused by Enterobacteriaceae and Pseudomonas aeruginosa.
Methods: The minimal inhibitory concentrations (MICs) of CZA against Enterobacteriaceae and P. aeruginosa isolated from blood cultures at member hospitals in BRICS (Blood Bacterial Resistant Investigation Collaborative System) in 2019 were determined by broth micro-dilution methodology. A 10,000-patient Monte Carlo simulation (MCS) was used to calculate the probability of target attainment (PTA) and cumulative fraction of response (CFR) for different CZA dosage regimens to evaluate their efficacies and optimize the best initial dosage regimen.
Results: Altogether, 6487 Enterobacteriaceae and P. aeruginosa strains were isolated from the blood cultures. The overall CZA resistance rate was 2.31%, of which the Enterobacteriaceae and P. aeruginosa rates were 1.57% and 14.29%, respectively. The MCS showed that the greater the MIC value, the worse the therapeutic effect. When the CZA MIC was ≤ 8 mg/L, the standard dose (2.5g iv q8h) achieved 90% PTA in the subset of patients with creatinine clearance (CrCl) values from 51 to 120 mL/min. Although the high-dose regimen (3.75g iv q8h) achieved 90% PTA in patients with CrCl values from 121 to 190 mL/min, implementing the low-dose regimen (1.25g iv q8h) was also effective for patients in the 51– 89 mL/min CrCl range. Generally, the high-dose regimen (3.75g iv q8h) reached 90% CFR against all of the strains. Conversely, in patients with CrCl values of 121– 190 mL/min, the standard dose (2.5g iv q8h) failed to reach 90% CFR against some Enterobacteriaceae members and P. aeruginosa. When the dose was reduced to the low-dose regimen (1.25g iv q8h), no patients reached 90% CFR against some Enterobacteriaceae members and P. aeruginosa.
Conclusion: CZA has good antibacterial activity against Enterobacteriaceae and P. aeruginosa in bloodstream infections. Clinicians could make individualized treatment regimens in accordance with the sensitivity of the strains and the level of renal function in their patients to best predict the drug-related clinical responses.
Keywords: Gram-negative bacteria, extended-spectrum β-lactamase, dosage regimens, pharmacokinetics, pharmacodynamics, minimum inhibitory concentration
Introduction
Gram-negative bacteria exist widely in natural environments and hospitals, and are the most common nosocomial infection-causing pathogens. In recent years, extensive antibiotics use and the ability of Gram-negative bacteria to readily obtain antibiotic resistance genes has created severe challenges in treating infections caused by these microbes.1 Ceftazidime/avibactam (CZA), a new antibacterial agent, exhibits high bactericidal activity against multidrug-resistant Gram-negative bacteria (including extended-spectrum β-lactamase, AmpC enzyme- and serine carbapenemase-producing Enterobacteriaceae and Pseudomonas aeruginosa).2–4 CZA was approved by the United States Food and Drug Administration to treat complicated abdominal infections in adults, complicated urinary tract infections, hospital-acquired pneumonia, and ventilator-associated pneumonia. Indeed, CZA is a good choice for clinical treatment of carbapenem-resistant Gram-negative bacterial infections.
Monte Carlo simulation (MCS) is a probability analysis method that uses the pharmacokinetic parameters of antimicrobial agents in the human body, combined with the minimum inhibitory concentrations (MICs) obtained for large numbers of bacteria, and takes various pharmacokinetic (PK) and pharmacodynamic (PD) (pharmacokinetic/ pharmacodynamic, PK/PD) parameters as target values to predict and evaluate the antibacterial effect of antibacterial drugs and optimize their administration schemes.5,6 MCS is considered an accurate and rapid PD evaluation tool, and is widely used for comparison, optimization and evaluation of antimicrobial therapy. Based on the CZA resistance monitoring reports for Enterobacteriaceae and P. aeruginosa collected from BRICS in 2019, the probability of target attainment (PTA) and cumulative fraction of response (CFR) for the three different administration regimens were calculated by MCS with the objective of providing a reference for the clinical treatment of bloodstream infections (BSIs) caused by Enterobacteriaceae and P. aeruginosa.
Materials and Methods
Bacterial Isolates
Altogether, 6487 Enterobacteriaceae and P. aeruginosa bloodstream-sourced isolates were collected in the BRICS program during 2019. Repeat isolates from the same patient were excluded. Pathogens were isolated and identified in accordance with clinical microbiological methods using the API20 system (bioMéiieux, Durham, NC, USA). After the purified isolates were shipped to our laboratory, the pathogens were re-identified by matrix-assisted laser desorption ionization-time-of-flight mass spectrometry (VITEK® MS, bioMérieux, Nürtingen, Germany).
Antimicrobial Susceptibility Testing
The MICs of CZA (Pfizer, Zavicefta, Ringaskiddy, Ireland) were determined by the agar dilution method according to Clinical and Laboratory Standards Institute (CLSI) guidelines. CLSI criteria were used to interpret the results according to the interpretive standards for CZA (≤8 mg/L susceptible; ≥16 mg/L resistant).7 Escherichia coli ATCC 25922, Klebsiella pneumoniae ATCC BAA-1705, and P. aeruginosa ATCC 27853 were the quality control strains.
Pharmacokinetics (PKs)
A previously published one-compartment population-based PK model for CZA derived from 10 critically ill patients was used.8 The assay used different dosing regimens (3.75g iv q8h, 2.5g iv q8h and 1.25g iv q8h) to determine the drug serum concentrations, and an adequate PK analysis with appropriate parameters was performed, including the volume of distribution (Vd) in liters at steady state, the total body clearance (CL) in liters per hour, and the fraction (F) of unbound drug, as summarized in Table 1. In this model, the CL of each drug was parametrized as a linear function of CrCL: CL = CLs×CrCL + CLi, where the slope term CLs represents renal clearance and the intercept term CLi represents nonrenal clearance.
 |
Table 1 The Pharmacokinetic Parameters Used in the Monte Carlo Simulations8 |
Monte Carlo Simulation
CZA displays time-dependent PDs, and its bactericidal effect best correlates with %T>MIC. Multiple 10,000-patient Monte Carlo simulations (Crystal Ball, Oracle Corp.) were performed for the CZA dosing regimens based on CrCl. The PTA was assessed over a range of MICs between 0.03 and 256 mg/L in doubling dilutions. The PD index target for avibactam was a free concentration above 1 mg/L (fT>1 mg/L) for 70% of the dosing interval, whereas that for ceftazidime was ≥70% f T>MIC.9 In all the simulations, the fraction of free ceftazidime was 90%, whereas the avibactam-free drug fraction was randomly sampled from a uniform distribution between 92% and 94%.10 Based on the PK index from the different dosage regimens and the MIC results, Monte Carlo simulation was used to simulate the PK/PD characteristics of the different dosage regimens to obtain the best one. The CFR was calculated to evaluate the efficacy of these regimens, and the %T>MIC results were calculated using the following equation: f%T>MIC=ln (Dose×fu×Vd−1×MIC−1)×Vd×CLt−1×100×DI−1, where Ln is the natural logarithm, dose is the intermittent dose in mg, MIC is the minimum inhibitory concentration in mg/L, and DI is the dosing interval in hours.
Results
MIC Determination
Altogether, 6487 bloodstream-sourced strains of Enterobacteriaceae and P. aeruginosa were isolated by the BRICS program in 2019, including E. coli (n=3,687), K. pneumoniae (n=1,656), Salmonella (n=117), Enterobacter cloacae (n=266), Serratia (n=83), Proteus (n=70) and other Enterobacteriaceae genera (n=160), Klebsiella genera (n=70), and P. aeruginosa (n=378). From these, 1881 and 624 were confirmed to be extended-spectrum-β-lactamase (ESBL)-producing E. coli and K. pneumoniae, respectively, by ESBL phenotype tests (Table 2). The ESBL rates for the BSIs caused by E. coli and K. pneumoniae were 51.02% and 37.68%, respectively. We analyzed the MIC data for CZA in these strains and established discrete MIC distributions for each population based on the MIC frequencies. The overall CZA resistance rate was 2.31%, of which the Enterobacteriaceae and P. aeruginosa rates were 1.57% and 14.29%, respectively. MIC50 and MIC90 values for CZA against ESBL-producing E. coli and K. pneumoniae were 0.5 mg/L and 2 mg/L, and 1 mg/L and 4 mg/L, respectively; these values were slightly higher than those for non ESBL-producing strains. The MIC50 (0.06 mg/L) and MIC90 (0.25 mg/L) values for CZA against Proteus were the lowest. The MIC50 (8 mg/L) and MIC90 (16 mg/L) values for CZA in P. aeruginosa were the highest (Table 2).
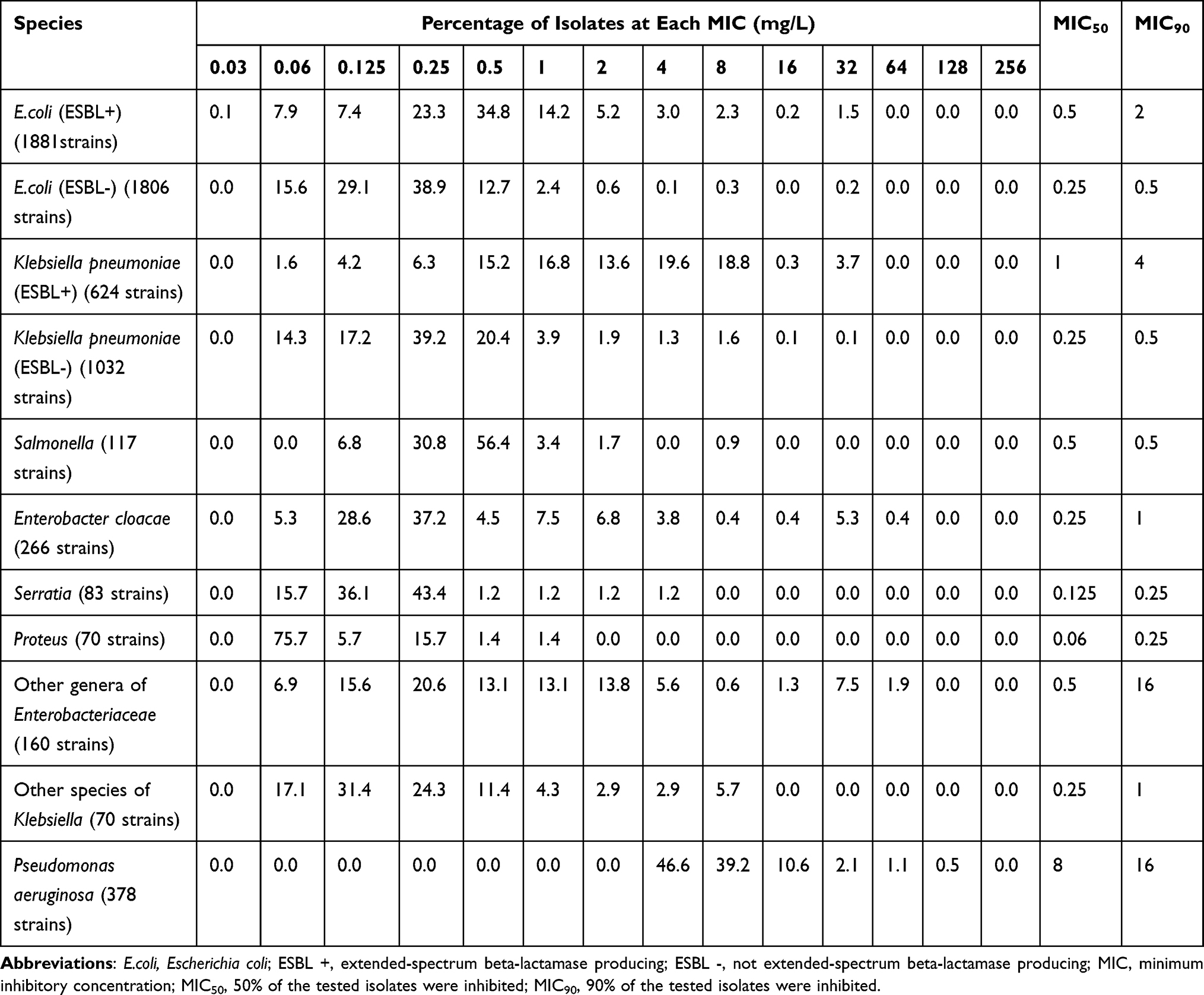 |
Table 2 Frequency Distributions of CZA MICs Against Enterobacteriaceae and Pseudomonas aeruginosa Isolated from BRICS |
Monte Carlo Simulation
In this study, an MCS with 10,000 subjects was performed to calculate PTA and CFR values based on the PK data for CZA from the different regimens. The PTA values for the three doses used for the patients with different renal functions are shown in Table 3 and Figure 1. The PTA values were close to 100% at low MIC values and decreased rapidly to 0 at high MICs. At the susceptibility breakpoint of 8 mg/L, the standard dose (2.5g iv q8h) achieved 90% PTA for the subset of patients with a CrCl range of 51–120 mL/min. For patients with a CrCl range of 121–190 mL/min, the high-dose regimen (3.75g iv q8h) achieved a PTA exceeding 90% at 8 mg/L, and although the PTA only increased from 51.67% to 80.93% at 16 mg/L there was no significantly increased benefit for other types of patient. When the dose was reduced to the low-dose regimen (1.25g iv q8h), it was effective for patients with a CrCL range of 51–89 mL/min. As shown in Table 4, the high-dose regimen (3.75g iv q8h) reached a 90% CFR against all the strains. For patients in whom the CrCl range was 121–190 mL/min, the standard dose (2.5g iv q8h) did not reach a CFR of 90% against some Enterobacteriaceae genera and P. aeruginosa. When the low-dose regimen (1.25g iv q8h) was used, none of the patients reached a CFR of 90% against some Enterobacteriaceae genera and P. aeruginosa.
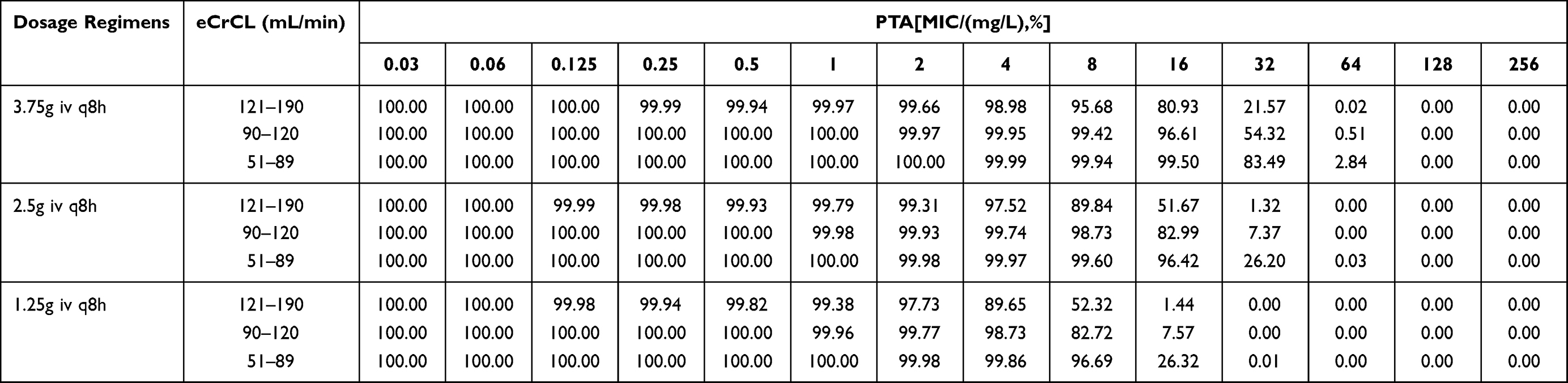 |
Table 3 PTA for Bactericidal Responses (70% of the Time Above the MIC) to CZA at Different Dosage Regimens |
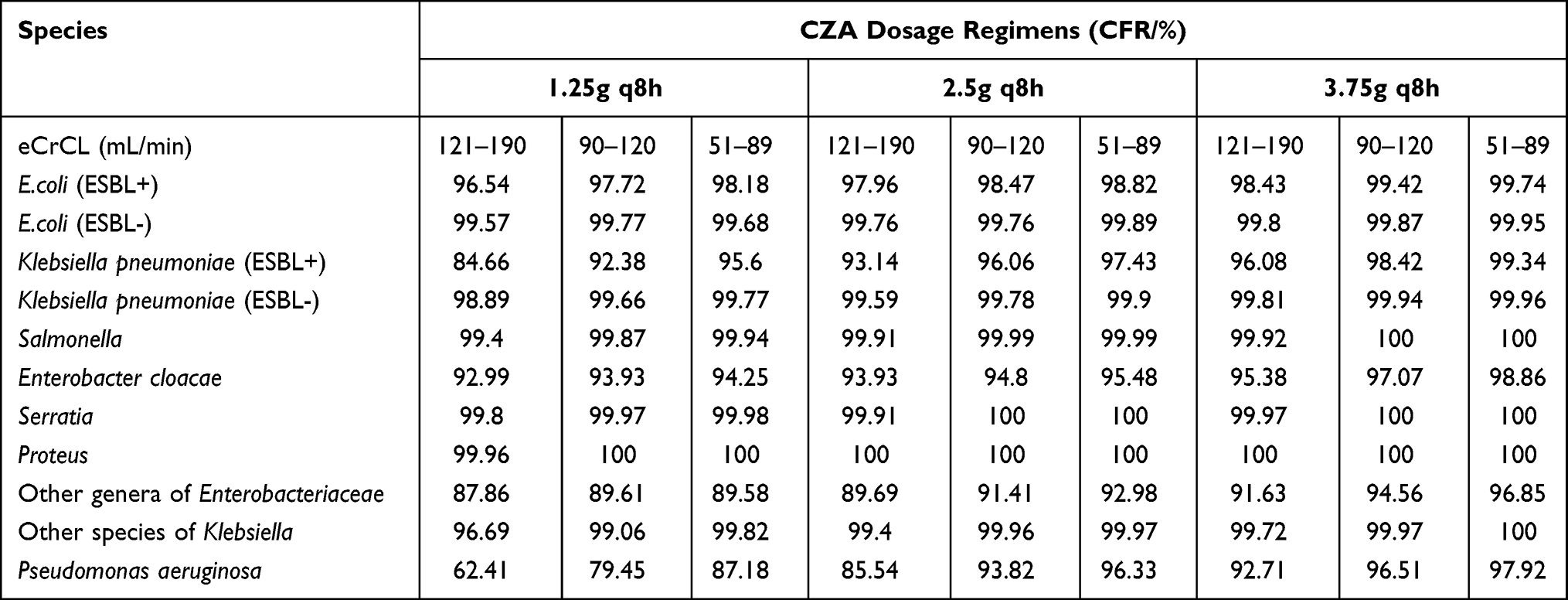 |
Table 4 CFR of the Different Dosage Regimens for CZA Against Enterobacteriaceae and Pseudomonas aeruginosa Isolated from BRICS |
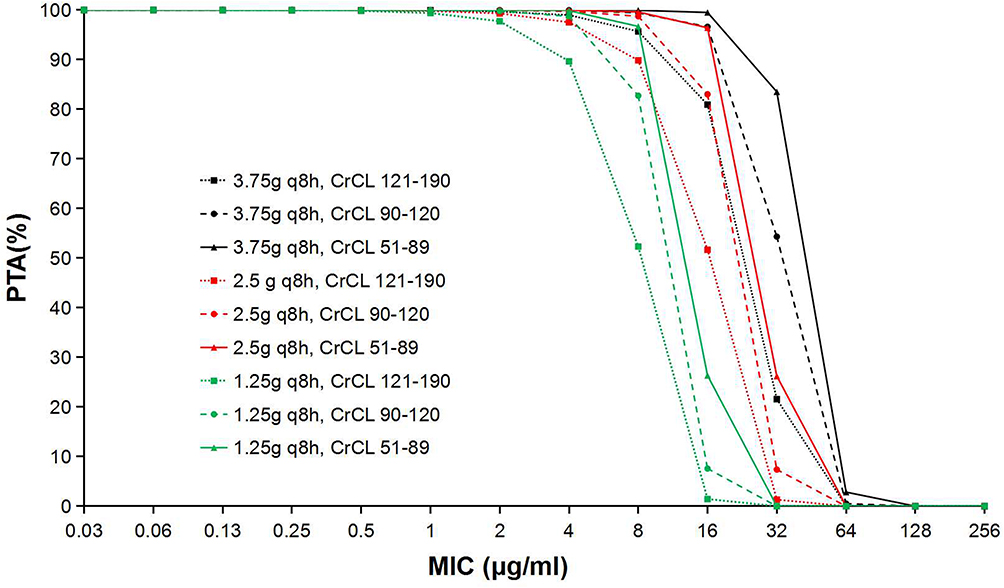 |
Figure 1 PTA at a pharmacodynamic target of 70% T>MIC for CZA. |
Discussion
BSIs are commonly seen in hospitals,11 but finding the most appropriate antimicrobial regimen for patients with suspected BSIs is not straightforward.12 Gram-negative bacteria, particularly Enterobacteriaceae and P. aeruginosa have emerged as the predominant BSI-causing pathogens.13 The increasing rates of β-lactam-related antibiotic resistance, the spread of bacteria with ESBLs, and the emergence of carbapenem-resistant isolates, have made it particularly challenging to select appropriate antibiotic treatments. CZA, a new type of β-lactam/β-lactamase inhibitor combination, can widely and effectively treat infections caused by carbapenem-resistant Gram-negative bacteria.14 Among them, ceftazidime is a third-generation cephalosporin, whereas avibactam, a new β-lactamase inhibitor type with a strong molecular activity, can inhibit the activity of class A, class C and some class D Ambler enzymes but it is inactive against metallo-β-lactamases and OXA-type carbapenemases. Avibactam has no antibacterial activity per se, but it can restore or improve the antibacterial performance of ceftazidime. CZA can inhibit Enterobacteriaceae that produce ESBLs, K. pneumoniae carbapenemase, AmpC and OXA-48 enzyme types and carbapenem-resistant P. aeruginosa, but it has no effect on Acinetobacter and Stenotrophomonas,14 so they were excluded from this study.
Our results showed that CZA was highly active against Enterobacteriaceae isolated from BSIs. In fact, 98.43% of the Enterobacteriaceae isolates were susceptible to CZA, a finding similar to that reported previously.15 However, we also observed that the MIC90s of some Enterobacteriaceae genera were high, and the MIC values were widely distributed among them, ranging from 0.06 mg/L to 64 mg/L, a finding possibly related to the inability of CZA to inhibit class B-metallo β-lactamase production. An in vitro study showed that the P. aeruginosa resistance rate to CZA was 3.4%, while that of extensively drug-resistant bacteria was 25.0%.15 In another study by Chinese researchers,16 the MIC50 and MIC90 values of CZA against the P. aeruginosa strains isolated from 30 medical centers in China in 2017 were 2 and 16 mg/L, respectively, but in our study the P. aeruginosa resistance rate to CZA was 14.29% and the MIC50 and MIC90 values were 8 and 16 mg/L, respectively. These results show that the susceptibility of P. aeruginosa to CZA decreased in 2019, and we speculate that this may be related to the rapid increase in multidrug-resistant P. aeruginosa strains occurring in BSIs in recent years. These data indicate that it may become more difficult to achieve the PK/PD target.
MCS, a statistical modeling approach, is based on PK parameters and microbiological susceptibility information. It can simulate the medication situation for thousands of virtual patients and therefore predict the probability of success of therapeutic targets using different treatment regimens.17 We calculated PTA and CFR values to explore the optimal breakpoints for different simulated dose regimens and to determine the appropriate dosage regimens with the highest success rates for treating pathogens. A high level of clinical efficacy is assured when the PTA is at least 90%. The MCS results predict that the standard regimen (2.5g iv q8h) will achieve the 90% PTA goal for CZA against organisms with MICs ≤8 mg/L, except for the subset of patients with a CrCl range of 121–190 mL/min. A similar finding was also reported for adult patients with cystic fibrosis and acute pulmonary exacerbation.18 Therefore, before empirical treatment, clinicians should be mindful of the bacterial culture and drug sensitivity tests and select the best treatment according to the MIC results. We found that the low-dose (1.25g iv q8h) CZA treatment against E. coli and ESBL-negative K. pneumoniae, Salmonella, Enterobacter cloacae, Serratia, Proteus and other Klebsiella species isolated from BSIs exceeded a CFR of 90%, and the standard CZA regimen (2.5g iv q8h) against ESBL-positive K. pneumoniae and some other isolated Enterobacteriaceae and P. aeruginosa exceeded 90% of the CFR. Furthermore, the high-dose CZA regimen (3.75g iv q8h) only benefitted patients within the CrCl range of 121–190 mL/min whose CFRs ranged from 89.69% to 91.63% for some Enterobacteriaceae and from 85.54% to 92.71% for P. aeruginosa. The benefits for patients with other bacterial infections did not increase significantly.
There were some limitations to this study. First, the PK parameters for CZA were obtained from critically ill patients who had adequate renal function (CrCl=50–190 mL/min). These data may differ from the data from patients in daily clinical practice because of differences in race/ethnicity, obesity, renal impairment, illness severity, and other factors. Second, in clinical practice, infectious diseases are often mixed infections, and there may be infections in other body parts and/or other antibiotic-resistant strains occurring at the same time, and the CFR will also be variable. Third, we did not assess the activity of CZA against the different carbapenemase-producing strains.
Conclusions
CZA has a significant antibacterial activity against Enterobacteriaceae and P. aeruginosa isolates. Although the FDA set the CZA breakpoint at 8 mg/L, the wide MIC distribution for CZA in bacteria indicates that its clinical use can be more flexible. Clinicians can make individualized treatment regimens according to the sensitivity of strains and the level of renal function in patients to best predict their clinical drug-related responses.
Ethics Approval
Ethics approval was not required for this study, which used anonymized blood culture strains which were routinely collected from member hospitals.
Acknowledgments
We thank all BRICS member hospitals for providing bacterial data.
Author Contributions
All authors made significant contributions to the work reported, whether in the conception, study design, execution, data acquisition, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Key Research and Development Program of Zhejiang Province (No. 2021C03068).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Leal HF, Azevedo J, Silva GEO, et al. Bloodstream infections caused by multidrug-resistant gram-negative bacteria: epidemiological, clinical and microbiological features. BMC Infect Dis. 2019;19(1):609. doi:10.1186/s12879-019-4265-z
2. Aktaş Z, Kayacan C, Oncul O. In vitro activity of avibactam (NXL104) in combination with β-lactams against Gram-negative bacteria, including OXA-48 β-lactamase-producing Klebsiella pneumoniae. Int J Antimicrob Agents. 2012;39(1):86–89. doi:10.1016/j.ijantimicag.2011.09.012
3. Livermore DM, Mushtaq S, Warner M, Miossec C, Woodford N. NXL104 combinations versus Enterobacteriaceae with CTX-M extended-spectrum beta-lactamases and carbapenemases. J Antimicrob Chemother. 2008;62(5):1053–1056. doi:10.1093/jac/dkn320
4. Crandon JL, Schuck VJ, Banevicius MA, et al. Comparative in vitro and in vivo efficacies of human simulated doses of ceftazidime and ceftazidime-avibactam against Pseudomonas aeruginosa. Antimicrob Agents Chemother. 2012;56(12):6137–6146. doi:10.1128/AAC.00851-12
5. Roberts JA, Kirkpatrick CM, Lipman J. Monte carlo simulations: maximizing antibiotic pharmacokinetic data to optimize clinical practice for critically ill patients. J Antimicrob Chemother. 2011;66(2):227–231. doi:10.1093/jac/dkq449
6. Sy SK, Zhuang L, Derendorf H. Pharmacokinetics and pharmacodynamics in antibiotic dose optimization. Expert Opin Drug Metab Toxicol. 2016;12(1):93–114. doi:10.1517/17425255.2016.1123250
7. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing. CLSI supplement M100. 30th Edition. 2020. Available from: http://www.clsi.org/.
8. Stein GE, Smith CL, Scharmen A, et al. Pharmacokinetic and pharmacodynamic analysis of Ceftazidime/Avibactam in critically Ill patients. Surg Infect. 2019;20(1):55–61. doi:10.1089/sur.2018.141
9. Kidd JM, Stein GE, Nicolau DP, Kuti JL. Monte carlo simulation methodologies for β-lactam/β-lactamase inhibitor combinations: effect on probability of target attainment assessments. J Clin Pharmacol. 2020;60(2):172–180. doi:10.1002/jcph.1510
10. Zasowski EJ, Rybak JM, Rybak MJ. The β-Lactams strike back: ceftazidime-avibactam. Pharmacotherapy. 2015;35(8):755–770. doi:10.1002/phar.1622
11. O’Brien JM, Ali NA, Aberegg SK, Abraham E. Sepsis. Am J Med. 2007;120(12):1012–1022. doi:10.1016/j.amjmed.2007.01.035
12. Rhodes A, Evans LE, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43(3):304–377.
13. Salmanov AG, Voronenko YV, Vozianov SO, et al. Bloodstream infections and antimicrobial resistance of responsible pathogens in Ukraine: results of a multicenter study (2013–2015). Wiad Lek. 2019;72(11 cz 1):2069–2075.
14. Zhanel GG, Lawson CD, Adam H, et al. Ceftazidime-avibactam: a novel cephalosporin/β-lactamase inhibitor combination. Drugs. 2013;73(2):159–177. doi:10.1007/s40265-013-0013-7
15. Zhang H, Xu Y, Jia P, et al. Global trends of antimicrobial susceptibility to ceftaroline and ceftazidime-avibactam: a surveillance study from the ATLAS program (2012–2016). Antimicrob Resist Infect Control. 2020;9(1):166. doi:10.1186/s13756-020-00829-z
16. Yin D, Wu S, Yang Y, et al. Results from the China antimicrobial surveillance network (CHINET) in 2017 of the in vitro activities of ceftazidime-avibactam and ceftolozane-tazobactam against clinical isolates of Enterobacteriaceae and Pseudomonas aeruginosa. Antimicrob Agents Chemother. 2019;63(4):e02431–18. doi:10.1128/AAC.02431-18
17. Trang M, Dudley MN, Bhavnani SM. Use of Monte Carlo simulation and considerations for PK-PD targets to support antibacterial dose selection. Curr Opin Pharmacol. 2017;36:107–113. doi:10.1016/j.coph.2017.09.009
18. Bensman TJ, Wang J, Jayne J, et al. Pharmacokinetic-pharmacodynamic target attainment analyses to determine optimal dosing of ceftazidime-avibactam for the treatment of acute pulmonary exacerbations in patients with cystic fibrosis. Antimicrob Agents Chemother. 2017;61(10):e00988–17. doi:10.1128/AAC.00988-17
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.