Back to Journals » Patient Preference and Adherence » Volume 17
Evaluation of a Standardized Training and Adherence Surveillance Programme to Overcome Quality-of-Life Impairments and Enhance Compliance in Patients Treated with Wearable Cardioverter Defibrillator
Authors Kellnar A ![]() , Fichtner S, Sams L, Stremmel C, Estner HL, Lackermair K
, Fichtner S, Sams L, Stremmel C, Estner HL, Lackermair K
Received 3 December 2022
Accepted for publication 25 January 2023
Published 16 February 2023 Volume 2023:17 Pages 433—440
DOI https://doi.org/10.2147/PPA.S400086
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Antonia Kellnar,1 Stephanie Fichtner,2 Lauren Sams,1 Christopher Stremmel,1 Heidi L Estner,1 Korbinian Lackermair1
1Department of Medicine I, University Hospital Munich, Ludwig Maximilian University, Munich, Germany; 2Department of Cardiology, Krankenhaus Landshut-Achdorf, Landshut, Germany
Correspondence: Antonia Kellnar, Department of Medicine I, University Hospital Munich, Marchioninistr. 15, Munich, DE-81377, Germany, Tel +49 89 4400 712621, Email [email protected]
Background: Treatment with wearable cardioverter defibrillators (WCD) is a non-invasive, transient therapy option for prevention of sudden cardiac death (SCD) in patients with temporary contraindications for implantation of a permanent cardioverter defibrillator. Due to the constant risk of fatal arrhythmias, compliance is the fundamental requirement for effectiveness of a WCD, but this might be hindered by the poor quality-of-life (QoL) during WCD therapy. In this retrospective single-center study, we examined if a standardized WCD training and adherence surveillance programme could enhance compliance and QoL.
Methods: All patients with a prescription for WCD treatment from January 2017 to August 2019 were included and received a standardized WCD training programme. QoL was validated using the modified EQ-5D-3L questionnaire. The findings were compared to a historical, previously published, retrospective cohort from our center (WCD prescription period 03/2012– 02/2016), not receiving the additional training programme. Endpoints comprised therapy adherence, arrhythmic episodes, and dimensions of QoL.
Results: Ninety-two patients underwent WCD treatment in the study cohort for a median of 49 days. Median daily wear time was enhanced in the study cohort (historical cohort vs study cohort 21.9 vs 23.3 hours/per day, p< 0.01) and artefact alarms occurred less frequently (67.9% vs 48.9%, p 0.01). Major restrictions in QoL in the study cohort were found in mobility (48%), daily routine (44%), and sleep (49%), but the dimensions pain (36% vs 4%, p< 0.01), mental health (43% vs 29%, p 0.03), and restrictions in daily routine (48% vs 30%, p 0.04) improved.
Conclusion: A standardized training and adherence surveillance programme might have beneficial effects on compliance and QoL. As these findings are essential for therapy success, they might potentially lead to a reduction in arrhythmic deaths in upcoming WCD trials.
Keywords: wearable cardioverter-defibrillator, sudden cardiac death, quality-of-life, ventricular tachycardia, ventricular fibrillation, life vest
Introduction
Approximately 50% of all cardiovascular deaths are due to sudden cardiac death and in most cases are caused by a malignant arrhythmia.1 Guidelines recommend Implantable Cardioverter Defibrillators (ICD) for patients with presumed high risk for malignant arrhythmias, but implantation is not always feasible at diagnosis due to recent myocardial infarction where recovery of ejection fraction could be anticipated or temporary contraindication.1–5 Wearable cardioverter defibrillator therapy (WCD, Lifevest) is a non-invasive, bridging treatment option in these cases.6–12
Over the past years the effectiveness of the WCD has been described in several studies, including two large registry trials.7,13–17 However, the only randomized trial could not demonstrate a benefit on the primary outcome of arrhythmic death of wearing the WCD in high risk patients after myocardial infarction.6 A central limitation in this trial was the poor adherence in the intervention group: the WCD was worn a median of 18 hours per day during the trial period and WCD therapy was interrupted prematurely by the majority of patients. This was inferior to preceding, registry studies, with median daily use of 23.1 hours15 and 22.5 hours,13 respectively. Due to the fact that WCD therapy is only effective if the vest is worn, compliance is the key to therapy success and clinicians should focus significant attention on achieving compliance.18
Although QoL displays a potential risk factor for reduced adherence during WCD treatment, only limited data is available. Previous trials have described premature treatment discontinuation due to comfort issues.16,19 One retrospective, single center study from our department showed a reduced QoL with impairment of mental health, mobility, daily routine, and freedom of pain during the investigational period, which might have led to limited therapy adherence as a consequence, with a mean daily wear time of 19.7 hours per day. Despite the low rates of inappropriate shock delivery (0.6–2.08%), fear of shock, discomfort of wearing the device, and a vast amount of inappropriate episodes may be associated with restrictions in daily life, whereas an actual life save only occurs in a few patients.6,9,13,15
In this study we investigated whether a standardized WCD training and adherence surveillance programme might improve daily wear time and device handling, and reduce inappropriate episodes due to enhanced recording quality. We further evaluated whether these improvements may reduce impairment of QoL.
Methods
Study Cohort
Consecutive patients receiving WCD therapy (LifeVest Zoll Inc, PA, USA) in our department from January 2017 to August 2019 were included. WCD was prescribed to patients with presumed high risk of arrhythmic death and a transient contraindication for ICD therapy at the discretion of the treating physicians. Clinical characteristics were obtained from electronic medical records at the time point of WCD prescription and device data during the trial period were extracted from the LifeVest network database. After WCD treatment every patient visited at least one more time for re-evaluation for permanent ICD therapy. No patient was burdened with additional examinations or treatment beyond routine clinical care. Our analysis was conducted in accordance with the declaration of Helsinki and was approved by the Ethics Committee of the Ludwig Maximilian University of Munich, because of the retrospective and anonymized data analysis and the confidentially patient data curation in the trial informed consent was waived (project number 17-662 and 20-641). Findings were compared to our previously published data evaluating QoL during WCD therapy (historical cohort).20 The design and methods have been described in detail previously, but to briefly summarize, patients were analyzed retrospectively with respect to compliance, appropriate and inappropriate therapy, and quality-of-life during WCD therapy, but without the additional training programme.20
Standardized Device-Related Training and Adherence Surveillance Programme
During the trial period all patients underwent an intensified device-related patient education performed by a medical technician of LifeVest. This contained an individual introductory lesson for patients and family members in regards to indication, proper handling, reactions to alarms, as well as the consequences of poor compliance. After registration in the LifeVest database, alarms, episodes, and daily wear time were validated on a daily basis via remote monitoring. In case of documentation of insufficient daily wear time (defined as wear time <95%) or high count of inappropriate episodes (defined as >1/day) due to mishandling the patient was contacted within 24 hours. The instruction was repeated as often as needed and if necessary was performed in the home environment in order to generate the best possible management with the device in the patient´s own environment. Additionally, components of the WCD system were replaced at home, if defective or misfitting.
Quality-of-Life Assessment
We performed QoL assessment either in this setting or by phone with a standardized, non-disease-specific questionnaire for validating health-related QoL (EQ-5D-3L).21,22 Non-disease-specific QoL was assessed by five dimensions including mobility, self-care, daily routine, pain, and mental health, on a categorized rating scale. In addition, four device-specific polar questions were included.
Statistics
Continuous, normally distributed variables are described as median and interquartile range, all other continuous variables as mean±standard deviation (SD). Nominal variables are analyzed using the Chi-square-test, continuous variables are compared by the Wilcoxon and median test. A two-tailed p-value ≤0.05 was rated as statistically significant. All statistical analyses were conducted using SPSS© version 25 (IBM Corp., Armonk, NY, USA).
Results
Patient Characteristics
From January 2017 to August 2019, 92 patients received WCD therapy at our department. Patient characteristics are depicted in Table 1 with descriptive comparison with the prior published historical cohort; 15.2% of our patients were female and median age was 56.0 years. WCD treatment was mostly prescribed for primary prevention (85.9%). Underlying disease was ischemic cardiomyopathy (ICM) in 35 patients (38.0%). Median ejection fraction was 25% (Table 1).
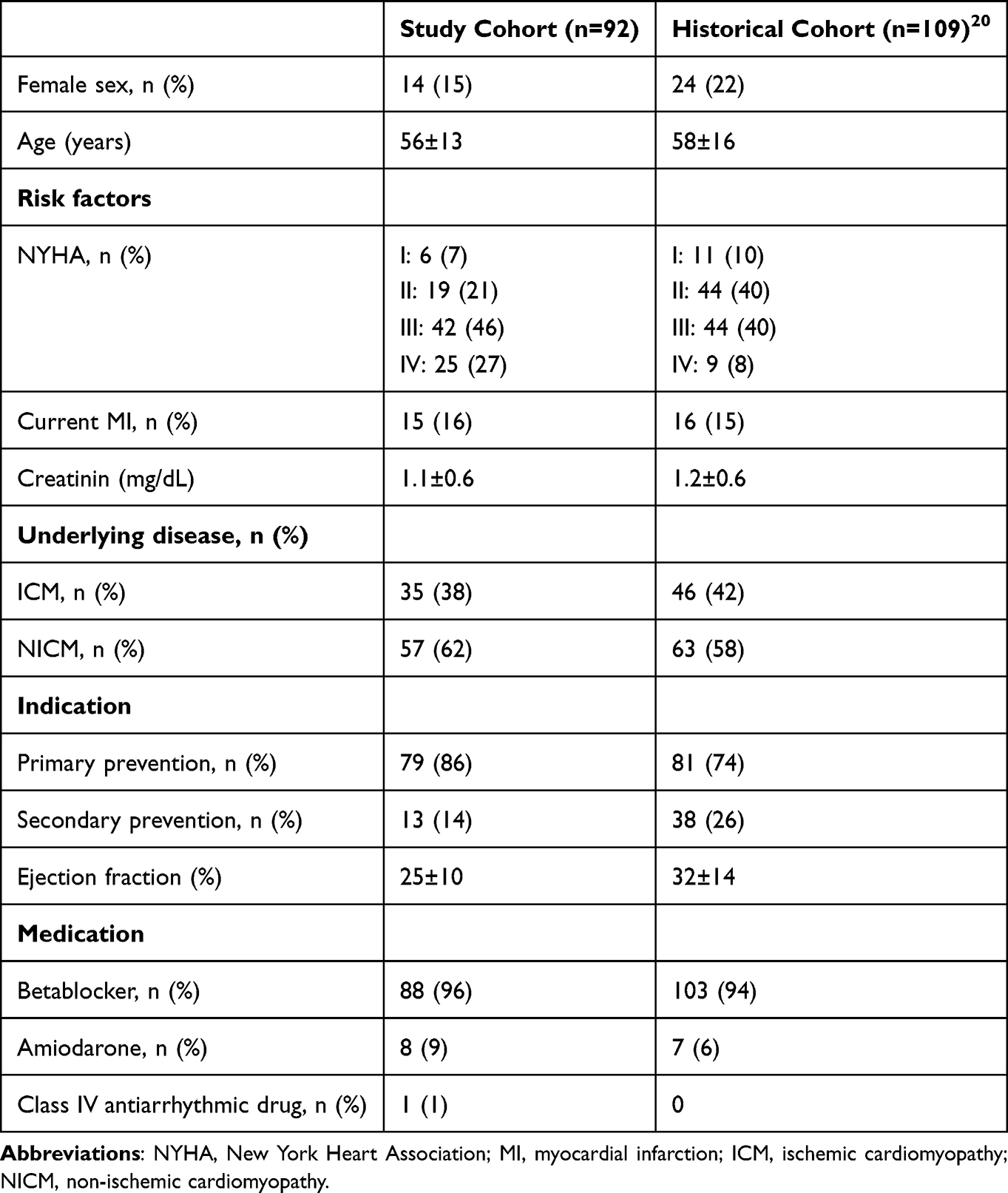 |
Table 1 Baseline Characteristics |
WCD adherence and therapy are presented in Table 2. The device was worn for a median of 49 days and 23.3 (21.2–23.7) hours per day. Median daily wear time with WCD as a measure of compliance of each single patient of the study group is depicted in Figure 1. In our historical cohort the median wear time was 48 days, with 21.9 (18.1–23.1) hours per day (p<0.01).
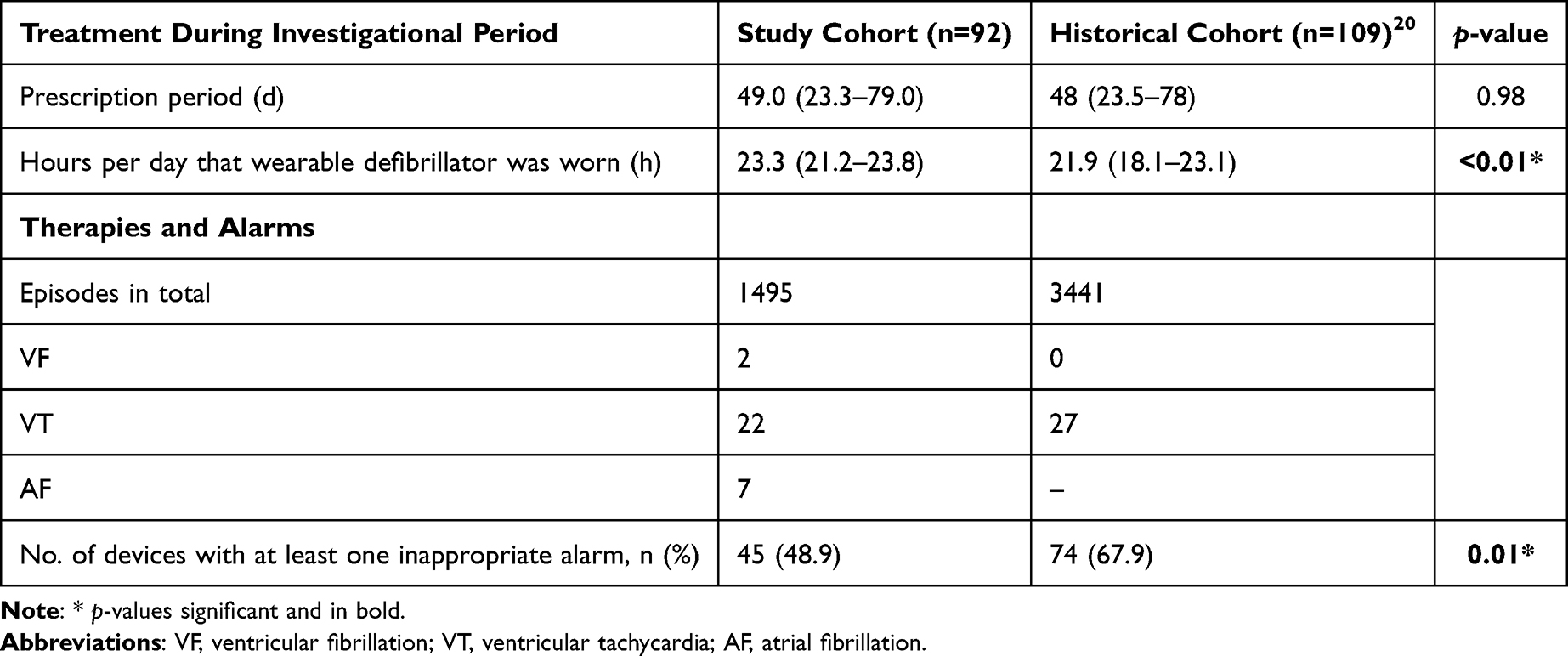 |
Table 2 WCD Adherence and Therapy |
 |
Figure 1 WCD compliance of the study cohort. This figure depicts the distribution of the median daily wear time of the wearable cardioverter defibrillator. Abbreviations: Q, Quartile; WCD, wearable cardioverter defibrillator. |
In total, 1,495 episodes were recorded, of which 24 (1.6%) episodes were correctly annotated as ventricular arrhythmias: 22 episodes of non-sustained ventricular tachycardia and two episodes of ventricular fibrillation. An appropriate shock was delivered in two patients, with three shocks within two episodes of ventricular fibrillation in one patient and one shock for ventricular fibrillation for the other patients. We did not detect a sustained ventricular tachycardia in our study cohort. In the historical cohort, 3,441 episodes were recorded, of which 0.7% were appropriate. Twenty-seven sustained VTs occurred (<1%), which terminated spontaneously or therapy was inhibited by the patient. In our study cohort at least one inappropriate alarm occurred in nearly half of all patients, significantly less frequent when compared to control (67.9, p 0.01).20 The reasons for inappropriate alarms in the study cohort were artefact sensing due to oversensing and noise (91.3%) and episodes of supraventricular arrhythmia (2.2%) and atrial fibrillation (6.5%) (Table 2).
At the time of ICD re-evaluation, the ejection fraction improved significantly from a median of 25% to 36% (p<0.01) and half of the study cohort had no persistent indication for ICD therapy, consecutively. A permanent cardioverter defibrillator was implanted in 37% of our patients, three individuals rejected implantation; in the control cohort 35 patients (44.9%) received an ICD. One patient received heart transplantation during the investigational period and two patients died (one due to malignant disease, one died for unknown reason not wearing the WCD).
Assessment of QoL using the modified EQ-5D-3L questionnaire was available in 53 patients of our study cohort, with more than half of the patients not experiencing limitations in any QoL dimension. Major patient concerns were a mild impairment of mobility, daily routine, mental health, and sleep; 76% of all patients felt safe. Figures 2 and 3 illustrate the comparisons of the QoL restrictions between the current study and a historical control cohort, demonstrating significant improvement of the dimensions pain, mental health, and restrictions in daily routine.
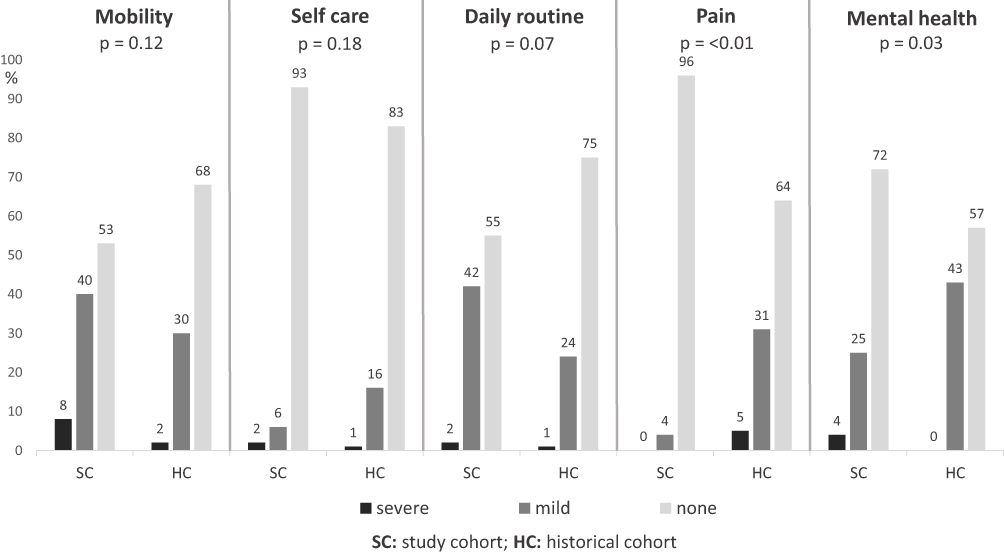 |
Figure 2 Impairment of quality-of-life (non-disease-specific questions; EQ-5D-3L): comparison of the study and the historical control cohort (percentage of patients). Mobility: SC: severe n=4, mild n=21, none n=28 – HC: severe n=2, mild n=26, none n=59; self care: SC: severe n=1, mild n=3, none n=49 – HC: severe n=1, mild n=14, none n=72; daily routine: SC: severe n=1, mild n=23, none n=29 – HC: severe n=1, mild n=21, none n=65; pain: SC: severe n=0, mild n=2, none n=51 – HC: severe n=4, mild n=27, none n=56; mental health: SC: severe n=2, mild n=13, none n=38 – HC: severe n=0, mild n=37, none n=50. |
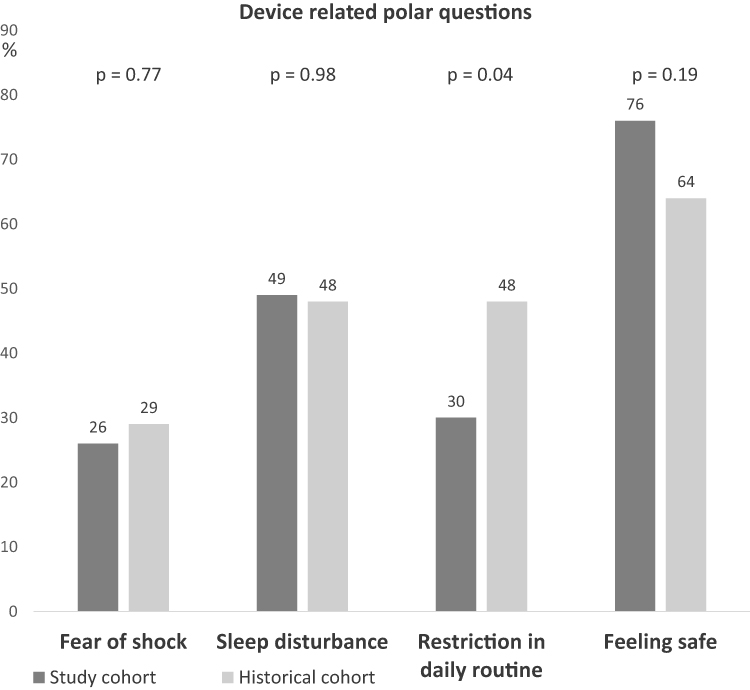 |
Figure 3 Impairment of quality-of-life (device specific polar questions; EQ-5D-3L): comparison of the study and the historical control cohort (percentage of patients). Fear of shock: SC n=14 – HC n=25; sleep disturbance: SC n=26 – HC n=42; restriction in daily routine: SC n=16 – HC n=42; feeling safe: SC n=40 – HC n=56. |
Discussion
In this retrospective cohort trial we evaluated if a standardized WCD-related training and adherence surveillance programme affects compliance and restrictions in patients´ QoL. Several retrospective trials, including two large registry studies, identified potential benefits of the WCD on prevention of SCD in high risk patients.1,3,11–13,15 Yet, the only randomized trial on WCD therapy did not reveal a lower rate of arrhythmic death compared to the control during the trial period of 90 days after myocardial infarction and an ejection fraction of 35% or less, but daily wear time of the WCD was notably lower in this study than in other registry trials.6 Because of the constant risk of cardiac arrhythmias, compliance is the fundamental requirement for effectiveness of a wearable cardioverter-defibrillator.18 One retrospective analysis from our center addressed the impact of WCD therapy on daily patient life and displayed a remarkable reduction of QoL during the trial period,20 which might cause poor therapy adherence. Therefore, we conducted a standardized WCD training and adherence surveillance programme to optimize patient compliance and evaluate the effect on daily wear time and QoL and compared the results with the above-mentioned retrospective cohort from our center.
The major finding was a benefit of our standardized training programme on daily wear time of the WCD: With a median of 23.3 hours per day a desirable therapy adherence was achieved, which was significantly improved over the lower daily wear time (21.9 hours per day) in our historical cohort. The enhanced compliance was comparable to two large registry trials (WEARIT-II Registry and a German nationwide registry for WCD therapy) with a median daily wear time of 22.5 and 23.1 hours per day, respectively. In these registry trials a safe and valuable use of WCD therapy in high risk patients was noted in a non-randomized pattern. The VEST trial revealed poor therapy adherence with a median daily wear time of 18.0 hours per day – a fact that the authors discussed as the main limitation for WCD effectiveness, as the hypothesized prevention of arrhythmic deaths could not be confirmed in this study.6 Our findings on compliance are furthermore in line with the median wearing time of 23.5 hours from the Austrian WCD registry, in which a nurse-based training programme was integrated to support the patient during treatment.23
A further aspect that might be associated with intensified training and thereby improved patient management was the significantly lower rate of artefact alarms in patients receiving the training and adherence surveillance programme. Only half of the study cohort was exposed to at least one episode of an artefact alarm compared to more than two thirds in our control cohort. These findings in our historical cohort are in line with a notably larger number of artefact alarms in the VEST trial, where 9.6% of the patients experienced more than 100 alarms over the trial period. In our cohort no inappropriate shocks were delivered, a remarkable improvement when compared to an inappropriate shock rate of 0.4–0.6% in previously published data.6,13,15 Of all detected arrhythmic episodes, 1.6% were correctly annotated arrhythmias, an increased ratio when compared to <1% appropriate episodes in our historical control cohort.20 Since correct fitting of the device and adequate handling of artefact alarms are essential for error-free recording of the WCD and therapy effectiveness, an intensified training and adherence surveillance programme might be a major advantage for the prevention of arrhythmic death.
Still, WCD therapy had a persisting impact on QoL despite the comprehensive assistance and training: major restrictions were found in mobility, daily routine, and sleep. Notably, nearly no patient experienced pain wearing the device and when compared to our historical cohort our current data may indicate a benefit on the dimensions pain, mental health, and restrictions in daily routine.20
To summarize, WCD therapy still has a persistent impact on the QoL of our cohort. Patients are continuously reminded of the existing risk of sudden cardiac death, as wearing the device leads to discomfort, restrictions in daily routine, eg, personal care and daily mobility and exposition to artefact alarms. Yet, a significant improvement of QoL dimensions as a result of our standardized training and adherence surveillance program could be demonstrated, as patients may have felt sufficiently supported and the need of the daily wear time could be repeatedly clarified. Nevertheless, as no inappropriate shock was delivered and two life saves occurred in our cohort, WCD therapy is considered to be a safe and non-invasive treatment option for patients being at transient high risk for arrhythmic deaths.
Our study has several important limitations: First, QoL assessment could not be gathered from every subject, which might affect the results because QoL assessment, especially from the more distressed patients, may be missing. Second, since inclusion was performed in a non-randomized, non-matched design and at different time points, statistical comparisons to the historical cohort were limited and as a consequence as was generalizability of the effect of the WCD training and adherence surveillance programme on compliance and QoL. Furthermore, the impact on QoL and compliance might be altered by evolving therapy of heart failure over time, whereas WCD therapy was unchanged during both time points of inclusion. These circumstances underline the need for larger, preferably randomized trials on this topic.
Conclusion
Therapy adherence is the fundamental determinant for the effectiveness of treatment with a wearable cardioverter-defibrillator. We could demonstrate that a standardized training and adherence surveillance programme has a beneficial effect on adherence. Nevertheless, limitations in quality-of-life during WCD therapy abide.
Abbreviations
SCD, sudden cardiac death; ICD, implantable cardioverter-defibrillator; WCD, wearable cardioverter-defibrillator; QoL, quality-of-life; SD, standard deviation; ICM, ischemic cardiomyopathy.
Data Sharing Statement
The data underlying this article will be shared anonymized on reasonable request to the corresponding author.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
Heidi L. Estner has received honoraria for lectures from Boehringer Ingelheim, Boston Scientific, Medtronic and honoraria for advisory board activities from Boston Scientific. The authors report no other conflicts of interest in this work.
References
1. Zeppenfeld K, Tfelt-Hansen J, de Riva M, et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J. 2022;43(40):3997–4126. doi:10.1093/eurheartj/ehac262
2. Defibrillators, Antiarrhythmics versus Implantable “Investigators”. A comparison of antiarrhythmic-drug therapy with implantable defibrillators in patients resuscitated from near-fatal ventricular arrhythmias. N Engl J Med. 1997;337(22):1576–1583. doi:10.1056/NEJM199711273372202
3. Connolly SJ, Hallstrom AP, Cappato R, et al. Meta-analysis of the implantable cardioverter defibrillator secondary prevention trials. AVID, CASH and CIDS studies. Antiarrhythmics vs Implantable Defibrillator study. Cardiac Arrest Study Hamburg. Canadian Implantable Defibrillator Study. Eur Heart J. 2000;21(24):2071–2078. doi:10.1053/euhj.2000.2476
4. Zaman S, Kovoor P. Sudden cardiac death early after myocardial infarction. Circulation. 2014;129(23):2426–2435. doi:10.1161/CIRCULATIONAHA.113.007497
5. Buxton AE, Lee KL, Fisher JD, Josephson ME, Prystowsky EN, Hafley G. A randomized study of the prevention of sudden death in patients with coronary artery disease. N Engl J Med. 1999;341(25):1882–1890.
6. Olgin JE, Pletcher MJ, Vittinghoff E, et al. Wearable cardioverter–defibrillator after myocardial infarction. N Engl J Med. 2018;379(13):1205–1215. doi:10.1056/NEJMoa1800781
7. Kovacs B, Reek S, Krasniqi N, Eriksson U, Duru F. Extended use of the wearable cardioverter-defibrillator: which patients are most likely to benefit? Cardiol Res Pract. 2018;2018:7373610. doi:10.1155/2018/7373610
8. Kirolos I, Jones D, Hesterberg K, Yarn C, Khouzam RN, Levine YC. Recent updates in the role of wearable cardioverter defibrillator for prevention of sudden cardiac death. Curr Treat Options Cardiovasc Med. 2019;21(9):49. doi:10.1007/s11936-019-0746-z
9. Nguyen E, Weeda ER, Kohn CG, et al. Wearable Cardioverter-defibrillators for the prevention of sudden cardiac death: a meta-analysis. J Innov Card Rhythm Manag. 2018;9(5):3151–3162. doi:10.19102/icrm.2018.090506
10. Reek S, Burri H, Roberts PR, et al. The wearable cardioverter-defibrillator: current technology and evolving indications. Europace. 2017;19(3):335–345. doi:10.1093/europace/euw180
11. Priori SG, Blomström-Lundqvist C, Mazzanti A, et al. 2015 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: the Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC)Endorsed by: association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J. 2015;36(41):2793–2867. doi:10.1093/eurheartj/ehv316
12. Zishiri ET, Williams S, Cronin EM, et al. Early risk of mortality after coronary artery revascularization in patients with left ventricular dysfunction and potential role of the wearable cardioverter defibrillator. Circ Arrhythm Electrophysiol. 2013;6(1):117–128. doi:10.1161/CIRCEP.112.973552
13. Kutyifa V, Moss AJ, Klein H, et al. Use of the wearable cardioverter defibrillator in high-risk cardiac patients: data from the prospective registry of patients using the wearable cardioverter defibrillator (WEARIT-II Registry). Circulation. 2015;132(17):1613–1619. doi:10.1161/CIRCULATIONAHA.115.015677
14. Piccini JP, Allen LA, Kudenchuk PJ, Page RL, Patel MR, Turakhia MP. Wearable cardioverter-defibrillator therapy for the prevention of sudden cardiac death: a science advisory from the American Heart Association. Circulation. 2016;133(17):1715–1727. doi:10.1161/CIR.0000000000000394
15. Wassnig NK, Gunther M, Quick S, et al. Experience with the wearable cardioverter-defibrillator in patients at high risk for sudden cardiac death. Circulation. 2016;134(9):635–643. doi:10.1161/CIRCULATIONAHA.115.019124
16. Chung MK, Szymkiewicz SJ, Shao M, et al. Aggregate national experience with the wearable cardioverter-defibrillator: event rates, compliance, and survival. J Am Coll Cardiol. 2010;56(3):194–203. doi:10.1016/j.jacc.2010.04.016
17. Klein HU, Goldenberg I, Moss AJ. Risk stratification for implantable cardioverter defibrillator therapy: the role of the wearable cardioverter-defibrillator. Eur Heart J. 2013;34(29):2230–2242. doi:10.1093/eurheartj/eht167
18. Sears SF, Tripp C, Huber NL, et al. Collaborative care for the wearable cardioverter defibrillator patient: getting the patient and medical team “vested and active”. J Cardiovasc Electrophysiol. 2020;31(9):2509–2515. doi:10.1111/jce.14708
19. Am F, Klein H, Tchou P, et al. Use of a wearable defibrillator in terminating tachyarrhythmias in patients at high risk for sudden death. Pacing Clin Electrophysiol. 2004;27(1):4–9. doi:10.1111/j.1540-8159.2004.00378.x
20. Lackermair K, Schuhmann CG, Kubieniec M, et al. Impairment of quality of life among patients with wearable cardioverter defibrillator therapy (LifeVest(R)): a preliminary study. Biomed Res Int. 2018;2018:6028494. doi:10.1155/2018/6028494
21. Brooks R. EuroQol: the current state of play. Health Policy. 1996;37(1):53–72. doi:10.1016/0168-8510(96)00822-6
22. Nord E. EuroQol: health-related quality of life measurement. Valuations of health states by the general public in Norway. Health Policy. 1991;18(1):25–36. doi:10.1016/0168-8510(91)90141-J
23. Odeneg T, Ebner C, Mortl D, et al. Indications for and outcome in patients with the wearable cardioverter-defibrillator in a nurse-based training programme: results of the Austrian WCD registry. Eur J Cardiovasc Nurs. 2019;18(1):75–83. doi:10.1177/1474515118790365
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.