Back to Journals » Medical Devices: Evidence and Research » Volume 19
Evaluation of a Portable Ultrasound System for Peripheral Intravenous Access: Performance and Safety in a Clinical Setting
Authors Kessel M, Bernal VR ![]() , Galer-Siegfried R
, Galer-Siegfried R ![]() , Steele TJ
, Steele TJ ![]()
Received 11 June 2026
Accepted for publication 3 July 2026
Published 8 July 2026 Volume 2026:19 631735
DOI https://doi.org/10.2147/MDER.S631735
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mohamad Bashir
Matthew Kessel,1 Victor Ryan Bernal,1 Rebecca Galer-Siegfried,1 Trevor J Steele2
1Division of Emergency Ultrasound, Brookdale University Hospital & Medical Center, Brooklyn, NY, USA; 2Becton, Dickinson and Company, Franklin Lakes, NJ, USA
Correspondence: Matthew Kessel, Email [email protected]
Background: Ultrasound-guided vascular access has been increasingly used in clinical practice with studies supporting improved insertion success and reduced complications. To meet the needs of various vascular access applications, ultrasound systems have been evolving with specific features. This study evaluated the safety and performance of a recently developed portable ultrasound system with needle tracking technology for peripheral intravenous catheterization.
Methods: The prospective observational clinical study was conducted at one US medical center between November 2025 and January 2026. Eligible participants requiring peripheral intravenous access underwent ultrasound-guided insertion for peripheral intravenous catheterization. Primary endpoints included successful visualization of target vasculature and successful intravenous access. Safety was assessed by the incidence of device-related adverse events. Descriptive statistics and exact binomial confidence intervals were calculated.
Results: A total of 149 subjects were enrolled, including 17 pediatric (1– 17 years) and 132 adult (≥ 18 years) patients. Ninety-six of these patients presented with at least one DIVA risk factor, including no visible veins, no palpable veins, a history of difficult IV access, IV drug use, or a BMI ≥ 30 kg/m2. With ultrasound guidance, visualization of vasculature was achieved in all participants (100%; 95% CI: 97.6%, 100.0%), and the overall catheter insertion success rate was 100% (95% CI: 97.6%, 100.0%). The mean number of attempts to achieve successful vascular access was 1.05± 0.25. While the overall first-attempt success rate was 95.3%, a rate of 100% was observed in pediatric patients and 94.7% in adult patients. For the adults with any DIVA risk factor, the first-attempt success rate was 92.0%. There were no device-related adverse events observed in the study.
Conclusion: The portable ultrasound system was associated with high first-attempt insertion success and high vascular visualization for peripheral intravenous access with no adverse events. The portable ultrasound system can be successfully used for bedside vascular access in a real-world environment.
Keywords: ultrasound, SiteRite 9, difficult intravenous access, DIVA, insertion success, needle tracking
Introduction
Peripheral venous access is one of the most frequently performed procedures in healthcare settings worldwide. Although peripheral intravenous catheters (PIVCs) are generally considered safe, failure rates remain high, with estimates ranging from 20–80%.1–3 A proportion of these failures has been linked not only to complications but also to inappropriate vascular access device (VAD) selection that does not align with patient needs.4 Failed peripheral catheterization often necessitates catheter replacement or escalation to alternative access options such as peripherally inserted central catheters (PICC) or central venous catheterization, which may increase patient discomfort, the development of complications, and healthcare costs.5 Further, challenges in establishing peripheral venous access are commonly reported in pediatric patients, critically ill patients, or patients with difficult intravenous access (DIVA).6,7 Ultrasound guidance has been reported to prevent the need for escalation to central lines in 85% of patients which is notable given two reports found that 13.1–15% of DIVA patients required a PICC or central venous catheter following failed ultrasound guided PIVC insertion.8,9 To address the above challenges, increasing adoption of ultrasound guidance has been utilized to improve insertion success, enhance patient satisfaction, and reduce procedure related risks.1,10–12
When compared with the traditional landmark technique for peripheral venous catheterization, growing evidence supports that ultrasound guidance significantly improves first attempt success and overall success rates, particularly in DIVA and pediatric patients.13,14 In patients with DIVA, the overall catheterization success with the landmark technique was reported within the range from as low as 1.9% to 64%,10,15,16 while the success rate was 70% to 96.5% in these patients following ultrasound guidance.5,7,10,15 The mean number of attempts has also been reported to be lower with ultrasound guidance versus landmark technique.16,17 Additional outcomes including improved patient comfort, higher patient satisfaction, and reduced pain have also been observed following use of ultrasound guidance in these studies.16,17 In addition, based on sufficient evidence, clinical practice guidelines recommend ultrasound guidance for peripheral venous catheterization in adults and pediatric patients with moderate to difficult venous access, in both emergency and elective situations.18–20
Despite these recommendations, implementation of ultrasound guided vascular access remains inconsistent due to several identified barriers, including the lack of standardized training, equipment availability and cost, workflow and time restrictions, cultural resistance, and lack of institutional policy.21,22 These limitations have driven the development of ultrasound platforms that reduce technical and workflows barriers.1 Ultrasound systems are now being developed to include built in training, simplified user interfaces, integrated all in one designs, and vessel detection and assessment tools.1
However, variability in first-attempt success persists, particularly in patients with DIVA, and multiple attempts are still required in some cases.10 These challenges relate to needle–ultrasound alignment and variability in training and workflow integration and have led to the development of newer ultrasound systems with needle tracking, integrated training, and a portable design.21,23 The BD SiteRite 9 Ultrasound System is an example of a recently developed portable ultrasound device designed to address many of these challenges. The ultrasound system has built-in training to provide standardized training on screen and is equipped with a needle tracking technology to address the technical challenge of misalignment with the ultrasound beam and access needle during catheterization.23 In addition, the portable design supports workflow efficiency and timely bedside use. Given the recent advancements in ultrasound technology, this study aimed to investigate the safety and performance of this portable ultrasound device for peripheral catheter insertion in a real-world clinical setting.
Methods and Procedures
Study Design
The prospective, observational clinical study was designed to evaluate the safety and performance of the BD SiteRite 9 Ultrasound System (Becton, Dickinson and Company, Franklin Lakes, New Jersey, USA). The study was conducted at the Brookdale University Hospital & Medical Center (1 Brookdale Plaza, Brooklyn, NY, USA) between November 2025 and January 2026. The study adhered to the ethical principles of the Declaration of Helsinki and ISO 14155:2020 (Good Clinical Practice). Institutional Review Board (IRB) approval was obtained through an external IRB, Advarra, as authorized by the Brookdale University Hospital and Medical Center IRB (Ref. no. Pro00088014), which approved the study. The study was registered with ClinicalTrials.gov (Identifier: NCT06632509) prior to recruitment. In compliance with U.S. regulations, a summary of this clinical trial is publicly available on ClinicalTrials.gov. This summary excludes any information that could be used to identify individual participants.
Study Devices
The SiteRite 9 Ultrasound System is a portable ultrasound device designed specifically for vascular imaging and guidance during vascular access device placement. The system includes integrated visualization tools such as the Cue™ Needle Tracking System to provide clinicians with continuous and real-time needle tracking, and the Sherlock 3CG+™ Tip Confirmation System to ensure proper catheter tip navigation and location. The device provides real-time 2D imaging with on-screen guidance for clinicians, color doppler technology, vessel measurement tools including an integrated catheter-to-vein ratio calculator, and optional integration with hospital systems for documentation and analytics. Additionally, the device features a large 15.6-inch touch screen with built-in training aimed to provide consistent instruction and ease the learning curve. Catheters used in the study were PIVCs and midline catheters.
Patient Population
Eligible participants included pediatric and adult patients aged ≥ 1 year who required placement of a peripheral intravenous catheter or midline catheter by a clinician. The consent form was discussed with every patient or their legal representatives in depth prior to participation. Patients were required to verbally confirm their voluntary agreement to participate; however, patient signatures were not required. The user explaining the consent would then check off that the patient understood. This approach was approved by the IRB/Ethics Committee given the non-interventional nature of the study and that the procedures were planned as part of routine care. The Principal Investigator or designated representative documented the consent process by signing and dating the IRB/EC-approved informed consent form. Exclusion criteria included conditions in which ultrasound-guided procedures could interfere with standard medical care or impose undue hardship; known or suspected allergies to materials in the SiteRite 9 device or its accessories; and prior medical history or localized anatomical factors that could impede completion of the ultrasound-guided procedure.
Patient subgroups were categorized by DIVA risk factors, defined as no visible veins, no palpable veins, a history of difficult IV access, IV drug use, and/or a BMI ≥ 30 kg/m2. Participants could present with one or multiple DIVA risk factors and were categorized as having 0, 1, 2, 3, 4, or 5 DIVA risk factors (Table 1).
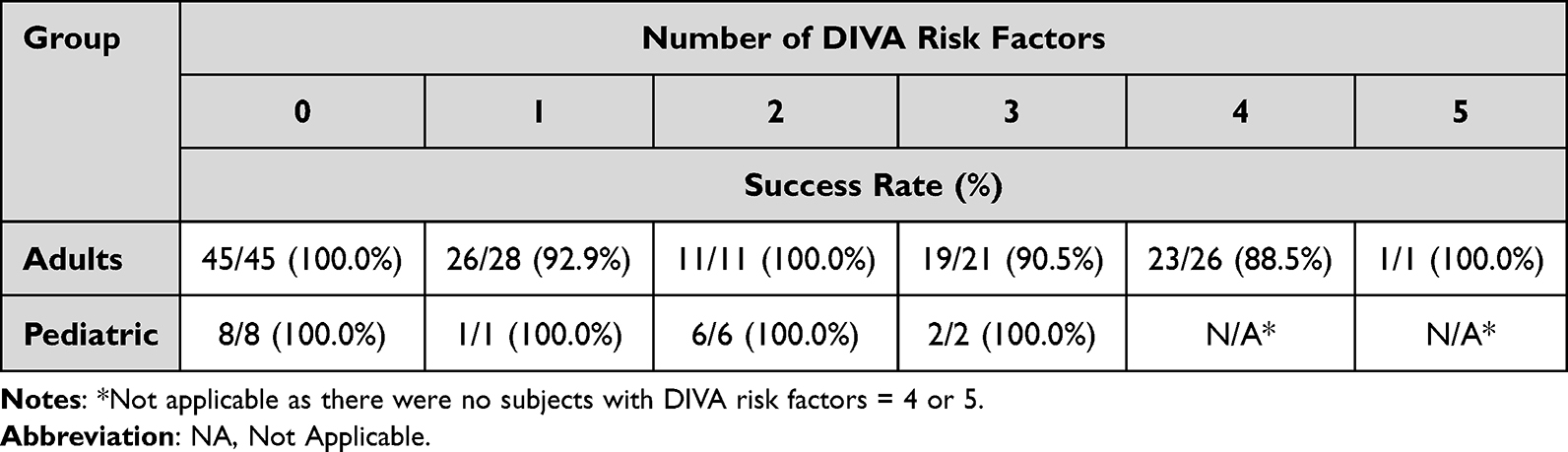 |
Table 1 Successful First-Attempt Vascular Access by DIVA Risk Factors |
Study Procedures
Demographic and baseline clinical data including age, sex, height, weight, and vascular access history were collected for all the study participants. Following enrollment, professional clinicians initiated the ultrasound-guided vascular access using the SiteRite 9 Ultrasound System. Use of needle tracking was at the discretion of the clinician and was not required for all procedures. The procedure involved visualizing the patient’s vasculature, identifying a suitable vein, and attempting vascular access. Successful access was defined by either confirmation of blood return or successful catheter cannulation. Procedural data were collected from the initiation of ultrasound imaging through completion of the vascular access attempt. Study participation for each participant was considered complete 15 minutes following the procedure, allowing for observation and documentation of any immediate post-procedural adverse events and device deficiencies. The end of the study was defined as the completion date of the final study assessment for the last enrolled participant.
Study Endpoints
The primary performance endpoints were the rate of visualization of target vasculature, and the rate of successful vascular access with confirmation of blood return. The primary safety endpoint was the incidence of adverse events experienced by either the patient or the user due to the use of the SiteRite 9 Ultrasound System.
Successful first-attempt access was also assessed, and exploratory subgroup analyses were performed to evaluate the association between first‑attempt success rate and DIVA risk factors.
Data Collection
Patient baseline data and procedural data were recorded by device users. Procedural data included visualization of subject vasculature; identification of a suitable vein or, if no vein was identified, the reason; confirmation of blood return or successful catheter cannulation. Additional data collected included name of vein, laterality, and location, number of insertion attempts and the reason for failure when first attempt success was not achieved.
Statistical Analysis
Procedural success and device performance were documented in written forms and subsequently transcribed into electronic case report forms. Summary descriptive statistics were calculated for all endpoints, with proportions presented alongside 95% confidence intervals using the exact binomial method. No interim analysis was planned, and missing data were excluded from analysis. Normality of continuous variables was assessed using the Kolmogorov–Smirnov test. As only a few variables deviated from normality; data are presented as mean ± standard deviation (SD) and median with interquartile range (IQR). Analyses were performed using SAS® software, Version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Patient Demographics and Baseline Characteristics
A total of 149 participants, including 17 pediatric participants (1–17 years) and 132 adults (≥ 18 years), were enrolled in the study. All participants met the inclusion criteria with no screening failures reported. The majority of the participants (n=144) were ≤ 89 years, with a mean age of 47.0 ± 21.7 years, median 48.0 (1–87) years. There were 84 (56.4%) female and 65 (43.6%) male participants. Ninety-six participants (64.4%) have had at least one DIVA factor. Detailed demographics and baseline characteristics are provided (Table 2).
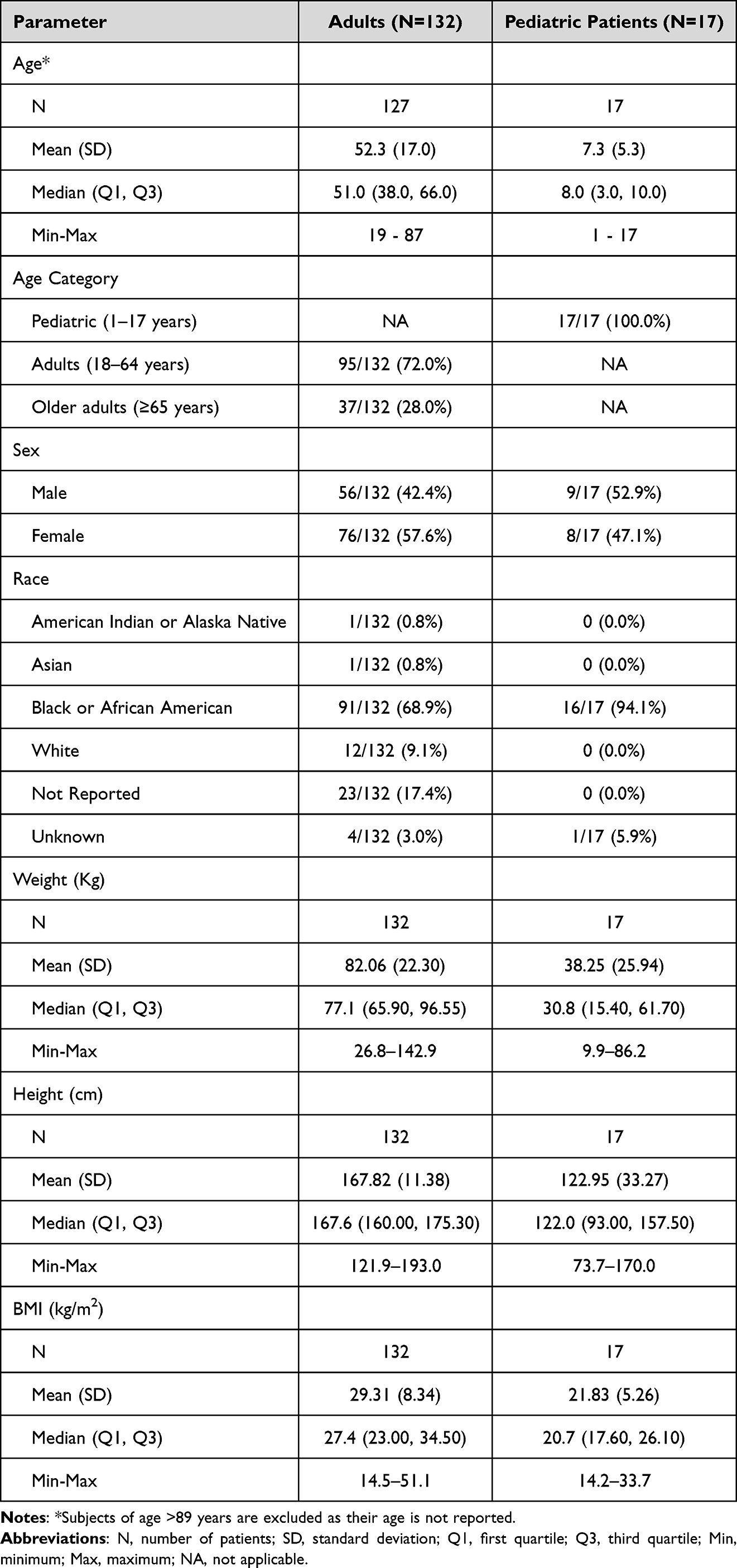 |
Table 2 Demography and Baseline Characteristics |
Procedure Overview
Ultrasound successfully visualized vasculature in all 149 participants, with an appropriate target vein identified successfully in each case. The Cue Needle Tracking technology was used in 29 (19.5%) of the cases. All catheters, including 140 PIVCs and nine midline catheters, were successfully cannulated with blood return observed (100%). There were no procedural adverse effects or complications reported (Table 3).
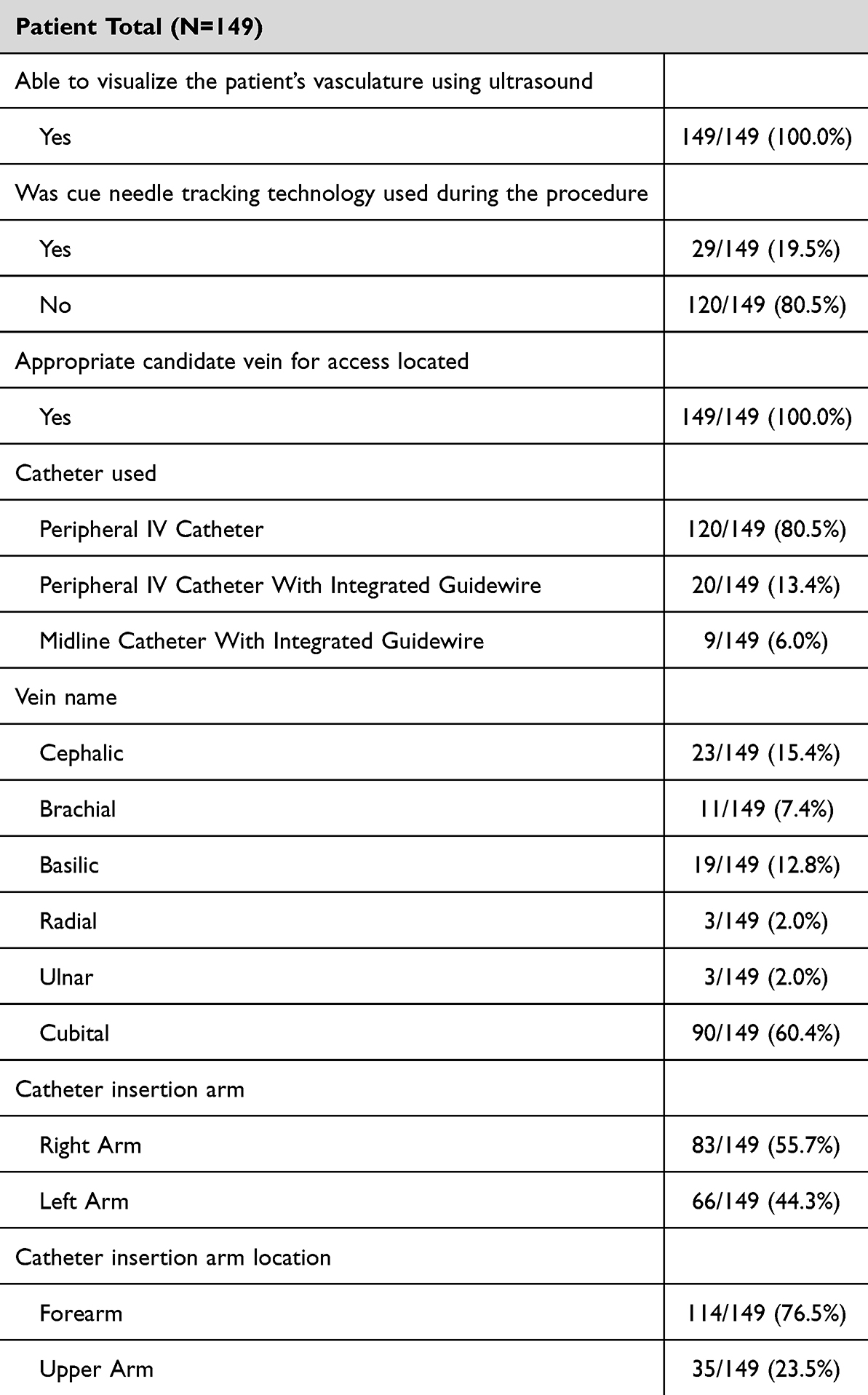 |
Table 3 Procedural Details |
Performance Results
The primary performance results revealed that the ultrasound device successfully visualized the target vasculature in all 149 participants (100%; 95% CI: 97.7%, 100.0%). Vascular access with a catheter as confirmed by blood return was achieved in all enrolled participants (100%; 95% CI: 97.6%, 100%). Vascular access at first attempt was successful in 142 (95.3%) participants, with 100% success in the 17 pediatric participants (Table 4).
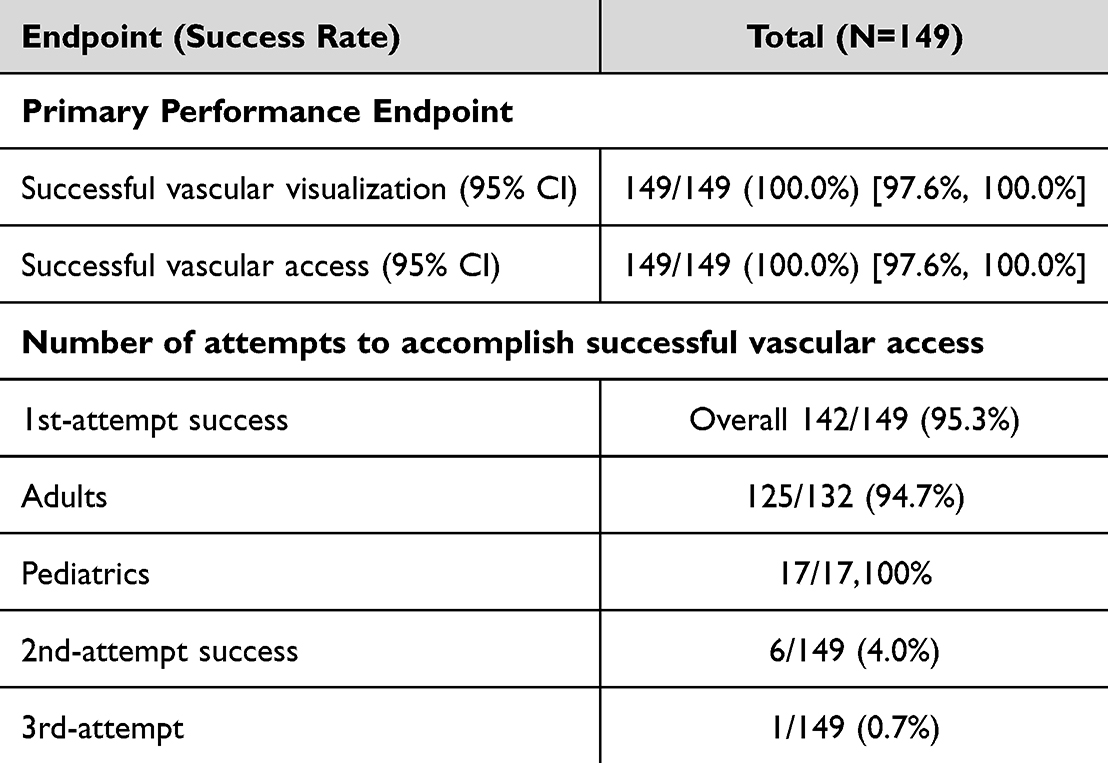 |
Table 4 Performance Results |
The results of first attempt success rates stratified by the number of DIVA risk factors for both adult and pediatric participants are represented in Table 1. The first attempt was successful in 125/132 (94.7%) adults and in 17/17 (100%) pediatric participants. Within the adult group, first attempt success was 100% with the 45 participants without DIVA risks. For the 87 adults with DIVA risk factors, the first-attempt success rate was 80/87 (92.0%). The total number of attempts were demonstrated to be a mean 1.05 ± 0.25.
Safety Results
The primary safety results showed that no adverse events occurred during the study, and no deaths were reported during the study. One device deficiency was observed with a Linear 25 mm probe at system power-on, where a probe assessment error indicated failure of at least one transducer element. Although the probe remained functional, image artifacts were noted. The clinician assessed the image quality and confirmed that it remained acceptable for clinical use. The affected probe was used in 11 (7.4%) participants before being replaced. This deficiency was resolved by replacing the probe and did not result in any adverse events or serious health threat to any of the participants.
Discussions
This study demonstrated high success across both primary performance endpoints: visualization of target vasculature and successful vascular access at a rate of 100%. In comparison, other studies have reported overall success rates for ultrasound-guided techniques ranging from 80% to over 90%.7,10,16,24 Multiple meta-analyses corroborate these findings in both adults and pediatric patients in achieving higher overall success rates with ultrasound guidance.25–28 The present study findings align with existing evidence supporting ultrasound-guided vascular access.7,10,14,26,29
The overall first-attempt success rate observed was 95.3% for the study population, with 100% success in pediatric patients and 94.7% in adult patients. As needle tracking was used in a subset of cases, the overall performance outcomes observed in this study reflect use of the ultrasound system as a whole rather than the isolated effect of this feature. The results suggest the portable ultrasound device can be successfully used for peripheral catheterization. When investigating the effectiveness in adult DIVA patients, first attempt success was 92.0% (80/87) in patients with at least one DIVA risk factor and 100% (45/45) in patients without DIVA risks. The first attempt success data are similar to rates reported in recent systematic reviews. In a recent meta-analysis of RCTs, the first attempt success rates were observed to be between 78.9% and 85.4% for ultrasound guided PIVC insertion in patients with DIVA risks.10 In an RCT with a pediatric patient population (0–18 years), the first attempt success rate for ultrasound guided PIVC insertion was 85.7%.14 The observed first-attempt success rates were higher than those reported in previous studies; however, differences in study design and population should be considered when interpreting these findings. The mean number of insertion attempts was 1.05±0.25 in this study and is on the lower end of the range reported among other studies between 1 to 2.37 insertion attempts.10,12,15 This is noteworthy and the performance data aligns with available literature indicating that the use of the portable ultrasound device achieves high first attempt insertion success and a reasonable mean number of insertion attempts in DIVA patients.5,7,12
No adverse events were observed in this study. While one (0.67%) device deficiency occurred with the 25mm probe, it was resolved without clinical impact. Ultrasound‑guided vascular access has been associated with reduced complication rates compared with traditional insertion techniques.14,26,29,30 A meta-analysis comparing ultrasound guided and landmark venipuncture found that the use of ultrasound guidance reduced the incidence of vascular injury (p<0.00001) and the probability of hematoma formation and pneumothorax formation during puncture (p=0.008).30 Another study found reduced self-reported pain during insertion in pediatric patients eight years or older when using ultrasound guided insertion compared with landmark insertion.14 Although, it should be noted that some research identified no difference between ultrasound guidance and landmark techniques for extravasation, pain, bleeding, local inflammation or accidental catheter removal (p>0.05).29
This study has several limitations including the use of a single urban medical center which limits generalizability of the results to other clinical settings, including rural hospitals or different geographic locations. The observational, non-interventional design limits causal inference between device performance and clinical outcomes. Key procedural variables (eg., catheter gauge, vessel size, insertion time, operator experience) were not collected, which limits interpretation of performance outcomes, including success rates. The short study duration and small sample size limit the ability to assess long-term clinical outcomes and economic impact. Another limitation was that clinician training background and user feedback data were not collected which may have introduced operator-related variability. These limitations should be considered when interpreting the results of the study.
The findings of this study suggest several potential clinical benefits associated with the use of this device. Successful vascular access may reduce the need for escalation to more invasive approaches, such as central venous catheter placement. In addition, the overall first-attempt success rates may contribute to improved patient satisfaction by reducing repeated attempts. From an operational perspective, the use of this technology may also support workflow efficiency by shortening procedure times and optimizing resource utilization in busy clinical settings. However, these implications are inferred from the observed outcomes and were not directly evaluated in this study. Future randomized controlled studies, with targeted patient populations and clinician user groups across broader clinical settings, should be conducted to further investigate the effectiveness and utility of this portable ultrasound device.
Conclusions
This single-center, prospective, observational study suggests that a portable ultrasound device with needle tracking is safe and can be successfully used for peripheral intravenous access. The device was associated with high first-attempt success rates in this study, with 100% observed success in non-DIVA patients, and no device related adverse events were reported. Future randomized comparative studies with larger sample sizes are warranted to further investigate its use.
Data Sharing Statement
The datasets generated during the current study are available from the corresponding author on reasonable request.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and IRB approval was obtained through an external IRB, Advarra, as authorized by the Brookdale University Hospital and Medical Center IRB (Ref. no. Pro00088014), which approved the study.
Consent to Participate
The consent form was written and fully discussed with every patient in depth prior to participation. Patients were required to verbally confirm their voluntary agreement to participate; however, patient signatures were not required. The user explaining the consent would then check off that the patient understood. This approach was approved by the IRB/Ethics Committee given the non-interventional nature of the study and that the procedures were planned as part of routine care. The Principal Investigator or designated representative documented the consent process by signing and dating the IRB/EC-approved informed consent form.
Acknowledgments
We gratefully acknowledge Frank Garofalo and Nicholas Vaccari, MD, for their intellectual and administrative support throughout this project. We also thank DeJuan Kinchelow, MD; Mona Rosenzweig, MD; and Aluko Gift, MD, for their contributions to subject recruitment and enrollment. Their support was essential to the successful completion of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Becton, Dickinson and Company (BD), Franklin Lakes, NJ, USA.
Disclosure
TJS is an employee of and owns stock options from Becton, Dickinson and Company (BD), Franklin Lakes, NJ, USA. The authors report no other conflicts of interest in this work.
References
1. Bruant A, Normand L. Recent advances in ultrasound-guided peripheral intravenous catheter insertion. Nurs Rep. 2025;15(10):359. doi:10.3390/nursrep15100359
2. Webster J, Osborne S, Rickard CM, et al. Clinically-indicated replacement versus routine replacement of peripheral venous catheters. Cochrane Database Syst Rev. 2019;2019(1). doi:10.1002/14651858.CD007798.pub5
3. Marsh N, Webster J, Ullman AJ, et al. Peripheral intravenous catheter non-infectious complications in adults: a systematic review and meta-analysis. J Adv Nurs. 2020;76(12):3346–10. doi:10.1111/jan.14565
4. Pinelli F, Firenzuoli F, Romagnoli S, et al. Appropriate selection of vascular access devices in the hospitalized patient: a prospective observational pilot study. J Anesth Analg Crit Care. 2026;6(1). doi:10.1186/s44158-026-00365-z.
5. Álvarez-Morales L, Gómez-Urquiza JL, Suleiman-Martos N, et al. Ultrasound-guided peripheral intravenous canulation by emergency nurses: a systematic review and meta-analysis. Int Emerg Nurs. 2024;73:101422. doi:10.1016/j.ienj.2024.101422
6. Casal-Guisande C, López-Domene E, Fernández-Antorrena S, et al. Peripheral vascular access in infants: is ultrasound-guided cannulation more effective than the conventional approach? A systematic review. Medicina. 2025;61(8). doi:10.3390/medicina61081321.
7. Berlanga-Macias C, Díez-Fernández A, Martínez-Hortelano JA, et al. Ultrasound-guided versus traditional method for peripheral venous access: an umbrella review. BMC Nurs. 2022;21(1):307. doi:10.1186/s12912-022-01077-9
8. Au AK, Rotte MJ, Grzybowski RJ, et al. Decrease in central venous catheter placement due to use of ultrasound guidance for peripheral intravenous catheters. Am J Emergency Med. 2012;30(9):1950–1954. doi:10.1016/j.ajem.2012.04.016
9. Pare JR, Pollock SE, Liu JH, et al. Central venous catheter placement after ultrasound guided peripheral IV placement for difficult vascular access patients. Am J Emergency Med. 2019;37(2):317–320. doi:10.1016/j.ajem.2018.11.021
10. Anderssen LM, Petersen MS, Wang AG, Mohr M, Fjallheim AS. The efficacy of ultrasound-guided peripheral intravenous cannulation versus the landmark technique in emergency department patients with difficult intravenous access: a systematic review and meta-analysis. J Vasc Access. 2025;11297298251347816. doi:10.1177/11297298251347816
11. Tian Y, Zhong Z, Dougarem D, et al. The ultrasound-guided versus standard technique for peripheral intravenous catheter placement by nurses: a systematic review and meta-analysis. Heliyon. 2024;10(9):e30582. doi:10.1016/j.heliyon.2024.e30582
12. Zaki HA, Elmelliti H, Ponappan B, et al. Outcomes of POCUS -Guided peripheral intravenous access in difficult venous access patients: a systematic review and meta-analysis. J Clin Ultrasound. 2025;53(8):1846–1859. doi:10.1002/jcu.24059
13. Mitchell EO, Jones P, Snelling PJ. Ultrasound for pediatric peripheral intravenous catheter insertion: a systematic review. Pediatrics. 2022;149(5). doi:10.1542/peds.2021-055523
14. Kleidon TM, Schults JA, Royle RH, et al. First-Attempt success in ultrasound-guided vs standard peripheral intravenous catheter insertion: the EPIC superiority randomized clinical trial. JAMA Pediatr. 2025;179(3):255–263. doi:10.1001/jamapediatrics.2024.5581
15. Poulsen E, Aagaard R, Bisgaard J, et al. The effects of ultrasound guidance on first-attempt success for difficult peripheral intravenous catheterization: a systematic review and meta-analysis. Eur J Emerg Med. 2023;30(2):70–77. doi:10.1097/MEJ.0000000000000993
16. Kuo CC, Lee WJ, Ke YT. Ultrasound-guided peripheral intravenous access in adults: a randomized crossover controlled trial. Int Emerg Nurs. 2025;79:101571. doi:10.1016/j.ienj.2025.101571
17. Salleras-Duran L, Fuentes-Pumarola C, Fontova-Almató A, et al. Pain and satisfaction perceptions of ultrasound-guided versus conventional peripheral intravenous catheterization: a randomized controlled trial. Pain Manag Nurs. 2024;25(1):e37–e44. doi:10.1016/j.pmn.2023.07.010
18. Vegas A, Wells B, Braum P, et al. Guidelines for performing ultrasound-guided vascular cannulation: recommendations of the American society of echocardiography. J Am Soc Echocardiogr. 2025;38(2):57–91. doi:10.1016/j.echo.2024.12.004
19. Lamperti M, Biasucci DG, Disma N, et al. European Society of Anaesthesiology guidelines on peri-operative use of ultrasound-guided for vascular access (PERSEUS vascular access). Eur J Anaesthesiol EJA. 2020;37(5):344–376. doi:10.1097/EJA.0000000000001180
20. Nickel B, Gorski L, Kleidon T, et al. Infusion therapy standards of practice, 9th edition. J Infus Nurs. 2024;47(1):S1–s285. doi:10.1097/NAN.0000000000000532
21. Schults JA, Marsh N, Ullman AJ, et al. Improving difficult peripheral intravenous access requires thought, training and technology (DART(3)): a stepped-wedge, cluster randomised controlled trial protocol. BMC Health Serv Res. 2023;23(1):587. doi:10.1186/s12913-023-09499-0
22. Schoch M, Fielding C, Marticorena RM, et al. Barriers and facilitators to vascular access point-of-care ultrasound in haemodialysis: an international survey of haemodialysis clinicians. J Ren Care. 2024;50(4):405–412. doi:10.1111/jorc.12503
23. Kimbowa A, Pieters A, Tadayon P, et al. Advancements in needle visualization enhancement and localization methods in ultrasound: a literature review. Artificial Intelligence Surg;2024. 149–169. doi:10.20517/ais.2024.20
24. Privitera D, Mazzone A, Pierotti F, et al. Ultrasound-guided peripheral intravenous catheters insertion in patient with difficult vascular access: short axis/out-of-plane versus long axis/in-plane, a randomized controlled trial. J Vasc Access. 2022;23(4):589–597. doi:10.1177/11297298211006996
25. Van Loon FHJ, Buise MP, Claassen JJF, et al. Comparison of ultrasound guidance with palpation and direct visualisation for peripheral vein cannulation in adult patients: a systematic review and meta-analysis. Br J Anaesth. 2018;121(2):358–366. doi:10.1016/j.bja.2018.04.047
26. Tran QK, Flanagan K, Fairchild M, et al. Nurses and efficacy of ultrasound-guided versus traditional venous access: a systemic review and meta-analysis. J Emerg Nurs. 2022;48(2):145–158.e1. doi:10.1016/j.jen.2021.12.003
27. Ye X, Li M. Comparison of ultrasound guided and conventional techniques for peripheral venous catheter insertion in pediatric patients: a systematic review and meta-analysis of randomized controlled trials. Front Pediatr. 2021;9:797705. doi:10.3389/fped.2021.797705
28. Stolz LA, Stolz U, Howe C, et al. Ultrasound-guided peripheral venous access: a meta-analysis and systematic review. J Vasc Access. 2015;16(4):321–326. doi:10.5301/jva.5000346
29. Bridey C, Thilly N, Lefevre T, et al. Ultrasound-guided versus landmark approach for peripheral intravenous access by critical care nurses: a randomised controlled study. BMJ Open. 2018;8(6):e020220. doi:10.1136/bmjopen-2017-020220
30. Xiong X, Xiong Y, Liu G. Systematic review and meta-analysis: safety of ultrasound-guided peripheral venipuncture and catheterization. Ann Palliat Med. 2021;10(11):11721–11732. doi:10.21037/apm-21-3163
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.